Embed Size (px)
Citation preview
Prepared by:Abdul Qadeer MBBS, MPH, CPHI(C), CIC Public Health PractitionerSeptember 22 , 2014
Lets Be AWARE!• Antibiotic resistance is a threat at focal, local
and global level.• The data collected so far is a snapshot of the
complex problem of antibiotic resistance .• An immediate action is required to address the
threat.• The consequences of inaction may be
catastrophic.


Microbial Threats to Mankind
CampB
Gonorrhea
Acinetobacter
Anthrax
MRSA
Salmonella
MTB
VRE VISA/VRSA
Influenza
Malaria
Candida
CPE
Information to Share with You Today!
• What are CPE and how they are different from other ARO?
• The mechanism of antimicrobial resistance.
• Global distribution of CPE.
• Current status of CPE in Ontario.
• Why are CPE of concerns?
• Why surveillance of CPE is necessary?
• The guidelines for controlling the transmission of CPE.

Resources used

CPE Has Arrived Here
September 22, 2014
Myths about Superbugs
1. Antibiotic resistant organisms are more virulent.2. Irrational use of drugs (antimicrobials) cause
antibiotic resistance.
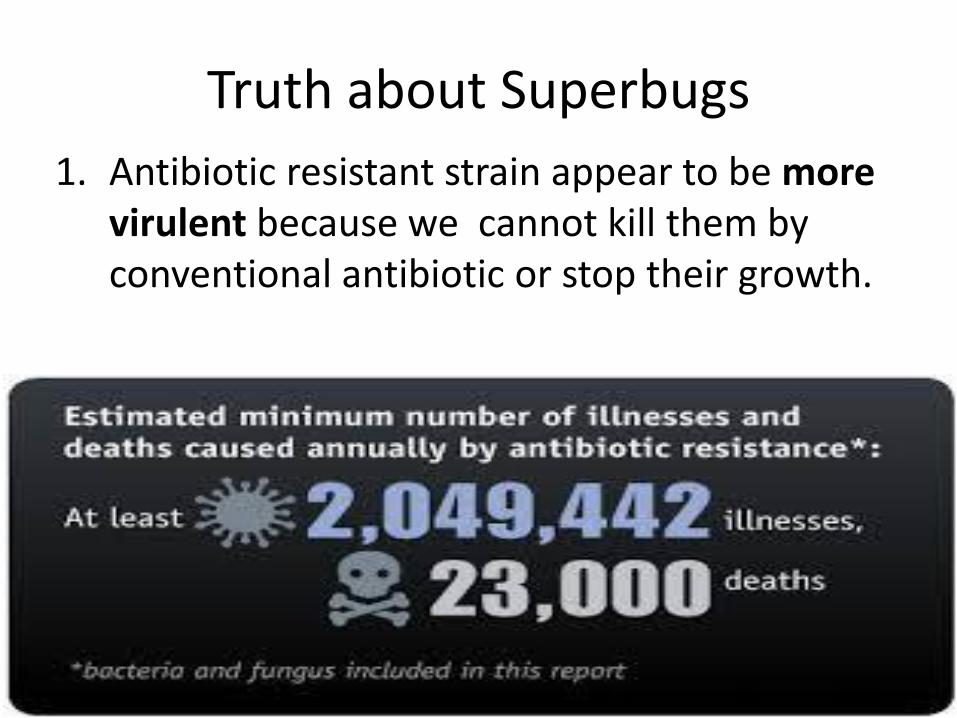
Truth about Superbugs
1. Antibiotic resistant strain appear to be more virulent because we cannot kill them by conventional antibiotic or stop their growth.
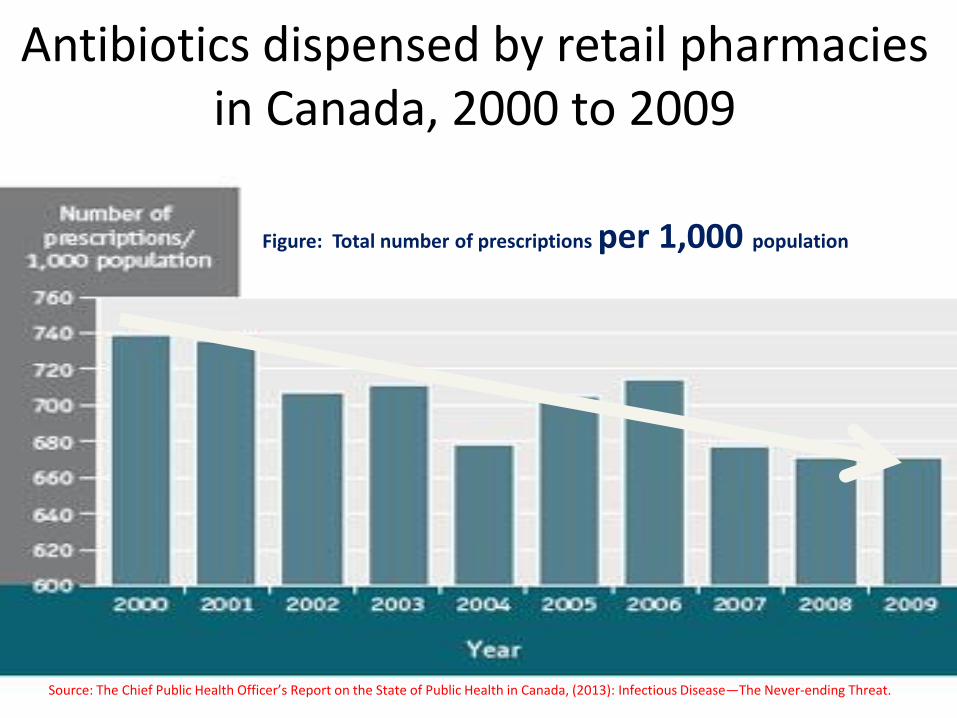
Antibiotics dispensed by retail pharmacies in Canada, 2000 to 2009
Source: The Chief Public Health Officer’s Report on the State of Public Health in Canada, (2013): Infectious Disease—The Never-ending Threat.
Figure: Total number of prescriptions per 1,000 population
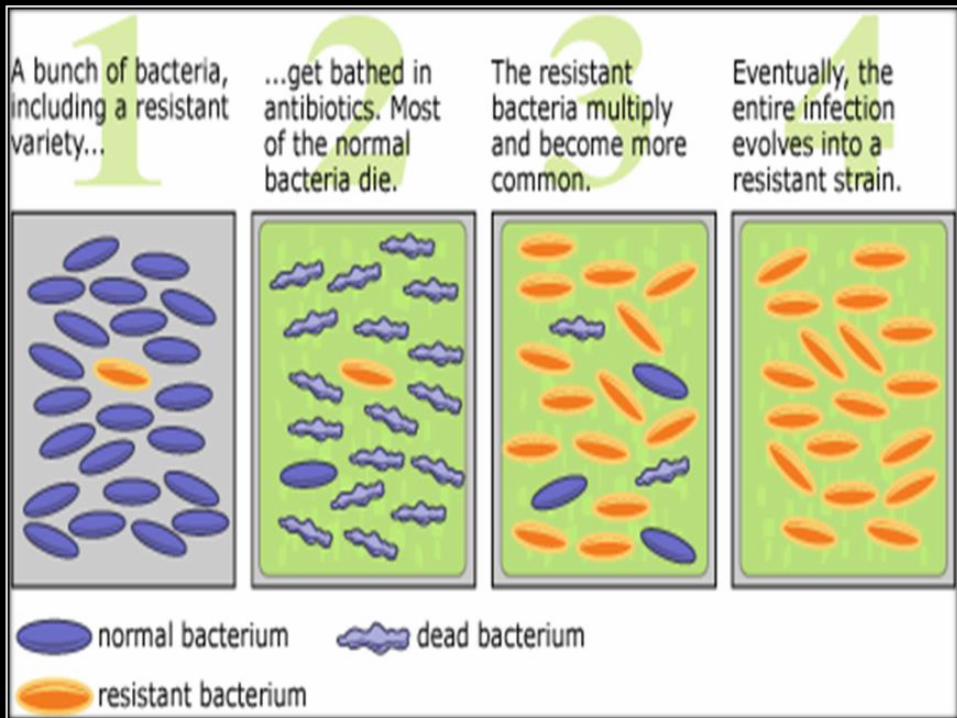
Truth about Superbugs
•2. Antibiotic select out the resistant strain.
• Faulty use or widespread use of antibiotics
• increases the probability of such selection.
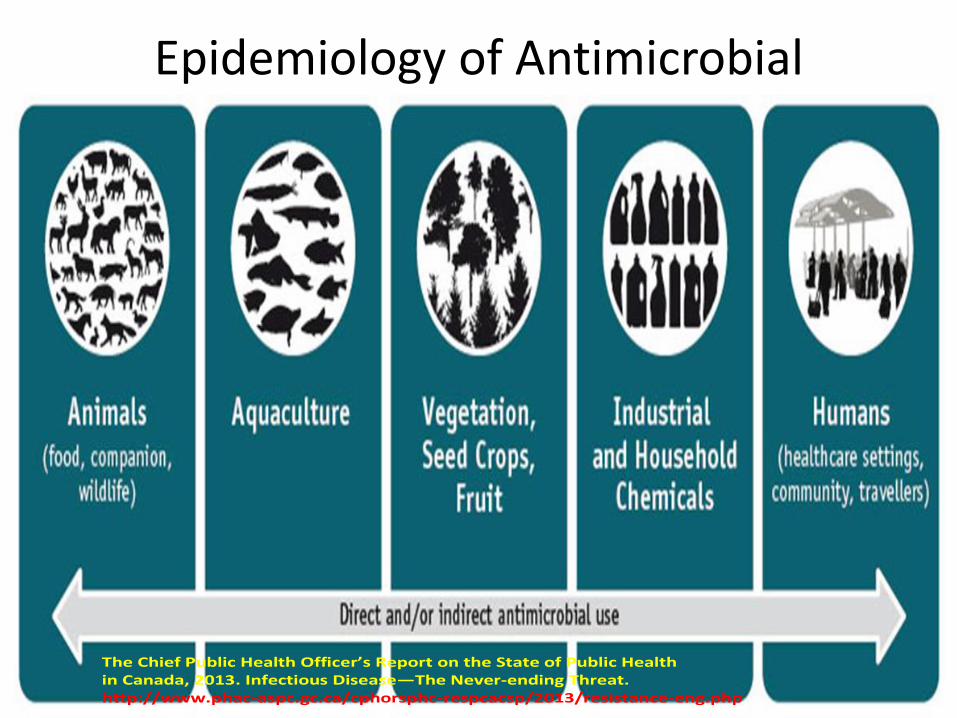
Epidemiology of Antimicrobial Resistance
The Chief Public Health Officer’s Report on the State of Public Health in Canada, 2013. Infectious Disease—The Never-ending Threat. http://www.phac-aspc.gc.ca/cphorsphc-respcacsp/2013/resistance-eng.php

Simply Overloaded
Intrinsic Microbial Resistance
Bacteria may be naturally resistant or insensitive to antimicrobial agents.
resistance occurs by different mechanisms.
the MAJORITY of the strains of bacterial species can show intrinsic resistance.
