Embed Size (px)
Citation preview

Technical Guidelines
Health Service Referral System
West Nusa Tenggara
Cooperation between:
West Nusa Tenggara Province Health Office and GTZ Siskes Mataram
First Print, Mataram, 2009
B
AA
DK AT SI H U

Technical Guidelines Health Service Referral System
West Nusa Tenggara Province
Cooperation between:
West Nusa Tenggara Province Health Office and GTZ Siskes Mataram, 2008.
1

No............. Catalogue in Publication, NTB West Nusa Tenggara Provincial Health Office p Title: Technical Guidelines for the Health Service Referral
System. Cooperation of the West Nusa Tenggara Provincial Health
Office & GTZ Siskes First Edition, Mataram, September 2008.
2

3
FOREWORD
Praise to God Almighty, for through His Grace and Blessing, these Technical Guidelines on the Health Service Referral System in West Nusa Tenggara Province have been developed. These technical guidelines are derived from Decree of the Minister of Health 032/Birhup /1972 dated 2 September 1972 concerning Referral Systems, and are for use by personnel in health service facilities in West Nusa Tenggara Province.
These technical guidelines received input from the results of the assessment of the referral system in five districts/municipalities – Mataram Municipality, Lombok Barat District, Sumbawa District, Sumbawa Barat District, and Bima Municipality – conducted by a joint team from the West Nusa Tenggara University Research Centre and GTZ Siskes in 2007; and from the outputs of various workshops involving health personnel from village midwifery clinics, primary health centres, district and provincial general hospitals, the health offices of these five districts/municipalities, the provincial health office, and professional organisations (Association of Indonesian Doctors and Association of Indonesian Midwives) in West Nusa Tenggara province, as well as resource people from the Ministry of Health’s Directorate General of Medical Services, and GTZ Siskes Mataram.
After conducting field trials in Lombok Barat District in the fourth quarter of 2008, these technical guidelines will be distributed to all public and private health facilities in West Nusa Tenggara Province to be used as standards by health personnel implementing health service referrals, including maternal and neonatal referrals and referrals of poor patients.
I would like to thank GTZ Siskes, who have worked with us to strengthen the referral system and health development in West Nusa Tenggara Province; and also the design team from the West Nusa Tenggara Provincial Health Office and resource people for the hard work they put in to completing these technical guidelines.
Feedback and suggestions from users for improving these technical guidelines will be welcomed.
Mataram, September 2008.
Head of Health West Nusa Tenggara Provincial Health Office
Dr. Baiq Magdalena Level 1 Senior Administrator, IV/c Civil Service No. 140 186 344

4
FOREWORD
The “Deutsche Gesellschaft fuer Technische Zusammenarbeit (GTZ) GmbH” is an international cooperation agency of the Federal Republic of Germany contributing to sustainable development through technical cooperation projects in developing countries. One of the projects supported by GTZ in Indonesia is SISKES which is co-financed by the German and the British governments and is implemented jointly with the Ministry of Health and provincial governments of East Nusa Tenggara for a period of 2000-2009 and West Nusa Tenggara for 2006-2009.
The GTZ/SISKES project in NTB focuses as well on health system management aspects with a specific focus on maternal and neonatal health as on health services management and their clinical service quality. Integrated planning, performance budgeting and data based monitoring, health financing, especially for the poor are part of the support across the province as well as community empowerment and participation in health related action in selected districts linked to maternal health.
A health system that has clear guidance how each part of the system is interlinked and shows fast action throughout the levels of the system in case of emergency is crucial in order to achieve MDGs and to improve the health indicators. For this reason, GTZ SISKES warmly welcomes and supports the development and publication of these technical guidelines for the referral health system for West Nusa Tenggara province being based on MoH guidelines for MPS referral from 2004 and the general guidelines on referral from 1972. Proper dissemination and utilization of the guidelines at all levels of health service providers, including village maternity clinics, village health posts, primary health centres, district hospitals and provincial hospitals across the whole province will contribute to strengthening the local health system and is expected to contribute to the reduction in maternal and neonatal fatalities.
My appreciation goes to the team having produced and revised this output and I hope that the guidelines will be of benefit to the people of West Nusa Tenggara Province, particularly the poor and the vulnerable, and assist other provinces in Indonesia to follow the example of West Nusa Tenggara.
Mataram, April 2009.
Dr. Gertrud Schmidt-Ehry, MPH Principal Advisor GTZ Siskes and HRD.

5
TABLE OF CONTENTS Page
TITLE PAGE i
FOREWORD BY THE HEAD OF THE NTB PROVINCIAL HEALTH OFFICE iii
FOREWORD BY THE HEAD OF GTZ SISKES iv
TABLE OF CONTENTS vii
LIST OF TERMS viii
CHAPTER I INTRODUCTION 1
A. Background 1
B. Goal & Objectives 3
C. Situational Analysis 3
CHAPTER II TECHNICAL ASPECTS OF IMPLEMENTATION OF THE REFERRAL SYSTEM
5
A. Definition 5
B. Activities included in the referral system 5
C. Organisation and management of the implementation of the referral system
7
CHAPTER III PROCEDURES FOR IMPLEMENTATION OF THE REFERRAL SYSTEM
10
A. Referring and Receiving Referred Patients 10
B. Referring and Receiving Referred Specimens 15
C. Knowledge and Specialist Referrals 18
D. Procedure for Monitoring and Evaluating Implementation of the Referral System
20
CHAPTER IV THE PRINCIPLES OF REFERRAL OF OBSTETRIC AND NEONATAL EMERGENCIES
21
A. Principles and Authority of Service Facilities 21
B. Principles of Making and Receiving Maternal and Neonatal Patient Referrals
26
CHAPTER V CONCLUSION 27
BIBLIOGRAPHY 28
APPENDICES

