Costs of Neurostimulation. Can We Afford The Therapy in 2020?. Krishna Kumar MBBS MS FRCS(C) Member Ord. of Canada, Saskatchewan Ord. of Merit Clinical Professor of Neurosurgery Department of Neurosurgery Regina Canada. Syed Rizvi MD Department of Neurology University of Saskatchewan - PowerPoint PPT Presentation
Slide 1
Costs of NeurostimulationCan We Afford The Therapy in
2020?Krishna Kumar MBBS MS FRCS(C) Member Ord. of Canada,
Saskatchewan Ord. of MeritClinical Professor of
NeurosurgeryDepartment of NeurosurgeryRegina Canada
Syed Rizvi MDDepartment of NeurologyUniversity of Saskatchewan
Regina Canada1DisclosuresAct as a consultant for Medtronic Inc. And
Boston Scientific.
Have received research grants from Medtronic Inc.
Disclosures2DisclosuresPolicymakers require evidence of
comparative cost-effectiveness in order to continue to make funding
decisions
To make the case for neurostimulation we use SCS as a
prototype
This presentation illustrates the long-term cost-effectiveness
of SCS compared with CMM as projected for the year 2020
Introduction3National Institute of Arthritis and Musculoskeletal
Skin Diseases website. News and Events Page.
ghttp://www.niams.nih.gov/ne/highlights/spotlight/2006/back_pain_study.htm.
Institute of Medicine. Relieving Pain in America: A Blueprint for
Transforming Prevention, Care, Education, and Research. Washington,
DC: The National Academies Press. 2011. Darrell J. Gaskin, Patrick
Richard. The Economic Costs of Pain in the United States. The
Journal of Pain, 2012; 13 (8): 715 DOI:
10.1016/j.jpain.2012.03.009Projected4DisclosuresTo evaluate the
cost impact of SCS against CMM over time we will project costs for
4 commonly encountered chronic pain syndromes:
FBSS (Failed Back Surgery Syndrome)CRPS (Complex Regional Pain
Syndrome)PAD (Peripheral Arterial Disease)RAP (Refractory Angina
Pectoris)
Introduction5MethodsMarkov model developed to evaluate the
cost-effectiveness of SCS versus CMMModel inputs derived from 313
patients
Costs and outcomes followed in six-month cycles
Health effects expressed as quality-adjusted life years (QALYs)
gained
Costs and effects were evaluated over an 8-year time horizon
(2012-2020) and discounted at 3.5% per annum
Methods6Cost-effectiveness was identified by deterministic and
probabilistic sensitivity analysis (50,000 Monte-Carlo
iterations)
Outcome measures presented:
CostEffectiveness (EQ-5D)Incremental cost-effectiveness ratio
(ICER)Incremental net monetary benefit (INMB)Acceptability of
treatment (CEAC)Expected value of perfect information
(EVPI)Strategy selection frequencyMethods7Judging
Cost-effectiveness:Willingness-to-Pay (WTP)USA and Canada: $50,000
/ QALY 1 , 2
United Kingdom: 20,000- 30,000 / QALY 3Willingness to
Pay:Judging Cost-effectiveness 1Braithwaite RS, Meltzer DO, King JT
Jr, Leslie D, Roberts MS. Med Care 2008; 46(4): 343-5.2King JT Jr,
Tsevat J, Lave JR, Roberts MS. Med Decis Making 2005; 25(6):
667677.3Devlin N, Parkin D. Health Economics 2004; 13(5):
437-452.8Markov ModelTreatment OptionsSCSTrialCMMSuccessOptimal
Health StateSuboptimal Health StateCMMCMMOptimal Health
StateSuboptimal Health StateFailureImplantDeathDeathTreeAge Pro
2011 (TreeAge Software Inc., Williamstown
MA)9FBSSCRPSPADRAPVariableBase CaseStd DevBase CaseStd DevBase
CaseStd DevBase CaseStd DevCost SCSPre-implant (Source: Hospital
Finance Department)$4,120$515$4,161$495$4,165$529$4,249$546Implant
procedure (Source: Hospital Finance
Department)$22,750$2,844$23,226$2,764$23,834$3,027$21,981$2,825Complications
(Source: Neuromodulation
Clinic)$467$58$425$51$481$61$443$57Maintenance (Source:
Neuromodulation
Clinic)$3,170$396$3,696$440$4,236$538$3,783$486Adjunctive therapy
(Source: Neuromodulation
Clinic)$1,130$141$1,141$136$1,142$145$1,165$150Pharmacotherapy
(Source: Neuromodulation
Clinic)$267$33$269$32$269$34$275$35CMMEvaluations and follow-up by
health care providers (Source: Patient
Database)$785$98$793$94$794$101$810$104Imaging (Source: Patient
Database)$1,450$181$1,465$174$1,466$186$1,495$192Pharmacotherapy
(Source: Neuromodulation
Clinic)$800$100$808$96$809$103$825$106Alternative therapy (Source:
Patient
Database)$2,355$294$2,379$283$2,381$302$2,429$312Intermittent
hospitalization/Emergency Room visits (Source: Patient
Database)$1,500$188$1,515$180$1,517$193$1,547$199EQ-5D (Source:
Patient Database)Optimal CMM health state
0.540.070.520.060.510.060.540.07Optimal SCS health
state0.620.080.590.070.550.070.560.07Suboptimal CMM health
state0.320.040.270.030.220.030.210.03Suboptimal SCS health
state0.410.050.420.050.370.050.320.04Probability (Source: Patient
Database)Optimal CMM health
state0.200.030.200.020.180.020.220.03Optimal SCS health
state0.600.080.650.080.600.080.850.11Transitioning from SCS
suboptimal health state to an optimal health state in the CMM
strategy0.200.030.220.030.170.020.160.02Suboptimal CMM health
state0.700.090.660.080.720.090.630.08Suboptimal SCS health
state0.300.040.280.030.360.050.310.04Transitioning from SCS
suboptimal health state to a suboptimal health state in the CMM
strategy0.700.090.690.080.710.090.750.10Death0.010.000.010.000.050.010.050.01This
the input table for the model and includes the cost, effectiveness,
and probability values that were input into the Markov
model.10Results11Costs, Effectiveness, and ICERs associated with
