Embed Size (px)
Citation preview

342 J Formos Med Assoc | 2011 • Vol 110 • No 5
Contents lists available at ScienceDirect
Journal of the Formosan Medical Association
Journal homepage: http://www.jfma-online.com
J Formos Med Assoc 2011;110(5):342–346
Journal of the Formosan Medical Association
ISSN 0929 6646
Formosan Medical AssociationTaipei, Taiwan
Volume 110 Number 5 May 2011
XMRV: Not a mousy virusPrevalence of telomerase activity in human cancerIncreased risk of mortality in overweight adultsIschemic stroke with dural arteriovenous fistulas
Case Report
Craniofacial Skeletal Dysplasia of Opposite-sexDizygotic TwinsSzu-Ting Chou,1 Yu-Chuan Tseng,1 Chin-Yun Pan,1 Jenny Zwei-Chieng Chang,2 Hong-Po Chang1*
Craniofacial skeletal dysplasia can lead to different skeletal malocclusions. Both environmental factorsand heredity contribute to the formation of malocclusions. There are strong familial tendencies in the development of Angle’s Class II and III malocclusions. Cases such as opposite-typed (Class II and III) mal-occlusions with skeletal and dentoalveolar discordance in siblings or dizygotic (DZ) twins have seldombeen reported. We describe the rare case of a pair of opposite-sex DZ twins with completely different skeletalmalocclusions, and discuss the clinical considerations for treatment. The patients were twins aged 13 yearsand 4 months. The girl had mandibular prognathism and a Class III dentoskeletal relationship, whereasthe boy had skeletal Class II with mandibular retrusion. Several morphological traits have been implicatedwith hormonal effect. However, there was no evidence of whether the masculinization effect had any impact on jaw size in the female fetus or whether this effect lasted into adolescence. We suggest that, although DZ twins share the same growth environment, genetic or other unknown extrinsic factors canresult in discordance of characteristics of the craniofacial skeleton, dentition, and occlusion.
Key Words: dizygotic twins, malocclusion, opposite-sex twins, orthodontic treatment, skeletal dysplasia
Skeletal dysplasia of craniofacial structures can
lead to different types of malocclusion.1 Skeletal
components of Class II malocclusion include:
mandibular retrusion with a normally developed
midface,2 maxillary protrusion with a normally
positioned mandible, or a protrusive maxilla with
reduced total mandibular length.3 On the contrary,
mandibular prognathism, maxillary retrognathism,
or a combination of both might contribute to the
formation of Class III malocclusion.4
Both hereditary and environmental influences
have been suggested as etiological factors of skele-
tal dysplasia and its associated malocclusions.5–8
Kawala et al have used twin-method analysis to
examine malocclusions and have shown that the
differences in monozygotic (MZ) twins depend
©2011 Elsevier & Formosan Medical Association. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1Department of Orthodontics, Kaohsiung Medical University Hospital, and Faculty of Dentistry, College of Dental Medicine,Kaohsiung Medical University, Kaohsiung, and 2Department of Orthodontics, National Taiwan University Hospital, andSchool of Dentistry, College of Medicine, National Taiwan University, Taipei, Taiwan.
Received: August 7, 2008Revised: February 25, 2009Accepted: April 8, 2009
*Correspondence to: Dr Hong-Po Chang, Department of Orthodontics, Kaohsiung MedicalUniversity Hospital, 100 Tzyou 1st Road, Kaohsiung 80756, Taiwan.E-mail: [email protected]
Skeletal dysplasia of dizygotic twins
J Formos Med Assoc | 2011 • Vol 110 • No 5 343
on environmental activity, whereas in dizygotic
(DZ) twin pairs, they can be because of genetic
or environmental factors.5
It is accepted that strong familial tendencies
exist in the development of Angle’s Class II and
Class III malocclusions,6 and there are highly sig-
nificant correlations between those parents and
offspring and between siblings.9 Cases such as
opposite-typed (Class II and III) malocclusions
with skeletal and dentoalveolar discordance in
siblings of the same family or in DZ twins have
seldom been reported. Harris and Kowalski even
have reported that it is rare to find a patient who
differs greatly from the rest of his or her family.10
We present the rare case of a pair of opposite-sex
(OS) DZ twins with opposite-typed skeletal mal-
occlusions, and discuss the clinical considerations
for treatment.
