Embed Size (px)
Citation preview

HEALTH ECONOMICSHealth Econ. 17: 833–848 (2008)Published online 13 September 2007 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/hec.1299
COST INEFFICIENCY AND HOSPITAL HEALTH OUTCOMES
NICCIE L. MCKAYa,*,y and MARY E. DEILYb,z
aDepartment of Health Services Research, Management and Policy, University of Florida, Gainesville, FL, USAbDepartment of Economics, Lehigh University, Bethlehem, PA, USA
SUMMARY
This study explores the association between cost inefficiency and health outcomes in a national sample of acute-carehospitals in the US over the period 1999–2001, with health outcomes being measured by both mortality andcomplications rates. The empirical analysis examines health outcomes as a function of cost inefficiency and otherdeterminants of outcomes, using stochastic frontier analysis to obtain hospital cost inefficiency scores. The resultsshowed no systematic pattern of association between cost inefficiency and hospital health outcomes; the basicresults were unchanged regardless of whether cost inefficiency was measured with or without using instrumentalvariables. The analysis also indicated, however, that the association between cost inefficiency and health outcomesmay vary substantially across geographical regions. The study highlights the importance of distinguishing between‘good’ costs that reflect the efficient use of resources and ‘bad’ costs that stem from waste and other forms ofinefficiency. In particular, the study’s results suggest that hospital programs focused on reducing cost inefficiencyare unlikely to be associated with worsened hospital-level mortality or complications rates, while, on the otherhand, across-the-board reductions in cost could well have adverse consequences on health outcomes by reducingefficient as well as inefficient costs. Copyright # 2007 John Wiley & Sons, Ltd.
Received 21 December 2006; Revised 22 June 2007; Accepted 7 August 2007
KEY WORDS: hospital efficiency; hospital costs; hospital outcomes; hospital mortality; hospital complications
Quality improvement and cost containment in hospitals are central objectives of current health policy.A continuing policy concern is that efforts to control costs could lead to worsened health outcomes.Although the precise nature of the relationship between costs and health outcomes in hospitals is stillthe subject of considerable debate, logically, if costs are reduced enough, at some point poorer healthoutcomes would result. However, if cost containment programs focus on and are successful ineliminating primarily wasteful costs, rather than simply reducing costs, the more important question isthe association between cost inefficiency and health outcomes, the topic of this study.
A key contribution of this study is the distinction between two components of total costs – costs thatreflect the best use of resources under current circumstances (‘good’ costs) and costs associated withwaste or inefficiency (‘bad’ costs). That is, even the most efficient and productive hospital must incur acertain level of cost to operate effectively and safely. However, studies indicate that on average hospitalsalso have some costs that are due to waste or poor decision-making (Chirikos, 1998/1999; McKay et al.,2002/2003; Rosko, 2001; Zuckerman et al., 1994). The major objective of this study is to examine therelationship between costs due to inefficiency and patient health outcomes in hospitals.
In a previous study of urban hospitals in Florida over the period 1999–2001, we found a positive andsignificant relationship between cost inefficiency and in-hospital mortality, controlling for expected
*Correspondence to: Department of Health Services Research, Management and Policy, University of Florida, PO Box 100195,Gainesville, FL 32610-0195, USA. E-mail: [email protected] Professor.zProfessor.
Copyright # 2007 John Wiley & Sons, Ltd.

mortality (Deily and McKay, 2006). A key limitation of the study is that it used data from a single state,raising the question of whether the results could be generalized to other states. This study builds on ourprevious work by examining the relationship between costs and health outcomes in a national sampleover the same period. In addition, the current study examines risk-adjusted complications as well asrisk-adjusted mortality as measures of hospital-level health outcomes, and uses a different method ofrisk adjustment.
Specifically, in this study we explore the association between cost inefficiency and outcomes asmeasured by mortality and complication rates in a national sample of acute-care hospitals in the USover the period 1999–2001. The study examines health outcomes as a function of cost inefficiency andother determinants of outcomes, using stochastic frontier analysis to obtain hospital cost inefficiencyscores.
With health-care costs again rising at a rapid rate, understanding the links between cost inefficiencyand health outcomes is critical. The results of this study have important policy implications for hospitalsand policymakers seeking to accomplish simultaneously cost control and quality improvementobjectives. If higher levels of cost inefficiency are associated with better health outcomes (which seemsunlikely), hospitals would face extremely difficult tradeoffs between controlling costs and improvinghealth outcomes. If cost inefficiency has no effect on health outcomes, cost control programs could beundertaken without expected adverse effects on health outcomes. Finally, if higher levels of costinefficiency are associated with poorer health outcomes, programs aimed at reducing cost inefficiencywould also be expected to be associated with better health outcomes.
PREVIOUS RESEARCH
There are extensive literatures on factors affecting hospital costs and hospital health outcomes.However, relatively few studies have addressed the relationship between costs and health outcomes, andeven fewer have examined the link between cost inefficiency and outcomes.
Previous studies of the relationship between overall costs and health outcomes in hospitals have cometo conflicting conclusions. Some studies have found a positive association between costs and healthoutcomes in hospitals, while others have concluded that cost reduction and improvements in healthoutcomes are compatible goals (see, for example, Carey and Burgess, 1999; Fleming, 1991; Mukamelet al., 2001).
A somewhat different approach has been to examine characteristics associated with hospitalperformance as measured jointly by costs and health outcomes. A recent study by Jiang et al. (2006)classified hospitals on performance measured by both cost per discharge and a composite mortalityscore using Healthcare Cost and Utilization Project data for 10 states in 1997 and 2001, and found thatfor-profit ownership, hospital competition and the number of HMOs were positively associated with thelikelihood of attaining high-quality/low-cost performance.
Morey et al. (1992) appear to be the first to examine cost–quality relationships where the differencebetween efficient and inefficient costs was considered. They investigated the relationship betweenefficient cost and excess mortality; using data for 300 hospitals in 1983, the study found that a 1%decrease in the ratio of observed-to-predicted deaths was associated with a 1.34% increase in efficientcost, as measured using Data Envelopment Analysis (DEA).