SCS+CMM and CMMStrategySCS+CMMCMMFBSSCost
(CAN$)$89,094$82,654Effectiveness (QALY)3.062.18ICER (cost per QALY
gained)$7,318CRPSCost (CAN$)$105,049$91,968Effectiveness
(QALY)1.823.18ICER (cost per QALY gained)$9,618PADCost
(CAN$)$96,113$88,017Effectiveness (QALY)1.652.76ICER (cost per QALY
gained)$7,294RAPCost (CAN$)$99,043$110,932Effectiveness
(QALY)1.673.13ICER (cost per QALY gained)$8,143The ICER is
calculated by dividing the difference in cost by the difference in
QALY. The ICER of SCS over CMM for FBSS is thus $7,318 per QALY
gained. In other words, to gain 1 QALY one must be willing to spend
an additional $7,318 over CMM. 12Similar diagram for other pain
pathologies
Incremental Cost-Effectiveness RatioDeterministic Sensitivity
Analysis: Tornado Diagram for FBSSThe tornado diagram displays the
results of the deterministic sensitivity analysis. It highlights
the model parameters that most significantly affect the results of
our cost-effectiveness analysis. The most important parameters in
order of their influence are: 1) Probability of achieving an
optimal health state with CMM 2) Cost of achieving a suboptimal
health state with CMM and 3) Probability of achieving a suboptimal
CMM health state after failing SCS trial. Thus adjusting these 3
variables will most significantly affect the analysis. 13
Probabilistic Sensitivity Analysis: ICER Scatter plot for
FBSSThe incremental cost-effectiveness scatter plot
diagrammatically represents the results of the probabilistic
sensitivity analysis. The majority of simulations are tightly
clustered, indicating good analytical validity. It is evident that
SCS provides increased effectiveness (x-axis) but at an increased
cost (y-axis) over CMM.
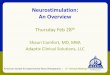
14Incremental Net Monetary Benefit of SCS over CMMThe
incremental Net monetary benefit encapsulates the
cost-effectiveness argument from the payers perspective. In fact,
for any WTP threshold $7,000/QALY SCS generates a positive
incremental net monetary benefit over CMM. For a program
administrator deciding between two strategies, the incremental net
monetary benefit tells you which strategy is better in terms of
benefits relative to cost. The INMB is calculated by analyzing the
difference in NMB between SCS and CMM. A positive incremental net
monetary benefit indicates that SCS should be implemented over CMM
for these patients with FBSS as the benefits of therapy outweigh
the costs. There is a linear increase in incremental Net monetary
benefit for SCS over CMM as WTP increases. At commonly accepted WTP
thresholds, SCS generates a positive incremental net monetary
benefit over CMM. The incremental net monetary benefit is
calculated by subtracting the Net monetary benefit of each strategy
(SCS and CMM in this case). The net monetary benefit of each
strategy can be calculated by the following formula:Net monetary
benefit = Effectiveness [(QALY) x WTP] Cost.
15Cost-Effectiveness Acceptability Curve: SCS over CMMThe
cost-effectiveness acceptability curve is generated through our
probabilistic simulations. Non-parametric bootstrapping methods
were used to estimate the distribution of incremental costs and
effects associated with SCS compared to CMM in order to generate
the cost-effectiveness acceptability curve.
The cost-effectiveness acceptability curve represents the
probability that SCS is a more cost-effective alternative to CMM at
various willingness to pay thresholds. The willingness to pay
threshold are plotted on the x-axis. The probability of
cost-effectiveness (which ranges from 0-1) is plotted on the
y-axis. For instance, at a willingness to pay threshold of $50,000
per QALY (a figure often cited) there is a 73% likelihood that SCS
is more cost-effective to CMM in the management of FBSS.
16Strategy Selection FrequencyBased on a simulation of 50,000The
strategy selection frequency indicates the proportion of
simulations in which a strategy generated the most economical
results. 64% of the time SCS was a more optimal strategy than
CMM.
17Reliability of the Model:Expected Value of Perfect Information
(EVPI)The strategy selection frequency indicates the proportion of
simulations in which a strategy generated the most economical
results. 64% of the time SCS was a more optimal strategy than
CMM.
18Comparative Study of Rechargeable and Non-rechargeable IPGWe
separately analyzed the cost-effectiveness of rechargeable
(RestoreAdvanced) and non-rechargeable (PrimeAdvanced) IPGs. The
lifespan of the non-rechargeable IPG is plotted on the x-axis while
the Net monetary benefit is plotted on the y-axis. A positive NMB
indicates that the benefits outweigh the costs.
From the graph is it is evident that the rechargeable IPG is the
preferred solution if the lifespan of the non-rechargeable IPG is
less than 4.25 years. 19ConclusionBased on our projections SCS will
remain a cost-effective therapy in the management of neuropathic
and ischemic pain in the year 2020
SCS provided a positive INMB over CMM at WTP thresholds $7,000
per QALY
The probability of SCS providing a cost-effective alternative to
CMM ranged from 74-95%, depending on pathology and WTP
The rechargeable IPG is more cost-effective if the lifespan of a
non-rechargeable IPG 4.25 years20