Embed Size (px)
DESCRIPTION
CPTN Personal Training Certification. The Art & Science of Personal Training (First Weekend). Instructor: Jeff Boris, B.PHE, CPT-CPTN.M. - PowerPoint PPT Presentation
Citation preview
CPTN CPTN Personal Training Personal Training
CertificationCertificationThe Art & Science of The Art & Science of
Personal TrainingPersonal Training
(First Weekend)(First Weekend)
Instructor: Jeff Boris, B.PHE, CPT-CPTN.MInstructor: Jeff Boris, B.PHE, CPT-CPTN.M
ABOUT THE CPTN The Certified Professional Trainers Network, formerly known as the Canadian Personal Trainers Network, was launched in 1993. The CPTN integrates current research and practical applications for education, communication, professional development and marketing opportunities for Personal Trainers to maintain a leading edge on professional training developments.
•Develops and certifies trainers through the course entitled “The Art and Science of Personal Training Level 1: The Essentials” and the "Fast Track Course on Personal Training.”
•Launched Canada's first personal trainers Conference.
•Launched Canada's first National personal trainer certification (1994)
•Featured in Macleans, YOU, Your Health, Canadian Living, Canadian Fitness, Fitness Management, Confidante, Chatelaine, CITY-TV, CBC Marketplace, The Athlete, and The Toronto Star.
•Contributed to NFLAC's Specialist Guidelines for Personal Trainers as a committee member.
•International Recognition through IDEA Health and Fitness Association. It has a worldwide distribution in over 80 countries with over 19,000 members.

• Able to start own business as a personal trainer
• Access to Sport Insurance from other bodies
• National recognition of commitment to the highest standards of excellence
• International Recognition through IDEA fitness
• Listed on CPTN's web site as a Personal Trainer referral
• Earn CECs with professional Distance Education Courses
• Eligible to join CPTN's leadership team of Practical Assessors, Course Conductors and Mentors
• The CPTN Report Newsletters
• Monthly E-news and client handout via e-mail
• Access to Personal Trainer Job Listings
• Access to Fitness Training Facilities Listings
• Discounts on Educational Books and Multi-media
• Discounts on CTPN Conferences & Workshops
• Discounts on Products & Services through Suppliers
CPTN CERTIFICATION BENEFITS
CPTN CERTIFICATION REQUIREMENTS
• Must be an adult age 18 or older • Current CPR (Basic Rescuer) and current Emergency First Aid • Passing grade on 120 multiple choice Theory ExamTheory Exam of 75% or higher • Passing grade on the Practical ExamPractical Exam of 75% or higher • Documentation of a minimum of 20 personal training hours (Complete a Personal Trainer Log) OR a degree/diploma in the physical education/kinesiology field (copies of proof to be submitted to CPTN)
Note:Note: Requirements are to be completed within 6 months from exam writing date.
Certification RenewalCPTN certification status is due for renewal each year or every two years. In addition to having current CPR and First Aid, you require 7 CECs to renew for 1 year or 14 CECs to renew for 2 years. One hour of continuing education equals 1 CPTN CEC.

OTHER CPTN CERTIFICATIONS & COURSES
POST-REHABILITATION CONDITIONING SPECIALIST
PILATES MAT & BALLWORK SPECIALIST
YOGA SPECIALIST
CPTN/TBI (Tudor Bompa Institute) SPECIALTY CERTIFICATIONS (On-Line)
Ice Hockey Conditioning Specialist Certification
Junior Athletes Training Specialist Certification
Periodization Planning Specialist Certification
Strength and Conditioning Expert Certification
Website: Website: www.cptn.com
WELCOME TO “THE ART & SCIENCE OF PERSONAL TRAINING”
• Evidence-based Information Evidence-based Information (From Current Knowledge to Emerging Theory)(From Current Knowledge to Emerging Theory)
• Experiential & Interactive Learning Experiential & Interactive Learning (Individual, Partner, Group)(Individual, Partner, Group)
1.1. Your Mind is Open:Your Mind is Open: “We do not know what we do not know.”
2.2. Your Manual is a Reference:Your Manual is a Reference: “Knowledge is in the manual, Wisdom is in the application.”
3.3. Your Outcome is Your Input:Your Outcome is Your Input: “Contribution enhances everyone’s learning experience.”
WHY PERSONAL TRAINING? FIVE REASONS
INTELLECTUAL INTELLECTUAL DISTRIBUTIONDISTRIBUTION WELLNESS WELLNESS
REVOLUTIONREVOLUTION
BABY BABY BOOMERSBOOMERS
HEALTH CRISIS, HEALTH CRISIS, LIFESTYLE LIFESTYLE EPIDEMICEPIDEMIC
TOP 10 TOP 10 PROFESSIONS, PROFESSIONS,
FASTEST FASTEST GROWING GROWING
SEGMENT OF SEGMENT OF FITNESS INDUSTRYFITNESS INDUSTRY
PERSONAL TRAINER The “SELF-CARE SPECIALIST”
NaturalNatural Self-Care is… Self-Care is…
An Attitude of self-responsibility, taking personal responsibility for your health and being accountable for your actions. This includes a willingness to learn, improve yourself and do whatever it takes.
Corrective Action giving the body what only you can give it, addressing root causes with approaches that are intelligently aligned with your body’s real and natural needs, to create a healthy environment conducive to longevity, peak performance and a better quality of life.
CONSULTING & INTERPERSONAL COMMUNICATION SKILLS
LEARNING OBJECTIVESLEARNING OBJECTIVES
1. To understand the role of consulting in personal training
2. To understand the significance of developing versatility in interpersonal communication skills
3. To understand the theories, concepts, and strategies associated with consulting and interpersonal communication skills
4. To develop greater self-awareness of one’s role in personal training and develop a mission statement
“WHAT DO YOU DO?”“HOW DO YOU DO IT?”“WHY DO YOU DO IT?”
WHO ARE YOU?
Defining and marketing your role Defining and marketing your role as a personal trainer.as a personal trainer.
“WHAT DO YOU DO?”“HOW DO YOU DO IT?”“WHY DO YOU DO IT?”
WHO ARE YOU?
JEFF BORIS, B.PHE, CPTN.CPT.MJEFF BORIS, B.PHE, CPTN.CPT.M
Holistic Fitness Trainer, Nutrition & Health Research EducatorHolistic Fitness Trainer, Nutrition & Health Research Educator
“There is an immense disconnect and unacceptable delay between scientific data and public awareness and prevention.” – Dr. Larry Silver, Clinical Professor at Georgetown Medical Centre, past president of Learning Disabilities Association of America
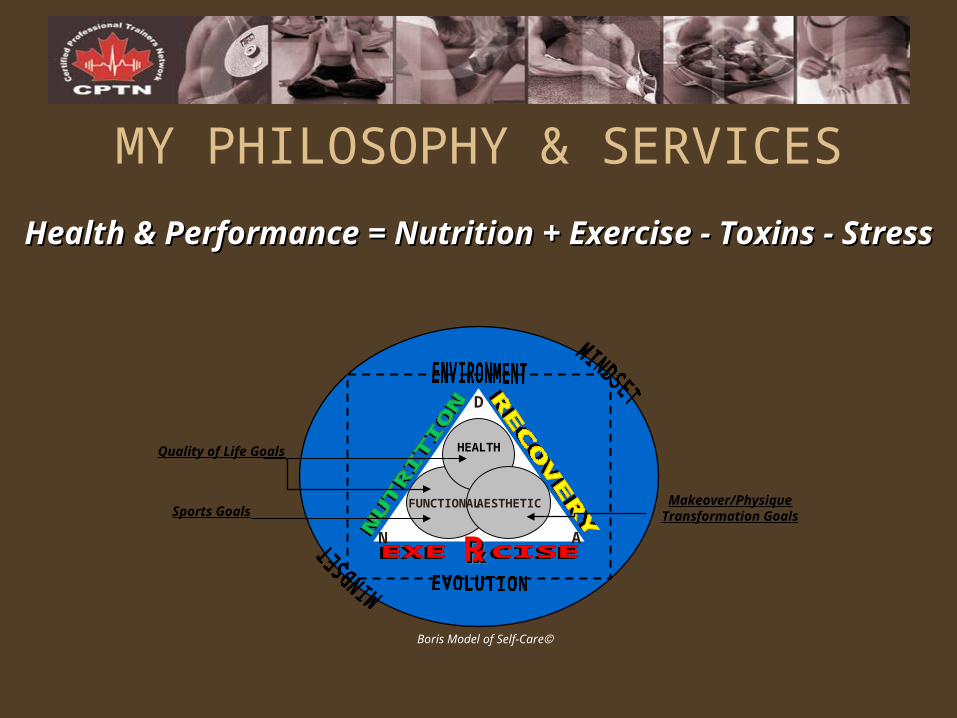
Health & Performance = Nutrition + Exercise - Toxins - StressHealth & Performance = Nutrition + Exercise - Toxins - Stress
MY PHILOSOPHY & SERVICES
Sports GoalsMakeover/Physique
Transformation Goals
Quality of Life Goals
AESTHETIC
Boris Model of Self-Care
HEALTH
FUNCTIONAL
℞℞℞℞
D
N A

B.PHE
My Background
My Background
General Manager
My First Personal Training Studio
Personal Training
Coordinator
Senior Fitness SpecialistPersonal Training Program Manager
R.A.C.
Natural Health Products Specialist & Research Educator
Education Coordinator
“Professor of Personal Training”
Professional Development Chair
Course Conductor, Practical Assessor
Holistic Fitness & Nutrition Health Research Education
Professional Services Innovative Products
Profitable Partnerships
A Few Highlights…
MY MISSION STATEMENT
Educate, motivate, empower and inspire people from all walks of life to discover and
realize their unlimited human potentialfor achieving health, happiness and success!
Who are YOU?Why are YOU here??
1. DEVELOPING YOUR PERSONAL MISSION STATEMENT
Why personal training?How does PTR serve your purpose/goals/mission/career?How is PTR in alignment with what’s important to you?Why should I hire you as my Personal Trainer?What’s great about you? (List of 10)
2. YOUR PERSONAL MISSION STATEMENT (2-3 sentences)
3. CREATING THE “PERFECT” PERSONAL TRAINING BUSINESSa) Who are your clients?b) What kind of environment do you work out of?c) What are your area(s) of specialization?d) What hours will you work?e) Will you complement your PTR services with something? What?f) How much will you earn? What are you worth?
PERSONAL TRAINER = LEADERROLE-MODELLINGROLE-MODELLING
1. What are YOUR personal health & fitness goals?
2. What is YOUR minimal commitment to a healthy lifestyle?
3. What motivates YOU?
ASSIGNMENT:ASSIGNMENT:
Answer questions above.
List your S.M.A.R.T. Goals
S.M.A.R.T. GOALSSSpecific, MMeasurable, AAction-oriented, RRealistic, TTrackable
2. What will affect PROGRAM ADHERENCE?2. What will affect PROGRAM ADHERENCE?
3. Develop a CONTINGENCY PLAN.3. Develop a CONTINGENCY PLAN.
4. Develop a SELF-CONTRACT.4. Develop a SELF-CONTRACT.
1. COLLECT BACKGROUND INFORMATION1. COLLECT BACKGROUND INFORMATION
STAGE OF THE CLIENT TRAINER RELATIONSHIP
Rapport BuildingInvestigative
PlanningAction
Consulting & Interpersonal Communication Skills
• “Trainers and clients work with each other over time in a consultative fashion which invites equitable input from both trainer and client.”– Encouragement from the trainer should be
promoting client self sufficiency.
Effective FeedbackA) It is specificB) It is contingent on performanceC) It provides corrective information for the
learner
Styles Include:
Visual, Auditory, Kinesthetic, Tactile
HUMAN RELATIONS MODELS1. ABRAHAM MASLOW: Hierarchy of Needs
Describe how understanding the relationship between upper level and lower level needs might enhance empathy for clients’ apparent disinterest or lack of focus/compliance.
2. CHRIS ARGYRIS: Interpretation & Choice
Analyze a “typical” client-trainer or learner-expert encounter. How are issues of dominance and control played out in a training environment?
3. JACK GIBB: Open Communication vs. Defensive Communication
Discuss how the content and manner of delivery can manifest defensive communication
4. MANAGERIAL vs. HUMAN RELATIONS and the IMPERSONAL-INTERPERSONAL CONTINUUM
Provide examples of each characteristic on the Impersonal-Interpersonal Continuum
EXERCISE PHYSIOLOGY & PROGRAM DESIGN FOR CARDIOVASCULAR FITNESS
LEARNING OBJECTIVESLEARNING OBJECTIVES
1. To understand the relationship between acute and chronic responses to CV exercise and central versus peripheral adaptations
2. To understand the formula for oxygen consumption and its relationship to central versus peripheral adaptations
3. To understand the relationship between various methods of monitoring intensity and their applications
4. To apply an understanding of the various energy systems in the design of CV exercise programs
5. To apply the fundamental principles of training to the O.F.I.T.T. prescription method of program design
6. To understand the application of O.F.I.T.T. in the CV training continuum (improvement vs. maintenance vs. over-training)
7. To explore controversies in CV program design
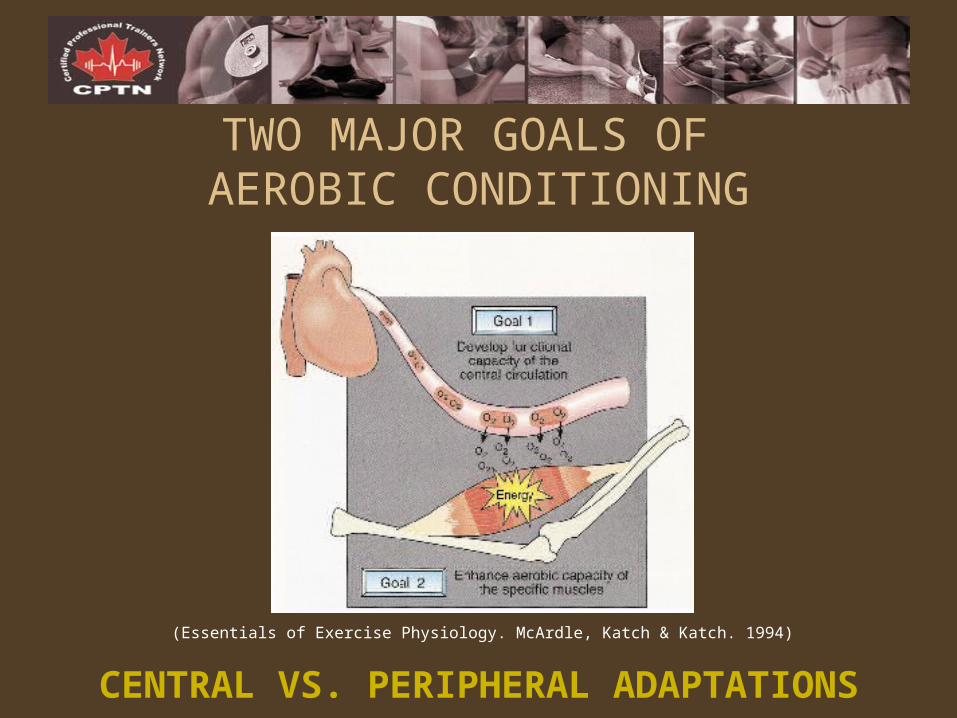
TWO MAJOR GOALS OF AEROBIC CONDITIONING
(Essentials of Exercise Physiology. McArdle, Katch & Katch. 1994)
CENTRAL VS. PERIPHERAL ADAPTATIONS
ACUTE RESPONSES VS. CHRONIC ADAPTATIONS
Increased interior dimensions of heart
Ventricular hypertrophy
Exercise heart rate drops with maintained work intensity
Depressed resting heart rate
Increased cardiac output
Increased capillarization and blood flow to muscles
Increased # and density of mitochondria
Enhanced O2 extraction
Increased VO2 max
Increased anaerobic threshold
Increased use of fat as a fuel source
Glycogen sparing
Increased glycogen stores
Increased sensitivity of cells to insulin
Increase in heart rate
Increase in stroke volume
Increase in cardiac output
Dilation of vessels
Shunting of blood from visceral tissues
Increased rate & depth of breathing
Increased systolic pressure
Central vs. PeripheralCentral vs. Peripheral
Aerobic vs. Anaerobic AdaptationsAerobic vs. Anaerobic Adaptations
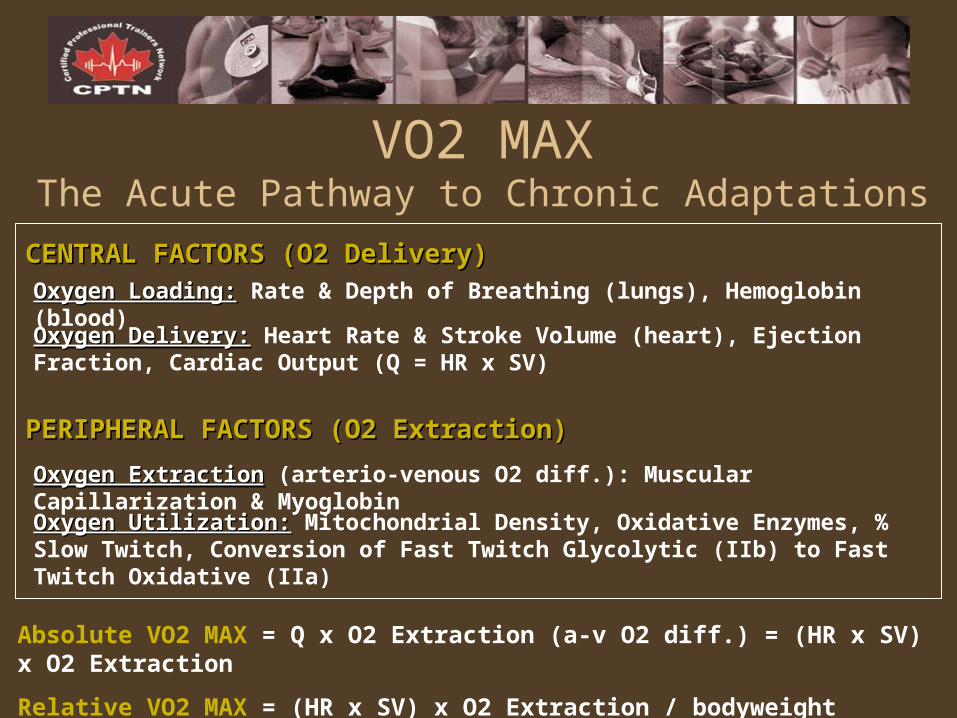
VO2 MAXThe Acute Pathway to Chronic Adaptations
CENTRAL FACTORS (O2 Delivery)CENTRAL FACTORS (O2 Delivery)
PERIPHERAL FACTORS (O2 Extraction)PERIPHERAL FACTORS (O2 Extraction)
Oxygen Loading:Oxygen Loading: Rate & Depth of Breathing (lungs), Hemoglobin (blood)
Oxygen Delivery:Oxygen Delivery: Heart Rate & Stroke Volume (heart), Ejection Fraction, Cardiac Output (Q = HR x SV)
Oxygen ExtractionOxygen Extraction (arterio-venous O2 diff.): Muscular Capillarization & Myoglobin
Oxygen Utilization:Oxygen Utilization: Mitochondrial Density, Oxidative Enzymes, % Slow Twitch, Conversion of Fast Twitch Glycolytic (IIb) to Fast Twitch Oxidative (IIa)
Absolute VO2 MAX = Q x O2 Extraction (a-v O2 diff.) = (HR x SV) x O2 Extraction
Relative VO2 MAX = (HR x SV) x O2 Extraction / bodyweight
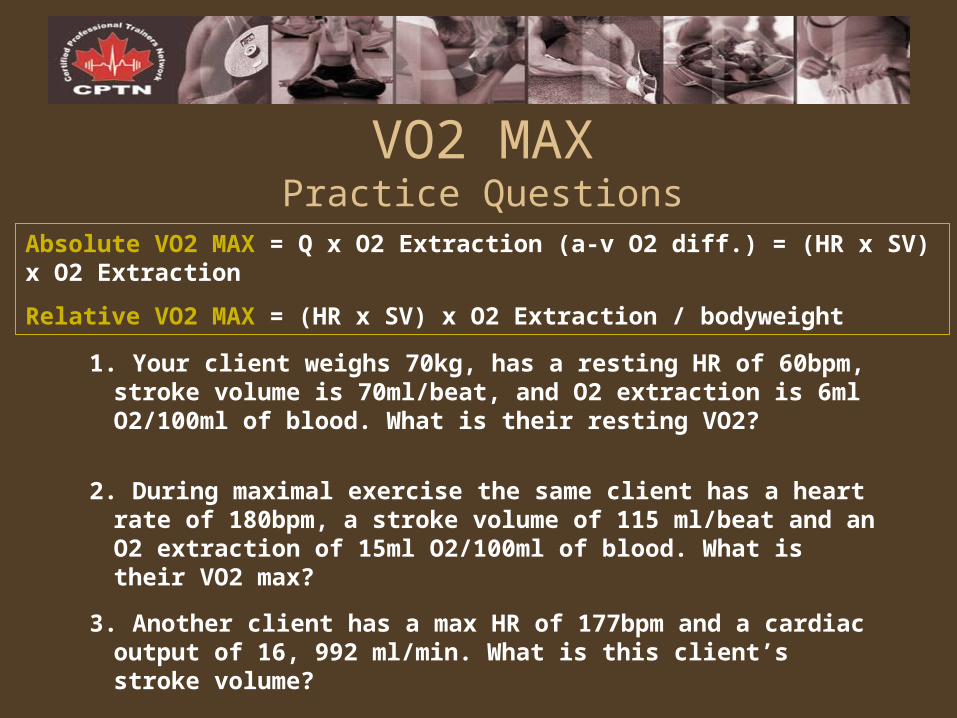
VO2 MAXPractice Questions
1. Your client weighs 70kg, has a resting HR of 60bpm, stroke volume is 70ml/beat, and O2 extraction is 6ml O2/100ml of blood. What is their resting VO2?
2. During maximal exercise the same client has a heart rate of 180bpm, a stroke volume of 115 ml/beat and an O2 extraction of 15ml O2/100ml of blood. What is their VO2 max?
3. Another client has a max HR of 177bpm and a cardiac output of 16, 992 ml/min. What is this client’s stroke volume?
Absolute VO2 MAX = Q x O2 Extraction (a-v O2 diff.) = (HR x SV) x O2 Extraction
Relative VO2 MAX = (HR x SV) x O2 Extraction / bodyweight
METSPractice Questions
1 MET = 3.5ml O2/kg/min
1. Your client has a maximal HR of 178bpm, a stroke volume of 103 ml/beat, an O2 extraction of 14ml O2/100ml of blood and weighs 64kg. What is their relative VO2 max? What is the VO2 equivalent in METS? Describe an activity that would fulfill this value.
2. What is the VO2 equivalent to 4 METS? Describe an activity that would fulfill this value.
MONITORING EXERCISE INTENSITY
PARTNER EXERCISE:PARTNER EXERCISE: Calculate the Target Heart Rate for your Case Study Client.