In a more recent study, Deily and McKay (2006) examined the effect of cost inefficiency on observedin-hospital mortality rates for urban, acute-care hospitals in Florida over the period 1999–2001. Theresults indicated that cost inefficiency had a stable, positive, and statistically significant effect on theobserved mortality rate, controlling for risk-adjusted expected mortality and other factors affectingmortality. At the mean values of the control variables, a 1% point reduction in cost inefficiency wasassociated with 1 fewer death per 10 000 discharges.
N. L. MCKAY AND M. E. DEILY834
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

In a related study, McKay and Deily (2005) examined characteristics associated with high- and low-performing hospitals, measuring performance in terms of both risk-adjusted excess mortality and costinefficiency using data for urban, Florida hospitals over the period 1999–2001. The results indicatedthat hospitals in the high-performing group were more likely to be for-profit and used fewer patient-carepersonnel per admission than all other hospitals; however, managed care presence, measured by theproportion of HMO-PPO admissions, was not a significant factor in differentiating hospitalperformance groups.
CONCEPTUAL FRAMEWORK
The standard economic theory of the firm posits a production function, in which a production processtransforms inputs into outputs, and assumes that, for a given set of input prices, the firm chooses the setof inputs that will minimize the cost of producing a given amount of output at a given level of quality.The production process itself is taken as given, with no description of how inputs are transformed intooutput. In this approach, any inefficiency occurs only temporarily, and randomly, as the firm adjuststoward optimization.
Hospitals use inputs, such as nurses, physicians, buildings, and equipment, to provide a given amountof hospital care output, such as number of inpatient days, admissions, and outpatient visits. Thedemonstrated existence of non-random cost inefficiency in hospitals (Chirikos, 1998; McKay et al.,2002/2003; Rosko, 2001; Zuckerman et al., 1994) indicates that on average hospitals are not minimizingcosts, which we assume stems from problems with the production process.
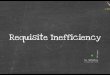
However, analyzing the relationship between hospital costs and health outcomes is complicated byissues related to quality. Hospital quality is typically defined in terms of: (1) structure, or quality ofinputs, (2) process, and (3) outcomes, or quality of outputs (Donabedian, 1980). In this categorization,patient health outcomes thus are a component of output quality. Combining the standard theory of thefirm with these different elements of hospital quality, the conceptual framework has inputs of a givenquantity, quality, and price, which are transformed by a production process that yields output of a givenquantity and quality produced at some total cost (see Figure 1). Holding input quality, input prices, andoutput quantity constant, both costs and output quality will depend on the production process (or,more realistically in the case of a complex service such as hospital care, processes). Moreover, becauseon average hospitals are not minimizing costs, total cost typically has two components – costsassociated with optimal choices (best-practice cost) and costs associated with waste or non-optimalchoices (cost inefficiency).
The link between cost inefficiency and health outcomes thus depends on the nature of the productionprocesses in the hospital and the extent to which they affect cost inefficiency and health outcomesindependently. One possibility is that some production processes affect primarily cost inefficiency, whileothers primarily influence output quality. For example, cost inefficiency may depend largely onprocesses related to inventory control or management of administrative activities, which presumptivelywould have little effect on health outcomes such as in-hospital mortality rates. Or, the production
Inputs: Quantity
PRODUCTION PROCESSES
Outputs: Quantity
Outputs: QualityInputs: Quality
Inputs: Prices Best-Practice
InefficiencyCosts
Figure 1. Hospital production function.
COST INEFFICIENCY AND HOSPITAL HEALTH OUTCOMES 835
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

processes may have joint effects on cost inefficiency and output quality. Improvements in informationtechnology, for instance, could well affect both cost inefficiency (e.g. reducing duplication ofdocumentation and reporting) and output quality (e.g. reducing medication errors).
How cost inefficiency influences hospital health outcomes thus is largely an empirical question. Ifproduction processes for the most part affect costs and output quality independently, we would expectno association between cost inefficiency and health outcomes. Or, if the production processes typicallyaffect costs and output quality jointly and similarly, we would expect a higher level of cost inefficiencyto be associated with worsened health outcomes. The final possibility that production processestypically affect costs and output quality jointly but inversely seems unlikely. While higher total cost mayresult in better outcomes, such as lower complications rates, it is hard to think of an example in which ahigher level of cost inefficiency would be associated with better health outcomes.
DATA, VARIABLES, AND METHODS
Data for the study come from three sources: Medicare Cost Reports from the Centers for Medicare andMedicaid (CMS), the American Hospital Association (AHA) Annual Survey, and Solucient, a privatehealth-care information company. The national data on hospital characteristics and costs from CMSand AHA are widely used. (The CMS data files were read using SAS programs created by Jean Roth atthe NBER and available at http://www.nber.org/data/hcris.html.) Solucient, our source for outcomesdata, has supplied similar data to other researchers. For example, Griffith et al. (2006) used dataprovided by Solucient to examine trends in general performance measures such as risk-adjustedmortality and expense per adjusted discharge for hospitals over the period 1999–2003.
For comparability with our previous study using data from only one state, data in this national studyare for 1999–2001. For each year, the data set includes only short-term, acute-care hospitals that were inoperation for the full year, and excludes observations with obviously incorrect values (e.g. total costs of$106). Also excluded are hospitals with fewer than 16 beds or fewer than 100 discharges, due topotential small-number problems with the observed mortality rate and the case-mix index. All variablesexpressed in dollars were adjusted to constant 2000 dollar values using the gross domestic productimplicit price deflator. The final data set contains 3384 observations in 1999, 3343 observations in 2000,and 3183 observations in 2001, for a total of 9910 across the three years.
