Embed Size (px)
Citation preview
Course Outline and Syllabus for Students
Name: Bioequivalence
Course Number: PHM362
Course Title: Assessing the Bioavailability and Bioequivalence of Medicinal Drug Products
Course Description: This course introduces regulatory, clinical, statistical, and logistical considerations in assessing the relative bioavailabilities of formulations. A heavy emphasis is placed on clinical trial design, and biostatistics involved in second entry drug applications to regulatory bodies. Students will learn about the methods, regulations, techniques, pharmacokinetics, and biostatistics involved in creating bioequivalence studies, at an introductory level. The course has a heavy mathematical bias, with a component dedicated to mathematical modeling and basic programming in R-project, an open source statistical package. After taking this course, students will understand the steps required to set up single-dose or steady-state pilot and pivotal bioequivalence trials using parallel, crossover, and replicate designs. Students will be able to take a data set of plasma concentrations and be able to process and interpret the results of the trial. Students will gain a deeper understanding and context of the regulatory differences involved in generic drug testing between Canada, the United States, and Europe.
Required: PHM141H1; PHM144H1; PHM241H1
Elective:
Semester: Fall
Enrolment: No maximum (target: 48 students)
1. Course Learning Objectives:
Upon completion of this course, students will have achieved the following level of learning objectives:
Introductory = knowledge and comprehension of concepts, definitions, Intermediate = application of concepts to simple situations Advanced = application of concepts to more complex situations with ability to synthesize and evaluate
Knowledge Introductory Level:
• Understand the historical regulatory treatment of generic drug products
• Describe the common pharmacokinetic parameters required for reporting in bioequivalence trials
• Recognize the basic concepts of the statistical power of a test, sensitivity, and Type I and II errors
• Identify which regulatory guidances pertain to bioequivalence clinical trial design in Canada, the United States, and Europe. Become familiar with where these guidances are posted, and how to access and understand them
• Describe the proper meaning and use of standard deviation, coefficient of variation, standard error, and 90% confidence interval
Intermediate Level:
• Understand the proper use of basic clinical trial structures: equivalence, bioequivalence, superiority, non-inferiority
• Be able to state and implement regulatory approaches dealing with subjects removed due to adverse events, and specific adverse events such as vomiting and diarrhea
Advanced Level: Skills
Introductory Level:
• Identify the appropriate reference drug product depending on the country of submission.
• Selecting key clinical trial parameters (e.g. fasted vs. fed, appropriate study population). Intermediate Level:
• Be able to perform basic noncompartmental pharmacokinetic analysis on analytical data, including fitting Cmax, AUCt,
AUCinf, λ, and t1/2.
• Understand how to adjust for missed sampling times, concentrations reported as below the limit of quantitation during pharmacokinetic parameter estimation
• Calculate appropriate sample sizes, including adjustments for anticipated drop-outs and withdrawals, using literature estimates of the inter- and intrasubject variabilities of the appropriate pharmacokinetic parameters
• Selecting the appropriate analyte of study and required analytical sensitivity
• Estimate the appropriate washout period for crossover and replicate trials Advanced Level:
• Characterize the expected pharmacokinetic parameters of a given drug, and the anticipated variabilities of parameters involved in the assessment of bioequivalence
• Use course-developed programs in MS Excel and R-project for sample size determination, and compartmental model fitting
• Given simulated clinical trial data, calculate the 90% confidence intervals of the Test/Reference ratios of Cmax, AUCt, and AUCinf and determine whether or not the trial passed
• Correctly assess and interpret ANOVA output including the detection of period, sequence, and treatment effects
• Become familiarized with and develop a working knowledge of common concepts employed in outlier analysis, including use of the Shapiro-Wilk test, Grubb’s test, R-studentized Residuals Test, and bootstrapping
• Assess the goodness of fit of a model
Attitudes/Values
Introductory Level:
• Understand how ethics are involved in human clinical trials, including concepts such as informed consent and Institutional Review Board review/approval
• Understand the ethics involved in selecting a sample size and population appropriate for the drug of study
• Realize the complexity of regulatory requirements concerning generic drug products Intermediate Level: Advanced Level: 2. Rationale for Inclusion in the Curriculum:
Pharmacists are frequently asked by the public whether or not generic drugs work as well as innovator products. Drug plans typically cover the generic version of drugs and not the innovator product. It is very important for the pharmacist to understand the process and endpoints of generic drug testing, and to have a more than an anecdotal understanding of whether or not generic drug products are truly interchangeable. In some circumstances, critical dose drugs (e.g. warfarin, cyclosporine) are deemed bioequivalent under more stringent criteria in Canada; however, should still not be interchanged in the middle of a drug therapy regimen. A thorough understanding of the regulatory and biostatistical treatment of clinical trial data will bring pharmacokinetic issues to light, such as non-linear pharmacokinetics, fast-onset drugs, therapeutic drug monitoring, and narrow therapeutic range drugs. This course will equip the pharmacist with a solid working knowledge of how generic drug products are assessed, and to what extent pharmacokinetics is used as a surrogate marker for drug efficacy. It is a very applied extension of the introductory course PHM144H1, with a heavy industrial perspective.
3. Pre-requisites:
PHM141H1 (Pharmaceutics):
Course outline: This course will focus on the biopharmaceutical considerations and physicochemical foundation of dosage forms, and will include discussion on the various drug dosage forms. Discussion will include preformulation factors (melting point, solubility, viscosity, dissolution, particle and solid state properties), rheology, pharmaceutical solutions, colloids and dispersions, complexation, chelation, and protein binding, solid dosage forms, topicals, and other delivery systems.
Connection with This Proposed Course: Pharmaceutics concepts lay a foundation of the theory behind drug delivery. Small formulation differences often result in therapeutic differences, which has resulted in using drug pharmacokinetic behaviour to assess bioequivalence and relative bioavailability. This course will draw on historical examples of problematic historical formulation differences, such as digoxin and chloramphenicol.
PHM144H1 (Pharmacokinetics):
Course Outline: This course will examine how physiologic and biochemical processes influence the fate of drugs in the body. The interrelationship between the physiochemical properties of the drug and the rate/extent of absorption will be explored. Mathematical modeling of the plasma concentration time curves following drug administration will constitute a major part of the course. Fundamental pharmacokinetic principles and quantitative relationships will be used to determine approaches in designing dosage regimens, evaluating pharmacologic response and explaining mechanisms of drug-drug interactions. The resulting theory will form the basis for selecting a particular route of drug administration, determining the frequency of administration and identifying patient factors which require a modification of normal drug dosing regimen.
Connection with This Proposed Course: A foundation in pharmacokinetics will be a useful springboard when discussing noncompartmental pharmacokinetics and model fitting. Knowledge of drug absorption, distribution, metabolism, excretion, and drug-drug interactions become invaluable in planning bioequivalence clinical trials.
PHM241H1 (Topics in Pharmaceutical Quality and Clinical Laboratory Medicine):
Course Outline: This course will provide an introduction to pharmaceutical analysis and discuss the importance of assuring the pharmaceutical quality of medicinal products with an emphasis on establishment of quality control assays and specifications, bioequivalence testing of generic drugs, special considerations for biopharmaceutical products, and the regulatory process in Canada. In addition, the course will discuss the application of analytic techniques in clinical laboratory medicine with a focus on commonly used tests to monitor patient health and the therapeutic use of drugs, including tests for personalized drug therapy. The course includes a laboratory component which will present drug formulation and related quality control issues.