a) Calculate THR using standard MHR Formula
THR = (220 – age) x Exercise Intensity %
b) Calculate THR using the Karvonen FormulaHRR = [(220 – age) – RHR] x Exercise Intensity % + RHR
1.1. Target Heart RateTarget Heart Rate
2.2. Talk TestTalk Test
3.3. RPE (Rating of Perceived Exertion, Borg Scale)RPE (Rating of Perceived Exertion, Borg Scale)
ENERGY SYSTEMS1.1. ATP-CP / PHOSPHAGEN SYSTEM ATP-CP / PHOSPHAGEN SYSTEM
(Anaerobic Alactic)(Anaerobic Alactic)
2.2. ANAEROBIC GLYCOLYSIS ANAEROBIC GLYCOLYSIS (Anaerobic Lactic)(Anaerobic Lactic)
3.3. AEROBIC GLYCOLYSISAEROBIC GLYCOLYSIS
4.4. FATTY ACID OXIDATION / FATTY ACID OXIDATION / OXIDATIVE PHOSPHORYLATIONOXIDATIVE PHOSPHORYLATION
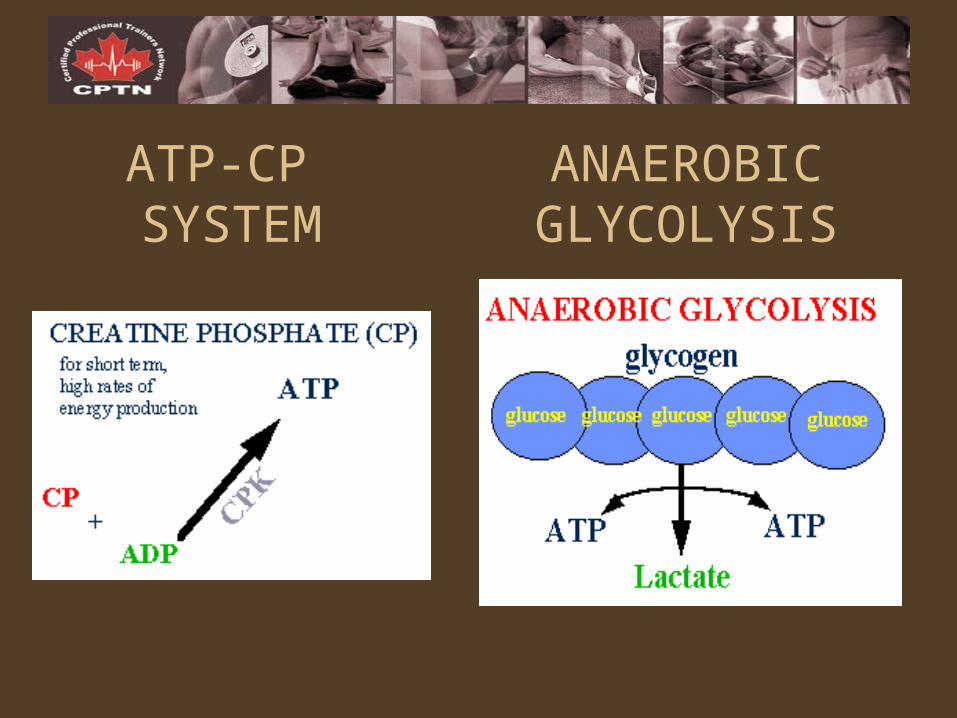
ATP-CP SYSTEM
ANAEROBIC GLYCOLYSIS
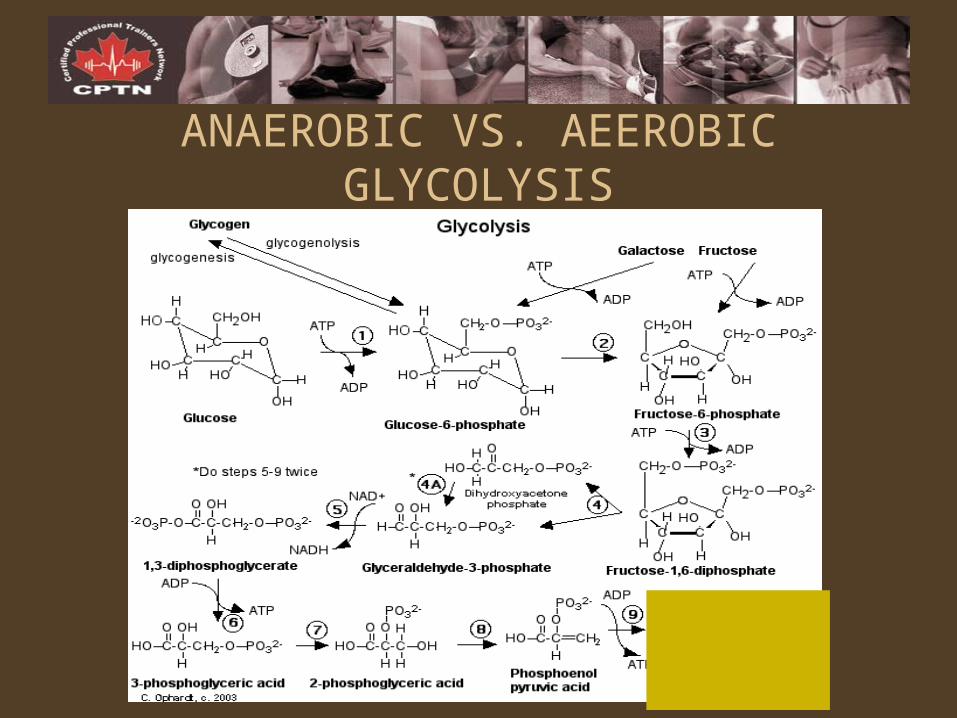
ANAEROBIC VS. AEEROBIC GLYCOLYSIS
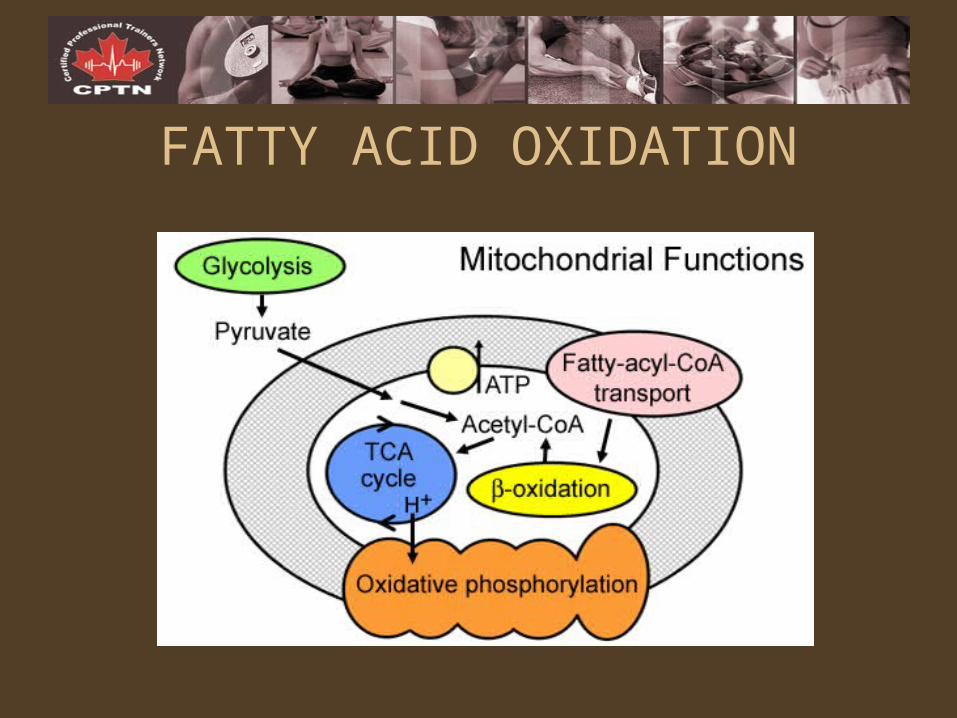
FATTY ACID OXIDATION

Energy Source Summary
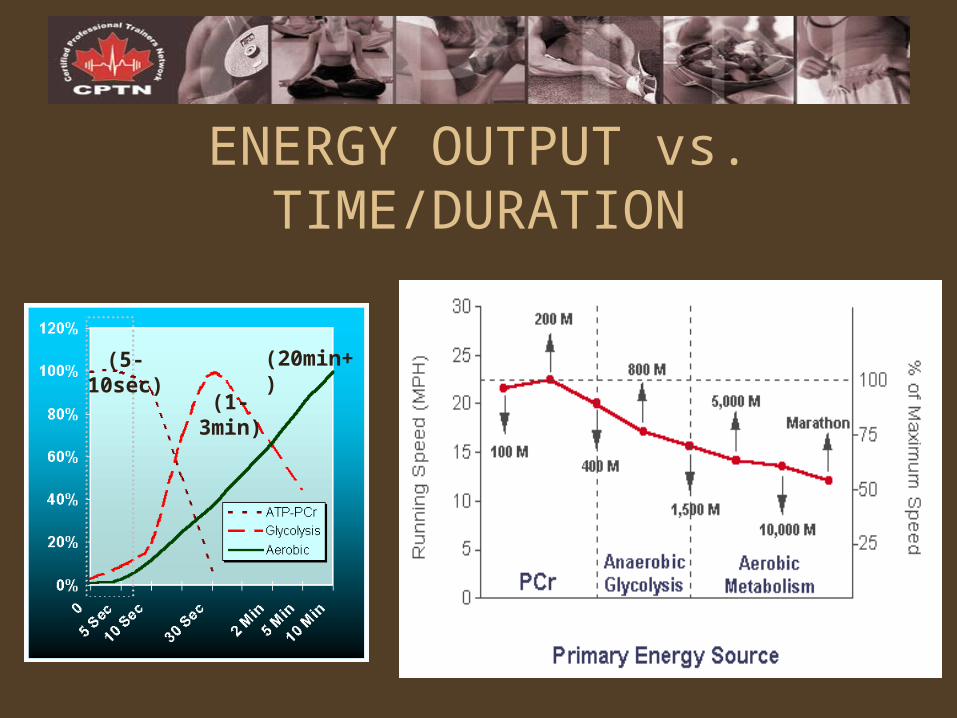
ENERGY OUTPUT vs. TIME/DURATION
(5-10sec)
(1-3min)
(20min+)
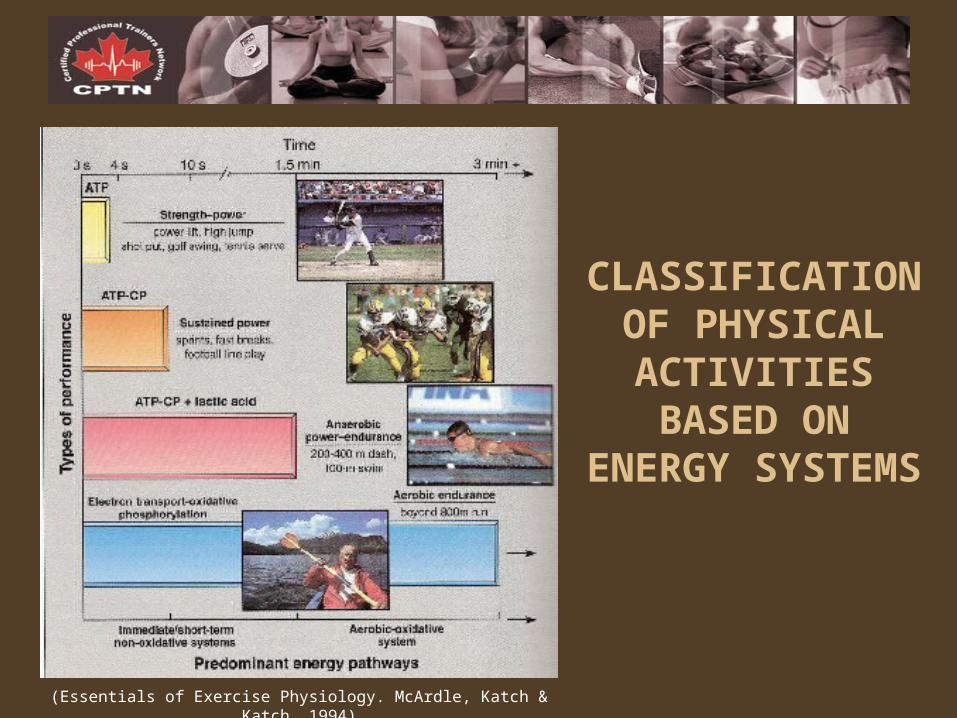
(Essentials of Exercise Physiology. McArdle, Katch & Katch. 1994)
CLASSIFICATION OF PHYSICAL
ACTIVITIES BASED ON ENERGY
SYSTEMS
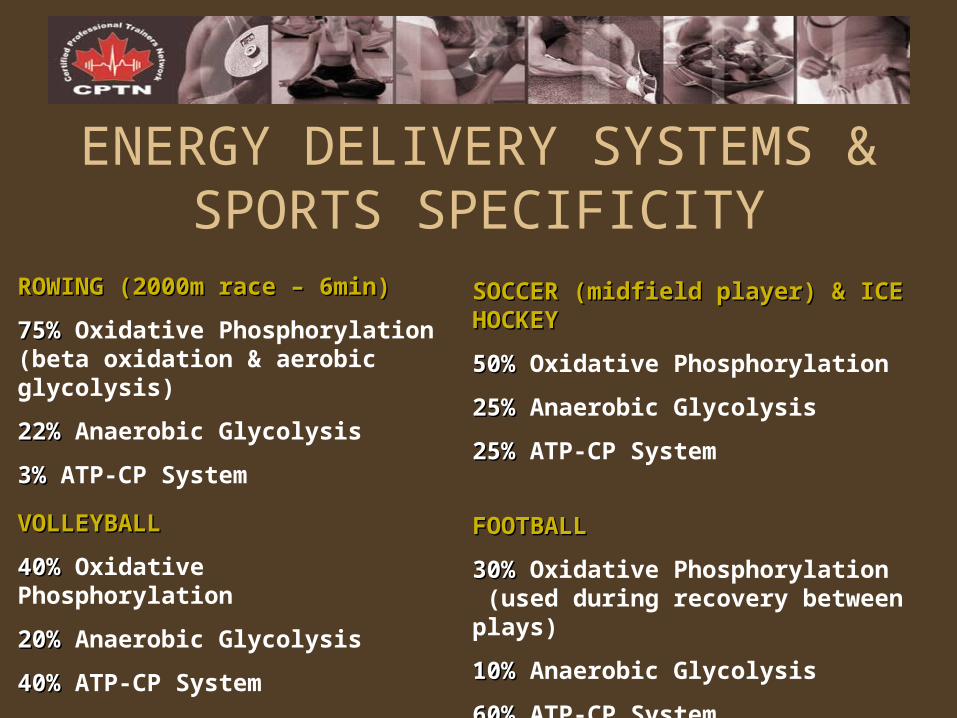
ENERGY DELIVERY SYSTEMS & SPORTS SPECIFICITY
ROWING (2000m race – 6min)ROWING (2000m race – 6min)
75%75% Oxidative Phosphorylation (beta oxidation & aerobic glycolysis)
22%22% Anaerobic Glycolysis
3%3% ATP-CP System
SOCCER (midfield player) & ICE HOCKEYSOCCER (midfield player) & ICE HOCKEY
50%50% Oxidative Phosphorylation
25%25% Anaerobic Glycolysis
25%25% ATP-CP System
VOLLEYBALLVOLLEYBALL
40%40% Oxidative Phosphorylation
20%20% Anaerobic Glycolysis
40%40% ATP-CP System
FOOTBALLFOOTBALL
30%30% Oxidative Phosphorylation (used during recovery between plays)
10%10% Anaerobic Glycolysis
60%60% ATP-CP System
O.F.I.T.T.
• Objective:Objective: Based on S.M.A.R.T. Goals
• Frequency:Frequency: Affected by Intensity & Duration
• Intensity:Intensity: Dictates specific physiologic & metabolic changes
• Time:Time: Duration which intensity level is maintained; Duration & Intensity inversely related (“You can train hard or you can train long, but you can’t do both”)
• Type:Type: Exercise/Equipment selection
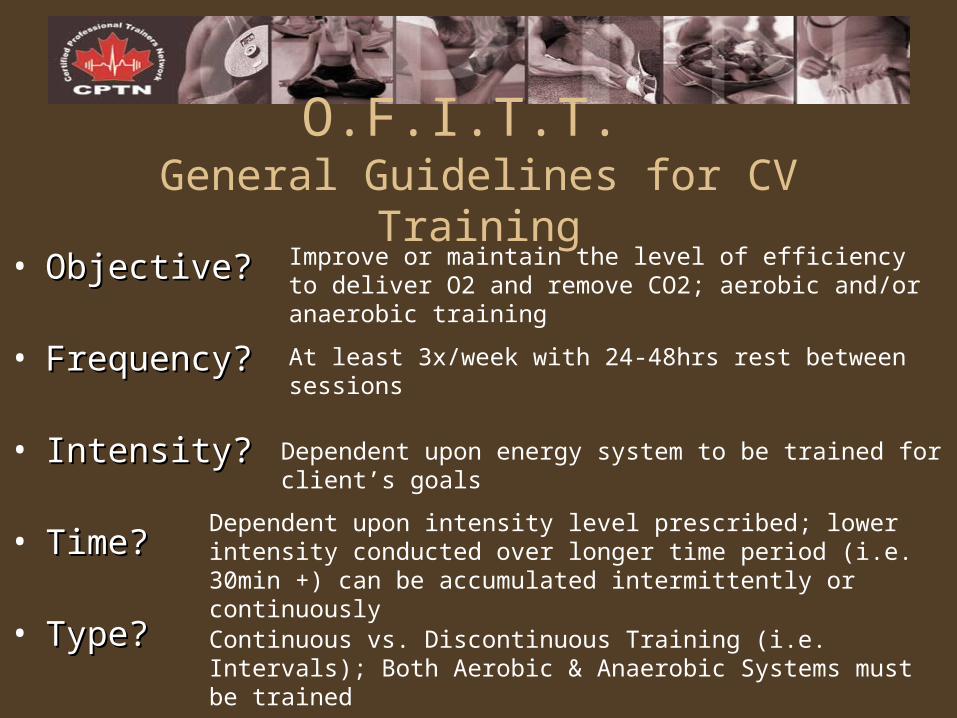
O.F.I.T.T. General Guidelines for CV Training
• Objective?Objective?
• Frequency?Frequency?
• Intensity?Intensity?
• Time?Time?
• Type?Type?
Improve or maintain the level of efficiency to deliver O2 and remove CO2; aerobic and/or anaerobic training
At least 3x/week with 24-48hrs rest between sessions
Dependent upon energy system to be trained for client’s goals
Dependent upon intensity level prescribed; lower intensity conducted over longer time period (i.e. 30min +) can be accumulated intermittently or continuously
Continuous vs. Discontinuous Training (i.e. Intervals); Both Aerobic & Anaerobic Systems must be trained
PARTNER EXERCISE:PARTNER EXERCISE: Using the case study assigned to you from the back of the manual determine 1) your client’s S.M.A.R.T. Goals, and 2) apply the O.F.I.T.T. principle to design their CV program. Be prepared to share with the rest of the class.
Improvement & Maintenance1. What is the minimum FREQUENCY, INTENSITY and DURATION/TIME
required to maintain aerobic fitness (the central factors)?
2. What is the minimum FREQUENCY, INTENSITY, DURATION/TIME and EFFORT INTERVALS required to maintain anaerobic fitness (the peripheral factors)?
Objective: Enhance muscle’s ATP-CP energy capacity– 5-10 second max output bursts followed by 30-120sec active
recovery; Alternate between 2+ work intervals and 2+ recovery intervals
– Adaptation occurs within 2-4 weeks. Detraining will take effect within 2 weeks.
• Note: high risk training; potential injuries associated with this type of training.
• Especially important to warm up and cool down. • Benefits = sprinters/events lasting less than 20 sec.
Specific Guidelines for ATP-CP System
Objective: Elevate Lactate Threshold Levels– Sub max levels of intensity will not stimulate adaptation.
Need to train at level that will elicit lactic acid production.
– Train 2-3x/week (ample time for recovery); 2-3 min effort intervals followed by 2-3 min recovery intervals; repeat 2-12x
– 2-3 min recovery is not enough time to deplete lactic acid from blood, therefore lactate threshold must elevate to accommodate the training stimulus.
• Note: complete LT training at least 2 weeks before competition• Benefits: Everyone, but the highest injury rate.
Specific Guidelines for Glycolytic System
Objective: Improve body’s ability to deliver O2 and remove CO2 through central factors
– Sub-maximal training; 60-80% MHR, 20min +– Not necessarily “sport specific”– Most benefits are central adaptations involving the
heart circulatory and respiratory systems.• Note: the most appropriate introductory cardiovascular
program to start with to build a good fitness base.
Specific Guidelines for Oxidative System
ATP-CP INTERVAL TRAINING: 5-10 second max output bursts (95-100% HRR; RPE = 9-10) followed by 30-120sec active recovery; Alternate between 2+ work intervals and 2+ recovery intervals
GLYCOLYTIC INTERVAL TRAINING: 2-3 min effort intervals (85-95% HRR; RPE = 7-8) followed by 2-3 min recovery intervals; repeat 2-12x
Example 1:Example 1: 30sec (max intensity) / 30sec (active rest), repeat 4-12x
Example 2:Example 2: 90sec (90% HRR) / 90sec (recovery), repeat 10x
Example 3:Example 3: 60sec (85% HRR) / 120sec (70% HRR), repeat 7x
Example 4:Example 4: 120sec (85% HRR) / 60sec (70% HRR), repeat 7x
Example 5:Example 5: 3min (75-85% HRR) / 1min (60% HRR), repeat 11x
SMALL GROUP EXERCISE: Sample Interval Training Programs
Indicate the training objective for each sample program:
Over-trainingIndicated by a plateau or drop in performance over a period of several
days; caused by too little recovery time between sessions
A)TRACK RESTING HEART RATE
B)TRACK TRAINING HEART RATE
>10% over previous values = over-training
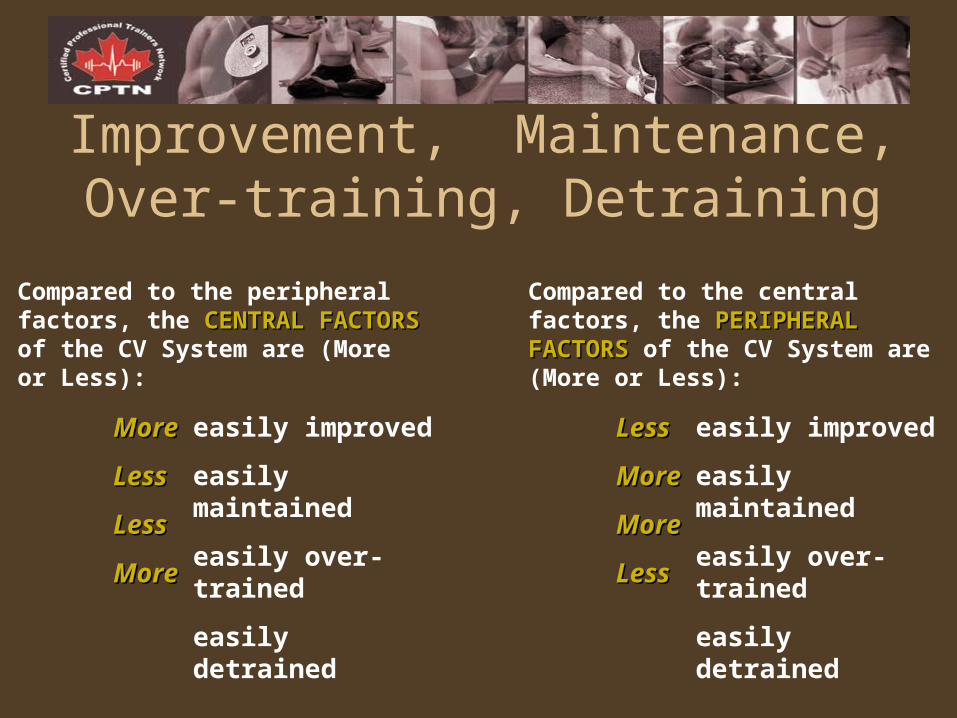
Improvement, Maintenance, Over-training, Detraining
Compared to the peripheral factors, the CENTRAL FACTORSCENTRAL FACTORS of the CV System are (More or Less):
Compared to the central factors, the PERIPHERAL FACTORSPERIPHERAL FACTORS of the CV System are (More or Less):
easily improved
easily maintained
easily over-trained
easily detrained
easily improved
easily maintained
easily over-trained
easily detrained
MoreMore
LessLess
LessLess
MoreMore
LessLess
MoreMore
MoreMore
LessLess
ASSIGNMENT: The Great Debates
1. Which is better for fat loss…Longer Duration, Lower Intensity OR Shorter Duration, Higher Intensity?
2. Which is a better workout order…Cardio before or after Weights?
CARDIO CONFUSIONCARDIO CONFUSION
EXERCISE PHYSIOLOGY & PROGRAM DESIGN FOR MUSCULAR FITNESS
LEARNING OBJECTIVESLEARNING OBJECTIVES
1. To understand the neuromuscular responses and adaptations to resistance training
2. To understand muscle microstructure, and the role of actin and myosin in muscle actions
3. To apply an understanding of the relationship between different muscle fibre types and muscle fibre recruitment to the design of resistance training programs
4. To understand the relationship between the various energy systems and muscle fibre types
5. To understand the application of the fundamental principles of training to the design of resistance training programs
6. To understand the relationship between the different training objectives of Strength, Power, Endurance and Mass and the application of O.F.I.T.T. in the design of resistance training programs that meet these objectives
7. To understand the application of O.F.I.T.T. in the resistance training continuum (improvement vs. maintenance vs. over-training vs. detraining)
8. To explore controversies in the design of resistance training programs
MAJOR GOALS OF STRENGTH CONDITIONING
STRENGTHSTRENGTH
ENDURANCEENDURANCE
POWERPOWER
MUSCLE MASS & TONEMUSCLE MASS & TONE
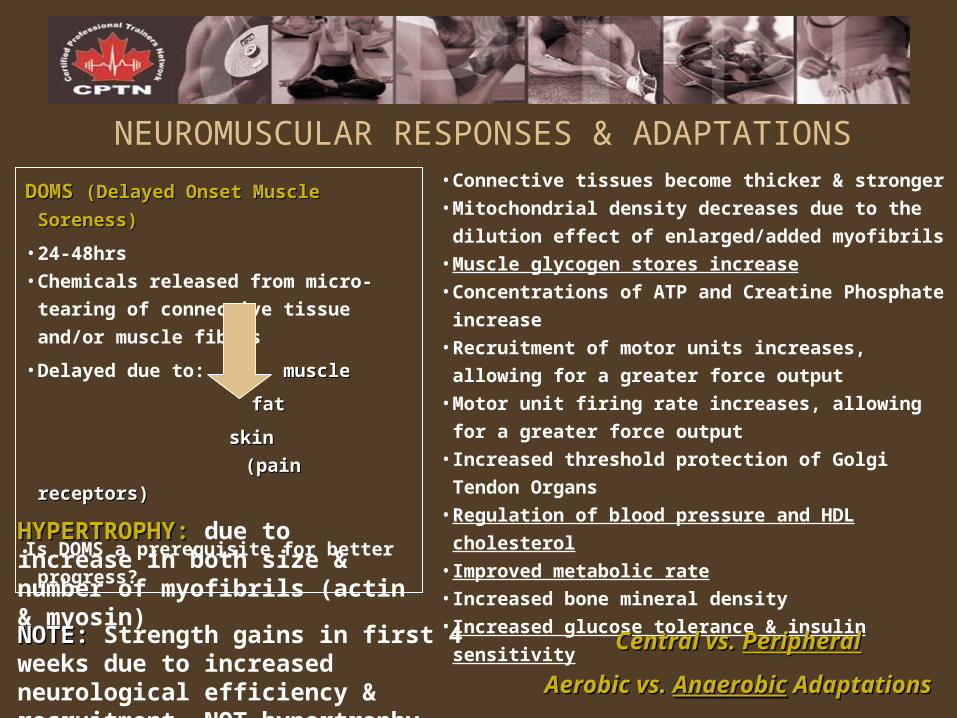
NEUROMUSCULAR RESPONSES & ADAPTATIONS• Connective tissues become thicker & stronger
• Mitochondrial density decreases due to the dilution
effect of enlarged/added myofibrils
• Muscle glycogen stores increase
• Concentrations of ATP and Creatine Phosphate increase
• Recruitment of motor units increases, allowing for a
greater force output
• Motor unit firing rate increases, allowing for a greater
force output
• Increased threshold protection of Golgi Tendon Organs
• Regulation of blood pressure and HDL cholesterol
• Improved metabolic rate
• Increased bone mineral density
• Increased glucose tolerance & insulin sensitivity
DOMS DOMS (Delayed Onset Muscle Soreness)(Delayed Onset Muscle Soreness)
• 24-48hrs
• Chemicals released from micro-tearing of
connective tissue and/or muscle fibres
• Delayed due to: musclemuscle
fatfat
skinskin
(pain receptors)(pain receptors)
Is DOMS a prerequisite for better
progress?
Central vs. Central vs. PeripheralPeripheral
Aerobic vs. Aerobic vs. AnaerobicAnaerobic Adaptations Adaptations
HYPERTROPHY:HYPERTROPHY: due to increase in both size & number of myofibrils (actin & myosin)
NOTE:NOTE: Strength gains in first 4 weeks due to increased neurological efficiency & recruitment, NOT hypertrophy
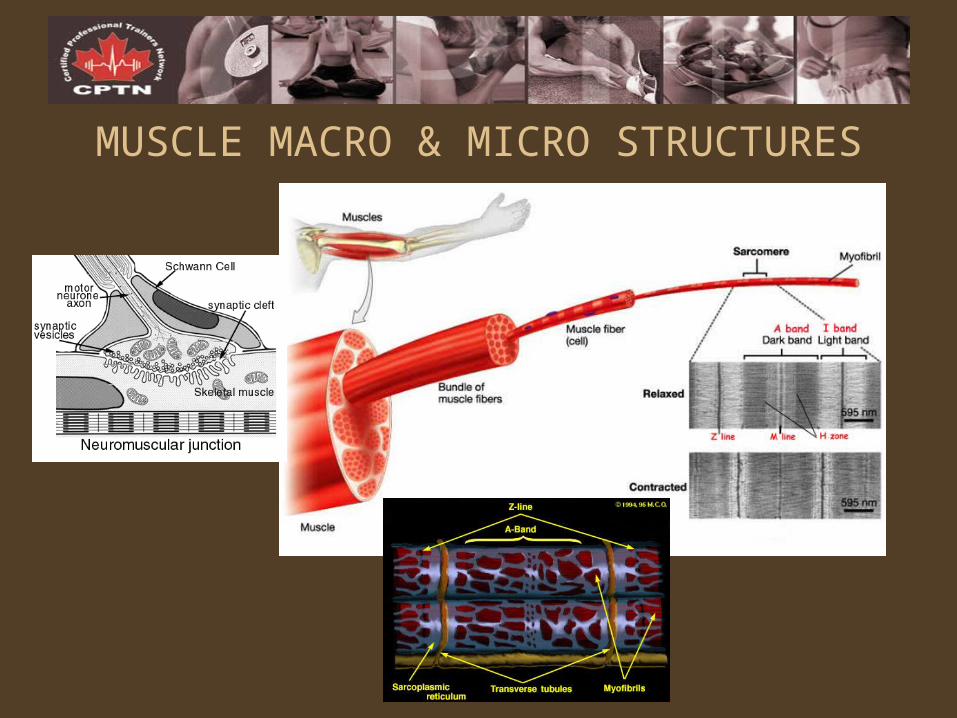
MUSCLE MACRO & MICRO STRUCTURES
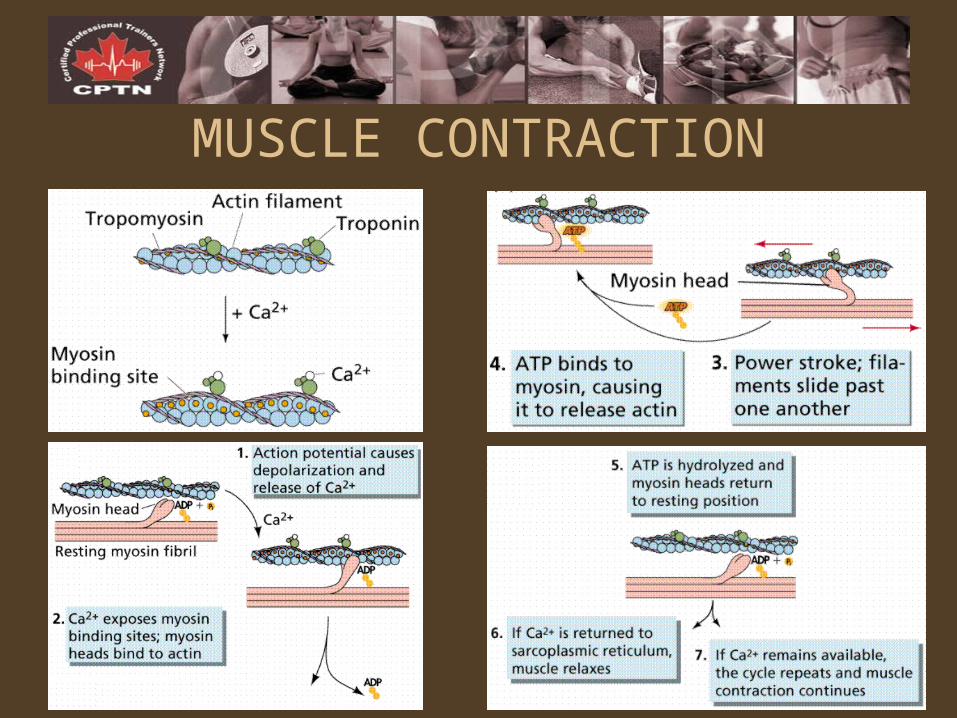
MUSCLE CONTRACTION
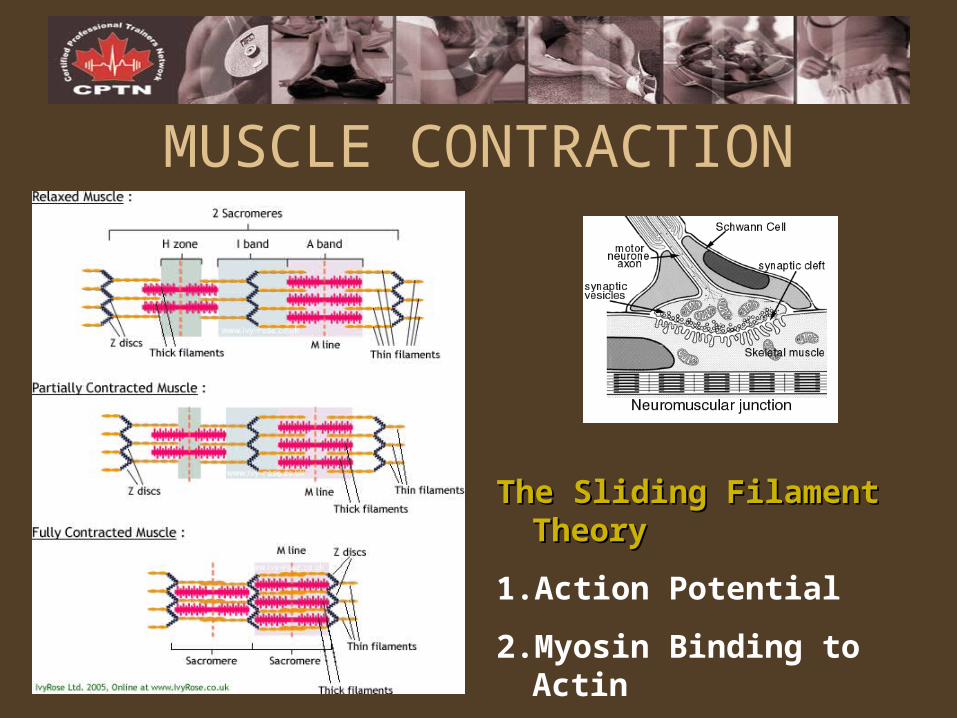
MUSCLE CONTRACTION
The Sliding Filament TheoryThe Sliding Filament Theory
1. Action Potential
2. Myosin Binding to Actin
3. The Power Stroke
TYPES OF MUSCLE ACTIONSISOMETRIC:ISOMETRIC: Muscle contracts with no change in its length during force production.