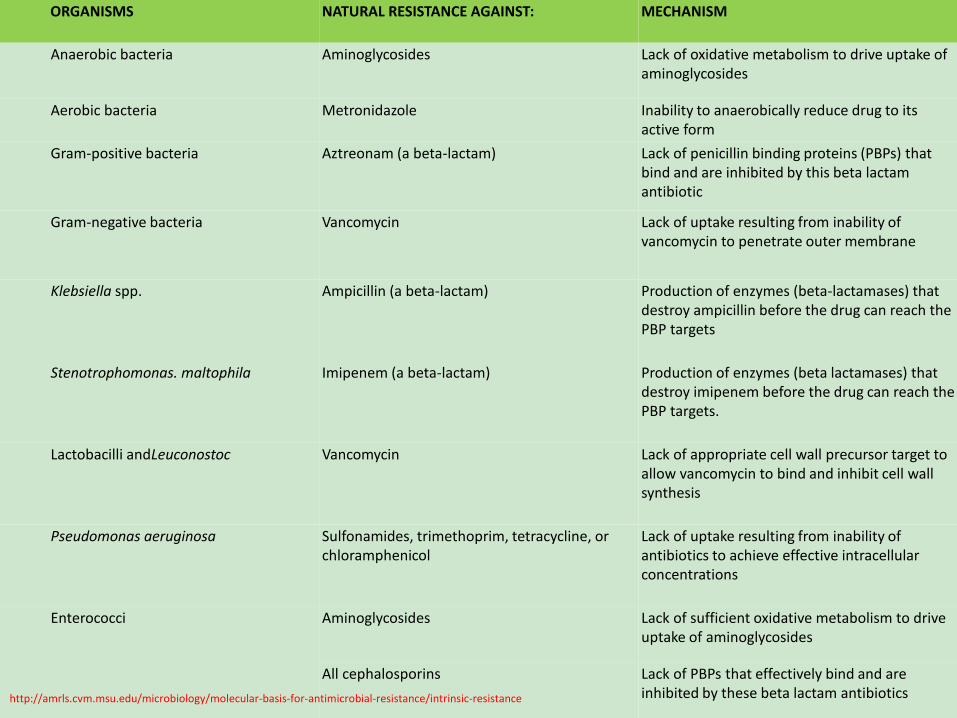
ORGANISMS NATURAL RESISTANCE AGAINST: MECHANISM
Anaerobic bacteria Aminoglycosides Lack of oxidative metabolism to drive uptake of aminoglycosides
Aerobic bacteria Metronidazole Inability to anaerobically reduce drug to its active form
Gram-positive bacteria Aztreonam (a beta-lactam) Lack of penicillin binding proteins (PBPs) that bind and are inhibited by this beta lactam antibiotic
Gram-negative bacteria Vancomycin Lack of uptake resulting from inability of vancomycin to penetrate outer membrane
Klebsiella spp. Ampicillin (a beta-lactam) Production of enzymes (beta-lactamases) that destroy ampicillin before the drug can reach the PBP targets
Stenotrophomonas. maltophila Imipenem (a beta-lactam) Production of enzymes (beta lactamases) that destroy imipenem before the drug can reach the PBP targets.
Lactobacilli andLeuconostoc Vancomycin Lack of appropriate cell wall precursor target to allow vancomycin to bind and inhibit cell wall synthesis
Pseudomonas aeruginosa Sulfonamides, trimethoprim, tetracycline, or chloramphenicol
Lack of uptake resulting from inability of antibiotics to achieve effective intracellular concentrations
Enterococci Aminoglycosides Lack of sufficient oxidative metabolism to drive uptake of aminoglycosides
All cephalosporins Lack of PBPs that effectively bind and are inhibited by these beta lactam antibioticshttp://amrls.cvm.msu.edu/microbiology/molecular-basis-for-antimicrobial-resistance/intrinsic-resistance
Acquired Microbial Resistance
Acquired resistant develop after exposure to antimicrobial agents. It can occur through:
• Alteration in cell wall that restrict drug entry into the microbial cell (e.g. porin loss).
• Presence of ‘pumps’ which remove antimicrobial.• Development of substitute ‘proteins’ that are not
targeted by drugs.• Development of ‘enzyme’ that destroy or inactivate
antimicrobials. Acquired resistance is LESS COMMON, existing only in
some bacterial strains.
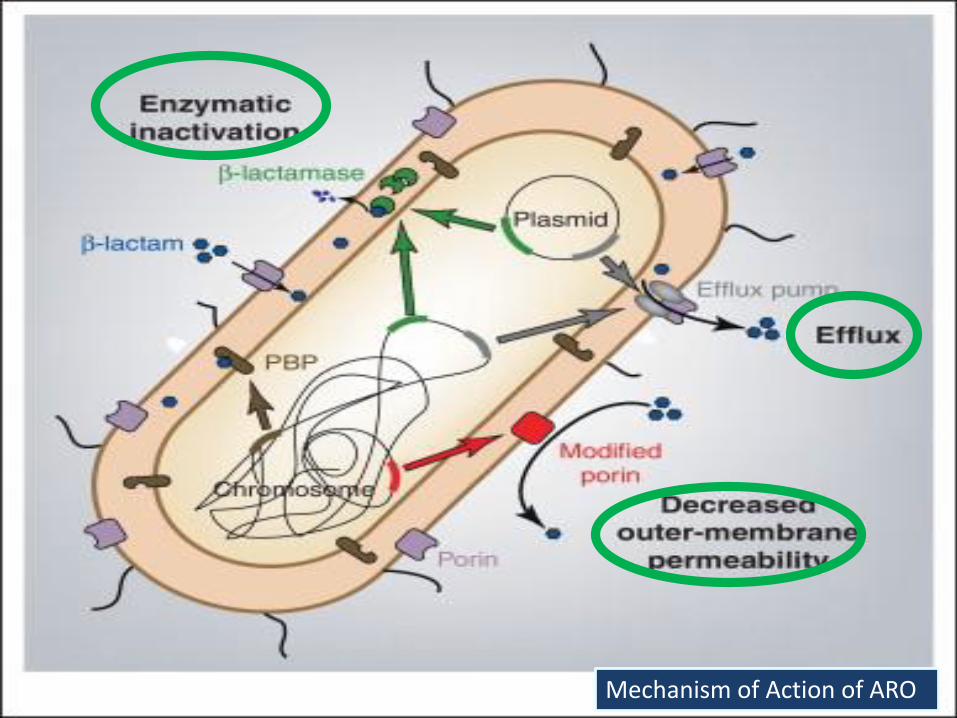
Mechanism of Action of ARO
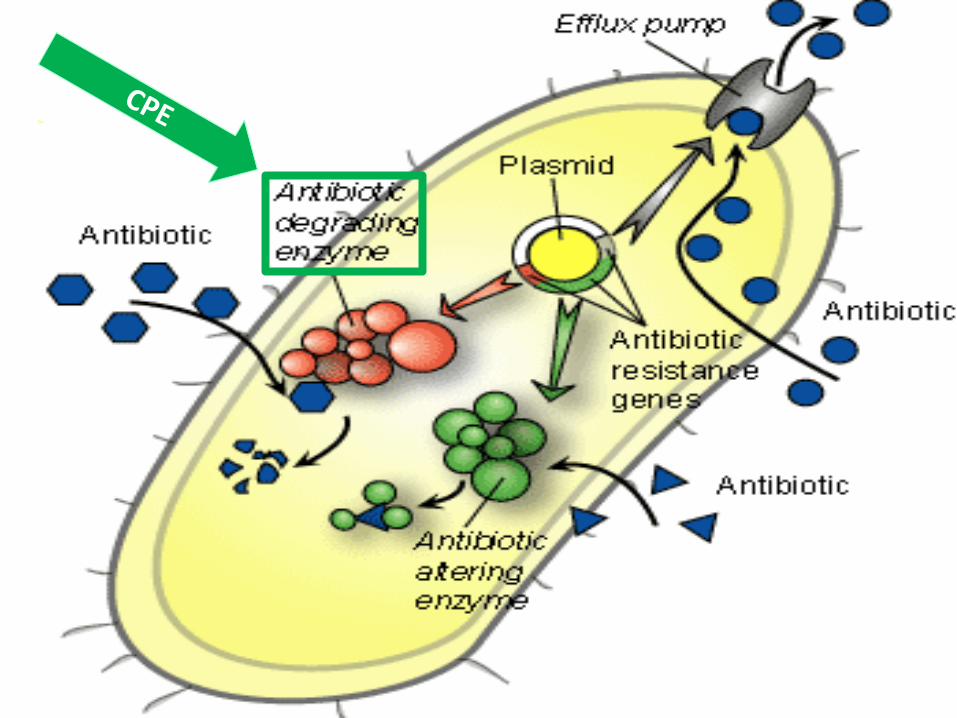
Carbapenemase Producing Enterobacteriacea (CPE)
are bacteria:
• in the family of Enterobacteriaceae
• acquired resistant to carbapenem is due to Cabapenemase enzyme.
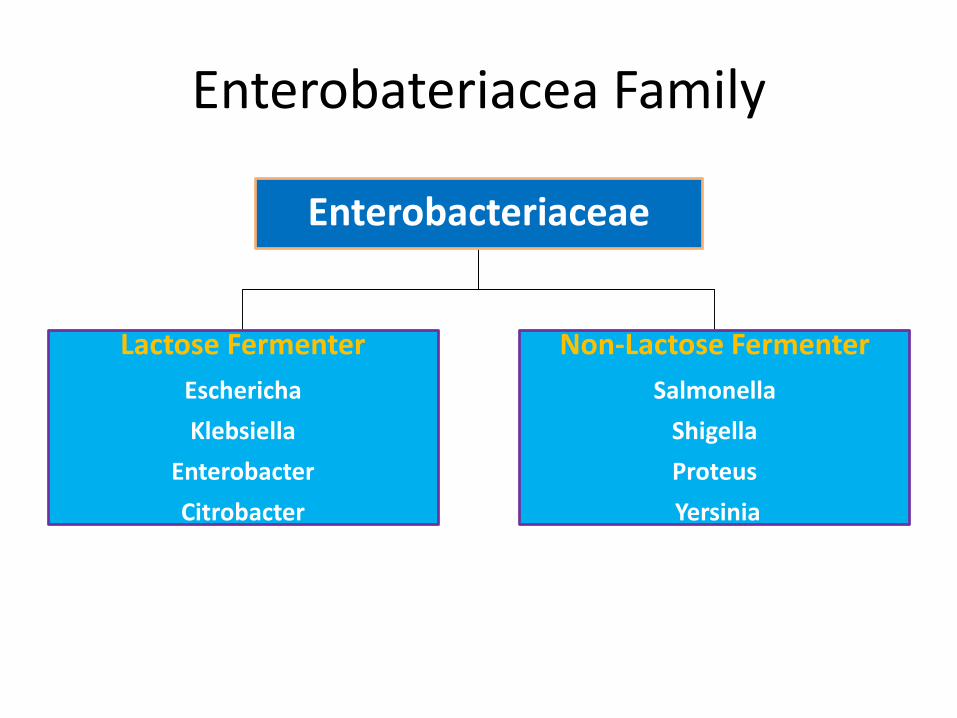
Enterobateriacea Family
Enterobacteriaceae
Lactose Fermenter
Eschericha
Klebsiella
Enterobacter
Citrobacter
Non-Lactose Fermenter
Salmonella
Shigella
Proteus
Yersinia
Generalities of Enterobacteriaceae
All Gram negative rods, resident of GI & Urinary tract.