Connection with This Proposed Course: The lecture component of this course specifically deals with bioequivalence in a very introductory manner. This provides an excellent seguay into the elective. In addition, concepts in the laboratory component, such as drug dissolution and reformulation, will provide a good foundation for discussions in this elective.
4. Statement of agreement from course coordinators of courses for which this course is a pre-requisite: None.
5. Co-requisites: (for the current and subsequent year) None.
6. Statement of agreement from coordinators of courses for which this course is a co-requisite:
Not applicable.
7. Course Contact Hours and Teaching Methodologies:
Didactic (lecture) 24 hours
Large group problem-based or case-based learning 0 hours
Large Group Size (eg 30, 60, 120, 240) Up to 240 persons (The second half of Section 4 will be taught in smaller groups of 20-60, depending on the class size)
Laboratory or Simulation 0 hours
Tutorial/Seminar/Workshop/Small Group 2 hours
Small Group Size (eg 5, 10, 15, 20, 25) 0 persons
Experiential 0 hours
On-line 0 hours
Other (please specify)* 0 hours
* Other specific information:
Total course contact hours 26 hours
Notes: A laptop computer or netbook is recommended for the in-class workshop using Microsoft Excel® and R-project.

8. Estimate and description of student's weekly out-of-class preparation time excluding exam preparation:
Two hours a week to work on course problem sets.
9. Course Coordinator and contact information:
Dr. David Dubins. Room PB 802. Tel 416-946-5303. E-mail: [email protected]
10. Course Instructors and contact information:
Dr. David Dubins. Room PB 802. Tel 416-946-5303. E-mail: [email protected]
11. Required Resources/Textbooks/Readings:
None. PowerPoint notes, programs, and links to required resources will be provided.
12. Recommended Resources/Textbooks/Readings:
Links to regulatory guidances pertaining to relative bioavailability and bioequivalence will be provided.
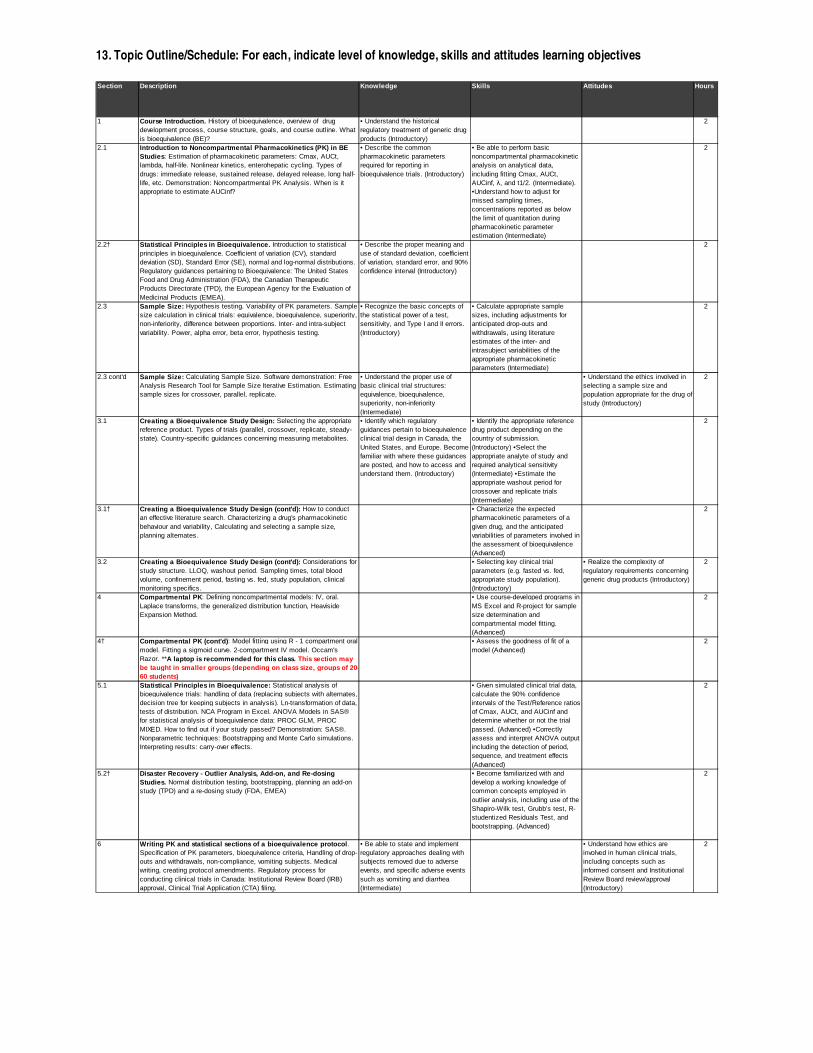
13. Topic Outline/Schedule: For each, indicate level of knowledge, skills and attitudes learning objectives
Section Description Knowledge Skills Attitudes Hours
1 Course Introduction. History of bioequivalence, overview of drug development process, course structure, goals, and course outline. What is bioequivalence (BE)?
• Understand the historical regulatory treatment of generic drug products (Introductory)
2
2.1 Introduction to Noncompartmental Pharmacokinetics ( PK) in BE Studies : Estimation of pharmacokinetic parameters: Cmax, AUCt, lambda, half-life. Nonlinear kinetics, enterohepatic cycling. Types of drugs: immediate release, sustained release, delayed release, long half-life, etc. Demonstration: Noncompartmental PK Analysis. When is it appropriate to estimate AUCinf?
• Describe the common pharmacokinetic parameters required for reporting in bioequivalence trials. (Introductory)
• Be able to perform basic noncompartmental pharmacokinetic analysis on analytical data, including fitting Cmax, AUCt, AUCinf, λ, and t1/2. (Intermediate). •Understand how to adjust for missed sampling times, concentrations reported as below the limit of quantitation during pharmacokinetic parameter estimation (Intermediate)
2
2.2† Statistical Principles in Bioequivalence. Introduction to statistical principles in bioequivalence. Coefficient of variation (CV), standard deviation (SD), Standard Error (SE), normal and log-normal distributions. Regulatory guidances pertaining to Bioequivalence: The United States Food and Drug Administration (FDA), the Canadian Therapeutic Products Directorate (TPD), the European Agency for the Evaluation of Medicinal Products (EMEA).
• Describe the proper meaning and use of standard deviation, coefficient of variation, standard error, and 90% confidence interval (Introductory)
2
2.3 Sample Size: Hypothesis testing. Variability of PK parameters. Sample size calculation in clinical trials: equivalence, bioequivalence, superiority, non-inferiority, difference between proportions. Inter- and intra-subject variability. Power, alpha error, beta error, hypothesis testing.
• Recognize the basic concepts of the statistical power of a test, sensitivity, and Type I and II errors. (Introductory)
• Calculate appropriate sample sizes, including adjustments for anticipated drop-outs and withdrawals, using literature estimates of the inter- and intrasubject variabilities of the appropriate pharmacokinetic parameters (Intermediate)
2
2.3 cont'd Sample Size: Calculating Sample Size. Software demonstration: Free Analysis Research Tool for Sample Size Iterative Estimation. Estimating sample sizes for crossover, parallel, replicate.