Hospital health outcomes
The specification for the health outcomes regressions is
OUTCOMEi ¼ aþ b1IEi þ b2jSEVERITYi;j þ b3kQUALITYi;k
þ b4lVOLUMEi;l þ b5mOTHERi;m þ ei ð1Þ
where i is the hospital and e is the usual normally distributed random error.Hospital health outcomes can be measured in a variety of ways. At the hospital level, examples
include in-hospital mortality rates, 30-day post-admission mortality rates, complication rates, failure torescue rates, post-surgical adverse events, and infection rates (Encinosa and Bernard, 2005; Kovneret al., 2002; Mukamel et al., 2001; Seshamani et al., 2006; Thornlow and Stukenborg, 2006). Anotherapproach is to measure health outcomes such as mortality rates or complication rates for specific typesof procedures or diagnoses (Birkmeyer et al., 2002; Needleman et al., 2002).
Because the primary objective of this study is to examine the effect of cost inefficiency on healthoutcomes and because cost inefficiency is measured for the hospital as a whole, measures of healthoutcomes are also at the hospital level. Hospital-level outcomes are fundamental and summary
N. L. MCKAY AND M. E. DEILY836
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

measures of the overall effect that hospitals have on patients’ health status, although they could obscuredifferences in health outcomes for specific procedures or diagnoses.
The dependent variables are the observed mortality rate (observed in-hospital deaths/totaladmissions) and the observed complications rate (observed complications/total admissions), wherethe complications rate measures the incidence of 48 negative clinical events such as post-operativeinfection, post-operative hemorrhage, or nosocomial pneumonia. The dependent variable in somestudies has been excess mortality or excess complications, i.e. observed rate – risk-adjusted expected rate(Hartz et al., 1993; Keeler et al., 1992). This study uses the approach in which the observed rate is thedependent variable and the risk-adjusted expected rate is an independent variable (Manheim et al.,1992; Mukamel et al., 2001) in order to isolate effects on observed deaths or complications, holdingother factors, including patient-risk factors, constant. For example, if excess mortality were thedependent variable, then parameter estimates would show how this difference, which depends onboth actual and expected mortality, changed with changes in an independent variable. In contrast, theresults of this study measure the effect of an independent variable on actual mortality, all else equal. Asshown in Table I for the pooled sample, the mean observed mortality rate was 3.8% (range of 3.7–4%over the three years) and the mean observed complications rate was 2.4% (2.3–2.5% over thethree years).
The independent variable of primary interest is the cost inefficiency score, discussed in detail below.As explained in the Conceptual Framework section, the expected coefficient of this variable is eitherzero (if cost inefficiency has no impact on health outcomes) or positive (if higher cost inefficiency isassociated with poorer health outcomes).
Other factors influencing hospital health outcomes can be categorized as controlling for severity,quality, volume, or other hospital characteristics (see Table I for descriptive statistics). For severity, theexpected mortality rate (expected deaths/total admissions) and the expected complications rate(expected complications/total admissions) are key control variables in the respective regressions. Foreach hospital, Solucient provided risk-adjusted expected deaths and complications. Solucient collectsdata on short-term, general, non-federal US hospitals from Medicare reports and billing files, thenadjusts the data for risk, using logistic regression models based on published, peer-reviewedmethodologies; their inpatient database contains discharge summary data on almost 20 millioninpatients each year. Specifically, expected deaths for each ICD-9-CM principal diagnosis are adjustedfor patient age, sex, procedures, and comorbidities; facility location, size, and teaching status; andurban/rural. Expected complications are adjusted for risk using a model similar to that used formortality. The coefficients of these variables are expected to be positive, because the observed mortalityrate and the observed complications rate should increase as the respective predicted rates increase, otherfactors held constant.
Other variables included to control for patient severity are intensive-care days as a percentage of totaldays, emergency visits as a percentage of total outpatient visits, and percentage of total outpatient visitsthat are surgeries (Manheim et al., 1992; Mukamel et al., 2001). The expectation is that observedmortality and complications would increase as patient severity increases, holding other factors constant.
Variables included to control for differences in input quality are accreditation by the JointCommission on Accreditation of Health Organizations (JCAHO), membership in the Council ofTeaching Hospitals (COTH), percentage of total full-time equivalent nurses who are registered nurses,presence of an open-heart program, presence of a transplant program, and the number of the followingradiological services that are offered – radiation therapy, computed-tomography, diagnostic radio-isotope, magnetic resonance imaging, positron emission tomography, single photon emissioncomputerized tomography, and ultrasound (Keeler et al., 1992; Kovner et al., 2002; Manheim et al.,1992; Mark et al., 2004; Mukamel et al., 2001; Needleman et al., 2002). Coefficients of these variablesare expected to be negative; higher quality would be expected to be associated with lower observedmortality and complications.
COST INEFFICIENCY AND HOSPITAL HEALTH OUTCOMES 837
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

A number of studies have found that increased volume is associated with better hospital healthoutcomes (see review in Dudley et al., 2000). To control for volume effects, the regressions include totaladmissions, with the expectation that a higher volume would be associated with lower observedmortality and complications. Although the data set does not include information about the volume ofspecific procedures, a recent study by Birkmeyer et al. (2002) found that total hospital volume wassignificantly related to operative mortality for six types of cardiovascular procedures and eight types ofmajor cancer resections.
Finally, other hospital characteristics may affect health outcomes. Control variables for hospitalcharacteristics are urban location and ownership, as well as dummy variables to control for regionaldifferences in outcomes (Keeler et al., 1992; Manheim et al., 1992; Mukamel et al., 2001; Needlemanet al., 2002).
