Embed Size (px)
Citation preview
COVID Monitor Quick Reference Guide INTAKE ASSESSMENT (Health Direct Staff)
Please use the following guidance when completing an Intake Assessment on COVID Monitor if you are a Monash Health or Health Direct employee assisting with COVID Positive Care Pathways. Please see the COVID Monitor Login Quick Reference Guide if you need assistance to login.
Patient Allocation Patients are allocated to Monash Health twice daily from SEPHU, before 9am and before 3pm. Patients are allocated based on their home postcode. At times patients from outside the Monash Health catchment will be allocated to the Monash pathway (for example if they are complex paediatric patients, if they are maternity patients or if they are Monash Health employees). So you will see some patients with an address outside the Monash catchment.
As soon as patients are allocated to Monash Health, they will receive a short survey with 4 questions – vaccination status, symptom start date, pregnancy status (if applicable) and if they have comorbidities. They then get a symptom survey. The answers provided allow us to prioritise the Intake Assessment (i.e. who we need to call first).
Intake Assessment We aim for all patients coming into the pathway to have an Intake Assessment. However, at times of very
high demand, there may be some patients that do not receive a personal phone call, but these patients will
be well (no or mild symptoms) and with no co-morbidities or social complexity, so unlikely to require
medical care or referral for social assistance.
The aim of the Intake Assessment is to stream patients into a Care Pathway, that defines the type of care
they will receive and who will provide that care. Details are in the below table:
Care Pathway Care Provider Care Provided
Community
Health /
Primary Care
LOW
General Practitioner
Community Health Service
Telehealth GP appointments
Symptom monitoring
Monash Health
MEDIUM
Complex Care
Plus MC@H for paeds
Plus Maternal Fetal Medicine
(MFM) for maternity
Symptom monitoring
Telehealth from medical or nursing
Home visits (as required)
Monash Health
HIGH
Inpatient Unit Inpatient care, usually at a Monash Health facility
It is the assessors role to complete the Intake Assessment for their allocated patients and decide which Care
Pathway the patient should be steamed to. There is an algorithm behind the assessment on COVID Monitor,
however clinical reasoning should be applied in addition to ensure the patient receives the right care from
the right provider, and that health service resources are reserved for the patients who need it most.
Pending Assessment List Patients who require an Intake Assessment will appear on the Pending Assessment list, found by clicking on
the 3 horizontal bars in the top left of the screen.
COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 2
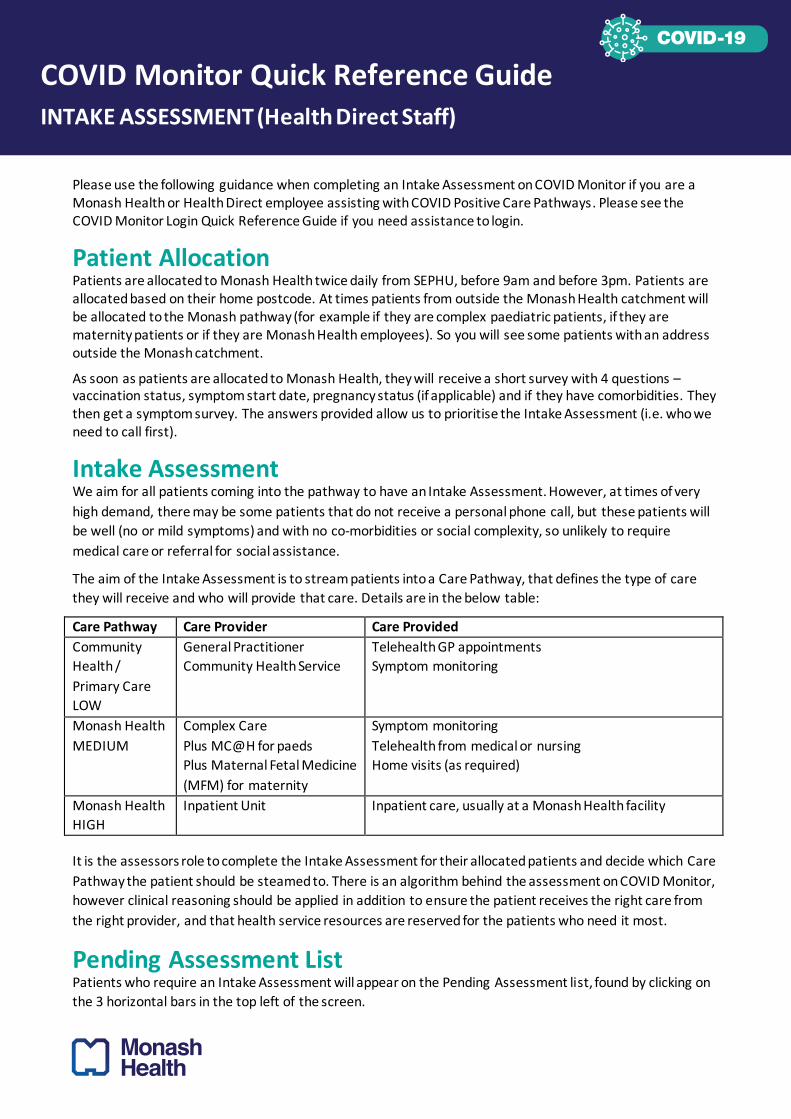
Select Pending Assessment.