CONCENTRIC:CONCENTRIC: Positive muscle action whereby the muscle is shortened under its own force.
ECCENTRIC:ECCENTRIC: Negative muscle action whereby the muscle resists while it is forced to lengthen.
During which type of contractions can you lift a) the most weight, and b) the least amount of weight?
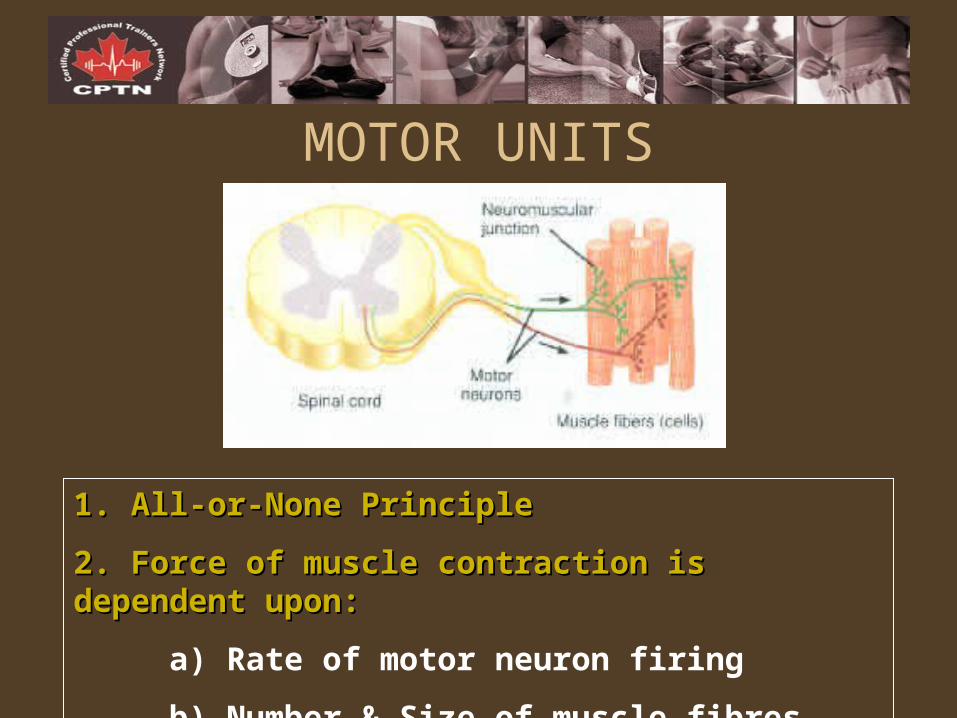
MOTOR UNITS
1. All-or-None Principle1. All-or-None Principle
2. Force of muscle contraction is dependent upon:2. Force of muscle contraction is dependent upon:
a) Rate of motor neuron firing
b) Number & Size of muscle fibres innervated
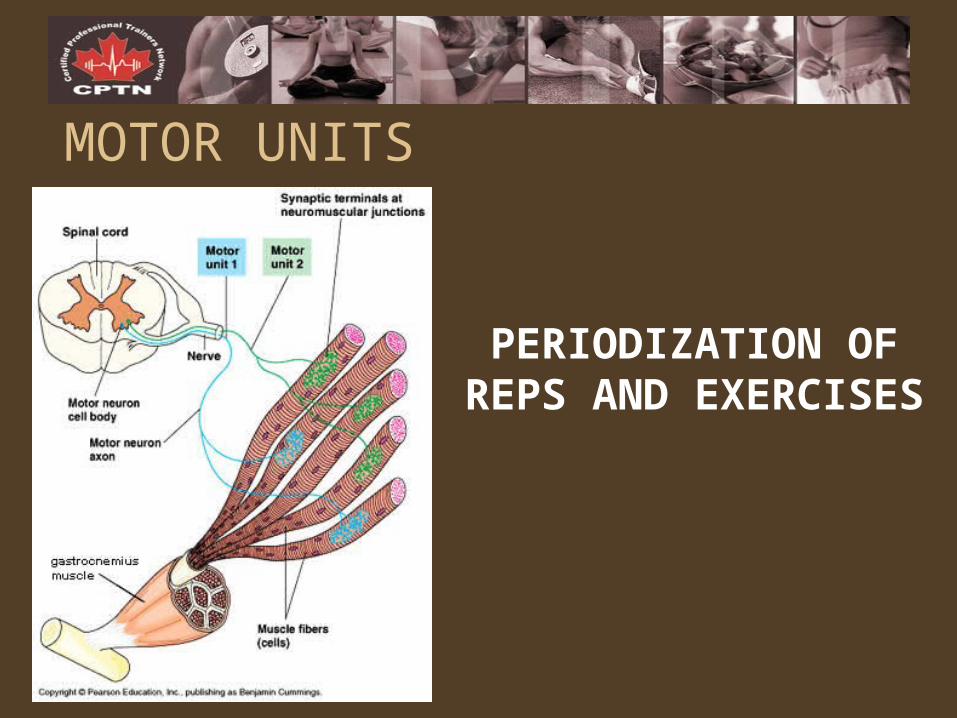
MOTOR UNITS
PERIODIZATION OF REPS AND EXERCISES
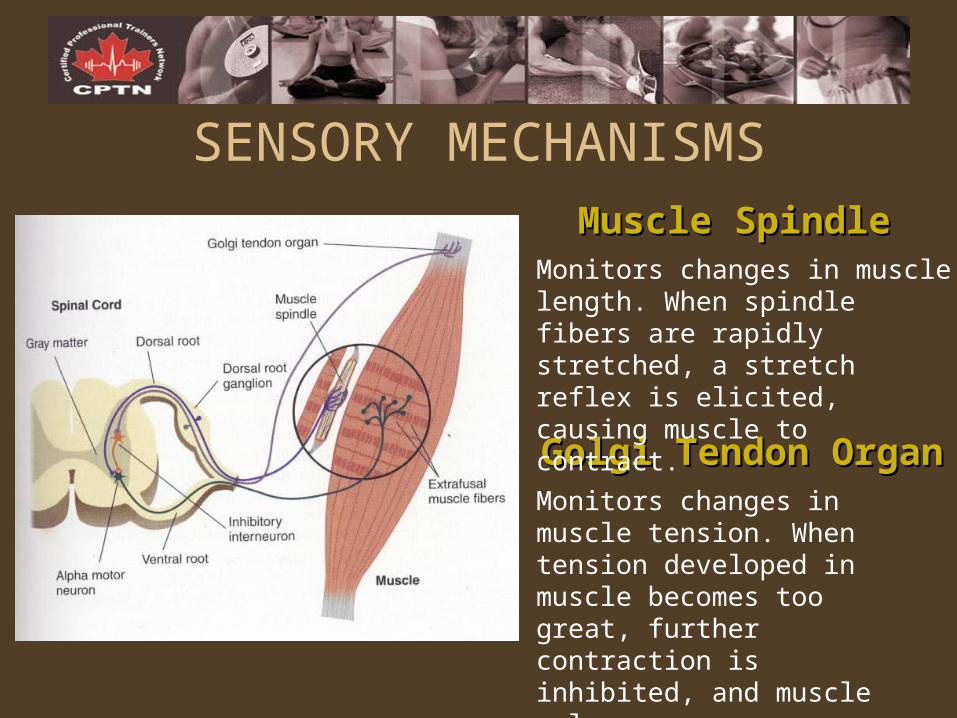
SENSORY MECHANISMS
Golgi Tendon OrganGolgi Tendon Organ
Muscle SpindleMuscle SpindleMonitors changes in muscle length. When spindle fibers are rapidly stretched, a stretch reflex is elicited, causing muscle to contract.
Monitors changes in muscle tension. When tension developed in muscle becomes too great, further contraction is inhibited, and muscle relaxes.
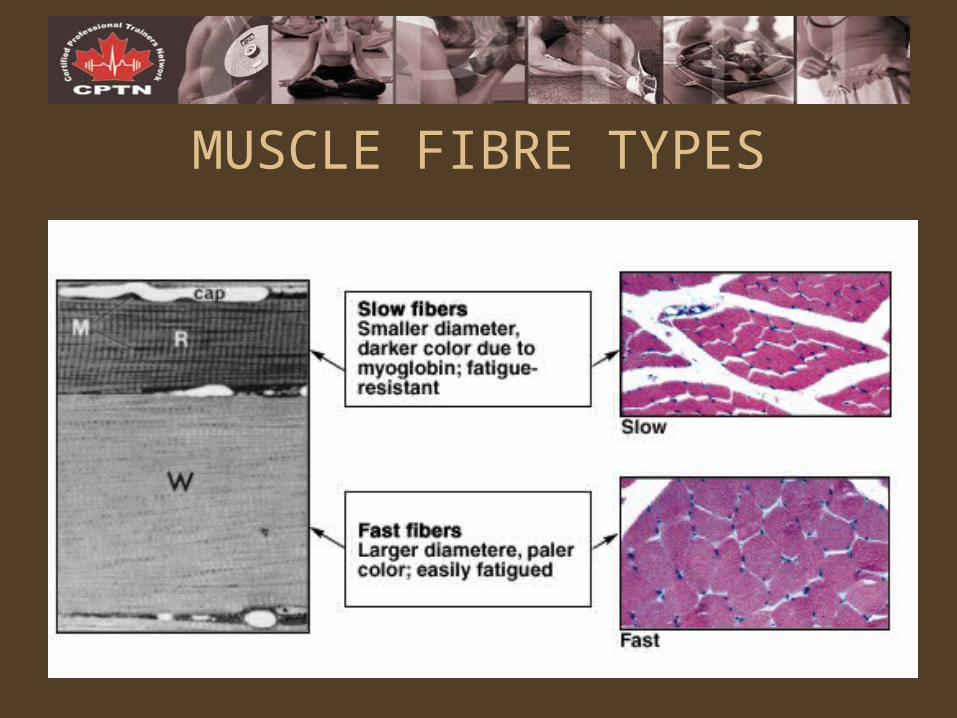
MUSCLE FIBRE TYPES
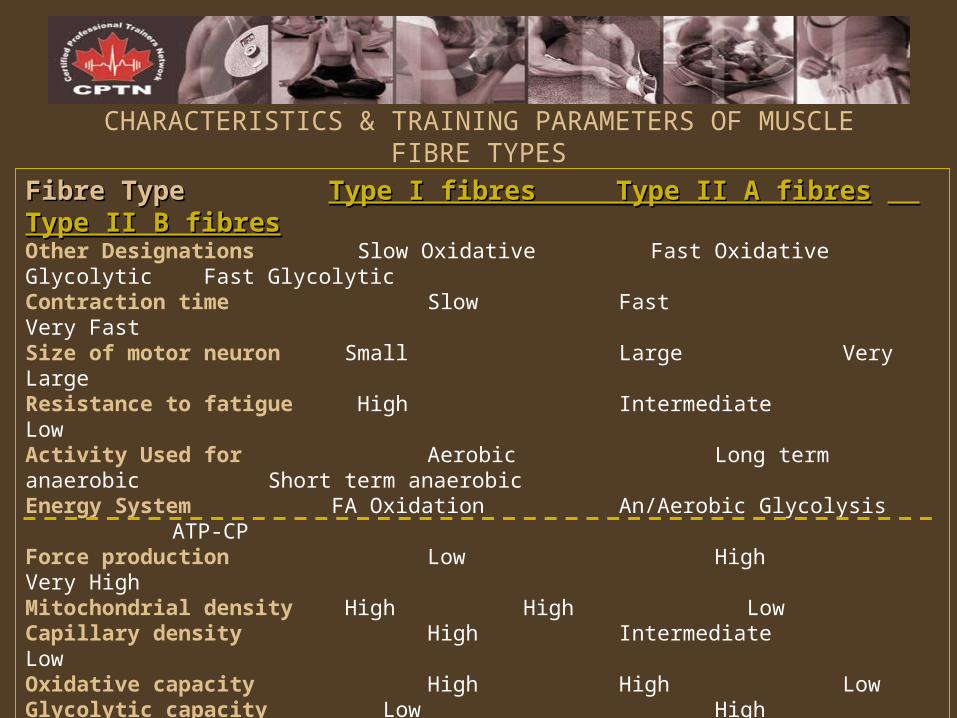
CHARACTERISTICS & TRAINING PARAMETERS OF MUSCLE FIBRE TYPES
Fibre TypeFibre Type Type I fibres Type II A fibresType I fibres Type II A fibres Type II B fibres Type II B fibres Other Designations Slow Oxidative Fast Oxidative Glycolytic Fast GlycolyticContraction time Slow Fast Very Fast Size of motor neuron Small Large Very LargeResistance to fatigue High Intermediate LowActivity Used for Aerobic Long term anaerobic Short term anaerobicEnergy System FA Oxidation An/Aerobic Glycolysis ATP-CPForce production Low High Very HighMitochondrial density High High LowCapillary density High Intermediate Low Oxidative capacity High High LowGlycolytic capacity Low High HighMajor storage fuel Triglycerides CP, Glycogen CP, Glycogen
Training Objective Endurance Mass, Strength Strength, PowerType of Adaptation Biochemical Structural NeuralIntensity (%RM) <70% 85-70% 95-85%Repetitions 15-30 6-12 3-6Sets 1-3 3-5 B=3-5, A=5-8Rest Between Sets 20-90sec 30-120sec 2-5min Rep Speed slow/med/fast slow to med slow/med/fast
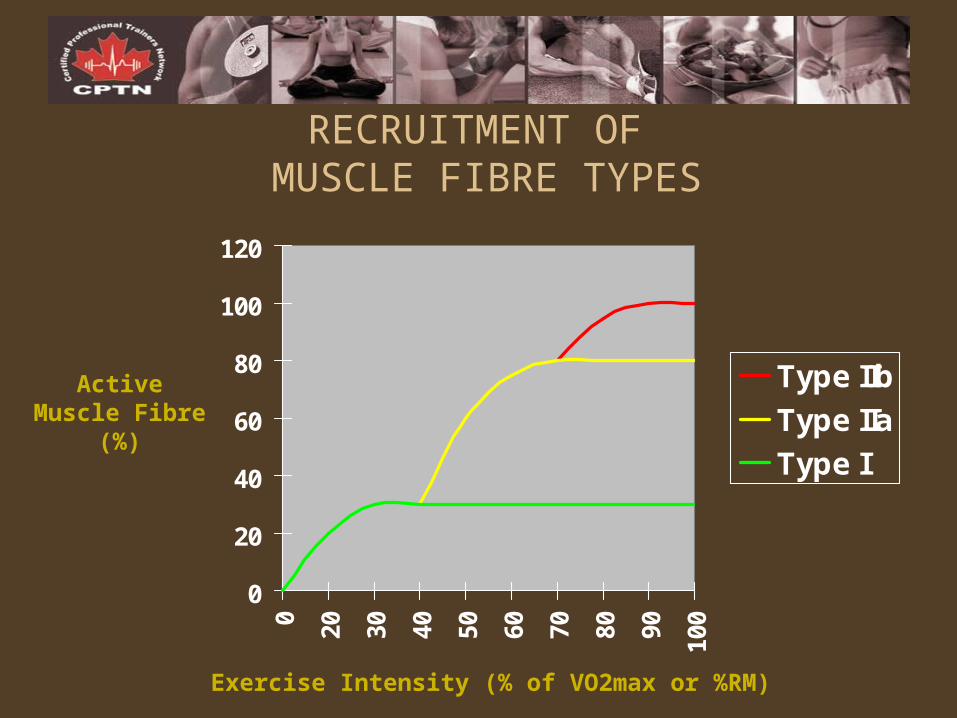
RECRUITMENT OF MUSCLE FIBRE TYPES
0
20
40
60
80
100
120
0 20 30 40 50 60 70 80 90 100
Type IIb
Type IIa
Type I
Exercise Intensity (% of VO2max or %RM)
Active Muscle Fibre (%)
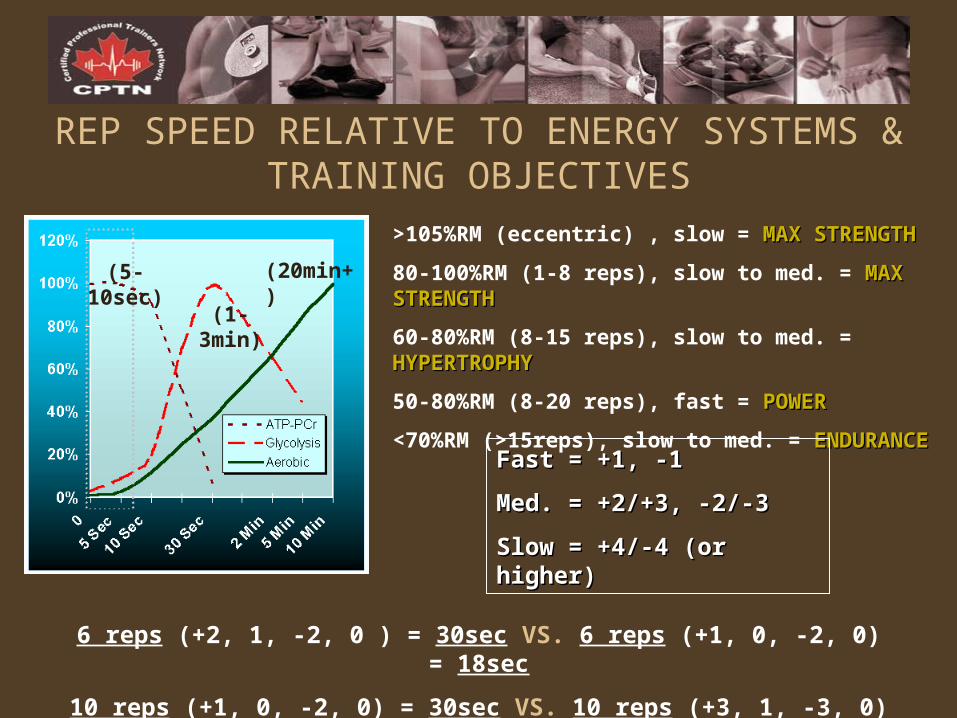
REP SPEED RELATIVE TO ENERGY SYSTEMS & TRAINING OBJECTIVES
>105%RM (eccentric) , slow = MAX STRENGTHMAX STRENGTH
80-100%RM (1-8 reps), slow to med. = MAX STRENGTHMAX STRENGTH
60-80%RM (8-15 reps), slow to med. = HYPERTROPHYHYPERTROPHY
50-80%RM (8-20 reps), fast = POWERPOWER
<70%RM (>15reps), slow to med. = ENDURANCEENDURANCE
(5-10sec)
(1-3min)
(20min+)
Fast = +1, -1Fast = +1, -1
Med. = +2/+3, -2/-3Med. = +2/+3, -2/-3
Slow = +4/-4 (or higher)Slow = +4/-4 (or higher)
6 reps (+2, 1, -2, 0 ) = 30sec VS. 6 reps (+1, 0, -2, 0) = 18sec
10 reps (+1, 0, -2, 0) = 30sec VS. 10 reps (+3, 1, -3, 0) = 70sec
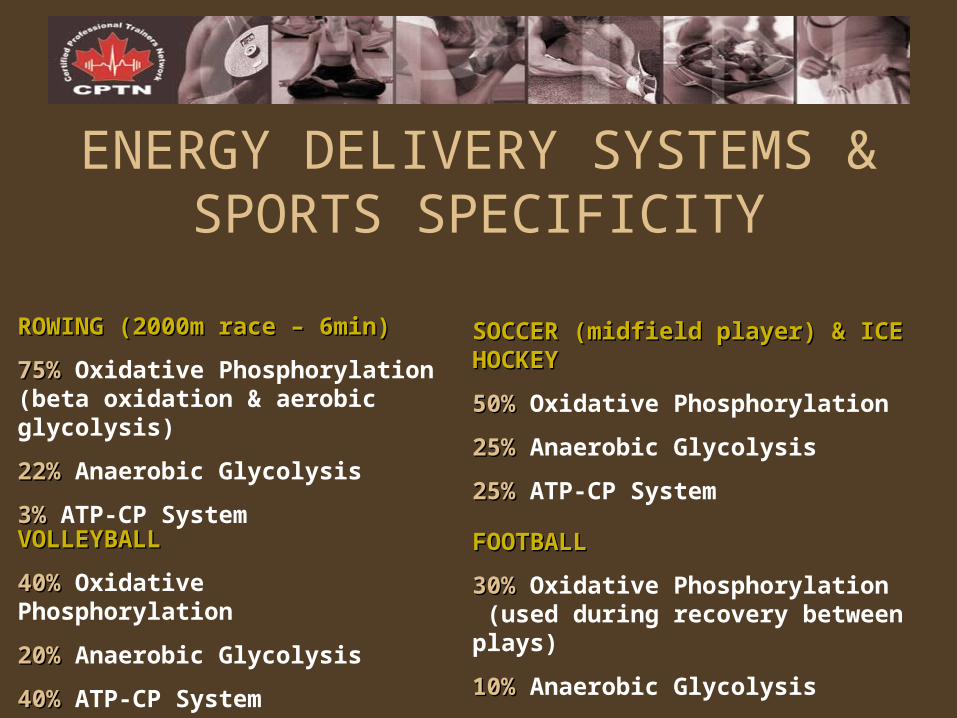
ENERGY DELIVERY SYSTEMS & SPORTS SPECIFICITY
ROWING (2000m race – 6min)ROWING (2000m race – 6min)
75%75% Oxidative Phosphorylation (beta oxidation & aerobic glycolysis)
22%22% Anaerobic Glycolysis
3%3% ATP-CP System
SOCCER (midfield player) & ICE HOCKEYSOCCER (midfield player) & ICE HOCKEY
50%50% Oxidative Phosphorylation
25%25% Anaerobic Glycolysis
25%25% ATP-CP System
VOLLEYBALLVOLLEYBALL
40%40% Oxidative Phosphorylation
20%20% Anaerobic Glycolysis
40%40% ATP-CP System
FOOTBALLFOOTBALL
30%30% Oxidative Phosphorylation (used during recovery between plays)
10%10% Anaerobic Glycolysis
60%60% ATP-CP System
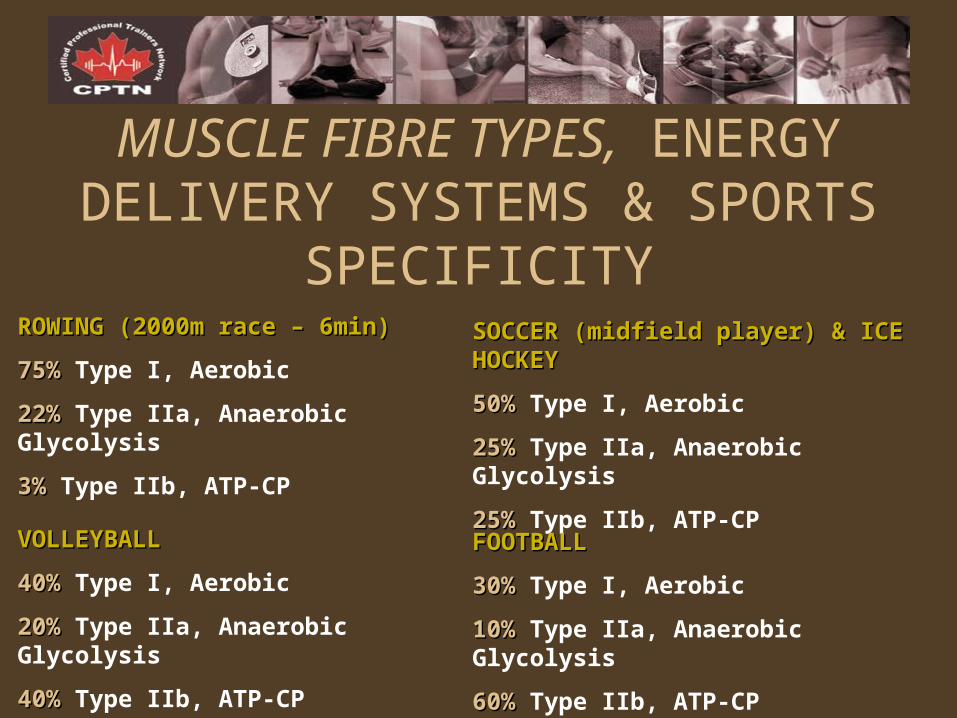
MUSCLE FIBRE TYPES, ENERGY DELIVERY SYSTEMS & SPORTS
SPECIFICITYROWING (2000m race – 6min)ROWING (2000m race – 6min)
75%75% Type I, Aerobic
22%22% Type IIa, Anaerobic Glycolysis
3%3% Type IIb, ATP-CP
SOCCER (midfield player) & ICE HOCKEYSOCCER (midfield player) & ICE HOCKEY
50%50% Type I, Aerobic
25%25% Type IIa, Anaerobic Glycolysis
25%25% Type IIb, ATP-CP
VOLLEYBALLVOLLEYBALL
40%40% Type I, Aerobic
20%20% Type IIa, Anaerobic Glycolysis
40%40% Type IIb, ATP-CP
FOOTBALLFOOTBALL
30%30% Type I, Aerobic
10%10% Type IIa, Anaerobic Glycolysis
60%60% Type IIb, ATP-CP
METABOLIC & BIOMECHANIC SPORTS SPECIFICITY
Energy Systems
Muscle Fibre Types
Movement Patterns
Muscle Groups
Nutritional Needs
- Energy expenditure
- Energy pathways
- Biochemical vs. Structural vs. Neural adaptations
Contraction Types
RESISTANCE TRAINING TERMINOLOGYISOKINETIC CONTRACTION:ISOKINETIC CONTRACTION: Muscle action through a constant speed causing the muscle to exert a continuous and maximum force throughout a given ROM.