• Transmission:
Fecal-oral
Ascending migration to urethra
Colonization of lumen of Foley and Central lines
• Toxin: Produce enterotoxin
• Pathology:
Diarrhoea
Pneumonia
E. coli
Normal flora of colon; Motile and become virulent.
Virulence factors:
Mucosal adherence with pilli, intestinal epithelial invasion
Toxin production (exo & endo)
Clinical: 6 serotypes Diarrhea (ETEC-TD); (EHEC- HUS, BD); (EIEC- BD with WBC)
UTI
Neonatal meningitis
Sepsis in hospitalized pts
Treatment: Cephalosporin, Aminoglycoside, Fluoroquinolones
Klebsiella pneumoniae
• Non-motile enteric
• 2nd most common cause of HAI
Pathology:
HA-UTI and Sepsis
HA- pneumonia with bloody sputum, commonly in alcoholics or those with underlying lung Ds.
Treatment: 3rd gen. Cephalosporin and Cipro
Initially resistant G nve organism called - CRO
Resistant Enterobateriaceae called – CRE• Resistance developed due to combinations of a β-lactamase
enzyme and porin loss.
• These strains rarely spread.
Resistant Enterobacteriacea due to Carbapenemase
enzyme that inactivate Carbapenems - CPE
• CPE are the more serious risk and are beginning to spread
worldwide.
Confusing Terms used for Carbapenem Resistance
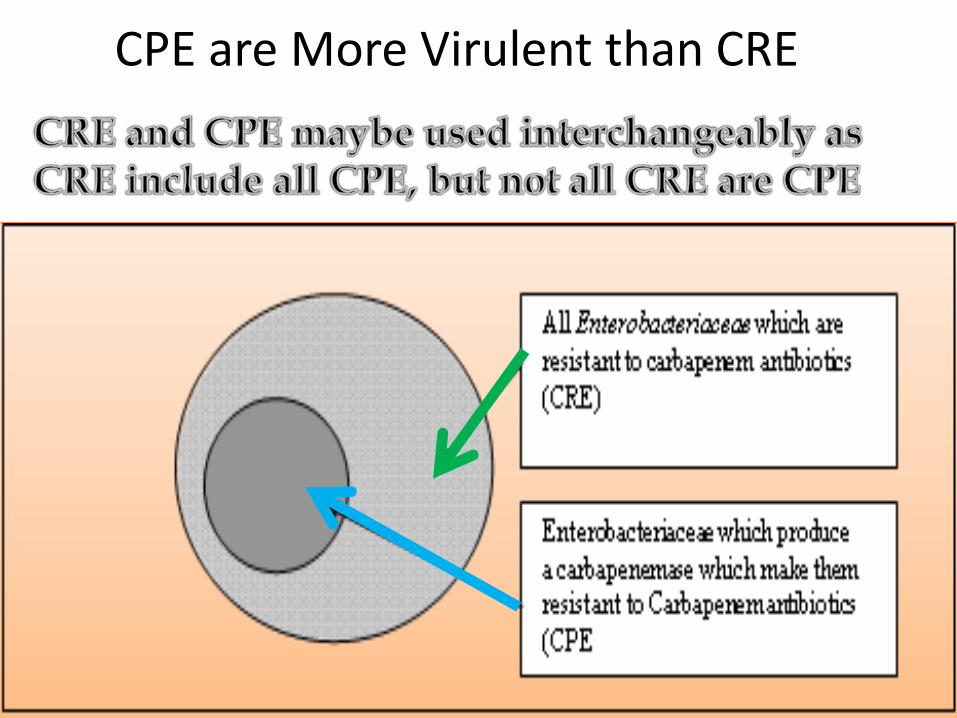
CPE are More Virulent than CRE
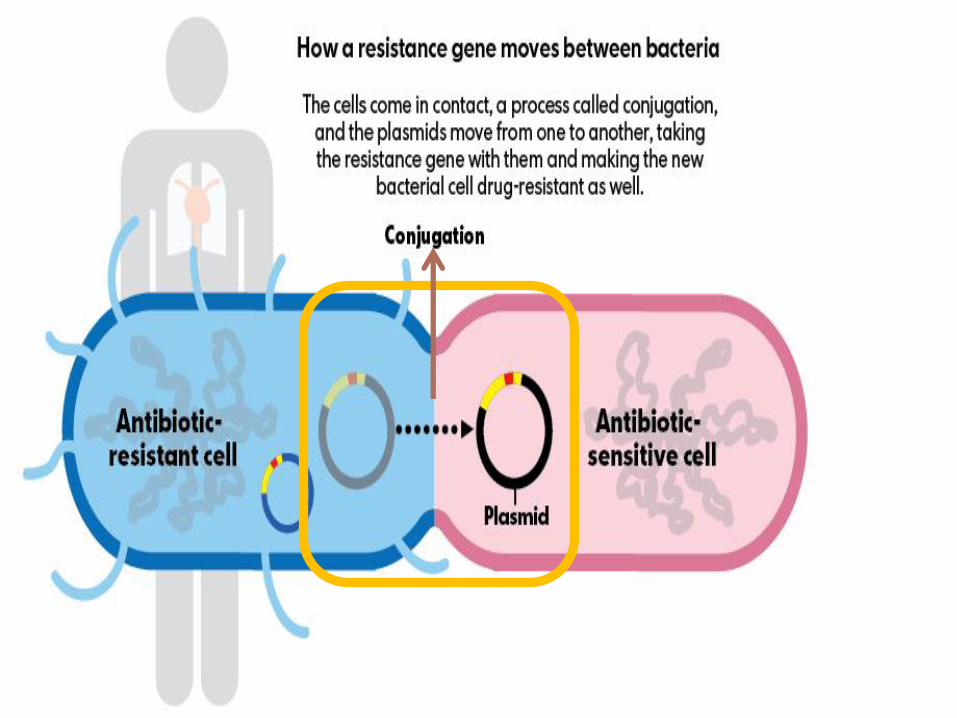
BIG Concern about CPE
o CPE have highly mobile genetic elements which allows them to transfer resistance genes very rapidly between different bacteria.
o EVIDENCE suggested that plasmid spread has occurred among and between K.pneumoniae
and E.colli via conjugation.
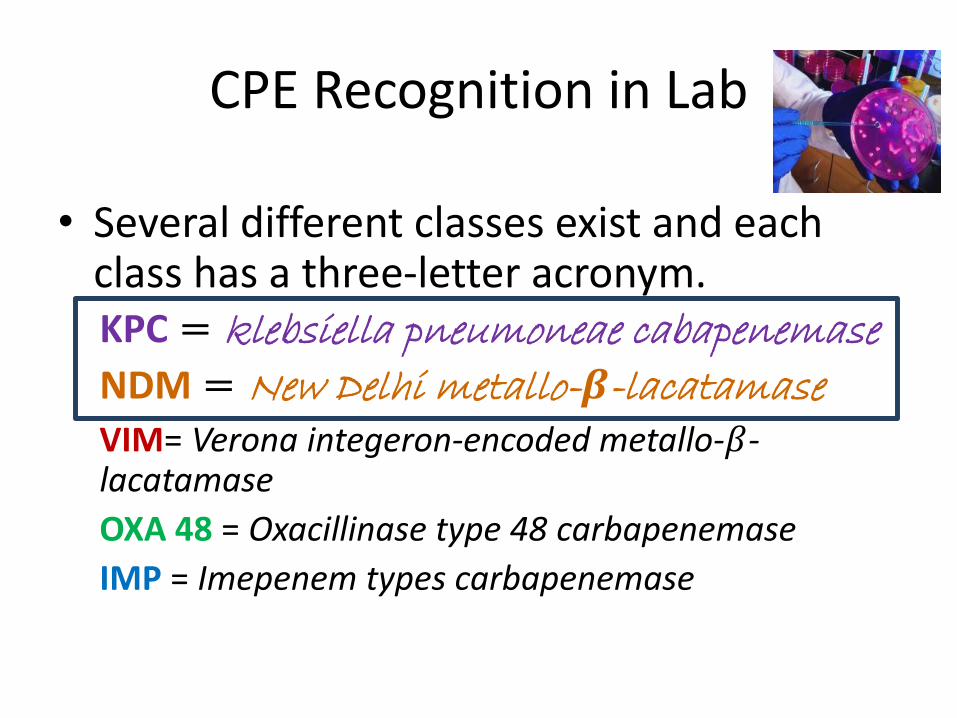
CPE Recognition in Lab
• Several different classes exist and each class has a three-letter acronym.KPC = klebsiella pneumoneae cabapenemase
NDM = New Delhi metallo-𝜷-lacatamaseVIM= Verona integeron-encoded metallo-𝛽-lacatamase
OXA 48 = Oxacillinase type 48 carbapenemase
IMP = Imepenem types carbapenemase
E.Coli and K. pneumoniae are CRE & CPE
o E.Coli & K. pneumoniae that have developed resistance due to β-lactamase enzyme and porin loss are called -
o E.Coli & K. pneumoniae that have acquired multi-drug resistance due to production of Cabapenemase enzyme – . These species are more serious risk.
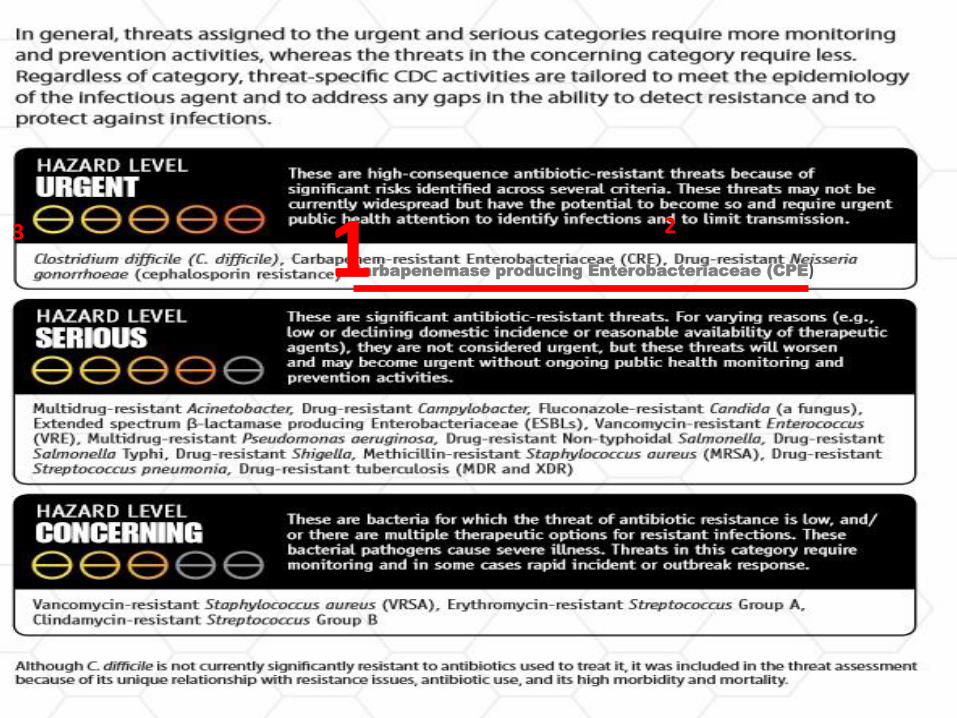
Carbapenemase producing Enterobacteriaceae (CPE)
23 1
CPE Surveillance in Ontario!
o Reported (imported) in Ontario since 2008.
o PHO and MOHLTC initiated a voluntary surveillance program to assess the
epidemiology of CPE in 2011.
o Epidemiological data is critical for informing IPAC policies and procedures that will help prevent the likelihood of CPE becoming endemic in Ontario.