Measuring hospital cost inefficiency
Cost inefficiency in the outcomes regressions is measured using the stochastic frontier approach, whichassumes that a hospital’s cost function is affected both by stochastic factors, over which the hospital has
Table I. Descriptive statistics: pooled sample ðn ¼ 9910Þ
Mean Std. dev
Dependent variableOBSMORTR (observed mortality rate) 0.038 0.024OBSCOMPR (observed complications rate) 0.024 0.018
Inefficiency scorea
IE-Baseline (inefficiency score from baseline cost function) 0.151 0.062IE-IV (inefficiency score from instrumented cost function) 0.260 0.112
Control variablesEXPMORTR (risk-adjusted, expected mortality rate) 0.040 0.027EXPCOMPR (risk-adjusted expected complications rate) 0.023 0.015ICPCT (intensive-care inpatient days/total inpatient days) 0.088 0.062ER (emergency-room visits/total outpatient visits) 0.276 0.174OUTSURG (outpatient surgeries/total outpatient visits) 0.040 0.045JCAHO (1 ¼ accredited by JCAHO, 0 ¼ not) 0.826 0.379COTH (1 ¼ member of Council of Teaching Hospitals, 0 ¼ not) 0.068 0.252RNPCT (FTE registered nurses/total FTE nurses) 0.826 0.135OHEART (1 ¼ presence of open-heart surgery, 0 ¼ not) 0.241 0.428TRANSP (1 ¼ presence of transplant program, 0 ¼ not) 0.054 0.226RADb (number of radiological services, 0–7) 3.97 1.64TOTADM (total admissions) 7298 8226NFP (1 ¼ not-for-profit ownership, 0 ¼ not) 0.644 0.479FP (1 ¼ for-profit ownership, 0 ¼ not) 0.120 0.325GOVT (1 ¼ government ownership, 0 ¼ not) 0.236 0.425URBAN (1 ¼ urban location, 0 ¼ not) 0.564 0.496RURAL (1 ¼ rural location, 0 ¼ not) 0.436 0.496NEWE (1 ¼ New England region, 0 ¼ not) 0.045 0.208MIDATL (1 ¼Mid-Atlantic region, 0 ¼ not) 0.105 0.306STHATL (1 ¼ South Atlantic region, 0 ¼ not) 0.149 0.356ENC (1 ¼ East North Central region, 0 ¼ not) 0.171 0.376ESC (1 ¼ East South Central region, 0 ¼ not) 0.090 0.286WNC (1 ¼West North Central region, 0 ¼ not) 0.134 0.341WSC (1 ¼West South Central region, 0 ¼ not) 0.148 0.355MOUNT (1 ¼Mountain region, 0 ¼ not) 0.060 0.238PAC (1 ¼ Pacific region, 0 ¼ not) 0.098 0.298
aFrom stochastic cost function results.bNumber of following radiological services offered: radiation therapy, computed-tomography, diagnostic radioisotope, magneticresonance imaging, positron emission tomography, single photon emission computerized tomography, ultrasound.
N. L. MCKAY AND M. E. DEILY838
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

no control, and by errors in the hospital’s choices that lead to inefficiency. The cost function thusincludes two error terms – one to measure random error and one to measure inefficiency.
The cost function estimated in this study is a hybrid functional form that incorporates features ofboth the structural translog cost function (based on standard economic theory) and an ad hoc costfunction that includes regressors other than output and input prices found to have an importantinfluence on hospital costs (Grannemann et al., 1986; Zuckerman et al., 1994). The general specificationof the cost function is
ln TOTALCOST ¼ aþXi
bi ln OUTPUTi þ1
2
Xij
bijðln OUTPUTiÞðln OUTPUTjÞ
þXk
ck ln INPUTPRICEk þ1
2
Xkl
dklðln INPUTPRICEkÞðln INPUTPRICElÞ
þXik
eikðln OUTPUTiÞðln INPUTPRICEkÞ þXm
fmOTHERFACTORSm þ mþ n
ð2Þ
where n is the usual normally distributed random error and m is the inefficiency residual, which isassumed to have the half-normal distribution (Vitaliano and Toren, 1994). The Appendix provides adetailed discussion of the cost inefficiency scores, including variables used in the cost estimations, thefinal specification of the cost function, econometric issues, and the formula for calculating theinefficiency residuals.
Hausman tests rejected the null hypothesis of exogeneity for the prices of capital and labor and forboth outputs in the cost function. Consequently, instrumented variables were created for the price oflabor, the price of capital, total admissions, and total outpatient visits. Because the explanatory powerof the instruments was weak and the use of poor instruments can be problematic (Bartels, 1991; Boundet al., 1995), we estimate and use in the outcomes regressions two sets of cost inefficiency scores – oneusing the actual values for all variables (Baseline) and the other using instrumented values for totaladmissions, total outpatient visits, the price of labor, and the price of capital (IV).
The stochastic frontier approach yields a cost inefficiency score (IE) for each hospital in each year.The mean inefficiency scores calculated from the baseline cost function were 0.142 in 1999, 0.164 in2000, and 0.148 in 2001 (0.151 for the pooled sample, as shown in Table I). Thus, on average hospitalsin the data set had actual costs that were approximately 14–16% higher than the frontier, or best-practice, level; these estimates are comparable with those from previous studies (Chirikos, 1998/1999;McKay et al., 2002/2003; Rosko, 2001; Zuckerman et al., 1994). The IV cost function, however, yieldedconsiderably different results, with mean cost inefficiency being 0.258 in 1999, 0.273 in 2000, and 0.250in 2001 (0.260 for the pooled sample).
Sensitivity of hospital inefficiency scores
One criticism of the stochastic frontier approach is that it requires strong assumptions about theinefficiency error structure (Skinner, 1994). To investigate the effects of using an error structure otherthan half-normal, the cost functions were re-estimated for exponential and truncated (at zero) normaldistributions for the inefficiency residuals. Cost inefficiency residuals based on the exponentialdistribution were highly correlated with residuals based on the half-normal distribution (0.96–0.97across the three years for both the baseline and IV cost functions). There was also a high correlationbetween inefficiency residuals based on the half-normal and truncated normal distributions (0.99 in eachof the three years for both the baseline and IV cost functions). Consequently, we report results onlyassuming the half-normal distribution for the inefficiency residuals.
