Embed Size (px)
Citation preview

COUNCIL OF GOVERNORS MEETING
23 January 2018
Overall Page 3 of 64

Overall Page 4 of 64

COUNCIL OF GOVERNORSTuesday 23 January 2018 5:00pm – 7:00pm
Education Centre, 1st Floor West Wing, 250 Euston Road, London NW1 2PG
AgendaAgenda item Lead
1. Welcome and apologies for absence David Prior
2. Minutes of the last meeting held on 16 October 2017 David Prior
3. Action tracker and matters arising David Prior
4. Declarations of Interest - oral David Prior
5. Presentation: Financial Plan 2018/19 Tim Jaggard
6.
6.1
6.2
6.3
Reports from Governors:
Lead Governor’s report
Quality and safety Committee report
High Quality Patient Care Group report
Claire Williams
Veronica Beechey
Veronica Beechey
7. Chief Executive’s Report Marcel Levi
8. Any other urgent business not included in the above reports
9. Date of the next meeting
Wednesday 25 April 2018
Overall Page 5 of 64

Overall Page 6 of 64

Council of Governors
Minutes of the meeting held in Public on Monday 16 October 2017
Present – members
Javed Ahmed, Staff Governor Annabel Kanabus, Patient GovernorDonna Beck, Staff Governor John Knight, Patient GovernorVeronica Beechey, Patient Governor Isaac Kohn, Public GovernorJanet Clarke, Staff Governor Frances Lefford, Public GovernorGraham Cooper, Patient Governor Jessica Lipman, Staff GovernorCaroline Dux, Staff Governor Christine Mackenzie, Patient GovernorAdam Elliott, Patient Governor Richard Murley, Chairman (meeting Chair)John Green, Patient Governor Brian Potter, Patient GovernorKate Hall, Stakeholder Governor Claire Williams, Stakeholder GovernorKathryn Harley, Staff Governor Martha Wiseman, Patient Governor
In attendance
Geoff Bellingan Medical Director, Surgery & Cancer BoardGuy Dentith Deputy Finance DirectorJulie Hogg Deputy Chief NurseCharles House Medical Director, Medicine BoardMarcel Levi Chief Executive OfficerTonia Ramsden Director of Corporate ServicesRachel Stoukas Trust Administrator
1. Welcome, introduction and apologies1.1 Apologies were received from Governors: Danny Beales, John Bird, Philip Brading, Leslie
Brantingham, Maggie Gormley, Michael Hanna, Ammara Hughes, Warren Turner, Jo Wagerman.
2. Minutes of the last meeting 2.2 The minutes of the last meeting held on the 3 July 2017 were agreed subject to amendment of
minute 2.9 to read: Veronica Beechey asked about the Trust’s discharge arrangements and whether they were satisfactory and safe. The Chief Executive confirmed the Trust had robust processes in place and worked with many other healthcare providers to facilitate patient discharges.
3. Action tracker and matters arising3.1 The action tracker was noted. Completed items would be closed.
4. Lead Governors report4.1 The Lead Governor report was noted. A special thanks and fond farewell was made to Richard
Murley who would be retiring from the Trust in December after seven and a half years as Chairman.
5. Patient Experience Committee (PEC) Annual report5.1 Christine MacKenzie introduced the report which outlined how patient experience had improved
in the Trust over the last year. The Chairman reported he had met with the Chief Executive, the Chief Nurse and the Chair of the PEC (Althea Efunshile) and discussed lifting the profile of
Overall Page 7 of 64

patient experience. He explained plans were in place to improve the governance process and for PEC to become a formal Board committee. The Chief Nurse and the Head of Patient Experience were currently in the process of refreshing the committee terms of reference and planning the new structure.
5.2 The report noted some areas where patient experience was an issue including the robotic voice patient information systems which had not been a success with older patients, and the friends and family test for the emergency department (ED). There was a positive response about the Access and Patient Administration Programme (APA) which had seen some helpful improvements including admin jobs being standardised into four groups with training and career progression.
5.3 Claire Williams asked about the inpatient friends and family test and what more could be done to increase responses. Charles House explained plans were in place to increase electronic devices across adult wards and to re-introduce card surveys on paediatric wards, it was hoped this would increase response rates.
5.4 The Patient Experience Committee Annual Report was noted.
6. Chairman’s report6.1 The Chairman welcomed the newly elected Governors to the Council; Isaac Kohn, Brian Potter
and Martha Wiseman. In addition Kate Hall had joined as the Governor representing UCLPartners and two reserve Governors had joined the Council; Ann Fahey and Javed Ahmed.
6.2 The report highlighted the Chairman’s visit to the A&E redevelopment site in August. Caroline Dux and John Green enquired about the progress and explained that on a recent Governor walk round of the area they were surprised to see a lack of space particularly in A&E majors. They were worried that patients had to wait in corridors during busy periods. The Chairman noted these concerns and explained these would be addressed urgently. He explained all was on track with the redevelopment, which when completed would create a lot more space.
6.3 The Governors noted the National Hospital redevelopment update including three new ward openings. There were questions relating to when the new patient information centre would be opened, if an adequate discharge lounge was in scope and what could be done in the near future to help those patients waiting for transport. Julie Hogg informed Governors that although a discharge lounge at The National was in scope, available property space was a major limitation. With regards to the timeline of the patient information centre and the immediate improvement for patients waiting for transport, it was agreed these would be added to the action tracker for further consideration and review.
Action CoG/3/17 (Julie Hogg with Gill Gaskin)
The Chairman’s report was noted.
7. Chief Executive’s report7.1 The Chief Executive opened his report focusing on month 4 performance.
7.2 A&E – 4 hour wait targetIn July performance decreased to 88.2% against the 95% four hour standard and was below the agreed trajectory with NHS Improvement (NHSI). Charles House explained the Trust had experienced a very difficult period with increased visits, lack of bed availability and waits for speciality review leading to breaches. The Chief Executive explained the actions being taken to
Overall Page 8 of 64

address the issues including freeing up beds in the Tower earlier to facilitate flow, addressing staffing issues and increasing Consultant reviews on the wards to strengthen the discharge process.
7.3 Martha Wiseman asked about the significant number of beds that were occupied in A&E by patients with mental health issues. The Chief Executive explained the Trust had seen a rise in patients with mental health problems however had good support from the Camden and Islington Mental Health team and he confirmed the Trust worked closely with other organisations to discharge those patients, who did not need to be in A&E for medical care, to appropriate community settings.
7.4 There was a query regarding the closure of beds on the oncology ward due to nurse staff vacancies. The Chief Executive and the Chairman both explained that there had been difficulty in finding registered oncology nurses and it was important for the Trust to ensure its wards were staffed safely and adequately. The Chief Executive confirmed there had been no harm to patients as a result of the closed beds.
7.5 Winter planningClaire Williams asked about the Trust’s flu preparedness process. The Chief Executive confirmed robust winter planning was progressing in line with department of health and NHSI guidance. Staff were being encouraged via daily communication bulletins to have the flu vaccination. Currently the uptake of staff was 64%.
7.6 Cancer waiting timesGeoff Bellingan provided an update. He explained that for the past two months the Trust had achieved the internal target for patients to be treated within 62 days of a suspected cancer referral from primary care. This was a good improvement. He went on to explain that the 31 day first treatment standard had not been met. This was mostly due to late referrals for prostate surgery treatments. He also described delays being caused in other cancer specialities owing to inter trust transfers (ITT). Challenges occur when patient information particular medical results are missing or delayed from the referring hospital. A comprehensive cancer recovery action plan had been agreed with the commissioners and NHSI and some of the key actions to be delivered included review of the MDT coordinator resourcing and processes, and improving pathways across all cancer types. To help with the urology service, the addition of a second robot for prostatectomies had provided more capacity to deal with the surge in referrals.
7.7 Governors discussed the performance report, particularly the cancer and A&E performance. Annabel Kanabus asked what assurance could be provided that the actions described would work. The Chief Executive explained the Trust was working very hard to optimise cancer and A&E performance. In addition the Trust had jointly commissioned an externally led review of cancer waits. These would offer the Trust some important recommendations. Draft reports were expected in two weeks.
7.8 Referral to treatment and diagnostic waitsThe Governors discussed and noted the updates in relation to referral to treatment (RTT) incomplete standard and diagnostic waits.
7.9 EHRS and recruitment and retentionThere were specific queries regarding EHRS recruitment and nursing vacancies. Annabel Kanabus asked how the Trust was managing with all the big projects underway (Phase 4, Phase 5 and EHRS) and the demands on individual’s time. She asked if internal recruitment to the
Overall Page 9 of 64

EHRS programme was causing problems in other areas of the Trust. She also asked about Governor representation on the EHRS project. The Chief Executive explained it was extremely important to recruit internally to EHRS vacancies as it was crucial to have staff who understood the Trust and could help design and build the system. The Chairman explained that currently it was important that the Executive were able to proceed with the programme and the Board were confident that Gill Gaskin as Senior Responsible Officer would involve patients and governors at the appropriate stage.
7.10 John Green asked about the current nurse recruitment challenges. Julie Hogg explained there was currently a 10.1% nursing vacancy rate, which was a reflective position nationally. She explained the Trust was being very proactive and looking at possibilities to increase recruitment particularly in hard to recruit areas. In response to John Knight’s query about the effect of Brexit on the retention and recruitment of nurse staffing, Julie confirmed this had been an issue with the Trust seeing less applications from European nurses since the Brexit decision. A retention and recruitment group had been set up to review the vacancy position and to consider what enhancements could be made to retain staff.
7.11 Jessica Lipman asked what more could be done to help staff experiencing abuse on the wards, particularly in the evenings. The Chief Executive explained the Trust was committed to ensuring staff were safe and provided with ongoing training and support.
7.12 Financial performanceGuy Dentith provided an overview of the current financial performance. He explained that as of 31 August 2017, the Trust’s income and expenditure performance before donation adjustments and other exceptional items for the year to date is a deficit of £7.1m which is £8.4m worse than plan. The Trust’s full-year forecast shows that cost improvement programme (CIP) schemes totalling £34.2m have now been identified which is 82% of the full year target.
7.13 Governors discussed the financial performance update and noted particular concern across all three clinical boards which were reporting positions behind plan at August. Governors asked what the issues were. The Chief Executive explained the main cause across all three Boards was under delivery of CIP and over performance on income from outpatient and non-elective activity. In addition corporate directorates were also behind plan on CIP schemes and delivery.
7.14 Governors understood that the Trust Board were addressing the decline in the financial position and had appointed a Turnaround Director on a short term contract to focus on improving the financial forecast / run rate for the Trust’s poorer performing divisions and corporate directorates and oversee delivery of the Trust-wide CIP and recovery schemes.
7.15 2017/19 corporate objectives deliveryGovernors noted that delivery against the majority of strategic objectives were on track with the exception of two. These related to improving patient pathways and achieving financial sustainability.
7.16 Care quality commission report updateThe care quality commission inspection update report and progress against the Trust-wide action plan was noted.
7.17 Patient TransportChristine Mackenzie expressed governors continuing concerns about the patient transport service. The number of complaints about the service had continued to rise and patients were
Overall Page 10 of 64

waiting too long for transport. C House explained key performance indicators were in the process of being progressed and the task and finish transport contract recovery group were meeting fortnightly to address key actions against a recovery plan. Leslie Brantingham and Christine Mackenzie both attended the task and finish group. Christine asked if they were permitted to provide feedback to other governors following the meetings. It was agreed The Chief Executive and Charles House would consider this.
Action CoG/4/17 (C House and M Levi)
8. Annual report of the Audit committee8.1 The Council noted the 2016/17annual report of the Audit committee.
9. Register of Governors’ interests9.1 The report which listed the interests of new Governors was noted.
10. Any other business10.1 On behalf of the Governors, Veronica Beechey noted thanks to Richard Murley who she
described as being a great support to Governors. She thanked him for his positive impact on the Trust as a whole and noted he would be greatly missed.
11. Date and time of next meeting in public11.1 Tuesday 23 January 2018, 5:00pm, The Education Centre, 250 Euston Road.
Overall Page 11 of 64