• Understand the proper use of basic clinical trial structures: equivalence, bioequivalence, superiority, non-inferiority (Intermediate)
• Understand the ethics involved in selecting a sample size and population appropriate for the drug of study (Introductory)
2
3.1 Creating a Bioequivalence Study Design: Selecting the appropriate reference product. Types of trials (parallel, crossover, replicate, steady-state). Country-specific guidances concerning measuring metabolites.
• Identify which regulatory guidances pertain to bioequivalence clinical trial design in Canada, the United States, and Europe. Become familiar with where these guidances are posted, and how to access and understand them. (Introductory)
• Identify the appropriate reference drug product depending on the country of submission. (Introductory) •Select the appropriate analyte of study and required analytical sensitivity (Intermediate) •Estimate the appropriate washout period for crossover and replicate trials (Intermediate)
2
3.1† Creating a Bioequivalence Study Design (cont'd): How to conduct an effective literature search. Characterizing a drug's pharmacokinetic behaviour and variability, Calculating and selecting a sample size, planning alternates.
• Characterize the expected pharmacokinetic parameters of a given drug, and the anticipated variabilities of parameters involved in the assessment of bioequivalence (Advanced)
2
3.2 Creating a Bioequivalence Study Design (cont'd): Considerations for study structure. LLOQ, washout period. Sampling times, total blood volume, confinement period, fasting vs. fed, study population, clinical monitoring specifics.
• Selecting key clinical trial parameters (e.g. fasted vs. fed, appropriate study population). (Introductory)
• Realize the complexity of regulatory requirements concerning generic drug products (Introductory)
2
4 Compartmental PK : Defining noncompartmental models: IV, oral. Laplace transforms, the generalized distribution function, Heaviside Expansion Method.
• Use course-developed programs in MS Excel and R-project for sample size determination and compartmental model fitting. (Advanced)
2
4† Compartmental PK (cont'd) : Model fitting using R - 1 compartment oral model. Fitting a sigmoid curve. 2-compartment IV model. Occam's Razor. **A laptop is recommended for this class. This section may be taught in smaller groups (depending on class siz e, groups of 20-60 students)
• Assess the goodness of fit of a model (Advanced)
2
5.1 Statistical Principles in Bioequivalence: Statistical analysis of bioequivalence trials: handling of data (replacing subjects with alternates, decision tree for keeping subjects in analysis). Ln-transformation of data, tests of distribution. NCA Program in Excel. ANOVA Models in SAS® for statistical analysis of bioequivalence data: PROC GLM, PROC MIXED. How to find out if your study passed? Demonstration: SAS®. Nonparametric techniques: Bootstrapping and Monte Carlo simulations. Interpreting results: carry-over effects.
• Given simulated clinical trial data, calculate the 90% confidence intervals of the Test/Reference ratios of Cmax, AUCt, and AUCinf and determine whether or not the trial passed. (Advanced) •Correctly assess and interpret ANOVA output including the detection of period, sequence, and treatment effects (Advanced)
2
5.2† Disaster Recovery - Outlier Analysis, Add-on, and R e-dosing Studies. Normal distribution testing, bootstrapping, planning an add-on study (TPD) and a re-dosing study (FDA, EMEA)
• Become familiarized with and develop a working knowledge of common concepts employed in outlier analysis, including use of the Shapiro-Wilk test, Grubb’s test, R-studentized Residuals Test, and bootstrapping. (Advanced)
2
6 Writing PK and statistical sections of a bioequival ence protocol . Specification of PK parameters, bioequivalence criteria, Handling of drop-outs and withdrawals, non-compliance, vomiting subjects. Medical writing, creating protocol amendments. Regulatory process for conducting clinical trials in Canada: Institutional Review Board (IRB) approval, Clinical Trial Application (CTA) filing.
• Be able to state and implement regulatory approaches dealing with subjects removed due to adverse events, and specific adverse events such as vomiting and diarrhea (Intermediate)
• Understand how ethics are involved in human clinical trials, including concepts such as informed consent and Institutional Review Board review/approval (Introductory)
2
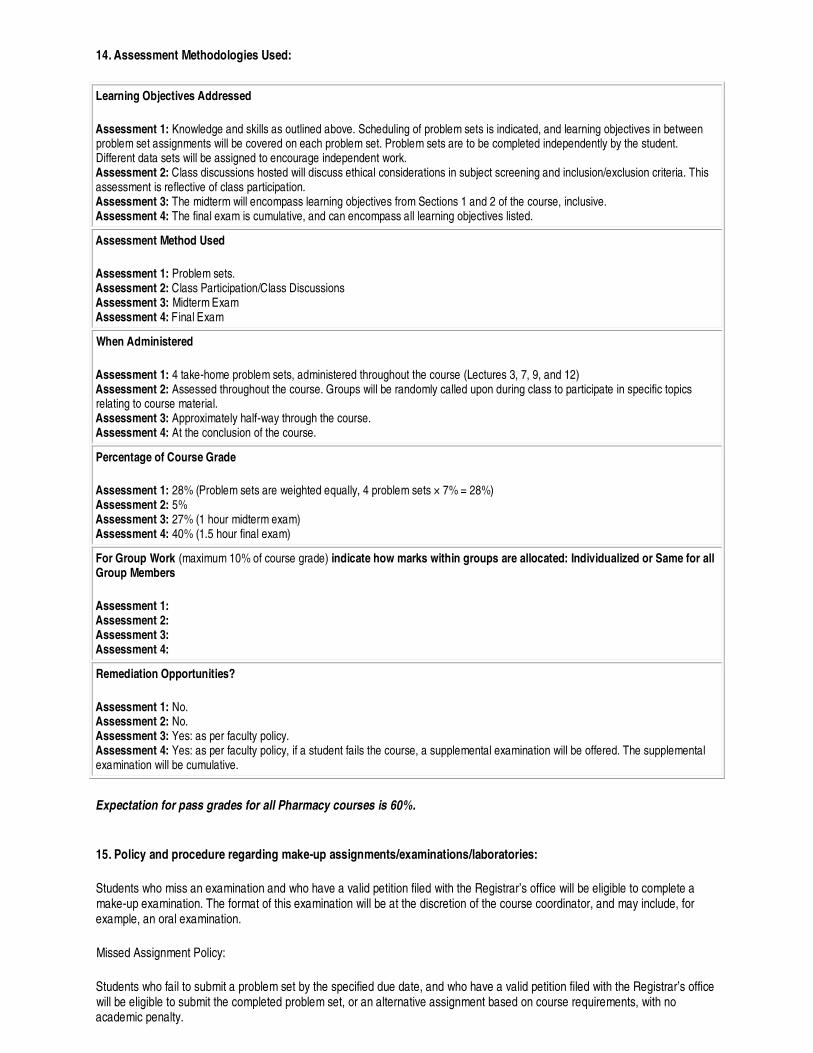
14. Assessment Methodologies Used:
Learning Objectives Addressed
Assessment 1: Knowledge and skills as outlined above. Scheduling of problem sets is indicated, and learning objectives in between problem set assignments will be covered on each problem set. Problem sets are to be completed independently by the student. Different data sets will be assigned to encourage independent work. Assessment 2: Class discussions hosted will discuss ethical considerations in subject screening and inclusion/exclusion criteria. This assessment is reflective of class participation. Assessment 3: The midterm will encompass learning objectives from Sections 1 and 2 of the course, inclusive. Assessment 4: The final exam is cumulative, and can encompass all learning objectives listed.