COST INEFFICIENCY AND HOSPITAL HEALTH OUTCOMES 839
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

Another concern is that the inefficiency residuals could be picking up cost differences among hospitalsthat reflect higher costs due to higher quality care, and some studies have included variables related tohospitals’ health outcomes (e.g. excess mortality) in the cost function. Because the objective of this studyis to examine the association between cost inefficiency and health outcomes, the estimated inefficiencyscores do not hold risk-adjusted mortality and risk-adjusted complications constant. However, as arobustness check, both the baseline and IV cost functions were re-estimated including excess mortalityand excess complications as regressors. The resulting inefficiency scores were highly correlated with thereported inefficiency scores (0.99 for each of the three years for both the baseline and IV cost functions),indicating that excluding these variables from the cost function had little effect on the rankings byinefficiency score among hospitals in the sample.
RESULTS
Tables II and III present the regression results for mortality rates and complication rates, respectively.In each table, the first column reports results using inefficiency scores calculated from the baseline costfunction (IE-Baseline), while in the second column inefficiency scores were calculated from the costfunction estimated with instrumental variables (IE-IV). Other than having different IE variables, thedata for the outcomes regressions and the estimation methods were identical, with the outcomesequations being estimated using ordinary least squares (OLS) with White’s correction forheteroskedasticity. Finally, because the hospital inefficiency measures used in the outcomes equations
Table II. Results: mortality rate regressions (dependent variable is observed mortality rate, n ¼ 9910)
Parameter estimates(bootstrapped standard errors in parentheses)
IE scores from IE scores fromVariable baseline cost Fn IV cost Fn
Constant 0.006 (0.001)nn 0.007 (0.001)nn
IE (cost inefficiency score) 0.005 (0.002)n �0.00002 (0.001)Year ¼ 2000 �0.001 (0.0003)nn �0.001 (0.0003)nn
Year ¼ 2001 �0.001 (0.0003)nn �0.001 (0.0003)nn
EXPMORTR (expected mortality rate) 0.752 (0.015)nn 0.753 (0.015)nn
ICPCT (% intensive-care inpatient days) �0.004 (0.002) �0.004 (0.002)ER (% outpatient visits to ER) 0.003 (0.001)nn 0.003 (0.0008)nn
OUTSURG (surgeries per outpatient visit) �0.006 (0.003)n �0.006 (0.003)n
JCAHO (accreditation by JCAHO) 0.001 (0.0005) 0.001 (0.0005)COTH (teaching hospital) �0.003 (0.0003)nn �0.003 (0.0003)nn
RNPCT (% RN nurses) �0.005 (0.001)nn �0.005 (0.001)nn
OHEART (does open-heart surgery) 0.001 (0.0003)nn 0.001 (0.0003)nn
TRANSP (has transplant program) �0.0003 (0.0004) �0.0003 (0.0004)RAD (index of radiological services, 0–7) 0.0004 (0.0001)nn 0.0004 (0.0001)nn
TOTADM (total admissions) �0:14E� 6 (0:17E� 7)nn �0:14E� 6 (0:22E� 7)nn
FP (for-profit ownership) �0.003 (0.0004)nn �0.003 (0.0004)nn
GOVT (government ownership) 0.002 (0.0003)nn 0.002 (0.0003)nn
URBAN (in urban area) �0.0006 (0.0003) �0.0006 (0.0003)NEWE (New England region) 0.006 (0.0005)nn 0.006 (0.0005)nn
MIDATL (Mid-Atlantic region) 0.010 (0.0004)nn 0.010 (0.0004)nn
STHATL (South Atlantic region) 0.005 (0.0004)nn 0.005 (0.0004)nn
ENC (East North Central region) 0.004 (0.0003)nn 0.004 (0.0004)nn
ESC (East South Central region) 0.010 (0.0006)nn 0.010 (0.0006)nn
WNC (West North Central region) 0.002 (0.0005)nn 0.002 (0.0005)nn
WSC (West South Central region) 0.004 (0.0004)nn 0.004 (0.0004)nn
MOUNT (Mountain region) �0.001 (0.0004)n �0.001 (0.0004)
n0:015p40:05:nnp40:01:
N. L. MCKAY AND M. E. DEILY840
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

are estimates, rather than the true, but unknown, variable, the usual standard errors may understate thetrue variance. Therefore, the standard errors presented in Tables II and III result from bootstrappingeach outcomes equation.
An F test comparing separate regressions by year against a pooled regression with dummy variablesfor year rejected the null hypothesis that the slope coefficients were the same across the years (F ¼ 2:44for mortality regression with IE-baseline, F ¼ 2:46 for mortality regression with IE-IV, F ¼ 2:34 forcomplications regression with IE-baseline, and F ¼ 2:38 for complications regression with IE-IV; the Fstatistic with degrees of freedom (239 884) is approximately 1.88 at the 0.01 confidence level).Nevertheless, the results reported in Tables II and III are from the pooled regressions with dummyvariables for year, for conciseness and because general conclusions about the control variables based onthe pooled regressions are virtually the same as those based on separate regressions by year.
Cost inefficiency scores
As shown in Table II, cost inefficiency had a positive coefficient and was statistically significant at the0.05 confidence level for the IE-Baseline scores, but for the IE-IV scores, the coefficient was negativeand not statistically significant. Moreover, the cost inefficiency parameter was not statisticallysignificant in any of the separate regressions by year using either the IE-Baseline scores or the IE-IVscores (results not shown). Thus, for the most part, cost inefficiency was not significantly associated withhospital mortality rates.