6
LIST OF TERMS
7T Timbang Berat Badan; Tekanan Darah; Tinggi Fundus Uterus; Tetanus Toxoid; Tablet Tambah Darah; Tatap muka; Tes Urine.
APN Asuhan Persalinan Normal ASKES Asuransi Kesehatan PT. ASKES BBL Bayi Baru Lahir BBLR Berat Badan Lahir Rendah BKMM Balai Kesehatan Matra Masyarakat Depkes Departemen Kesehatan GAKIN Keluarga Miskin IMD Inisiasi Menyusu Dini Jamkesmas Jaminan Kesehatan Masyarakat untuk Keluarga Miskin Jamsostek Jaminan Sosial Tenaga Kerja KB Keluarga Berencana KKP Kantor Kesehatan Pelabuhan LABKES Laboratorium Kesehatan MTBM Manajemen Terpadu Balita Muda MTBS Manajemen Terpadu Balita Sakit Obgyn Obstetri Gynecologi Polindes Pos Persalinan Desa (village maternity clinics) PONED Pelayanan Obstetri Neonatal Dasar PONEK Pelayanan Obstetri Neonatal Komprehensif Poskesdes Pos Kesehatan Desa (village health posts) Posyandu Pos Pelayanan Terpadu (integrated service posts) Pusk Puskesmas (primary health centres) Pustu Puskesmas Pembantu (auxiliary primary health centres) RB Rumah Bersalin (maternity clinics) RS Rumah Sakit RSU Rumah Sakit Umum RSUD Rumah Sakit Umum Daerah Sp.A Spesialis Anak Sp.OG Spesialis Obstetri dan Ginekologi
[translator’s note: this list of terms is not applicable as none of these terms appears in the English version]

7
CHAPTER I
INTRODUCTION A. Background
Implementation of the Health Referral System in West Nusa Tenggara
Province is based on Decree of the Minister of Health 032/Birhup/72 dated 4
September 1972 concerning Implementation of Referral Systems, Decree of the
Minister of Health 128/2004 concerning Basic Policy for Primary Health Centres,
and the 2007 Action Plan of the Directorate General of Medical Services, Ministry
of Health.
The referral system in West Nusa Tenggara Province covers three aspects
of primary health services: patient referrals, specimen referrals, and knowledge
referrals. All three may be horizontal, vertical, or a combination of the two, from a
lower level to a higher level. Primary health services are available at all levels,
from village maternity clinics, auxiliary primary health centres, primary health
centres, and private practices, through to district/municipal public hospitals and
provincial public hospitals. If a village maternity clinic, auxiliary primary health
centre, primary health centre or private practice receives or treats an emergency
case, but does not have the authority or does not feel it has the capacity to provide
certain medical care or supporting health services, it must refer the patient to a
level with more competent and comprehensive health facilities, such as the
nearest hospital.
Implementation of the health referral system in West Nusa Tenggara
Province is currently not optimised at all levels of health facilities, as indicated by
the incidence of maternal and child death and other cases that require referral and
counter referral but are not dealt with satisfactorily. There are several factors
contributing to this lack of referral including: 1) lack of comprehensive technical
guidelines for frontline health personnel, 2) lack of adequate counselling for
patients or their families by health personnel, and 3) the absence of analysis or
follow up by the local health office to address the problem of health referrals.
There are several types of referral primary health centres and their
equivalent can make, including obstetric referrals, neonatal referrals, referrals of

8
cases of child malnutrition and cases of communicable disease (suspicion for
outbreaks), specimen referrals, and knowledge referrals.
Assessment of referral systems in five districts/municipalities in West Nusa
Tenggara by consultants from West Nusa Tenggara University in 2007 identified
several problems that may have negative bearing on the implementation of patient
referrals, including:
1) The initial point of contact that emergency patients have is not with trained
medical personnel. Personnel at the initial point of contact tend only to go through
the routine procedure of accepting a patient, such as pointing out the registration
desk, asking the family to purchase a card, etc., and fail to take into account the
safety of the patient at the initial point of contact.
2) Doctors and midwives, as the trained personnel, are not in the frontline.
3) The slow procedure for accepting referrals due to bureaucratic administration,
including reporting.
4) Hospitals do not have blood banks or have blood banks that do not function
properly.
5) Not all districts/municipalities and blood banks in district/municipal hospitals
have blood transfusion units, there is no immediate supply of blood for patients
who need it.
6) Limited supporting diagnostic services due to a lack of health personnel,
facilities, and equipment.
7) The limited skills of primary health centre personnel for dealing with maternal
and neonatal emergencies.
8) Feedback or back referral from district/municipal hospitals is frequently ignored
by primary health centre or equivalent personnel because it is generally perceived
that the services provided by the district/municipal hospital have fully addressed
the problem referred.
9) The absence of locally adapted technical guidelines on the health referral
system.
10) Limited public knowledge of the signs of maternal and neonatal
emergencies frequently delays referrals.
11) Culturally, many members of the patient's family must be involved in decision
making, and the patient's inability to make independent decisions frequently
delays referrals.

