Embed Size (px)
Citation preview
SPECIAL ISSUE - ORIGINAL ARTICLE
Cranial translation of the humeral head on radiographs in rotatorcuff tear patients: the modified active abduction view
J. F. Henseler • P. B. de Witte • J. H. de Groot •
E. W. van Zwet • R. G. H. H. Nelissen •
J. Nagels
Received: 16 November 2012 / Accepted: 5 March 2013
� International Federation for Medical and Biological Engineering 2013
Abstract Cranial translation of the humeral head is rela-
ted to massive rotator cuff tears; however, it may be
unapparent in early-stage tears. The goal of this study was
to investigate whether active abduction leads to increased
active cranial humeral translation in early-stage tears. We
assessed 20 consecutive patients (9 full-thickness supra-
spinatus tears, 11 posterosuperior tears) using the newly
introduced modified active abduction view: acromiohu-
meral (AH) distance was measured on radiographs acquired
during rest and active isometric abduction and adduction
tasks with the arm alongside the body. Rest AH was 7.5 mm
(SD = 1.53); during abduction and adduction, it decreased
to 2.1 mm (95 % CI 1.28–3.01, p \ 0.001) and 1.1 mm
(95 % CI 0.46–1.65, p = 0.001), respectively. Cranial
translation during abduction was more severe in shoulders
with posterosuperior cuff tears (DAH = 3 mm, SD = 1.5)
compared to supraspinatus tears (DAH = 1 mm,
SD = 1.6), with a mean difference of 2 mm (95 % CI
0.64–3.58, p = 0.007). Both active isometric abduction
and adduction leads to active cranial translation in cuff tear
patients. Cranial translation is largest during active abduc-
tion. Furthermore, there is significant more cranial transla-
tion in posterosuperior cuff tear patients compared to
supraspinatus cuff tear patients. Possibly, radiographs
combined with active tasks offer new possibilities in diag-
nosing early-stage rotator cuff tears.
Keywords Rotator cuff � Shoulder pain � Radiography �Tear � Active abduction � Proximal migration
1 Introduction
Rotator cuff degeneration is responsible for a substantial
part of all shoulder complaints [14, 18]. It mainly affects a
population in the fifth to seventh decade of life, ranging
from subacromial impingement to full-thickness supraspi-
natus or posterosuperior (i.e., supraspinatus and infraspi-
natus) rotator cuff tears. Imaging studies demonstrated that
the prevalence of asymptomatic rotator cuff tears ranges up
to 54 % in the general population over 60 years-old [20].
Differentiation between symptomatic and asymptomatic
cuff rotator tears it difficult, even more since no causal
relation exists between shoulder symptoms and an observed
rotator cuff tear.
‘‘Fixed’’ proximal migration, which is synonymous to
passive cranial translation of the humeral head, with
respect to the glenoid leads to narrowing of the subacro-
mial space. It can be observed on standard radiographs and
is indicative for chronic massive rotator cuff tears [2, 10,
12, 13, 21, 27, 28]. Due to the lost supraspinatus and
infraspinatus function and degeneration of subacromial
tissues, the humeral head migrates cranially slowly over
time, sometimes even leading to actual contact between the
J. F. Henseler (&) � P. B. de Witte � R. G.
H. H. Nelissen � J. Nagels
Department of Orthopaedics, Leiden University Medical Center,
Postzone J11-R, Postbus 9600, 2300 RC Leiden,
The Netherlands
e-mail: [email protected]
J. F. Henseler � P. B. de Witte � J. H. de Groot
Laboratory for Kinematics and Neuromechanics,
Leiden University Medical Center, Leiden, The Netherlands
J. H. de Groot
Department of Rehabilitation, Leiden University
Medical Center, Leiden, The Netherlands
E. W. van Zwet
Department of Medical Statistics and BioInformatics,
Leiden University Medical Center, Leiden, The Netherlands
123
Med Biol Eng Comput
DOI 10.1007/s11517-013-1057-2
humerus and the acromion. However, imminent cranial
translation may be unapparent in early-stage rotator cuff
tears [1]. It has been reported that active abduction, through
prime deltoid activation, can lead to increased ‘‘dynamic’’
cranial translation in rotator cuff tear patients, which is
especially pronounced in the case of infraspinatus weak-
ness. Bloom applied this phenomenon as a clinical tool: the
active abduction view (AAV) [1]. With this method, the
acromiohumeral distance is measured on radiographs
acquired with the subjects’ arm in 90� of active abduction
or, if not capable of keeping the arm at 90�, with maximal
abduction. The AAV might have potential as an easily
available and inexpensive measure to quantify rotator cuff
dysfunction and diagnose early-stage rotator cuff tears [1,
26]. However, differences in abduction position, rotation
and scapular position can lead to large projection and
magnification errors when comparing AAV measurements
within and between subjects [16, 19].
