Embed Size (px)
Citation preview
Countdown to 2015 In-Depth Country
Case Study: Afghanistan
Presented by: Nadia Akseer, MSc, PhD Candidate
University of TorontoHospital for Sick Children
Toronto, Canada

Main Objectives
• To conduct a systematic, comprehensive assessment of RMNCH, nutrition, and survival trends in Afghanistan in the 2001-2014 “post-Taliban” era
• To perform an analysis of RMNCH-specific health systems components, policies, and financial flows
• To determine key predictors of change in health service utilization
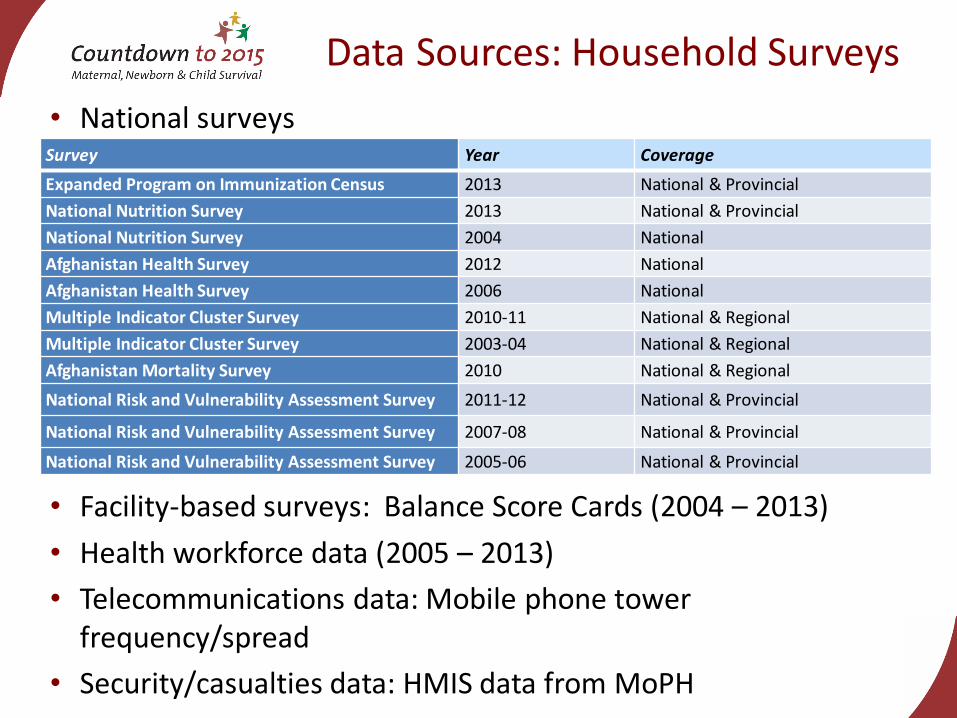
Data Sources: Household Surveys
Survey Year Coverage
Expanded Program on Immunization Census 2013 National & Provincial
National Nutrition Survey 2013 National & Provincial
National Nutrition Survey 2004 National
Afghanistan Health Survey 2012 National
Afghanistan Health Survey 2006 National
Multiple Indicator Cluster Survey 2010-11 National & Regional
Multiple Indicator Cluster Survey 2003-04 National & Regional
Afghanistan Mortality Survey 2010 National & Regional
National Risk and Vulnerability Assessment Survey 2011-12 National & Provincial
