Embed Size (px)
Citation preview

1,n~dian d. Peril_at. 35: 186. 1968
C R A N I O - F A C I A L D Y S O S T O S I S : C R O U Z O N ' S D I S E A S E ,
igEPOI{T OF A CASE
lq. D. 81NOlt AND O. P . BAJPA1
lndore
CrouZOll ill 1912 lirst dcseril)ed this a, uomaly in a family where the mother and her two sons presented with de- ]ormity of head and tTaee and opl~thalmoplegia. Cranio-facial dy- sostosis consists of craniai dy,strophy rel]ecting early eraniostenosis, con]- plex ilystrophy of the face involvhlg I)Pincil}al]y flie superior maxillae and llaSaJ bones al]d terminating in the arrest of growth ol the involved bones, loss of extensibility of the vamit and reduction of the cranial cavity. The syl}ostosis all c~'ts the coronal and nmtopi{, sutures. Tt~o lamboid su- tm'e is usually nob involved. In additi(m to the cral~iota(:ia] anomalies other ass{}eiated eo]]g{mtial anomalies mi~lli, 1)e ~cen in these eases, e.g., s.yn(lactylis:]~ and other anomalies of the ext Petal ties.
This is a heredit~l'y disease but sporadic c a s e s a r e I.:l]OWl] to occur. f)o&e el, al. (t{)5{)) r{'i)()rted tha~ in one-fourth o1' tl~e ('ase~,;, no hereditary or familial element was present and also suggested that sporadic cases may be lai;elled Cr(mzon's disease provided tg6 easential eraniot'aeial feature.~ of tim disorder are present. I)ayal et al. (-19/;1) reported a family
* F~cm the Department of l'ediatrics, M. G. BI. Medical College and M. g. Iffosi)ital , Indore.
v,l~erc .t o1' the eight siblings suffered lr(ml the disease suggesting a heredi- t try origin. Pathogenesis of early sym}stosis is not known. This may I)egin during foetal life or during the lirst nlont.h of exmmterine life. Crouzon and I{enault thought it to be a result of inflammation around the suture lines. The sutures of the taeial bones are involved as well.
Ida Mann (19~8) suggested it to be du<: to 8 defective development of tlle mesoderm from which these bones HPOSO.
(,,I'OUZ o n s Clinically the cases of ~ disease present with a central pro- minence in the frontal region, a peculiar nose resembling a beak, bilateral cxophthahnos, divergent psc'udo-strabismus, hypoplasia of the maxilla resulting in the overlapping of the upper teeth by the lower jaw giving an appearance of apparent !)rogna~hism. Other ocular manifes- tations are papilloedema and optic atrophy. During early infancy these eases may present with convulsions. Older patients may complain of head- ache. Mental function remains nor-
real. As the skull does not expand l)rol)ortionate to tim growth of the brain, the intraera.nial pressure is increased wliieh causes digital mark-

SINGIt AND BAJPAI---C1L~NIO-FACIAL DYSOSTOSIS 187
lngs on tile tuner table of the skull. ~n some cases deafness is also noticed.
After the age of :3 years the cranial lesions are irreversible so that an early operation is indicated in these children. Results of early operation arc remarkable in controlling intra- crania[ tension, exophthalmos, optic: atrophy, mental deterioration and hernia of the frontal bones. The ,ppearanaee of the head is also im- })roved. Once the optic atrophy has set in, the changes are not reversed ,bv operation. Surgery is usually ])~'et'erred bet'ore the age of one year. Ch mnels arc cut through the bone r either side of tile affected suture and are lined by a polythene film to i)revent healing. Orbital deeompres- ,~ion is require~l sometimes and the na~al passages may have to be opened ~t times.
Report of a Case . .2
N., a inale, 6 months old, was seen on 4'.6.g7 with the complaints ()f lml~ing of both eyes since birth. There was a 5istory of cough and fever for 10 days. The patient was the first: issue. There was no history (>f similar complaints in the family. Tim perinatal and neonatal periods were uneventful. The child was totally breast-fed. He had started Imldin~ the neck but was not able to sit.
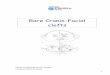
Physical examination revealed the following" weight 8 lhs, height 20", circumference of head la.y', pulse 130/rain, ~empera~aure 98~ and respira~/ory rate 3 0 / m i n . The fonta- helle was open with bilateral exophthalmos. The nose was beak- ahaped, the throat congested, maxillae hypoplastie and the lower jaw pro-
jeered forwards. (Fig. 1). A piloni- (la] sinus was atso present. Scattered crepltationa on both sides of the chest were heard. Other ssstems were normal.
Investigation. Hemoglobin was 1'2, (.L%, total leucocyte count 12,000/ cram., polymorphs 603/0, and lymph- ocytes 34%. Urine examination was normal. The fundus was also normal. X-ray of the skull show- e(l tlmt the vertical diameter of the skull was increased with a silver- l~eaten apl)earanee on the vault. The mandible was prominent and projec- ted forward beyond the hypoplastic maxilla.
Comment
Craniostenosis is not an uncommon disease but its association with other manifestations as has been deseri,bed in Crouzon's disease is not a common occurrence.
The ease under report presented with the classical clinical features of Crouzon's disease, viz. craniosteno- sis, bilateral exophf~halmos with a l)l)arent divergent strabismus, beak- shaped nose, hypoplastie maxillae and protruding lower jaw. Fundus examination /lid not show any evi- dence of optic atrophy probably be- cause the chiId was only six months old. This was a sporadic case in the family :lint as this was the firs~ child of the parents it is diffieultl to com- ment on the possible occurrence in future sibs.
Of 5 eases reported by Dodge et. a.1. (1.qS.q) 2 were hereditary In ongm whil.,~ the other 3 were sporadic. The former showed the presence of a fifth ventricle in th_e pneumoenocephalo- ~ram while the others did not reveal the presence of such a ventricle. In