picture
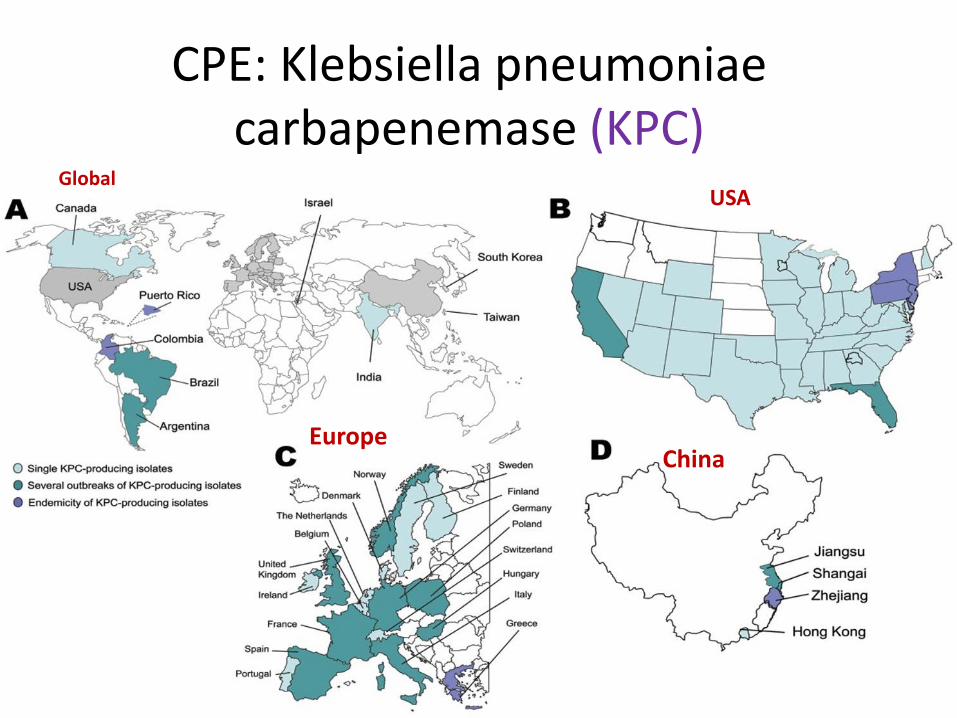
CPE: Klebsiella pneumoniae carbapenemase (KPC)
GlobalUSA
EuropeChina
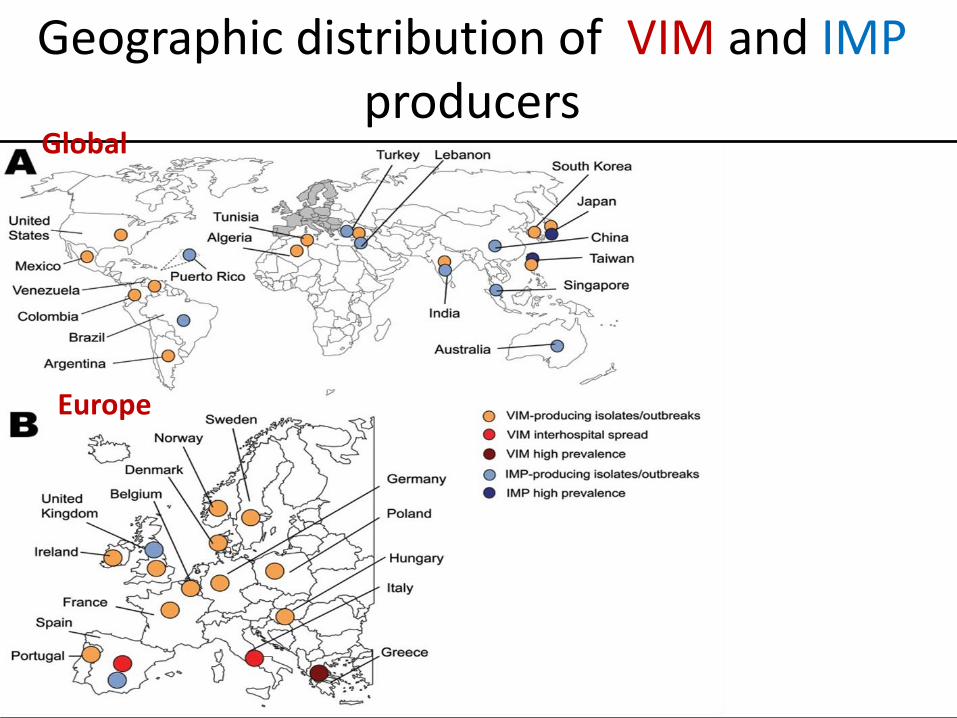
Geographic distribution of VIM and IMPproducers
Europe
Global
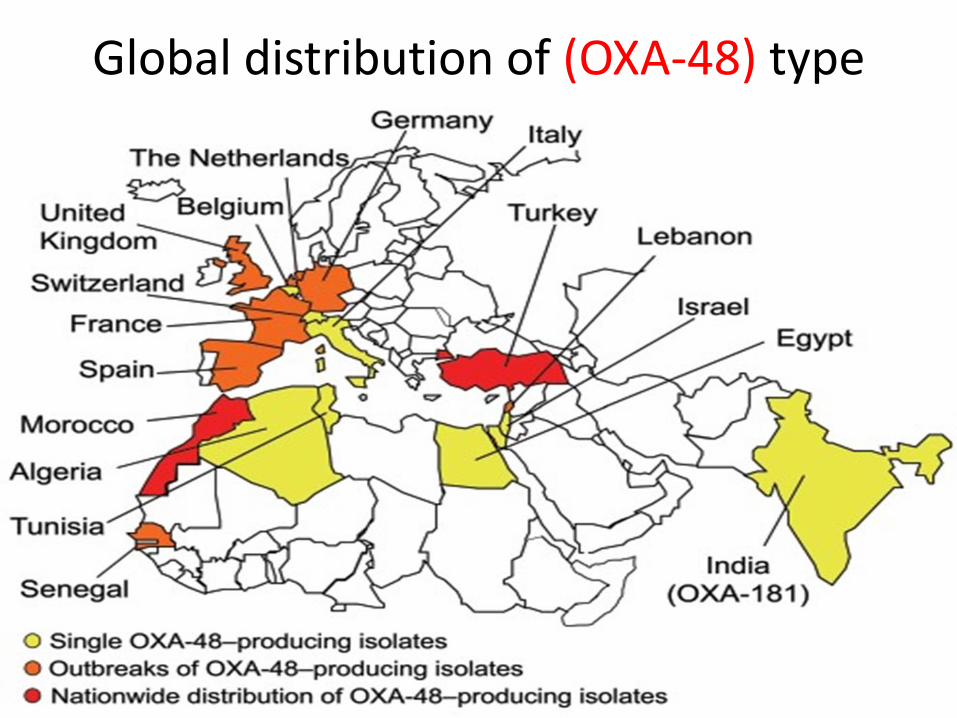
Global distribution of (OXA-48) type producers
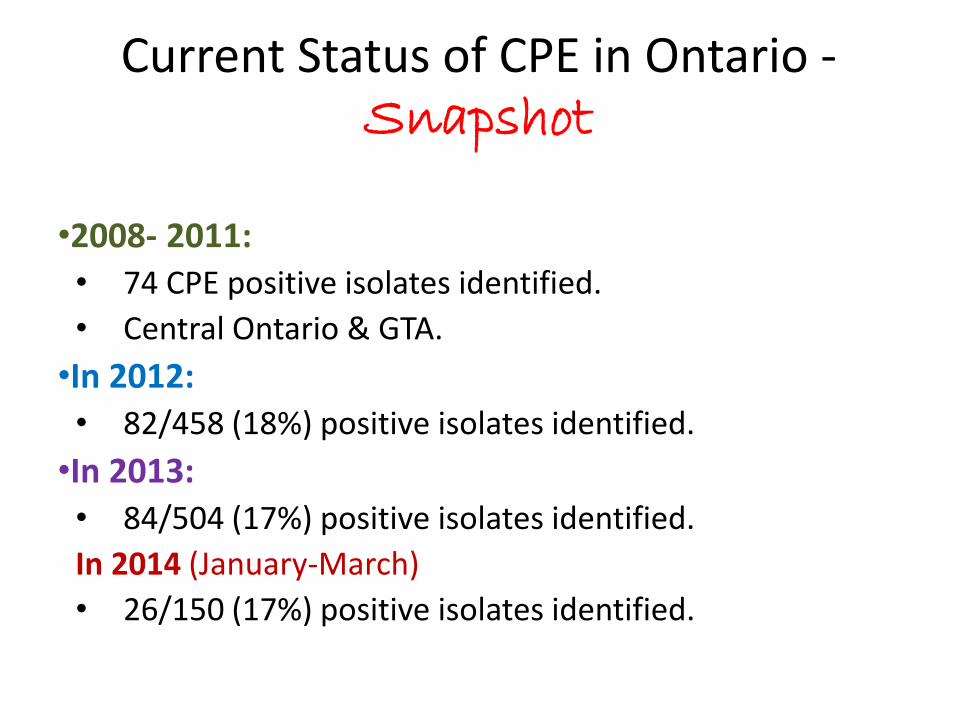
Current Status of CPE in Ontario -Snapshot
•2008- 2011: • 74 CPE positive isolates identified.
• Central Ontario & GTA.
•In 2012: • 82/458 (18%) positive isolates identified.
•In 2013: • 84/504 (17%) positive isolates identified.
In 2014 (January-March)
• 26/150 (17%) positive isolates identified.