National Risk and Vulnerability Assessment Survey 2007-08 National & Provincial
National Risk and Vulnerability Assessment Survey 2005-06 National & Provincial
• National surveys
• Facility-based surveys: Balance Score Cards (2004 – 2013)
• Health workforce data (2005 – 2013)
• Telecommunications data: Mobile phone tower frequency/spread
• Security/casualties data: HMIS data from MoPH
Mortality Trends: MMR
• Target: Reduce MMR to 50% of it’s 2003 level (i.e. reduce to 529 per 100K live births) by 2015
• Result: MMR decreased from 1057 in 2000 to 402 in 2013
• Reduction of 62% between 2000 to 2013
• Afghanistan has achieved MDG5a
Source: UN-MMEIG, 2014
*Note: IHME reports conflicting results indicating increase in MMR (885 in 2013)
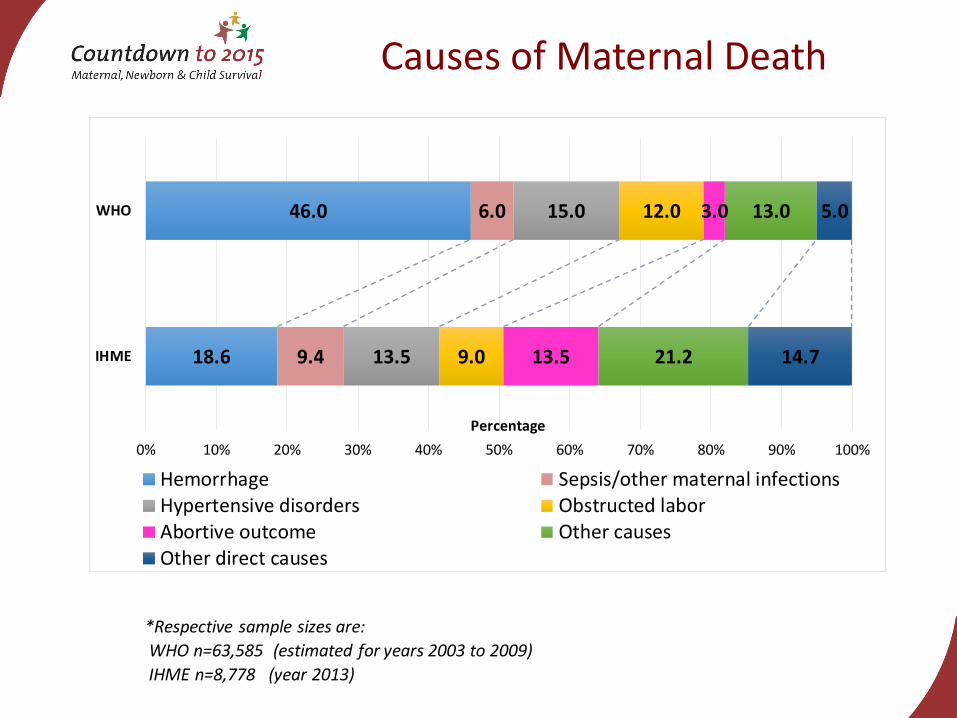
Causes of Maternal Death
18.6
46.0
9.4
6.0
13.5
15.0
9.0
12.0
13.5
3.0
21.2
13.0
14.7
5.0
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
IHME
WHO
Percentage
Hemorrhage Sepsis/other maternal infectionsHypertensive disorders Obstructed laborAbortive outcome Other causesOther direct causes
*Respective sample sizes are:
WHO n=63,585 (estimated for years 2003 to 2009)