Overall Page 12 of 64

COUNCIL OF GOVERNORS ACTION TRACKER (PUBLIC)
Action number Date of meeting Subject Action Responsible
director
Due date Update Status
CoG/3/17 16.10.17 Chairman’s report The Governors noted the National Hospital
redevelopment update including three new ward
openings. There were questions relating to when
the new patient information centre would be
opened, if an adequate discharge lounge was in
scope and what could be done in the near future to
help those patients waiting for transport. Julie
Hogg informed Governors that although a
discharge lounge at The National was in scope,
available property space was a major limitation.
With regards to the timeline of the patient
information centre and the immediate improvement
for patients waiting for transport, it was agreed
these would be added to the action tracker for
further consideration and review.
J Hogg and G Gaskin Ongoing Patients waiting for transport - to improve patient
experience patient support officer roles have been
created to be used at UCH, MCC and NHNN.
These staff will act as a liaison between G4S and
patients, provide assistance and information and
ensure patients are comfortable.
An update on the patient information centre at the
NHNN will be provided at the meeting
Open
CoG/4/17 16.10.17 Patient Transport Leslie Brantingham and Christine Mackenzie both
attended the task and finish group. Christine asked
if they were permitted to provide feedback to other
governors following the meetings. It was agreed
The Chief Executive and Charles House would
consider this.
M Levi and C House 01.11.2017 C House confirmed on 31.10.17 there were no
objections to the governors involved discussing
the content with others in a constructive and
sensitive manner.
Complete

Overall Page 14 of 64

UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
LEAD GOVERNOR’S REPORT TO THE COUNCIL OF GOVERNORS
23 JANUARY 2018
The Council is asked to note the report.
1 Lord Prior of Brampton, UCLH Chair
It is a great pleasure to welcome David Prior, who took up his appointment on 1 January 2018, as the new Chair of the Trust and of the Council of Governors. Governors were unanimous in approving David’s appointment in July 2017 and the whole Council was invited to meet David on 9 November 2017 as part of his induction. We enjoyed hearing his insights on a wide range of topics of interest to governors. We are particularly pleased that David comes with exactly the experience that the Board and Council hoped we would find in the new Chair.
David’s first week in post coincided with widespread news coverage of a crisis in English hospitals and A&E departments being unable to cope with the number of patients presenting for treatment. On his second day in the office, I asked David if he could tell the governors how UCLH was affected and planning to cope. I received a considered email from him telling me that he had just come back from visiting A&E and giving me his impression of how the Trust was coping. Several governors told me how much they appreciated the quality of his reply and that he was already out and about in the Trust talking to front-line staff and seeing for himself how things are going. We all look forward to working with David constructively and effectively for the benefit of patients and staff at UCLH. He has been appointed for an initial period of three years.
2 Patient transport service and additional Council meeting
In my last report, I set out the steps governors had taken since July 2017 to address the Council’s concerns about the quality of UCLH’s non-emergency patient transport service (NEPTS) as provided by G4S. It is particularly disquieting that incidences of poor performance of NEPTS place additional strain on patient flow through UCLH and on staff at the very time when there are substantial financial and operational challenges to be met.
The most obvious of our concerns about NEPTS is that far too many patients have experienced exceptionally long delays in being collected from UCLH hospitals – by exceptional delays, I mean patients waiting five, six, seven, or eight hours to be collected. This can mean patients waiting until very late at night to be collected from
Overall Page 15 of 64

hospital. Patients have had to stay for an extra night on the ward owing to delays or failures in their NEPTS booking. There has been evidence suggesting a lack of capacity in the service at night. Staff have sometimes waited with patients long after their shift has ended. It is particularly concerning that NEPTS delays and failures can cause patients to miss treatments and appointments at UCLH and other hospitals to which UCLH patients are due to be transferred. It is regrettable that there have been no systematic fall-back arrangements in place that staff can use to ensure a patient is taken home or transferred (or brought into UCLH) when NEPTS has failed to provide a timely service.
Governors have raised these concerns repeatedly with the Board. An additional Council meeting was held in closed session on 23 November 2017 specifically to discuss NEPTS. It was chaired by Harry Bush (Vice-Chairman) and was attended by Marcel Levi (Chief Executive), Charles House (Medical Director, Medicine Board), Tim Jaggard (Finance Director), Kieran Murphy (Non-Executive Director, Chair of the Trust’s Investment Committee) and 14 governors.
In addition, Leslie Brantingham and Christine Mackenzie have attended UCLH’s transport task to finish group (we are grateful to the Trust for its invitation to attend) and have represented patients’ perspectives on the group. Governors were also invited to comment on how contractual key performance indicators might be revised and I am pleased to report that some of these suggestions have been taken up by the Trust.
We await an update on NEPTS from the Trust at the Council of Governors meeting on 23 January 2018. We would also appreciate hearing the views of non-executive directors on progress since the meeting on 23 November 2017. We would be grateful for documentary assurance that any plans for improvement are indeed delivering the promised incremental enhancements in performance.
3 Governor seminars
Seminars and presentations given by UCLH directors and staff specifically for governors are a valuable opportunity for Council members to learn about the detail of developments at the Trust and, also, about some of the ‘behind the scenes’ areas of its work.
- UCLH finances
Governors were grateful to Tim Jaggard, Finance Director, for an exceptionally open and frank briefing on the current financial outlook at the Trust at the seminar on 15 November 2017. Governors left the seminar with a clear sense of the scale of the financial challenge facing UCLH over the next year or so and of the detailed
Overall Page 16 of 64

measures being considered to ensure it achieves its control target in 2017/18. Tim is to provide a further update at the Council on 23 January 2018.
- UCLH Institute
Dr Emma Taylor, Director of Education, and some of her colleagues from the UCLH Institute introduced aspects of the work of the Institute at a presentation to governors in the UCH Education Centre on 9 January 2018. Governors were invited to participate in a simulation of treating a patient. We saw how clinical staff can use simulations in the impressive facilities of the Education Centre to learn about how they work as part of team and respond to stress when faced with medical emergencies. We were grateful to Dr Taylor and her colleagues for a fascinating insight into how UCLH enables staff to enhance their clinical skills and medical knowledge through experiential learning.
4 MembersMeets
Two well attended MembersMeets, talks for members of the Foundation Trust, took place in the Education Centre at 250 Euston Road.
- Comprehensive Stroke Service
On 19 October 2017, Dr Rob Simister (Consultant and Clinical Lead for the UCLH Stroke Service) and his team spoke about the London stroke care model which has improved the outcomes for patients suffering with a stroke. He described how well the Ttrust’s Hyper Acute Stroke Unit on T7 at UCH is performing in terms of rapid treatment of patients presenting with stroke symptoms and improving outcomes for them. He also referred to new treatments such as clot retrieval that should improve outcomes further. Christine Mackenzie (patient governor), former governors, Dee Carter and Amanda Gibbon, and I then spoke about our study, ‘The stroke pathway; the patient experience’, at UCLH. The study drew on interviews with stroke patients and relatives to make recommendations for how UCLH could improve its stroke services. We were delighted that Dr Simister and his team have found imaginative ways to address all our recommendations including ways of improving communication with carers and GPs, both of whom are crucial to supporting stroke patients when they leave hospital.
- Dementia: the challenge of our age
On 30 November 2017, Professor Nick Fox (Professor of Neurology and MRC Senior Clinical Fellow), Dr Selina Wray (Alzheimer’s Research UK Senior Research Fellow) and Dr Tammaryn Lashley (Senior Research Associate) from the UCL Institute of Neurology spoke about dementia. Professor Fox spoke about
Overall Page 17 of 64

Alzheimer’s disease, the most common cause of dementia. The underlying process of dementia is destruction of nerve cells. His colleagues, Dr Wray and Dr Lashley, described their research to reveal the pathological processes underlying dementia, to discover what interventions might stop the progress of dementia symptoms and possibly even stop their initial development. Some exciting new techniques that should enable comparison of nerve cells from families with and without early onset dementia and testing of new drug treatments were also described. Slides from the presentation are available on the MembersMeet page on the UCLH website.
5 Governor walk rounds
Since my last report, governors have participated in five walk rounds in the Trust as part of a regular programme arranged for them by the patient experience team. These were to the nuclear medicine department in the UCH Tower, the restorative and oral medicine/surgery departments at the Eastman Dental Hospital, the ante-natal clinic in the EGA Wing at UCH, the Trust’s Evergreen Ward at St Pancras Hospital and the Royal National Throat, Nose and Ear Hospital. The pattern is that two governors attend, sometimes accompanied by a non-executive director, and are shown around a ward or department by senior nursing staff accompanied by a member of the staff from the patient experience team. Walk rounds are one of the most instructive opportunities open to governors to learn about patient and staff experience in the Trust. My experience is that they always lead to new insights about how UCLH works and valuable contacts with Trust staff.
6 Additional governance meeting
On 9 October 2017, the first of a new series of governance meetings that had been proposed by Richard Murley was held. Governors were briefed on aspects of the Trust’s systems for monitoring and managing risk by Catherine Mooney, Director for Quality and Safety. She and Richard then took questions from governors about information in the Trust’s risk register and serious incidents, details of which had been circulated to the Council in advance. The documents supplied and the discussion at the meeting provided valuable additional insights for governors into risks and issues at UCLH and opportunities to seek assurance as to action taken by the Trust to reduce their impact.
7 Governor appointments and retirements
Philip Brading, Chief Executive of UCLH Charity, retired as the stakeholder governor representing the Charities supporting UCLH on the Council. We will miss Philip’s detailed knowledge of the Trust. Most recently, he was a member of the Chair Appointment Committee of the Council that recommended the appointment of David Prior. We will also miss Councillor Danny Beales, who represented Camden Council,
Overall Page 18 of 64

and Dr Ammara Hughes, a Camden GP stakeholder governor representing Camden and Islington GPs, who have both stepped down as governors. Both Danny and Ammara drew skilfully on their areas of expertise to make valuable contributions to Council meetings.
It is a pleasure to welcome four new partner organisation (or stakeholder) governors to the Council: Dr Katie Coleman, a GP in Islington, representing Camden and Islington GPs, Councillor Rishi Madlani from Camden Council, Diarmid Ogilvy, a trustee of the National Brain Appeal, who now represents the Charities supporting UCLH on the Council, and Dr Kevan Ritchie, a GP in Camden, who represents Camden CCG for us. We look forward to working with them and value the breadth of experience and detailed knowledge that they bring to the Council of Governors as representatives of their partner organisations.
We are also delighted to welcome Ann Fahey as a patient governor. Ann’s first meeting as a governor was the meeting on 9 November 2017 with David Prior.
Claire Williams, Lead Governor, 11 January 2018
Overall Page 19 of 64