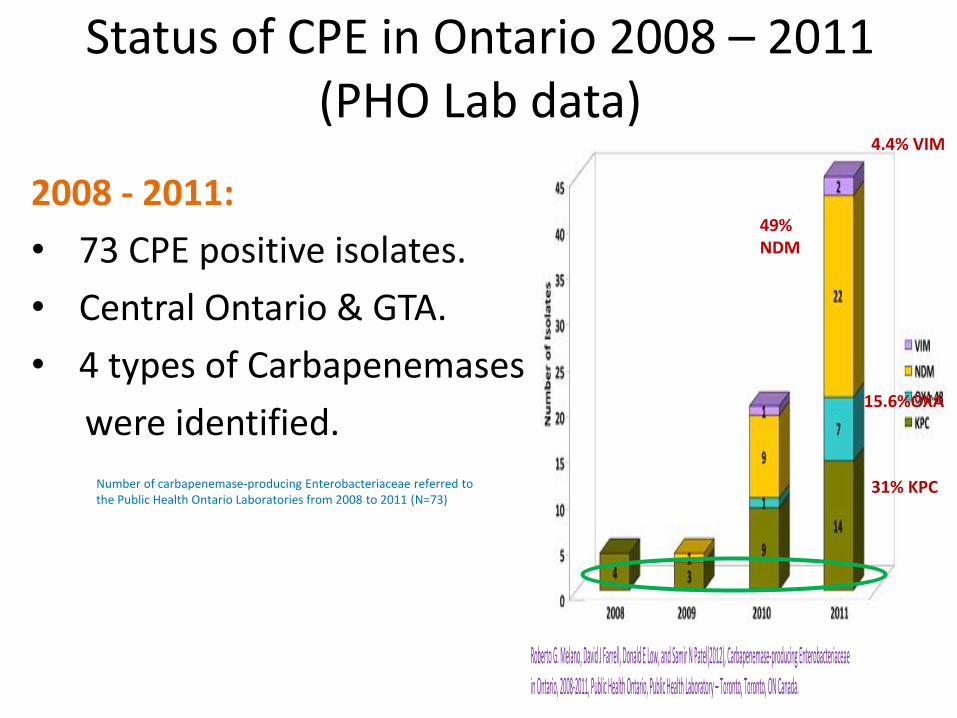
Status of CPE in Ontario 2008 – 2011 (PHO Lab data)
Number of carbapenemase-producing Enterobacteriaceae referred to the Public Health Ontario Laboratories from 2008 to 2011 (N=73)
2008 - 2011:
• 73 CPE positive isolates.
• Central Ontario & GTA.
• 4 types of Carbapenemases
were identified.
Roberto G. Melano, David J Farrell, Donald E Low, and Samir N Patel(2012), Carbapenemase-producing Enterobacteriaceae in Ontario, 2008-2011, Public Health Ontario, Public Health Laboratory – Toronto, Toronto, ON Canada.
49% NDM
15.6%OXA
4.4% VIM
31% KPC
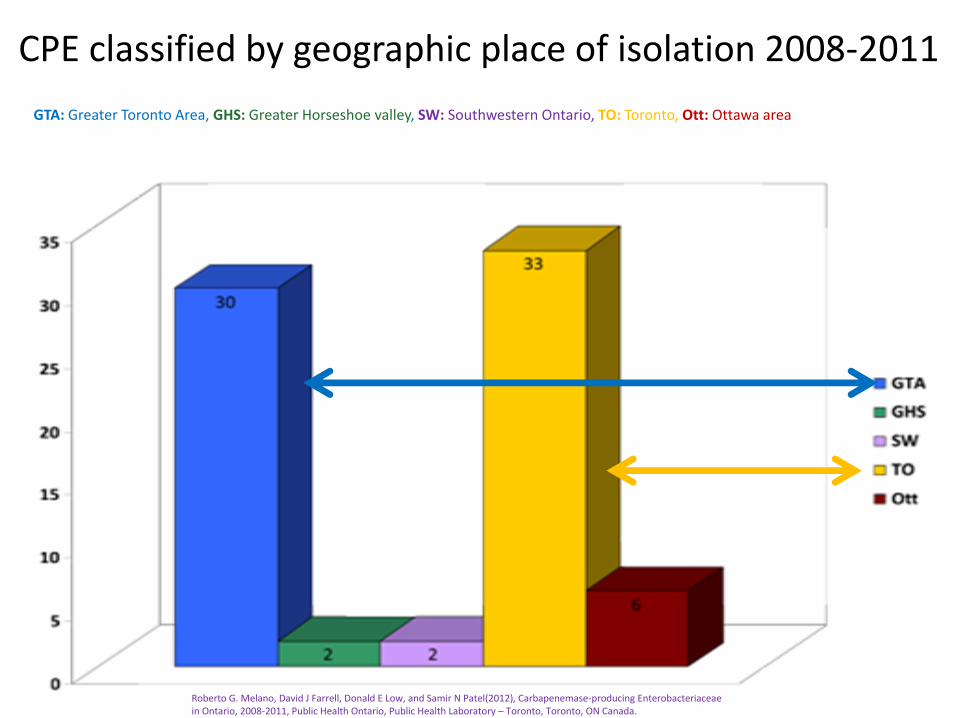
CPE classified by geographic place of isolation 2008-2011
GTA: Greater Toronto Area, GHS: Greater Horseshoe valley, SW: Southwestern Ontario, TO: Toronto, Ott: Ottawa area
Roberto G. Melano, David J Farrell, Donald E Low, and Samir N Patel(2012), Carbapenemase-producing Enterobacteriaceae in Ontario, 2008-2011, Public Health Ontario, Public Health Laboratory – Toronto, Toronto, ON Canada.
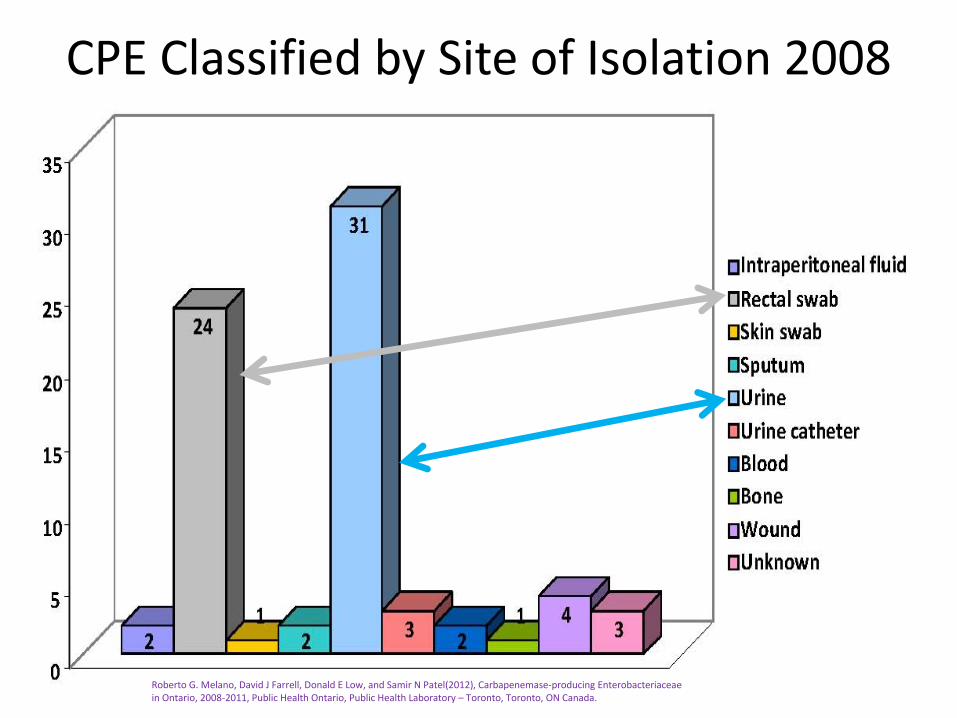
CPE Classified by Site of Isolation 2008 -2011
Roberto G. Melano, David J Farrell, Donald E Low, and Samir N Patel(2012), Carbapenemase-producing Enterobacteriaceae in Ontario, 2008-2011, Public Health Ontario, Public Health Laboratory – Toronto, Toronto, ON Canada.