IHME n=8,778 (year 2013)
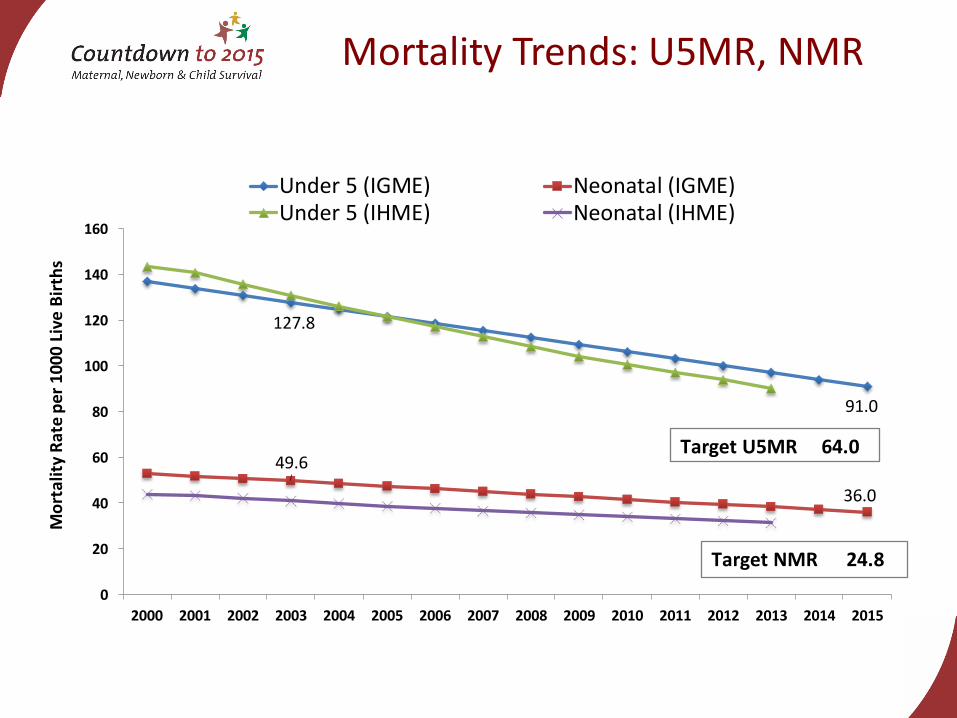
Mortality Trends: U5MR, NMR
127.8
91.0
49.6
36.0
0
20
40
60
80
100
120
140
160
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Mo
rtal
ity
Rat
e p
er 1
000
Live
Bir
ths
Under 5 (IGME) Neonatal (IGME)Under 5 (IHME) Neonatal (IHME)
Target U5MR 64.0
Target NMR 24.8
Neonatal Cause of Death
Major causes of neonatal (1-27 days) and post-
neonatal death have not changed from 2001
to 2013:
Neonatal
• Preterm birth complications (29% vs. 28%)
• Intrapartum related events (23% vs. 29%)
• Infections including sepsis, meningitis, and tetanus
(20% vs. 23%)
Post-neonatal
• Diarrhea (24% vs 20%)
• Pneumonia (26% vs 28%) Source: CHERG, 2014

Nutrition
60.554.1
43.1
8.813.2
9.0
33.925.1 25.5
0
10
20
30
40
50
60
70
80
90
100
2004 2011 2013
Pre
vale
nce
(%
)
Year
Stunting Wasting Underweight
Sources: National Nutrition Survey, 2004, 2013. Multiple Indicator Cluster Survey 2010/11.
Trends in anthropometric nutrition outcomes, children 6-59 months
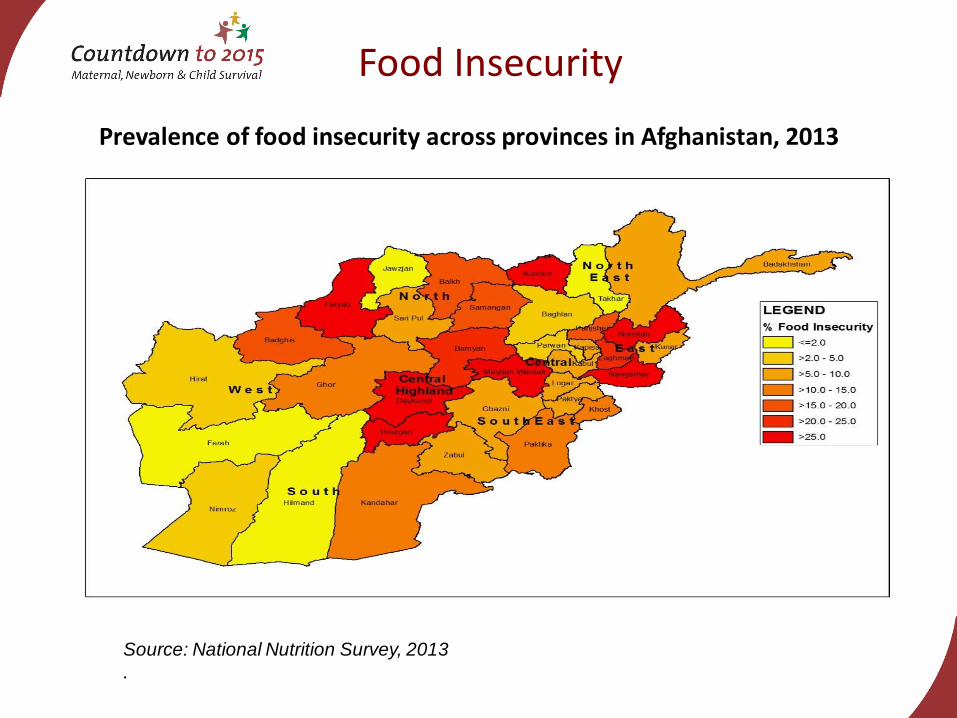
Food Insecurity
Source: National Nutrition Survey, 2013
.