Case Report
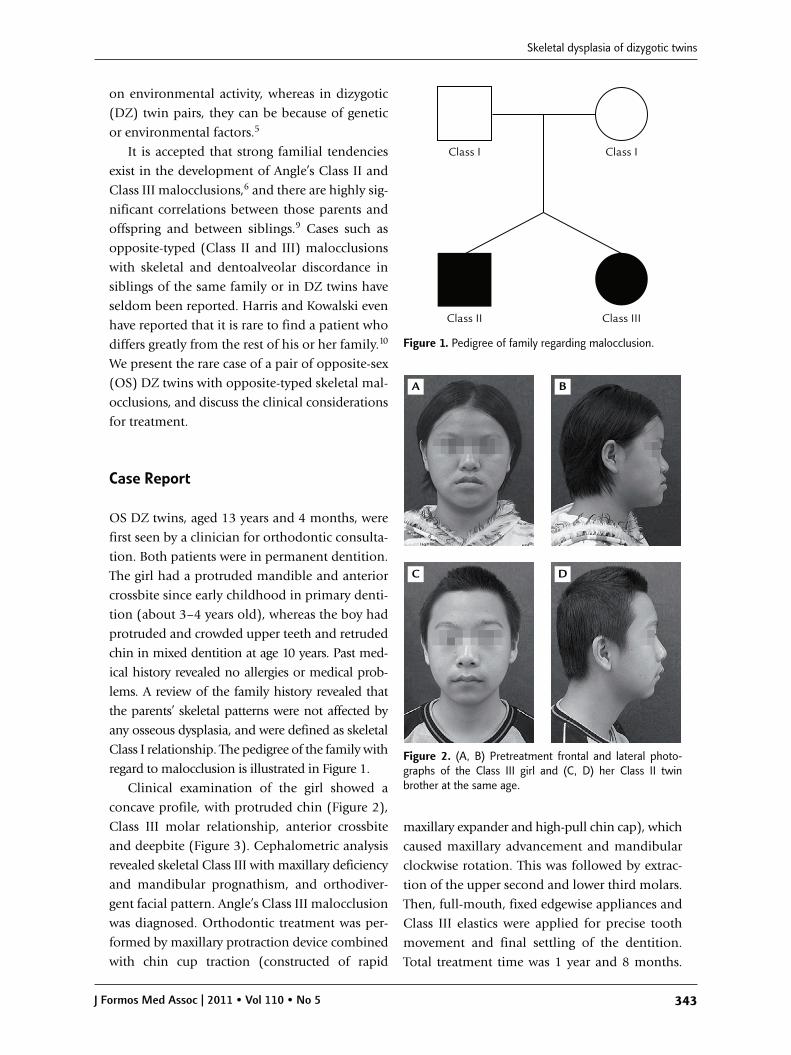
OS DZ twins, aged 13 years and 4 months, were
first seen by a clinician for orthodontic consulta-
tion. Both patients were in permanent dentition.
The girl had a protruded mandible and anterior
crossbite since early childhood in primary denti-
tion (about 3–4 years old), whereas the boy had
protruded and crowded upper teeth and retruded
chin in mixed dentition at age 10 years. Past med-
ical history revealed no allergies or medical prob-
lems. A review of the family history revealed that
the parents’ skeletal patterns were not affected by
any osseous dysplasia, and were defined as skeletal
Class I relationship. The pedigree of the family with
regard to malocclusion is illustrated in Figure 1.
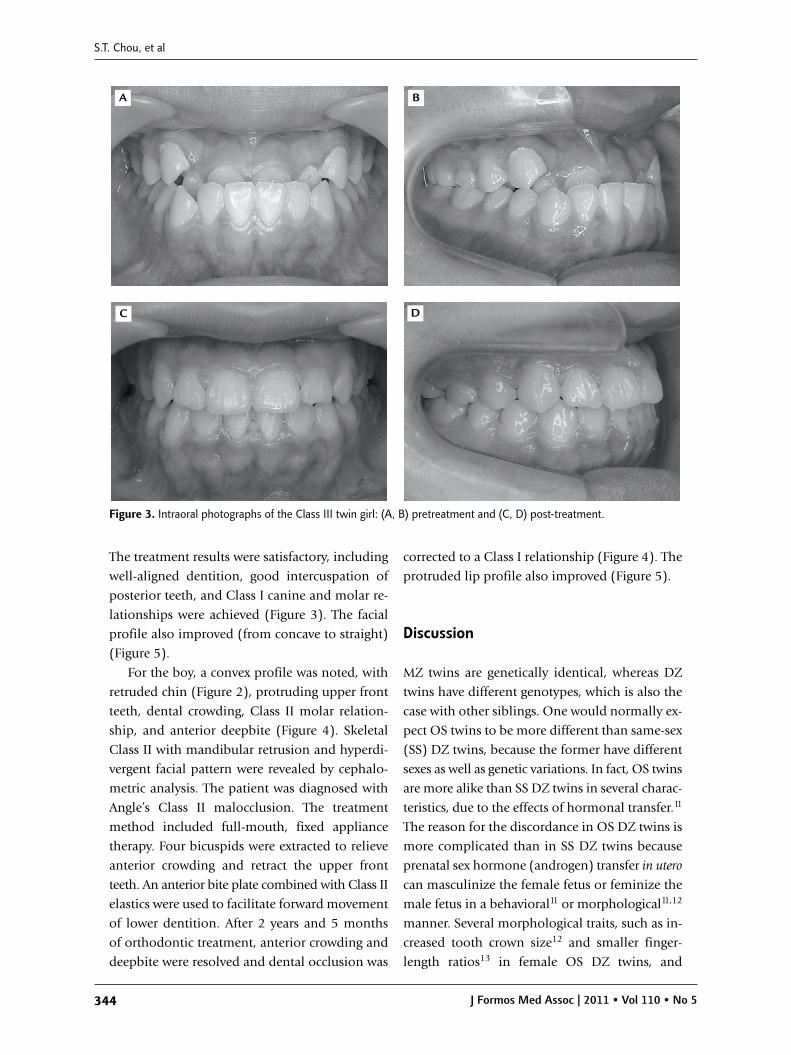
Clinical examination of the girl showed a
concave profile, with protruded chin (Figure 2),
Class III molar relationship, anterior crossbite
and deepbite (Figure 3). Cephalometric analysis
revealed skeletal Class III with maxillary deficiency
and mandibular prognathism, and orthodiver-
gent facial pattern. Angle’s Class III malocclusion
was diagnosed. Orthodontic treatment was per-
formed by maxillary protraction device combined
with chin cup traction (constructed of rapid
maxillary expander and high-pull chin cap), which
caused maxillary advancement and mandibular
clockwise rotation. This was followed by extrac-
tion of the upper second and lower third molars.
Then, full-mouth, fixed edgewise appliances and
Class III elastics were applied for precise tooth
movement and final settling of the dentition.
Total treatment time was 1 year and 8 months.
Class I Class I
Class II Class III
Figure 1. Pedigree of family regarding malocclusion.
A B
C D