Assessment Method Used
Assessment 1: Problem sets. Assessment 2: Class Participation/Class Discussions Assessment 3: Midterm Exam Assessment 4: Final Exam
When Administered
Assessment 1: 4 take-home problem sets, administered throughout the course (Lectures 3, 7, 9, and 12) Assessment 2: Assessed throughout the course. Groups will be randomly called upon during class to participate in specific topics relating to course material. Assessment 3: Approximately half-way through the course. Assessment 4: At the conclusion of the course.
Percentage of Course Grade
Assessment 1: 28% (Problem sets are weighted equally, 4 problem sets × 7% = 28%) Assessment 2: 5% Assessment 3: 27% (1 hour midterm exam) Assessment 4: 40% (1.5 hour final exam)
For Group Work (maximum 10% of course grade) indicate how marks within groups are allocated: Individualized or Same for all Group Members
Assessment 1: Assessment 2: Assessment 3: Assessment 4:
Remediation Opportunities?
Assessment 1: No. Assessment 2: No. Assessment 3: Yes: as per faculty policy. Assessment 4: Yes: as per faculty policy, if a student fails the course, a supplemental examination will be offered. The supplemental examination will be cumulative.
Expectation for pass grades for all Pharmacy courses is 60%.
15. Policy and procedure regarding make-up assignments/examinations/laboratories:
Students who miss an examination and who have a valid petition filed with the Registrar’s office will be eligible to complete a make-up examination. The format of this examination will be at the discretion of the course coordinator, and may include, for example, an oral examination.
Missed Assignment Policy:
Students who fail to submit a problem set by the specified due date, and who have a valid petition filed with the Registrar’s office will be eligible to submit the completed problem set, or an alternative assignment based on course requirements, with no academic penalty.

Late Assignment Policy:
Students who fail to submit a problem set by the specified due date will receive a deduction of 10% for each day beyond the due date (including weekends/holidays), to a maximum of 50%. Assignments will not be accepted for grading after 7 late calendar days.
16. Policy and procedure regarding supplemental assignments/examinations/laboratories:
Supplemental final examinations will be cumulative, covering lecture material. The format of this examination or test will be at the discretion of the course coordinator, and may include, for example, an oral examination.

SECTION TWO GUIDELINES:
INFORMATION FOR CURRICULUM COMMITTEE REVIEW AND APPROVAL
Constructs for Delivering Curriculum Outcomes
The curriculum is based on educating a professional pharmacist graduate who is fully competent in each of seven AFPC outcomes that, taken as a whole, define the role of the pharmacist in a national framework for training and assessment: Care Provider; Communicator; Collaborator; Manager; Advocate; Scholar; Professional. Please indicate the overall level (see chart above) and individual components (see Appendix), Each of these roles may involve elements of five curricular themes, including Patient Safety, Pharmaceutical Care/Patient Care process, Professionalism and Ethics, Critical Reasoning and Critical Appraisal. Indicate all that will be integrated in your course. For the purposes of Curriculum mapping and capstone planning, indication of student’s perceived performance components in each of them and /or levels for your course allow us to consider students’ progress and what further development should be aimed for in the relevant area,
Resources for Teaching and Assessment
Are they stipulated in sufficient detail? Do they seem reasonable in view of the course learning objectives, weighting and duration? Are other options offered or considered? Do they align with overall global resources in terms of feasibility and sustainability?
Evaluation:
Will this course design require review and refinement for the second iteration? What sorts of evaluation measures do we need to consider at the end of this first course offering? Ref: Dixon, J. Evaluation and the Health Professions 1978; 1: 47-65; Davis DA, Taylor Vaisey AL J Contin Educ Health Prof 1997; 17:207
Dixon’s Levels (1-4 increasing validity) Quantitative Measures Qualitative Measures
1 Evaluations Forms (‘Happiness’ Index) Focus groups / Interviews
2 Pre-testing versus Post-testing Results Participant Surveys / Questionnaires
3 Change daily practice or learning habits Structured Interviews
4 Improve Overall Outcomes Receiver Questionnaires

AFPC Educational Outcomes
Which AFPC Educational Outcomes will be addressed by this course? Refer to Appendix to select and check the appropriate boxes to select the AFPC Educational Outcomes
Below, indicate following at what level will these be addressed (beginner, intermediate, advanced)?
As Care Providers, pharmacy graduates:
As Communicators, pharmacy graduates:
As Collaborators, pharmacy graduates:
As Managers, pharmacy graduates:
As Advocates, pharmacy graduates:
As Scholars, pharmacy graduates:
As Professionals, pharmacy graduates:
2. Please estimate resource implications associated with teaching methodologies to be used.
3. Please estimate resources implications associated with assessment methodologies to be used.
It is estimated that 78 Teaching Assistant hours would be sufficient for marking the four problem sets, midterm, and final exam, based on an enrolment of 50 students. This should preferably be divided into 2 x TAships of 38 hours each.
4. Which of the five curricular themes will be covered in this course? How will integration of these themes be achieved through teaching and assessment methods used?
Approval from Theme Coordinator (name of theme coordinator): Olavo Fernandez (Patient Safety)
5. Which of the following course evaluation measures will you incorporate in your course to facilitate review and iterative refinement?
Dixon’s Levels (1-4 increasing validity) Quantitative Measures Qualitative Measures
1 Evaluations Forms (‘Happiness’ Index) Focus groups / Interviews
2 Pre-testing versus Post-testing Participant Surveys / Questionnaires
3 Change daily practice or learning habits Structured Interviews
4 Improve Outcomes Receiver Questionnaires
6. Please note any other relevant information for Curriculum Committee review purposes.
A longer version of this course has been successfully running for 8 years in the pharmaceutical chemistry program.