In this experimental study, we propose to modify the
AAV method with active isometric arm abduction, with the
subjects’ arms alongside the body, to measure active cra-
nial translations of the humeral head while eliminating
some of the methodological problems of the AAV. Our first
hypothesis was that active isometric abduction will result
in active cranial translation in symptomatic rotator cuff
patients, resulting in a smaller subacromial space during
isometric abduction as compared to a position in rest. In
contrast, isometric adduction will result in caudal transla-
tion, due to the caudally directed muscle lines of action of
the adductor muscles. Our second hypothesis was that
posterosuperior tear patients show more active cranial
translation compared to supraspinatus tear patients. We
further hypothesized that there is a strong positive relation
between active cranial translation of the humeral head and
shoulder pain.
2 Methods
In this experimental study, twenty consecutive patients
with a full-thickness supraspinatus or posterosuperior
rotator cuff tear were included by two experienced shoul-
der surgeons (JN and RN) at the outpatient clinic of the
Orthopaedic department at the Leiden University Medical
Center (LUMC) between April 2011 and February 2012.
Inclusion criteria were: shoulder symptoms C6 months,
aged [50 years, diffuse unilateral shoulder pain, pain at
night or incapable of lying on the shoulder and pain during
activities with arm abduction, elevation and/or internal
rotation (e.g., overhead activities). With clinical examina-
tion, patients had to have the following findings: a positive
Hawkins test, clinically observed scapulohumeral dyski-
nesia characterized by increased and/or decreased scapular
lateral rotations, a classic painful arc at abduction and a
positive empty can test. The diagnosis was confirmed with
magnetic resonance imaging with arthrography (MRA)
and/or ultrasound. All patients had a full-thickness tear of
the supraspinatus and 11 patients (55 %) also had a tear of
the infraspinatus (i.e., posterosuperior tear) (Table 1).
There were 11 (55 %) males and 9 (45 %) females and the
mean age was of the total group was 65 (SD = 9.8).
Patients were excluded if one or more of the following
criteria were found on the concerning shoulder: prior
shoulder dislocations or positive apprehension test or sul-
cus sign (shoulder instability), previous surgery, subscap-
ularis tendon tear, osseous pathology, history of fracture,
osteoarthritis or rheumatoid arthritis of the glenohumeral or
acromioclavicular joint, capsulitis adhesiva (frozen shoul-
der syndrome), or a subacromial injection with anesthetics
and/or corticosteroids \6 weeks before intake. Further-
more, patients were excluded in case of cervical radicu-
lopathy, neuromuscular pathologies, or insufficient Dutch
language skills.
49 patients were considered for inclusion. Ten patients
declined informed consent and nineteen patients did not
fulfill the eligibility criteria: seven had a full-thickness
subscapularis tear, four patients had previous shoulder
surgery, four patients had a symptomatic acromioclavicular
osteoartritis, two patients had rheumatoid arthritis, one
Table 1 Patient characteristics
Supraspinatus
tear (n = 9)
Posterosuperior
tear (n = 11)
Total group
(n = 20)
Mean age (SD) 65 (9.5) 65 (10) 65 (9.8)
Sex, n (%)
Male 2 (22) 9 (82) 11 (55)
Female 7 (78) 2 (18) 9 (45)
Dominant arm affected, n (%)
Yes 5 (55) 7 (64) 18 (90)
No 4 (44) 4 (36) 2 (10)
Duration of symptoms, mo
Median (range) 36 (9–300) 24 (6–300) 30 (6–300)
CS (SD) 62 (17) 63 (15) 62 (15)
IPQ (SD) 47 (15) 41 (12) 44 (13)
WORC (SD) 58 (21) 57 (24) 57 (22)
Abduction
strength, N (SD)
90 (39) 73 (41) 81 (40)
Pain, VAS (SD)
VAS in rest 3.1 (2.3) 3.9 (2.8) 3.5 (2.5)
VAS during ADL 4.5 (3.4) 4.0 (2.3) 4.2 (2.7)
SD standard deviation, n number, mo months, CS constant score, IPQillness perception questionnaire, WORC Western Ontario Rotator
Cuff index, N Newton, VAS visual analog scale, ADL activities of
daily living
Med Biol Eng Comput
123
patient had Parkinson’s disease and one patient had prior
shoulder dislocations.
The institutional review board approved all stages of the
study. All subjects received oral and written information
about the study and signed informed consent. A sample
size of 20 participants was estimated with a power of 90 %
and two times the maximum previously reported SD of
1.14 mm for the acromiohumeral distance applied as the
standardized difference [16].
Prior to the radiograph series, a maximum voluntary
force (MVF) was measured for abduction and adduction.
For each subject, a series of three radiographs was acquired
to compare the position of the humeral head with respect to
the scapula in a subsequent order at rest and during iso-
metric abduction and adduction, respectively at 60 ±
3.75 % of the lowest absolute value of abduction and
adduction MVF. The target force for the abduction and
adduction tasks (Fmax) was equal in both directions. The
subjects performed at least one full practice trial before
imaging. Before these dynamic radiographs were made, the
constant score (CS), Western Ontario Rotator Cuff index
(WORC) and illness perception questionnaire (IPQ) were
acquired. VAS scores for pain at rest and during daily
activities in the last 2 weeks were obtained using a 10 cm
line, with 0 cm indicating no pain and 10 cm indicating
severe incapacitating pain. In addition, after each radio-
graph and task, a similar VAS score for shoulder pain was
recorded.