The Pending Assessment list looks like this:
Each colum heading is explain in the below table:
COLUMN HEADING FUNCTION
Priority Gives ability to sort the list by priority (criteria on next page)
Type P1, P2 etc in the box below the column heading to sort the list by priority
TREVI ID This is the unique patient identifier
UR This is the Monash UR number that most patients will not require
First name / Surname
/ DOB / Address /
Suburb
Self-explanatory – can be edited in the Patient Details screen if incorrect
Model of Care Standard for majority of patients
If patient is marked for Monash Children’s at Home, will say MC@H – Central
Bayside should not complete intake for these patients
Paediatric / Maternity Yes/No – enables filtering for paediatric and maternity patients
Last Obs Date When the patient last entered their observations
Symptomatic NA/Normal/Mild/Moderate/Severe – enables filtering for symptom severity by
typing the severity in the box below the column heading
SOB / Chest Pain Key symptoms that patient will have entered themselves
Self-symptom Onset /
TREVI Symptom Onset
These will help identify the date on which a patient can be discharged from the
pathway (Day 14 in most cases) – this cannot be edited in COVID Monitor
Day of Illness This is dictated by the date of symptom onset or their first positive swab date – you
cannot edit it
History Risk If the patients have answered YES to the pre-intake comorbidities question, it
means they have one or more of: respiratory disease, diabetes,
immunocompromised, cancer treatment in last 6 months, obesity (it is a Yes/No
COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 3
questions, so specific detail of which one will be captured in your assessment)
Vax Status Vaccination status – Not yet, one dose, two doses. Specific detail will be captured in
your assessment.
Clinical Pathway /
Pathway Severity
All new patients will default to Community and Low. As part of your intake
assessment, you may change the pathway to Monash Health and you may upgrade
severity to medium or high, depending on the outcome of your assessment.
Day of Allocatoin The date upon which the patient was allocated to the COVID Care Pathway
Assessment Should be NO for all cases on this list.
Discharged Should be NO for all cases on this list.
Deceased Hopefully NO for all cases on this list but if the patient is deceased you can note this
during your assessment.
Each assessor will have a pre-defined list of patients on which to complete Intake Assessment.
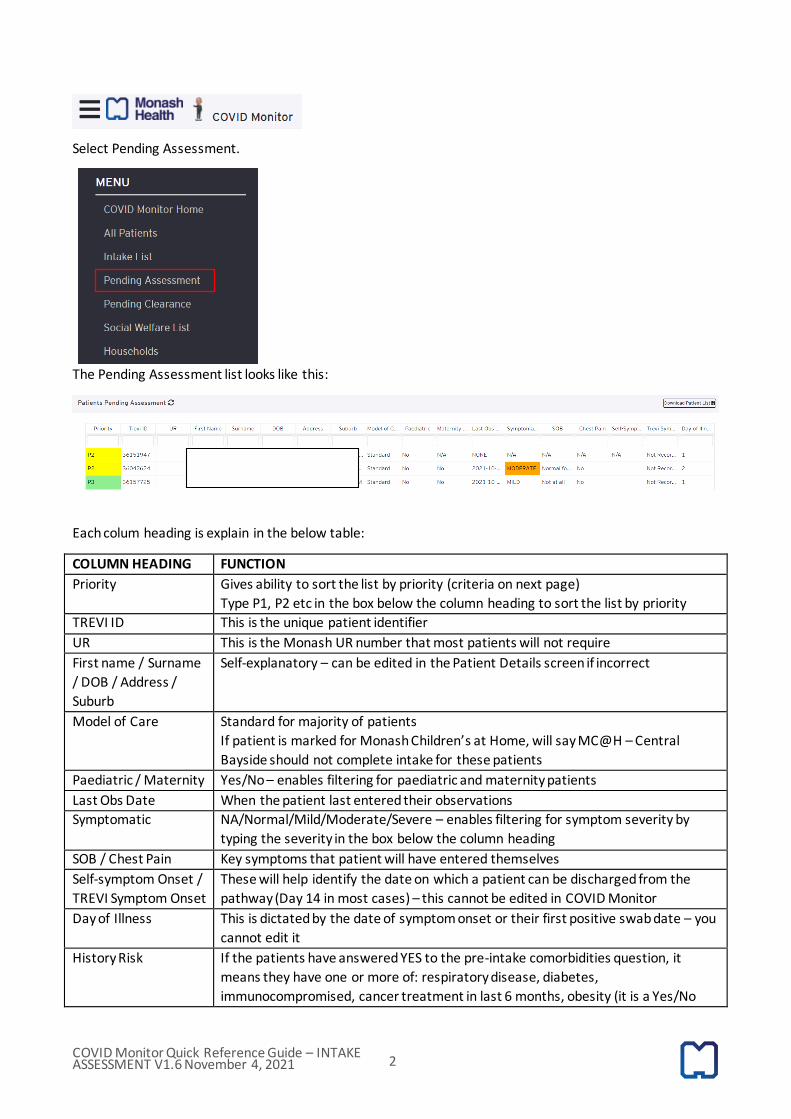
Intake Assessment Priority Criteria P1-4 is automatically set in the Pending Assessment list based on the criteria in the below diagram:
P1 cases should be assessed ideally within 4 hours and P2 should be assessed within 24 hours.
Within the P1 category, sub-priority should be given as follows: P1 (severe symptoms), P1 (moderate
symptoms with comorbidities), P1 (pregnant, no severe or moderate symptoms), P1 (very old, very young),
P1 (all remaining).
Within the P2 category, sub-priority should be given as follows: P2 (moderate symptoms), P2 (adults who
have not responded), P2 (adults or unvaccinated children overe 12 years with comorbidities and
mild/normal symptoms).
The prioritisation is dynamic, so patients will move between levels depending on the symptoms they enter.
Patient Details To perform your assessment you need to click on a patient in the Pending Assessment list and this will take
you to the Patient Details screen. This is where you complete you Intake Assessment. Please check that the

COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 4
patient hasn’t already had an Intake Assessment completed by scrolling to the bottom of the screen. If this
documentation appears, they have already been assessed:
The patient details appear as per below.
