Embed Size (px)
DESCRIPTION
Rationale Single-agent Gemcitabine maintenance results in significantly longer time to progression (TTP) compared to BSC (6.6 mos. vs 5.0 mos., P
Citation preview

C.P. Belani1, D.M. Waterhouse2, H.H. Ghazal3, S. Ramalingam 4 , J.M. Waples5, R.E. Bordoni6, G.A. Reznikoff7, C.P. Curran8, R. H. Greenberg9
1Penn State Hershey Cancer Institute, Hershey, PA, USA; 2Oncology Hematology Care, Cincinnati, OH; 3Kentucky Cancer Clinic, Hazard, KY);
4Emory University Winship Cancer Institute, Atlanta, GA, 5 Clearview Cancer Institute, Huntsville, AL; 6Georgia Cancer Specialists, Atlanta, GA; 7Medical Specialists of Fairfield,
Fairfield, CT; 8 Palmetto Hematology Oncology, Spartanburg, SC; 9The Center for Cancer and Hematologic Disease, Cherry Hill,
NJ
Randomized Trial of Gemcitabine-Carboplatin (G-Cb) Therapy Followed by Gemcitabine (G)
Maintenance or Best Supportive Care (BSC) in Advanced NSCLC
Abstract # 7507

Maintenance therapy represents a useful strategy to improve patient outcomes in advanced stage NSCLC
Recent studies of maintenance therapy (sequential, consolidation, ‘switch’ to a new agent), immediately following first-line therapy, have demonstrated a statistically significant survival benefit
Maintenance Therapy in Advanced NSCLC

Rationale
Single-agent Gemcitabine maintenance results in significantly longer time to progression (TTP) compared to BSC (6.6 mos. vs 5.0 mos., P<0.001) (Brodowicz et al, Lung Cancer, 2006; 52:155-163)
Given its ease of administration and favorable
safety profile, we evaluated maintenance Gemcitabine + BSC vs. BSC in non-progressors following 4 cycles of Gemcitabine/Carboplatin (G-Cb) in patients with advanced stage IIIB/IV NSCLC

Arm B
Gemcitabine 1000 mg/m2 d 1,8
q 21 days+
Best supportive care (BSC)
Arm A
Gemcitabine 1000 mg/m2 d 1,8
Carboplatin AUC 5 d 1q 21 days X 4 cycles
PD
Off study
CRPRSD
Study Design
1:1 Randomization Primary Endpoint =
OS
Chemonaïve Stage IIIB/IV NSCLC
Randomization factors: • PS• stage• best tumor response
Best supportive care (BSC)

BSC was the same in both arms and was defined as treatment given with the intent to maximize QOL without a specific antineoplastic regimen• Acceptable therapies included were:
– Treatment with antibiotics, analgesics, antimetics, thoracentesis pleurodesis, blood transfusions, nutritional support (enteral or parenteral)
BSC specifically excluded:• Surgery, immunotherapy, radiotherapy (exception of palliative
RT), anticancer hormonal therapy, and systemic chemotherapy
Best Supportive Care
Patients were evaluated every 9 wks (or three cycles) on both GEM+BSC and BSC alone arms for tumor
assessment

Histologic or cytologic diagnosis of stage IIIB with pleural effusion and/or positive supraclavicular nodes or stage IV NSCLC
Age ≥ 18 years ECOG performance status of 0 - 2 Adequate renal, hepatic and bone marrow function Patients with asymptomatic / treated & controlled brain
metastases were allowed Presence of measurable disease No prior chemotherapy for NSCLC Signed informed consent
Eligibility Criteria

Primary Objective Overall survival comparing Gemcitabine
maintenance +BSC vs. BSC following randomization
Secondary Objectives Objective response rate Progression-free survival following
randomization Safety and tolerability
Objectives

Sample size of 600 patients for initial therapy with G-Cb was planned to allow 332 patients to be randomized to maintenance Gemcitabine + BSC vs. BSC (assuming 45% progression to initial therapy) based on 80% power using two-sided alpha level of 0.05
Overall survival (OS) analysis planned after 238 events to achieve full power
Assumed hazard ratio of 0.69 comparing Gemcitabine + BSC vs. BSC on OS
Planned patient accrual time was 18 months
Statistical Design

Study Accrual
Patient enrollment was from January 2002 to August 2007
519 patients were enrolled to G-Cb phase of trial (87% of plan)
255 patients were randomized to maintenance Gemcitabine + BSC vs. BSC following initial treatment
Study was closed in September 2008 due to slow accrual
Final Analysis at 179 events amongst 255 randomized patients