CPE Epidemiological Data Summary 2012
January -December 2012
Source of submission No. of CPEpositive isolates
Percentage ofall positive isolates
(%)
Total submitted
isolates
Large community hospital48
59 231
Acute teaching hospital 19 23 95
Community laboratory 14 17 129
Complex Continuing Care& Rehabilitation
1 1 1
Small community hospital 0 0 2
Total 82 100 458
Number & percentage of CPE positive isolates by source of submission in Ontario
Source: Public Health Ontario Laboratories, Carbapenemase Producing Enterobacteriaceae database, extracted by Public Health Ontario [2013/07/02]
Attack rate
82÷458 ×100 =18%
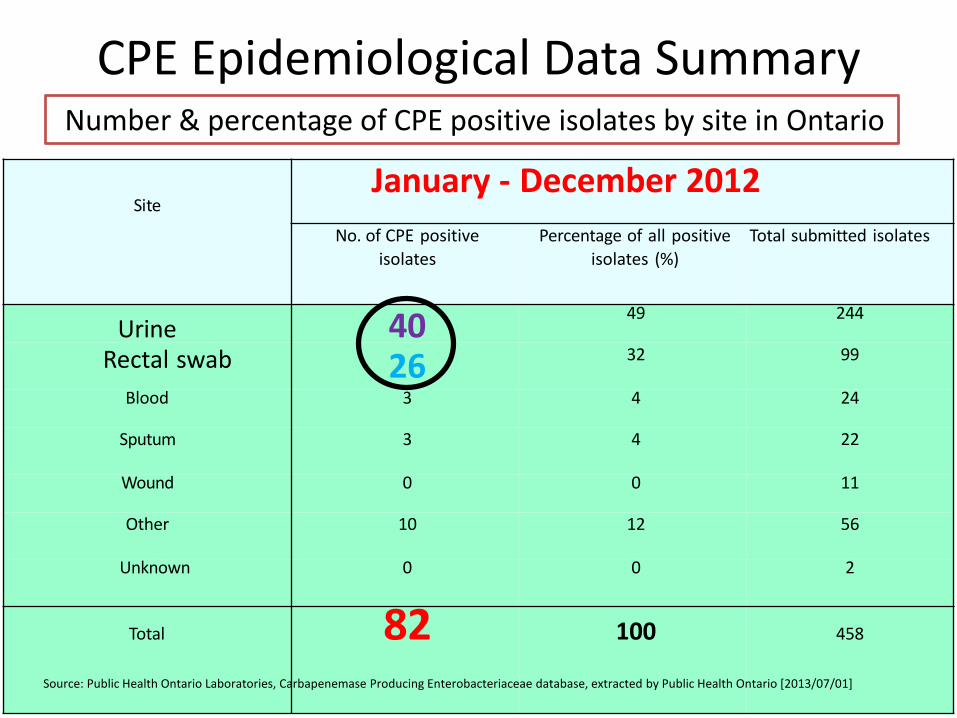
CPE Epidemiological Data Summary 2012
SiteJanuary - December 2012
No. of CPE positive
isolates
Percentage of all positive
isolates (%)
Total submitted isolates
Urine 40 49 244
Rectal swab 26 32 99
Blood 3 4 24
Sputum 3 4 22
Wound 0 0 11
Other 10 12 56
Unknown 0 0 2
Total 82 100 458
Number & percentage of CPE positive isolates by site in Ontario
Source: Public Health Ontario Laboratories, Carbapenemase Producing Enterobacteriaceae database, extracted by Public Health Ontario [2013/07/01]
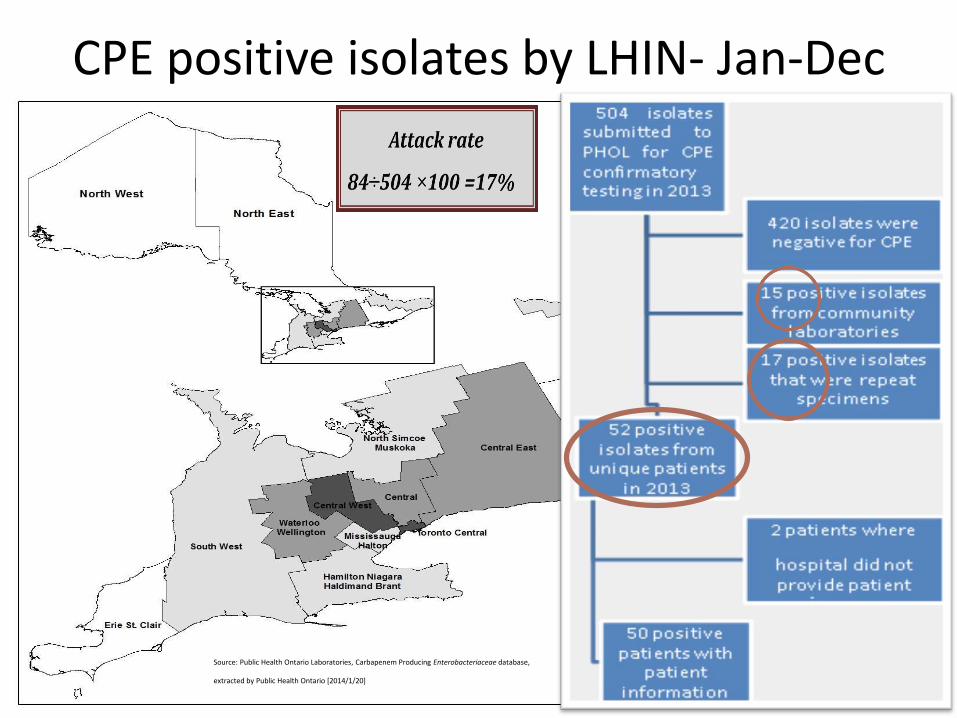
CPE positive isolates by LHIN- Jan-Dec 2013
Source: Public Health Ontario Laboratories, Carbapenem Producing Enterobacteriaceae database,
extracted by Public Health Ontario [2014/1/20]
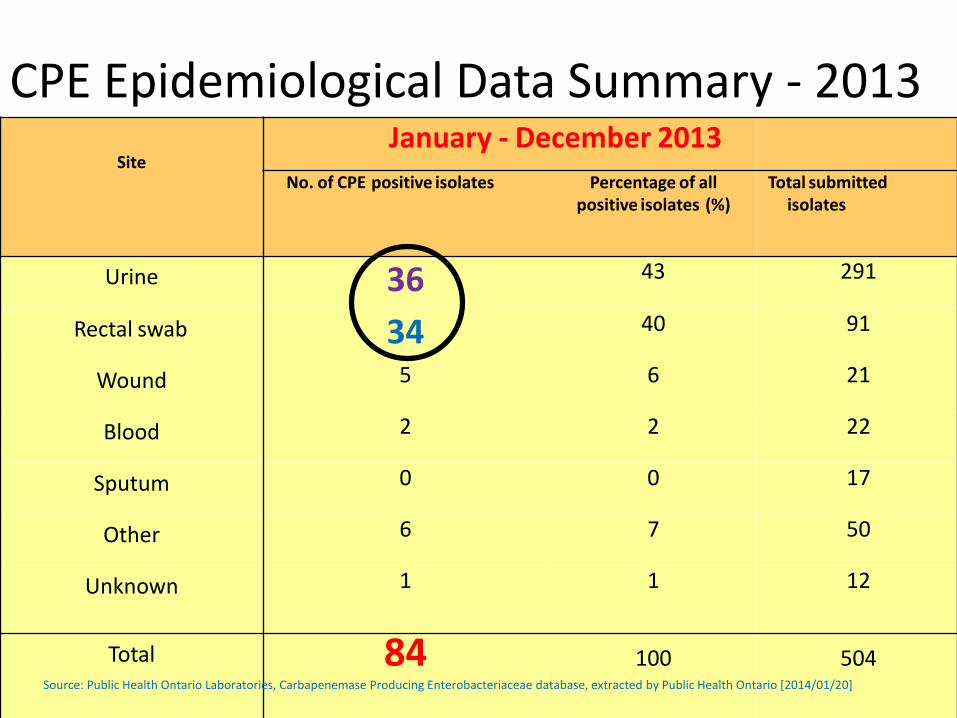
CPE Epidemiological Data Summary - 2013
SiteJanuary - December 2013
No. of CPE positive isolates Percentage of allpositive isolates (%)
Total submittedisolates
Urine 36 43 291
Rectal swab 34 40 91
Wound 5 6 21
Blood 2 2 22
Sputum 0 0 17
Other 6 7 50
Unknown 1 1 12
Total 84 100 504Source: Public Health Ontario Laboratories, Carbapenemase Producing Enterobacteriaceae database, extracted by Public Health Ontario [2014/01/20]
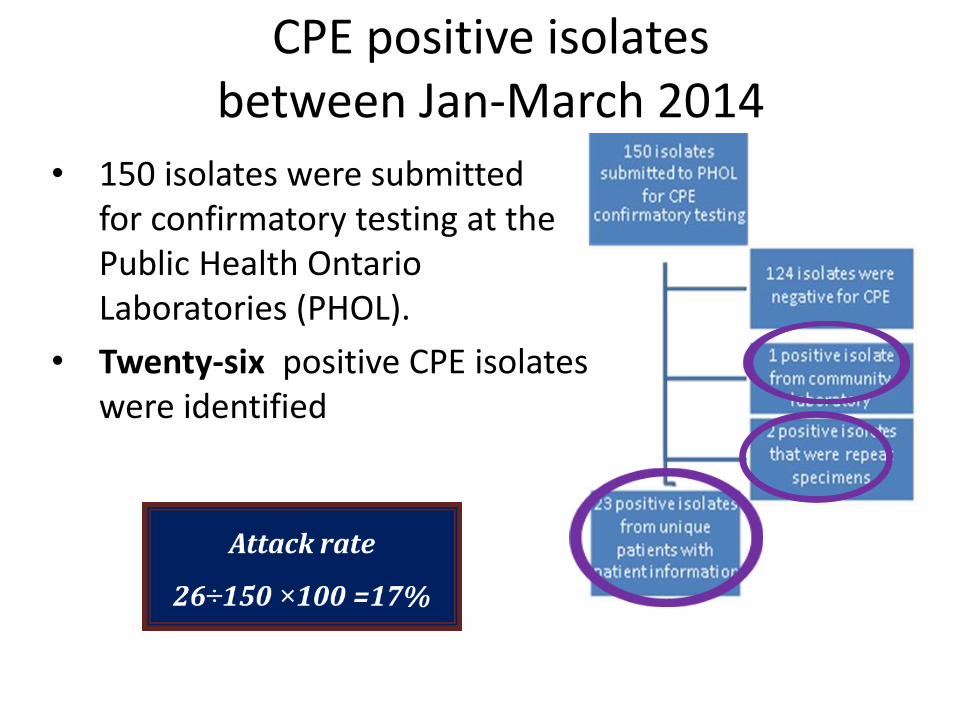
CPE positive isolates between Jan-March 2014
• 150 isolates were submitted for confirmatory testing at the Public Health Ontario Laboratories (PHOL).
• Twenty-six positive CPE isolates were identified
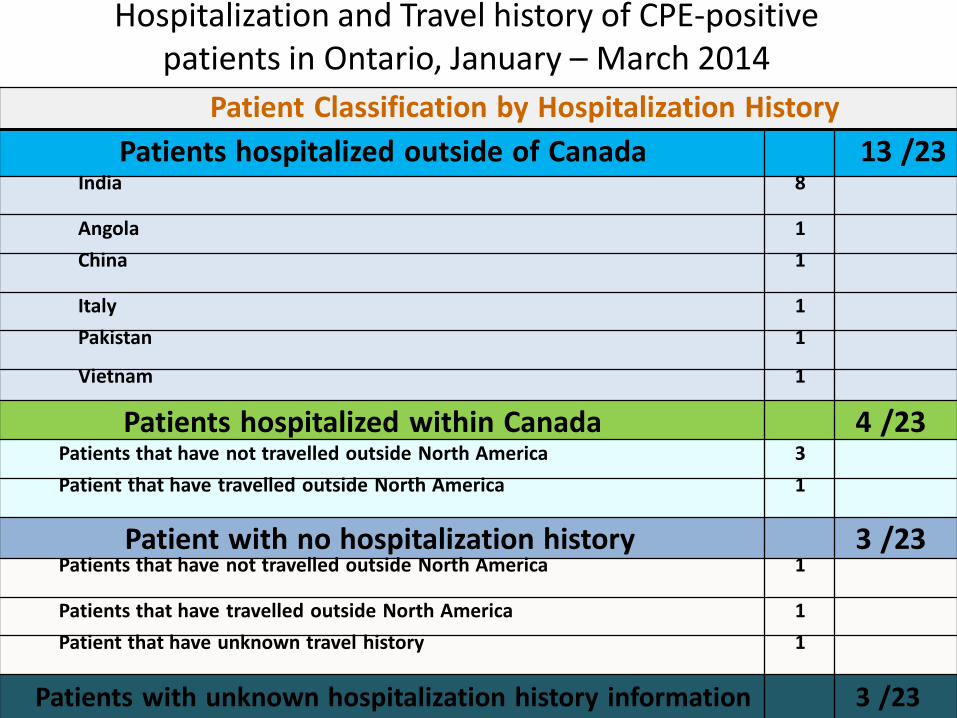
Hospitalization and Travel history of CPE-positive patients in Ontario, January – March 2014
Patient Classification by Hospitalization History
Patients hospitalized outside of Canada 13 /23India 8
Angola 1
China 1
Italy 1
Pakistan 1
Vietnam 1
Patients hospitalized within Canada 4 /23Patients that have not travelled outside North America 3
Patient that have travelled outside North America 1
Patient with no hospitalization history 3 /23Patients that have not travelled outside North America 1
Patients that have travelled outside North America 1
Patient that have unknown travel history 1
Patients with unknown hospitalization history information 3 /23
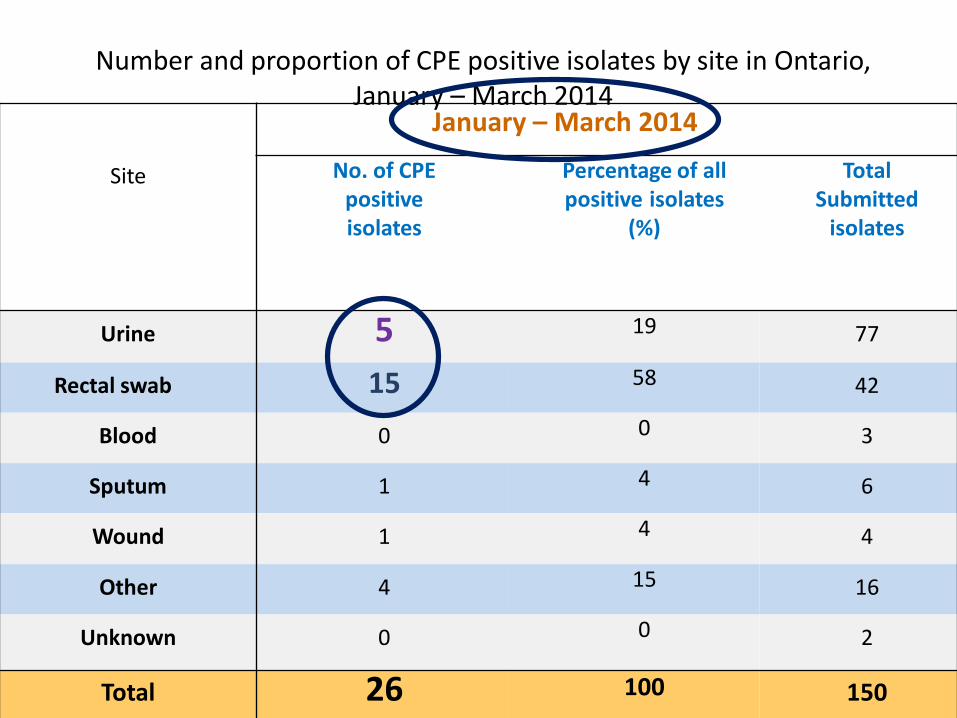
Number and proportion of CPE positive isolates by site in Ontario,January – March 2014
Site
January – March 2014
No. of CPEpositiveisolates
Percentage of allpositive isolates
(%)
TotalSubmitted
isolates
Urine 5 19 77
Rectal swab 15 58 42
Blood 0 0 3
Sputum 1 4 6
Wound 1 4 4
Other 4 15 16
Unknown 0 0 2
Total 26 100 150
The STATS of CPE in Ontario could be misleading
• These numbers are only a snapshot.