Table III. Results: complications rate regressions (dependent variable is observed complications rate, n ¼ 9910)
Parameter estimates(bootstrapped standard errors in parentheses)
IE scores from IE scores fromVariable baseline cost Fn IV cost Fn
Constant �0.005 (0.001)nn �0.005 (0.001)nn
IE (cost inefficiency score) 0.001 (0.001) �0.0008 (0.0009)Year ¼ 2000 �0.0002 (0.0002) �0.0002 (0.0002)Year ¼ 2001 �0.0004 (0.0002)n �0.0004 (0.0002)n
EXPCOMPR (expected complications rate) 1.03 (0.03)nn 1.03 (0.03)nn
ICPCT (% intensive-care inpatient days) 0.004 (0.002)n 0.004 (0.002)n
ER (% outpatient visits to ER) 0.001 (0.0005) 0.001 (0.0005)OUTSURG (surgeries per outpatient visit) �0.003 (0.002) �0.003 (0.002)JCAHO (accreditation by JCAHO) 0.0005 (0.0003) 0.0005 (0.0003)COTH (teaching hospital) 0.002 (0.0004)nn 0.002 (0.0004)nn
RNPCT (% RN nurses) 0.004 (0.0008)nn 0.004 (0.0008)nn
OHEART (does open-heart surgery) 0.001 (0.0004)n 0.001 (0.0004)n
TRANSP (has transplant program) 0.002 (0.0004)nn 0.002 (0.0004)nn
RAD (index of radiological services, 0–7) 0.0002 (0.0001)n 0.0002 (0.0001)n
TOTADM (total admissions) 0:24E� 7 (0:17E� 7) 0:35E� 7 (0:19E� 7)FP (for-profit ownership) �0.001 (0.0002)nn �0.001 (0.0002)nn
GOVT (government ownership) 0.0002 (0.0002) 0.0002 (0.0002)URBAN (in urban area) 0.0007 (0.0002)nn 0.0007 (0.0002)nn
NEWE (New England region) 0.0003 (0.0005) 0.0003 (0.0005)MIDATL (Mid-Atlantic region) �0.001 (0.0004)nn �0.001 (0.0004)nn
STHATL (South Atlantic region) �0.0007 (0.0004) �0.0007 (0.0004)ENC (East North Central region) �0.001 (0.0003)nn �0.001 (0.0004)nn
ESC (East South Central region) �0.001 (0.0003)nn �0.001 (0.0003)nn
WNC (West North Central region) 0.0003 (0.0004) 0.0003 (0.0004)WSC (West South Central region) �0.002 (0.0003)nn �0.002 (0.0003)nn
MOUNT (Mountain region) 0.003 (0.0005)nn 0.003 (0.0005)nn
n0:015p40:05:nnp40:01:
COST INEFFICIENCY AND HOSPITAL HEALTH OUTCOMES 841
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

For health outcomes measured by complications rates (see Table III), the coefficient of the costinefficiency score was not statistically significant for either IE-Baseline or IE-IV scores in either thepooled or separate regressions by year. The results thus strongly suggest a lack of association betweencost inefficiency and hospital complication rates.
As a sensitivity test for the outcomes results, we re-estimated the cost functions using OLS and thenused the residuals from the OLS estimations in the outcome regressions; the OLS residuals thus includethe effect of all unexplained factors on hospital costs, whether from inefficiency or white noise. Thepattern of results was highly similar to the results reported above, suggesting that the lack of associationbetween cost inefficiency and health outcomes was not due to the use of the stochastic frontier approachto estimate cost inefficiency.
The data set is an unbalanced panel across the three years, with some hospitals appearing in only oneor two of the three years. A total of 2663 hospitals appeared in all three years, accounting for slightlyover 80% of all observations in the pooled sample. As another sensitivity test, we re-estimated the costfunctions and then the outcomes regressions for the sample of hospitals appearing in all three years(pooled n ¼ 7989). Results using the balanced sample were substantively the same as the reportedresults, indicating that changes in the sample composition across the years did not affect the studyresults.
Control variables: mortality rate regressions
In the mortality rate regression results shown in Table II, the expected mortality rate (EXPMORTR)had a positive, large, and statistically significant effect on observed mortality. Thus, as would beexpected, a hospital’s observed mortality rate depends primarily on patient risk and severity factors.The percentage of ER outpatient visits (ER) also had a positive and statistically significant, but modest,effect on observed mortality, suggesting that the variable captured some additional aspects of patientrisk and severity. Other variables having a positive and statistically significant effect were the presenceof an open-heart program (OHEART) and the number of radiological services (RAD). Variables thatwere negatively and significantly associated with the observed mortality rate included the percentage ofRN nurses (RNPCT), being a teaching hospital (COTH), and more outpatient surgeries per outpatientvisit (OUTSURG).
Other interesting results relate to volume and ownership status. Total admissions (TOTADM) had anegative and statistically significant effect, indicating that observed mortality rates were lower forhospitals with more admissions, other factors held constant; however, the magnitude of the effect wasquite small. Results for ownership exhibited a strong and consistent pattern with for-profit hospitals(FP) having lower mortality rates and government hospitals (GOVT) having higher mortality rates thanotherwise comparable not-for-profit hospitals. Finally, there were strong regional differences inmortality rates.
Control variables: complications rate regressions
For complications, the expected complications rate (EXPCOMPR) had the expected positive, large, andstatistically significant effect on observed complications, as shown in Table III. Other variables having apositive and statistically significant effect were the percentage of intensive-care days (ICPCT), thepresence of an open program (OHEART), presence of a transplant program (TRANSP), and thenumber of radiological services (RAD). Interestingly, two other variables that were positively andsignificantly associated with the observed complications rate – the percentage of RN nurses (RNPCT)and being a teaching hospital (COTH) – had a negative and significant association with the observedmortality rate. This is unexpected, particularly for the percentage of RN nurses, because it indicates thata higher percentage of RN nurses was associated with a higher level of output quality measured in termsof mortality rates but a lower level when output quality was measured by complications rates.
N. L. MCKAY AND M. E. DEILY842
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

Another interesting finding is that volume (TOTADM) did not have a statistically significant effect inthe complications regressions, in contrast to its negative association with observed mortality. And for-profit hospitals (FP) had lower complications rates than not-for-profit hospitals, which is consistentwith the mortality results, but the coefficient for government ownership (GOVT) was not statisticallysignificant in the complications regressions. The coefficient for urban location (URBAN) was positiveand statistically significant for complications rates, and regional patterns for complications ratesdiffered in several cases from those for mortality rates.