2.1 Radiography
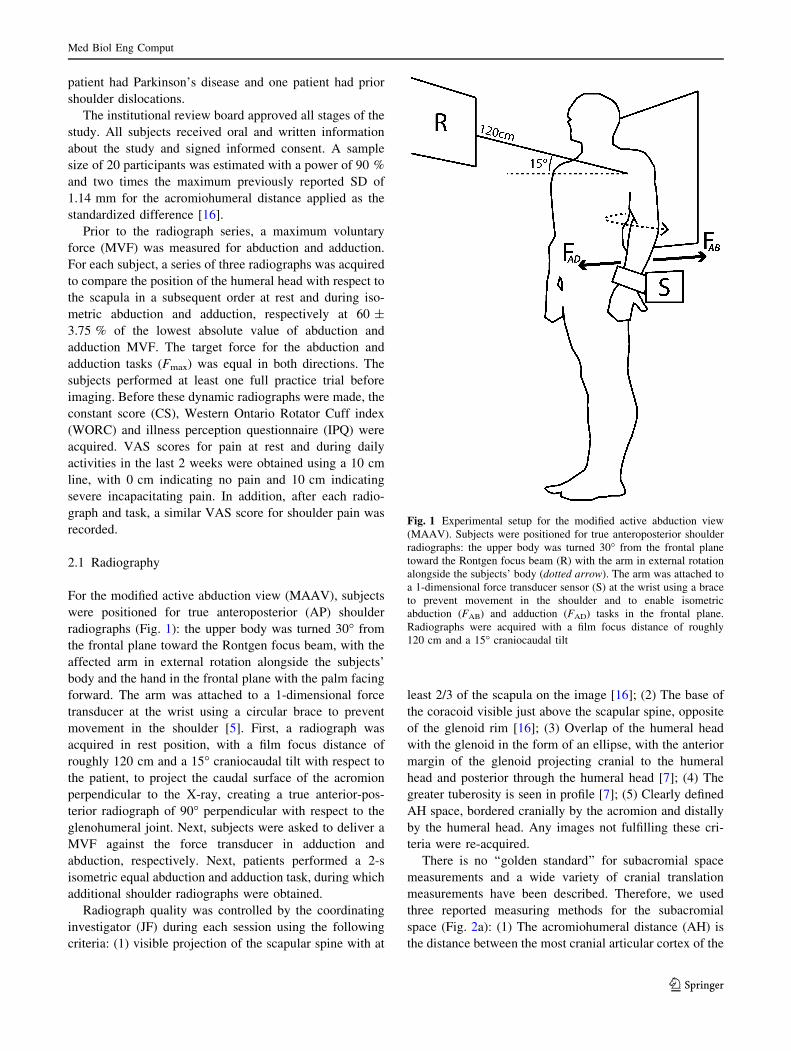
For the modified active abduction view (MAAV), subjects
were positioned for true anteroposterior (AP) shoulder
radiographs (Fig. 1): the upper body was turned 30� from
the frontal plane toward the Rontgen focus beam, with the
affected arm in external rotation alongside the subjects’
body and the hand in the frontal plane with the palm facing
forward. The arm was attached to a 1-dimensional force
transducer at the wrist using a circular brace to prevent
movement in the shoulder [5]. First, a radiograph was
acquired in rest position, with a film focus distance of
roughly 120 cm and a 15� craniocaudal tilt with respect to
the patient, to project the caudal surface of the acromion
perpendicular to the X-ray, creating a true anterior-pos-
terior radiograph of 90� perpendicular with respect to the
glenohumeral joint. Next, subjects were asked to deliver a
MVF against the force transducer in adduction and
abduction, respectively. Next, patients performed a 2-s
isometric equal abduction and adduction task, during which
additional shoulder radiographs were obtained.
Radiograph quality was controlled by the coordinating
investigator (JF) during each session using the following
criteria: (1) visible projection of the scapular spine with at
least 2/3 of the scapula on the image [16]; (2) The base of
the coracoid visible just above the scapular spine, opposite
of the glenoid rim [16]; (3) Overlap of the humeral head
with the glenoid in the form of an ellipse, with the anterior
margin of the glenoid projecting cranial to the humeral
head and posterior through the humeral head [7]; (4) The
greater tuberosity is seen in profile [7]; (5) Clearly defined
AH space, bordered cranially by the acromion and distally
by the humeral head. Any images not fulfilling these cri-
teria were re-acquired.