• May not be a complete data.
• All important enzymes have been implicated in several Ontario hospitals.
• Data from private lab is also missing.
• Data from March-September 2014 is not tabulated yet.
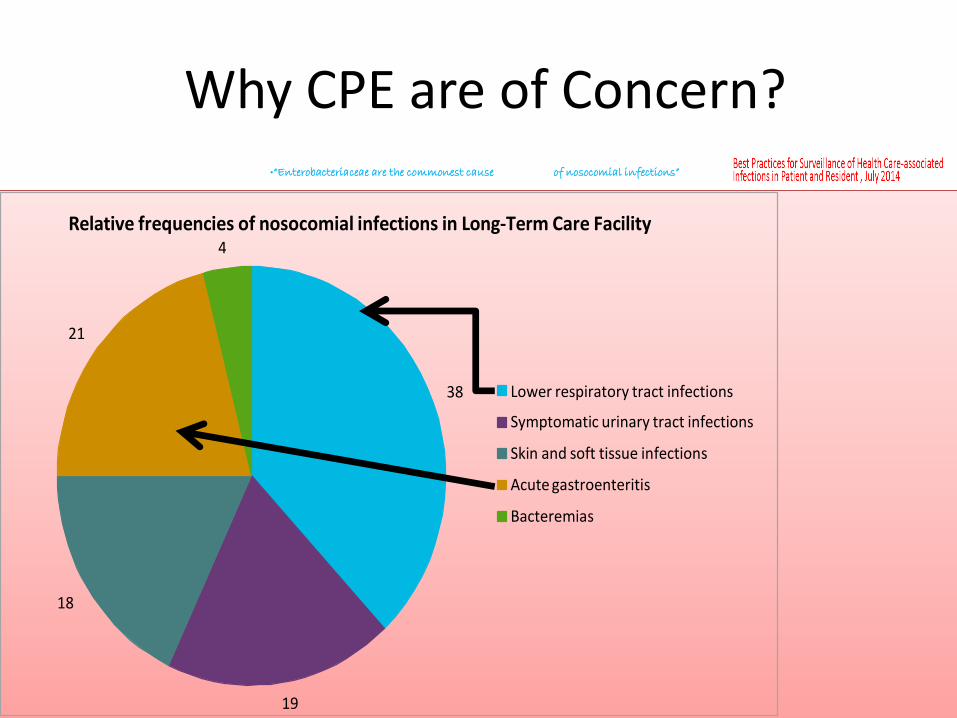
Why CPE are of Concern?•“Enterobacteriaceae are the commonest cause of nosocomial infections”
Relative frequencies of nosocomial infections in Long-Term Care Facility 4
21
38 Lower respiratory tract infections
Symptomatic urinary tract infections
Skin and soft tissue infections
Acute gastroenteritis
Bacteremias
18
19
Why CPE are of Concern?
• Enterobacteriaceae have become resistant to many antibiotics such as, Cephalosporines , Penicillines, Fluroquinolones and Aminoglycosides.
• Now resistant to Carbapenems.
• Panresistant is possible due to mobile plasmids.
• There are no new antibiotics in development that have actively against the resistant gene.
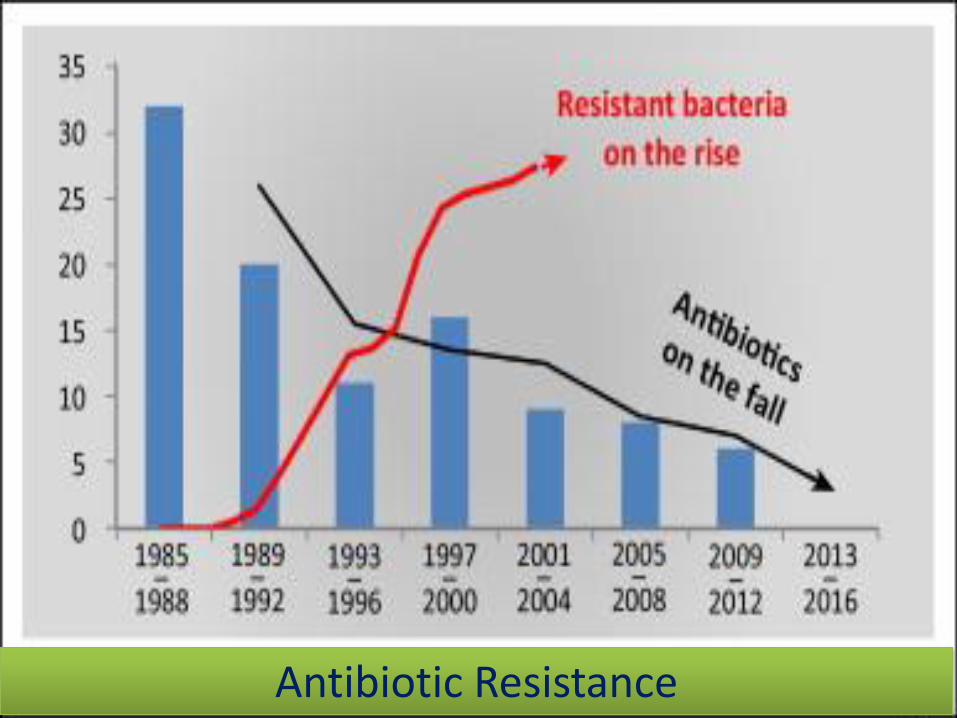
Antibiotic Resistance

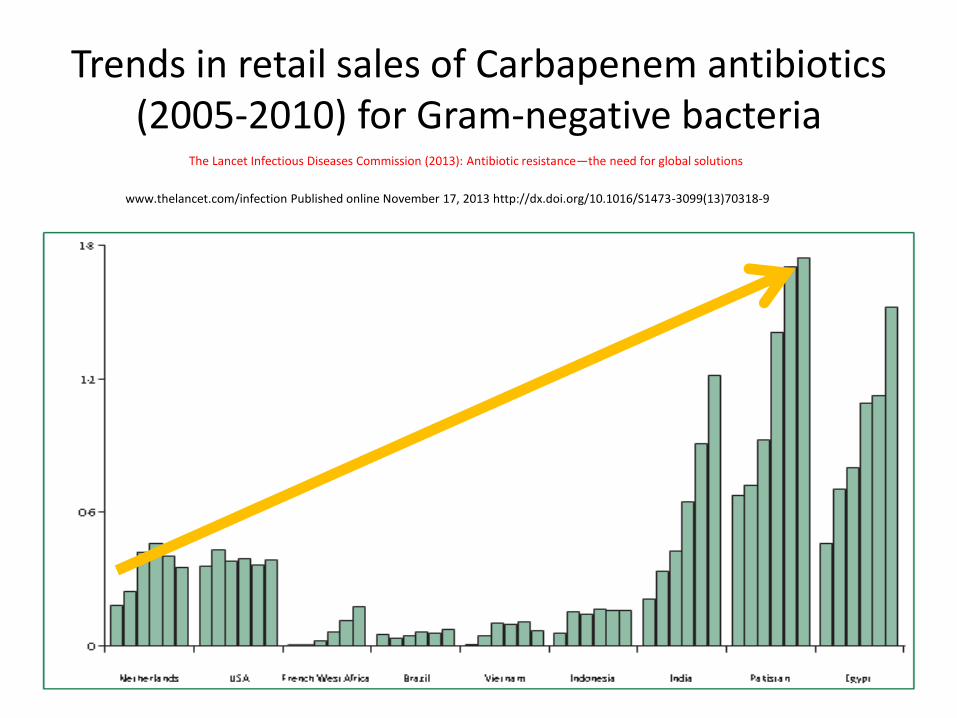
Trends in retail sales of Carbapenem antibiotics (2005-2010) for Gram-negative bacteria
www.thelancet.com/infection Published online November 17, 2013 http://dx.doi.org/10.1016/S1473-3099(13)70318-9
The Lancet Infectious Diseases Commission (2013): Antibiotic resistance—the need for global solutions
More alarming concerns about CPE
• Once colonized CPE may not be eradicated as these organisms are part of the normal gut flora- Resistant Gut Flora.
• The therapeutic options for CPE infections are very limited now.
• Colistin is only option right now. Serious side effects.
• Lab test for Carbapenemases may fail.
• CFR could be 50%
This Superbug may visit your facility too!!
o The Village of Walkerville is receiving its first CPE case (Mr. Brown) from the hospital after rehabilitation.
o The staff at the facility has challenges to handle this situation.
o Which of the following strategies facility can adopt in implementing a surveillance programfor this MDRO?
1) Screen all patients for CPE on admission.
2) Implement routine practices all the time.
3) Placed all colonized or infected patients on contact precautions.
4) Placed all colonized or infected patients on contact precautions.