DYNAMIC CONSTANT CONTRACTION (ISOTONIC):DYNAMIC CONSTANT CONTRACTION (ISOTONIC): Muscle action against a constant resistance.
DYNAMIC VARIABLE CONTRACTION:DYNAMIC VARIABLE CONTRACTION: Muscle action against a changing resistance.
REPETITION:REPETITION: A single, complete action of any one given exercise beginning from starting position, progressing to its ending position, and returning to its starting position.
SETS:SETS: A given number of complete and continuous repetitions performed consecutively without resting.
LOAD:LOAD: The amount of resistance against which a muscular force is being applied.
REP RANGE:REP RANGE: Includes both a lower limit (least # of reps to be completed) as well as an upper limit (most # of reps to be completed).
REPETITION MAXIMUM:REPETITION MAXIMUM: Maximum load that can be lifted during an exercise in an all-out effort over a given number of reps.
RESISTANCE TRAINING TERMINOLOGYCIRCUIT TRAINING ROUTINE:CIRCUIT TRAINING ROUTINE: Several different exercises are completed, one immediately after another, within the resistance training session.
REGULAR RESISTANCE TRAINING ROUTINE:REGULAR RESISTANCE TRAINING ROUTINE: Concentrating on one exercise at a time, multiple sets are completed for each exercise included within the resistance training session
STANDARD RESISTANCE TRAINING ROUTINE:STANDARD RESISTANCE TRAINING ROUTINE: For any one given exercise included within a regular resistance training session, the resistance, reps, and rest between sets remains constant.
VARIABLE RESISTANCE TRAINING ROUTINE:VARIABLE RESISTANCE TRAINING ROUTINE: For any one given exercise included within a regular resistance training session, the resistance, reps and/or rest between sets vary.
SMALL GROUP EXERCISE:SMALL GROUP EXERCISE: Design a “Standard Resistance Training Routine” and a “Variable Resistance Training Routine” for a muscle group of your choice.
FUNDAMENTAL PRINCIPLES OF TRAINING
Progressive ResistanceProgressive Resistance (The Double Progression System of Resistance Training)
1. Start with a conservative weight and reps consistent with the lower limit of the appropriate rep range.
2. With each successive resistance training session, increase reps by at least one at a time: Lower Limit +1, Lower Limit +2,…Upper Limit
3. When the upper limit of the rep range is completed with the initial weight, increase the intensity one level and drop the reps to the lower limit of the identified rep range
4. Complete the rep progression with the new weight.
PARTNER EXERCISE:PARTNER EXERCISE: Demonstrate the application of Progressive Resistance by performing 3 sets (10-15 reps/set) of an exercise (i.e. push-ups, lateral raises, bicep curls, etc.) and record the reps for each set. What will be your goal for your next workout with this exercise?
FUNDAMENTAL PRINCIPLES OF TRAINING
Progressive OverloadSpecificity (S.A.I.D.)IndividualityReversibilityVariabilityPeriodization
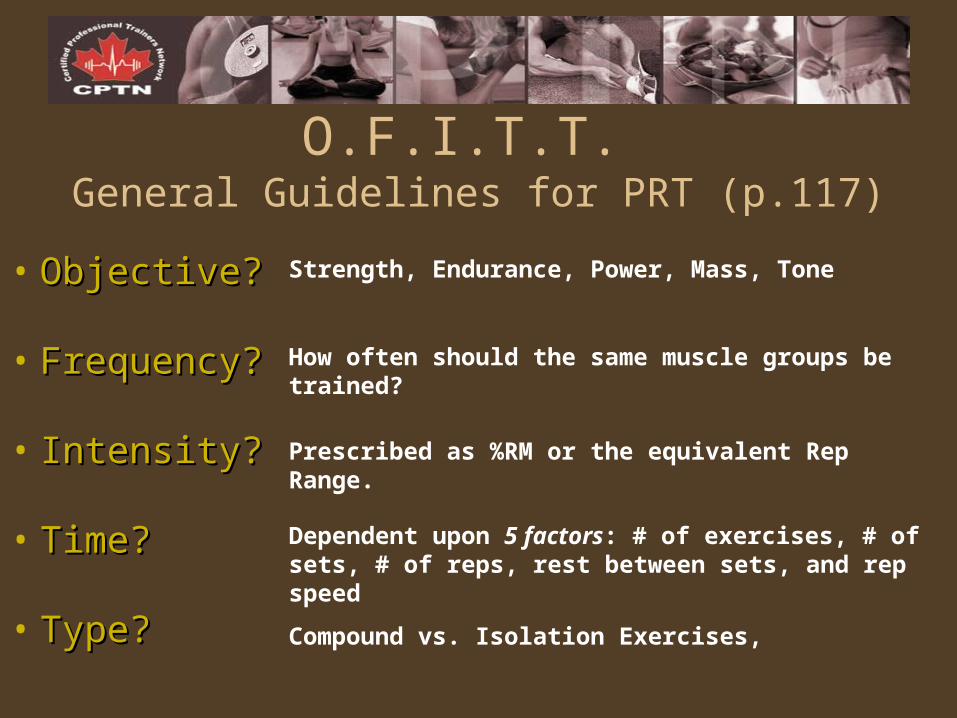
O.F.I.T.T. General Guidelines for PRT (p.117)
• Objective?Objective?
• Frequency?Frequency?
• Intensity?Intensity?
• Time?Time?
• Type?Type?
Strength, Endurance, Power, Mass, Tone
How often should the same muscle groups be trained?
Prescribed as %RM or the equivalent Rep Range.
Dependent upon 5 factors: # of exercises, # of sets, # of reps, rest between sets, and rep speed
Compound vs. Isolation Exercises,
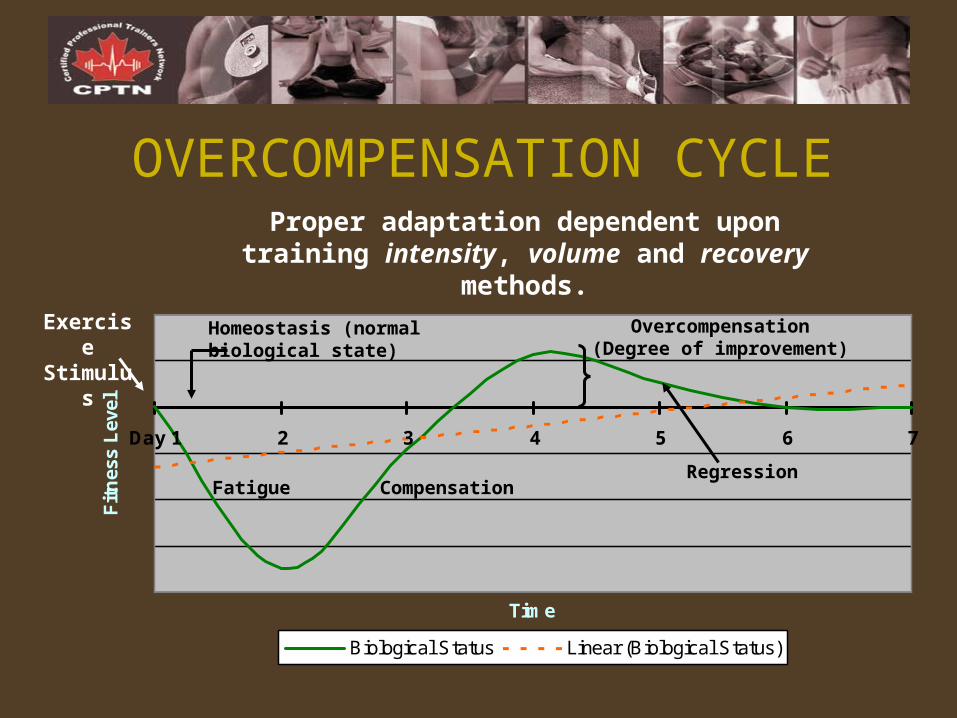
OVERCOMPENSATION CYCLE
Day 1 2 3 4 5 6 7
Time
Fit
nes
s L
evel
Biological Status Linear (Biological Status)
Proper adaptation dependent upon training intensity, volume and recovery methods.
Homeostasis (normal biological state)
Overcompensation(Degree of improvement)
Exercise Stimulus
Fatigue CompensationRegression
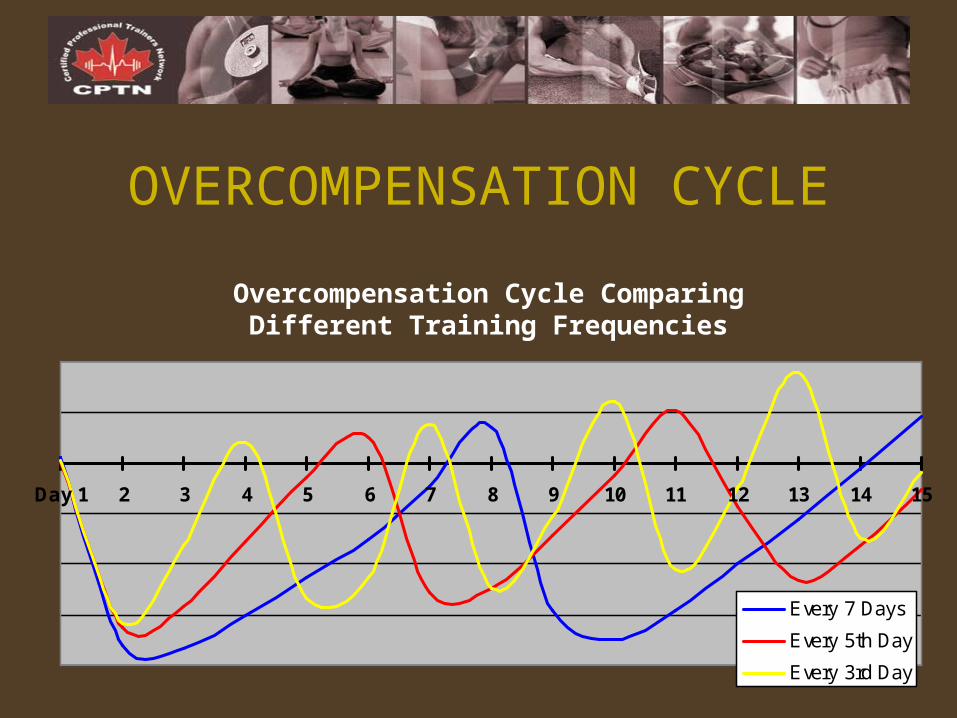
Day 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Every 7 Days
Every 5th Day
Every 3rd Day
OVERCOMPENSATION CYCLE
Overcompensation Cycle Comparing Different Training Frequencies
Improvement & Maintenance of Resistance Training Objectives
1. Your client has hit a plateau in their training program. Provide examples of 3 strategies you could apply to help stimulate new progress.
2. Your work schedule and family commitments are interfering with your personal fitness program. How can you adjust your training frequency, intensity, sets, reps and exercises to maintain your muscular fitness?
PARTNER EXERCISEPARTNER EXERCISE
Over-trainingIndicated by a plateau or drop in performance over a period of several
days; caused by too little recovery time between sessions
Risk of resistance over-training is associated with:
• Failure to schedule adequate rest between similar training sessions
• Failure to schedule “active rest” periods within micro-cycles
• Failure to schedule “active rest” periods within meso-cycles
• Failure to vary exercise intensities
• Increase in the number of sets per exercise beyond 4
• Increase in the number of exercises for a given muscle group
• Failure to vary exercises for a given muscle group
ASSIGNMENT: The Great Debates
1. Which is better for burning fat, what burns more calories…Cardio or Weight Training?
2. How much Cardio and how much Weight Training should I be doing to lose weight?
3. I don’t want to build muscle, I just want to tone. What kind of exercise program should I be following?
4. I have a difficult time putting on muscle…How do I build bigger arms and a bigger chest?
MUSCLE MYSTERIESMUSCLE MYSTERIES
ANATOMY (Upper Body) & PROGRAM DESIGN FOR MUSCULAR FITNESS
LEARNING OBJECTIVESLEARNING OBJECTIVES
1. To know the origin, insertion and line of action for the muscles of the upper body.
2. To apply knowledge of anatomy to effective exercises and be able to distinguish between the agonists, antagonists, synergists and stabilizers.
3. To apply an understanding of the advantages and disadvantages of compound versus isolation exercises in the design of resistance training programs.
4. To understand the application of general strength training guidelines in the design of programs.
5. To apply an understanding of a variety of specific resistance training principles commonly used in the design of programs.
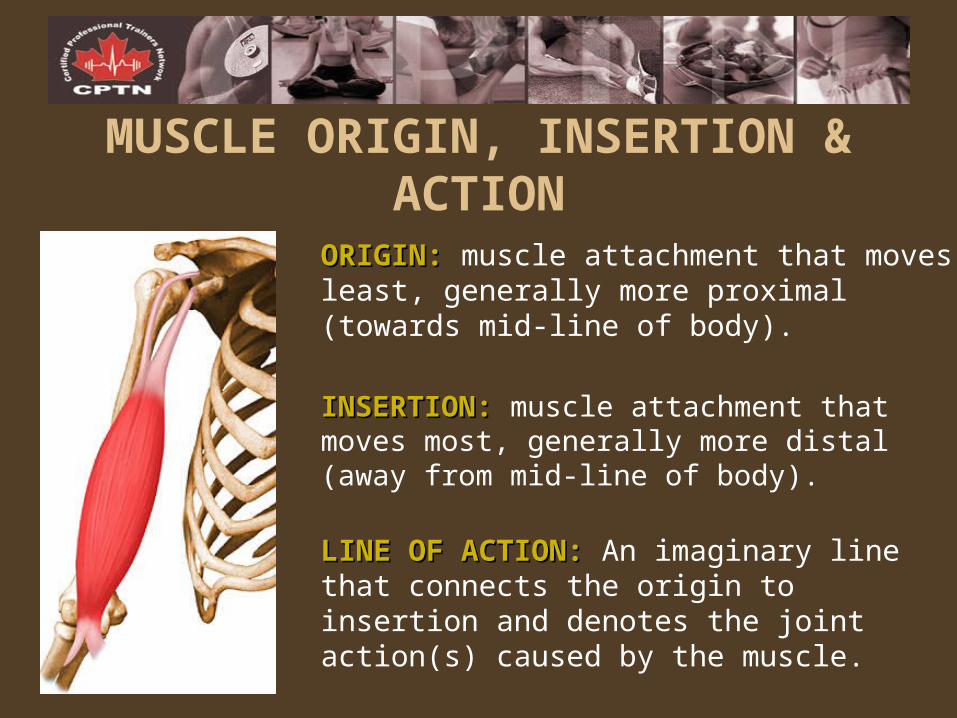
ORIGIN:ORIGIN: muscle attachment that moves least, generally more proximal (towards mid-line of body).
INSERTION:INSERTION: muscle attachment that moves most, generally more distal (away from mid-line of body).
LINE OF ACTION:LINE OF ACTION: An imaginary line that connects the origin to insertion and denotes the joint action(s) caused by the muscle.
MUSCLE ORIGIN, INSERTION & ACTION
Muscular ClassificationsAGONIST (prime mover):AGONIST (prime mover): muscle most directly involved with the movement
ANTAGONIST:ANTAGONIST: muscle opposite to the agonist that assists in joint stabilization and can slow down or stop the intended movement
SYNERGIST:SYNERGIST: muscle that assists the prime mover in a movement
STABILIZER:STABILIZER: muscle that stabilizes a joint; usually contracts isometrically as a joint is moved
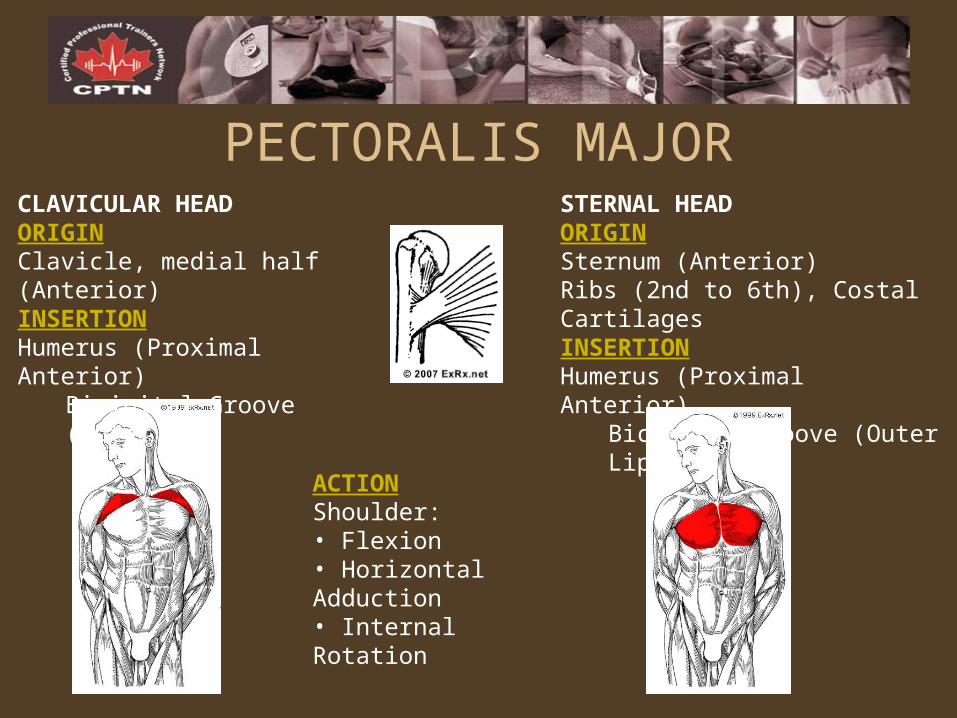
CLAVICULAR HEADORIGINClavicle, medial half (Anterior) INSERTIONHumerus (Proximal Anterior)
Bicipital Groove (Outer Lip)
STERNAL HEADORIGINSternum (Anterior) Ribs (2nd to 6th), Costal Cartilages INSERTIONHumerus (Proximal Anterior)
Bicipital Groove (Outer Lip)
ACTIONShoulder:• Flexion• Horizontal Adduction • Internal Rotation
PECTORALIS MAJOR
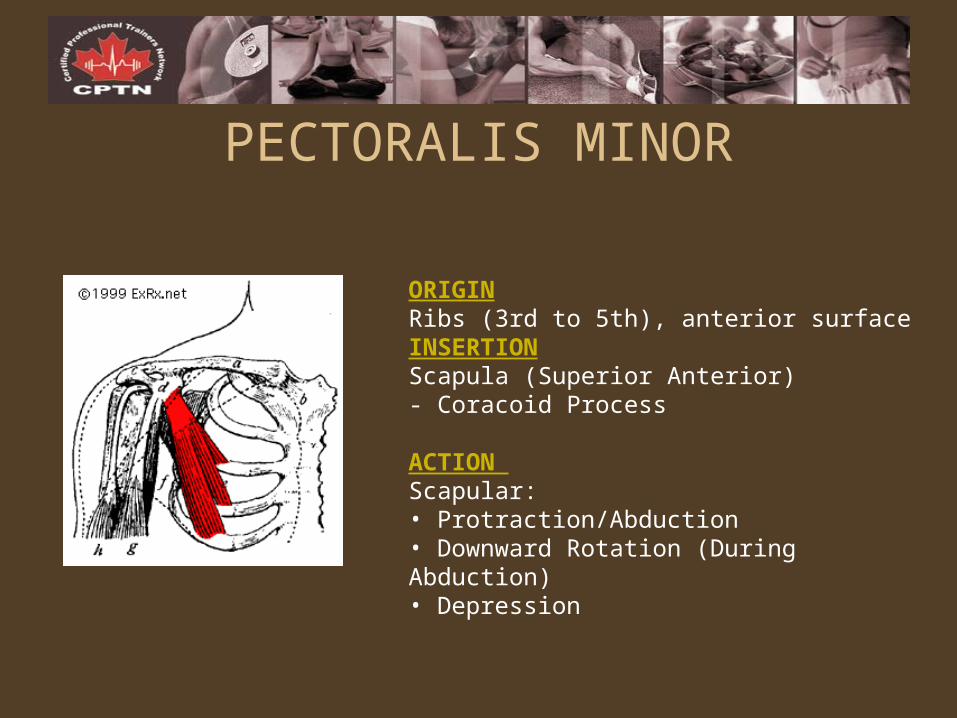
ORIGINRibs (3rd to 5th), anterior surface INSERTIONScapula (Superior Anterior)- Coracoid Process
ACTION Scapular:• Protraction/Abduction • Downward Rotation (During Abduction) • Depression
PECTORALIS MINOR
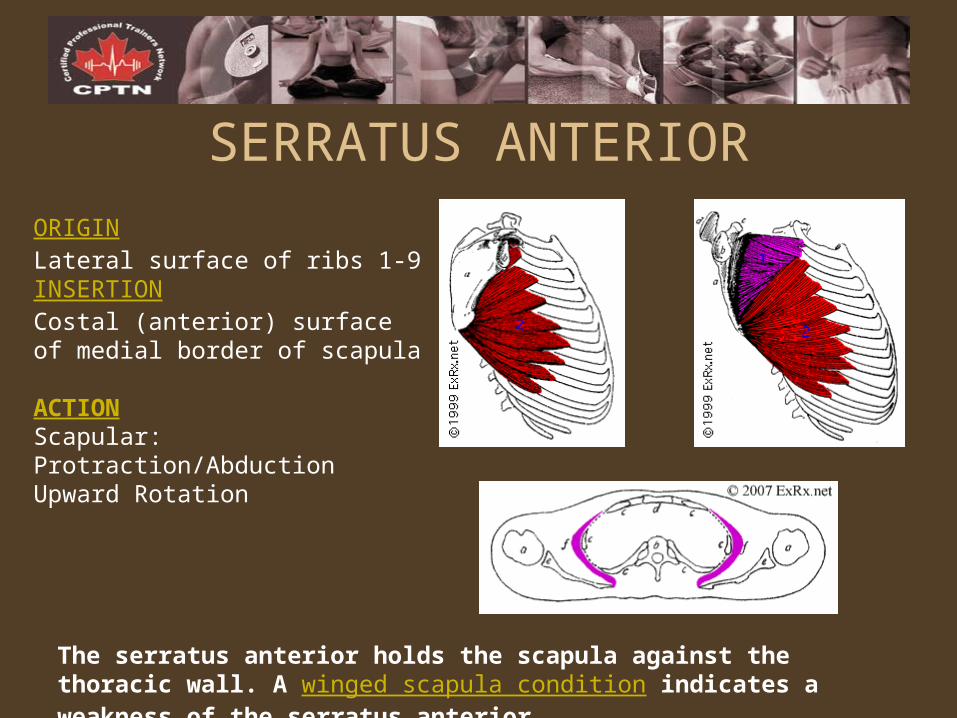
The serratus anterior holds the scapula against the thoracic wall. A winged scapula condition indicates a weakness of the serratus anterior.
ORIGINLateral surface of ribs 1-9 INSERTIONCostal (anterior) surface of medial border of scapula
ACTIONScapular:Protraction/AbductionUpward Rotation
SERRATUS ANTERIOR
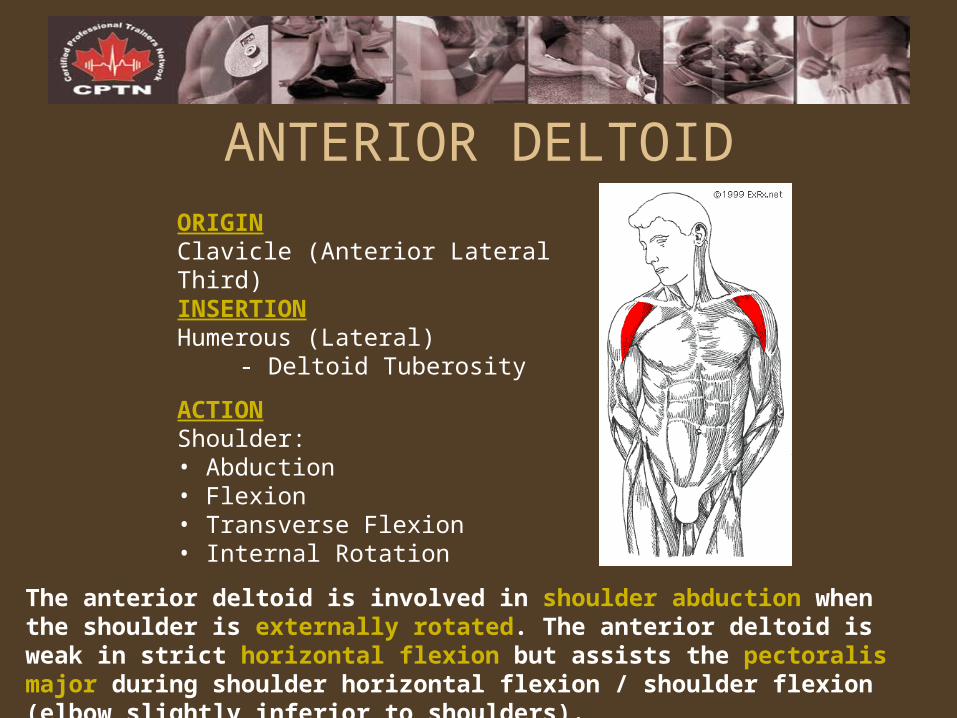
The anterior deltoid is involved in shoulder abduction when the shoulder is externally rotated. The anterior deltoid is weak in strict horizontal flexion but assists the pectoralis major during shoulder horizontal flexion / shoulder flexion (elbow slightly inferior to shoulders).
