Embed Size (px)
Citation preview

CPC #2: 38 year old woman with HIV/AIDS and altered mental status
October 9, 2007

Lungs
Combined weight 2,200 gm (normal 685-1,050) Most of weight increase due to pulmonary edema Multiple discrete nodules with necrotic centers Bronchopneumonia CMV infection

Pulmonary edema

Necrotizing nodules – no AFB or fungi ID’d
CD20 – B-cells
CD3 – T-cells

Bronchopneumonia

Bronchopneumonia – and CMV infection

CMV in alveoli and around necrotizing masses

Disseminated CMV
Kidney Adrenal Pancreas

Disseminated CMV
Spleen Ovary

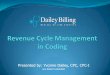
Brain: multiple poorly defined massesRight frontal lobe
Left striatum *
Right striatum *
Left insula
Left cerebellum

Primary CNS lymphoma

Primary CNS lymphoma
Tumor cells in vessel walls Diffuse parenchymal invasion

Primary CNS lymphoma - EBV
CD20 – B-cells CD3 – T-cells EBV

Cause of death
Part I
a) B-cell lymphoma, brain
b) Acquired immunodeficiency syndrome
Part II
a) Disseminated CMV infection

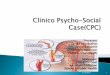
HIV neuroinvasion: “Trojan Horse hypothesis”
Viral entrance into CNSInfected monocytes enter, differentiate into perivascular
macrophagesInfected CD4+ T cellsDirect entrance of virusTranscytosis of virus across endothelial cells
Productive infection of macrophages and microgliaRestricted infection of astrocytesInfection of oligodendrocytes and especially neurons is
questionable
Ghafouri et al. Retrovirology 2006; 3:28

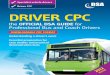
CNS infections in AIDS Fungi
Cryptococcus AspergillusCoccidioides
http://www.vfce.arizona.edu/VFCE%20OLD/jpg/2330034.jpg

CNS infections in AIDS
FungiCryptococcus
Aspergillus
Coccidioides
ParasitesToxoplasma

CNS infections in AIDS Fungi
Cryptococcus AspergillusCoccidioides
ParasitesToxoplasma
Viruses (encephalitis)Cytomegalovirus (CMV)HIV
Ellison & Love: Neuropathology 2e © 2004 Elsevier Ltd.

CNS infections in AIDS Fungi
Cryptococcus AspergillusCoccidioides
ParasitesToxoplasma
Viruses (encephalitis)Cytomegalovirus (CMV)HIV
Viruses (other pathology)JC virus (PML, demyelination)Epstein-Barr virus (EBV) - lymphoma

Primary CNS lymphoma (PCNSL)
More frequent in both immunocompromised and immunocompetent patients (especially elderly) over last 20 years6-20% of AIDS patients
EBV implicated in most immunocompromised and some immunocompetent individuals (nearly all AIDS patients)
Usually diffuse large B-cell tumors Occur anywhere in brain
Incidence proportional to volume (i.e., most common in frontal lobe)
Often multifocal in AIDS patients
Symptoms reflect location

Primary CNS lymphoma (PCNSL)
Imaging (without AIDS): homogeneous enhancement Imaging (with AIDS): “ring-enhancing”, often multifocal Histology:
Solid sheets of tumor cells (often necrotic) blending into less cellular zones
Angiocentric and angioinvasive
Positive for B-cell markers, EBV (immunocompromised)
Treatment: radiation and / or chemotherapy Prognosis:
Immunocompetent: median survival 18 months
Immunocompromised: median survival 4 months

References
Burger et al. Surgical Pathology of the Nervous System and Its Coverings. Fourth Edition. 2002. Churchill Livingston.
Ellison et al. Neuropathology. A reference text of CNS pathology. Second Edition. 2004.
http://www.emedicine.com/neuro/topic519.htm