Overall Page 20 of 64

UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUSTQuality and Safety Committee (QSC)
Report to Council of Governors 23 January 2018
I was asked to fill a gap which arose when Diana Scarrott left the Quality and Safety Committee (QSC) and am pleased to give an account of some of the issues from the November and December meetings.
I was unwell in the period when I had planned to write a thorough report so I have not been able to give it the time that I would have liked. I am therefore taking advantage of the excellent report on QSC issues produced by the quality and safety team for the recent Board meeting to assist me in putting together some comments which I hope will interest governors.
The first thing to say is that the committee covers a wide range of patient safety and quality issues and is brilliantly chaired by David Lomas who is one of our Non-Executive Directors. He is always very well informed and insists that issues discussed are actively followed up by Cathy Mooney, Director of Quality and Safety and her team. It is worth noting that the committee’s terms of reference were changed in November to reflect the need for committee process and safety work to be balanced with more quality improvement activity. This seems like a very good idea.
Appended to this report is a summary of the Clinical Quality Review Group meetings which has been prepared by Trust Member and previous Lead Governor, Diana Scarrott.
November meeting
1. Annual Patient Reported Outcome Measures (PROMs) ReportI sat on an earlier version of this committee when PROMs were first introduced. They have of course since developed. In the most recent evidence, data shows that at UCLH, groin hernia is the same as the national average; the index for hip replacements is just above the national average, which is good. The index for varicose veins is below the national average and there has been some improvement in 2014-2015 knee replacement data. PROMs participation rates for quarters 1 and 2 (2015-16 data) for pre-operative surveys were slightly above the English rate but the rate for post-operative questionnaires was 58.9% compared with 72.1% for England. The response rate obviously needs to improve but the QSC noted the improvement in outcomes.
2. Cerebral palsy claimsThe committee had a detailed discussion of a national review of legal cases concerning cerebral palsy claims. It was interesting to learn that among areas requiring more effort was a need to further involve parents in investigative
Overall Page 21 of 64

processes. The report shows that UCLH was compliant with key recommendations. I asked whether the findings of this report have ramifications for patients with different conditions in the Trust (they do) and was interested to learn that some wider work in this area is being developed elsewhere in North East London.
3. Quality and safety “state of the nation” updateThis was Tony Mundy’s response to progress since the March CQC inspection and it was extremely interesting. He started off by saying that a year ago his list of issues would have been acute medicine, leadership, learning and meeting targets. Today, by contrast, mental health issues would have a prominent role because concerns about them have at last increased in both national and local agendas. He provided information about areas where health issues are of particular concern and also provided a summary of care using a range of indicators in the Emergency Department (ED) and Acute Medicine Unit (AMU). The update took into consideration a recent unannounced peer group inspection by Guys and St Thomas staff in these areas. It is good to see such reciprocal arrangements with other trusts being introduced. This was a splendid presentation from Tony Mundy who spoke verbatim at length and was very lucid and informative.
4. Monthly quality and safety performance updateMuch of this update was concerned with inpatient falls: 120 inpatient falls in September, 92 with no harm, 21 with low harm, 4 with moderate harm, and 2 with serious harm. Specific investigations show that none of these incidents were caused by poor care and it was reassuring to learn that 2 deaths were also not attributable to Trust failings. I have had a particular interest in patient falls and learned something new here when I subsequently had a conversation with Cathy Mooney about 2 deaths from falls and how reviews are undertaken in these circumstances. Apparently the Trust undertakes 72 hour reviews which are different from serious incidents (SI) and after action reviews (AARs), although they may eventually lead to an SI if appropriate. These are led by a senior member of the division or board concerned (often Charles House), include one of the deputy chief nurses and involve staff who have been engaged with what has happened. The aim is to have a joint discussion of events, whether these are serious falls or cardiac arrests, and the purpose is to get a coherent account in writing which everyone involved can agree with. The 72 hour review also checks whether staff are being supported and duty of candour is being undertaken.
5. Friends and family test It is disappointing to learn that the friends and family test was below target in September and all showed a decline with the exception of inpatient and day case response rates (this was partly related to a technical error). The patient experience committee requested more clarity on the plans to improve our response rates.
Overall Page 22 of 64

December meeting
As in November this meeting covered a great deal of valuable information. A selection of issues follows.
1. Genomic England There was an interesting discussion about a joint consensus statement from the Human Tissue Authority and Health Research Authority and its implications for diagnostic pathways for NHS cancer genomic sampling and development of the 100,000 genomes project. UCLH forms part of the North Thames NHS Genomic Medicine Centre. As a result of the change in policy UCLH will be able to collect extra samples of blood for research without seeking further consent. The change in policy will hopefully make things easier for the relevant staff.
2. CQC executive steering group report Once again there is a huge amount of information from this committee which inspects and monitors services and other developments. It was interesting to read that the staff from the National Hospital for Neurology and Neurosurgery (NHNN) visited the Walton Centre NHS Foundation Trust in Liverpool, another welcome collaborative venture. The NHNN staff were encouraged by the possibility that an “outstanding” rating is possible as the Walton Centre has been rated outstanding by the CQC. It was also interesting to read that the service level agreement with Camden and Islington and a standard operating procedure are to be finalised and agreed. Next year the Mental Health Act will be amended so that a police station is no longer a “place of safety”. This will undoubtedly put more pressure on the ED.
3. Venous thromboembolism (VTE) root cause analysis We received an interesting and thorough report from VTE root cause analysis by Dr Hannah Cohen. VTE is a complex issue and one that the Trust is concerned about especially where hospital acquired venous thromboembolisms are concerned. Root cause analyses contain a great deal of useful information and the conclusions suggest that work to improve VTE reporting is progressing. The forward plan includes launching and rolling out the RCA process across the Trust, amendment of the Trust priority score card and recruitment of a new administrator who is urgently needed. I found this a very thorough piece of work.
4. Flu We had a useful discussion about flu which had started to appear in the Trust at the time of our December meeting. We were told that both A and B types were present. It was interesting to learn at that point that the vaccine used was 60% effective among the under 65 population but it appeared to be less effective among older people. At the time it was mainly older people and young ones who were presenting with flu. It was great to hear that it was possible to get test results quickly and that the ED had been amazing. Obviously these figures would not be accurate today but it was interesting to hear how the condition was developing and being treated in its early stages.
Overall Page 23 of 64

5. Patient safety committee This paper reported on a new regular patient safety committee which met in November. All boards were represented at this and there was a good multi-disciplinary attendance. The aim of the committee is to learn from serious incidents, internal red incidents and near misses. Each division will be asked to present an SI and the main point of the project is to share learning from incidents, especially SIs. QSC members welcomed the emphasis that the committee places on supporting shared learning and I felt particularly enthusiastic about this innovation.
6. Patient experience committeeThis was the last meeting of this important group which will now be a sub-committee of the Trust’s Board of Directors. The report commented on an improving experience group, which covers the Patient advice and liaison services (PALS), an update on the patient feedback system, the family and friends test, emergency department national survey results from 2016, cancer patient experience survey results, and a patient transport update. Personally I was disappointed because I had specifically requested that that a member of the UCLH staff would be present in areas where transport patients are picked up and dropped off in order to secure their safety. Governors have evidence that the input into the atrium is outstanding but there have been problems at the NHNN where this is not happening and there is a G4S member of staff with the same role. David Lomas was happy that I made this proposal (that a UCLH member of staff be present for patient transport pick-ups at NHNN) and agreed that it should be minuted and followed up. I was therefore disappointed that it had been omitted from the minutes and asked it if it could be reinstated.
7. Goodbye to RichardWe had a brief celebration and a fond farewell to Richard Murley who I believe has been a member of the QSC ever since he joined the Trust nine years ago. He will be missed.
Veronica BeecheyPatient Governor- with thanks to Cathy Mooney
Overall Page 24 of 64

Appendix to the QSC report to the Council of Governors 23 January 2018
Report from Trust member representative on the Clinical Quality Review Group
CQRG provides a forum for commissioners and Trusts to discuss quality issues, share information and challenge each other. Most of the papers put to the group by the Trust have been produced for Trust purposes already, so the group does not generate much new paperwork. A lot of ground is covered, as these examples show.
Sharing information
In November 2016 Jeremy Hunt announced a plan to reduce the incidence of gram-negative blood stream infections (especially eColi) by 50%. The Trust had a plan but wanted to know what was being done in primary and community care. The CCG was challenged to pull together the plans of different sectors into a single action plan and that has now been done.
The Trust has briefed CQRG on the new patient feedback system, introduced in June 2016. Commissioners, like Governors, want to know what is possible and see that the new system is being used to its full potential.
There will be a presentation to CQRG on EPIC (the upcoming electronic patient information system at the February meeting.
Asking the next question
Where access targets are missed, commissioners want to know whether delays caused harm. The Trust has agreed a process with commissioners which defines categories of case to be reviewed. Reports go to CQRG each month. The most recent Trust report concluded: ‘our clinical harm reviews have consistently not identified harm’.
Questions about harm also arise in relation to transport incidents; the harm classification for incidents doesn’t work for transport incidents which involve poor patient experience whereas the incident reporting system is based on physical harm.
Reporting how things really are
A GP on CQRG reported that email receipts were not being sent after gastroscopy referral forms were submitted - they should have been. The Trust is investigating.
A GP member also reported cancellation of urgent surgery because the anaesthetist asked for a cardiology report. The problem was sorted and the surgery took place. However, the Trust will look for ways to avoid this sort of postponement which can easily lead to an RTT breach.
Working out how they ought to be
There is ongoing discussion about reactivation of patient pathways after DNA or a patient-initiated deferral. GPs want to avoid writing referral letters again and again and the Trust also wants reactivation without a new referral. A trial of a new system is starting this month in orthopaedics.
Benchmarking against other Trusts
A new maternity dashboard is coming into use in maternity units at UCLH, Barnet, North Middlesex and the Royal Free. All four will collect the same data so that comparisons can be made. UCLH has provided data already.
Overall Page 25 of 64

Falls comparisons are also being made, but with UCLH data distorted by a high fall rate at Gowers Ward where patients have epilepsy. An adjusted falls measure is needed where UCLH is being compared with Trusts without such a unit.
Identifying wider issues
The Trust reports mixed sex breaches regularly – 37 in October for example. One of NHS England’s responses to winter pressures has been to be more relaxed about these breaches. But there is another issue, discussed briefly at this month’s meeting. In a hospital doing a lot of specialist work, is it more important to separate men from women or to have patients in the right ward for the specialty they are using? As the chief nurse said, the Trust needs to use available capacity in the best way and that might mean mixed sex bays.
Diana Scarrott
UCLH FT Member
Overall Page 26 of 64

University College London Hospitals NHS Foundation Trust
High Quality Patient Care Report to Council of Governors
23 January 2018
The HQPC group has continued to have been very involved and busy, with many interesting, new and on-going projects. Members are very engaged and keep generating new and appropriate working streams.
Presentations and Discussion
Experience mapping project with stroke patients (HASU)
Dr. Rob Simister, Associate Clinical Director Stroke Unit, Kate Petts, Deputy Divisional Manager NHNN and Dee Carter , previous Governor and patient member, came to present the key findings from the Stroke study and to give the Group a progress update on how any recommendations were being delivered.
This was a fascinating presentation and many questions were posed and answered.it was felt that this would be beneficial to stroke patients.
New project suggestions - End of Life Project
Christine Mackenzie updated the Group on a new patient experience mapping project which has been previously discussed. Due to the sensitivity of this project it is taking longer than anticipated to produce a proposal. The draft project outline will be presented at the next HQPC meeting.
Current Projects
1. Review of pharmacy services at UCLH
Governors have been looking at issues relating to the length of time patients have to wait to collect their medication. Improving this experience is also being discussed using examples from other hospitals. A final report will be presented to the next meeting of HQPC on 20.2.18
2. On-going discussion relating to the meaning of high quality patient care
Following the Governors visit to see Emergency Department major improvement work a follow up visit was proposed approximately 3 months after all building works have been completed. This will be arranged.
3. Atrium development and improvement of refreshment facilities
Caroline Dux reported that the she still had not heard back from various staff members were regarding this proposal. Tonia Ramsden kindly offered to see if she could expedite these; it was subsequently referred to the Capital and Estates Team.
In summary, HQPC continues to a very active group with very motivated and involved members
Caroline Dux
HQPC Group, Vice Chair.
Overall Page 27 of 64

Overall Page 28 of 64

UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
CHIEF EXECUTIVE’S REPORT TO THE COUNCIL OF GOVERNORS
23 January 2018
SUMMARY This report gives an update on the key issues of focus since the last Council meeting. As we start the last quarter of the 2017/18 financial year the focus for the Trust remains on delivering excellent patient care, improving our financial position and meeting key targets including cancer waiting times, referral to treatment pathways and A&E 4 hour wait. In addition we are also preparing for winter pressures and possible capacity constraints. We are working hard to minimise the effect on our emergency and elective patients.1. Finance and Contracting update
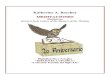
This report provides an update on the Trust’s financial performance as at 30th November 2018.The Trust’s income and expenditure performance, before donation adjustments and other exceptional items, for the year- to- date to November is a surplus of £3.2m, which is £6.5m worse than the planned position (see table 1 below).Taking account of the profit on disposal of the Trust’s share in Radiology Reporting Online and year to date EHRS costs results in a year-to-date surplus of £6.1m, which represents an adverse variance of £3.6m against the Trust’s control total.The Trust’s month 8 position also incorporates a £5.9m shortfall on sustainability and
transformation funding (STF), resulting from:a) Non-delivery of the control total (£4.1m).b) Emergency Department performance that was not in line with the A&E trajectory
(£1.8m).The month 8 year-to-date financial position is set out in table 1, below:
Table 1 – UCLH month 8 year-to-date financial position
Overall Page 29 of 64