ORIGINClavicle (Anterior Lateral Third) INSERTIONHumerous (Lateral)
- Deltoid Tuberosity
ACTIONShoulder:• Abduction • Flexion • Transverse Flexion • Internal Rotation
ANTERIOR DELTOID
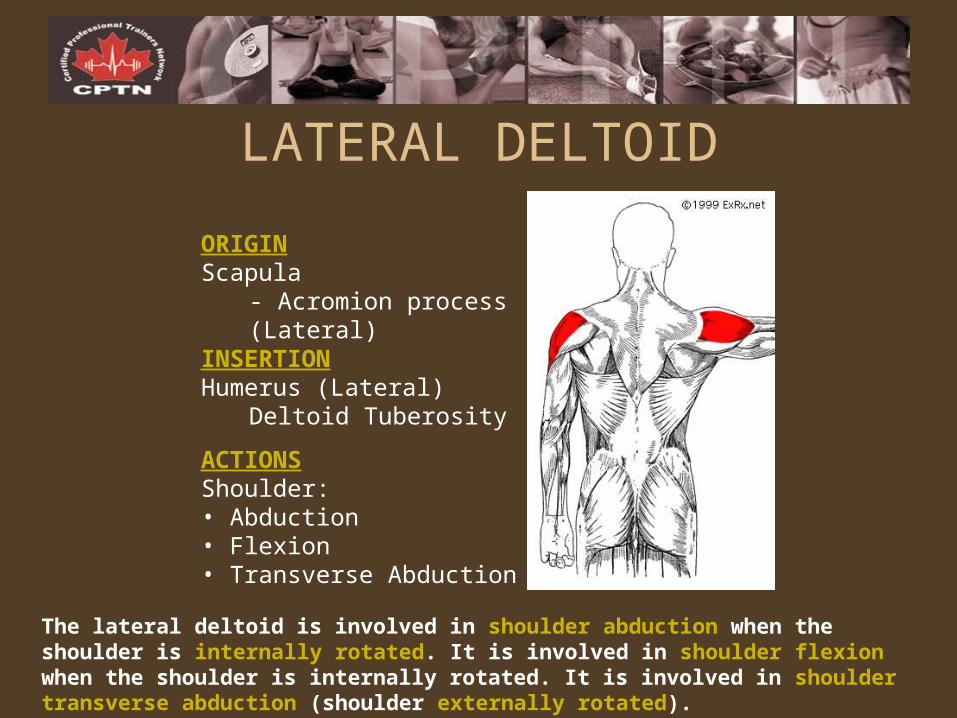
The lateral deltoid is involved in shoulder abduction when the shoulder is internally rotated. It is involved in shoulder flexion when the shoulder is internally rotated. It is involved in shoulder transverse abduction (shoulder externally rotated).
ORIGINScapula
- Acromion process (Lateral)
INSERTIONHumerus (Lateral)
Deltoid Tuberosity
ACTIONSShoulder:• Abduction • Flexion • Transverse Abduction
LATERAL DELTOID
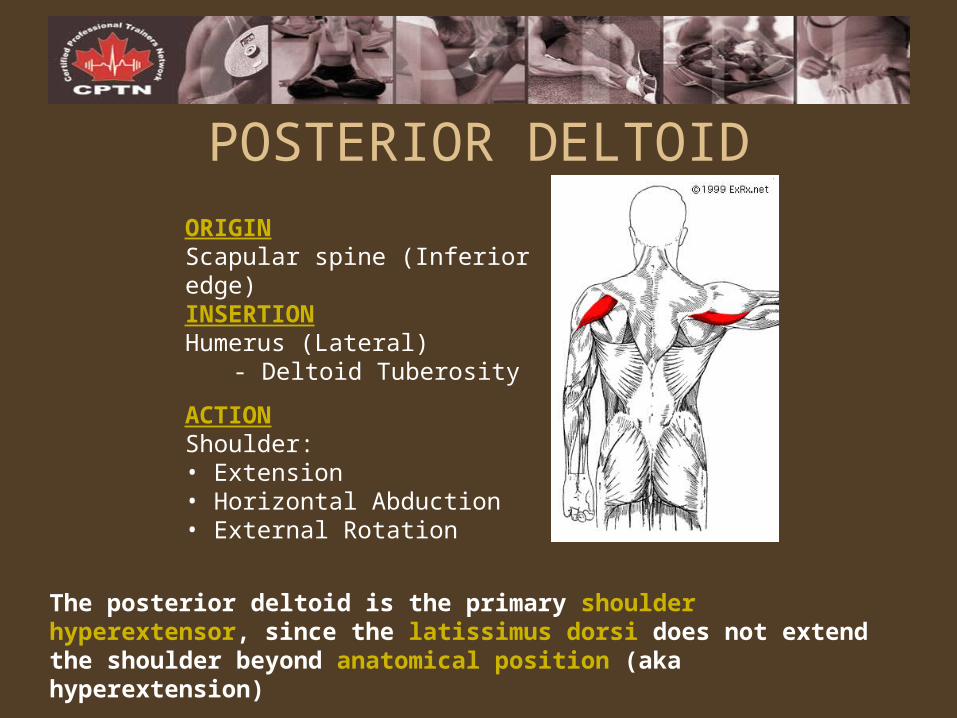
The posterior deltoid is the primary shoulder hyperextensor, since the latissimus dorsi does not extend the shoulder beyond anatomical position (aka hyperextension)
ORIGINScapular spine (Inferior edge) INSERTIONHumerus (Lateral)
- Deltoid Tuberosity
ACTIONShoulder:• Extension • Horizontal Abduction • External Rotation
POSTERIOR DELTOID
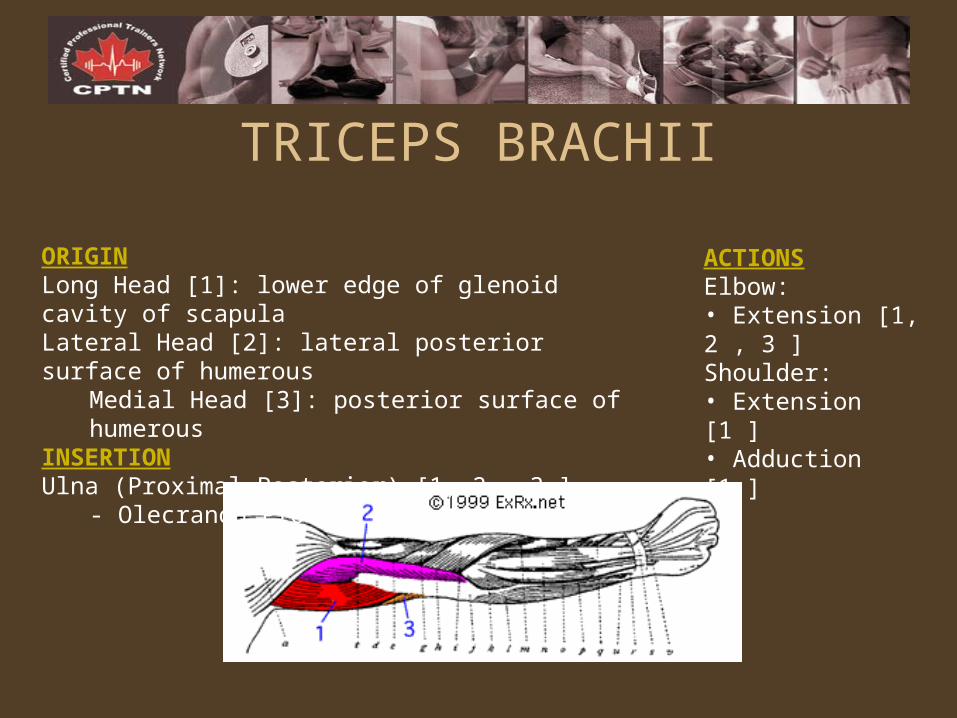
ORIGINLong Head [1]: lower edge of glenoid cavity of scapula Lateral Head [2]: lateral posterior surface of humerous
Medial Head [3]: posterior surface of humerous INSERTIONUlna (Proximal Posterior) [1, 2 , 3 ]
- Olecranon Process
TRICEPS BRACHII
ACTIONSElbow:• Extension [1, 2 , 3 ] Shoulder:• Extension [1 ] • Adduction [1 ]
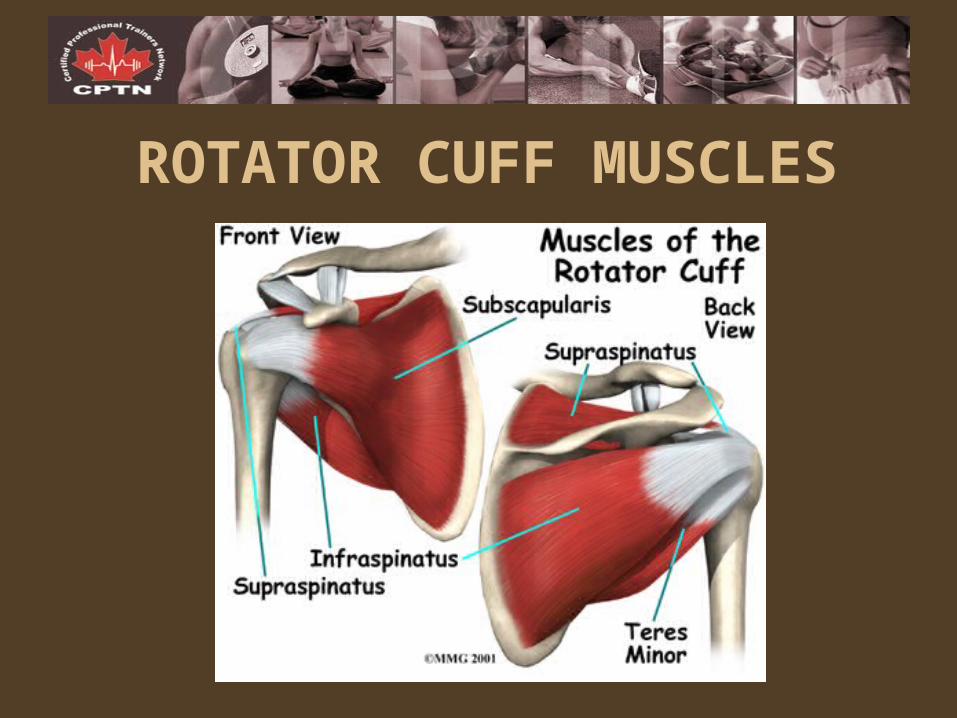
ROTATOR CUFF MUSCLES
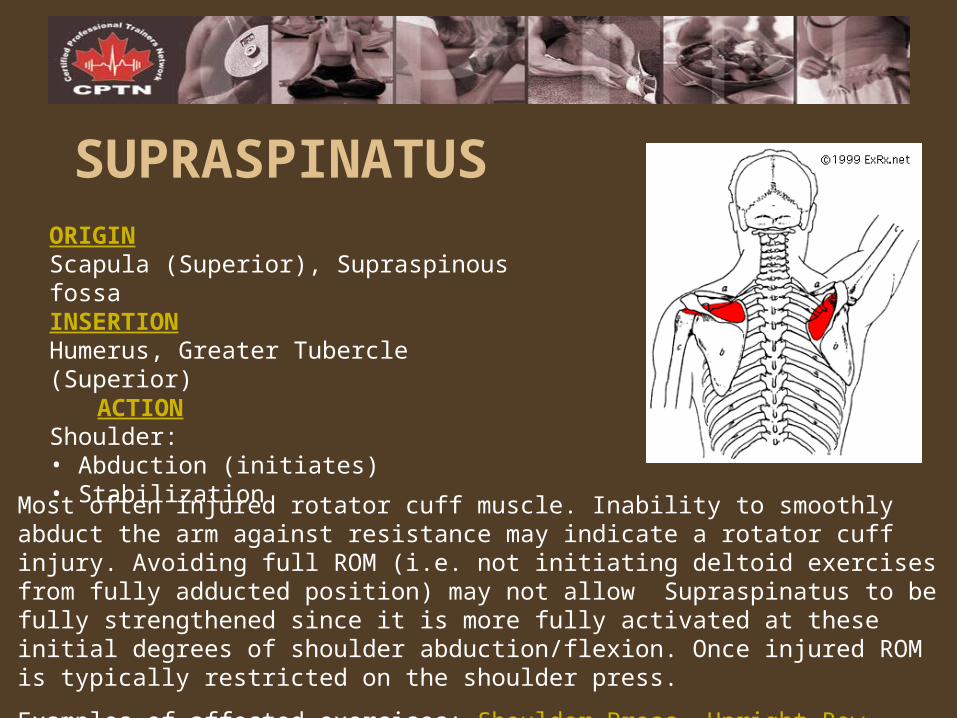
ORIGINScapula (Superior), Supraspinous fossa INSERTIONHumerus, Greater Tubercle (Superior)
ACTION Shoulder:• Abduction (initiates)• Stabilization
SUPRASPINATUS
Most often injured rotator cuff muscle. Inability to smoothly abduct the arm against resistance may indicate a rotator cuff injury. Avoiding full ROM (i.e. not initiating deltoid exercises from fully adducted position) may not allow Supraspinatus to be fully strengthened since it is more fully activated at these initial degrees of shoulder abduction/flexion. Once injured ROM is typically restricted on the shoulder press.
Examples of affected exercises: Shoulder Press, Upright Row, Lateral Raise Example preventative / corrective exercises: Front Lateral Raise, Lying Lateral Raise
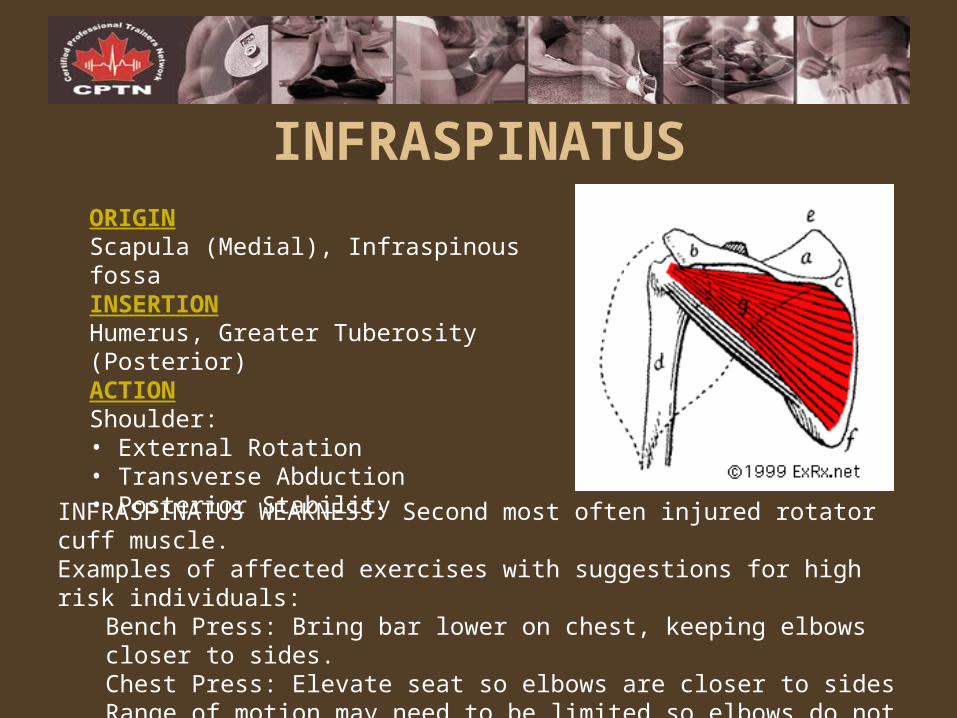
ORIGINScapula (Medial), Infraspinous fossa INSERTIONHumerus, Greater Tuberosity (Posterior)ACTIONShoulder:• External Rotation • Transverse Abduction • Posterior Stability
INFRASPINATUS
INFRASPINATUS WEAKNESS: Second most often injured rotator cuff muscle. Examples of affected exercises with suggestions for high risk individuals:
Bench Press: Bring bar lower on chest, keeping elbows closer to sides. Chest Press: Elevate seat so elbows are closer to sides Range of motion may need to be limited so elbows do not go behind shoulders
Example preventative / corrective exercises: Lying External Rotation, Rows
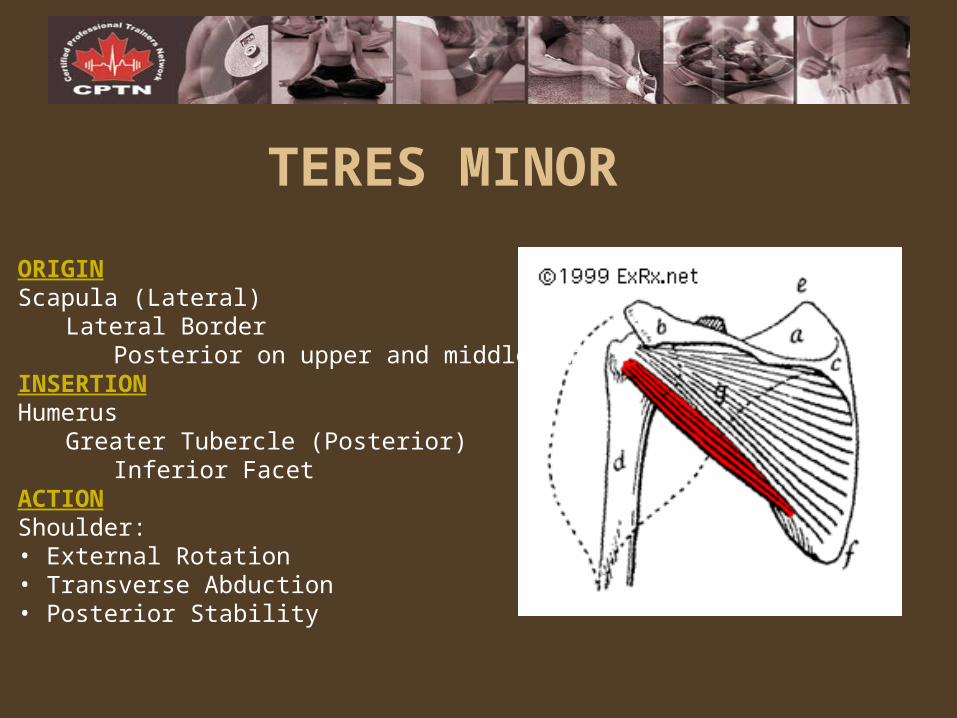
TERES MINOR
ORIGINScapula (Lateral)
Lateral Border Posterior on upper and middle part
INSERTIONHumerus
Greater Tubercle (Posterior) Inferior Facet
ACTIONShoulder:• External Rotation • Transverse Abduction• Posterior Stability
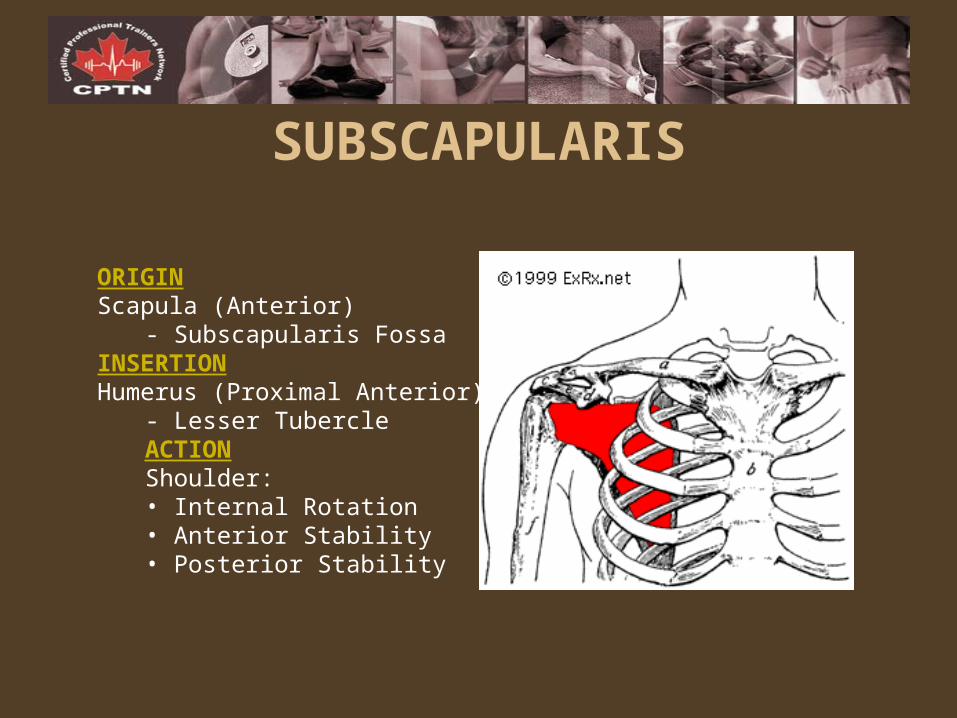
ORIGINScapula (Anterior)
- Subscapularis Fossa INSERTIONHumerus (Proximal Anterior)
- Lesser TubercleACTIONShoulder:• Internal Rotation • Anterior Stability • Posterior Stability
SUBSCAPULARIS
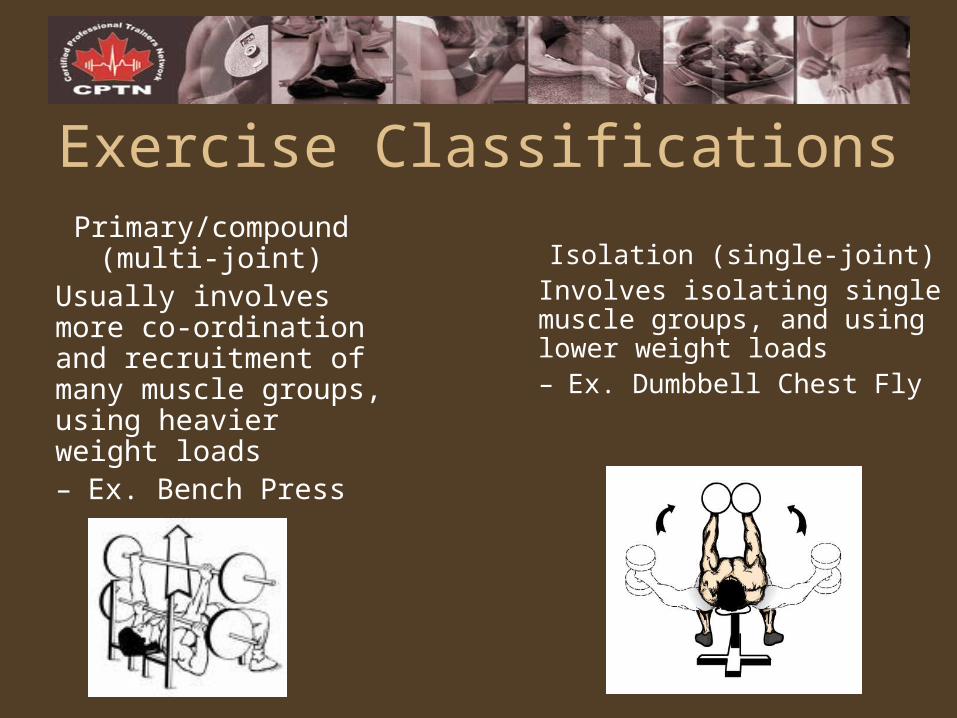
Exercise ClassificationsPrimary/compound
(multi-joint)Usually involves more co-ordination and recruitment of many muscle groups, using heavier weight loads– Ex. Bench Press
Isolation (single-joint)Involves isolating single muscle groups, and using lower weight loads– Ex. Dumbbell Chest Fly
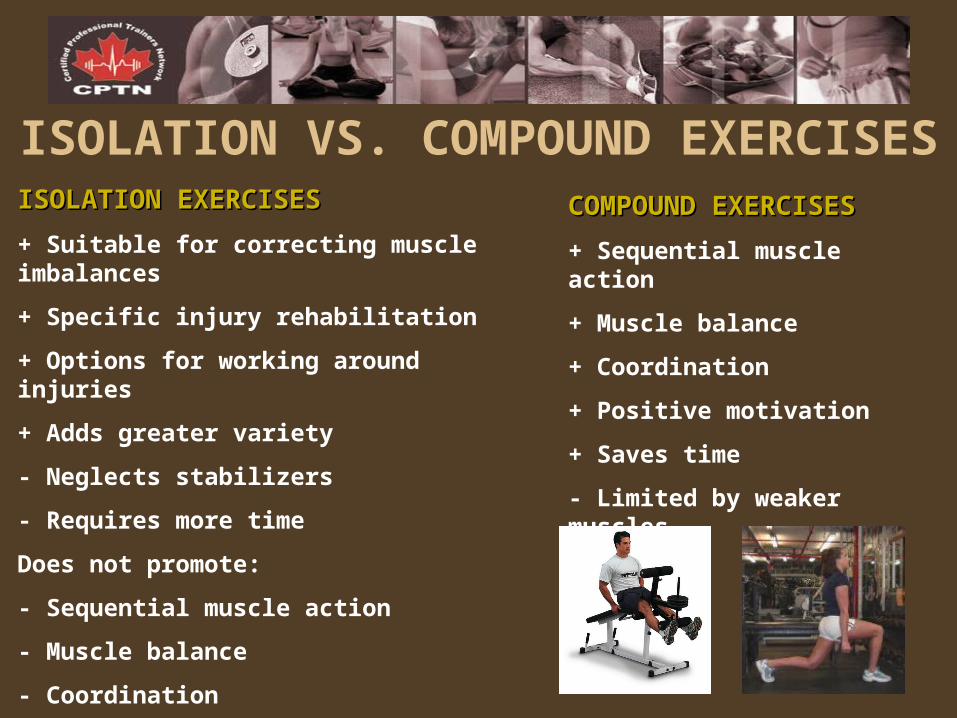
ISOLATION VS. COMPOUND EXERCISESCOMPOUND EXERCISESCOMPOUND EXERCISES
+ Sequential muscle action
+ Muscle balance
+ Coordination
+ Positive motivation
+ Saves time
- Limited by weaker muscles
ISOLATION EXERCISESISOLATION EXERCISES
+ Suitable for correcting muscle imbalances
+ Specific injury rehabilitation
+ Options for working around injuries
+ Adds greater variety
- Neglects stabilizers
- Requires more time
Does not promote:
- Sequential muscle action
- Muscle balance
- Coordination
- Positive motivation
Exercise Sequence• Exercises spaced throughout program so as to rest one
area while working another
• Compound exercises precede isolation exercises requiring the same muscle
• Exercises requiring larger muscles precede exercises requiring smaller muscles
• Exercises requiring muscles closer to the mid-line precede exercises requiring muscles further from the midline
• Exercises requiring less developed muscles precede exercises requiring more developed muscles
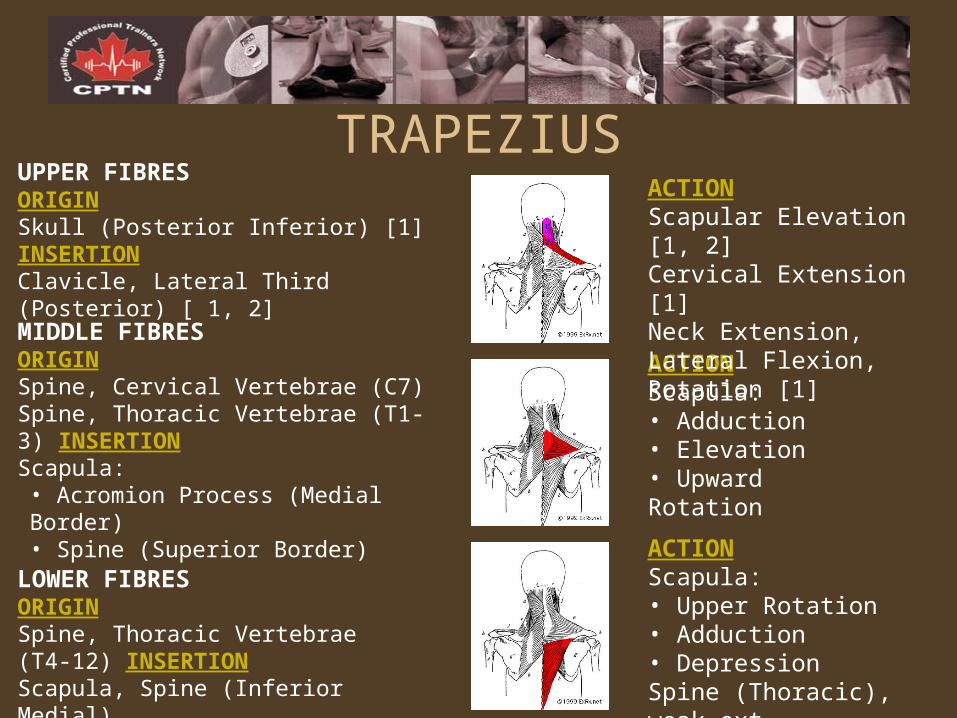
LOWER FIBRESORIGINSpine, Thoracic Vertebrae (T4-12) INSERTIONScapula, Spine (Inferior Medial)
MIDDLE FIBRESORIGINSpine, Cervical Vertebrae (C7) Spine, Thoracic Vertebrae (T1-3) INSERTIONScapula:• Acromion Process (Medial Border) • Spine (Superior Border)
ACTIONScapula:• Upper Rotation • Adduction • Depression Spine (Thoracic), weak ext.