9
In view of the above, technical guidelines on the health referral system in
West Nusa Tenggara Province, need to be prepared as a reference for all
personnel in all health facilities.
B. Goal & Objectives 1. Goal
Implementation of a standard health referral system across all levels
of health facilities in West Nusa Tenggara Province.
2. Objectives a. Implementation of standard technical and administrative procedures
for case referral and back referral,
b. Implementation of standard technical and administrative procedures
for specimen referral and back referral,
c. Implementation of standard technical and administrative procedures
for medical / midwifery knowledge referral.
d. Implementation of referral and back referral recording and reporting
systems in health facilities.
C. Situational Analysis 1. Primary Health Centres, Auxiliary Primary Health Centres, and Village
Maternity clinics The number of primary health centres in West Nusa Tenggara Province is
increasing, from 127 in 2005, to 130 in 2006, and 135 in 2007 and 142 in
2008. They include 53 primary health centres with in-patient facilities, and
89 primary health centres without in-patient facilities. Similarly, the number
of auxiliary primary health centres and village maternity clinics has been
growing, reaching a total of 528 and 550 units respectively as at the end of
2007. The average ratios are 1 primary health centre per 32,000
population, or 3.1 primary health centres per 100,000 population; 1 auxiliary
primary health centre per 8,200 population or 12.2 auxiliary primary health
centres per 100,000 population; and 1 village maternity clinic per 7800
population or 12.7 village maternity clinics per 100,000 population.
10
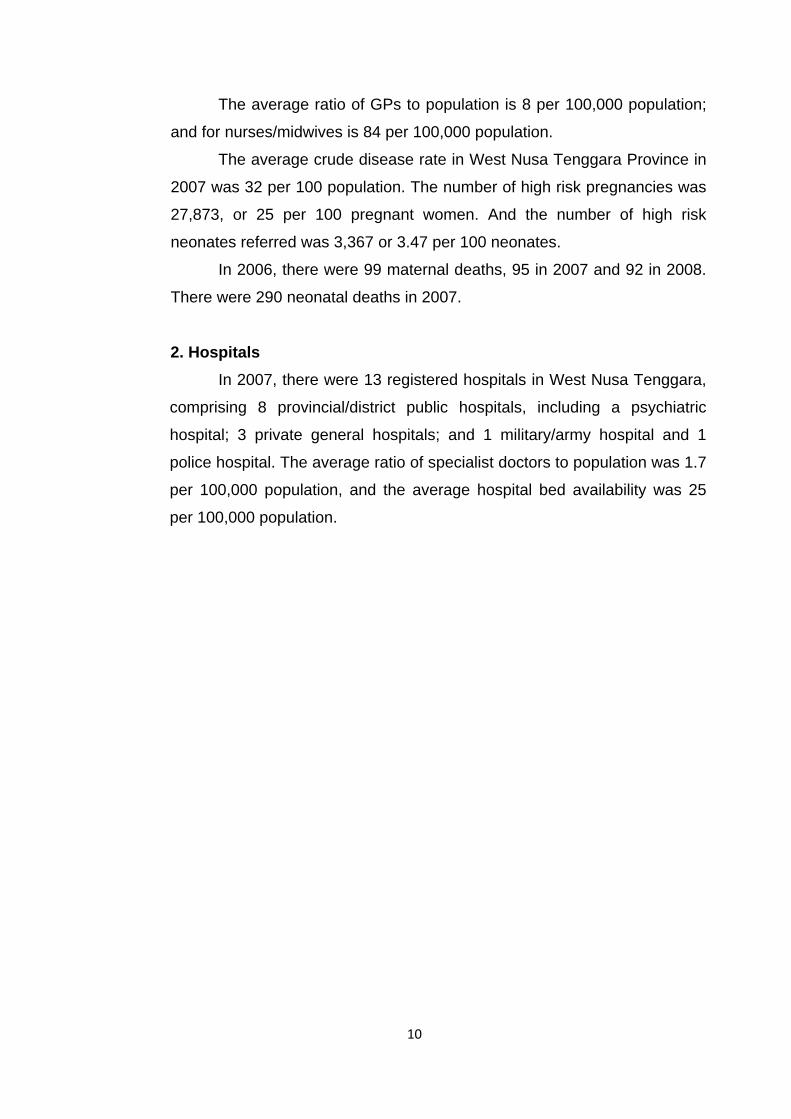
The average ratio of GPs to population is 8 per 100,000 population;
and for nurses/midwives is 84 per 100,000 population.
The average crude disease rate in West Nusa Tenggara Province in
2007 was 32 per 100 population. The number of high risk pregnancies was
27,873, or 25 per 100 pregnant women. And the number of high risk
neonates referred was 3,367 or 3.47 per 100 neonates.
In 2006, there were 99 maternal deaths, 95 in 2007 and 92 in 2008.
There were 290 neonatal deaths in 2007.
2. Hospitals In 2007, there were 13 registered hospitals in West Nusa Tenggara,
comprising 8 provincial/district public hospitals, including a psychiatric
hospital; 3 private general hospitals; and 1 military/army hospital and 1
police hospital. The average ratio of specialist doctors to population was 1.7
per 100,000 population, and the average hospital bed availability was 25
per 100,000 population.

11
3. District/Municipal Health Offices In 2008, there were nine district/municipal health offices (10 in 2009)
on the island of Lombok (4 (5) districts/municipalities) and the island of
Sumbawa (5 districts/municipalities). Regarding the referral system and
outbreak management, the head of the district/municipal health office
provides assistance for referral facilities to primary health centres and other
health facilities in the district/municipality, and in turn, may request the
assistance of referral facilities and health personnel from the head of the
provincial health office, the nearest district/municipal health office, other
source.
4. West Nusa Tenggara Provincial Health Office. The Head of the West Nusa Tenggara Provincial Health Office has
the authority to regulate the implementation, coordination, and supervision
of the health referral system in West Nusa Tenggara Province. In situations
where organisation of this health referral system requires the involvement of
other sectors/parties, the Head of the West Nusa Tenggara Health Office
may consult with the head of that other sector/party on the approval of
Governor of West Nusa Tenggara, or consult directly with the Minister of
Health or other relevant official in the Ministry of Health.

12
CHAPTER II
TECHNICAL ASPECTS OF IMPLEMENTATION OF HEALTH SERVICE REFERRAL SYSTEMS
A. Definition
Implementation of this health referral system was developed based on
Decree of the Minister of Health 032/Birhup/72 concerning Referral Systems,
which is defined in Chapter I, General Provisions, Article 1 as follows: “A referral system is a health service measure between various levels of medical service units within a certain region, or across the Republic of Indonesia." In the Indonesian version of these Technical Guidelines, 'referral
system' is referred to as 'sistem rujukan'.
B. Activities included in the referral system
1. Sending patients Patients should be referred as early as possible for further care or
treatment to a more fully-equipped health facility. If the patient has received
further treatment, the health service unit receiving the referral must refer the
patient back to the health facility that sent him or her, for monitoring of
treatment and care, including subsequent rehabilitation.
2. Sending specimens a. Consultation
A specimen sent to a referral laboratory for accurate laboratory
examination.
b. Cross check Some specimens examined in primary health centre/hospital
laboratories are sent to district/municipal laboratories to cross-check
and validate the results of the first examination.
3. Transfer of knowledge and skills Specialists from hospitals may periodically visit primary health
centres. Assistant specialists / senior residents may be placed in
district/municipal hospitals that need them or in districts that do not have