There is no ‘‘golden standard’’ for subacromial space
measurements and a wide variety of cranial translation
measurements have been described. Therefore, we used
three reported measuring methods for the subacromial
space (Fig. 2a): (1) The acromiohumeral distance (AH) is
the distance between the most cranial articular cortex of the
Fig. 1 Experimental setup for the modified active abduction view
(MAAV). Subjects were positioned for true anteroposterior shoulder
radiographs: the upper body was turned 30� from the frontal plane
toward the Rontgen focus beam (R) with the arm in external rotation
alongside the subjects’ body (dotted arrow). The arm was attached to
a 1-dimensional force transducer sensor (S) at the wrist using a brace
to prevent movement in the shoulder and to enable isometric
abduction (FAB) and adduction (FAD) tasks in the frontal plane.
Radiographs were acquired with a film focus distance of roughly
120 cm and a 15� craniocaudal tilt
Med Biol Eng Comput
123

humeral head and the caudal cortex marking of the caudal
surface of the acromion [9, 13, 29]. (2) The upper migra-
tion index (UMI) is the quotient of the distance from the
center of the humeral head to the caudal cortex of the
acromion and the radius of the humeral head [10, 27, 28].
(3) The scapular spine-humeral head center method (SHC)
is defined as the perpendicular distance between a line
running through the linear part of the supraspinatus fossa
floor and the geometric center of the humeral head [16].
The AH method is still the most commonly used cranial
translation measurement, although it is prone to projection
and magnification errors [16]. The magnification error of
AP shoulder radiographs is reduced when using the upper
migration index, making direct intra- and intersubject
comparisons of the measurements during different tasks
more reliable [16, 27]. The SHC method is reported least
sensitive to projection errors because the scapular spine lies
roughly in the same coronal and axial planes as the center
of the humeral head [16]. The SHC method has not been
validated in vivo, but is reported to be least susceptible to
changes to the anatomic measurement landmarks in an
in vitro study [16]. All subacromial space measurements
were reported in mm, except for the upper migration index,
which is a relative measure. Humeral head translation
during active abduction and adduction translations were
measured with respect to the position at rest, thus mea-
suring active cranialization or active caudalization. These
relative translations were expressed as DAH, DUMI, and
DSHC. One observer (JF) conducted all of the subacromial
space measurements, blinded for the specific task. When
the necessary anatomic landmarks could not be identified,
the measurement was not performed and was reported as
missing.
2.2 Statistical analyses
The mean differences in subacromial space, expressed in
AH, UMI, and SHC, between rest and isometric abduction
and adduction radiographs were assessed by means of
paired students’ t tests to determine active cranial transla-
tion. The independent students’ t test was used for subgroup
analyses, comparing the differences in active cranial
translation (DAH, DUMI and DSHC) between rest and
abduction in patients with superior and posterosuperior
rotator cuff tears. The relation between AH and VAS pain
(dependant variable) was assessed using linear mixed model
analyses, accounting for the performed task (abduction,
adduction, and rest). The linear mixed model included a
random effect for repeated measures in each subject.
p values of B0.05 (two-sided) were considered statisti-
cally significant. Statistical analysis was done using PASW
statistics 17 (IBM Inc., USA).
3 Results
The results of the subacromial space measurements during
the rest, abduction, and adduction tasks are presented in
Table 2. In one instance, the scapular spine could not be
unambiguously ascertained and this measurement was
excluded from further analyses. On average, there was
significant active cranial translation of the humeral head
during both active abduction and adduction compared to
rest. In rest, the mean AH was 7.5 mm (SD = 1.53), and,
during active isometric abduction, it decreased to 5.4 mm
(SD = 2.60), resulting in a mean AH difference of 2.1 mm
(95 % CI [1.28, 3.01], p \ 0.001). During active isometric
adduction the AH decreased to 6.4 mm (SD = 2.30),
resulting in a mean difference of 1.1 mm (95 % CI [0.46,
1.65], p = 0.001) compared to rest. Similar results were
observed for the UMI and SHC measurements (Table 2).
Fig. 2 a Subacromial space measuring methods example of suba-
cromial space measurement techniques used during a rest task. AHacromiohumeral distance method; UMI upper migration index; SHCscapular spine-humeral head center method; Cor base of the coracoid;
R radius of the humeral head; C center of the humeral head; », parallel
lines; :, right 90� angle. b Example of subacromial space measure-
ment techniques used during active isometric abduction, demonstrat-
ing active cranial translation compared to the rest measurements (a).