Prevalence of food insecurity across provinces in Afghanistan, 2013
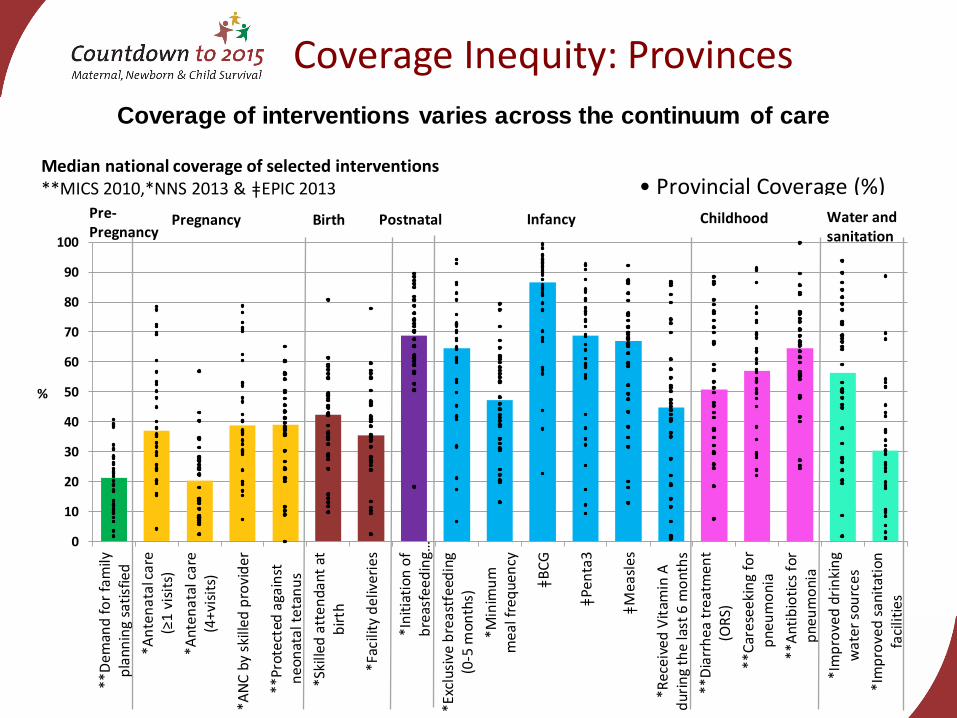
Coverage Inequity: Provinces
0
10
20
30
40
50
60
70
80
90
100
**D
eman
d fo
r fa
mily
pla
nnin
g sa
tisf
ied
*An
ten
atal
car
e (≥
1 v
isit
s)
*Ant
enat
al c
are
(4+v
isit
s)
*AN
C b
y sk
illed
pro
vid
er
**Pr
otec
ted
aga
inst
ne
on
ata
l te
tan
us
*Ski
lled
att
enda
nt a
tb
irth
*Fac
ility
del
iver
ies
*In
itia
tion
of
bre
asfe
ed
ing…
*Exc
lusi
ve b
rea
stfe
edin
g(0
-5 m
onth
s)
*Min
imu
mm
eal f
req
uen
cy
ǂB
CG
ǂPe
nta
3
ǂM
easl
es
*Rec
eive
d V
itam
in A
dur
ing
the
last
6 m
ont
hs
**D
iarr
hea
tre
atm
ent
(OR
S)
**C
ares
eeki
ng
for
pne
um
oni
a
**A
ntib
ioti
cs f
orp
neu
mo
nia
*Im
pro
ved
dri
nki
ng
wat
er s
ou
rces
*Im
pro
ved
sani
tati
onfa
cilit
ies
%
Pregnancy Birth Postnatal Infancy Childhood Water and sanitation
Pre-Pregnancy
Median national coverage of selected interventions**MICS 2010,*NNS 2013 & ǂEPIC 2013 • Provincial Coverage (%)
Coverage of interventions varies across the continuum of care
Health Systems & Policies
High-impact initiatives
• Implementing the Basic Package of Health Services (BPHS)
• Adapting the contracting-out mechanism
• Implementing a standardized national salary policy to motivate health care workers to work in rural areas
• Implementing national programmes (EPI, Malaria, TB, HIV/AIDS, CBHI, Nutrition, etc.)