13
specialists. Transfer of knowledge and skills to GPs, midwives and nurses
from primary health centres or district/municipal general hospitals may take
the form of internships in better equipped hospitals.
4. Referral Information Systems Information on patient referrals is prepared by the referring health
personnel and recorded in the patient's referral letter sent to the doctor the
patient is being referred to. The letter should have a reference number and
include information about the date and time patient was sent, the status of
the patient's family (poor or not poor and general information), whether or
not the patient has Askes health insurance or Jamsostek health insurance,
the purpose of the referral, the name and identity of the patient, a resume of
the patient's medical history, results of physical examination, diagnosis,
action taken and drugs given, including supporting examinations, treatment
progress, and any other information considered necessary (see form R/1/a,
Patient Referral Letter).
Back referral information is prepared by the doctor receiving the
referred patient, and having treated the patient, he or she records the back
referral information in a back referral letter which is sent to the person who
referred the patient. The letter should be dated and have a reference
number, and include information about the status of the patient's family
(poor or not poor and general information), whether or not the patient has
Askes health insurance or Jamsostek health insurance, the purpose of the
referral, the name and identity of the patient, post treatment diagnosis,
condition of the patient on discharge from treatment, and recommended
follow up (See Form R/1/b, Counter Referral Letter), if any.
Information about specimens sent is provided by the person sending
the specimen by completing the Specimen Referral Form, which has a
reference number and is dated, and includes information about the status of
the patient's family (poor or not poor and general information), whether or
not the patient has Askes health insurance or Jamsostek health insurance,
the purpose of the referral, the type of specimen sent and specimen
number, the date the specimen was taken, the type of examination

14
requested, the name and identity of the patient providing the specimen, and
the clinical diagnosis. (See Form R/2, Specimen Referral Letter).
Back information about the results of the examination of the referred
specimen is prepared by the laboratory receiving the specimen and
immediately sent to the person referring the specimen using the
laboratory's forms as applicable.
Information on requests for specialists is prepared by the Head of the
Primary Health Centre or District/Municipal General Hospital and sent to the
Head of the District / Municipal Health Office or by the District/Municipal
Health Office and sent to the Provincial Health Office, by completing a
Letter of Request for Specialist, which is dated, has a reference number,
has as its subject 'Request for Specialist', and indicates the type of
specialisation required, the time and place the specialisation is requested
for, the purpose of the request for the specialisation, and the source of
funding or amount of funding available (See Form R/3, Request for
Specialist).
Information on the sender, carer, or person requesting the specialist
must include his or her name, clearly written, the name of the institution,
and contact landline or mobilie phone number. Open communication
between the sender and receiver in terms of providing additional
information is necessary for the safety of the patient, specimen or medical
specialist.
For referral information system recording and reporting, the standard
form is RL.1 for hospitals and form R.4. for primary health centres (see
appendix). The follow up of referral reporting shall follow the established
reporting flow.
C. Organisation and Management in Implementation of the Referral System For this referral system to be implemented effectively and efficiently,
attention should be given to its organisation and management. The chain of
authority and responsibility of each health service unit involved, with regard to
regulation and coordination, must be clear. The following is a description of the
15
criteria for division of service areas within the referral system and for
coordination between health service units.
1. Criteria for division of service areas in the referral system Because health personnel and health funding are limited, effective and
efficient use must be made of available medical service facilities. The
government has established the concept of division of service areas in the
public health system.
In this referral system, each health unit, including village maternity
clinics, auxiliary primary health centres, primary health centres, and
hospitals, will provide health services to the public according to its area and
the competence of its personnel and facilities. The exception to this rule is
emergency referrals. Thus, division of service areas in the referral system
are based not only on government administrative boundaries, but also on
other criteria, including:
a. The competency or comprehensiveness of the health facility, for
example hospital facilities according to their classification.
b. Cooperation between the hospital and a medical faculty.
c. The existence of a transport system or facilities that can be used to
travel to the referral health facility or hospital.
d. The geographical condition of the area where the health facility is
located.
In implementing the concept of referral areas, the wishes of the patient
/ the patient's family will be a major determining factor in the choice of
referral facility.
2. Coordination of referrals between health facilities Provision of equally distributed health services to the public requires
effective coordination in provision of referral health services. This
coordination can be achieved by drawing lines of authority and
responsibility for each health service unit. The lead in the coordination of
referrals is the Head of the West Nusa Tenggara Provincial Health Office.
Because the referral system area covers more than one
district/municipality, coordination between the district/municipal health

16
offices concerned is vital. The highest referral hospital in West Nusa
Tenggara Province is Mataram General Hospital.
3. Referral Flow The differences and similarities in level, area and competence of each
health facility in West Nusa Tenggara Province make it necessary to design
a general flow for patient referrals, not including emergency referrals or
special referrals. There are several aspects that need to be taken into
account in the referral flow:
a. Hospital Classification Provincial general hospitals are classified B, and are the referral
centres for district/municipal general hospitals classified C or D or other
health facilities, such as the Military Hospital, Bhayangkara Hospital and
private hospitals in West Nusa Tenggara Province.
b. Location of District/Municipality District/municipal hospitals are the referral facilities for primary health
centres. District / municipal general hospitals have specialists in four main
fields who should be able to deal with referrals from the nearest
district/municipal general hospitals that do not have specialists in that
particular field. Primary health centres are the main referral facilities for
primary health centres, auxiliary primary health centres, village maternity
clinic, desa siaga, cadres, and members of the public in their area.
c. Coordination between technical units Other technical units that are referral facilities coordinated at the
West Nusa Tenggara provincial level include: the Regional Health
Laboratory, the psychiatric hospital, eye clinic, and Port Health Office.