AH acromiohumeral distance method, UMI upper migration index;
SHC scapular spine-humeral head center method; Cor base of the
coracoid; R radius of the humeral head; C center of the humeral head;
», parallel lines; :, Right 90� angle
Med Biol Eng Comput
123
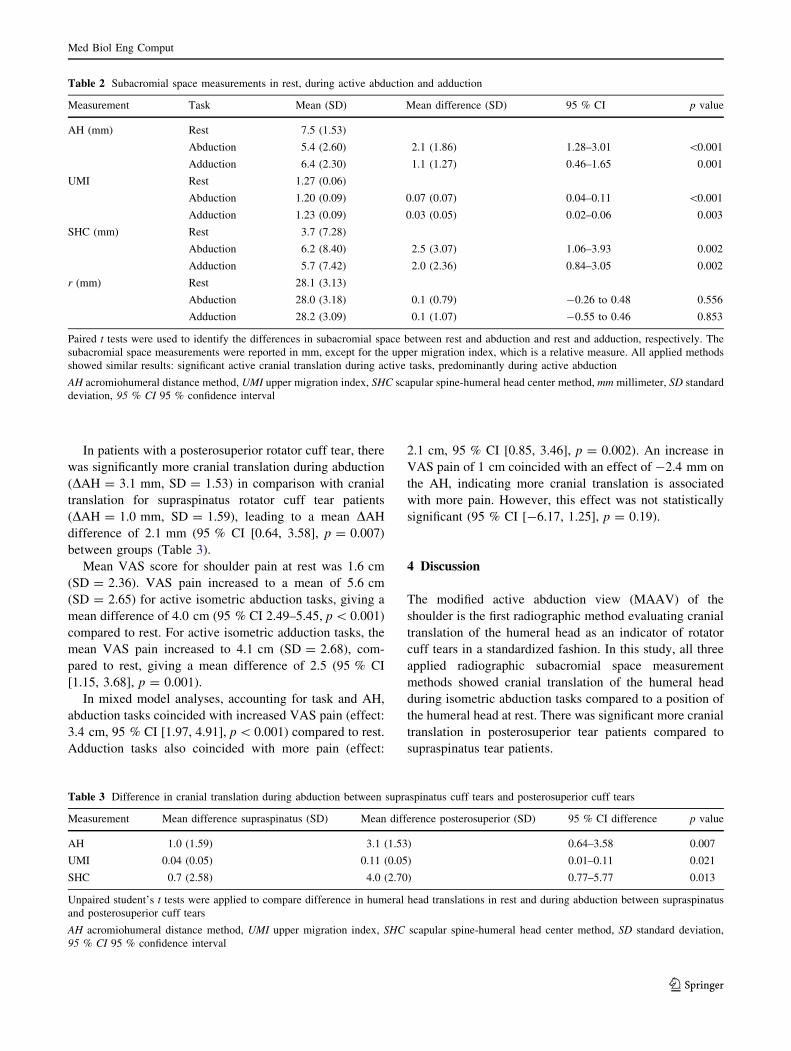
In patients with a posterosuperior rotator cuff tear, there
was significantly more cranial translation during abduction
(DAH = 3.1 mm, SD = 1.53) in comparison with cranial
translation for supraspinatus rotator cuff tear patients
(DAH = 1.0 mm, SD = 1.59), leading to a mean DAH
difference of 2.1 mm (95 % CI [0.64, 3.58], p = 0.007)
between groups (Table 3).
Mean VAS score for shoulder pain at rest was 1.6 cm
(SD = 2.36). VAS pain increased to a mean of 5.6 cm
(SD = 2.65) for active isometric abduction tasks, giving a
mean difference of 4.0 cm (95 % CI 2.49–5.45, p \ 0.001)
compared to rest. For active isometric adduction tasks, the
mean VAS pain increased to 4.1 cm (SD = 2.68), com-
pared to rest, giving a mean difference of 2.5 (95 % CI
[1.15, 3.68], p = 0.001).
In mixed model analyses, accounting for task and AH,
abduction tasks coincided with increased VAS pain (effect:
3.4 cm, 95 % CI [1.97, 4.91], p \ 0.001) compared to rest.
Adduction tasks also coincided with more pain (effect:
2.1 cm, 95 % CI [0.85, 3.46], p = 0.002). An increase in
VAS pain of 1 cm coincided with an effect of -2.4 mm on
the AH, indicating more cranial translation is associated
with more pain. However, this effect was not statistically
significant (95 % CI [-6.17, 1.25], p = 0.19).
4 Discussion
The modified active abduction view (MAAV) of the
shoulder is the first radiographic method evaluating cranial
translation of the humeral head as an indicator of rotator
cuff tears in a standardized fashion. In this study, all three
applied radiographic subacromial space measurement
methods showed cranial translation of the humeral head
during isometric abduction tasks compared to a position of
the humeral head at rest. There was significant more cranial
translation in posterosuperior tear patients compared to
supraspinatus tear patients.