Appendix
Writing Learning Objectives using Bloom's Taxonomy
The SOLO taxonomy and Miller's Levels of Competency
Statements related to Missed Assessments within Courses
AFPC Educational Outcomes
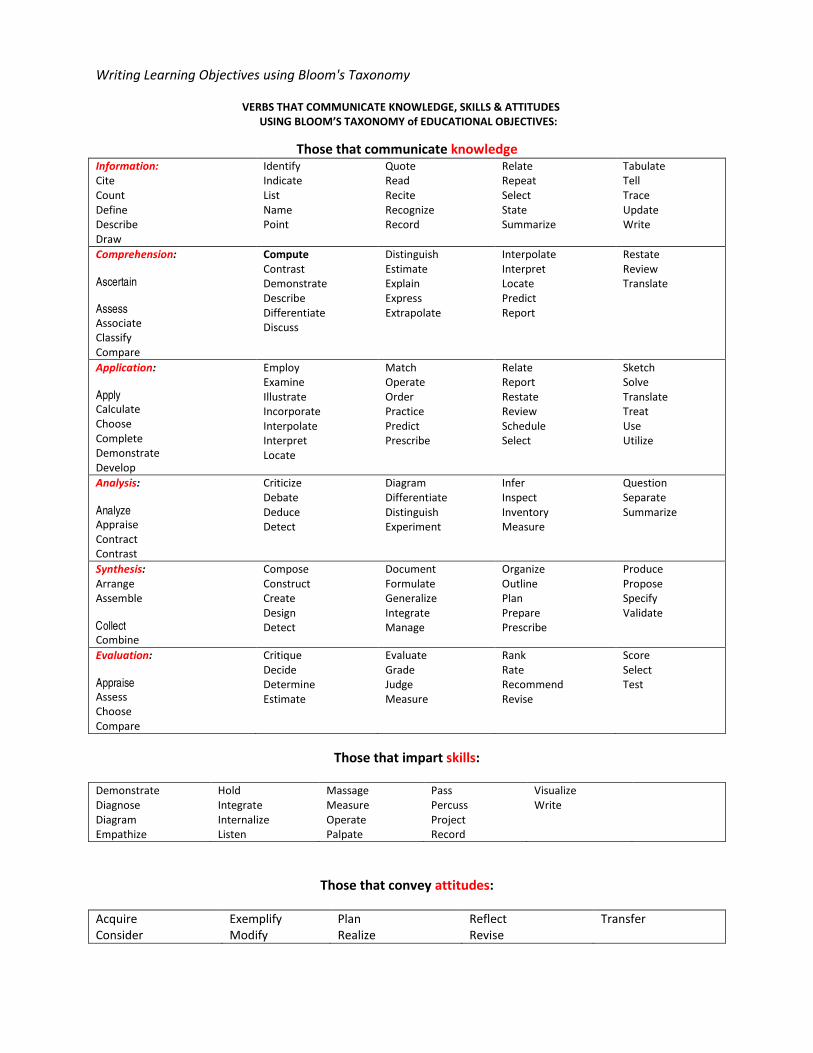
Writing Learning Objectives using Bloom's Taxonomy
VERBS THAT COMMUNICATE KNOWLEDGE, SKILLS & ATTITUDES
USING BLOOM’S TAXONOMY of EDUCATIONAL OBJECTIVES:
Those that communicate knowledge
Information:
Cite
Count
Define
Describe
Draw
Identify
Indicate
List
Name
Point
Quote
Read
Recite
Recognize
Record
Relate
Repeat
Select
State
Summarize
Tabulate
Tell
Trace
Update
Write
Comprehension:
Ascertain
Assess Associate
Classify
Compare
Compute
Contrast
Demonstrate
Describe
Differentiate
Discuss
Distinguish
Estimate
Explain
Express
Extrapolate
Interpolate
Interpret
Locate
Predict
Report
Restate
Review
Translate
Application:
Apply Calculate
Choose
Complete
Demonstrate
Develop
Employ
Examine
Illustrate
Incorporate
Interpolate
Interpret
Locate
Match
Operate
Order
Practice
Predict
Prescribe
Relate
Report
Restate
Review
Schedule
Select
Sketch
Solve
Translate
Treat
Use
Utilize
Analysis:
Analyze Appraise
Contract
Contrast
Criticize
Debate
Deduce
Detect
Diagram
Differentiate
Distinguish
Experiment
Infer
Inspect
Inventory
Measure
Question
Separate
Summarize
Synthesis:
Arrange
Assemble
Collect Combine
Compose
Construct
Create
Design
Detect
Document
Formulate
Generalize
Integrate
Manage
Organize
Outline
Plan
Prepare
Prescribe
Produce
Propose
Specify
Validate
Evaluation:
Appraise Assess
Choose
Compare
Critique
Decide
Determine
Estimate
Evaluate
Grade
Judge
Measure
Rank
Rate
Recommend
Revise
Score
Select
Test
Those that impart skills:
Demonstrate
Diagnose
Diagram
Empathize
Hold
Integrate
Internalize
Listen
Massage
Measure
Operate
Palpate
Pass
Percuss
Project
Record
Visualize
Write
Those that convey attitudes:
Acquire
Consider
Exemplify
Modify
Plan
Realize
Reflect
Revise
Transfer
Does
Shows
How
Knows How
Know
Knows About
Heard Of
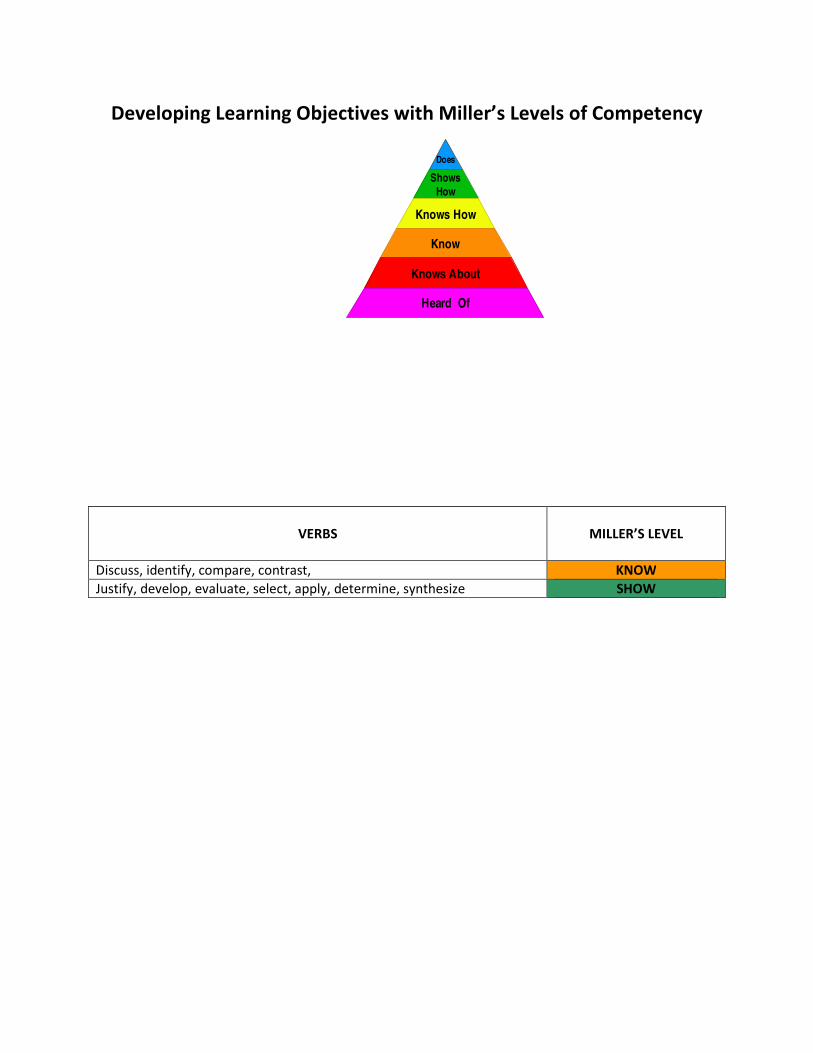
Developing Learning Objectives with Miller’s Levels of Competency
VERBS
MILLER’S LEVEL
Discuss, identify, compare, contrast, KNOW
Justify, develop, evaluate, select, apply, determine, synthesize SHOW
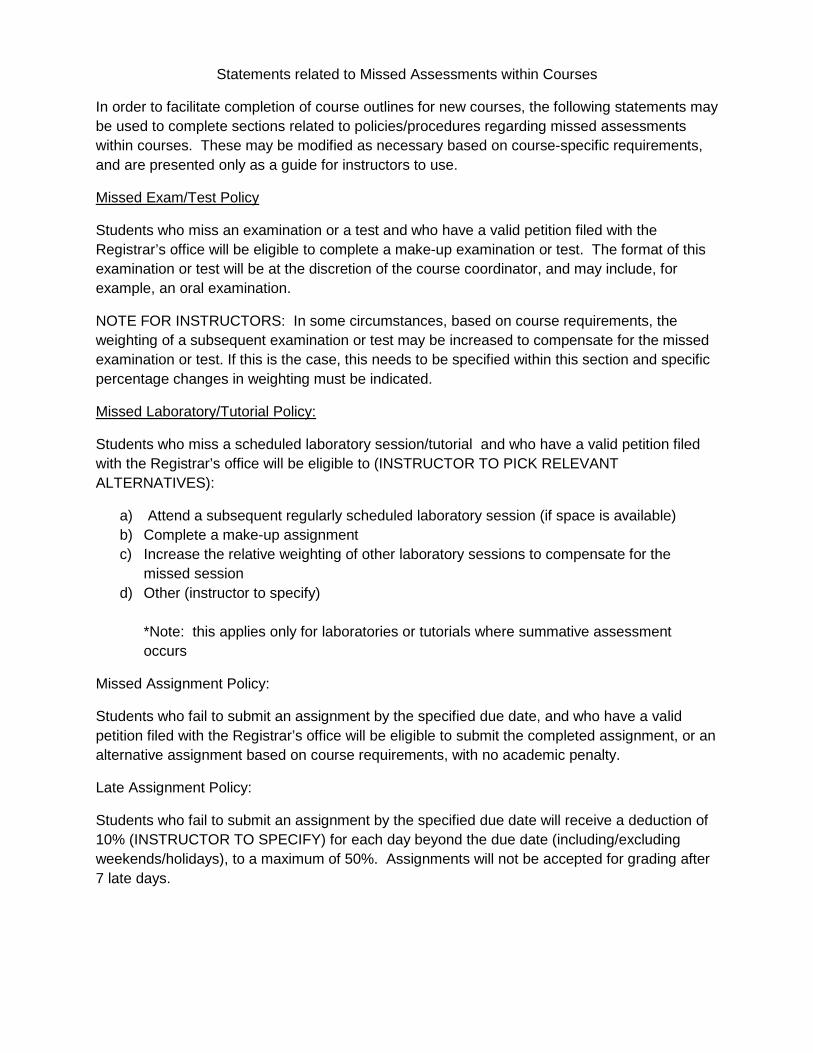
Statements related to Missed Assessments within Courses
In order to facilitate completion of course outlines for new courses, the following statements may be used to complete sections related to policies/procedures regarding missed assessments within courses. These may be modified as necessary based on course-specific requirements, and are presented only as a guide for instructors to use.
Missed Exam/Test Policy
Students who miss an examination or a test and who have a valid petition filed with the Registrar’s office will be eligible to complete a make-up examination or test. The format of this examination or test will be at the discretion of the course coordinator, and may include, for example, an oral examination.
NOTE FOR INSTRUCTORS: In some circumstances, based on course requirements, the weighting of a subsequent examination or test may be increased to compensate for the missed examination or test. If this is the case, this needs to be specified within this section and specific percentage changes in weighting must be indicated.
Missed Laboratory/Tutorial Policy:
Students who miss a scheduled laboratory session/tutorial and who have a valid petition filed with the Registrar’s office will be eligible to (INSTRUCTOR TO PICK RELEVANT ALTERNATIVES):
a) Attend a subsequent regularly scheduled laboratory session (if space is available) b) Complete a make-up assignment c) Increase the relative weighting of other laboratory sessions to compensate for the