TRAPEZIUS
ACTIONScapula:• Adduction • Elevation • Upward Rotation
UPPER FIBRESORIGINSkull (Posterior Inferior) [1]INSERTIONClavicle, Lateral Third (Posterior) [ 1, 2]
ACTIONScapular Elevation [1, 2] Cervical Extension [1] Neck Extension, Lateral Flexion, Rotation [1]
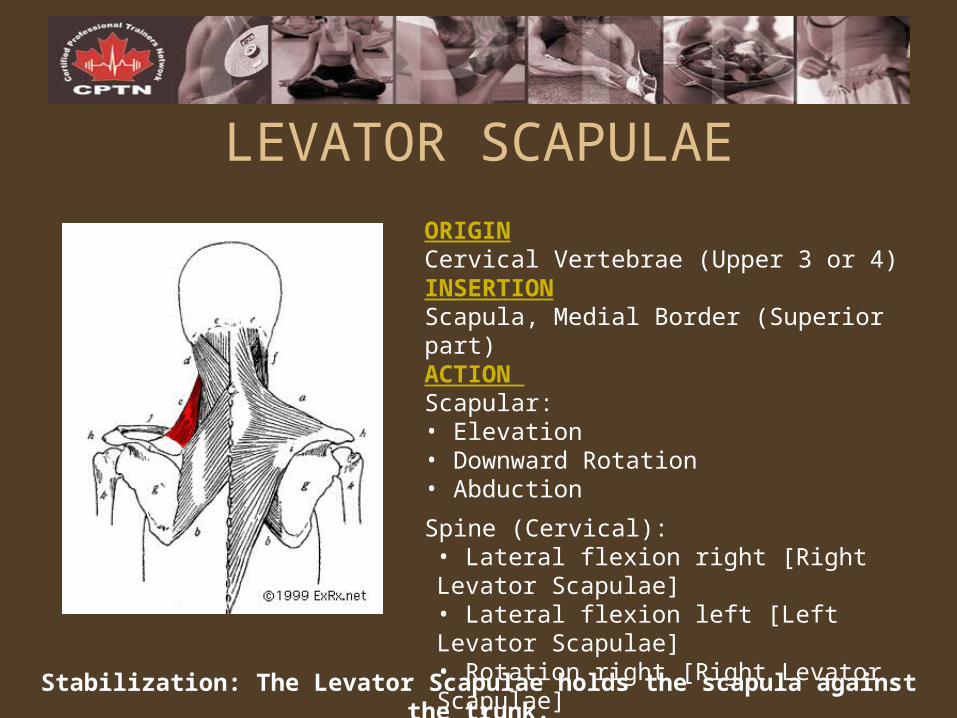
ORIGINCervical Vertebrae (Upper 3 or 4) INSERTIONScapula, Medial Border (Superior part) ACTION Scapular:• Elevation • Downward Rotation • Abduction
Spine (Cervical):• Lateral flexion right [Right Levator Scapulae] • Lateral flexion left [Left Levator Scapulae] • Rotation right [Right Levator Scapulae] • Rotation left [Left Levator Scapulae]
LEVATOR SCAPULAE
Stabilization: The Levator Scapulae holds the scapula against the trunk.
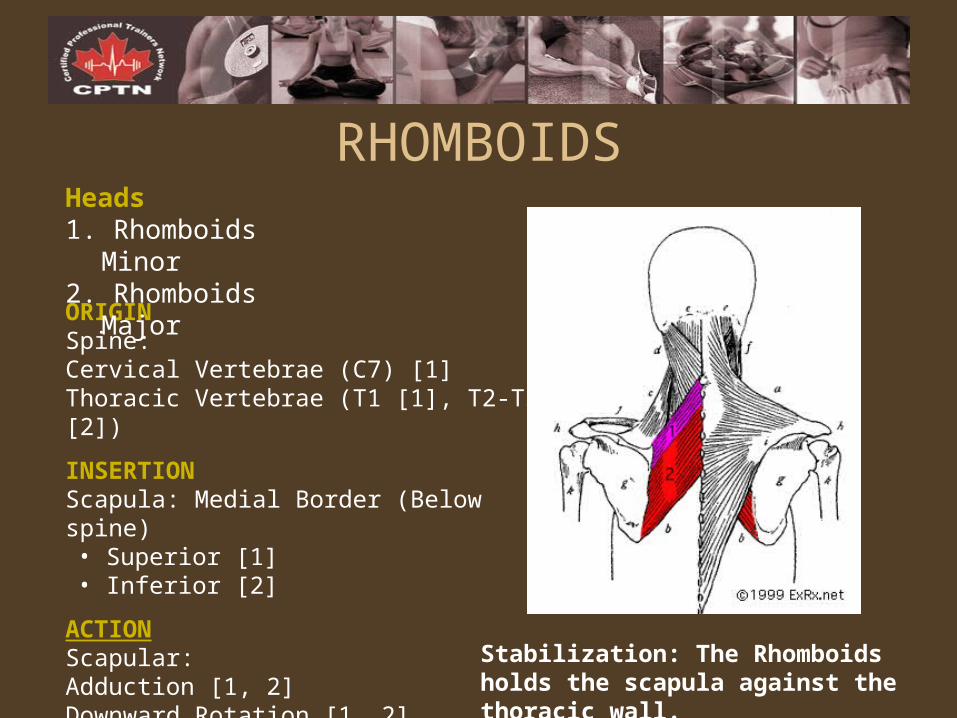
ORIGINSpine:Cervical Vertebrae (C7) [1] Thoracic Vertebrae (T1 [1], T2-T5 [2])
INSERTIONScapula: Medial Border (Below spine) • Superior [1] • Inferior [2]
ACTIONScapular:Adduction [1, 2] Downward Rotation [1, 2]
RHOMBOIDSHeads1. Rhomboids Minor 2. Rhomboids Major
Stabilization: The Rhomboids holds the scapula against the thoracic wall.
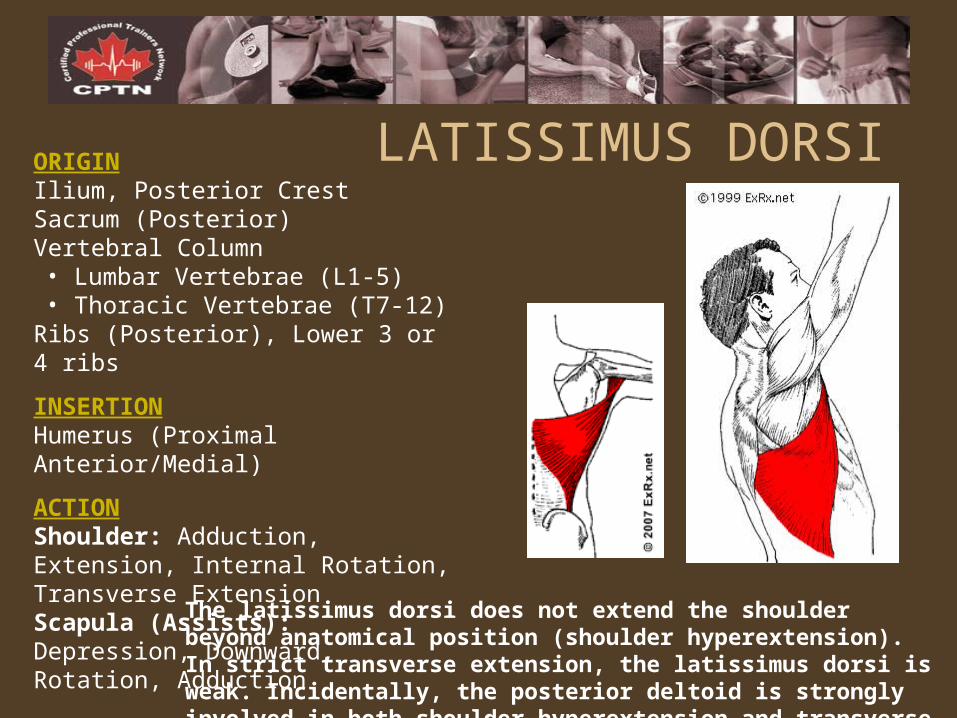
ORIGINIlium, Posterior Crest Sacrum (Posterior) Vertebral Column• Lumbar Vertebrae (L1-5) • Thoracic Vertebrae (T7-12)
Ribs (Posterior), Lower 3 or 4 ribs
INSERTIONHumerus (Proximal Anterior/Medial)
ACTIONShoulder: Adduction, Extension, Internal Rotation, Transverse Extension Scapula (Assists): Depression, Downward, Rotation, Adduction
LATISSIMUS DORSI
The latissimus dorsi does not extend the shoulder beyond anatomical position (shoulder hyperextension). In strict transverse extension, the latissimus dorsi is weak. Incidentally, the posterior deltoid is strongly involved in both shoulder hyperextension and transverse extension.
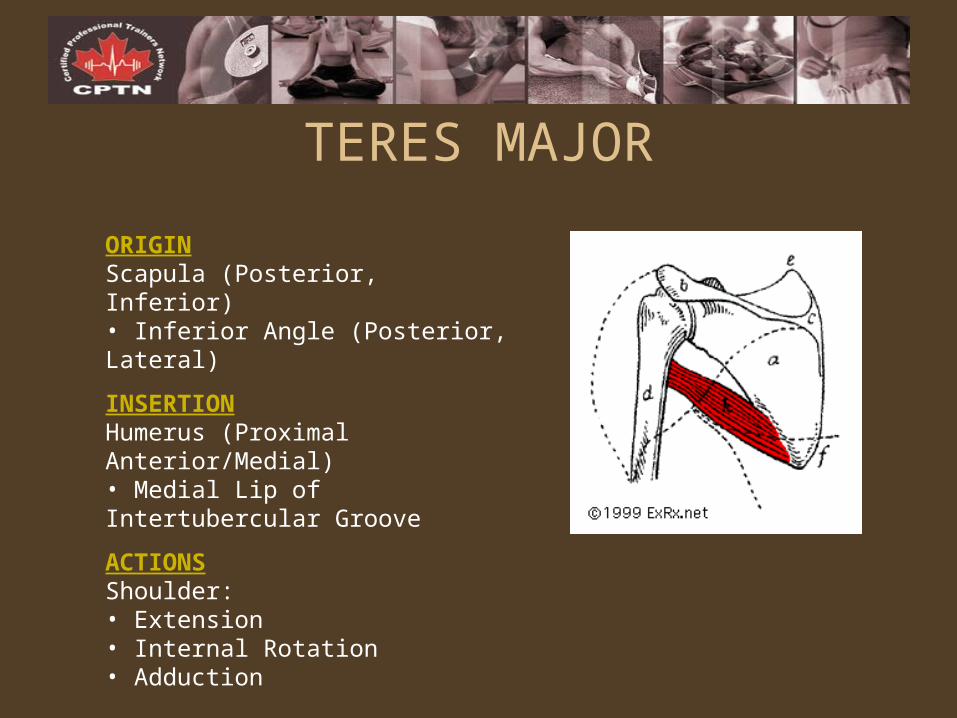
ORIGINScapula (Posterior, Inferior) • Inferior Angle (Posterior, Lateral)
INSERTIONHumerus (Proximal Anterior/Medial) • Medial Lip of Intertubercular Groove
ACTIONSShoulder:• Extension • Internal Rotation • Adduction
TERES MAJOR
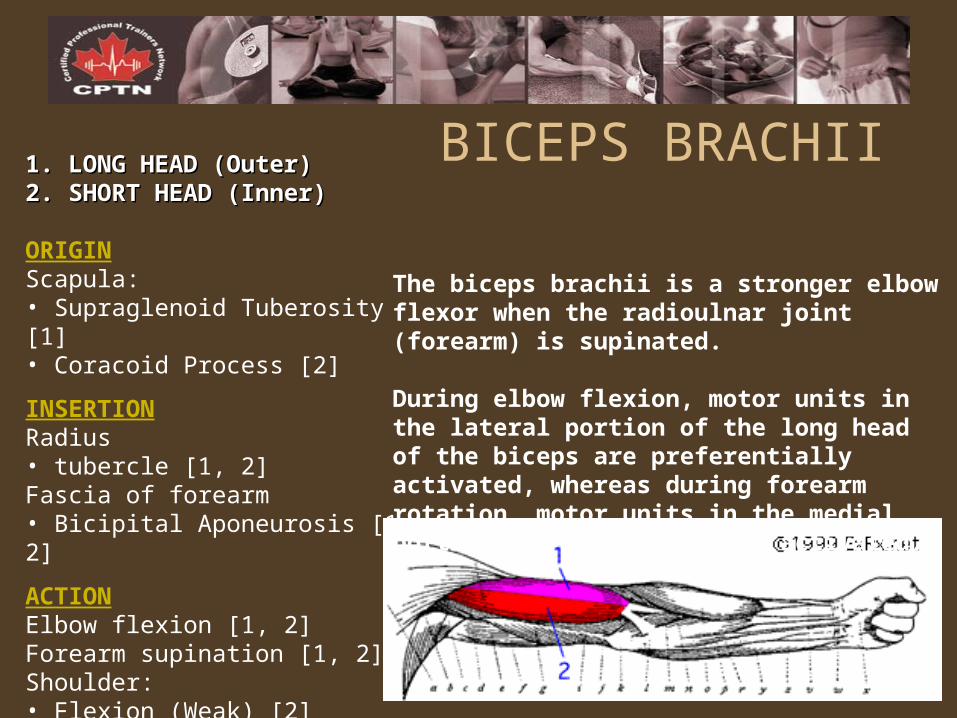
1. LONG HEAD (Outer) 1. LONG HEAD (Outer) 2. SHORT HEAD (Inner) 2. SHORT HEAD (Inner)
ORIGINScapula:• Supraglenoid Tuberosity [1] • Coracoid Process [2]
INSERTIONRadius• tubercle [1, 2] Fascia of forearm• Bicipital Aponeurosis [1, 2]
ACTIONElbow flexion [1, 2] Forearm supination [1, 2] Shoulder:• Flexion (Weak) [2] • Transverse Flexion (Weak) [2]
BICEPS BRACHII
The biceps brachii is a stronger elbow flexor when the radioulnar joint (forearm) is supinated.
During elbow flexion, motor units in the lateral portion of the long head of the biceps are preferentially activated, whereas during forearm rotation, motor units in the medial portion are preferentially activated.
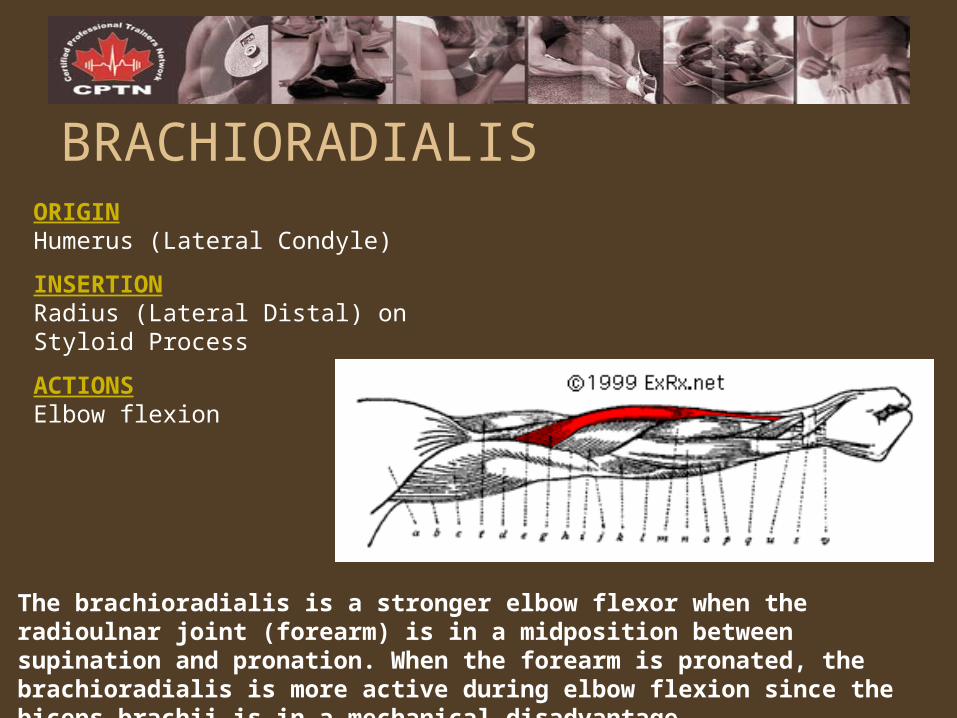
ORIGINHumerus (Lateral Condyle)
INSERTIONRadius (Lateral Distal) on Styloid Process
ACTIONSElbow flexion
BRACHIORADIALIS
The brachioradialis is a stronger elbow flexor when the radioulnar joint (forearm) is in a midposition between supination and pronation. When the forearm is pronated, the brachioradialis is more active during elbow flexion since the biceps brachii is in a mechanical disadvantage.
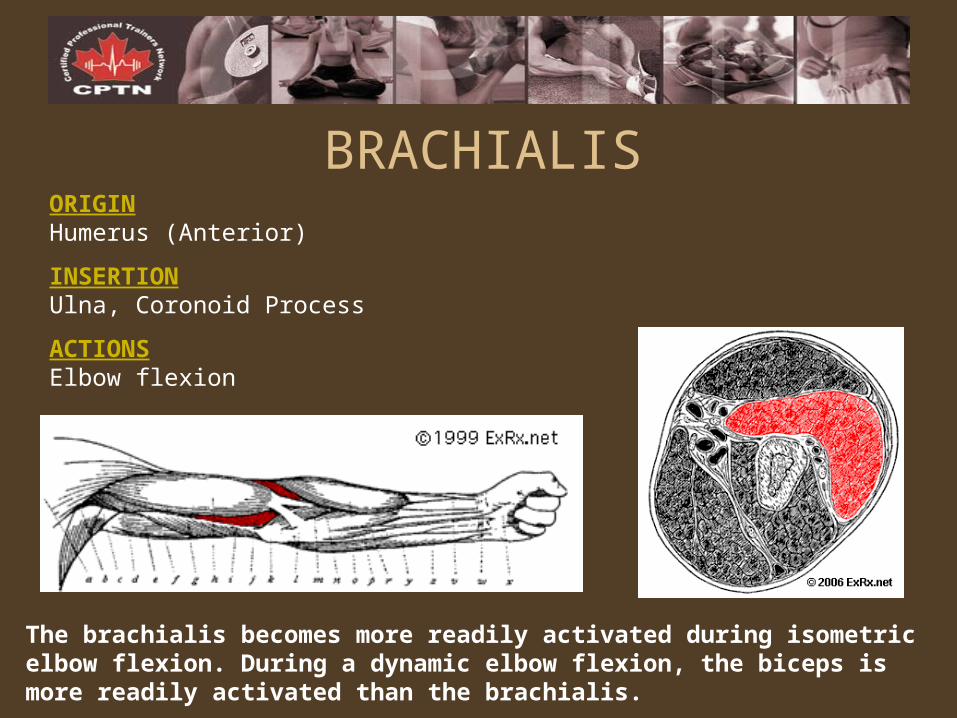
BRACHIALISORIGINHumerus (Anterior)
INSERTIONUlna, Coronoid Process
ACTIONSElbow flexion
The brachialis becomes more readily activated during isometric elbow flexion. During a dynamic elbow flexion, the biceps is more readily activated than the brachialis.
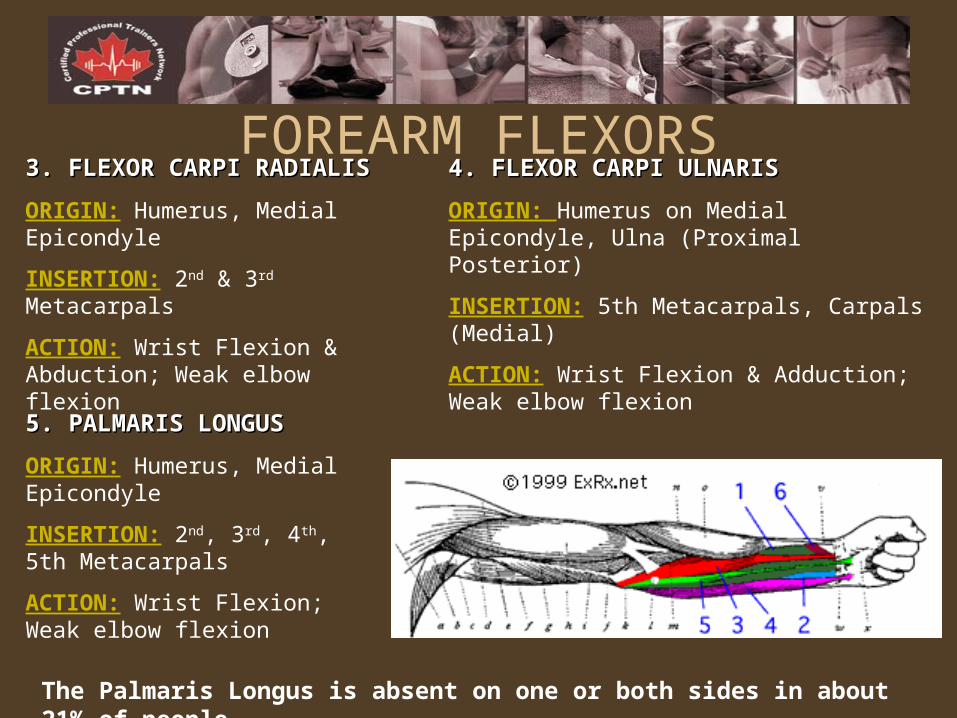
FOREARM FLEXORS3. FLEXOR CARPI RADIALIS3. FLEXOR CARPI RADIALIS
ORIGIN: Humerus, Medial Epicondyle
INSERTION: 2nd & 3rd Metacarpals
ACTION: Wrist Flexion & Abduction; Weak elbow flexion
5. PALMARIS LONGUS5. PALMARIS LONGUS
ORIGIN: Humerus, Medial Epicondyle
INSERTION: 2nd, 3rd, 4th, 5th Metacarpals
ACTION: Wrist Flexion; Weak elbow flexion
4. FLEXOR CARPI ULNARIS4. FLEXOR CARPI ULNARIS
ORIGIN: Humerus on Medial Epicondyle, Ulna (Proximal Posterior)
INSERTION: 5th Metacarpals, Carpals (Medial)
ACTION: Wrist Flexion & Adduction; Weak elbow flexion
The Palmaris Longus is absent on one or both sides in about 21% of people.
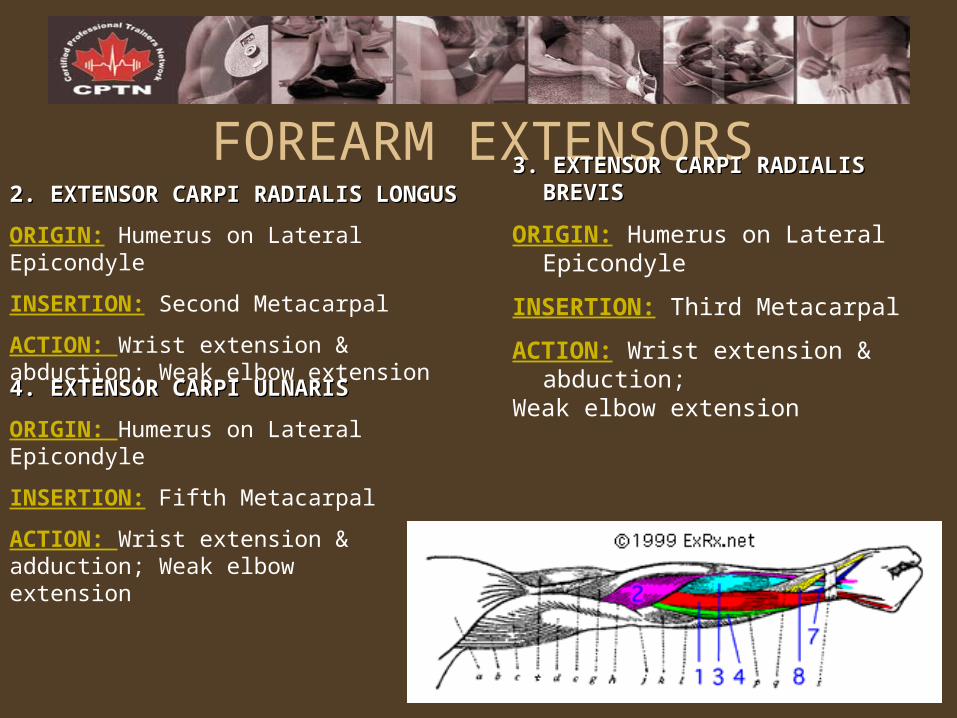
FOREARM EXTENSORS2. EXTENSOR CARPI RADIALIS LONGUS2. EXTENSOR CARPI RADIALIS LONGUS
ORIGIN: Humerus on Lateral Epicondyle
INSERTION: Second Metacarpal
ACTION: Wrist extension & abduction; Weak elbow extension
3. EXTENSOR CARPI RADIALIS BREVIS3. EXTENSOR CARPI RADIALIS BREVIS
ORIGIN: Humerus on Lateral Epicondyle
INSERTION: Third Metacarpal
ACTION: Wrist extension & abduction; Weak elbow extension
4. EXTENSOR CARPI ULNARIS4. EXTENSOR CARPI ULNARIS
ORIGIN: Humerus on Lateral Epicondyle
INSERTION: Fifth Metacarpal
ACTION: Wrist extension & adduction; Weak elbow extension
General Guidelines for Proper Technique
• Perform proper warm-up• Maintain a neutral spine• Avoid using momentum; Use controlled movements• Use full range of motion• Breath rhythmically (positive/concentric = exhale,
negative/eccentric = inhale)• Do not use too much or too little resistance• Train muscle groups proportionately in a balanced manner• Train larger muscle groups before smaller
Specific Strength Training Principles & Systems
• Muscle Confusion• Muscle Priority• Isolation• Flushing• Holistic• Split System• Pyramiding• Supersets
CASE STUDY PARTNER ASSIGNMENTCASE STUDY PARTNER ASSIGNMENT
Design one PRT program for your case study client in Appendix A utilizing 2 different principles/systems. Please indicate which principles/systems you chose and why.
PROGRAM DESIGN FOR FLEXIBILITY
LEARNING OBJECTIVESLEARNING OBJECTIVES
1. To differentiate between BALLISTIC, DYNAMIC, STATIC and PNF stretching and understand their different applications in program design.
2. To apply an understanding of flexibility training guidelines using the O.F.I.T.T. principle.
3. To understand the application of O.F.I.T.T. in the flexibility training continuum (improvement vs. maintenance vs. over-training vs. detraining)
4. To explore controversies in the application and benefits of stretching for flexibility and injury prevention.
TYPES OF STRETCHING
BALLISTIC, DYNAMIC, STATIC, PNFBALLISTIC, DYNAMIC, STATIC, PNF
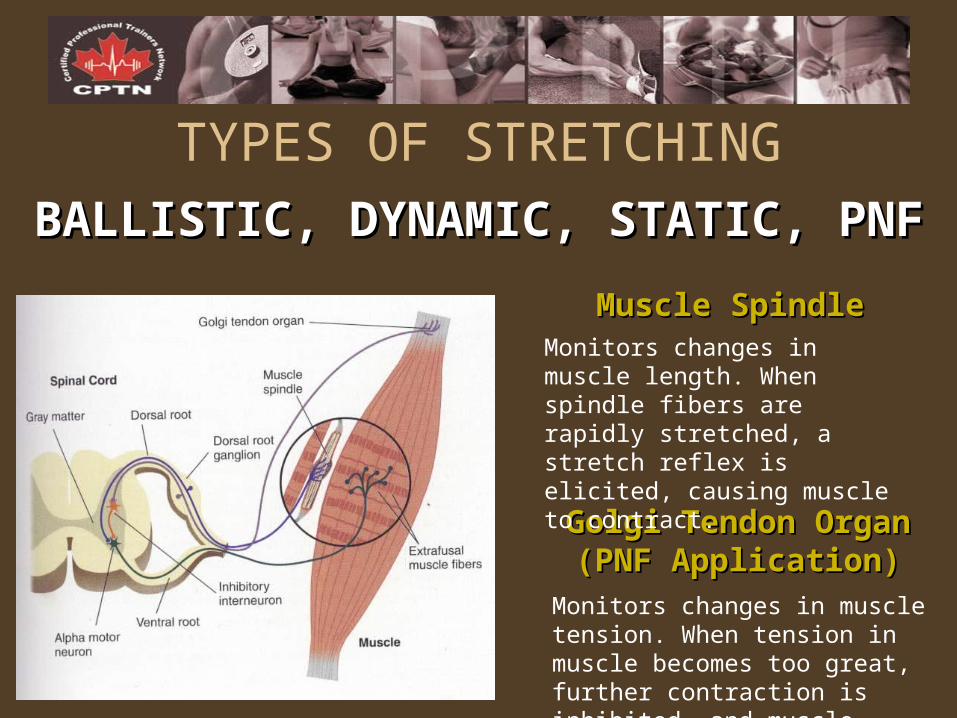
TYPES OF STRETCHING
BALLISTIC, DYNAMIC, STATIC, PNFBALLISTIC, DYNAMIC, STATIC, PNF
Golgi Tendon Organ Golgi Tendon Organ (PNF Application)(PNF Application)
Muscle SpindleMuscle SpindleMonitors changes in muscle length. When spindle fibers are rapidly stretched, a stretch reflex is elicited, causing muscle to contract.