£2.4m of the Trust’s £10m Board contingency has been released, with a further £0.8m being committed to fund the Trust's recovery programme management office. This results in £6.8m of contingency being available for the remainder of year, of which £1.8m has been accrued into the year-to-date position.The year-to-date results, as reported in the Trust’s month 8 financial return to NHS Improvement, represent a use of resources rating of 3 (on a scale of 1 to 4, with 1 being the lowest risk).Year-to-date CIP achievement is reported as £20.3m, £6.1m short of the £26.4m year to date plan.The Trust’s full-year forecast shows that CIP schemes totalling £32.6m have now been identified, which is 78% of the full-year target of £42mThe overall year-to-date picture can be summarised from a subjective view point, as follows:
Over-performance on income from outpatient and non-elective activity, Under-performance on income from elective (daycase and inpatient) and A&E activity, and income relating to drugs, devices and pass-through items and, A significant under-recovery on other non-patient related income, and Favourable positions against budget on pay and non-pay expenditure.
All three of the Trust’s clinical boards are reporting year-to-date positions that are behind plan at month 8, primarily as a result of a year-to-date shortfall in performance against CIP plans and clinical income under-performance.The Trust’s year-end forecast to NHS Improvement assumes delivery of the control total, however this will require the use of the remaining Board contingency and other available reserves, as well as requiring the Trust’s recovery programme to deliver approximately £2.7m of additional improvement.
Contract Performance at Month 8
Our 5 main NCL CCGs (Camden, Islington, Barnet, Enfield and Haringey) are over-performing against contract by £4.81m (3.6%) at month 8. In essence this means that we are seeing more patients than commissioners planned for. This level of over performance has been fairly consistent throughout the year and is primarily a product of an increase in emergency activity.
Our NHSE Specialist commissioners are also over performing against contract by £7.88m (3.3%). The main driver for this over-performance is the non-delivery of commissioner activity reduction initiatives.In Year Contract Management
Quarterly Reconciliation: We have completed the quarter 1 reconciliation process with both NHSE and our local CCG commissioners and have agreed quarter 1 over performance payments. The final position for quarter 2 was reported in the middle of November and we are now working with commissioners to complete the quarter 2 reconciliation process.
Service Developments: Since the last report to Governors we have agreed 2 new service developments with commissioners:
Telemedicine - We have agreed with commissioners to pilot the use of telemedicine (trialling the use of Skype for Business as the digital platform) across four specialities: Stroke; Maternity; Dementia; and Haematology. The pilot will test the use of Skype as an alternative to follow-up outpatient clinics (Dementia, Stroke and Maternity), in ward rounds for remote Consultant assessments (Stroke and haematology), and as a triage tool (dementia). The pilot is expected to begin in January.
Paediatric Assessment Unit - We have agreed with commissioners to pilot a Paediatric Assessment Unit which we hope will reduce time spent in A&E and also reduce hospital admissions. The pilot began on the 6th November.
Overall Page 30 of 64

Outsourced Pharmacy - We are planning to outsource our outpatient pharmacy at University College Hospital which we anticipate will deliver significant patient benefits. It will also deliver financial savings to the NHS as VAT will not be charged on prescribed items. We need to agree with our commissioners how these financial savings will be shared and therefore issued a proposal to commissioners at the end of August. Unfortunately to date we have not been able to reach an agreement and this is preventing the project progressing and delaying quality benefits to patients and financial benefits to the NHS. A senior escalation meeting with NHS England specialist commissioners involving Tim Jaggard and Simon Knight was held on the 4th January and we are hopeful of reaching an agreement soon.
Complementary Therapies - We undertook an audit with CCG commissioners to review our compliance with their Procedures of Limited Clinical Evidence (PoLCE). As a result of this audit we have introduced a new notification process to allow commissioners an opportunity to review our decisions to treat and ensure that we are compliant with the policy. Commissioners are also planning to consult on the commissioning of complementary therapies across NCL, with a very clear intended direction of travel being to further restrict routine access to such treatment. It is likely that they will begin this process in January. This would have an impact on UCLH services, particularly those provided at the RLHIM as well as other providers. We have asked to be involved for the outset and believe that we will bring a balanced and informed clinical view to the consultation.
New Service Developments (QS): We have held an initial scoping meeting with NHSE to discuss a small number of service developments at the National Hospital for Neurosurgery that we believe will deliver both benefits to patients and potential financial savings for the health economy. The intention is to present these in greater detail at a meeting in late January from which we hope to receive an agreement to proceed.
18-19 Contract Planning: We are in the middle of a two year contract and therefore we do not need to re-negotiate our contracts with commissioners. We do however need to agree the activity and finance baseline schedules of the contract for 2018-19. We have made good progress with our local NCL CCGs and do not anticipate there being a significant problems. We have also issued proposals to all other CCG commissioners and again do not anticipate any significant issues. We will work on a proposal for NHSE in January.
National Contract Variation: Although we are in the middle of a 2 year contract NHSE published a consultation document that proposed a small number of variations to the national contract. NHSE has now completed the consultation exercise with the revised terms and conditions to be implemented from the 1 February 2018. The main issue of note for the Trust is the initiation of non-payment for non-electronic referrals from the 1 October 2018 and the requirement on providers and commissioners to put in place a prompt, safe process for handling the return of any non-electronic referrals to GPs.
2. Performance and Corporate Objectives Update
This report covers the Trust’s performance at month seven of 2017/18. I attach the performance pack (attachment A) and highlight below the key messages.
Infection – MRSA and Clostridium difficile (C diff)
We are achieving our threshold for both absolute cases of C diff and cases of C diff attributed to lapses in care by the Trust. As at the end of October our worst case could be 17 against a threshold of 55: two cases were found to be lapses in care due to the Trust; the remaining 15 cases are under review.
There were no cases of MRSA reported in May through to October.
A&E – 4 hour wait target
Emergency Department (ED) performance continues to face challenges. We reported 88% for quarter 2, which means we missed the 90% minimum required to receive STF monies.
Overall Page 31 of 64

Lack of bed availability, waits for specialty review, and delays within the ED department itself have led to breaches. In addition nursing staff shortage had led to beds being closed on the T10 oncology ward, although these have now re-opened.
In order to recover our performance, we have refreshed our Remedial Action Plan (RAP). This improvement work is led by Charles House, Medical Director, and delivery is monitored through the Emergency Care Recovery Board (ECRB) on a weekly basis.
We have prioritised actions that will have maximum impact on improving flow through UCH, discharges and ED processes.
Key actions in the refreshed plan include: Launch of the electronic co-ordination centre to provide real-time information patients’
movements through the hospital to improve flow across our sites Implementation of an electronic tool and supporting processes to identify and manage patients
who are medically fit for discharge but have had their discharge delayed Working with partners across North Central London to implement improved discharge
pathways for patients requiring ongoing health or social care. These include agreeing a model whereby patients are discharged to receive their social and community care assessments in their homes rather than waiting to have them done as inpatients.
Completion of the ED site redevelopment to provide more and enable optimal use of space to support admission avoidance.
Establishing a surge area outside of ED to ease pressures during times of high demand
We successfully bid for national winter funds to enhance these schemes and linked to this, we have refreshed our trajectory to deliver the 95% standard by March 18.
Cancer waiting times
We were behind our trajectory for patients to be treated within 62 days of a suspected cancer referral from primary care in October, reporting 71.4% against our agreed position of 82.6%.
Performance for patients on internal pathways improved in July and was met in August. However, we reported 76.9% against the 85% standard for October. Some of these delays were due to clinical complexity and others initiated by patients.
We jointly commissioned an externally led review of cancer waits with NHS Improvement. The purpose of the review was to: understand underlying causes of non-achievement; define reasonable expectation for performance recovery; and provide assurance that we are doing everything we can to support delivery of cancer waiting times in the wider sector. There were two workstreams: operational delivery led by a senior clinician from Bart’s Health, and governance led by NHSI. We have now received the final reports and recommendations.
We have also undertaken a series of bi-lateral meetings with other trusts where we share cancer pathways. These have led to the production of jointly agreed action plans to shorten waiting times.
In light of the review and bi-laterals we are refreshing our trajectory to deliver compliance from July 2018.
We are refreshing our remedial action plan to drive this improved level of performance. Led by Geoff Bellingan, Medical Director, the following are some of the key actions within the revised plan:
Implementing tighter management and escalation of pathways (internal and shared) based on key criteria that enable us to respond to potential delays as early as possible.
Linked to the above, review of the MDT co-ordinator resource to ensure we have optimum tracking processes in place.
Strengthened clinical leadership in relation to cancer waits across all tumour sites.
Overall Page 32 of 64

Reinstating the Performance Committee from February 2018 to provide the Board with an independent and objective oversight of performance issues.
We regained compliance with the 31 day first treatment standard in October. Previous non-compliance had been driven by continued late tertiary referrals for prostate surgery treatments, predominantly from Barking, Havering and Redbridge University NHS Trust who have been reducing their volume of long waiting pathways. The urology services commissioned a second robot for prostatectomies which has provided more capacity to deal with future referral surges. We maintained the two week wait standard throughout July to October.
Referral to treatment (RTT) and diagnostic six week wait targets
We did not achieve the RTT 92% incomplete standard between July and November, despite having performed strongly since our return compliance in 2015.
Our decline in performance has been predominantly driven by the following divisions: RNTNE – 84.5% Queen Square – 89% EDH 89.5%.
All challenged reporting units have been asked to prepare recovery plans. Key actions will include: Ensuring maximum booking of clinic, day care and inpatients lists Reducing the number of patients who do not attend appointments, through good
administration, phone and text message reminders Ensuring patients are seen in order of clinical priority and longest waiter Undertaking additional outpatient and inpatient procedures Recruitment to vacant or newly-established posts.
In addition services who are meeting the standard have been asked to ensure they are doing everything possible within their current resource to reduce waiting times.
We have prepared a recovery plan that will deliver compliance by March. Geoff Bellingan, Medical Director, is the executive lead and we are driving delivery through the Elective Access Board.
We have sustained compliance against the diagnostic standard for tests to be undertaken within six weeks.
UCLH 2017/19 Corporate Objectives: delivery at Q2
We are tracking delivery against our five strategic objectives (attachment B). Each is underpinned by a number of annual objectives with specific measures and deliverables. Most of these are on track or have minor slippage at the end of Q2. However, below are the key exceptions:
Strategic objective 2: Improve patient pathways through collaboration with partners Work with system partners to shorten waits for patients in our emergency department and
avoid admission where possible: We missed the Q2 four hour wait trajectory and so did not achieve the associated transformation monies. We have refreshed our recovery plan and prioritised actions related to ED processes, patient flow through UCH, and discharge to improve performance.
Shorten waiting times at all stages of the pathways for cancer patients: We did not meet the Q2 cancer waits trajectory. NHS Improvement concluded a review of our governance and approach to delivering cancer waiting times. Recommendations will be included in our refreshed recovery plan. In parallel we have undertaken a series of meetings with other providers where we share cancer pathways to produce joint action plans to improve performance. We are now refreshing our trajectory to deliver the standard.
Strategic objective 3: Achieve financial sustainability Achieve financial targets and deliver the £42m cost improvement programme: We are behind
plan at Q2 and forecasting a significant shortfall against plan by year-end. The Board has now
Overall Page 33 of 64