Table 2 Subacromial space measurements in rest, during active abduction and adduction
Measurement Task Mean (SD) Mean difference (SD) 95 % CI p value
AH (mm) Rest 7.5 (1.53)
Abduction 5.4 (2.60) 2.1 (1.86) 1.28–3.01 \0.001
Adduction 6.4 (2.30) 1.1 (1.27) 0.46–1.65 0.001
UMI Rest 1.27 (0.06)
Abduction 1.20 (0.09) 0.07 (0.07) 0.04–0.11 \0.001
Adduction 1.23 (0.09) 0.03 (0.05) 0.02–0.06 0.003
SHC (mm) Rest 3.7 (7.28)
Abduction 6.2 (8.40) 2.5 (3.07) 1.06–3.93 0.002
Adduction 5.7 (7.42) 2.0 (2.36) 0.84–3.05 0.002
r (mm) Rest 28.1 (3.13)
Abduction 28.0 (3.18) 0.1 (0.79) -0.26 to 0.48 0.556
Adduction 28.2 (3.09) 0.1 (1.07) -0.55 to 0.46 0.853
Paired t tests were used to identify the differences in subacromial space between rest and abduction and rest and adduction, respectively. The
subacromial space measurements were reported in mm, except for the upper migration index, which is a relative measure. All applied methods
showed similar results: significant active cranial translation during active tasks, predominantly during active abduction
AH acromiohumeral distance method, UMI upper migration index, SHC scapular spine-humeral head center method, mm millimeter, SD standard
deviation, 95 % CI 95 % confidence interval
Table 3 Difference in cranial translation during abduction between supraspinatus cuff tears and posterosuperior cuff tears
Measurement Mean difference supraspinatus (SD) Mean difference posterosuperior (SD) 95 % CI difference p value
AH 1.0 (1.59) 3.1 (1.53) 0.64–3.58 0.007
UMI 0.04 (0.05) 0.11 (0.05) 0.01–0.11 0.021
SHC 0.7 (2.58) 4.0 (2.70) 0.77–5.77 0.013
Unpaired student’s t tests were applied to compare difference in humeral head translations in rest and during abduction between supraspinatus
and posterosuperior cuff tears
AH acromiohumeral distance method, UMI upper migration index, SHC scapular spine-humeral head center method, SD standard deviation,
95 % CI 95 % confidence interval
Med Biol Eng Comput
123
Cranial translation of the humeral head during active
abduction has been reported in earlier studies. Both Deu-
tsch et al. [6] and Bloom [1] found significant cranial
translation on AP radiographs at different elevation angles
during active abduction in patients with rotator cuff
pathology. Graichen et al. [8] found similar results at dif-
ferent abduction angles using open MRI to measure the
subacromial space during active arm abduction tasks. We
found a similar magnitude of humeral head translations
compared to studies measuring translation in elevated arm
positions using radiographs, ultrasound, and open MRI [1,
6, 8]. However, these measurements are not directly
comparable with the current series, as we specifically did
not assess cranial translation at different abduction angles,
but with shoulder radiographs in a standardized arm posi-
tion during simultaneous isometric force tasks. Further-
more, we used regular radiographs in a standardized setup.
The current study is the first to measure active cranial
translation of the humeral head in full-thickness rotator
cuff tear patients in similar arm positioning during active
isometric tasks.
Active cranial translation of the humeral head is con-
sidered to be elicited by activity of the deltoid [8, 15]. In
rotator cuff tear patients, there is increased deltoid activity,
as the deltoid compensates for lost rotator cuff abduction
moment, while generating a destabilizing cranial force [23,
24]. The combination of the increased superiorly directed
forces of the deltoid during abduction and the impaired
stabilizing function of the torn rotator cuff lead to exces-
sive cranial translation and thereby narrowing of the sub-
acromial space [8, 22–24]. Surprisingly, we also found
cranial translation during isometric adduction tasks, albeit
to a lesser extent. In biomechanical and electromyograph-
ical studies, adductor co-activation has been reported in
rotator cuff tear patients during abduction tasks [22, 25]. In
theory, adductor activation leads to caudally directed for-
ces on the humerus [22, 25]. Obviously, the cranially
directed forces of the deltoid on the humerus exceed the
caudally directed forces during both abduction and
adduction, respectively. In the absence of supraspinatus
and infraspinatus force, the only remaining muscles for
glenohumeral stabilization are the deltoid and potentially
the superior part of the subscapularis [15, 23].
We found significantly more cranial translation in
patients with a posterosuperior rotator cuff tear than in the
supraspinatus tear group on radiographs acquired during
isometric active abduction (modified AAV). The present
findings support the idea that the infraspinatus plays an
important role in the mechanical force and torque balance
centering the humeral head onto the glenoid [11]. Loss of
infraspinatus abduction torque requires additional deltoid
forces resulting in a nett increase of the cranial force
component and subsequent additional cranial translation
[22]. In the only non-designer AAV study, Umans et al.
[26] were unable to detect any differences in the subacro-
mial space during active abduction compared to rest in
partial and full-thickness supraspinatus rotator cuff tear
patients. However, they did not use isometric abduction
tasks and did not include posterosuperior tear patients,
where both the supraspinatus and infraspinatus functions
are impaired.
We did not find a strong relation between increased
active cranial translation and shoulder pain. Our results
suggest that, if present, mechanical osseous impingement
due to narrowing of the subacromial space seems only for a
minor part responsible for reported pain in rotator cuff tear
patients. Our results are consistent with previous studies
[11, 17, 23]. Individual pain perception is subjective and is
considered difficult to measure directly. Tolerance to pain
varies considerably among patients and may affect the
relation between cranial translation and shoulder pain, so
the interpretations of the current results must be drawn with
caution. However, these measurements are repeated after
each task and tolerance to pain is considered intraobserver
reliable [4]. The underlying causes of symptomatic rotator
cuff tears have traditionally been identified as either
intrinsic degeneration of the rotator cuff, altering the nor-
mal biomechanics of the glenohumeral joint or extrinsic
mechanisms impinging the rotator cuff under the coraco-
acromial arch, e.g., cranial translation of the humeral head
and acromion shape. Although Neer’s [17] theory is widely
accepted and focuses on the extrinsic mechanism, we found
only a minor effect of osseous impingement. The spectrum
of causality of symptoms in rotator cuff tears as both partly
intrinsic and partly extrinsic possibly explains the great
clinical variability observed in these patients.