Monitors changes in muscle tension. When tension in muscle becomes too great, further contraction is inhibited, and muscle relaxes.
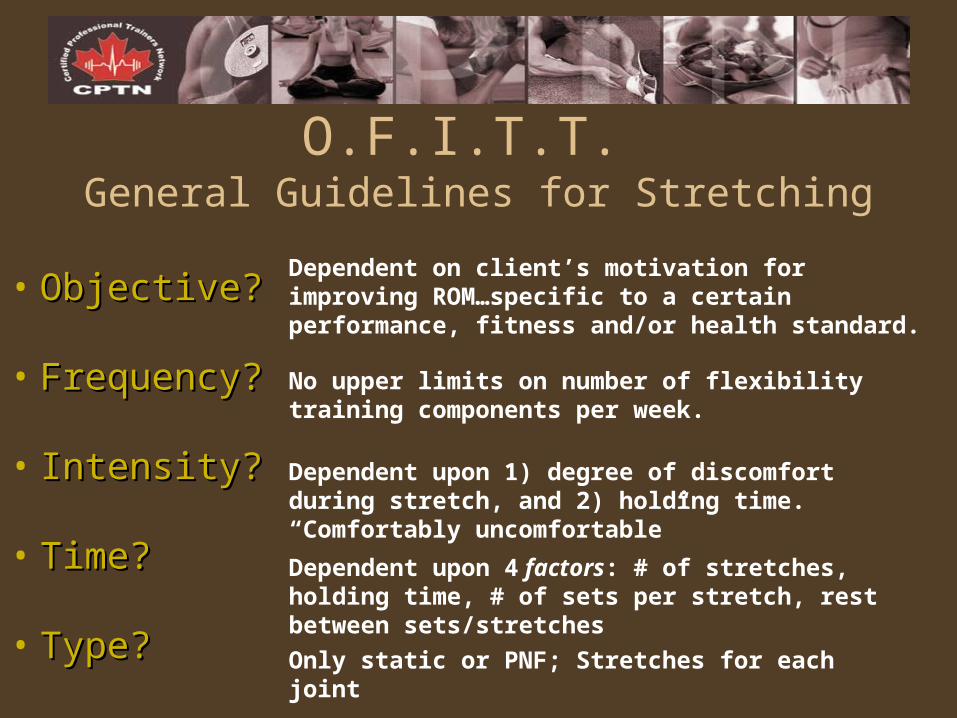
O.F.I.T.T. General Guidelines for Stretching
• Objective?Objective?
• Frequency?Frequency?
• Intensity?Intensity?
• Time?Time?
• Type?Type?
Dependent on client’s motivation for improving ROM…specific to a certain performance, fitness and/or health standard.
No upper limits on number of flexibility training components per week.
Dependent upon 1) degree of discomfort during stretch, and 2) holding time. “Comfortably uncomfortable”
Dependent upon 4 factors: # of stretches, holding time, # of sets per stretch, rest between sets/stretches
Only static or PNF; Stretches for each joint
ANATOMY (Lower Body) & PROGRAM DESIGN
LEARNING OBJECTIVESLEARNING OBJECTIVES
1. To know the origin, insertion and line of action for the muscles of the lower body including the GLUTES, ABDUCTORS, ADDUCTORS, QUADRICEPS, HAMSTRINGS, and CALVES.
2. To apply knowledge of anatomy to effective exercises and be able to distinguish between the agonists, antagonists, synergists and stabilizers.
3. To learn proper exercise and spotting technique and practice exercise instruction using the Seven Step Process.
4. To apply the Principles of Training and specific program design methods in the instruction and performance of mini exercise routines for different muscle groups.
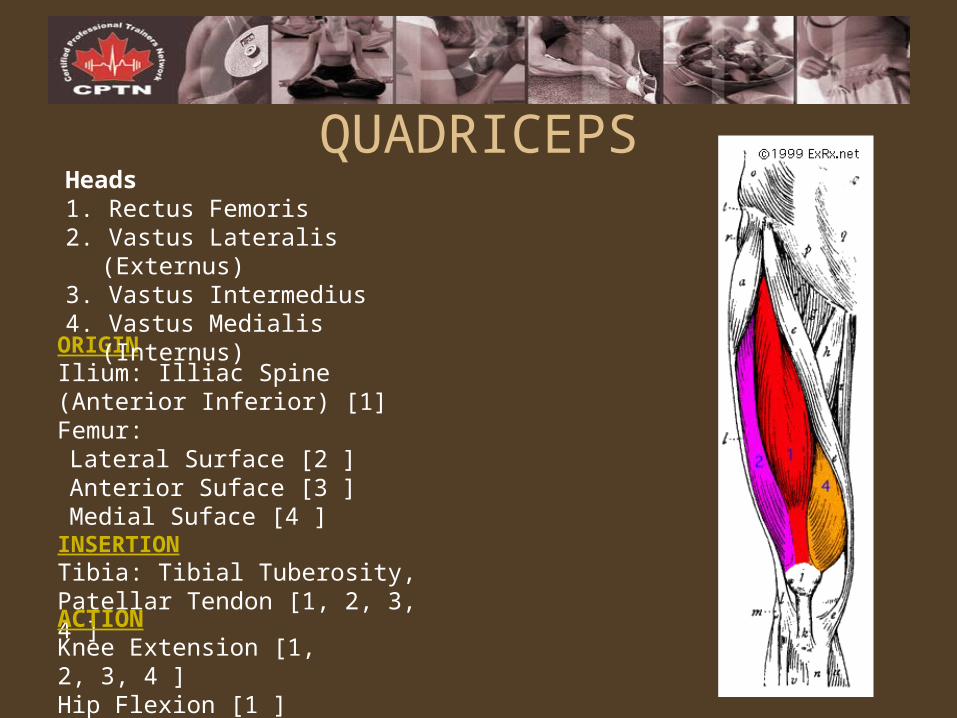
ORIGINIlium: Illiac Spine (Anterior Inferior) [1] Femur:Lateral Surface [2 ] Anterior Suface [3 ] Medial Suface [4 ]
INSERTIONTibia: Tibial Tuberosity, Patellar Tendon [1, 2, 3, 4 ]
ACTIONKnee Extension [1, 2, 3, 4 ] Hip Flexion [1 ]
QUADRICEPSHeads1. Rectus Femoris 2. Vastus Lateralis (Externus) 3. Vastus Intermedius 4. Vastus Medialis (Internus)
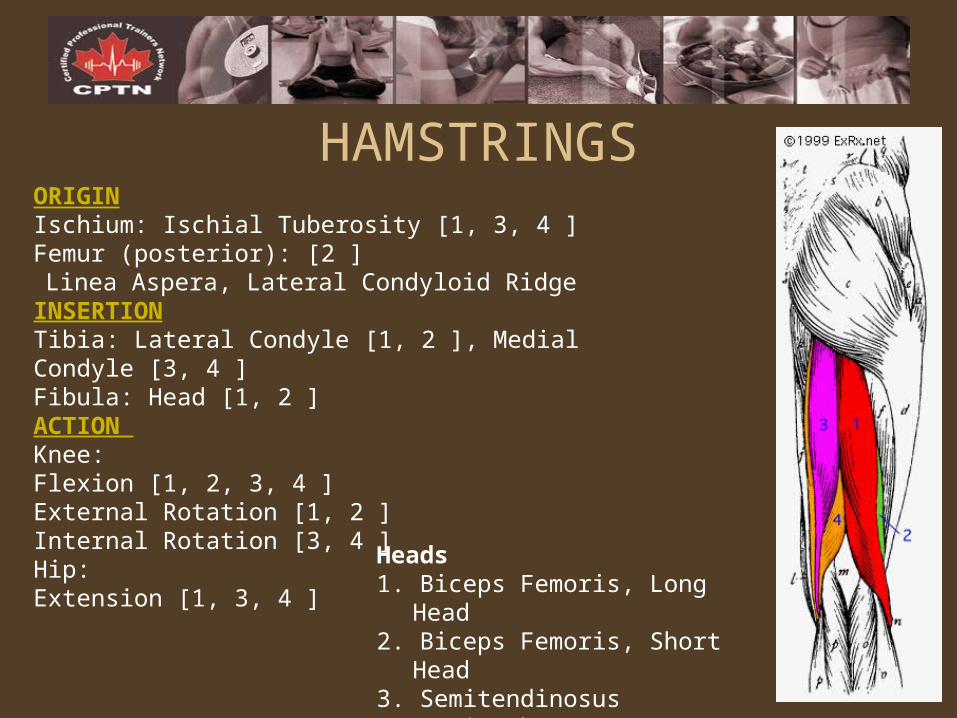
ORIGINIschium: Ischial Tuberosity [1, 3, 4 ] Femur (posterior): [2 ] Linea Aspera, Lateral Condyloid Ridge
INSERTIONTibia: Lateral Condyle [1, 2 ], Medial Condyle [3, 4 ] Fibula: Head [1, 2 ] ACTION Knee:Flexion [1, 2, 3, 4 ] External Rotation [1, 2 ] Internal Rotation [3, 4 ]Hip:Extension [1, 3, 4 ]
HAMSTRINGS
Heads1. Biceps Femoris, Long Head 2. Biceps Femoris, Short Head 3. Semitendinosus 4. Semimembranosus
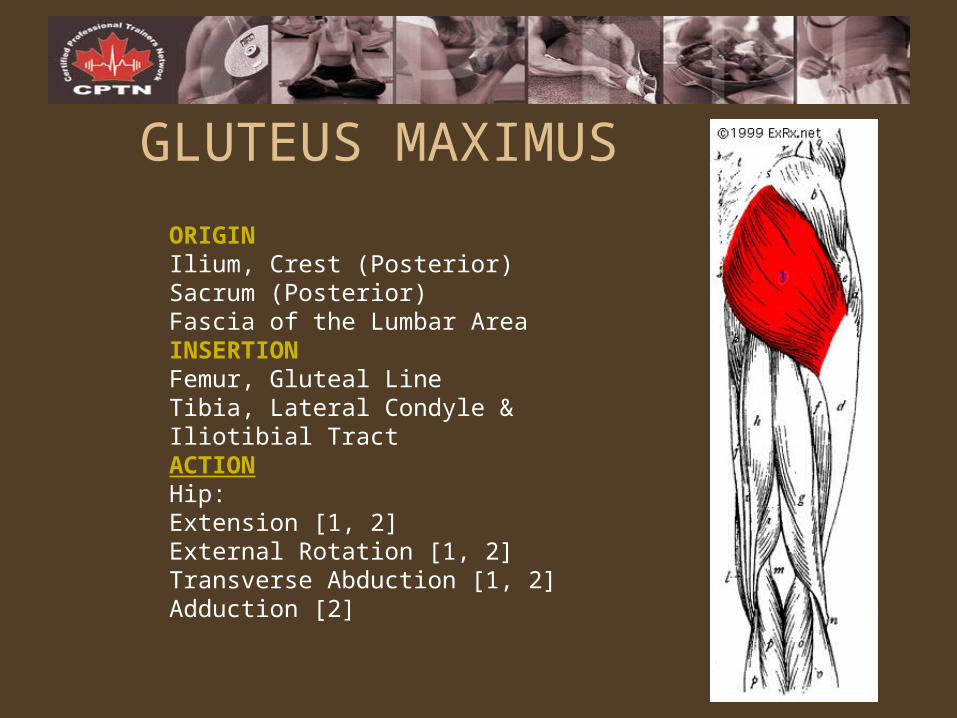
ORIGINIlium, Crest (Posterior) Sacrum (Posterior)Fascia of the Lumbar AreaINSERTIONFemur, Gluteal LineTibia, Lateral Condyle & Iliotibial TractACTIONHip:Extension [1, 2] External Rotation [1, 2] Transverse Abduction [1, 2] Adduction [2]
GLUTEUS MAXIMUS
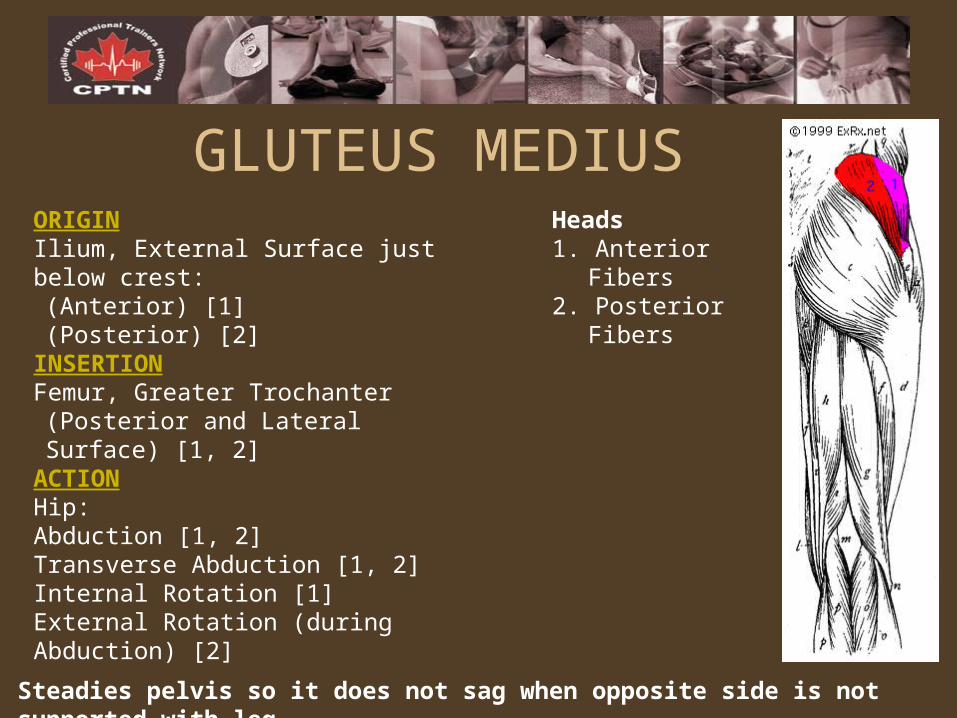
ORIGINIlium, External Surface just below crest:(Anterior) [1] (Posterior) [2]
INSERTIONFemur, Greater Trochanter(Posterior and Lateral Surface) [1, 2]
ACTIONHip:Abduction [1, 2] Transverse Abduction [1, 2] Internal Rotation [1] External Rotation (during Abduction) [2]
Steadies pelvis so it does not sag when opposite side is not supported with leg.
GLUTEUS MEDIUSHeads1. Anterior Fibers 2. Posterior Fibers
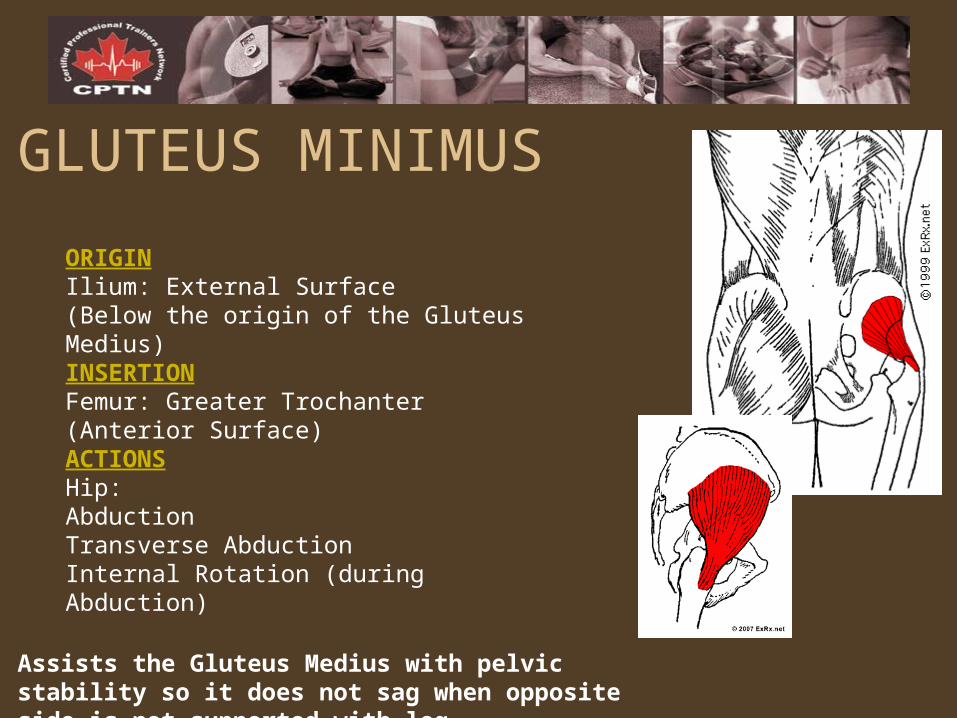
ORIGINIlium: External Surface (Below the origin of the Gluteus Medius)INSERTIONFemur: Greater Trochanter (Anterior Surface)ACTIONSHip:Abduction Transverse Abduction Internal Rotation (during Abduction)
GLUTEUS MINIMUS
Assists the Gluteus Medius with pelvic stability so it does not sag when opposite side is not supported with leg.
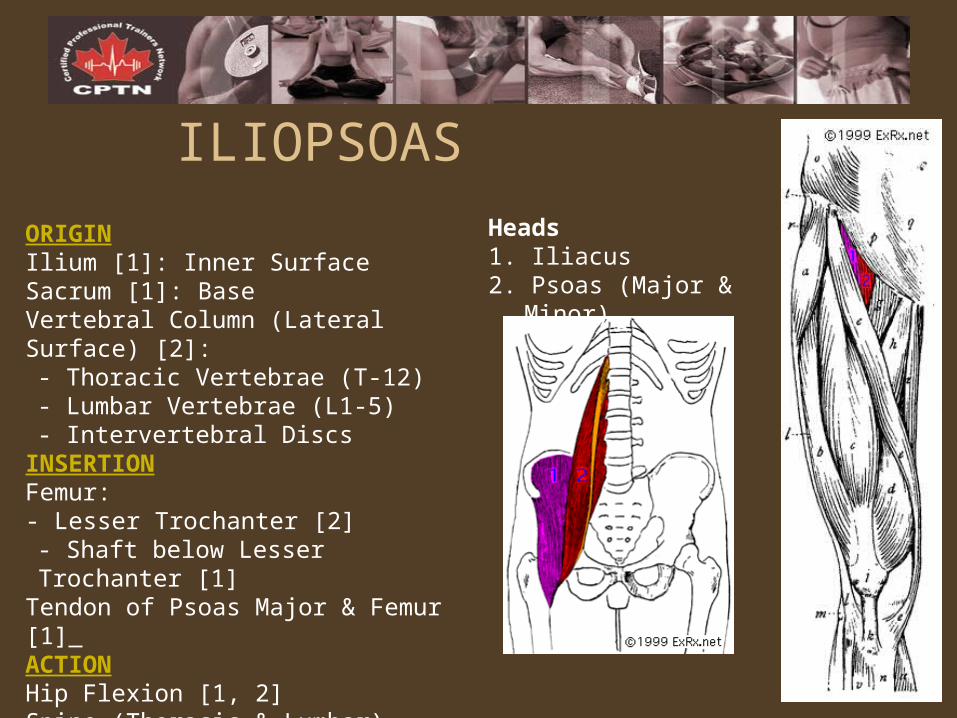
ORIGINIlium [1]: Inner Surface Sacrum [1]: Base Vertebral Column (Lateral Surface) [2]:- Thoracic Vertebrae (T-12) - Lumbar Vertebrae (L1-5) - Intervertebral Discs
INSERTIONFemur: - Lesser Trochanter [2] - Shaft below Lesser Trochanter [1]
Tendon of Psoas Major & Femur [1] ACTIONHip Flexion [1, 2] Spine (Thoracic & Lumbar) Rotation [2]
ILIOPSOASHeads1. Iliacus 2. Psoas (Major & Minor)
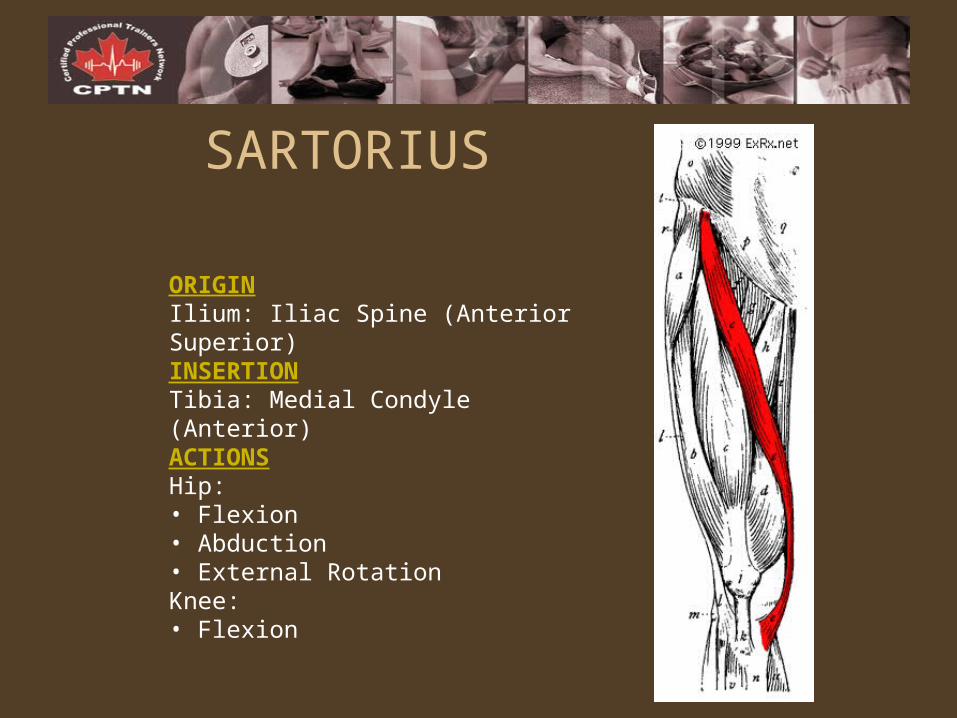
ORIGINIlium: Iliac Spine (Anterior Superior) INSERTIONTibia: Medial Condyle (Anterior) ACTIONSHip:• Flexion • Abduction • External Rotation Knee:• Flexion
SARTORIUS
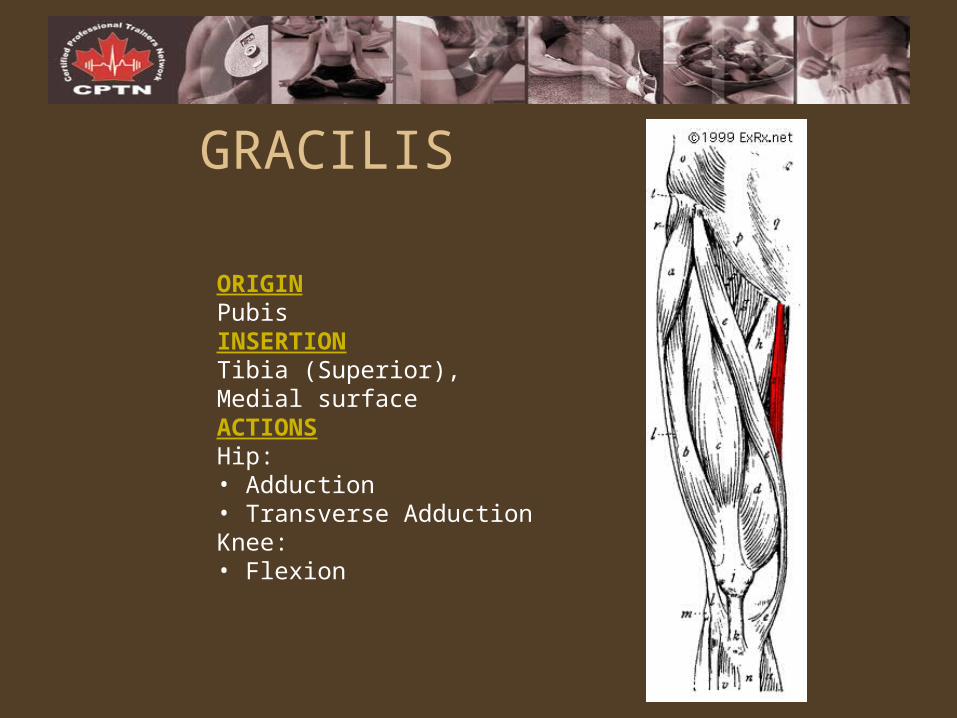
GRACILIS
ORIGINPubisINSERTIONTibia (Superior), Medial surface ACTIONSHip:• Adduction • Transverse Adduction Knee:• Flexion
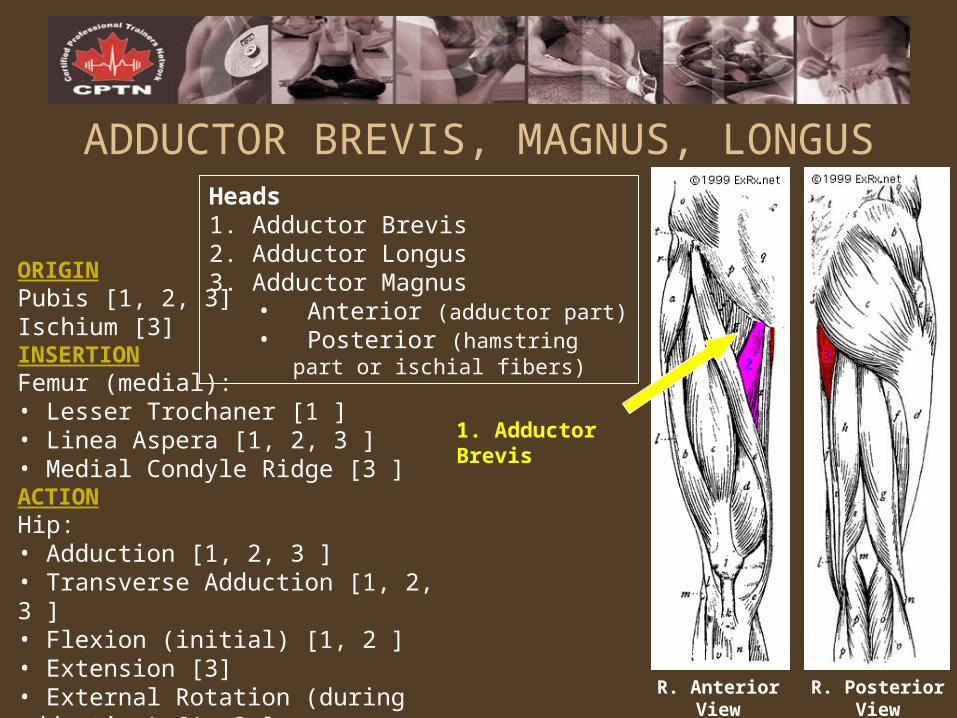
ADDUCTOR BREVIS, MAGNUS, LONGUS
ORIGINPubis [1, 2, 3] Ischium [3] INSERTIONFemur (medial):• Lesser Trochaner [1 ] • Linea Aspera [1, 2, 3 ] • Medial Condyle Ridge [3 ] ACTIONHip:• Adduction [1, 2, 3 ] • Transverse Adduction [1, 2, 3 ] • Flexion (initial) [1, 2 ] • Extension [3] • External Rotation (during adduction) [1, 3 ]
Heads1. Adductor Brevis 2. Adductor Longus 3. Adductor Magnus
• Anterior (adductor part) • Posterior (hamstring part or
ischial fibers)
1. Adductor Brevis
R. Posterior ViewR. Anterior View
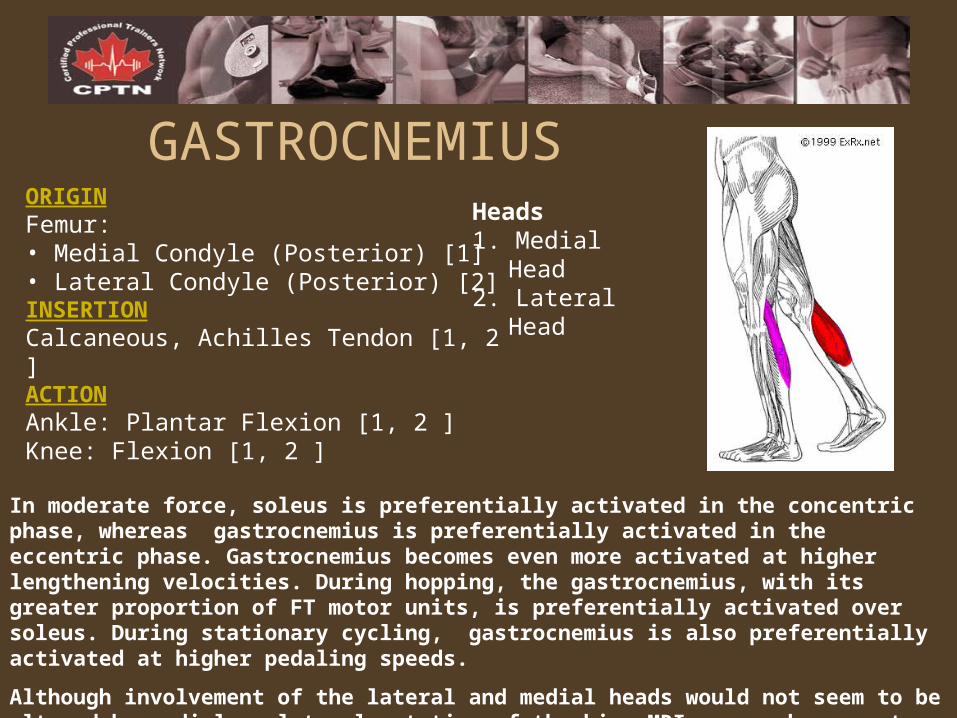
GASTROCNEMIUSORIGINFemur:• Medial Condyle (Posterior) [1] • Lateral Condyle (Posterior) [2] INSERTIONCalcaneous, Achilles Tendon [1, 2 ] ACTIONAnkle: Plantar Flexion [1, 2 ] Knee: Flexion [1, 2 ]
Heads1. Medial Head 2. Lateral Head
In moderate force, soleus is preferentially activated in the concentric phase, whereas gastrocnemius is preferentially activated in the eccentric phase. Gastrocnemius becomes even more activated at higher lengthening velocities. During hopping, the gastrocnemius, with its greater proportion of FT motor units, is preferentially activated over soleus. During stationary cycling, gastrocnemius is also preferentially activated at higher pedaling speeds.