appointed a turnaround director and strengthened programme management office to help us deliver in-year savings and to improve financial performance.
3. Patient TransportI am aware that the patient transport service remains of great concern to Governors and note those raised in the Lead Governor report. An operational update is provided below.ComplaintsThe contract is now in its fourteenth month. The number of complaints in the systems are 41 (October = 15, November =15, December =7). We are awaiting 23 overdue responses from G4S. All of the 23 overdue complainants awaiting a full response have been sent letters of apology for the delay and a revised date for the complaint response to be sent. PerformanceThe performance for November showed a movement from 48% to 50% in arrivals 15 minutes prior to appointment and a drop from 48% to 46% in patients collected within 1 hour. The nature of our outpatients appointments, means that it is complex to plan and schedule a return journey time for certain specialties. We have worked with G4S and the majority of the UCLH outpatient sites to put in place realistic return times of 2 hours which takes into account patients needing to spend extended times in hospital . As of the 1st of February and subject to G4S approval, the majority of outpatients attendees can expect to be picked up within 2 hours of their appointment finishing.Quality monitoring and assuranceThe “task to finish “ group chaired by Dr Robert Urquhart, Clinical Director has now been concluded and much work has been done to improve the booking process, improve patient information and improve the key performance indicators. There was an in-depth discussion at the Investment committee on the 3rd or January and the Board of Directors meeting on the 10th January to approve a process for ongoing quality monitoring and assurance which will address patient experience in more detail:
To formally constitute a Transport Service Development and Quality Improvement Board (TSDQIB) which will meet at least quarterly to discuss the SD&I Plan provided by the Contractor is accordance with the Contract. The members and remit of the of the TSDQIB to be confirmed.
To include “quality of service” as a standing agenda item of the monthly Contract Management Meeting.
To track the reasons for and resolution of Complaints through the Contract Management Meetings and to rigorously enforce the contractual provisions relating to complaint management.
To use the NHS Outcomes Framework Domains and Indicators as guiding principles to developing terms of reference and scope of the TSDQIB. NEPTS is a facilitative patient service and should support the achievement of all the NHS Outcomes Framework, specifically Domain 4 - Ensuring people have a positive experience of care and Domain 5 - Treating and caring for people in safe environment and protecting them from avoidable harm.
To set out locally defined outcomes that aligns to the KPI’s and defines clearly the “quality requirements” to be discussed at the monthly contract management meeting.
Patient experienceThe patient transport leaflet has now been revised and distributed. Transport operations are working with the patient experience team and external patient survey company to develop a more robust way of gauging feedback from patients.Transport operations – Electronic patient booking has been trialled on T14 North and South. The next trial will take place on T7 and David Ferrier ward and Lady Ann ward. Transport operations have
Overall Page 34 of 64

seconded an additional staff member to help with the e-booking trial and support the management of complaints.
4. Care Quality Commission In my October report you received an update from the CQC executive steering group (CQCESG) on progress against actions on the Trust-wide recommendations. The CQCESG has a robust programme of review. The attached report (attachment c) provides an update on progress since October 2017.
Marcel LeviJanuary 2018
Overall Page 35 of 64

Overall Page 36 of 64

Council Of Governors Meeting 23 January 2018
Chief Executive's ReportAttachment A - Performance Report
Overall Page 37 of 64

Meeting date: 23 January 2018 Month 7 - October
Council of Governors' Performance Report
Month 7 - October
Overall Page 38 of 64

1. Executive summaries
2. Finance 3. Delivery of CIP
4. Access
5. Patient Safety and Quality metrics
6. Workforce
7. Externally Reported Frameworks
Page Con
Chief Executive Performance report to the Governing BodyContents
Month 7 - October
Overall Page 39 of 64

3. Delivery of CIP3.3 Efficiency and productivity
Tru
st
Tow
er
ele
ctive
theatr
e
Queen S
quare
theatr
e
Westm
ore
land S
t
theatr
es
Cancer
Centr
e
theatr
e
RN
TN
E theatr
es
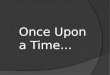
% Touchtime Utilisation 82.0% 82.5% 86.0% 82.0% - 78.4%
% Opportunity for additional cases 15.5% 14.2% 7.0% 15.9% - 16.0%
% 4-hour-equivalent sessions closed
or unused21.8% 11.1% 49.1% 3.3% - 4.1%
Number of 4-hour-equivalent sessions
closed or unused
Tru
st
thre
shold
Tru
st
actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
Average length of stay for key
specialties - Elective admissions
Average length of stay for key
specialties - Non-elective admissions
Outpatient DNA rate 8% 12.4% 15.3% 12.5% 11.5%
Month 7 - October
This month
* Trust excludes Cancer Centre. Tower theatre excludes EGA,
DSU & Hybrid. Queen Square excludes IMRI & Virtual
We have adopted the Four Eyes methodology for measuring utilisation: Touchtime utilisation is the actual session minutes used expressed as a percentage of allocated session minutes. Actual session minutes used is calculated from start of anaesthetic to the time of exiting the operating room for each patient in the session. Early starts and overruns are included in minutes used, but gaps between procedures are not. Opportunity for additional cases on the lists is the number of additional cases expressed as a percentage of total scheduled cases. Additional cases are the number of cases, based on average procedure times of a surgeon and list, that could be performed in the unused minutes of each list.
We are currently changing the indicators over for the scorecards so that divisions will have sight of the new metrics. This process is currently being completed and commentary for performance will be available next month.
Length of stay is better than threshold for elective and non elective admissions. Elective breast, non elective gynaecology, and non elective obstetrics are implementing enhanced recovery to support reduced length of stay on complex pathways. In thoracic surgery an enhanced recovery system is being implemented but is in the early stages and is expected to have an effect later in the year.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Tower
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Queen Square
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Westmoreland Street
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
RNTNE
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Trust
The Risk Adjusted Length of Stay Index (RALI) via CHKS is being updated and currently unavailable. It willbe released next month
Overall Page 40 of 64

4. Access4.1 Emergency flow
Tru
st
thre
shold
Tru
st
actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
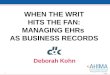
All A&E attendances within 4 hours 95% 87.6% 87.6%
UTC attendances within 4 hours 97% 94.4% 94.4%
A&E to admission conversion rate 20% 14.4% 14.4%
Tower bed occupancy
Delayed transfers of care days 602 338 106 158
% discharges by noon 15.8% 21.0% 17.3% 12.1%
This month
Month 7 - October
9500
10000
10500
11000
11500
12000
12500
80%
82%
84%
86%
88%
90%
92%
94%
96%
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17
A&
E a
ttendances w
ithin
4 h
ours
A&E attendances
A&E Attendances A&E attendances within 4 hours Target
Emergency department performance was 87.6% in October. Our trajectory for October was 92.6%.
As with our position in September, breaches were due to a combination of bed, specialty, and ED delays. The periods with lower performance levels (<90%) were due to a combination of staff shortages and lack of bed capacity. We continued to have a 16 bed ward (T10 oncology) and a 5 bed bay (T7 Care of the Elderly) closed in the tower due to nursing staff shortages, which contributed to bed pressures. All beds have now re-opened to address this issue. We have also seen delays owing to middle grade doctor shortages on certain days. Recruitment is underway to fill these posts.
We achieved STF monies in Q1. We did not achieve the required 90% across quarter 2, which means that we will not receive the STF monies. Through the Emergency Care Recovery Board (ECRB) we have refreshed and prioritised the RAP actions and re-set the trajectory to reach 95% by March. Please see separate item on the refreshed RAP. There are three broad areas – ED, operational flow and discharge. Progress will be reviewed at weekly ECRB meetings to ensure delivery against targets.
Work packages which will have greatest impact include the implementation of the Clinical Utilisation Review, reviewing the specialty referral model and rolling out the Discharge to Assess model in November. The ECRB will continue to track delivery of actions and realise their benefits, and develop further actions to improve our current forecast.
0
200
400
600
800
1000 Breach reasons
Bed Specialty delay Diagnostic ED Delay Other Transfers
Overall Page 41 of 64

4. Access4.2 Access Targets - Referral to treatment
Tru
st
thre
shold
Tru
st
actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
% incomplete pathways < 18 weeks 92% 90.6% 96.1% 95.2% 88.1%
Patients waiting > 52 weeks 0 5 1 4
Patients waiting 40-52 weeks 47 5 1 41
% data quality issues on waiting list 5% 8.1% 10.0% 12.3% 6.4%
% Diagnostic waiting list within 6 weeks 99% 99.1% 100.0% 100.0% 96.9%
% Last Minute Cancellations to Elective
Surgery0.6% 1.6% 1.6% 1.6% 1.6%
% Cancelled Operations Readmitted Within
28 Days95% 100.0% 100.0% 100.0% 100.0%
Outpatient Cancellation Rate – Hospital
(adjusted to include only postponed
appointments)
2.9% 2.4% 4.0% 2.5%
This month
Month 7 - October
90%
91%
92%
93%
94%
95%
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17% I
ncom
ple
te p
ath
ways
< 1
8 w
eeks
Referral to treatment
% incomplete pathways < 18 weeks
70%
75%
80%
85%
90%
95%
100%
105%
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17
% Diagnostic waiting list within 6 weeks
% Diagnostic waiting list within 6 weeks Target
Our plan had been to recover overall RTT performance by January 2018. However, October's performance (90.6%) deteriorated by 0.2% compared to September and the total number of patients waiting over 18 weeks was 314 higher than our plan.
The following divisions were non-compliant: -RNTNE – 84.53 (down 1.3%) Performance deterioration was driven predominantly by adult ENT (82.8%) where we reported 225 patients more than plan waiting over 18 weeks. Most of these are for community ENT services. -Eastman Dental Hospital – 89.5% (up 0.9%) -Queen Square – 89.1% (up 0.5%)
To address our under performance, the RTT improvement group has reviewed all specialty level plans, including compliant reporting units. This has led to a revised trajectory that could deliver compliance in February. However, this is contingent upon our understanding of the ENT backlog increase and our ability to take action to rapidly reduce this. Please see separate update for further details.
We reported five 52 week waiters: - 3 (2 neurosurgery and 1 ENT) were found during validation. All had incorrect clock stops earlier in their pathways. All were planned for treatment in November. Clinical harm reviews did not identify harm associated with their extended waiting times. We are working with the divisions to ensure shared learning from mistakes to reduce likelihood of recurrence. - 1 neurosurgery breach resulted from a tertiary referral from BHRUT at week 48. A clinical harm review has not identified harm. - 1 dermatology patient was also reported last month. They have treatment planned in Novembe.r A clinical harm review will be carried out after treatment but the suspicion of harm is low.
We sustained compliance with the six week diagnostic waits standard in October. Non-compliant modalities were: MRI (98.8%, 28 breaches at QS), uro-neurophysiology (93.1%, 16 breaches), urodynamics (87.1%, 8 breaches) and sleep studies (98.8, 2 breaches at QS).
Overall Page 42 of 64

4. Access4.3 Access Targets – Cancer
Thre
shold
Tru
st actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
Last m
onth
valid
ate
d
perf
orm
ance
Two week wait from referral to date first seen93% 93.9% 94.4% 92.9% 95.2% 89.9%
Two week wait from referral to date first seen: breast symptoms 93% 96.9% 96.9% 95.0%
31-day wait from diagnosis to first treatment 96% 96.9% 100.0% 94.0% 97.1% 98.8%
31-day wait for second or subsequent treatment: surgery94% 94.9% 100.0% 86.1% 100.0% 100.0%
31-day wait for second or subsequent treatment: drug treatments98% 94.9% 100.0% 100.0% 100.0%
31-day wait for second or subsequent treatment: Radiotherapy94% 99.0% 96.7% 100.0% 97.8%
31-day wait for second or subsequent treatment: other98.0% 100.0% 92.9% 100.0% 73.3%
62-day wait for first treatment from urgent GP referral to treatment85% 70.0% 100.0% 66.9% 76.9% 68.7%
62-day wait for first treatment from screening service referral90% 84.6% 100.0% 50.0% 66.7%
62-day wait for first treatment from urgent GP referral to treatment
Internal only85% 79.2%
Number of 104 day waits (from GP referral) Internal6 0 1 5 40
Number of 104 day waits (from GP referral) External10 0 2 8 12
% Inter trust referrals treated within 24 days of referral
* The trust threshold is an aggregate of individual clinical board thresholds
Month 7 - October
This month (not yet validated)
0%10%20%30%40%50%60%70%80%90%
100%
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17
Cancer 62 day referral targets
Target (GP referral to treatment) Cancer 62 day referral from screening to treatment
Target (screening to treatment) Cancer 62 Day GP referral to treatment
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17
Cancer 2 week referral targets
Cancer GP referral to appointment Cancer 14 day wait from referral (symptomatic breast) Target
We met our 62 day STF trajectory for August for internal pathways, but did not meet the internal trajectory for September and for October. We did not achieve the overall trajectory for September and are unlikely to meet this in the current financial year, although we are close to finalising plans with other providers that would deliver compliance in (Q1/Q2) 2018/19. We have reported 9 internal breaches (one fewer than September): breast (1), urology (3), Upper GI (2), lung (1), and head and neck (1). Some of these were due to complex reasons. A number of delays were initiated by patients. In general our improvement actions are focussed on much closer management of these patients' pathways so that we spot potential delays as early in the pathway as possible. We have received one output from the governance strand and are awaiting the final output from the operational strand of NHS Improvement's review of cancer performance. Please see the EB cancer recovery update for more information. October's provisional position for the 31 day first treatment is that we have met the standard for the first time in six months, as a result of clearing much of the backlog caused by a surge in external referrals 10 months ago. We reported compliance with the two week wait standard , although we narrowly missed the breast symptomatic two week wait target.
Overall Page 43 of 64