5) Minimize invasive devices.
6) Communicate results to Healthcare providers.
Circle your Strategies for Surveillance of CPE
What Should You Do About It?
o Understand the Epi Triad:
Host risk factors
Environmental risk factors
o Implement Surveillance:
o Use IPAC interventions:
Before a case is identified
After a case is identified
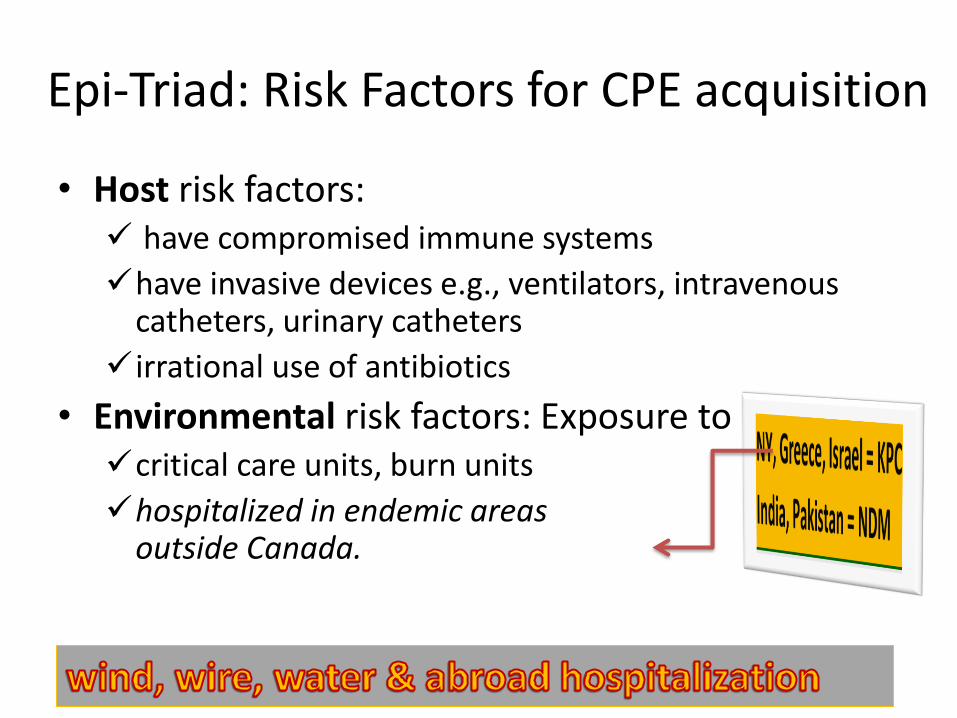
Epi-Triad: Risk Factors for CPE acquisition
• Host risk factors: have compromised immune systems
have invasive devices e.g., ventilators, intravenous catheters, urinary catheters
irrational use of antibiotics
• Environmental risk factors: Exposure tocritical care units, burn units
hospitalized in endemic areas outside Canada.
Epi-Triad: Transmission of CPE
•Transmission is via:
direct contact: person to person
via wound, stool, sputum
indirect contact:
environment surfaces, sinks
Epi-Triad - Interventions
1. Preventing transmission the colonized or infected patient is identified.
2. Preventing transmission the colonized or infected patient is identified.
Interventions a case is identified
• Routine Practices
• Antimicrobial stewardship Program (ASP)
Developing an ASP program in your facilityhttp://www.oahpp.ca/services/antimicrobial-stewardship-program.html
• Appropriate specimen testing, such as:
rectal swab, urine, blood, wound swab
Interventions a case is identified.
(Targeted)Public health notification Routine practices continued + Contact precautionsSignage for visitorsHealthcare worker education CPE screening based on risk factorsMinimize use of invasive devices Environmental sanitation CohortingInter-facility communication
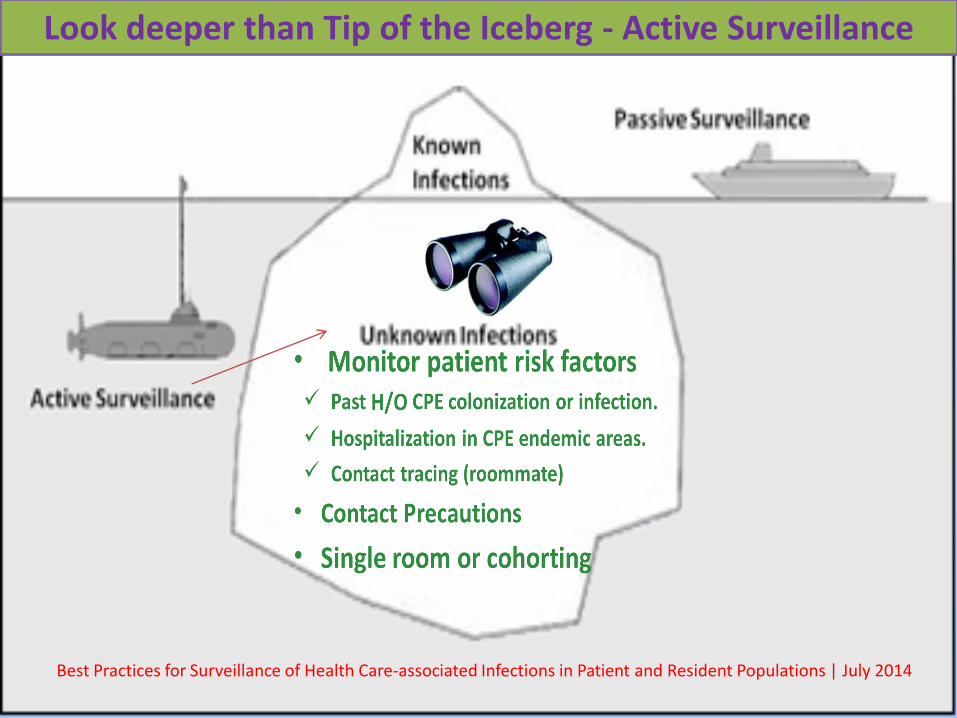
Look deeper than Tip of the Iceberg - Active Surveillance
Best Practices for Surveillance of Health Care-associated Infections in Patient and Resident Populations | July 2014
Active Surveillance for CPE
•Point prevalence screening: Whole unit screening, if a new case is
identified.
•In a CPE outbreak: Absolute cohorting and dedication of
equipment and PH notification.
•Flagging of known CPE carrier and rescreened on readmission.
Decolonization
CPE decolonization is NOT recommended unless to reduce the bio-burden in an uncontrolled
outbreak.
Occupational Health & Safety Requirements
• OH&S in hospitals and LTCH do not requireroutine screening of staff unless there is an epi-link to the transmission of CPE.
• If CPE is acquired due to an occupational exposure, it is reportable to WSIB.
Inter-Facility Communication (info sharing)
• Ensure if patient transferred within the facility that Routine practices are continued.
• Ensure if patient transferred to another facility patient information(CPE) is shared with accepting facility.
Antimicrobial Resistance is a Shared Responsibility
ACT AS A TEAM
CONCLUSION- ARO
• ARO is inevitable, but can be delayed.
• ARO are not restricted to healthcare facilities.
• Inappropriate use of antimicrobial agents and limited research into and development of new agents have helped accelerate antimicrobial resistance.
• Treatment of diseases caused by antimicrobial-resistant organisms takes more time, uses more resources and is more costly.
The Chief Public Health Officer’s Report on the State of Public Health in Canada, 2013; Infectious Disease—The Never-ending Threat, Antimicrobial Resistance—A Shared Responsibility. PHA Canada.
CONCLUSION- ARO
• The WHO has recognized antimicrobial resistance as one of the most serious public health threats to the treatment of
infectious diseases worldwide.
• Managing antimicrobial use is everyone’s responsibility.
• Lets PLAY responsibly!

References • By Roberto G. Melano, David J Farrell, Donald E Low, and Samir N Patel
(2012), Carbapenemase-producing Enterobacteriaceae in Ontario, 2008-2011, Public Health Ontario, Public Health Laboratory – Toronto, Toronto, ON Canada.
• Patrice Nordmann, Thierry Naas, and Laurent Poirel (2011): Global Spread of Carbapenemase- producing Enterobacteriaceae, Emerging Infectious Diseases , www.cdc.gov/eid , Vol. 17, No. 10.
• Guidance for control of Carbapenem-resistant Enterobacteriaceae(CRE):CDC 2012 CRE Toolkit.
• Monnet DL. Update on EARS-NET AMR & HAI activities and workplan[for] 2012. [Presentation] Warsaw 2011 November 23-25 [cited 2012 July 11]. www.EARSnet.europa.eu/en/activities/diseaseprogrammes/ARHAI/Presentations2011Warsaw/ARHAI-networks-meeting_parallel-session-five-1-Dominique-Monnet-AMR-HAI-activities.pdf.130
References
• PIDAC Annex A- screening, testing and surveillance of antibiotic resistant organisms (AROs) in ALL health Care Settings-Feb 2013.
• Routine practices and Additional precautions in ALL HC Settings 3rd edition Nov. 2012, PHO, PIDAC.
• APIC Text of Infection Prevention and Control 3rd edition, 2009
• Carbapenemase-producing Enterobacteriaceae (CPE) Surveillance Report, VOLUME 3, ISSUE 1 (2013 ANNUAL SUMMARY) PUBLISHED IN JUNE 2014.
• The Chief Public Health Officer’s Report on the State of Public Health in Canada, 2013; Infectious Disease—The Never-ending Threat, Antimicrobial Resistance—A Shared Responsibility. PHA Canada.
• Best Practices for Surveillance of Health Care-associated Infections in Patient and Resident Populations | July 2014
References
• Carbapenemase Producing, Enterobacteriaceae (CPE) Surveillance Report,VOLUME 2, ISSUE 1 (OCTOBER 2013)
• Quarterly Carbapenemase Producing Enterobacteriaceae (CPE) Surveillance Report, VOLUME 1, ISSUE 3, December 2012.
• Carbapenemase Producing Enterobacteriaceae (CPE) Surveillance Report, VOLUME 1, ISSUE 4 (2012 ANNUAL SUMMARY)
• Public Health Ontario Laboratories, Carbapenemase Producing Enterobacteriaceae database, extracted by Public Health Ontario [2013/07/02]
• Ramanan Laxminarayan, Adriano Duse, Chand Wattal, et,al; (2013): Antibiotic resistance—the need for global solutions,The Lancet Infectious Diseases Commission. www.thelancet.com/infection Published online November 17, 2013 http://dx.doi.org/10.1016/S1473-3099(13)70318-9








![pc pc 2012 - examenbac.com · NS28 / (aq) (s) (s) (aq) 10 —2 + = ] (aq) i 4(aq) mol. L; 1 + = ' (aq) i (aq) 4(aq) 7m +Cu2+ + 4....*àA.Z = 5.1036 F = 9, 65.104 C.mol- —2](https://img.pdfslide.us/doc/110x75/5b9bedcb09d3f29b498bc24a/pc-pc-2012-ns28-aq-s-s-aq-10-2-aq-i-4aq-mol-l-1-.jpg)