In previous studies, differences in abduction position,
arm rotation and glenohumeral configuration could have
lead to large projection and magnification errors with over-
estimation of the observed effect [16, 19]. This makes it
difficult to compare cranial translations of the humeral head
within and between subjects with previously reported
methods. With the proposed modified AAV, the abduction
position and glenohumeral configuration is kept constant.
The experimental setup was easy to use for both rest and
active abduction radiographs. However, although this pro-
vided a uniform method for MAAV radiographs, we still
observed a great intra- and inter-individual variation in
projection of the acromion and scapular spine between the
radiographs, resulting in relative large dispersions of the
SHC measurements [16]. However, there were no clear
systematic differences between rest, abduction and adduc-
tion tasks. Furthermore, our observations fall between -10�and ?10� spinal tilt, which were previously estimated with
3D scapular position measurements in 0� abduction [3]. The
three measuring methods for cranial translation supported
Med Biol Eng Comput
123

each other, displaying similar results. Each measurement
has its own advantages and shortcomings [16]. More
research is needed to assess which radiographic measure-
ment method is most reliable and responsive for active
cranial translation.
There are several issues concerning the collection and
interpretation of the data. First, we are unable to ascertain
whether the observed effect is group specific as we did not
measure e.g., healthy individuals or asymptomatic rotator
cuff tear patients. However, earlier reports indicate that the
caudal translations of the humeral head in healthy indi-
viduals are less than 1 mm during arm abduction from 0� to
120� [6]. Second, it might be difficult to differentiate
between symptomatic and asymptomatic cuff rotator tears.
It is possible that some patients in our study had shoulder
symptoms which were not derived from the diagnosed cuff
tear. However, inclusion was performed by two experi-
enced orthopedic shoulder surgeons, using extensive
imaging techniques and strict eligibility criteria based on
current knowledge to have as homogeneous a study group
as possible. Lastly, systematic measurement errors are
common for shoulder radiographs. Patient positioning
might greatly influence the projection of the glenoid and
subacromial space on an AP radiographs. When using this
experimental setup, care must be taken to keep patient
positioning constant. All cranial translation measurements
were performed by one observer and we did not control for
intraobserver variance. However, earlier reports state that
the applied measurements on AP radiographs are highly
reproducible within and between investigators [16, 27].
In conclusion, active isometric abduction leads to active
cranial translation of the humeral head in symptomatic
rotator cuff tear patients using the MAAV method for
radiographs. The MAAV can be used to quantify cranial
translation of the humeral head in rotator cuff tear patients.
More research is needed to determine if the MAAV can
differentiate between healthy subjects, asymptomatic and
symptomatic cuff tear patients. Possibly, combining
radiographs with active tasks offers new possibilities in
diagnosing and detecting massive rotator cuff tears
functionally.
Acknowledgments We gratefully acknowledge the work of H.
Fraterman for building the experimental setup. The institution of the
authors has received funding from Dutch Arthritis Association (grant
number 09-1-303).