5. Quality5.1 Infection
Tru
st
thre
sh
old
Tru
st a
ctu
al
Me
dic
ine
Su
rge
ry &
Ca
nce
r
Sp
ecia
list
Ho
sp
ita
ls
Number of MRSA Bacteraemias 0 1 0 1 0
Number of clostridium difficile cases
reported (excluding successful
appeals)
55 17 6 6 4
Number of clostridium difficile cases
due to lapses in care2 0 1 1
Number of clostridium difficile cases
under review15 6 5 3
Number of clostridium difficile cases
successfully appealed21 9 5 7
Number of MSSA Bacteraemias 15 21 6 9 6
% - Infection control improvement
compliance (this month)95.0% 95.7% 92.1% 96.4% 96.5%
* The trust threshold is an aggregate of individual clinical board thresholds
YEAR TO DATE
Month 7 - October
0
1
2
3
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
MRSA bacteraemia / infections - All Services
MRSA actuals monthly MRSA threshold monthlyMRSA actuals YTD MRSA threshold YTD
0
50
100
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
Clostridium difficile infections post 48 hrs - All Services
CDiff Actuals Monthly excl. successful appeals CDiff Threshold Monthly
CDiff Actuals YTD excl. successful appeals CDiff Threshold YTD
We have reported 38 cases of C diff as at the end of October. 21 of these have been successfully appealed and 15 cases are under review. Two cases of C diff have been found to be a lapse in care by the Trust. Therefore, our worst case position currently is 17 cases against the September year to date threshold of 55. There were four cases of MSSA for October. One was within infection. The case is still under investigation via post infection review (PIR). Early indications suggest bacteraemia may be secondary to a urinary catheter change. Critical care had an MSSA infection. The root cause analysis showed better line documentation was needed. The MSSA in Queen Square is currently still being investigated; we will feed back on this next month. This is similar for the cancer division, where there was an MSSA on T13 and the division are awaiting the PIR . Infection control improvement compliance was better than threshold for the trust. The medicine board are slightly worse than threshold. The infection division is actively identifying areas for improvement. An action plan has been drawn up in conjunction with infection control (IC) team to address IC learning and practices on T8. This was presented at November T8 ward governance meeting.
Overall Page 44 of 64

Tru
st
thre
shold
Tru
st
actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
% Harm free care (National Safety
Thermometer)95.0% 96.7% 92.9% 95.7% 99.6%
% Harm free care (Hospital acquired
only)95.0% 97.9% 96.4% 96.5% 100.0%
Patients with preventable dose
omissions8.0% 5.2% 11.3% 3.8% 4.0%
Dose omissions audit - % submission
compliance100.0% 27.5% 33.3% 21.4% 30.0%
% eVTE Risk Assessments completed 95.0% 96.4% 93.7% 97.7% 95.9%
The trust threshold is an aggregate of individual clinical board thresholds
This month
Month 7 - October
5.2 Safety
5. Quality
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
10.0%
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17
Patients with preventable dose omissions- All Services
Preventable dose omissions Target
90%
91%
92%
93%
94%
95%
96%
97%
98%
99%
100%
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17
VTE risk assessment - All Services
Percentage of Completed eVTE Risk Assessments Target
We were better than the threshold of 95% for the National Safety Thermometer harm free care indicator at 96.7%. However medicine board is not achieving compliance which is reflective of a number of patients that acquired issues in the community which must nonetheless be reported against UCLH (see figures in table for hospital acquired percentage). The trust was compliant for the VTE assessment measure. However medicine were worse than threshold. This was mostly driven by medical specialties whose compliance was 92.5%.
Overall Page 45 of 64

5. Quality5.3 Safety
Tru
st
thre
shold
Tru
st
actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
Inpatient falls with serious harm 0 1.0 1 0 0
Falls per 1000 beddays 1.5 4.5 6.0 1.9 6.1
Falls with harm per 1000 bed days 0.9 1.3 0.9 0.6
Pressure ulcers acquired 4 7 3 3 1
Grade three pressure ulcers acquired 0 1 0 1 0
Grade four pressure ulcers acquired 0 0 0 0 0
The trust threshold is an aggregate of individual clinical board thresholds
This month
* falls with serious harm include severe, and death categories in Datix
Month 7 - October
0
1
2
3
4
5
6
0
20
40
60
80
100
120
140
160
180
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17
Patient falls per 1,000 bed days and Overall - All Services
Inpatient falls with harm Patient falls Falls per 1000 beddays
0
2
4
6
8
10
12
14
16
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17
Pressure Ulcers acquired at UCLH split by Grade/Category - All Services
Grade 4 Grade 3 Grade 2
There were 119 falls in total in October 2017; 96 no harm and 22 low harm. There was one severe fall, where unfortunately the patient died after surgery; a patient in the last stages of life fell and fractured their hip. A 72 hour review has occurred and the decision regarding whether this is a serious incident is still pending. Performance deteriorated this month with a total of seven pressure ulcers reported, six Grade 2 pressure ulcers against a trust threshold of four and one grade 3 pressure ulcer, against a threshold of 0. The grade 3 occurred on T6. This was a patient who had recently been diagnosed as terminally ill. On investigation there were no errors or omissions, with the patient clear with the clinical team that they did not want to comply with regular turns or pressure ulcer management and care.
Overall Page 46 of 64

5. Quality5.4 Outcomes
Tru
st
thre
sh
old
Tru
st
actu
al
Me
dic
ine
Su
rge
ry &
Ca
nce
r
Sp
ecia
list
Ho
sp
ita
ls
Emergency readmissions within 30
days
% Complete vital signs collected 96.0% 97.8% 97.1% 98.0% 98.0%
% deteriorating patients escalated
according to protocol90.0% 99.4% 98.5% 99.3% 100.0%
Local summary hospital-level mortality
indicator (1 yr rolling data)
This month
Month 7 - October
75%
80%
85%
90%
95%
100%
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17
% Complete Vital Signs collected - All Services
Percentage of Complete Vital Signs New Target Linear (Percentage of Complete Vital Signs New)
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17
Emergency readmissions within 30 days (with PbR exclusions)
Emergency readmissions within 30 days (with PbR exclusions)
Emergency admissions data is currently not available due to an upgrade to the trust's data warehouse. This should be available for next month's pack. We were compliant in achieving the threshold for vital signs observations in October.
Will be available next month
Overall Page 47 of 64

5. Quality5.5 Patient Experience
Tru
st th
resh
old
Tru
st a
ctu
al
Me
dic
ine
Su
rge
ry &
Ca
nce
r
Sp
ecia
list
Ho
sp
ita
ls
Complaints responded to within target
time85.0% 69.4% 46.2% 73.9% 90.9%
Inpatient friends and family test 96.5% 94.7% 94.3% 95.0% 94.5%
A and E friends and family test 95.0% 84.0% 84.0%
Outpatient friends and family test 93.0% 91.4% 90.3% 91.6% 91.6%
Response rate -Friends & Family Test (IP
survey)30.0% 18.9% 18.5% 17.2% 19.7%
Response rate- Friends & Family Test
(AE survey)20.0% 14.0% 14.0%
Response rate- Friends & Family Test
(OP survey)91.4%
.
% of hospital appointments postponed by
hospital2.9% 2.4% 4.0% 2.5%
Choose and book slot issues (two
months in arrears)17.3% 22.0% 29.2% 8.5%
This month
Month 7 - October
0
20
40
60
80
100
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17
Patient experience - Complaints received
Number of Patient Complaints Complaints responded to within target time Target
0%
20%
40%
60%
80%
100%
Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17
Patient Experience - FFT scores and response rate (IP & AE)
Friends & Family Test (IP survey) New FFT AE score Friends and Family - IP Response Rate FFT AE response rate %
We were worse than threshold for patient complaints response times in October at 69.4%. Medicine was worse than threshold at 46.2%. All divisions within the board had 100% compliance but for clinical support at 16%. This was due to patient transport with a significant increase in complaints over the last three months . Sickness in the team restricted the ability to respond to complaints in required timescales so they have agreed a process with complaints to try and make it more manageable. They are reliant on G4S for a lot of the complaint response. Cancer division were worse than threshold at 66%, this was due to one complaint narrowly missing the deadline. Imaging was 50% due to a backlog of responses due to staff moving to EPIC. Surgical specialties were worse than threshold but have improved performance following gaps in management team being filled. There has been an improvement in our FFT scores in all areas this month although we are still below target. Some of this improvement has been due to the adjustment of the ‘survey fatigue setting’ from 6 months to 4 months which means there have been more responses from patients. In A&E we have also started collecting feedback from paediatric patients which has improved both our response rate and score. We continue to have issues with the data extract due to technical errors, this has meant that we lost some data this month which could have affected our response rate for those areas that use text/video messaging. A report on FFT scores and response rates including a comparison with other trusts has now been shared with IEG and PEC. PEC has requested that further comparison against our peers is completed which will be used to inform our targets for next year.
Overall Page 48 of 64

6. Workforce 6.1 Performance indicators
Tru
st T
hre
sho
ld
Tru
st A
ctu
al
Me
dic
ine
Bo
ard
Surg
ery
& C
ance
r B
oar
d
Spec
ialis
t H
osp
ital
s B
oar
d
Co
rpo
rate
Bo
ard
Staff in Post (WTE) NA 7948.5 1558.3 2535.4 3067.0 787.8
% Temporary Staffing Filled via Bank 90.6% 85.0% 92.8% 92.0% 97.4%
Vacancy Rate 6.5% 8.0% 9.8% 8.0% 8.6% 1.6%
Voluntary Turnover Rate (12m Rolling) 12.5% 13.1% 14.9% 12.1% 12.9% 14.5%
The Trust Threshold Target and Trust Actual for Turnover excludes Corporate
Month 7 - October
This month Staff in Post: Staff in post rose by 89.5 WTE, from 7859 WTE to 7948.5 WTE in Month 7 Temporary Staffing: The percentage of temporary staffing filled by bank fell from M6 (91.8%) to M7 (90.6%). Overall use of temporary staffing fell -2.6% from M6 to M7, but, is 18% higher than in October 2016. Vacancies: The vacancy rate has reduced in M7 reflecting a growth of 89.5 wte in our substantive establishment with more than half of this growth in nursing and midwifery. Turnover: Turnover has decreased slightly from 13.5% to 13.1% month-on-month.
Overall Page 49 of 64

6. Workforce 6.2 Performance indicators
Establishment FTE*
Tru
st
thre
shold
Tru
st actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
Corp
ora
te
Functions
Sickness absence rate (%) 12m
RollingN/A 3.3% 3.1% 3.2% 3.8% 2.2%
All appraisals completed (Tier 1, 2 & 3)
All Staff above Band 7
95% (by the
end of Sep
2017)
88.9% 84.0% 89.9% 90.2% 90.3%
% Statutory and mandatory training
compliance95% 91.0% 90.5% 90.9% 90.9% 92.9%
Average time to recruit (request pack -
start date) (weeks)NA 14.0 14.2 13.7 15.3 10.7
Average time to recruit (request pack
received - unconditional offer) (weeks)N/A 10.5 11.0 10.0 11.2 8.3
Month 7 - October
This month
Sickness absence: Sickness absence has held steady at 3.3% for the last 4 months. Short term absence increased in September . Appraisal: The completion rate for appraisal in all tiers at the end of October was 88.9%. The completion rate for Tier 2 is 95.8%, and for Tier 3 was 86.4%. The Director for Education is continuing to keep compliance under regular review. Divisions are receiving reports of late appraisals on an individual basis. Mandated Training: Mandatory training rates have fallen slightly in M7. Honorary contract holders were added to our central record from this month. The Core Skills and Education Team are working with divisions to improve rates of compliance. Time to recruit: Time to recruit has remained at 10.5 weeks, preserving the slight improvement between M5 (10.6) to M6 (10.5).
Overall Page 50 of 64