There are a number of buttons on the right side of the screen:
COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 5
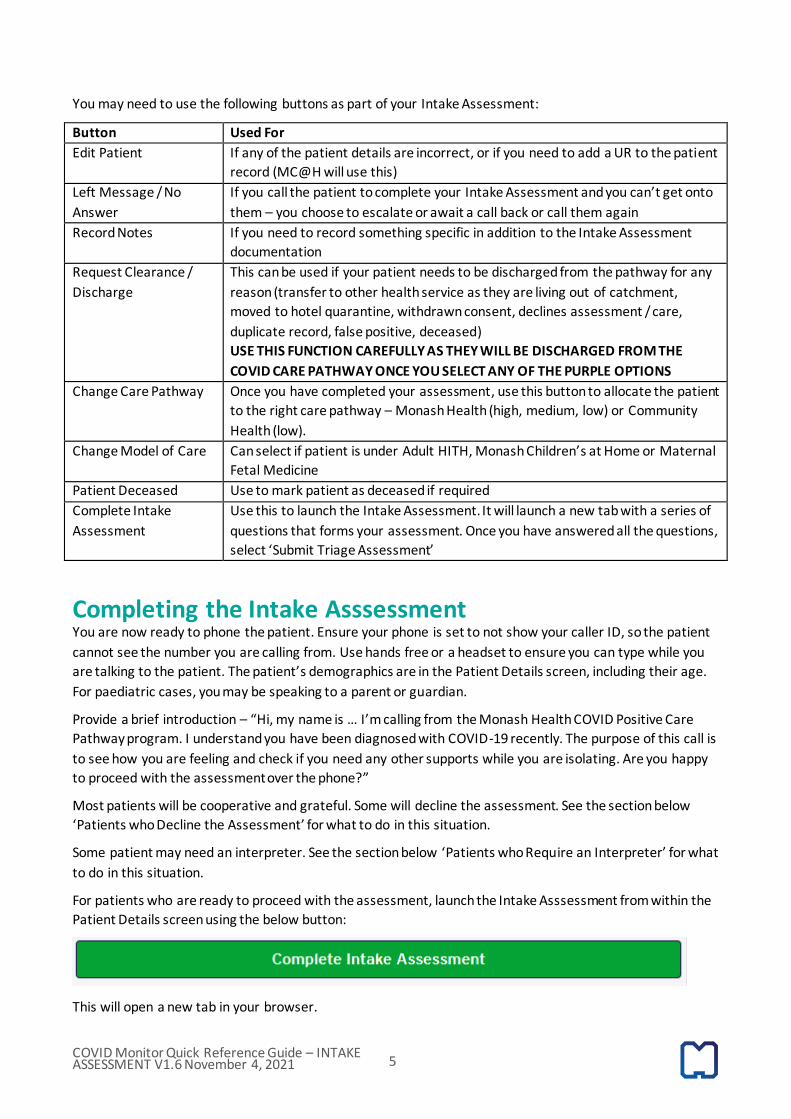
You may need to use the following buttons as part of your Intake Assessment:
Button Used For
Edit Patient If any of the patient details are incorrect, or if you need to add a UR to the patient
record (MC@H will use this)
Left Message / No
Answer
If you call the patient to complete your Intake Assessment and you can’t get onto
them – you choose to escalate or await a call back or call them again
Record Notes If you need to record something specific in addition to the Intake Assessment
documentation
Request Clearance /
Discharge
This can be used if your patient needs to be discharged from the pathway for any
reason (transfer to other health service as they are living out of catchment,
moved to hotel quarantine, withdrawn consent, declines assessment / care,
duplicate record, false positive, deceased)
USE THIS FUNCTION CAREFULLY AS THEY WILL BE DISCHARGED FROM THE
COVID CARE PATHWAY ONCE YOU SELECT ANY OF THE PURPLE OPTIONS
Change Care Pathway Once you have completed your assessment, use this button to allocate the patient
to the right care pathway – Monash Health (high, medium, low) or Community
Health (low).
Change Model of Care Can select if patient is under Adult HITH, Monash Children’s at Home or Maternal
Fetal Medicine
Patient Deceased Use to mark patient as deceased if required
Complete Intake
Assessment
Use this to launch the Intake Assessment. It will launch a new tab with a series of
questions that forms your assessment. Once you have answered all the questions,
select ‘Submit Triage Assessment’
Completing the Intake Asssessment You are now ready to phone the patient. Ensure your phone is set to not show your caller ID, so the patient
cannot see the number you are calling from. Use hands free or a headset to ensure you can type while you
are talking to the patient. The patient’s demographics are in the Patient Details screen, including their age.
For paediatric cases, you may be speaking to a parent or guardian.
Provide a brief introduction – “Hi, my name is … I’m calling from the Monash Health COVID Positive Care
Pathway program. I understand you have been diagnosed with COVID-19 recently. The purpose of this call is
to see how you are feeling and check if you need any other supports while you are isolating. Are you happy
to proceed with the assessment over the phone?”
Most patients will be cooperative and grateful. Some will decline the assessment. See the section below
‘Patients who Decline the Assessment’ for what to do in this situation.
Some patient may need an interpreter. See the section below ‘Patients who Require an Interpreter’ for what
to do in this situation.
For patients who are ready to proceed with the assessment, launch the Intake Asssessment from within the
Patient Details screen using the below button:
This will open a new tab in your browser.
COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 6
Complete all questions in the Patient Information, Patient History and Intake Screening Questions sections .
No questions are mandatory but please fill in as much information as you can and use the free text fields to
add information not captured elsewhere.