• Training midwives
• Implementing the Essential Package of Health Services (EPHS)

Essential health system factors
• Strong stewardship by Ministry of Public Health
• Effective coordination and communication
• Regular monitoring
• Health management information system
• Health system performance assessment and facility surveys (Balance Score Cards) conducted through 3rd-party mechanisms
Health Systems & Policies
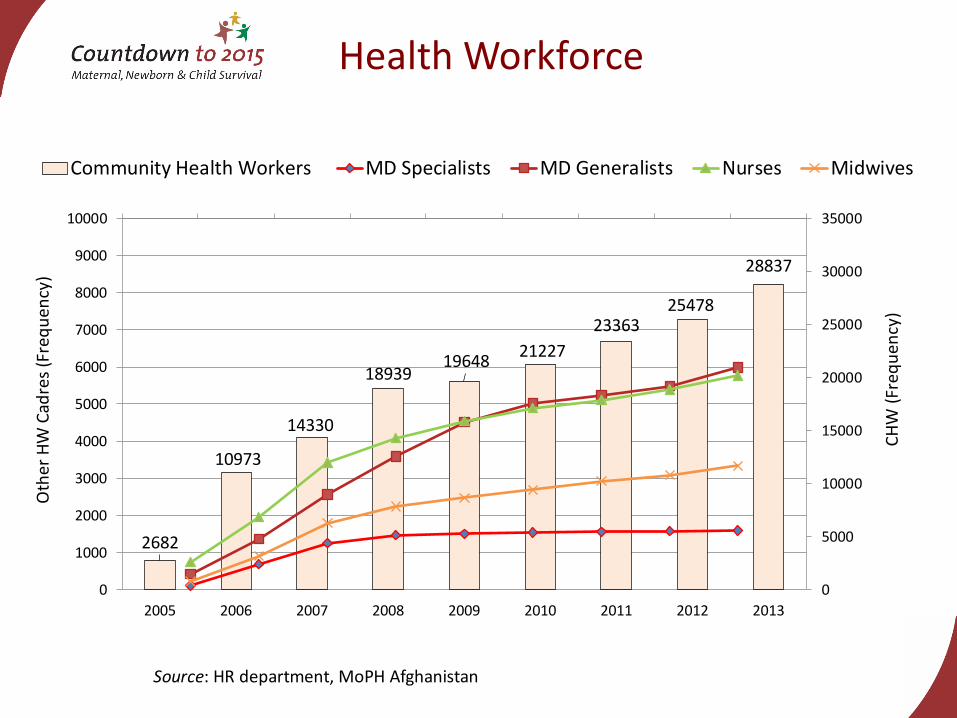
Health Workforce
Source: HR department, MoPH Afghanistan
2682
10973
14330
1893919648
21227
2336325478
28837
2005 2006 2007 2008 2009 2010 2011 2012 2013
0
5000
10000
15000
20000
25000
30000
35000
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
CH
W (
Freq
uen
cy)
Oth
er H
W C
adre
s (F
req
uen
cy)
Community Health Workers MD Specialists MD Generalists Nurses Midwives
Lives Saved Tool (LiST)
• Over 85% of all deaths could be averted by scaling up all intervention packages to 90% coverage level by 2025
– Approx. 135,000 deaths averted annually
– 84% of neonatal, 92% of post-neonatal, and 89% of maternal deaths
Lives Saved Tool (LiST)
• Most high impact: + 50% in EmOC and immediate newborn care ~9,900 newborn lives saved
• + 90% ~30,900 newborn/4,400 maternal lives saved
• Universal coverage of immunization 30,700 child deaths averted annually
• Water, hygiene, and sanitation interventions scaled up by 75% from current levels 16,100 child deaths averted
• Infant and young child feeding programs scaled up by 25% from current levels ~12,100 post-neonatal lives saved
Key Findings
• Afghanistan has made remarkable progress over a decade, but vast subnational inequities remain.
• Donor support, strong stewardship, effective health policy frameworks, improved access to care, and increases in skilled health workers contributed to success
• Further reductions in under-5 mortality require substantial investment in newborn care and in interventions to target stunting
• Contextual factors, including education and infrastructure(communication and transport systems), and health system strengthening are critically important

The Way Forward
Afghanistan must focus on
• increased investments in social determinants of health
• interventions to address newborn survival
• Strategies to reduce health inequities
Afghanistan Case Study Research Team
Nadia Akseer, MSc, PhD (Candidate)
Ahmad S Salehi, MD, MSc, MBA, PhD (Candidate)
S M Hossain, MD, MPH, MBA
M Taufiq Mashal, MD, PhD
M Hafiz Rasooly, MD, MSc
Zaid Bhatti, MSc
Arjumand Rizvi, MSc
Zulfiqar A Bhutta, MD, PhD





