Figure 1.
REFERRAL SYSTEM FLOWCHART
GP / midwifery practices
Class A/Special Hospitals Jakarta/Surabaya
Provincial Public / Private General Hospitals
in NTB provincial capital
Class C Public/Private General Hospitals
In Districts/Municipalities
Class D Public/Private General Hospitals
In Districts/Municipalities
Health Labs KES Psychiatric Hosp. Special Hosp. Eye Clinic
Port Health Office
in Mataram
Primary health centers, Primary Health Centers with Inpatient Facilities, Primary Health Centers Providing Basic Obstetric and Neonatal Services
Maternity clinics / Individuals
Integrated Health Posts
Village Health Posts
Village Maternity clinics
Aux. Primary Health Centers
MEMBER OF PUBLIC / CADRE WITH THE PROBLEM
Note: This flowchart does not apply to emergency/special referrals.
17
18
CHAPTER III.
PROCEDURES FOR IMPLEMENTATION OF THE REFERRAL SYSTEM
To provide guidelines for health service units on implementation of the
referral system, this section describes the following:
1) Standard procedure for referring patients and receiving referred patients.
2) Standard procedure for referring specimens and receiving referred
specimens.
3) Standard procedure for knowledge and specialist referrals.
4) Procedure for monitoring and evaluation of the referral system.
A. Referring Patients and Receiving Referred Patients. Patients should be examined properly for referral. A patient can be referred
if at least one of the following criteria is met:
1) The results of the physical examination confirm that the case cannot be
dealt with.
2) The results of the physical examination and supporting medical examination
confirm that the case cannot be dealt with.
3) There is a need for further supporting medical examination requiring the
presence of the patient.
4) Even after treatment and care, there is a need for additional examination,
treatment and care at a more competent health facility.
In the procedures for referring and receiving referred patients, there are two
parties involved, the party making the referral (referral source) and the party
receiving the referral (referral target). These procedures are described in detail in
this section:
1) Standard procedure for referring patients,
2) Standard procedure for receiving referred patients,
3) Standard procedure for back referral of patients,
4) Standard procedure for receiving back referral of patients.

19
1. Standard procedure for referring patients
a. Clinical procedure:
1) Take anamnesis, perform physical examination, and define possible
differential diagnosis and main symptoms.
2) Perform pre-referral measures as indicated: for example set up oxygen
supply, drip, administer injections as needed, and prevent bleeding if
necessary.
3) Decide where the patient is to be referred to.
4) Emergency cases must be accompanied by medical
personnel/paramedic.
5) If the patient is transported by primary health centre vehicle or
ambulance, the vehicle must wait for the patient at the appointed
emergency unit until the patient has been treated and a decision has
been made as to whether the patient is to be treated as an inpatient or
outpatient.
b. Administrative Procedure:
1) Do this after the patient has received pre-referral measures.
2) Record the identity of the patient in the patient referral register. 3) Make notes on the patient’s medical record, and prepare a resume of
the medical record to be given to the referral unit when the referred
patient is received.
4) Prepare a patient referral letter in duplicate (Form R/1/a, attached). The
top copy should be sent to the referral unit with the patient. The bottom
copy is filed for reference purposes.
5) Arrange transportation and as soon as possible make contact with the
referral unit.
6) The patient should be dispatched as soon as the administration is
completed.

20
2. Standard procedure for receiving referred patients.
a. Clinical Procedure:
1) Immediately receive and deal with the referred patient as per procedure.
2) Stabilise the patient.
3) Send the patient to an elective care room for further treatment, or refer
the patient to a more competent health facility.
4) Monitor and evaluate the patient’s clinical condition.
b. Administrative Procedure:
1) Receive and sign the patient referral letter, which will be attached to the
patient card.
2) Check and sign the patient’s medical record cards, if the patient can be
received, then prepare a patient receipt as per unit procedure.
3) If the unit (primary health centre or hospital) is not equipped to treat the
case, the patient must be referred to a more competent hospital, by
preparing a patient referral letter in duplicate (see Form R/1 attached).
The original should be sent with the patient, following the same
procedure for referring patients.
4) Record the identity of the patient in the appropriate register.
5) Note the results of examination and treatment and care on the referral
medical card, and send this to the treatment unit appropriate to the
patient’s condition.
6) Prepare letter of informed consent (concerning treatment, inpatient care,
early discharge, etc)
7) Immediately inform the accompanying health personnel/patient’s family
about decisions on action to take / care to be given.
8) Hospitals must prepare quarterly reports using form RL.1 (page 2, point
7, and page 6, point 24.3).

21
3. Standard procedure for back referral of patients.
a. Clinical Procedure:
1) A hospital or primary health centre receiving a referred patient must
refer the patient back to the hospital / primary heath centre / village
maternity clinic that referred the patient, upon completion of the
following process:
a) Medical examination, treatment and care have been administered,
but recovery requires follow up by the hospital / primary heath centre
/ village maternity clinic that referred the patient
b) After medical examination, clinical emergency measures have been
taken, but further treatment and care can be administered by the
hospital / primary heath centre / village maternity clinic that referred
the patient.
2) Conduct physical examination and diagnose that the patient can be
released from the care of the hospital / primary health centre, where:
a) The patient is fit and healthy.
b) Sufficient clinical progress has been made as to allow outpatient
treatment.
c) No clinical progress has been made, and the patient must be
referred elsewhere.
d) The patient dies.
3) If a referred patient is released, the hospital / primary health centre that
received a referred patient must provide a report / medical information /
feedback to the hospital / primary heath centre / village maternity clinic
that referred the patient concerning the patient’s most recent clinical
condition. This also includes providing information on a patient’s death
and its cause.
b. Administrative Procedure:
1) The hospital / primary health centre caring for the patient must prepare a
back referral letter (see form R/1/b attached) for each referral patient
received, for the hospital / primary heath centre / village maternity clinic
that referred the patient.