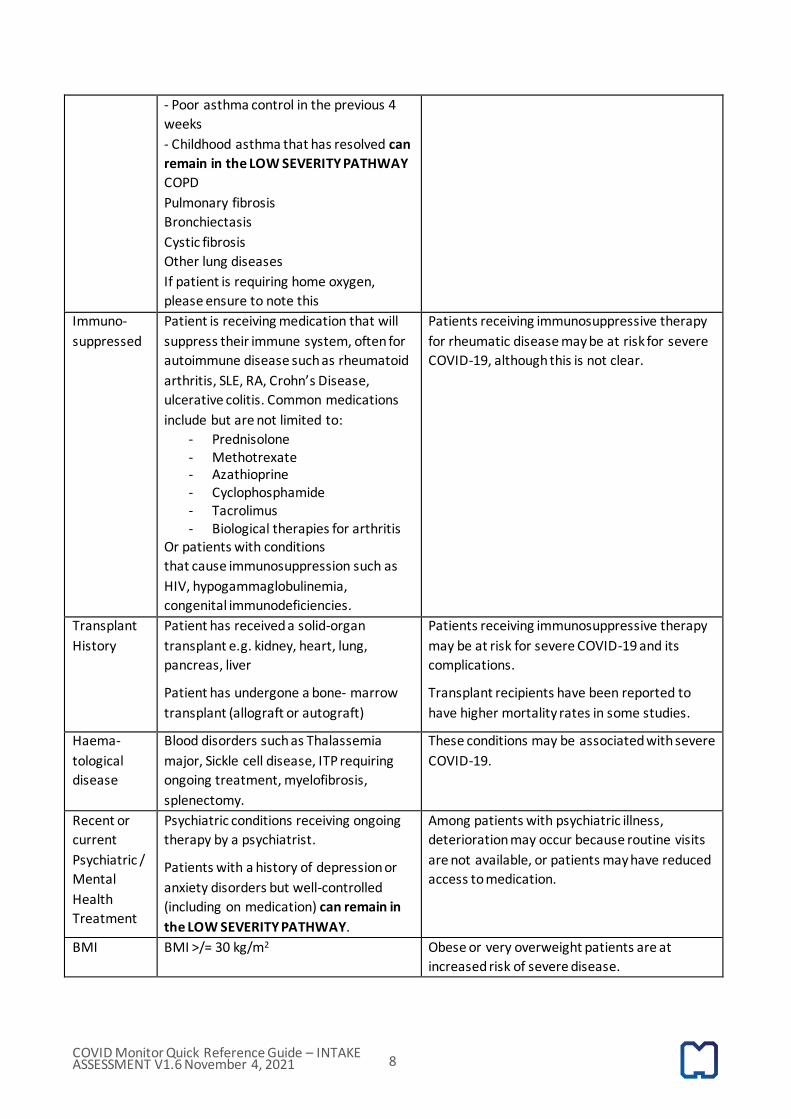
Patient Information Please check the patient information on the Patient Details screen, particularly their home address, to
ensure we have up to date details for the patient. Please complete all sections in the Patient Information,
especially the Next of Kin details so we have an alternative contact number in case we cannot contact the
patient directly. Update any general demographics via the Edit Patient button.
Once you launch the Intake Assessment, ensure you select the correct screening organisation and put your
name in correctly.
Fill in all the fields in the Patient Information section, particularly the Next of Kin details.
Note that all patients who are Refugees or Aboriginal / Torres Strait Islanders should be in the MEDIUM
SEVERITY PATHWAY.
Patient History The table below explains the relevance of the Patient History questions for adult patients. The following co-
morbidities are risk-factors for severe COVID-19. Unless otherwise specified, patients who have one of the
following comorbidities should be in the MEDIUM SEVERITY PATHWAY.
History
Question
Definition Explanation
Pregnant Pregnancy confirmed by biochemical test
or ultrasound
Pregnant women are at increased risk of severe
disease and may have increased frequency of
preterm birth or Caesarean delivery.
Age Age > 55 years Older age is associated with severe disease and
increased mortality.
Cardiac
Disease
Previous Acute Myocardial Infarct
History of angina
History of cardiac failure
Cardiomyopathy
Ischaemic heart disease (+/-
CABG/stents)
Patients with cardiovascular disease are at
increased risk of a poor prognosis.
Patients with severe infection may require
higher cardiac output, which may not be met in
patients with pre-existing cardiac disease.
In some patients, COVID-19 may result in
myocardial injury.
High Blood History of hypertension. Patients Hypertension may be a risk factor for severe

COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 7
Pressure requiring a single antihypertensive
medication with a well-controlled BP can
remain in the LOW SEVERITY PATHWAY
COVID-19.
Cancer Patients with a diagnosis of active solid
tumour cancer (excluding isolated skin
cancers) OR haematological cancer e.g.
lymphoma, leukemia, myeloma.
They may be currently receiving
chemotherapy, radiotherapy or other
treatments, or recently completed
treatment in the last 6 months.
Patients that have been treated for
cancer more than 6 months ago and now
completely recovered can remain in the
LOW SEVERITY PATHWAY
Patients with hematologic and non-hematologic
malignancy may be at increased risk of severe
COVID-19.
Liver Failure Liver failure
Cirrhosis
Hepatitis B or C without liver disease can
remain in the LOW SEVERITY PATHWAY
Patients with liver disease may be at higher risk
of severe COVID-19.
Patients with cirrhosis may have a higher risk of
mortality.
Diabetes Patients with Type 2 Diabetes Mellitus on
oral hypoglycaemic agents and/or
receiving insulin therapy
Diet controlled Type 2 Diabetes
Patients with Type 1 DM
Patients with Type 2 diabetes are more likely to
have serious complications, more ICU
admissions and have higher mortality rates
from COVID-19.
There is little data to inform whether poor
glycaemic control prior to COVID-19 infection
impacts on the risk of severe infection.