Comparison to previous findings for Florida
The findings of this study for mortality rates differ from results in our previous study using data forurban, Florida hospitals (Deily and McKay, 2006), in which there was a positive and statisticallysignificant relationship between a hospital’s inefficiency score and its observed mortality rate, otherfactors held constant. Although the previous study covered the same years, it used a different datasource, a different risk-adjustment methodology, somewhat different control variables, and includedonly urban hospitals. Therefore, an important question is whether the differing results stem primarilyfrom variations in the data source and risk-adjustment methodology or from differences betweenFlorida hospitals and hospitals in the US as a whole.
To investigate this question, we re-estimated the mortality rate regressions for urban hospitals inFlorida (90 observations in 1999, 109 observations in 2000, and 89 in 2001, for a total of 288 across thethree years), using a pooled regression with dummy variables for year for comparability. The results aresimilar to the previous study, in which the coefficient of IE was 0.013 (p50:01). In this study, using onlyurban hospitals in Florida and inefficiency scores from the baseline cost function, the coefficient of IEwas 0:011 ðp ¼ 0:02Þ; for the IV cost function, the coefficient of IE was 0.014 ðp50:0000Þ: This suggeststhat the relationship between cost inefficiency and mortality may differ across geographical regions, apoint discussed further in the next section.
SUMMARY AND DISCUSSION
The results of this study showed no systematic pattern of association between cost inefficiency andhospital health outcomes, as measured by mortality and complications rates, in a sample of acute-carehospitals in the US over the period 1999–2001. The basic results were unchanged regardless of whethercost inefficiency was measured using the stochastic frontier approach (with or without instrumentalvariables) or by using residuals from an OLS cost function.
Other than this study and a previous study based on Florida hospitals (Deily and McKay, 2006), weare not aware of other empirical studies examining the relationship between cost inefficiency andhospital health outcomes. The differing findings in the two studies thus were of concern – that is, theprevious study found a positive and statistically significant relationship between a hospital’s inefficiencyscore and its observed mortality rate, other factors held constant. However, we found results similar tothose of the previous study when we estimated our mortality equation using data from the current studyfor urban Florida hospitals alone.
The contrasting findings between the US and Florida studies, and the consistently significant regionaleffects in the mortality regressions, suggest the possibility of a relationship between cost inefficiency andmortality that may differ systematically across geographical regions, a topic we plan to explore in futurestudies. Although US and Florida hospitals differ across a variety of hospital characteristics, aparticularly striking difference is the profile of ownership. Specifically, 12.0% of US hospitals in oursample were for-profit (see Table I), with the corresponding value for Florida hospitals in the previousstudy being 39.9%; 64.4% of US and 43.8% of Florida hospitals were not-for-profit, respectively, withgovernment hospitals accounted for 23.6% of US and 16.3% of Florida hospitals, respectively.
COST INEFFICIENCY AND HOSPITAL HEALTH OUTCOMES 843
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

Although further study is clearly needed, these substantially different ownership patterns are certainlyintriguing, especially given the considerable variation in ownership across states and regions in the US.
Finally, although not the focus of our study, a comparison of the estimated coefficients for thecontrol variables in Tables II and III shows rather different patterns for mortality and complications.As mentioned in the Results section, of particular interest is the fact that both the percentage of RNnurses (RNPCT) and teaching status (COTH) were negatively and significantly associated withmortality, but positively and significantly associated with complications. A possible explanation is thatrisk adjustment may be incomplete for complications, given that the complications rate measures theincidence of 48 separate clinical events, rather than a single event as is the case for the mortality rate. Ifsome components of patient severity are not fully incorporated in the risk-adjusted complications rate,RNPCT and COTH could be reflecting additional aspects of patient severity, rather than input quality,which would explain the positive association with complications.
Limitations
A limitation of this study is that it measures health outcomes at the hospital level, which might obscuredifferences in outcomes across medical conditions. However, the measure we have of cost inefficiency isat the hospital level; little cost data for individual medical conditions are available, particularly for anational sample of hospitals. In addition, hospital-level outcomes provide important summaryinformation on the overall effect that hospitals have on patients’ health status.
When examining health outcomes such as mortality or complications, controlling for patient-riskfactors is a major concern. The most important variables included in this study to control for patient-risk factors are expected mortality and expected complications rates, which are aggregated measuresbased on patient-level data. Although any risk adjustment method will have some drawbacks, hospitalsthroughout the country routinely purchase Solucient’s risk-adjusted data, suggesting that their methodsof risk adjustment are widely accepted methods of controlling for patient severity and case mix.Additional variables to control for patient-risk factors, measured at the hospital level, includedintensive-care days as a percentage of total days, emergency visits as a percentage of total outpatientvisits, and percentage of total outpatient visits that are surgeries. However, as noted above, the riskadjustment may be more complete for mortality than for complications.
Another limitation relates to the use of a stochastic frontier approach to estimate cost inefficiency.Criticisms of the stochastic frontier method have centered on the instability of hospital rankings acrossspecifications of the cost function (Chirikos, 1998; Street, 2003) and the difficulty of controlling forquality (Newhouse, 1994). However, other studies have concluded that the stochastic frontier approachis an improvement over OLS or the DEA methods of measuring cost inefficiency (Wagstaff, 1989) andthat, in comparing various specifications for the stochastic method, group mean inefficiencies wererobust to the variations (Folland and Hofler, 2001). It is important to emphasize, therefore, that thisstudy focuses on patterns that characterize hospitals as a group, rather than the rankings of individualhospitals.
Policy implications
In the conceptual framework, the link between cost inefficiency and health outcomes depended on thenature of the production processes in the hospital and the extent to which they affect inefficiency andoutcomes independently. The results of this study thus suggest that hospital production processes forthe most part affect costs and output quality independently.
A key policy implication for hospitals is that efforts to reduce cost inefficiency are unlikely to beassociated with worsened hospital-level mortality or complications rates. Cost containment programsthat focus on eliminating primarily wasteful costs, rather than simply reducing costs, thus would not beexpected to have adverse consequences for patient health outcomes.