22
2) The back referral letter may be delivered via the patient’s family, and
confirmation of the back referral information may be made by the health
personnel to whom it is addressed by any means, including telephone,
mobile, fax, etc.
3) Hospitals must complete quarterly reports, using form RL.1 (page 6,
point 24.3).
4. Standard procedure for receiving back referral patients.
a. Clinical procedure:
1) Visit the patient’s home and conduct a physical examination.
2) Take note of the action recommended by the hospital / primary health
centre that last cared for the patient.
3) Carry out public health follow up or care, and follow up on the clinical
condition of the patient until he or she has recovered. This includes
making home visits and should include IEC measures to avoid
preventable disease episodes in the future.
b. Administrative Procedure:
1) Examine the content of the back referral letter and record this
information in the referral patient register, then date and file the letter in
the patient’s medical record.
2) Immediately confirm receipt of the back referral letter with the doctor that
sent the patient.
B. Referring Specimens and Receiving Specimen Referrals.
Specimen examination may be referred if the examination requires more
laboratory equipment / expertise, and the specimen can be sent and examined
without the patient accompanying. The hospital or health unit that receives the
specimen referral must send a report of the results of the specimen
examination after it has been examined.
23
1. Standard procedure for sending specimen referrals.
a. Clinical procedure.
1) Package the specimen appropriately with due regard for sterility,
communicable disease contamination, the safety of the patient and
others, and in a manner suitable for the examination required.
2) Ensure that the specimen sent is in a suitable condition and its
identification is clear and unique for each.
b. Administrative Procedure.
1) Complete the form and specimen referral letter (see form R/3 attached) accurately and clearly, including letter reference number,
status of the patient (poor/not poor, Askes/Jamsostek health
insurance), information about the specimen, the examination
required, the identity of the patient, the preliminary diagnosis, and
the identity of the sender.
2) Record information required in the appropriate register.
3) Send the specimen referral letter to the target, and file the copy.
4) Monitor the estimated time of return of the referred specimen.
2. Standard procedure for receiving specimen referrals.
a. Clinical procedure.
1) Receive and examine the specimen in a manner appropriate to the
condition in which it is received, with due regard for: sterility,
communicable disease contamination, the safety of the patient and
others, and in a manner suitable for the examination required.
2) Ensure that the specimen is in a suitable condition to be examined as
requested.
3) Perform the standard laboratory or pathological examination, as per the
type and method of examination requested by the sender.
4) Make a written report of the results of the examination using the unit's
standard format to the head of administration.

24
b. Administrative Procedure.
1) Check the content of the specimen referral letter accurately and clearly,
including letter reference number, status of the patient (poor/not poor,
Askes/Jamsostek health insurance), information about the specimen,
the examination required, the identity of the patient, the preliminary
diagnosis, and the identity of the sender.
2) Record the necessary information in the appropriate unit register / file. 3) Make sure that confidentiality is guaranteed
3. Standard procedure for back referral of specimen examination results.
a. Clinical Procedure.
1) Ensure that standard and complete examination has been made of the
specimen as requested in the accompanying specimen referral letter.
2) Ensure that the results of the examination are accountable.
3) Double check that no mix-up and confusion between several specimen
can happen
b. Administrative Procedure.
1) Record the results of the examination in the register for filing.
2) Complete the unit's appropriate examination results report form.
3) Ensure that the results of the examination remain confidential and reach
the intended recipient.
4) Immediately send the results of the examination to the address of the
sender, and confirm by any communication means available that the
report has been received.

25
C. Knowledge / Specialist Referral.
Knowledge referrals may take the form of requests for and dispatch of
specialists in a particular field. A request may come from a primary health
centre or district / municipal general hospital and be directed to a hospital or
regional health office that is able to provide the specialist required.
Parties involved in specialist referrals include:
1) The hospital / primary health centre that requires the specialist, for example
a district / municipal general hospital.
2) The hospital / health facility that is able to provide the specialist, for
example the provincial general hospital.
3) The head of the district / municipal health office in which the hospital /
primary health centre requiring the specialist is located.
4) The head of the provincial health office in which the hospital that will be
providing the specialist is located.
The scope of specialist referrals includes:
1) Clinical guidance for early detection of referral cases.
2) Clinical guidance for pre-referral measures.
3) Clinical guidance for management of cases that are within the scope of
authority of primary health centres that provides basic obstetric and
neonatal services.
4) Clinical guidance for follow up of back referral cases received by primary
health centres, auxiliary primary health centres and village maternity clinics.
5) Short courses or refresher courses on clinical handling of common cases in
primary health centres, auxiliary primary health centres and village
maternity clinics.

26
1. Standard Procedure for Knowledge (Specialist) Referrals
a. The primary health centre / district/municipal hospital requiring the
specialist prepares a specialist request letter.
b. The request is directed to the head of the district / municipal health office
or the West Nusa Tenggara Provincial Health Office.
c. The head of the district/municipal health office or the provincial health
office forwards this request for a specialist to the director of the hospital
concerned, with a copy to the head of functional medical staff, within 14
days of receipt of the letter of request.
d. Prepare to receive the specialist, including agenda, accommodation,
honorarium or other incentives, as per local regulations.
e. Undertake monitoring and evaluation of the process and its
implementation.
f. Prepare an implementation report for the head of the local health office,
with a copy to the hospital or health facility sending the specialist.
g. Hospitals must complete quarterly reports on form RL.1 (page 6, point
24.2).
2. Standard Procedure for Sending Specialists
a. The hospital / health facility sending the specialist consults with the
provincial health office to match the request with the province's referral
program.
b. Upon approval from the provincial health office, the hospital / health
facility prepares a schedule for the visit and a letter of instruction for the
specialist as requested.
c. Evaluate and prepare implementation report, send to the provincial
health office, with a copy to the file.
d. Hospitals complete quarterly report form RL.1 (page 6, point 24.1).

27
D. Procedure for Monitoring and Evaluation of the Implementation of the Referral System.
Parties involved in the referral system are required to undertake monitoring
and evaluation as follows:
1) Collect data and information about the referral services that have been
provided by the health service unit.
2) The head of the health service unit prepares a referral system
implementation report (form R/4 for primary health centres and form RL1 for
hospitals), dan patient referral implementation report (form R/5/a, b, c and
R/6 attached.)
3) The report is typed, double space, and signed, in duplicate.
4) The top copy of the report is sent to the local health office as input for
evaluation of the implementation of the referral system.
5) The second copy of the report is filed by the health service unit.
Responsibility for monitoring and evaluation of the implementation of the
referral system lays with the head of the provincial health office and the heads
of district/municipal health offices. The role and tasks of personnel in the
district/ offices municipal and provincial health include:
1) Making regular visits to village maternity clinics, village health posts,
auxiliary primary health centres, health centres and hospitals, guided by
the monitoring and evaluation forms (forms R/5/a, b, c and R/6, attached).
2) Receive, read, study and assess reports from all health units in its area,
and reports from other sources, concerning problems with implementation
of the referral system.
3) Make decisions as to whether or not it is necessary to conduct a field
investigation. If necessary, a field visit must be conducted immediately,
and a report of its findings prepared.
4) Prepare periodic reports on the condition of the referral system in its area.
5) Reports of district/municipal health offices are submitted to the Head of
the West Nusa Tenggara Provincial Health Office.