Patients with Type 1 DM may be at higher risk
of severe COVID-19.
Renal Failure Patient with chronic kidney disease:
eGFR<30 mls/min if known, or currently
under review by a kidney specialist at
least twice a year.
Patients with end stage kidney disease
receiving haemodialysis or peritoneal
dialysis.
Patients with chronic kidney disease are at
increased risk of severe COVID-19.
Patients receiving haemodialysis at an
outpatient facility will require specialised
infection control measures when attending
outpatient haemodialysis.
Respiratory
Disease
Asthma
- Requiring blue puffer or reliever
medication (such as Ventolin, Asmol,
Airomir, Apo-Salbutamol or Bricanyl)
multiple times per week
- Asthma symptoms which wake them up
at night more than once/week
Chronic lung disease has been associated with
severe COVID-19.
COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 8
- Poor asthma control in the previous 4
weeks
- Childhood asthma that has resolved can
remain in the LOW SEVERITY PATHWAY
COPD
Pulmonary fibrosis
Bronchiectasis
Cystic fibrosis
Other lung diseases
If patient is requiring home oxygen,
please ensure to note this
Immuno-
suppressed
Patient is receiving medication that will
suppress their immune system, often for
autoimmune disease such as rheumatoid
arthritis, SLE, RA, Crohn’s Disease,
ulcerative colitis. Common medications
include but are not limited to:
- Prednisolone - Methotrexate - Azathioprine - Cyclophosphamide - Tacrolimus - Biological therapies for arthritis
Or patients with conditions
that cause immunosuppression such as
HIV, hypogammaglobulinemia,
congenital immunodeficiencies.
Patients receiving immunosuppressive therapy
for rheumatic disease may be at risk for severe
COVID-19, although this is not clear.
Transplant
History
Patient has received a solid-organ
transplant e.g. kidney, heart, lung,
pancreas, liver
Patient has undergone a bone‐ marrow
transplant (allograft or autograft)
Patients receiving immunosuppressive therapy
may be at risk for severe COVID-19 and its
complications.
Transplant recipients have been reported to
have higher mortality rates in some studies.
Haema-
tological
disease
Blood disorders such as Thalassemia
major, Sickle cell disease, ITP requiring
ongoing treatment, myelofibrosis,
splenectomy.
These conditions may be associated with severe
COVID-19.
Recent or
current
Psychiatric /
Mental
Health
Treatment
Psychiatric conditions receiving ongoing
therapy by a psychiatrist.
Patients with a history of depression or
anxiety disorders but well-controlled
(including on medication) can remain in
the LOW SEVERITY PATHWAY.
Among patients with psychiatric illness,
deterioration may occur because routine visits
are not available, or patients may have reduced
access to medication.
BMI BMI >/= 30 kg/m2 Obese or very overweight patients are at
increased risk of severe disease.

COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 9
Vaccination Status A patient’s vaccination status has been incorporated into the risk algorithm in COVID Monitor to determine
their risk of severe disease. A patient must be 14 days post their second dose of vaccination to be considered
fully vaccinated. Some patients remain at high risk of severe disease despite being fully vaccinated.
Vaccination status Clinical Pathway
Less than 75yo:
>14 days post 2nd dose
These patients will automatically be in the LOW SEVERITY PATHWAY
UNLESS they have any of the following conditions, in which case they will
remain in the Medium Pathway regardless of vaccination status:
- Pregnancy - Respiratory disease - Immunosuppressed (as defined in Table 1) - Renal replacement therapy - BMI >/= 30 mg/kg2 - Diabetes mellitus
Older than 75yo:
>14 days post 2nd dose
Patients > 75yo will remain in the MEDIUM SEVERITY PATHWAY
regardless of vaccination status
Intake Screening Questions The Intake Screening questions include both physical symptoms and social/welfare questions. Please answer
all questions to ensure a complete set of data.
Paediatric Patients The Intake Assessment is modified automatically for all patients less than 18 years of age. Questions are
phrased for a parent/carer to answer the questions about the child, however if the child is a teenager and
able to answer the questions for themselves, the questions can be asked directly to the patient.
The following table indicates which clinical pathway is suitable for paediatric patients based on age,
vaccination status, symptoms and comorbidities.
LOW SEVERITY MEDIUM SEVERITY HIGH SEVERITY
Age >1 month
(corrected)
<1 month (corrected)
If febrile, high severity
Any
Vaccination
status
Any Any Any
Symptoms Asymptomatic
Normal or mild
work of breathing,
OR
Normal or mildly
reduced feeding or
hydration OR mild
gastro symptoms
Moderate symptoms
Increased work of breathing OR
Poor feeding and hydration (~50% of
normal but not requiring NGIV fluids)
OR
Multiple episdoes of gastro
symptoms AND
Normal conscious state
Moderate to severe work of
breathing OR
Febrile neonate (<1 month
corrected)
Very poor feeding and
hydration (<50% of normal)
OR drowsy/abnormal
conscious state OR
persistent/severe chest pain
Kawasaki’s Disease/PIMS-TS
symptoms (rash with fever)

COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 10
Comorbidities Nil Immunosuppression
Severe/complex medical, cardiac,
respiratory or neurodevelopmental
chronic disease
Significant disability
Extreme obesity (>95 percentile)
Afebrile neonates (<1 month
corrected)
Pregnancy (maternity pathway)
Any
Social /
Welfare
Out of Home Care
The algorithm will recommend the correct pathway for the patients based on the answers to the Patient
History and the Screening questions. Most children should remain in the LOW SEVERITY PATHWAY. From an
age perspective, only babies less than one month in age will routinely be referred to the MEDIUM SEVERITY
PATHWAY (i.e. Monash Children’s at Home).