Figure 2. (A, B) Pretreatment frontal and lateral photo-graphs of the Class III girl and (C, D) her Class II twinbrother at the same age.
S.T. Chou, et al
344 J Formos Med Assoc | 2011 • Vol 110 • No 5
The treatment results were satisfactory, including
well-aligned dentition, good intercuspation of
posterior teeth, and Class I canine and molar re-
lationships were achieved (Figure 3). The facial
profile also improved (from concave to straight)
(Figure 5).
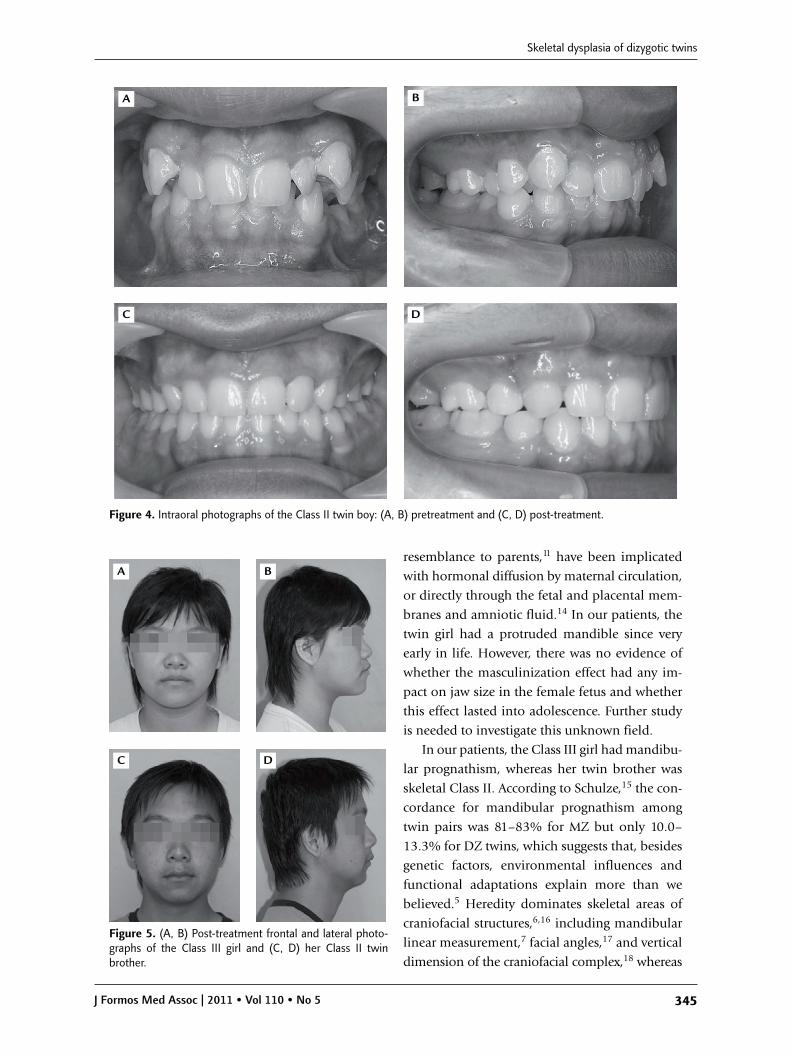
For the boy, a convex profile was noted, with
retruded chin (Figure 2), protruding upper front
teeth, dental crowding, Class II molar relation-
ship, and anterior deepbite (Figure 4). Skeletal
Class II with mandibular retrusion and hyperdi-
vergent facial pattern were revealed by cephalo-
metric analysis. The patient was diagnosed with
Angle’s Class II malocclusion. The treatment
method included full-mouth, fixed appliance
therapy. Four bicuspids were extracted to relieve
anterior crowding and retract the upper front
teeth. An anterior bite plate combined with Class II
elastics were used to facilitate forward movement
of lower dentition. After 2 years and 5 months
of orthodontic treatment, anterior crowding and
deepbite were resolved and dental occlusion was
corrected to a Class I relationship (Figure 4). The
protruded lip profile also improved (Figure 5).
Discussion
MZ twins are genetically identical, whereas DZ
twins have different genotypes, which is also the
case with other siblings. One would normally ex-
pect OS twins to be more different than same-sex
(SS) DZ twins, because the former have different
sexes as well as genetic variations. In fact, OS twins
are more alike than SS DZ twins in several charac-
teristics, due to the effects of hormonal transfer.11
The reason for the discordance in OS DZ twins is
more complicated than in SS DZ twins because