INDIAN J O U R N A L OF PEDIATRICS PLATE I1
Fig. l . - -Cl inical features.
SINOH AND BAJPAI.--CRANIO--FACIAL DYSOSTOSIS~ CROUZON'S DISEASE

188 INDIAN JOURNAL OF PEDIATRICS VOL. 35 No. 243
this series, one case had bilateral papilloedema, 2 la~d pallor of the disc and 2 had normal fundi. The princi- pal cause of optic atrophy is ,~trangu- lation of the nerve and ophthalmic artery iia the optic canal which is crushed by pushing back of the small wing of the sphenoid. Our ease did not reveal any abno[mality in the hindus. Deafness m (h'ouzon's disease can be of a varying etiology. If it is tubotyrnpanic in origin, early re-estal)lisbment of nasal 1)crmeal)ili- ty may cheek its appearance. Early operation in those ea,ses where there is evidence of optic neuritis results in improvement in eye abnormalities.
Summary
A brief review of the literature on Crouzon's disease with report of a sporadic case in a male ehihl, aged (i months, is presented.
We arc thanl;ful to l'roI. J. N. Pohowalla, l)r. B. N. Jmlgalwalla an,l i)r. 1~. F;hattacharyya I(a + I, Jlcir gtlliJdllcC :.tlld |~Gt'lrtl6.%ioll 11o publish tho l,al,cr.
References
(3r, mzon, Q. and ]lenault. Quoted by M. M. Parks and b'. ]). C~>stcnbad(r (195o).
Crouzou, Q. Quoted by ]). L. lh'evcs (1961). I):ly.ll, ]2. :5., l'rasad, ]~. and 3[athur, G-. l*.
(l'ali]). (3raniolacml dvsostosis (Crouzon's disease). lm~ian J. (:It. lllth. 10, 489.
l)odge, H. W. ,Jr., Wood, M. \V. and Kennedy, ]r O. (1959). Crrniofaci'll dysoslo~is: Crouzons disease. Pcdi,trics, 23, 9~.
Ford, ],'. F:. (1:)~;6). ])i~easo~ of the Nerv<m.~ System in Inf:mcS, Chihlhood and Adolescence. 5th J':d. Charles C. Thomas. Springfield, 11I. p. 127.
]ngraham, iv., Alexamler, E., and Matron, D. ll:}18). Clinical ntudies ira craniostenosis. Surgery, 24, 51.q.
Lemariey, A., Paquqlin, F. and Thomas, 1~.. (1962). Crcmzon's disease. Ann. Ore. Laryng. 79, 773.
Mann, I. (I928). Developmental abnormalities of the eye. London, Cambridge, Univ. Pres~. p. 51.
Park~, M. M. and Coslenlmder, F. D. (1950). Craniofacial dysostnsi.% Amer. J. Ophlh, 33, 77.
liccvc.-:, D. L. (1961). Practice of Paediatrie.% Bremwmnnn, J., IV~ F. Prior (~o. Inc. Vol. VI, (q~. 2.5/A p. 1-4.