Contact details for paediatric escalations are below:
Service Reason for Contact Contact Details
Paediatrician on call Urgent medical escalation 0487 019 649 (24 hours, 7 days)
Monash Children’s at Home To advise of medium severity
case or to confirm eligibility
for medium pathway
0414 427 371 (0730-1930)
When asking if parents need help and if there is anyone that could help them, please specify “If you are too
unwell to care for your child”. Please record the name and contact phone number of the adult able to
provide care in the event of parents being too unwell in the ‘Other Details’ text box at the end of the intake
assessment. If no contingency carer is available please refer to the Family Finding service – see section
below.
Maternity Patients Currently all pregnant patients should be classified as MEDIUM SEVERITY and referred to Complex Care and
the COVID Liaison Midwife at Monash Health (details below).
Contact details for maternity escalations are below:
Service Reason for Contact Contact Details
COVID Obstetric Fellow Urgent obstetric escalation Via Monash Switchboard
03 9594 6666 (24 hours, 7 days)
COVID Liaison Midwife To advise of new obstetric
cases and any obstetric
related queries
0423 790 756
(Monday – Friday service only)
On the weekends, please continue to send emails to the COVID Liaison Midwife, and these cases will be
picked up Monday morning. If there is an urgent clinical escalation over the weekend, contact the COVID
Obstetric Fellow using the above details.
COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 11
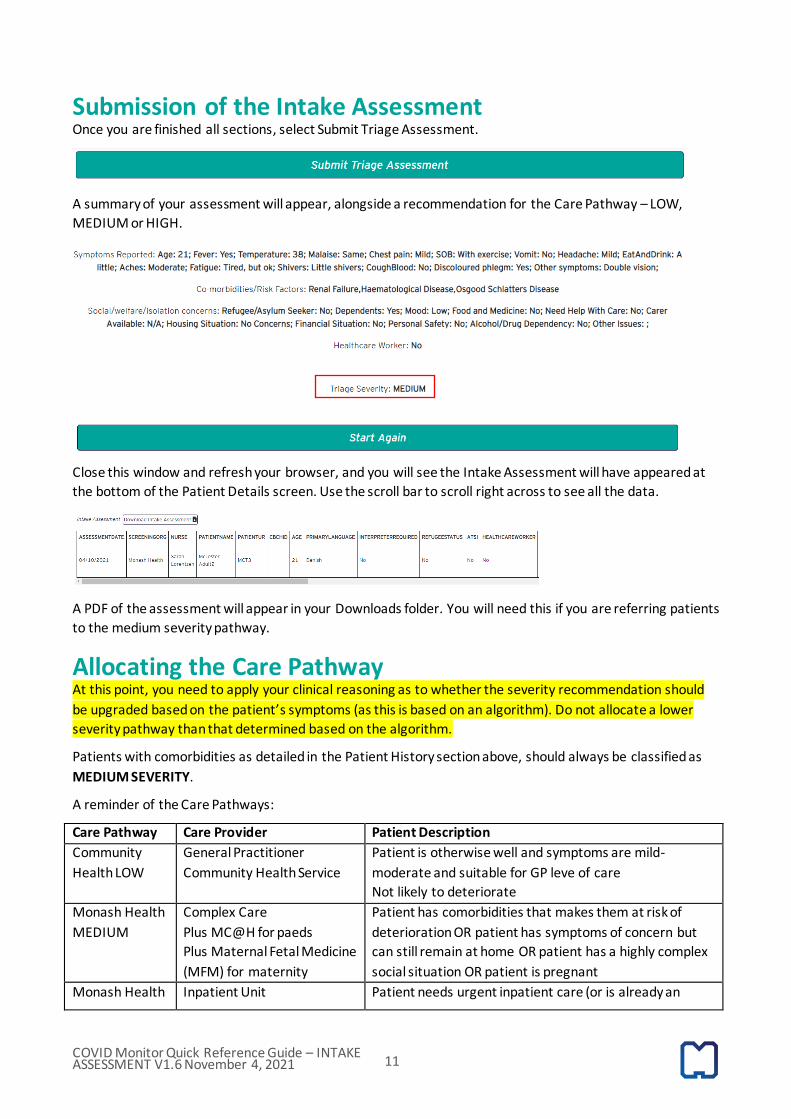
Submission of the Intake Assessment Once you are finished all sections, select Submit Triage Assessment.
A summary of your assessment will appear, alongside a recommendation for the Care Pathway – LOW,
MEDIUM or HIGH.
Close this window and refresh your browser, and you will see the Intake Assessment will have appeared at
the bottom of the Patient Details screen. Use the scroll bar to scroll right across to see all the data.
A PDF of the assessment will appear in your Downloads folder. You will need this if you are referring patients
to the medium severity pathway.
Allocating the Care Pathway At this point, you need to apply your clinical reasoning as to whether the severity recommendation should
be upgraded based on the patient’s symptoms (as this is based on an algorithm). Do not allocate a lower
severity pathway than that determined based on the algorithm.
Patients with comorbidities as detailed in the Patient History section above, should always be classified as
MEDIUM SEVERITY.
A reminder of the Care Pathways:
Care Pathway Care Provider Patient Description
Community
Health LOW
General Practitioner
Community Health Service
Patient is otherwise well and symptoms are mild-
moderate and suitable for GP leve of care
Not likely to deteriorate
Monash Health
MEDIUM
Complex Care
Plus MC@H for paeds
Plus Maternal Fetal Medicine
(MFM) for maternity
Patient has comorbidities that makes them at risk of
deterioration OR patient has symptoms of concern but
can still remain at home OR patient has a highly complex
social situation OR patient is pregnant
Monash Health Inpatient Unit Patient needs urgent inpatient care (or is already an
COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 12
HIGH inpatient)
Patients who meet the criteria for medium severity pathway based on age or co-morbidities must not
remain on the low pathway UNDER ANY CIRCUMSTANCES.