prenatal sex hormone (androgen) transfer in utero
can masculinize the female fetus or feminize the
male fetus in a behavioral11 or morphological11,12
manner. Several morphological traits, such as in-
creased tooth crown size12 and smaller finger-
length ratios13 in female OS DZ twins, and
A B
C D
Figure 3. Intraoral photographs of the Class III twin girl: (A, B) pretreatment and (C, D) post-treatment.
Skeletal dysplasia of dizygotic twins
J Formos Med Assoc | 2011 • Vol 110 • No 5 345
resemblance to parents,11 have been implicated
with hormonal diffusion by maternal circulation,
or directly through the fetal and placental mem-
branes and amniotic fluid.14 In our patients, the
twin girl had a protruded mandible since very
early in life. However, there was no evidence of
whether the masculinization effect had any im-
pact on jaw size in the female fetus and whether
this effect lasted into adolescence. Further study
is needed to investigate this unknown field.
In our patients, the Class III girl had mandibu-
lar prognathism, whereas her twin brother was
skeletal Class II. According to Schulze,15 the con-
cordance for mandibular prognathism among
twin pairs was 81–83% for MZ but only 10.0–
13.3% for DZ twins, which suggests that, besides
genetic factors, environmental influences and
functional adaptations explain more than we
believed.5 Heredity dominates skeletal areas of
craniofacial structures,6,16 including mandibular
linear measurement,7 facial angles,17 and vertical
dimension of the craniofacial complex,18 whereas
A B
C D
Figure 4. Intraoral photographs of the Class II twin boy: (A, B) pretreatment and (C, D) post-treatment.
C D
BA
Figure 5. (A, B) Post-treatment frontal and lateral photo-graphs of the Class III girl and (C, D) her Class II twinbrother.