Baseline CharacteristicsInitial Phase
Gemcitabine/Carboplatin(G-Cb)
Initial PhaseN=519
Median age, years 66.6Age ≥65 years /<65 years, % 57/42
Stage IIIB/IV disease, % 15/85Male/Female, % 63/37Caucasian/AA/Other, % 84/10/6ECOG PS 0/1/2, % 0/36/64

Gemcitabine/Carboplatin
(G-Cb)Initial Phase
N=519
Response rate (CR+PR) 28%Complete response 1%Partial response 27%Stable disease 37%Progressive disease 9%Unknown/not done 26%
Best Tumor Response to Therapy
Initial Phase

Gemcitabine/Carboplatin(G-Cb) N=519
No. patients treated 518Median no. cycles (range) 4 (1-4)Dose reductions 32 %Discontinuations due to drug-related toxicities 5%
Dose intensity 92% for G89% for Cb
Study TreatmentInitial Phase

Maintenance PhaseGEM
N=128%
BSCN=127
%Median age, years 67.2 67.5Age ≥65 years /<65 years 61/39 59/41
Stage IIIB/IV disease 22/78 9/91Male/Female 60/40 67/33Caucasian/AA/Other 83/13/4 88/6/6ECOG PS 0/1/2/3 0/44/52/4 0/43/54/4
Baseline CharacteristicsMaintenance Phase

Best Tumor Response to Therapy
Maintenance Phase
Maintenance Phase GEMN=128
BSCN=127
Response rate (CR+PR) 28% 6 %Complete response 5 % 0
Partial response 23 % 6 %
Stable disease 40 % 25 %
Progressive disease 9 % 17 %Unknown/not done 23 % 53 %

Study TreatmentMaintenance Phase
Maintenance Phase GEMN=112
BSCN=127
No. patients treated 112 -
Median no. cycles (range) 4 (1-9) - Dose reductions 26 % - Discontinuations due to drug-related toxicities 6 % -
Patients completing ≥6 cycles 31 % - Patients completing 9 cycles 19 % -
Dose intensity 91 % -

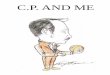
Overall Survival (Intent-to-treat Population)
Overall Survival (months)0 6 12 18 24 30 36 42 48 54 60
1.00.90.80.70.60.50.40.30.20.10.0
Gemcitabine 8.0 mos.
BSC 9.3 mos.
HR=0.97 (95% CI:0.72, 1.30)P =0.838

Progression-free Survival (Intent-to-treat Population)
Gemcitabine 7.4 months
BSC 7.7 months
HR=1.09 (95% CI:0.81, 1.45)P =0.575
Progression-free Survival (months)0 6 12 18 24 30 36 42 48 54 60
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0

Cox Regression Analysis
Variable Reference level
Hazard Ratio* 95% CI P value
PS ≥2 PS=1 1.50 1.10, 2.03 0.009
Male Female 1.59 1.15, 2.18 0.005
Significant variables in final model
*Modeling hazard ratio associated with worsened survival

Toxicities
Gemcitabine(N=112)
%
BSC(N=127)
%Grade 3-4 Grade 3-4
Neutropenia‡ 15 2Anemia‡ 9 2Thrombocytopenia 9 4Fatigue 5 2Nausea 0 <1Vomiting 0 <1
‡P <0.05 for grade 3/4 rates of neutropenia, anemia
Treatment-related Toxicities

Post-study TherapyGemcitabine
(N=128)%
BSC (N=127)
%Patients with known post-study therapy 16 17Most common post-study therapies Pemetrexed 9 10Bevacizumab 2 2Carboplatin 2 6Gemcitabine 2 3Docetaxel 3 6Vinorelbine 2 2Paclitaxel 2 2
Systemic Post-study Therapy

Lack of sub-histology information•Most of the patients categorized as NSCLC
High proportion of patients with PS 2 Low post-study treatment-rate
Study Limitations

This study failed to show a survival benefit for maintenance Gemcitabine in non-progressors following standard treatment of G-Cb for patients with advanced NSCLC
• Nearly two thirds of patients were ECOG PS 2 at study entry
Gemcitabine in the maintenance setting was well tolerated
Few patients received post-study therapy likely due to poor PS
Conclusions

• The authors would like to thank:– All the patients and their families– The investigators and the staff at each
participating center– Pharmatech and their research staff
Acknowledgements