Although involvement of the lateral and medial heads would not seem to be altered by medial or lateral rotation of the hip, MRI research suggests "toes in" activates both heads and "toes out" activates medial head to a higher degree.
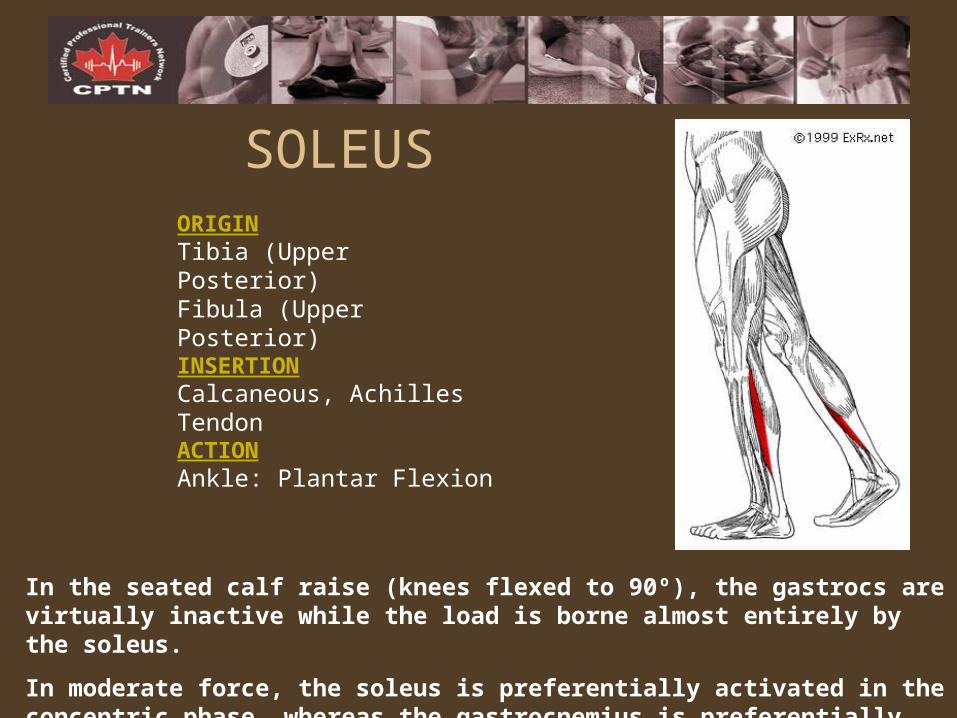
SOLEUS
ORIGINTibia (Upper Posterior) Fibula (Upper Posterior) INSERTIONCalcaneous, Achilles TendonACTIONAnkle: Plantar Flexion
In the seated calf raise (knees flexed to 90º), the gastrocs are virtually inactive while the load is borne almost entirely by the soleus.
In moderate force, the soleus is preferentially activated in the concentric phase, whereas the gastrocnemius is preferentially activated in the eccentric phase
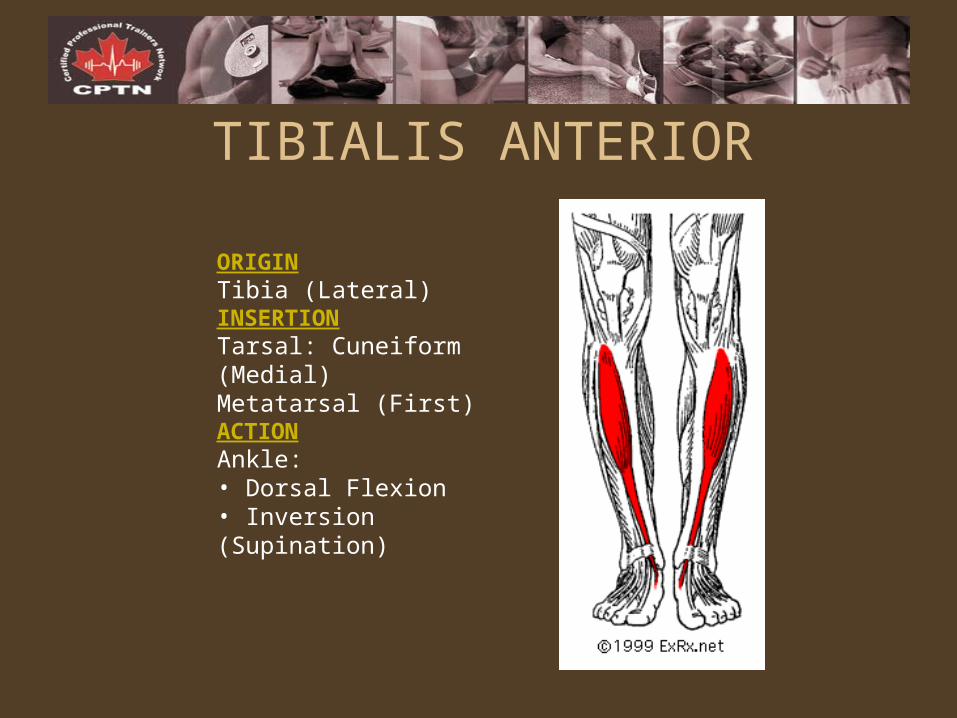
TIBIALIS ANTERIOR
ORIGINTibia (Lateral) INSERTIONTarsal: Cuneiform (Medial) Metatarsal (First) ACTIONAnkle:• Dorsal Flexion • Inversion (Supination)
BIOMECHANICS & PRINCIPLES OF MOVEMENT
LEARNING OBJECTIVESLEARNING OBJECTIVES
1. To understand the application of Newton’s laws of motion (i.e. inertia, acceleration, reaction) in exercise performance.
2. To understand force production relative to muscle length and position of muscle attachment.
3. To understand the factors which influence efficiency of movement.
4. To understand lever lengths relative to rotation and force production.
The Essentials of Biomechanical Concepts
• Motion AnalysisMotion Analysis (movement pattern/muscle sequence, forces, lever arms, acceleration)
• Force Force (magnitude, direction, internal, external)
• TorqueTorque• LeversLevers• StabilityStability
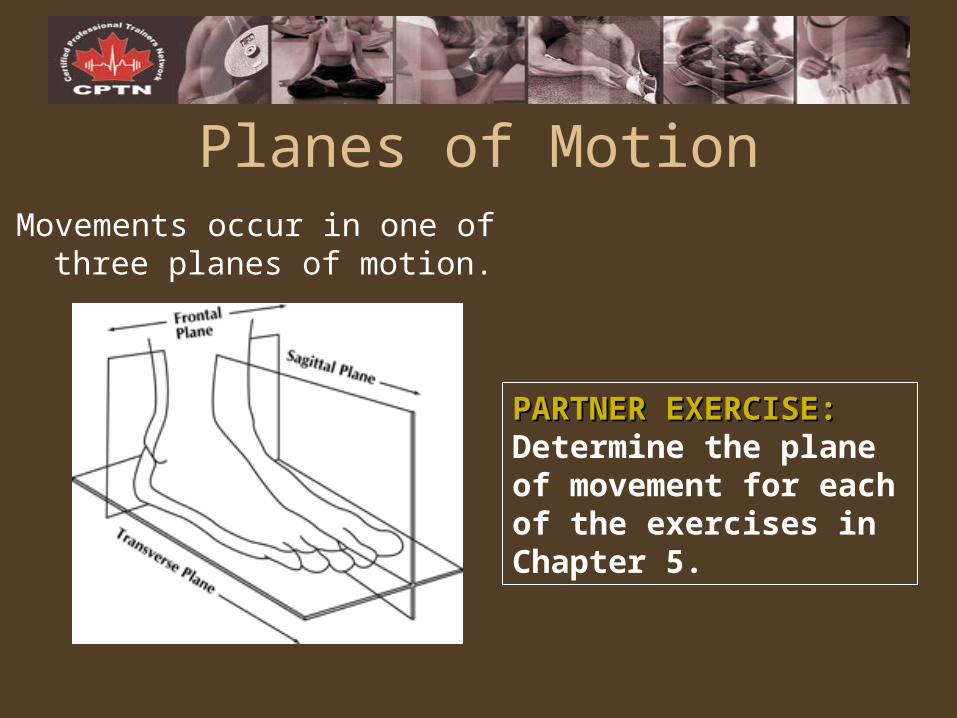
Planes of MotionMovements occur in one of
three planes of motion.
PARTNER EXERCISE:PARTNER EXERCISE: Determine the plane of movement for each of the exercises in Chapter 5.
LEVERSA lever is a rigid bar that rotates about an axis.
– Rotation is caused as force is applied to the lever.
– Two types of force act upon human levers, they are:
• Muscular force• Resistive force
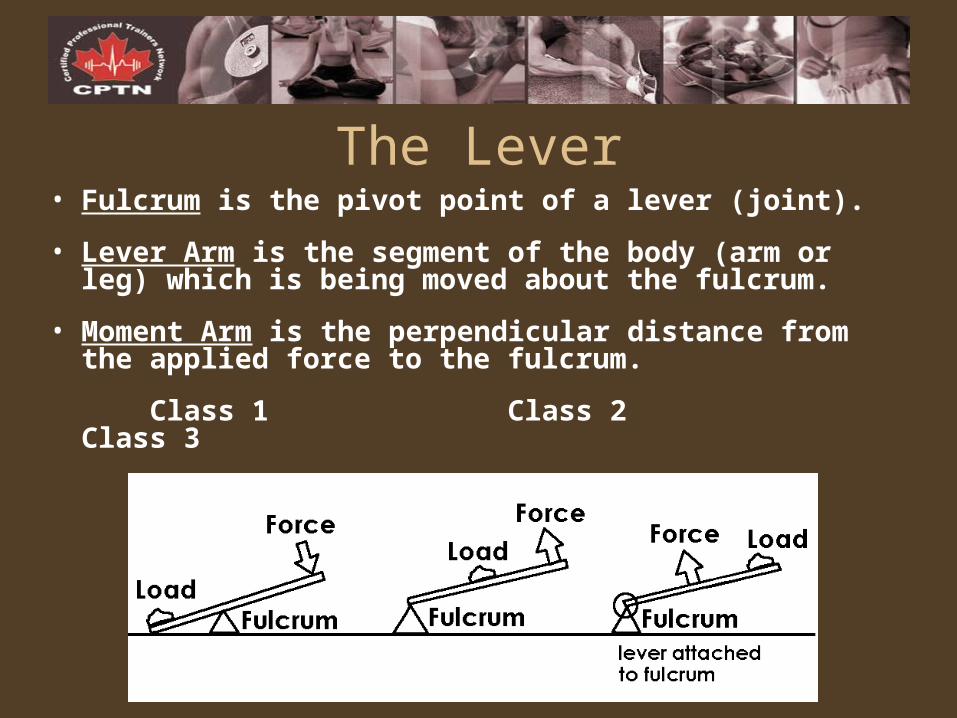
The Lever• Fulcrum is the pivot point of a lever (joint).
• Lever Arm is the segment of the body (arm or leg) which is being moved about the fulcrum.
• Moment Arm is the perpendicular distance from the applied force to the fulcrum.
Class 1 Class 2 Class 3
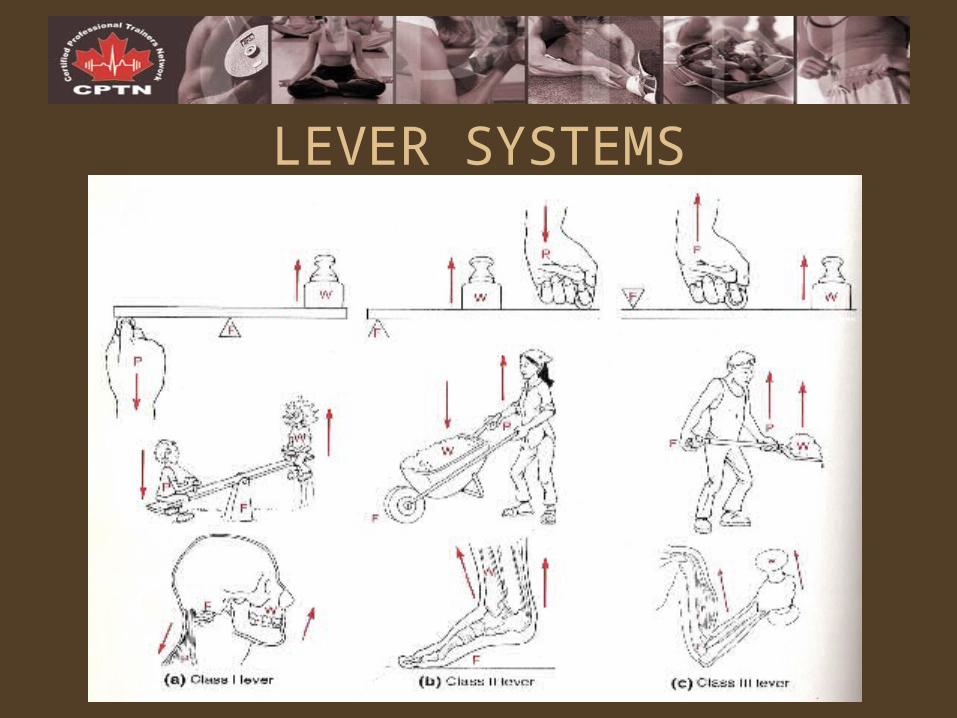
LEVER SYSTEMS
TorqueIs the degree to which a force tends to rotate a
lever about a fulcrum.Torque = F (rotational) x D (moment arm or force arm)
PARTNER EXERCISE:PARTNER EXERCISE:
1. Rank the following exercises in order according to which one produces the least amount of torque about the spine to the greatest.
BB Squat
BB Front Squat
Good Mornings
Stiff-Legged Deadlift
2. In what ways could proper technique reduce torque about the spine when squatting?
FORCE APPLICATIONSGROUP EXERCISE:GROUP EXERCISE: Provide an example for each of the following where the force either a) contributes to the intention of the exercise/movement, or b) works against the intention of the exercise/movement.
1. Static Friction
2. Kinetic Friction
3. Elastic Force
4. Air Resistance
5. Water Resistance
FORCE VECTORSPARTNER EXERCISE:PARTNER EXERCISE: Based upon the magnitude and direction of forces acting through the knee joint, rank the following versions of the lunge from the least stressful to the most stressful on the knees.• Reverse Lunge• Forward Lunge• Stationary Lunge
INTERNAL FORCES
BIOMECHANICAL FACTORS AFFECTING MUSCLE FORCEBIOMECHANICAL FACTORS AFFECTING MUSCLE FORCE
1. Length of Muscle (Optimal = 1.2x resting length)
2. Velocity of Muscle Contraction
- Concentrically: force decreases as velocity increases
- Eccentrically: force increases as velocity increases
3. Tendon Insertion
4. Changing Joint Angle
INCREASING FORCE GENERATIONPARTNER EXERCISE: PARTNER EXERCISE: Choosing one body part, provide a specific exercise example for manipulating each of the following factors in order to increase force generation in the muscle:
a) Stabilizing body segments
b) Increasing the range of motion of a particular exercise
c) Varying the speed of muscular contraction
d) Utilizing sequential movement
e) Increasing distance force is applied in selection of an exercise
f) Using strongest muscles available for a task
g) Using all the muscles that can contribute to a task
h) Pre-stretching a muscle just prior to contraction
i) Pre-loading the muscle prior to the task
Laws Governing Motion
Newton’s Three Laws
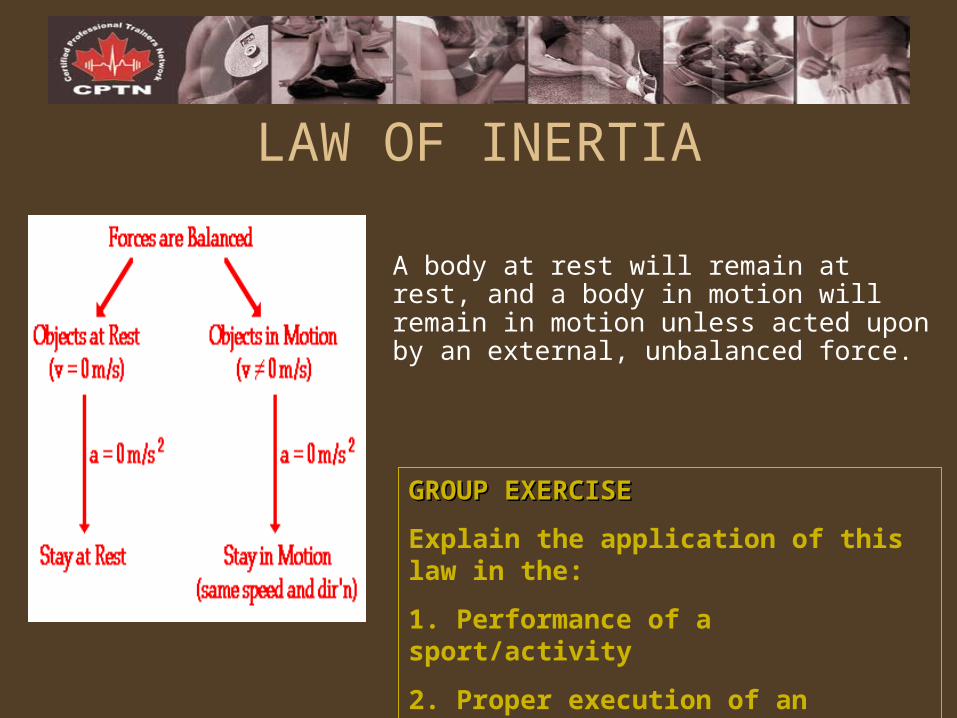
LAW OF INERTIA
A body at rest will remain at rest, and a body in motion will remain in motion unless acted upon by an external, unbalanced force.
GROUP EXERCISEGROUP EXERCISE
Explain the application of this law in the:
1. Performance of a sport/activity
2. Proper execution of an exercise
3. Design of PRT programs for Power
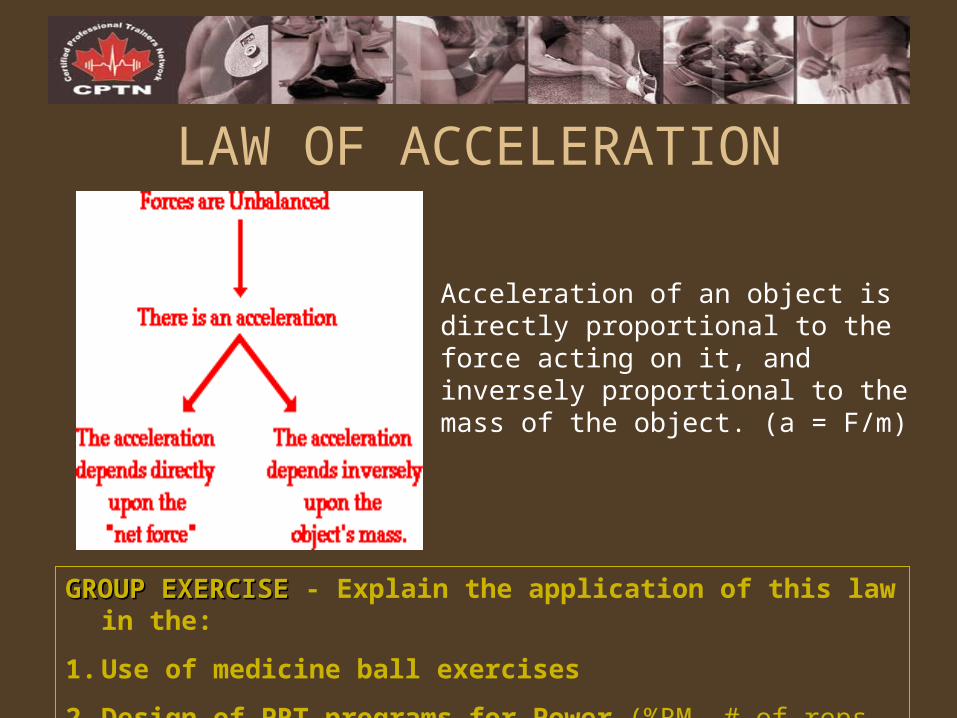
LAW OF ACCELERATION
Acceleration of an object is directly proportional to the force acting on it, and inversely proportional to the mass of the object. (a = F/m)
GROUP EXERCISEGROUP EXERCISE - Explain the application of this law in the:
1. Use of medicine ball exercises
2. Design of PRT programs for Power (%RM, # of reps, rep speed)
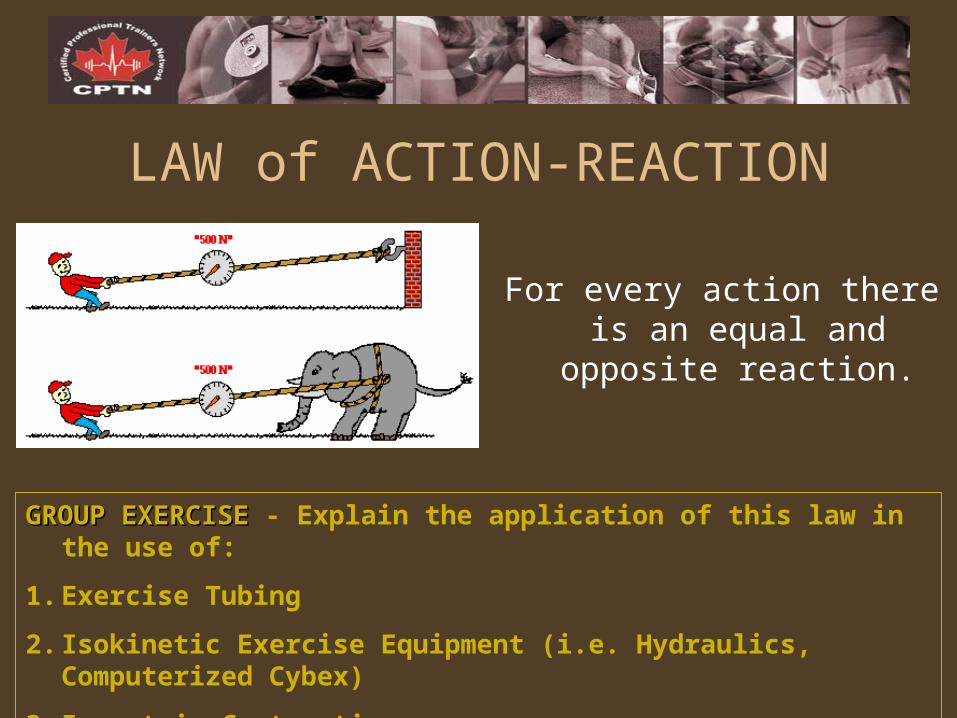
LAW of ACTION-REACTION
For every action there is an equal and
opposite reaction.
GROUP EXERCISEGROUP EXERCISE - Explain the application of this law in the use of:
1. Exercise Tubing
2. Isokinetic Exercise Equipment (i.e. Hydraulics, Computerized Cybex)
3. Isometric Contractions
Stability• Refers to the condition of balance where
the weight of an object (centre of gravity) is aligned perpendicularly over it’s base of supports.
• Stability is essential for proper execution of all exercises.
Factors Affecting Stability1.1. CENTRE OF GRAVITYCENTRE OF GRAVITYa) Location (more stability when COG closer to
centre of base of support)
b) Height (more stability when COG is lowered)
c) Force Application (more stability when force received close to COG)
2.2. BASE OF SUPPORTBASE OF SUPPORTa) Size of BOS (wide vs. narrow)
b) Contact Area
c) Number of Supports
d) Friction
3.3. MASSMASSa) Magnitude
b) Distribution
GROUP EXERCISE:GROUP EXERCISE: Referring to exercises using the stability ball, give examples of how the Factors Affecting Stability affect performance of the exercise.
MOTION ANALYSIS
PARTNER EXERCISE:PARTNER EXERCISE: Considering the amount of force exerted in relation to the amount of resistance present, and the direction of the applied force in relation to the direction of the resistance, determine the benefit-to-risk ratio (high vs. low) for the following examples:
1.DB Lateral Raise performed with arms straight vs. arms bent at 90 degrees
2.Loaded vs. Unloaded hip flexion while standing
3.Lying straight leg raises with a) no added resistance, b) added resistance, and c) actively applied acceleration





