6. Workforce 6.3 Nursing and Midwifery Detailed Workforce Dashboard
Month 7 - October
Overall Page 51 of 64

Estimated risk
Thresholds Weighting Oct 17 Q1 Q2 Q3
Q
4 Comments
55 1.0 17 14 14 17 8 cases successfully
reviewed
92% 1.0 90.6% 93.1% 90.7% 90.6%See page 8 for detail.
85% 70.0% 61.0% 66.7% 70.0%See page 15 for detail.
90% 84.6% 69.2% 78.3% 84.6%See page 9 for detail
94% 94.9% 84.9% 94.4% 94.9%See page 9 for detail
98% 94.9% 99.1% 99.5% 94.9%See page 9 for detail
94% 99.0% 99.2% 97.6% 99.0%See page 9 for detail
96% 0.5 96.9% 88.7% 89.2% 96.9% See page 9 for detail
93% 93.9% 94.2% 94.3% 93.9%See page 9 for detail
93% 96.9% 92.7% 93.0% 96.9%See page 9 for detail
95% 1.0 87.6% 91.1% 88.4% 87.6%See page 8 for detail
2 2 2 2 TBC
7. Externally Reported Frameworks 7.1 NHS Improvement Indicators – Compliance Framework
Indicators
62 day wait for first treatment from urgent GP referral
1.0
62 day wait for first treatment from consultant screening service referral
Incidence of Clostridium difficile year to date
Month 7 - October
31-day wait from diagnosis to first treatment (all cancers)
Two week wait from referral to date first seen: all cancers
0.5
Two week wait from referral to date first seen: symptomatic breast patients
Maximum time of 18 weeks from point of referral to treatment - incomplete pathways
Single Oversight Framework
31 day wait for second or subsequent treatment: Surgery
1.031 day wait for second or subsequent treatment: anti cancer drug treatments
31 day wait for second or subsequent treatment: Radiotherapy
A&E: Maximum waiting time of four hours from arrival to admission/ transfer/ discharge
The new Single Oversight Framework that has been put in place by NHS Improvement, and replaces the Monitor Assurance Framework. We have been notified that we have been placed in segment
two of this framework (this is of four segments; one denotes high performing, whilst four denotes formal turn-around). Our segment two status reflects non-compliance with three of the four
operational standards within the framework (diagnostic waits, A&E and cancer 62 day; we are achieving the RTT standard). This puts us in the bracket of requiring targeted, but not mandated, support
from NHSI
Overall Page 52 of 64

Council of Governors Meeting 23 January 2018
Chief Executive’s Report Attachment B – Corporate Objectives Q2 performance
Overall Page 53 of 64

UCLH 2017/19 Corporate Objectives: Tracking Delivery at Q2
Strategic Objective
Annual Objectives Lead Measures and deliverables Q2 update (currently showing Q1 update … please replace)
1 Provide Highest Quality Care within our resources
Align all clinical staff to work towards reducing avoidable harm
Tony Mundy
Reduce harm from unrecognised deterioration (including sepsis and AKI) - Deliver antibiotics to confirmed cases of sepsis within one hour
(Q1: 65%, Q2: 67.5%, Q3: 70%, Q4 72.5%). - Better understand how well we are recognising and treating
AKI in patients who develop AKI whilst inpatients, and see where any improvement work may be needed.
- Maintain average hospital-wide vital signs compliance of 96%. - Increase use SBAR tool when escalating to the PERRT team
(10% proportional increase on 16/17)
Reducing harm from surgery - Deliver planned programme of surgical safety walk rounds - Maintain 16/17 levels of surgical incident reporting - No surgical never events
Reducing harm from failure to follow up on radiology results - Repeat the audit to ensure that all areas have controls in
place to ensure that radiology results are followed up and that these controls are effective
36% (8/22) received antibiotics within 1 hour across Q2. Improvement plan being developed now trust AKI lead identified 98% vital signs achieved across Q2. Use of SBAR field in database at 60% compared to target of 54%. Increase of 7% since Q1. The programme is on target for Q2. Level of surgical incident reporting is slightly less than average. There have been no surgical never events. Asking all specialties how they monitor the effectiveness of their ‘safety nets’. Following up on actions from missed diagnosis serious incidents.
Improve how we learn from mortality, morbidity and serious incidents to sustain excellent outcomes
Tony Mundy
- Maintain current SHMI rating in top 4 of trusts - Implementation of learning from mortality in line with NHSI
guidance - Undertake structured judgement review (SJR) of deaths
identified by the UCLH selection tool - Increase percentage of SIs being investigated within 60 days
(75%)
Currently ranked 4th for SHMI Learning from deaths policy been agreed and published. SJR of deaths has started. The first report will go to the board in Q3. The mortality review group has agreed to pilot a new process for reviewing and learning from mortality. Currently reporting 83%
Improve patient experience
Flo Panel-Coates
- Improved trust FFT ratings and national inpatient and cancer patient surveys (FFT ratings 96% for inpatients and 94% for A&E)
- Improved use of patient stories - Improve patients experience of discharge – developing
metric to include in our local surveys
Q2 FFT ratings were: 92.9% for inpatients (92.3% inpatients and 93.4% day case) and 81.4% for A&E. Further work is ongoing to understand the drop in our A&E ratings. Paediatrics will be included in A&E scores from October 17
1
Overall Page 54 of 64

Strategic Objective
Annual Objectives Lead Measures and deliverables Q2 update (currently showing Q1 update … please replace)
- Improve patients’ reported access to CNS measured in national survey
We have seen significant improvement in the national cancer survey: 94% of patients reported that they were given the name of their CNS and 84% reported that it was easy to contact their CNS.
Ensure all contact with patients and GPs is timely, accurate and professional including a streamlined booking process
Gill Gaskin
- 80% of GP referrals booked via ERS by October - Delivery of advice and guidance services for GPs across
specialties that make up 35% of total GP referrals by year end
- Progress implementation of a patient portal
Our internal assessment demonstrates that we achieved 81% against the 80% October target for services available to GPs on e-Referrals. There is still some risk associated with the Q3 target, as previously reported, due to the challenge in achieving sufficient capacity for electronic bookings. New booking processes and patient portal will be built into EHRS design for implementation in April 2019.
Start implementation of an Electronic Health Record System and successfully implement pre-requisite systems
Gill Gaskin
- Delivery of the project according to agreed milestones - Implementation of co-ordination centre tracking (as a pre-
requisite to EHRS)
We have gained full board approval for EHRS, and the programme is on track. The co-ordination centre goes live on 5th December.
Achieve hospital acquired infection targets
Charles House
- Maintain current rates of C-diff per month - No MRSA cases
We are on track with our c-diff trajectory. We have reported 1 case of MRSA
2 Improve patient
Work with system partners to shorten waits for patients in our emergency department and avoid admission where possible
Charles House
- Deliver the A&E four hour wait trajectory (this varies from 91% - 95% per month)
- Maintain current conversion rate from ED (<12%)
We missed our agreed trajectory and delivery of STF monies in Q2. Actions based on ED processes, patient flow and discharge in place to improve. Conversion rate above target, attributed to reduced minors attendances.
pathways through collaboration with partners
Improve our patients’ experience of waiting, both from referral to diagnosis and treatment; and waiting in the building
Geoff Bellingan
- Deliver national standards for diagnostic 6 week wait (99%) - Deliver national standards for 18 weeks (92%) - Improve patient perception of waiting time in outpatients
(captured in our local surveys)
We continued to deliver the diagnostics standard across all months. We lost compliance with RTT in July. EAB has overseen the development and implementation of a recovery plan. The original aim was for January but this is at risk. A refreshed recovery trajectory for February is pending approval.
2
Overall Page 55 of 64

Strategic Objective
Annual Objectives Lead Measures and deliverables Q2 update (currently showing Q1 update … please replace)
Shorten waiting times at all stages of the pathways for cancer patients
Geoff Bellingan
- Deliver the performance trajectory for the cancer 62 day standard (achieving 85% by September)
- Deliver national standards for cancer 2 week waits (93%) - Deliver national standards cancer 31 days (96%)
We did not meet the Q2 cancer waits trajectory. However, we did meet internal compliance during August. NHSI recently concluded a review of cancer performance in relation to governance and operational delivery. This has led to a number of recommendations. In addition we have worked with the STP and UCLH cancer collaborative to conduct a series of bilateral meetings to produce shared pathway level action plans. We will have a defined trajectory for recovery once the sector position is clear and anticipate this in the next few weeks.
Deliver earlier diagnosis for cancer patients across the sector through the Cancer vanguard
Geoff Bellingan
- Successfully launch early diagnosis interventions to improve early diagnosis in priority areas (including lung and colorectal cancer)
- Scale up the multidisciplinary diagnostic centre model across the region
- Implement best practice diagnostic pathways in line with Vanguard delivery plan.
There are significant risks to delivery of the vanguard programme due to ongoing delays and uncertainty in receiving central funding. However, NEL has now achieved compliance with 62 days for the last quarter so there is strong likelihood that funding will be released for this part of the sector. Also there has been significant achievement in securing funding from non-NHS sources to support key programmes.
Deliver phase 4, phase 5, ED and Queen Square development milestones
Geoff Bellingan and Gill Gaskin
- Programmes delivered in line with project milestones The programmes are on track against the revised, agreed timeframes.
Work with local and specialist STP partners to develop new pathways and support preventative care for our local patients
Laura Churchward
- Progress partnership working with the Whittington in breast, bariatric, general surgery and maternity services
- Engage actively in STP urgent and emergency care; health and care closer to home; planned care and digital programmes
- Provide leadership for the cancer vanguard (for North Central and North East London STPs) and better births work-streams
- Engage in specialist STP as pathway discussions emerge - Engage actively in the Haringey & Islington Well-being
Partnership and Camden Local Care Delivery programmes
We are progressing work as planned through the Whittington/UCLH partnership board, with patients starting to move between sites and joint appointments being advertised and made. We have taken on significant additional leadership roles, including SRO for planned care programme. We are leading the neurology planned care workstream and are working with RNOH and WH on the potential of an orthopaedic hub.
3
Overall Page 56 of 64

Strategic Objective
Annual Objectives Lead Measures and deliverables Q2 update (currently showing Q1 update … please replace)
Our CD is the clinical lead for UEC and we lead simplified discharge and stroke pathways, with ‘Discharge to Assess’ now launched successfully. We are also heavily involved clinically and managerially in the Care Closer to Home Integrated Network, contributing to the H&I wellbeing partnership and the Camden Local Care Delivery boards.
3 Support
Improve staff experience
Ben Morrin
- Improve staff survey results - Reduce turn-over rates to 12.5%
Turnover increased to 13.1% (October), which is below the trajectory. A strategy is being developed to concentrate on key retention hotspots to improve turnover in the short term. UCLH is the STP lead with regards to tackling retention in the medium to long term. (2017 staff survey completion is a Q3 task)
the develop- ment of staff to achieve
Improve the quality of education and development
Ben Morrin
- Deliver plan for number of new apprentices in the trust - Increase number of staff on development programmes - 95% compliance with statutory and mandatory training
Apprenticeship numbers are lower than planned, mainly due to a delay in procurement for apprenticeship providers. However, plan to improve was agreed at SDT in October 2017. We are on target for 2000 staff to have attended development programmes. Mandatory training is at 91%, a slight decrease from 92% in Q1. We have changed 3 courses from e-learning to e-assessment and plan improved reporting to enable divisional managers to ensure completion in their areas and for subject matter experts to plan an adequate number of training sessions.
their full potential
Demonstrate that we are an employer of choice
Ben Morrin
- Sustain low vacancy rate of 6.5% - 95% appraisals completed by end September - Improve quality of appraisals as measured by staff survey - Deliver improvements to staff environment and facilities
within the CQUIN plan
The vacancy rate at end of September was 8.2%. This is above plan due to a slowing of recruitment activity and an increase in turnover in areas facing significant national and international shortages in supply. Retention plans are being developed to improve turnover.
4
Overall Page 57 of 64