missed session d) Other (instructor to specify)
*Note: this applies only for laboratories or tutorials where summative assessment occurs
Missed Assignment Policy:
Students who fail to submit an assignment by the specified due date, and who have a valid petition filed with the Registrar’s office will be eligible to submit the completed assignment, or an alternative assignment based on course requirements, with no academic penalty.
Late Assignment Policy:
Students who fail to submit an assignment by the specified due date will receive a deduction of 10% (INSTRUCTOR TO SPECIFY) for each day beyond the due date (including/excluding weekends/holidays), to a maximum of 50%. Assignments will not be accepted for grading after 7 late days.
AFPC Educational Outcomes (Please fill in this section)
1. Which AFPC Educational Outcomes will be addre ssed by this course (please list outcome unit and element)? At what level will these be addresse d?
Introductory = knowledge and comprehension of concepts, definitions, Intermediate = application of concepts to simple situations Advanced = application of concepts to more complex situations with ability to synthesize and evaluate
As Care Providers , pharmacy graduates:
A. Assess patients 1.1 Develop and maintain professional, collaborativ e relationships required for patient care.
1.1.1 establish and maintain a professional, caring practice environment;
1.1.2 demonstrate that the patient's goals are the priority;
1.1.3 determine when it is ethically and professionally appropriate to involve caregivers;
1.1.4 acknowledge and respect the roles and responsibilities of the pharmacist, the patient and/or caregivers, and the patient's other health care professionals (9). 1.2 Elicit and complete an assessment of required i nformation to determine the patient's medication related and other relevant health needs.
1.2.1 elicit the reason(s) for the patient's visit to the pharmacy or encounter with the pharmacist;
1.2.2 obtain and evaluate relevant history from the patient, his/her chart, caregivers and other health care professionals;
1.2.3 order, retrieve and assess relevant lab tests and diagnostic assessments;
1.2.4 perform and interpret findings of relevant physical assessments that are required to determine appropriate medication therapy, and;
1.2.5 complete an assessment of the patient's ability to take / use / administer his/her medications. 1.3 Assess if a patient's medication-related needs are being met;
1.3.1 evaluate the safety and effectiveness of a patient's medications with consideration of the patient's values and preferences, characteristics, conditions, functional capabilities, other medications and access to health care / monitoring;
1.3.2 determine whether a patient is appropriately managing his/her therapy, including appropriate administration and adherence in particular for chronic disease management;
1.3.3 determine whether a patient's medications are achieving the desired goals including consideration of efficacy and adverse effects;
1.3.4 determine whether a patient requires medication assessment and reconciliation;
1.3.5 where appropriate, identify a patient's medication-related needs as specific medication therapy problems, and:
1.3.6 determine if a patient requires additional care or services consistent with established collaborative practice agreements (see glossary). 1.4 Determine if a patient has relevant, priority h ealth and wellness needs.
1.4.1 recognize signs, symptoms and risk factors that relate to medical or health problems that fall into the scope of practice of other health care professionals.(Including, for example, signs and symptoms of diabetes mellitus, hypertension, arthritis, stroke, cardiac disease.)