S.T. Chou, et al
346 J Formos Med Assoc | 2011 • Vol 110 • No 5
environmental factors dominate the dental areas
of craniofacial structures.16 It has also been re-
ported that a strong genetic component overlaid
by functional adaptation is most prominent in
the dental area.8
Skeletal pattern is believed to be more re-
lated to genetic factors, but significant differences
between Class II and Class III patients have been
found for SNA angle, gonial angle, Ar-Go length,
and U1-nasal floor angle, and are assumed to be
influenced by the environment.6 For example,
nasoairway obstruction (enlarged tonsils) results
in mouth breathing and anterior positioning of
the tongue, which leads to protrusion of the man-
dible in skeletal Class III;19 nasoairway obstruc-
tion (adenoids), thumb-and-finger sucking, and
lip biting habits also induce downward–backward
rotation of the mandible and overgrowth of the
maxillary alveolar process in skeletal Class II.20
Distinguishing the variations that result from
genetic and environmental factors in Class II and
III malocclusions is important for clinical ortho-
dontists, because it is the region that is affected
by environmental factors that can be improved
by orthodontic treatment.6
Baccetti et al21 have assessed the ideal treatment
timing in dentofacial orthopedics and have con-
cluded that Class II treatment is most effective dur-
ing the circumpubertal growth period (CVM stage:
CS3–CS4 interval), in which the mandible is at
maximum growth spurt. However, prepubertal
treatment of skeletal Class III is effective in both
jaws, but later into puberty, the treatment effect is
greater in the mandible only.21 We must keep in
mind that redirection of mandibular growth pat-
tern can only be modified within biologically tol-
erated limits,8 therefore, long-term follow-up of
maxillary and mandibular developmental changes
is important until the cessation of skeletal growth.
References
1. Proffit WR. The etiology of orthodontic problems. In:Contemporary Orthodontics, 4th edition. St. Louis: Mosby,2007:160.
2. McNamara JA. Components of Class II malocclusion in children 8–10 years of age. Angle Orthod 1981;51:177–202.
3. Yu YC, Chang HP. Morphology of the midfacial complexand mandible in children with Angle Class II division 1malocclusion. J Taiwan Assoc Orthod 2005;17:31–8.
4. Chang HP. Components of Class III malocclusion inTaiwanese. Kaohsiung J Med Sci 1985;1:144–55.
5. Kawala B, Antoszewska J, Necka A. Genetics or environ-ment? A twin-method study of malocclusions. World JOrthod 2007;8:405–10.
6. Nakasima A, Ichinose M, Nakata S, et al. Hereditary fac-tors in the craniofacial morphology of Angle’s Class II andClass III malocclusion. Am J Orthod 1982;82:150–6.
7. Nakata M, Yu P, Davis B, et al. The use of genetic data inthe prediction of craniofacial dimensions. Am J Orthod1973;63:471–80.
8. Lobb WK. Craniofacial morphology and occlusal variationin monozygous and dizygous twins. Angle Orthod 1987;57:219–33.
9. Saunders SR, Popovich F, Thompson GW. A family studyof craniofacial dimensions in the Burlington Growth Centresample. Am J Orthod 1980;78:394–403.
10. Harris JE, Kowalski CJ. All in the family: use of familial in-formation in orthodontic diagnosis, case assessment, andtreatment planning. Am J Orthod 1976;69:493–510.
11. Miller EM. Prenatal sex hormone transfer: a reason to studyopposite-sex twins. Per Individ Differ 1994;17:511–29.
12. Dempsey PJ, Townsend GC, Richards LC. Increased toothcrown size in females with twin brothers: evidence forhormonal diffusion between human twins in utero. Am JHum Biol 1999;11:577–86.
13. Anders SM, Vernon PA, Wilbur CJ. Finger-length ratiosshow evidence of prenatal hormone-transfer between opposite-sex twins. Horm Behav 2006;49:315–9.
14. Meulenberg PMM, Hofman JA. Maternal testosteroneand fetal sex. J Steriod Biochem Mol Biol 1991;39:51–4.
15. Schulze C. On prognathism in twins. Stoma 1965;18:250–66.
16. Jiang RP, Fu MK. A genetic feature study in Class II, division1 malocclusion. J Modern Stomatol 2001;115:368–70.
17. Stein KF, Kelly TJ, Wood E. Influence of heredity in the etiology of malocclusion. Am J Orthod 1956;42:125–41.
18. Manfredi C, Martina R, Grossi GB, et al. Heritability of 39orthodontic cephalometric parameters on MZ, DZ twinsand MN-paired singletons. Am J Orthod Dentofac Orthop1997;111:44–51.
19. McNamara JA Jr. A method of cephalometric evaluation.Am J Orthod 1984;86:449–69.
20. Moyers RE. Handbook of Orthodontics, 3rd edition. Chicago:Year Book Medical Publishers Inc, 1973.
21. Baccetti T, Franchi L, McNamara JA Jr. The cervical verte-bral maturation (CVM) method for the assessment of opti-mal treatment timing in dentofacial orthopedics. SeminOrthod 2005;11:119–29.