Strategic Objective
Annual Objectives Lead Measures and deliverables Q2 update (currently showing Q1 update … please replace)
The HRBPs are working with departments to improve appraisal completion and ensure 95% are completed by year end. Steps to improve staff facilities are progressing in line with plan.
Improve working conditions for junior doctors and other staff in training
Ben Morrin
- Deliver improvement plan based on GMC survey feedback - Evidence of engagement with dental trainees in advance of
phase 5
GMC survey results show that we fare favourably with Shelford trusts and against national averages where there has been a decrease in satisfaction nationally
Collaborate with STP and others to design and develop the future health and care workforce
Ben Morrin
- Deliver shared staff bank - Deliver mechanism for shared staff contracts with partners
UCLH is tendering for our future supplier of a staffing bank. The tender allows for neighbouring trusts to commit to the same model. A mechanism for employment portability for UCLH and Whittington Health staff has been signed off at Executive Board level (by both) and shall shortly be launched.
Develop our staff to achieve transformational change
Ben Morrin
- Deliver plan for number of staff attending the institute quality improvement training
- Deliver plan for number of staff attending the leading change training
Our plan for staff attending QI training is on target at over 300 staff this calendar year. The band 5-7 leader development started in September and 3 cohorts have attended this programme.
4 Achieve
Achieve financial targets and deliver the £42m cost improvement programme
Tim Jaggard
- Deliver agreed CIP plan - Deliver the trust’s control total
We are behind plan at Q2 and are forecasting a significant shortfall against plan by year-end. The Board has appointed a turnaround director and strengthened programme management office to help UCLH deliver in-year savings and significantly improve run-rate financial performance
financial sustaina- bility
Deliver clinical productivity efficiencies in line with the Carter agenda
Gill Gaskin
- Improve use of electronic rotas for clinical staff - Reduce in-session opportunity lost in our theatre lists to 10% - Develop monitoring and then improve outpatient room
utilisation - Reduce LOS in line with agreed targets
Medirota is being rolled out across the Trust. We are developing outpatient room utilisation reporting but establishing a baseline capacity has been challenging. Pragmatic focus is therefore on increasing total number of attendances.
5
Overall Page 58 of 64

Strategic Objective
Annual Objectives Lead Measures and deliverables Q2 update (currently showing Q1 update … please replace)
Trust LOS is better than target for both non-elective and elective admissions at the end of Q2.
Take a leading role within the NCL and specialist sustainability and transformation partnerships (STPs) to support financial objectives
Tim Jaggard
- EB members to maintain leadership roles within STP - Deliver STP milestones as they emerge - Work with partner organisations in North Central London to
improve the financial sustainability of the Trust and the STP
We continue to lead a number of STP work-streams and the CEO has taken on the SRO role for planned care. We continue to play a leadership role in the financial and productivity work across the STP although the STP as a whole has a very significant financial gap to control totals.
Improve management of commercial relationships
Tim Jaggard
- Creation of contract register with contract management arrangements identified
- Roll out best-practice model for contract management - Deliver significant financial value from more robust contract
management, of at least £1m in 2017/18
Contract register created. Additional technology-enabled contract management support provided to the PFI and other contracts. On track to achieve the anticipated level of savings for 2017/18
Achieve value for money from our assets and estate
Tim Jaggard
- Work with STP estates work-stream to support NCL-wide benefit
- Reduce I&E impact of PFI charges to contribute towards cost improvement programme by at least £100k per year
- Use Carter data on estates and facilities costs to improve value for money across the PFI estate
UCLH sits on the NCL estates board to develop an NCL-wide estates strategy. Plans to dispose of the Eastman Dental Hospital to UCL are progressing, and there is ongoing work with NHSI and DH in relation to the PFI. Carter work has identified further opportunities for savings.
Deliver more efficient use of non-pay resources
Medical Directors
- Deliver pharmacy hospital transformation plan - Improve performance against on non-pay weighted output
measure
The hospital pharmacy transformation plan is progressing well. We have not yet seen an improvement in the non-pay weighted output measure.
5 Generate research
Deliver the promises of the Biomedical Research Centre bid
Tony Mundy
- Deliver Biomedical Research Centre project milestones - Increase numbers of patients in early phase clinical trials (by
5%)
Patient recruitment to early Phase clinical trials is comparable to previous years Number of research publications on course to meet the total number reported in 2016/17.
world class clinical
Give as many of our patients as possible the opportunity to be part of research trials
Tony Mundy
- Increase numbers of patients in research trials (by 5%) - Improve patients’ experience in research
The AboutMe project will implement consent for recall process across UCLH. The project is in the advanced stages of planning
Progress clinical academic appointments within UCL and other academic partners
Marcel Levi
- Increase number of clinical academic appointments in line with plan
We have developed and agreed on criteria in collaboration with academic colleagues. These are being discussed in the SDT in January and subsequently with the Provost and Vice-provost of UCL. We expect that the discussion will be finalised before April 2018.
6
Overall Page 59 of 64

Strategic Objective
Annual Objectives Lead Measures and deliverables Q2 update (currently showing Q1 update … please replace)
Work with partners, including HSL, to develop academically-linked, advanced diagnostics and embed genome testing.
Geoff Bellingan
- Plan for improving diagnostic capability in place and agreed with partners
- Plan delivered to time-frames - Use of genome testing in agreed areas
The programme is progressing but requires further clarity on details.
Improve utilisation of our clinical research facilities
Tony Mundy
- Increase activity in CRF (by 5%) - Increase activity in Leonard Wolfson (by 5%)
Activity volumes have increased in line with plan. Both CRF sites have specifically increased their volume of highly risky and highly intense first-in-man/phase I clinical trials
Develop and encourage research opportunities for junior doctors, nurses and all other staff across UCLH
Bryan Williams
- Specific plan to be developed by research and development department
Junior doctors – the first cohort of research fellows has been selected, with 27 funded fellows being supported to develop research activities alongside their clinical care duties.
7
Overall Page 60 of 64

Council of Governors Meeting23 January 2018
Chief Executive’s ReportAttachment C – CQC action plan
update
Overall Page 61 of 64

Attachment C
Care Quality Commission Inspection Update Report and Action Plans
1. Progress with the Trust-wide Action Plan2.1 Ensure mandatory training targets are met consistently (discussed at every meeting)
Honorary contract (HR) holders – A significant validation programme has been undertaken to establish which individuals are still at UCLH providing patient care and in which role. A significant reduction has been made in the number of HR contract holders of unclear status. The remainder are to be checked with supervisors. Any remaining will be removed from the system. If anyone has been removed who needs to be reinstated they can be quickly added when we have the correct details about position and manager.
Mandatory Training Passport – We are aiming to join the passport scheme, which would enable staff to move between organisations without the need to re-do training between each. It is possible that joining the scheme will require UCLH to increase the number of mandatory training courses, since we currently provide less than is expected in the Core Skills Framework)..
2.2 Recognising and responding to deterioration (discussed quarterly)
2.2.1 Maintain average hospital-wide vital signs compliance of 96%
We are maintaining a mean of 98.4% vital signs completion trust-wide.
2.2.2 Achieve a 10% relative increase in inpatients being escalated to PERRT using the communication tool SBAR/ ISBARD from the 2015/16 baseline of 63% to 69%: and a 10% relative increase in recording of this metric (by PERRT) from the 2016/17 baseline of 49% to 54% of referrals.
Data was only available for July and August. ‘Use of SBAR’* field was completed on the PERRT database in 60% of these referrals against a target of 54%. Of these where it was recorded, 55% used SBAR/ ISBARD* against a target of 69%. Recording whether SBAR has been used has increased from last quarter by 7% and the use of SBAR has dropped slightly by 2%. ISBARD was launched in September and it is anticipated that the percentage using ISBARD to communicate will increase next quarter. Regular audit data for ISBARD compliance will be available from March 18 via essence of care audits.*(I) Introduction, (S) Situation, (B) Background, (A) Assessment, (R) Recommendation, (D) Decision
2.3 Sepsis (discussed quarterly)
2.3.1 Deliver antibiotics (ABX) to confirmed cases of sepsis within one hour (Targets are: Q1: 65%, Q2: 67.5%, Q3: 70%, Q4 72.5%) Across the three months in quarter, of the patient records reviewed 22 patients in total met the sepsis criteria. 8/22 (36%) received ABX within one hour against a target of 67.5%. This means we did not meet the target for this section of the CQUIN this quarter.
2.3.2 Undertake a clinical review of antibiotics within 72 hours of giving the first dose in 90% of patients with sepsisBased on a random sample of blood culture requests we identified and collected this data for 30 patients in Q2 that met the UCLH sepsis criteria. 100% patients received a clinical review of antibiotics within 72 hours of giving the first dose.
2.3.3 Pain scores / documentation (discussed in January 2018)
Overall Page 62 of 64

In response to the CQC observation that NEWS scores were not always filled out, work has been carried out on T8 and AMU to improve completion of the pain section on the NEWS chart. Audit pre and post training has shown some improvement but it was noted that sustained change is difficult with the high turnover of staff (currently a 24% vacancy rate on AMU). We have been quite successful carrying out a culture change exercise around pain and have covered a range of staff in a number of ways, including training at the junior doctor induction day. Training effects decay over time so we want to implement a sustainable training system.
2.3.4 Dementia (discussed in January 2018)The CQC recognised that patients with dementia were identified by a forget-me-not blue flower, however, the CQC did not witness this being translated into person-centred care. Local audit has been carried out on AMU, T7 and T10M where 21 patients with dementia were identified. Most of them were highlighted on the wards via the flower next to their name on the main patient details board. Only a few patients had a THIS IS ME card completed (mainly by the nurse specialist in AMU). The card has been available for five years but the uptake is poor. Nurses and nursing assistants (NA) on wards can provide good information verbally about their patients but don’t routinely document it. Both national and local audit results reflect that we are delivering good patient care and know our patients’ needs, but don’t record it. In response to this, T10M is carrying out some exemplar ward work on an adaptation to the THIS IS ME cards, a simple sheet above the bed called ‘Improve my care’. Work is also taking place on Evergreen, with information on notes at the end of beds and information sharing at handover. The EHRS project is to be approached about incorporating these into the electronic patient record for assurance.
2. Divisional action plans3.1 Emergency department (ED) action plan (discussed in November 2017)
3.1.1 Capacity and patient flowThe new extension of the department was opened on 8th January, on schedule. It has been achieved by joining the main University College Hospital building and the Elizabeth Garrett Anderson Wing at the ground floor level. We now have:
One interconnected ED A new waiting area and reception New assessment rooms A new imaging and diagnostic suite A bigger urgent treatment centre with 12 bays and three treatment rooms A new entrance for ambulances.
The new coordination centre has opened so that Teletracking is now live and improving capacity,A new associate Clinical Director has been appointed to focus on patient flow.
3.1.2 Workforce Recent action has been to focus on workforce, such as decreasing the use of locums. On AMU, there has been work around duty medical registrar cover, medical registrar for acute work within ED and Infection. There has been some focused recruitment. A staff engagement programme commenced in August and early results are positive. There is a band 7 development programme in place across the division.
3.1.3 Patient experience There has been some bespoke work around pain management, with 75% of staff now trained and a recent audit has seen an improvement.
Overall Page 63 of 64

The recent ED patient survey results places UCLH at the top of London trusts and the Shelford Group for overall patient experience.
3.1.4 Mental health The service level agreement with Camden and Islington and standard operating procedure are to be finalised and agreed. The Mental Health Act will be amended next year so that a police station is no longer a ‘place of safety’. This will place increased demands on ED. There is an agreed escalation protocol with Camden and Islington in place however concerns about ED’s capacity to manage increasing activity in this area have been acknowledged.
3.1.5 Patient safety checklist NHS Improvement is recommending the use of the checklist and it is being launched in the ED.
3.2. Medical care (Discussed in November 2017)
Medical Documentation – The CQC inspection report commented that the quality of notes was poor for Medical Care. There is still no internal process to audit notes for medical staff. We take part in the national 7 day care audit twice a year and medical wards’ compliance was better in November.
4. Peer review visit by the Emergency team at Guy’s and St Thomas NHS Foundation Trust (GSTT)We are grateful to our colleagues from GSTT who conducted a peer review in the ED, AMU and on ward T7 in October. They provided useful feedback. Some of the issues they found will be rectified this month as the new ED has opened.
5. Next StepsWe will continue to monitor the action plans and have now developed an assurance tool which helps us to focus more on evidence of improvement. We will continue to monitor actions regularly.
Cathy MooneyDirector of Quality and Safety
Overall Page 64 of 64