28
CHAPTER IV
PRINCIPLES OF REFERRAL OF OBSTETRIC AND NEONATAL EMERGENCIES
Emergency obstetric and neonatal referral services are based on the
principle of: rapid and appropriate, efficient and effective response within the capacity and authority of the service facility.
A. Authority of Service Facilities
1. Village Maternity Clinics Village maternity clinics are one type of community-based health
measure set up by the community based on deliberated consensus.
The midwife in a village is the provider of village maternity clinic
services, and also the spearhead of maternal and neonatal health
measures that require basic knowledge of danger signs so that emergency
cases can be referred as soon as possible to a more suitably equipped
service unit once the patient is stabilised (pre-referral measures).
As well as providing normal delivery services, the midwife in a village
may also handle cases involving certain complications depending on her
level of authority and competence, or make referrals to primary health
centres, primary health centres with basic obstetric and neonatal facilities
(PONED), and hospitals with comprehensive obstetric and neonatal
facilities (PONEK).
The roles and functions of the village midwifery clinic include the
following:
1) A place providing maternal and child health services, and other health
services.
2) A place for guidance and extension activities and personal counselling
on maternal and child health.
3) The centre of community empowerment in maternal and child health.
4) The centre for partnerships with traditional birthing assistants (dukun
bersalin). In providing antenatal and postnatal examination services and

29
assisting deliveries at the village midwifery clinic, the midwife in the
village is expected to make use of these opportunities to forge
partnerships with traditional birthing assistants.
5) Providing off-site services. The midwife in the village not only provides
health services on site in the clinic, but also off site, for example doing
home visits, etc.
The type and scope of maternal and neonatal health services provided
at the village midwifery clinic include:
a. Antenatal check-ups, which include measuring body weight, blood
pressure and fundal height, administering tetanus toxoid immunisations,
supplying iron tablets, having face-to-face contact, and administering
urine tests (the so-called ’7T’ in Indonesian).
b. Delivery preparation
c. Prevention of postpartum and neonatal infection
d. Assisting normal deliveries
e. Postnatal check-ups, including initiating early breastfeeding
f. Neonatal health services (umbilical cord care, eye ointment, vitamin K
injections, first hepatitis B immunisation)
g. Integrated neonatal services (MTBM) and integrated management of
infant diseases (MTBS)
h. Contraceptive services for women of fertile age
i. Administering first aid in obstetric and neonatal emergencies the midwife
is qualified to perform, including:
(1) Stabilising obstetric and neonatal emergency patients
(2) Applying bimanual pressure to women with postpartum
haemorrhage.
(3) Manual extraction of the placenta in cases of placental retention
(4) Digital curettage in cases of partial placental retention
(5) Simple resuscitation in cases of neonatal asphyxia.
(6) Application of the kangaroo method for babies with a birth weight of
more than 2000 grams.
j. Making maternal and neonatal patient referrals

30
2. Standard primary health centres In terms of maternal and child health services, primary health
services are divided into primary health centres with basic obstetric and
neonatal facilities and standard primary health centres, which are primary
health centres that do not provide obstetric and neonatal services. The
function of standard primary health centres is similar to that of village
midwifery clinics, but they have more health personnel and more adequate
facilities and equipment, such as doctors, midwives, nurses, vehicles, etc.
Standard primary health centres may assist normal deliveries;
manage cases presenting certain complications according to their authority
and expertise, or make referrals to primary health centres with basic
obstetric and neonatal facilities and hospitals with comprehensive obstetric
and neonatal facilities.
Standard primary health centres must at least be able to stabilise
obstetric and neonatal emergency patients who come to the centre
voluntarily or are referred by a village midwife or traditional birth attendent
assistant/cadre, before being referred to a primary health centre with basic
obstetric and neonatal facilities or a hospital with comprehensive obstetric
and neonatal facilities.
The type and scope of maternal and neonatal health services provided
at standard primary health centres include:
a. Antenatal check-ups, which include measuring body weight, blood
pressure and fundal height, administering tetanus toxoid immunisations,
supplying iron tablets, having face-to-face contact, and administering
urine tests (the so-called ’7T’ in Indonesian).
b. Delivery preparation
c. Prevention of postpartum and neonatal infection
d. Assisting normal deliveries
e. Postnatal check-ups, including initiating early breastfeeding
f. Neonatal health services (umbilical cord care, eye ointment, vitamin K
injections, first hepatitis B immunisation)
g. Integrated neonatal services (MTBM) and integrated management of
infant diseases (MTBS)

31
h. Contraceptive services for women of fertile age
i. Administering first aid in obstetric and neonatal emergencies the midwife
is qualified to perform, including:
(1) Stabilising obstetric and neonatal emergency patients
(2) Applying bimanual pressure to women with postpartum
haemorrhage.
(3) Manual extraction of the placenta in cases of placental retention
(4) Digital curettage in cases of partial placental retention
(5) Simple resuscitation in cases of neonatal asphyxia.
(6) Application of the kangaroo method for neonates with a birthweight
of more than 2000 grams.
j. Making maternal and neonatal patient referrals
3. Primary health centres with basic obstetric and neonatal facilities
A primary health centres with basic obstetric and neonatal facilities is
a primary health centre that has a team of competent, trained and qualified
doctors and midwives and adequate facilities and equipment for providing
basic obstetric and neonatal services.
Primary health centres with basic obstetric and neonatal services
provide antenatal, delivery, postnatal and neonatal services to walk-in
patients and to patients referred by standard primary health centres, village
midwives, or cadres/traditional birthing assistants.
Primary health centres with basic obstetric and neonatal facilities
may assist deliveries or neonates presenting certain complications
according to their authority and expertise, or make referrals to hospitals with
comprehensive obstetric and neonatal facilities.
The type and scope of maternal and neonatal health services
provided by primary health centres with basic obstetric and neonatal
facilities include:
a. Antenatal check-ups, which include measuring body weight, blood
pressure and fundal height, administering tetanus toxoid immunisations,
supplying iron tablets, having face-to-face contact, and administering
urine tests (the so-called ’7T’ in Indonesian).