The Care Pathway is default set to Community Health LOW, so if you need to change the Care Pathway, use
the Change Care Pathway button and select the appropriate option.
Identifying the Patient’s General Practitioner (GP) All patients, regardless of their clinical pathway, should have their usual GP identified as part of the Intake
Assessment. Ask the patient ‘do you have a regular GP practice that you attend?’
Conplete this by clicking on the blue tick in the GP Practice section of the Patient Details screen.
Select the relevant practice from the dropdown list. If the patient does not have a GP, leave this as NONE.
Advise the patient that a GP will be arranged for them to provide care during their COVID episode if they
remain on the Low Severity pathway.
Low Severity Patients Low severity patients will receive telehealth care through their usual GP (if required) or their allocated GP
practice, as identified by our community partner, Central Bayside Community Health Service. They should
continue to enter their symptoms daily via the SMS that they will receive each morning around 8.30am.
Their symptoms will continue to be monitored by Central Bayside until they are discharged at Day 14.
Medium Severity Patients If patients have been identified as Medium Severity, they will receive care as per the below:
Patient Type Care Provider Contact
Adults Monash Complex Care 0404 084 273
Paediatrics Monash Children’s at Home 0414 427 371
Please let the relevant service know via email if you refer a medium severity patient to them. Attach the PDF
of your Intake Assessment so you don’t have to transpose any clinical details.
If you want to confirm your allocation decision, please phone the respective team as above, noting that all
pregnant patients will be MEDIUM SEVERITY as default.
If a case needs to be urgently discussed, please phone the doctor on call (details in Clinical Escalation
section). Do not send emails about urgent patients as these emails are not monitored all the time.

COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 13
High Severity Patients High Severity Patients by definition require inpatient care. If when you call the patient they advise you that
they are already in hospital, change their Care Pathway to Monash Health HIGH. You do not need to
complete the Intake Assessment on these patients.
If during the Intake Assessment you feel that the patient needs urgent inpatient care (i.e. transfer to ED),
please don’t hesitate to call 000. If the transfer is not time critical, escalate the issue with the COVID Positive
Care Pathway Medical Team. See the Clinical Escalation section for further details.
Additional Information Use the ‘Record Notes’ button to record any additional information about the patient, as required.
Clinical Escalations The below table and flow chart details criteria for clinical escalation based on reported patient symptoms.
The below diagram illustrates what to do based on the reported patient symptoms.
The pathway has medical staff on call daily for urgent escalations.
Doctor phone 1: 0407 899 263 (10.30am – 8.00pm)
Doctor phone 2: 0408 331 953 (11.00am – 8.30pm)

COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 14
Paediatric Doctor: 0487 019 649 (24 hours)
This is for advice only. Telehealth consultations with the patient are not available for patient undergoing
Intake Assessment.
Social and Welfare Needs If you identify that patients need support with the following issues:
Email Relief and Community Support on [email protected] and include the following information:
• Full name, address, phone number and TREVI number
• Number of household members (include ages of children)
• Urgent relief needs and timescale: Rapid (within 3 hours), Urgent (same day or within 24 hours) or
Non-urgent (24-48 hours)
If medication is required, low severity pathway patients should contact their GP for a prescription and
engage their local pharmacy to arrange contact-free delivery. For medium severity patients, medication
requirements should be handed over to Complex Care (or Monash Children’s at Home for paediatrics) so
they can be addressed.
Family Finding Service Family Finding is a service that can support parents/guardians plan alternative care arrangements for their
children with family or friends in the event that they require hospitalisation due to COVID-19.
The workflow is illustrated below.
Families involved with Child Protection are not in scope for Family Finding and should be referred to the
local Department of Families, Fairness and Housing Child Protection office.
Referrals can be sent to [email protected] with the subject line ‘Family Finding’. Email must
contain the following information:
• Name and contact number of the parent/guardian

COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 15
• Names and ages of all children
• Confirmation that the parents/guardians can identify a care options however the identified carer will
require support such as transport, food and other relief to maintain care arrangements OR the
parents/guardians cannot identify anyone who would be able to care for their children and require
support in identifying a care option
• Advice as to whether the family requires an interpreter
Referrals for Aboriginal children can be sent to the Victorian Aboriginal Child Care Agency (VACCA) via
[email protected]. VACCA can be contacted on their response number 0488 930 509.
Difficulty Isolating If you identify that a patient has difficulty isolating or if you suspect that the patient is not isolating as
instructed, please escalate to SEPHU so they can address the issue [email protected]
You can also make a direct referral to the IIATS service to request Hotel Quarantine, however the service is
significantly oversubscribed and it is not uncommon for referrals to go unanswered. Refer here.
If you have urgent issues with isolation (i.e. family violence) email [email protected]
Patients who Decline the Assessment If the patient declines the Intake Assessment, offer to call back later in the day or the next day. Record this
using the ‘Record Notes’ button in the Patient Details screen.
If the patient does not want you to call them back (i.e. does not want to be part of the pathway) then you
can discharge them using the ‘Request Clearance/Discharge’ button in the Patient Details Screen.
Select ‘Discharge: Declined assessment/clinical care’
The patient will receive a text message confirming that they have declined care. The message includes a
contact number if they change their mind and want to be included in the pathway.
Patients who Require an Interpreter Health Direct can utilise their own internal interpreting arrangement or call TIS National Interpreting Service
on 131 450.
Uncontactable Patients If you are attempting to complete an Intake Assessment and you cannot contact the patient, mark as Left
Message / No Answer (dark blue button). Do not discharge them as unable to contact at this point.

COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 16
A repeat attempt should be make to contact them later in the day and then again on the following day.
If after 2-3 attepmpts over 24 hours, they are still not-contactable, and they are not entering any symptoms,
then you can discharge them as unable to contact.
They will get a text to say that we have been unable to contact them, with a contact number should they
wish to join the pathway.
If they are entering symptoms, then do not discharge them, but leave them on the Pending Assessment list.
If they do continue to enter symptoms, but do not answer the phone, they can be left on the pathway until
day 14, when they will be routinely discharged. If their symptoms deteriorate to the point they become a P1,
attempts to contact them should continue.
Wrong Number / Number Disconnected / No Phone Number If you come across a patient where the phone number is incorrect or disconnected, please remove the
number from the patient’s file so that we do not continue to contact an incorrect number.
Do this via the Edit Patient button in the Patient Details screen:
The admin team will regularly check the whole patient list for patients who do not have phone numbers and
attempt to find alternative numbers where possible.
Release from Isolation and Discharge from the Pathway Patients are usually discharged from the COVID Positive Care Pathway at Day 14, provided they have no or
mild symptoms. Patients are also released from isolation on Day 14 via text message from the Public Health
Unit. Most patients do not need a repeat swab to be released from isolation and cleared of COVID.
Patients can be vaccinated (if not already) once they are fully recovered from their acute illness, unless they
have had a Sotrovimab infusion, in which case they need to wait 3 months.
Please see the Discharge QRG for further information on discharging patients from the pathway.
COVID Monitor Quick Reference Guide – INTAKE ASSESSMENT V1.6 November 4, 2021 17
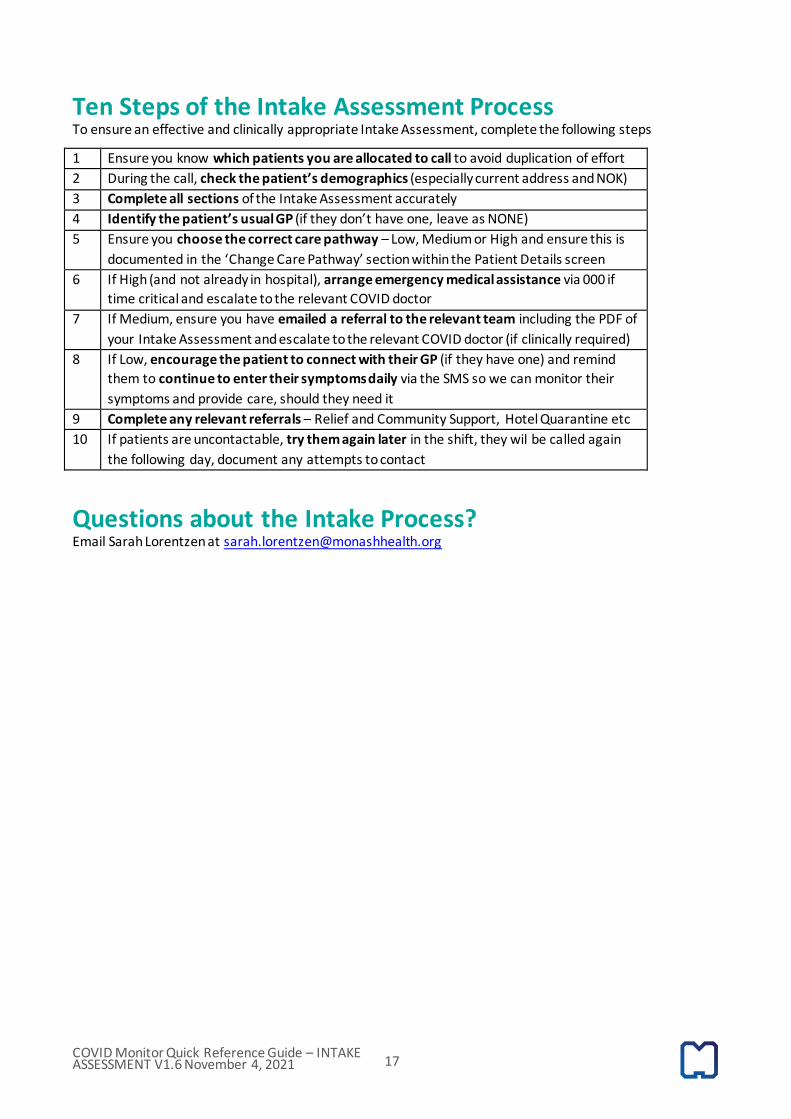
Ten Steps of the Intake Assessment Process To ensure an effective and clinically appropriate Intake Assessment, complete the following steps
1 Ensure you know which patients you are allocated to call to avoid duplication of effort
2 During the call, check the patient’s demographics (especially current address and NOK)
3 Complete all sections of the Intake Assessment accurately
4 Identify the patient’s usual GP (if they don’t have one, leave as NONE)
5 Ensure you choose the correct care pathway – Low, Medium or High and ensure this is
documented in the ‘Change Care Pathway’ section within the Patient Details screen
6 If High (and not already in hospital), arrange emergency medical assistance via 000 if
time critical and escalate to the relevant COVID doctor
7 If Medium, ensure you have emailed a referral to the relevant team including the PDF of
your Intake Assessment and escalate to the relevant COVID doctor (if clinically required)
8 If Low, encourage the patient to connect with their GP (if they have one) and remind
them to continue to enter their symptoms daily via the SMS so we can monitor their
symptoms and provide care, should they need it
9 Complete any relevant referrals – Relief and Community Support, Hotel Quarantine etc
10 If patients are uncontactable, try them again later in the shift, they wil be called again
the following day, document any attempts to contact
Questions about the Intake Process? Email Sarah Lorentzen at [email protected]