1.4.2 recognize signs and symptoms associated with medical emergencies;
1.4.3 recognize problems with activities of daily living important to the patient's well-being, and:
1.4.4 identify opportunities for advocacy, health promotion and disease prevention with individuals to whom they provide care.
B. Plan Care 1.5 Refer patients for management of priority healt h and wellness needs that fall beyond the scope of practice of pharmacists 1.6 Develop a care plan that addresses a patient's medication-therapy problems and priority health and wellness needs.
1.6.1 prioritize a patient's medication-related needs;
1.6.2 establish goals of medication therapy with the patient (desired endpoints, target values and timeframes for medication therapies)
1.6.3 assess alternative strategies and negotiate the therapeutic option best suited to the patient;
1.6.4 integrate the recommended therapeutic options for a patient's medication-related needs into a co-ordinated plan;
1.6.5 determine monitoring parameters for desired therapeutic endpoints and potential adverse effect, specifying target values and start, frequency and end time-points for monitoring;
1.6.6 decide specific actions to be taken by the pharmacist as necessary for management of medication-related needs, specifically determining whether it is appropriate to: • dispense a medication according to a new prescription; • dispense an authorized refill of a medication; • authorize an extension of refills of a medication; • modify a patient's medications; • recommend changes in medications; • prescribe medications or therapies; • administer a medication, and/or; • refer the patient to other health care professionals for assessment and management;
1.6.7 determine if a patient requires information or other support to facilitate his/her management of needs related to activities of daily living, health promotion or well-being, and:
1.6.8 negotiate the responsibilities of the pharmacist and patient, and when other health care professionals should be contacted.
1.7 Implement the care plan.
1.7.1 undertake specific actions as specified in the care plan (e.g. prescribing, ordering lab tests);
1.7.2 educate the patient regarding the care plan to facilitate understanding and adherence;
1.7.3 facilitate continuity of care through referral and communication with relevant care providers;
1.7.4 convey information on maintaining and promoting health;
1.7.5 convey information about available social support services to assist with daily living, and;
1.7.6 schedule required follow-up in accordance with a patient care plan.
C. Follow-up and Evaluate 1.8 Elicit clinical and / or lab evidence of patien t outcomes.
1.8.1 determine the clinical status of the patient, including completing physical assessments required for monitoring of medication therapy;
1.8.2 evaluate the efficacy of the care plan relative to the desired goals;
1.8.3 evaluate the safety of the care plan including the presence of adverse drug reactions or effects;
1.8.4 identify any medication errors or close calls (see glossary)(9), and:

1.8.5 determine changes in pharmacotherapy that are required. 1.9 Assess and manage patients’ new medication-rela ted needs.(Go back to assessing patients section.)
D. Document 1.10 Support the continuity of patient care by docu menting their patient care activities
1.10.1 document in a timely, retrievable, usable manner
1.10.2 fulfill professional responsibilities for documentation
1.10.3 report and document the reporting of adverse events and close calls (9). As Communicators , pharmacy graduates:
2.1. Communicate non-verbally and verbally with oth ers.
2.1.1. use active listening skills and respond appropriately;
2.1.2. exhibit empathy, tact and respect in their dealings with others;
2.1.3. demonstrate sensitivity, respect and empathy in intercultural and inter-professional situations;
2.1.4. when speaking, use organized processes and appropriate, precise expressions and vocabulary;
2.1.5. tailor the content of their communication to specific contexts and audiences, and:
2.1.6 adapt their communication techniques to facilitate efficient and effective clinical encounters. 2.2. Communicate in writing.
2.2.1. write clearly, using organized processes and appropriate vocabulary;
2.2.2. correctly apply the rules of syntax, grammar and punctuation, and:
2.2.3. adapt the content of their arguments to specific contexts and target audiences.
2.3. Present information.
2.3.1. appear comfortable, engage the audience, use appropriate tone and pace, and use nonverbal language appropriately;
2.3.2. are organized and can set and adhere to appropriate time limits, and:
2.3.3 respond to and manage interaction with the audience. 2.4. Use communication technology.
2.4.1. demonstrate sufficient understanding of information systems to integrate computer and related technology into effective communication, and;
2.4.2. use effective communication skills regardless of the media employed, including effective use of visual and educational aids. As Collaborators , pharmacy graduates:
3.1. Function as members of teams.
3.1.1 accept leadership roles where appropriate;
3.1.2 actively make their expertise available to others and willingly agree to share relevant information, using language that can be understood by all;
3.1.3 clarify roles, responsibilities and expertise of team members, identifying overlaps and gaps;

3.1.4 recognize and respect the roles, responsibilities and competence of other professionals;
3.1.5 make their points of view known, listen to and respect the opinions of others, defend points of view if necessary;
3.1.6 contribute to planning, organizing and performing of work to be done, and integrating evidence while evaluating the results;
3.1.7 respect the rules established by the group;
3.1.8 help maintain a healthy work environment and assist with conflict management, and:
3.1.9 support continued efforts of the group by providing positive feedback, including evidence of progress and impact. 3.2 Support team-based care in a community setting with geographically distinct centres of care.
3.2.1 develop and maintain collaborative relationships with a network of local health care professionals and care providers;
3.2.2 clarify pharmacist’s roles and responsibilities that are acceptable / appropriate;
3.2.3 fulfill commitments for provision and follow-up of care;
3.2.4 adapt their roles in teams and networks of care to the circumstances and requirements, and;
3.2.5 participate in local health initiatives as requested and appropriate. 3.3 Work collaboratively with the patient and his/h er health care professionals to provide care and services that facilitate management of the patient' s health needs.
3.3.1 negotiate the care and services that the pharmacist and other members of the health care team will provide as consistent with laws / regulations relevant to collaborative care;
3.3.2 ensure attainment and maintenance of training / certification / credentials required to provide collaborative care or to fulfill medical directives / delegation;
3.3.3 ensure legality of collaborative practice agreements / medical directives / delegation agreements;
3.3.4 plan the provision of care in a coordinated fashion;
3.3.5 provide agreed upon care and services;
3.3.6 document the provision of care and services, and:
3.3.7 communicate and review the care / services provided and patient status / outcome.
As Managers , pharmacy graduates:
4.1 Manage their personal practice.
4.1.1 set priorities and manage their time to balance patient care, workflow and practice requirements, and;
4.1.2 adapt their practice to fulfill evolving professional roles. 4.2 Manage the safe and efficient distribution of m edications.
4.2.1 utilize inventory control concepts to maintain an inventory control system;
4.2.2 manage the distribution of medication in a variety of settings,
4.2.3 evaluate the factors critical to safe and efficient medication distribution systems including pharmacy layout / design, workflow, technology and automation (9) and;
4.2.4 anticipate, recognize and manage human, environmental and medication distribution situations that place patients at risk (9). 4.3 Participate in quality assurance and improvemen t programs.

4.3.1 evaluate the quality of care and cost effectiveness of services they provide;
4.3.2 disclose, manage and report adverse drug events (9);
4.3.3 disclose, manage and report errors, incidents and unsafe practices (9);
4.3.4 participate in formal planning for practice change and implementation of services to meet patient's needs and/or improve the quality of care provided, and:
4.3.5 adapt to change, providing new or emerging services as consistent with management’s practice change plans. 4.4 Manage the staff under their direct supervision .