32
b. Delivery preparation
c. Prevention of postpartum and neonatal infection
d. Assisting normal deliveries
e. Postnatal check-ups, including initiating early breastfeeding
f. Neonatal health services (umbilical cord care, eye ointment, vitamin K
injections, first hepatitis B immunisation)
g. Integrated neonatal services (MTBM) and integrated management of
infant diseases (MTBS)
h. Contraceptive services for women of fertile age
i. Administering first aid in obstetric and neonatal emergencies the midwife
is qualified to perform, including:
(1) Stabilising obstetric and neonatal emergency patients
(2) Administering oxytocin parenterally or by intravenous drip
(3) Administering antibiotics by injection or intravenous injection
(4) Managing postpartum haemorrhage
(5) Performing manual extraction of the placenta in cases of placental
retention
(6) Performing curettage in cases of partial placental retention
(7) Management of pre-eclampsia / eclampsia by administering MgSO4
(8) Assisting breech presentation deliveries
(9) Assisting deliveries presenting shoulder dystocia
(10) Performing vacuum extractions and forceps extractions in cases of
partus protractus
(11) Management of postpartum infection
(12) Resuscitation in cases of neonatal asphyxia
(13) Management of neonates of low birthweight (1500 - 2500 grams)
(14) Management of neonatal hypothermia
(15) Management of neonatal hypoglycaemia
(16) Management of neonatal icterus
(17) Management of neonatal feeding problems
(18) Management of neonatal breathing problems
(19) Management of neonatal convulsions
(20) Management of neonatal infection
j. Making maternal and neonatal referrals
33
k. Hospitals with Comprehensive Obstetric and Neonatal Facilities In maternal and neonatal health services there are also hospitals
with comprehensive obstetric and neonatal facilities (PONEK). This is a
hospital that provide 24-hour obstetric and neonatal services and has a
team of competent and qualified obstetricians, paediatricians, and
midwives, and adequate supporting facilities and equipment to provide
basic and comprehensive emergency obstetric and neonatal services to
provide antenatal, delivery, postnatal and neonatal services to walk-in
patients and to patients referred by primary health centres with basic
obstetric and neonatal facilities, standard primary health centres, village
midwifery clinics, or members of the public/cadres/traditional birth
attendants.
In general hospitals with comprehensive obstetric and neonatal
services are district/municipal general hospitals that obstetricians and
paediatricians on staff.
The scope of maternal and neonatal health services provided at
hospitals with comprehensive obstetric and neonatal facilities is all obstetric
and neonatal services, including blood transfusions, caesarean sections,
and intensive neonatal care.
B. The Principles of Making and Receiving Maternal and Neonatal Patient Referrals
The procedure for making and receiving maternal and neonatal referrals is
based on these principles:
1) Avoiding delayed decision, delayed referral and delayed assistance (the so-
called ’3T’ in Indonesian). Maternal and neonatal referrals are emergency
patients and must be given immediate assistance.
2) Planned referrals. Patients who have been prepared for possible referral from
the first or any later antenatal check-up according to defined risks.
3) Stabilising the patient. Health personnel must stabilise the patient before
referring the patient.

34
4) Not within the competency of the personnel. A patient must be referred if the
patient requires care that the facility concerned does not have the authority to
administer.
5) Early communication. Make early contact with the facility that will be receiving
the referred patient to guard against the possibility of the facility not being able
to manage the patient or there being a delay in management of the patient
because the specialists required are not available.
The clinical procedure and administrative procedure for maternal and
neonatal patient referrals are the same as those for other patient referrals.
However, maternal and neonatal referral patients may go through the emergency
unit or directly to the on-call obstetric and neonatal polyclinic or the hospital’s
delivery room, or the day-time obstetric and neonatal polyclinic.
For maternal and neonatal patient referrals use the standard form for
patient referrals (see form R/1 attached).
The administrative and clinical procedures for receiving and making back
referrals of maternal and neonatal patients follow the standard procedure for back
referrals. If the patient is released from care / the hospital, use form R/1/b (attached) to prepare a back referral report to be sent to the party making the
referral.

35
CHAPTER V
CONCLUSION
These Technical Guidelines on Health Referral Services in West Nusa
Tenggara Province are based on Ministry of Health handbooks, the results of an
assessment of the referral system conducted by consultants from West Nusa
Tenggara University, and other sources.
Through two workshops at the provincial level and numerous discussions of
the internal design team, it has been agreed that these technical guidelines will be
piloted in Lombok Barat District in the fourth quarter of 2008, in 19 primary health
centres, 78 auxiliary primary health centres, 94 village maternity clinics, Patuh
Patut Patju General Hosptial in Lombok Barat District, and the Provincial General
Hospital in Mataram. The aim of this trial is to identify the feasibility of adopting
these guidelines in the field, for adoption across the board by all health facilities in
West Nusa Tenggara Province. After evaluation they final form will be adapted and
widely spread to all districts.
-f-

36
BIBLIOGRAPHY
1. Ministry of Health, Republic of Indonesia:
Guidelines for Development and Supervision of Health Service Referral Systems in Indonesia. Directorate of Hospitals, Ministry of Health. Jakarta. 1978
2 Ministry of Health, Republic of Indonesia:
Guidelines for Maternal and Neonatal Referral Systems at the District/Municipal Level. Directorate General of Public Health. Jakarta. 2005.
3 Ministry of Health, Republic of Indonesia:
Hospital Information Systems in Indonesia (Hospital Reporting System Revision V), Decree of the Minister of Health 1410/Menkes/SK/X/2003, dated 1 October 2003. Directorate General of Medical Services. Jakarta. 2003.
4. UNTB Research Unit, GTZ Siskes:
Report on the Assessment of the Health Referral System in West Nusa Tenggara Province. Cooperation between West Nusa Tenggara University Research Centre and GTZ-SISKES Mataram. 2007.