References
1. Bloom RA (1991) The active abduction view: a new maneuvre in
the diagnosis of rotator cuff tears. Skeletal Radiol 20:255–258
2. Chopp JN, O’Neill JM, Hurley K, Dickerson CR (2010) Superior
humeral head migration occurs after a protocol designed to
fatigue the rotator cuff: a radiographic analysis. J Should Elbow
Surg 19:1137–1144
3. de Groot JH, van Woensel W, van der Helm FC (1999) Effect of
different arm loads on the position of the scapula in abduction
postures. Clin Biomech (Bristol, Avon) 14:309–314
4. de Witte PB, Henseler JF, Nagels J, Vliet Vlieland TP, Nelissen
RG (2012) The Western Ontario Rotator Cuff index in rotator
cuff disease patients: a comprehensive reliability and respon-
siveness validation study. Am J Sports Med 40:1611–1619
5. de Witte PB, van der Zwaal P, Visch W, Schut J, Nagels J,
Nelissen RG, de Groot JH (2012) Arm adductor with arm
abduction in rotator cuff tear patients vs. healthy—design of a
new measuring instrument. Hum Mov Sci 31:461–471
6. Deutsch A, Altchek DW, Schwartz E, Otis JC, Warren RF (1996)
Radiologic measurement of superior displacement of the humeral
head in the impingement syndrome. J Should Elbow Surg 5:186–193
7. Goud A, Segal D, Hedayati P, Pan JJ, Weissman BN (2008)
Radiographic evaluation of the shoulder. Eur J Radiol 68:2–15
8. Graichen H, Hinterwimmer S, von Eisenhart-Rothe R, Vogl T,
Englmeier KH, Eckstein F (2005) Effect of abducting and
adducting muscle activity on glenohumeral translation, scapular
kinematics and subacromial space width in vivo. J Biomech
38:755–760
9. Gruber G, Bernhardt GA, Clar H, Zacherl M, Glehr M, Wurnig C
(2010) Measurement of the acromiohumeral interval on stan-
dardized anteroposterior radiographs: a prospective study of
observer variability. J Should Elbow Surg 19:10–13
10. Hirooka A, Wakitani S, Yoneda M, Ochi T (1996) Shoulder
destruction in rheumatoid arthritis. Classification and prognostic signs
in 83 patients followed 5–23 years. Acta Orthop Scand 67:258–263
11. Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K
(2009) Proximal humeral migration in shoulders with symptom-
atic and asymptomatic rotator cuff tears. J Bone Joint Surg Am
91:1405–1413
12. Lehtinen JT, Belt EA, Kauppi MJ, Kaarela K, Kuusela PP,
Kautiainen HJ, Lehto MU (2001) Bone destruction, upward
migration, and medialisation of rheumatoid shoulder: a 15 year
follow up study. Ann Rheum Dis 60:322–326
13. Lehtinen JT, Belt EA, Lyback CO, Kauppi MJ, Kaarela K,
Kautiainen HJ, Lehto MU (2000) Subacromial space in the
rheumatoid shoulder: a radiographic 15-year follow-up study of
148 shoulders. J Shoulder Elbow Surg 9:183–187
14. Matsen FA III (2008) Clinical practice. Rotator-cuff failure.
N Engl J Med 358:2138–2147
15. McCully SP, Suprak DN, Kosek P, Karduna AR (2006) Supra-
scapular nerve block disrupts the normal pattern of scapular
kinematics. Clin Biomech (Bristol, Avon) 21:545–553
16. Nagels J, Verweij J, Stokdijk M, Rozing PM (2008) Reliability of
proximal migration measurements in shoulder arthroplasty.
J Should Elbow Surg 17:241–247
17. Neer CS (1972) Anterior acromioplasty for the chronic
impingement syndrome in the shoulder: a preliminary report.
J Bone Joint Surg Am 54:41–50
18. Oh LS, Wolf BR, Hall MP, Levy BA, Marx RG (2007) Indica-
tions for rotator cuff repair: a systematic review. Clin Orthop
Relat Res 455:52–63
19. Rozing PM, Obermann WR (1999) Osteometry of the glenohu-
meral joint. J Should Elbow Surg 8:438–442
20. Sher JS, Uribe JW, Posada A, Murphy BJ, Zlatkin MB (1995)
Abnormal findings on magnetic resonance images of asymp-
tomatic shoulders. J Bone Joint Surg Am 77:10–15
21. Sneppen O, Fruensgaard S, Johannsen HV, Olsen BS, Sojbjerg
JO, Andersen NH (1996) Total shoulder replacement in rheu-
matoid arthritis: proximal migration and loosening. J Should
Elbow Surg 5:47–52
Med Biol Eng Comput
123

22. Steenbrink F, de Groot JH, Veeger HE, Meskers CG, van de
Sande MA, Rozing PM (2006) Pathological muscle activation
patterns in patients with massive rotator cuff tears, with and
without subacromial anaesthetics. Man Ther 11:231–237
23. Steenbrink F, de Groot JH, Veeger HE, van der Helm FC, Rozing
PM (2009) Glenohumeral stability in simulated rotator cuff tears.
J Biomech 42:1740–1745
24. Steenbrink F, Meskers CG, Nelissen RG, de Groot JH (2010) The
relation between increased deltoid activation and adductor mus-
cle activation due to glenohumeral cuff tears. J Biomech 43:
2049–2054
25. Steenbrink F, Nelissen RG, Meskers CG, van de Sande MA,
Rozing PM, de Groot JH (2010) Teres major muscle activation
relates to clinical outcome in tendon transfer surgery. Clin Bio-
mech (Bristol, Avon) 25:187–193
26. Umans HR, Pavlov H, Berkowitz M, Warren RF (2001) Corre-
lation of radiographic and arthroscopic findings with rotator cuff
tears and degenerative joint disease. J Should Elbow Surg
10:428–433
27. van de Sande MA, Rozing PM (2006) Proximal migration can be
measured accurately on standardized anteroposterior shoulder
radiographs. Clin Orthop Relat Res 443:260–265
28. van de Sande MA, Stoel BC, Rozing PM (2006) Subacromial
space measurement: a reliable method indicating fatty infiltration
in patients with rheumatoid arthritis. Clin Orthop Relat Res
451:73–79
29. Weiner DS, Macnab I (1970) Superior migration of the humeral
head. A radiological aid in the diagnosis of tears of the rotator
cuff. J Bone Joint Surg Br 52:524–527
Med Biol Eng Comput
123