4.4.1 supervise members of the pharmacy team, including pharmacy technicians, to ensure competent performance of functions;
4.4.2 ensure that pharmacy technicians and staff are delegated and undertake functions appropriate to their training and legislation;
4.4.3 manage workload to prioritize provision of professional services;
4.4.4 function as a role model for professional and support staff, and:
4.4.5 participate in staff selection, training, development and evaluation. 4.5 Manage to maintain the sustainability of the pr actice.
4.5.1 understand the impact of funding and payment policies on the provision of professional services;
4.5.2 create a business plan for the provision of professional services;
4.5.3 participate in strategic planning for their practice site;
4.5.4 understand marketing principles in the context of supply and demand for professional services, and;
4.5.5 incorporate the use of technology. As Advocates , pharmacy graduates:
5.1 Interpret the advocacy role of pharmacists / pr ofession of pharmacy.
5.1.1 describe the ethical and professional issues inherent in health advocacy, including altruism, social justice, autonomy, integrity and idealism;
5.1.2 explain the role of the profession in advocating collectively for health and patient safety, and:
5.1.3 describe how policy and procedures impact on the health of the populations served. 5.2 Promote the health of individual patients, comm unities, and populations
5.2.1 facilitate patient's interaction with the health care system through advice, education and/or guidance;
5.2.2 support patient's access to required health services by representing or speaking on behalf of patients;
5.2.3 represent patient's interests through participation in policy and procedure development within health systems;
5.2.4 participate in health promotion activities, public health campaigns and patient safety initiatives that are directed at disease prevention, risk factor reduction and/or harm minimization;
5.2.5 undertake relevant public health screening processes for early disease detection, and;
5.2.6 plan and implement public health promotion education and awareness raising campaigns with other health professionals.
5.3 Support the role of pharmacists in evolving hea lth care systems.
5.3.1 promote the impact of the pharmacist on patient outcomes;
5.3.2 promote the role of pharmacists in the development and implementation of health procedures and policies, and:
5.3.3 accept a leadership role to support the vision for advancement of the profession of pharmacy. As Scholars , pharmacy graduates:
6.1 Demonstrate a thorough understanding of the fun damental knowledge required of pharmacists and apply this knowledge in daily pract ice.
6.1.1 rationalize their recommendations and decisions with appropriate, accurate explanations and best evidence;
6.1.2 rely on professional experience to develop solutions to routine, previously encountered problems;
6.1.3 utilize established decision-making frameworks when faced with new situations to identify, analyze and develop solutions to problems, and:
6.1.4 undertake and apply learning required to manage new problems. 6.2 Provide drug information and recommendations.
6.2.1 identify needs for information, recommendations and decisions on medications;
6.2.2 conduct a systematic search for evidence using a variety of search methods and tools;
6.2.3 critically analyze information including primary research articles;
6.2.4 determine plausible solutions and select the most appropriate recommendation;
6.2.5 communicate information / recommendations;
6.2.6 evaluate the usefulness of the information provided, and:
6.2.7 document the information provided.
6.3 Educate regarding medications and appropriate medication use, including the pharmacist’s role.
6.3.1 identify learning needs of the audience;
6.3.2 select educational techniques appropriate for the learners;
6.3.3 select and organize content;
6.3.4 implement their educational plans, and:
6.3.5 assess the outcomes of their education. 6.4 Apply principles of scientific inquiry and crit ical thinking while participating in practice-based research.
6.4.1 understand the need for the generation and discovery of new information as it pertains to the continuous development of the profession, innovations in practice and optimization of pharmacotherapy;
6.4.2 recognize relevant practice or medication use problems;
6.4.3 define the parameters of relevant problems;
6.4.4 retrieve and assess reports/literature relevant to identified problems;
6.4.5 formulate research questions/hypotheses;
6.4.6 design practice-based research projects to address research questions, and:
6.4.7 contribute to the development of new knowledge by participating in practice-based research
projects. As Professionals , pharmacy graduates:
7.1 Demonstrate professionalism throughout patient encounters.
7.1.1 show respect for patients by acknowledging the patient as a person, listening actively and considering their needs and expectations;
7.1.2 accept responsibility for recognizing and meeting patients’ medication therapy needs;
7.1.3 maintain patient confidentiality, and:
7.1.4 maintain appropriate boundaries with patients. 7.2 Practice in an ethical manner which assures pri mary accountability to the patient.
7.2.1 involve the patient in decision-making, respecting their right to make their own choices;
7.2.2 fulfill requirements for obtaining patient consent;
7.2.3 integrate patient preferences related to culture, beliefs and practices;
7.2.4 use ethical frameworks as one component of professional judgement;
7.2.5 prioritize patient needs, accepting inconvenience and subordinating their personal interests to those of their patients;
7.2.6 ensure the continuity of patient care, abiding by the principle of nonabandonment, and:
7.2.7 recognize and manage situations presenting ethical dilemmas including conflicts of interest. 7.3 Maintain their competence to practice through l ife long learning.
7.3.1 adhere to regulatory requirements for maintenance of competence as consistent with the self-regulating status of a health professional;
7.3.2 evaluate their practice to identify areas for continuing professional development;
7.3.3 acknowledge and reflect on errors, omissions and close calls to identify limitations in competence / performance;
7.3.4 seek and accept feedback to identify limitations or strengths in competence / performance;
7.3.5 recognize their limits of competence and seek assistance;
7.3.6 plan and undertake learning activities to support maintenance of competence and professional development;
7.3.7 incorporate learning into their practice;
7.3.8 assess the impact of learning on competence and practice performance, and:
7.3.9 document their maintenance of competence. 7.4 Practice in manner demonstrating professional a ccountability.
7.4.1 comply with the legal and regulatory requirements of practice;
7.4.2 respect and fulfill professional standards of practice;
7.4.3 be accessible to patients and other health care professionals;
7.4.4 fulfill their professional tasks and commitments to patients in a diligent, timely, reliable, respectful manner;
7.4.5 accept responsibility for their decisions and recommendations with patients and colleagues;
7.4.6 use health care resources appropriately, including human and financial resources;
7.4.7 maintain a professional image, using appropriate language and demeanour;
7.4.8 maintain their professional composure even in difficult situations, and:
7.4.9 maintain appropriate professional boundaries. 7.5 Display a sense of pride in and commitment to t he profession and its evolving role in the health care system.
7.5.1 participate in peer review and quality assurance processes;
7.5.2 participate in education of future pharmacists by making practice-based learning opportunities available as a mentor / preceptor;
7.5.3 adapt their practice to provide all professional services required according to pharmacist’s scope of practice;
7.5.4 support the professional organizations in their efforts to advance the professional role of pharmacists, and:
7.5.5 contribute to the planning for implementation of change including strategies to identify and overcome barriers, and to capitalize on facilitators.












![fileCourse syllabus must be attached and completed according to Fitchburg State guidelines. E] Course Syllabus attached Required Signatures—Graduate and Continuing Education Course](https://img.pdfslide.us/doc/110x75/5e122588a8321604d45edfb8/syllabus-must-be-attached-and-completed-according-to-fitchburg-state-guidelines.jpg)
