N. L. MCKAY AND M. E. DEILY844
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

On the other hand, across-the-board cost reductions could well have adverse effects on healthoutcomes, because a certain level of cost is necessary for hospitals to provide safe, effective, high-qualitycare. This study thus highlights the importance for both health-care managers and policymakers ofdistinguishing between ‘good’ costs that reflect the efficient use of resources and ‘bad’ costs that stemfrom waste and other forms of inefficiency.
Programs to reduce inefficient hospital costs have the potential for considerable cost savings.Hospital expenditures in 2004 were $570.8 billion, accounting for approximately 30% of national healthexpenditures (Smith et al., 2006). Although hospitals clearly must maintain a certain level of excesscapacity due to the uncertain nature of demand and although mean estimates of cost inefficiency varyby cost specification, reducing hospital costs that are inefficient by 5%, which would seem a reasonabletarget, would result in savings of approximately $28.5 billion. Moreover, the results of this study suggestthat these savings, if targeted toward eliminating inefficiency, could be accomplished without adverseeffects on mortality or complications.
For the health system as a whole, the major policy implication is that proposed reimbursement andregulatory changes should be aimed primarily at reducing cost inefficiency, rather than focusing on costcontainment per se. Although this may seem an obvious suggestion, the distinction between efficient andinefficient costs has received relatively little attention from health policymakers. Changes in regulatorypolicy, for example, could result in considerable improvement in cost inefficiency. Hospitals are subjectto a bewildering array of sometimes conflicting regulations imposed by government at all levels – local,state, and federal. Policy changes that reduce duplication and streamline these regulations could resultin substantial and far-reaching reductions in cost inefficiency. Another possibility in the policy arenawould be to include cost efficiency objectives in the current move toward pay-for-performance methodsof reimbursement.
Research on the relationship between cost inefficiency and hospital health outcomes is still in itsinfancy. Additional studies are needed to see whether these results are consistent for other time periods,other data sets, and other measures of health outcomes. Of particular interest are the apparent regionaldifferences in cost inefficiency and outcomes. If, for example, certain regions systematically demonstratea pattern of better performance, holding other factors such as patient-risk factors and ownershipconstant, it might be possible to develop benchmarking guidelines that would assist other hospitals inimproving both cost and outcomes.
APPENDIX
Cost inefficiency is measured using the stochastic frontier approach to estimate a hybrid cost function,as explained in the text. Data for the cost function came from Medicare Cost Reports, obtained fromthe Centers for Medicare and Medicaid (CMS), and the American Hospital Association (AHA) AnnualSurvey.
The dependent variable is total hospital cost, calculated as the sum of total salaries, total capital-related costs, and total other costs from the Medicare Cost Report. Outputs include total admissionsand total outpatient visits, and input prices include the price of personnel (average annual salary perfull-time equivalent employee), the price of capital (capital-related costs per bed), and the price ofsupport services (other costs per bed). A variable indicating hospitals of less than 100 beds is included tocapture potential differences in production processes for smaller hospitals.
Other variables influencing hospital cost can be generally classified as controlling for patient-related risk factors or quality. Variables to control for patient-risk factors, such as case mix andseverity, include the Medicare case-mix index, intensive-care days as a percentage of total days,emergency visits as a percentage of total outpatient visits, and percentage of total outpatient visits thatare surgeries.
COST INEFFICIENCY AND HOSPITAL HEALTH OUTCOMES 845
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

A number of quality-related variables are included to control for variation in the depth and breadthof available hospital services, hospitals’ technological sophistication, and the training of their personal.These variables are accreditation by the Joint Commission on Accreditation of Health CareOrganizations (JCAHO), membership in the Council of Teaching Hospitals (COTH), percentage oftotal full-time equivalent nurses who are registered nurses, presence of an open-heart program, presenceof a transplant program, presence of a cancer program approved by the American College of Surgeons,and the number of the number of radiological services offered.
Estimation of a standard cost function assumes that input prices are exogenous to the firm. However,input prices in this case could be endogenous if they reflect, for example, the mix of different types oflabor chosen by the hospital. Hausman tests rejected the null hypothesis of exogeneity for the prices oflabor and capital. (Because the translog restrictions involve dividing through by one of the input prices,in this case the price of support services, that price drops out.) Consequently, instrumented variableswere created for the price of labor and the price of capital each year using variables assumed to beexogeneous to hospitals (county population, county per capita income, county unemployment rate, anddummy variables for urban location, state, year, and ownership). The explanatory power of theinstruments was somewhat disappointing, with an adjusted R2 across the three years of 0.35–0.38 forprice of labor and 0.23–0.25 for price of capital.
Cost function estimation also assumes that the firm’s outputs are exogenously determined. Hausmantests rejected the null hypothesis of exogeneity for both outputs, and as a consequence instrumentedvariables also were created for total admissions and total outpatient visits, using the exogenousvariables listed above. Again, the explanatory power of the instruments was rather low, with an adjustedR2 across the three years of 0.50–0.51 for total admissions and 0.42–0.44 for total outpatient visits.
Because the use of poor instruments can lead to worse results than accepting the bias due toendogeneity (Bartels, 1991; Bound et al., 1995), we estimate and present two sets of cost inefficiencyscores – one using the actual values for all variables (Baseline) and the other using instrumented valuesfor total admissions, total outpatient visits, the price of labor, and the price of capital (IV).
After imposing the usual restrictions necessary to ensure symmetry and homogeneity in input prices,we estimated the cost functions using the frontier regression routine in LIMDEP (full results for the costfunction estimations are available upon request). A likelihood ratio test at the 0.01 confidence levelrejected the null hypothesis that the slope coefficients in the cost functions were the same across thethree years. Consequently, the cost functions were estimated separately for each year. The full translogspecification of the cost function is used throughout, because likelihood ratio tests rejected the nullhypothesis that the second-order terms in the cost function were jointly equal to zero.
We chose not to use panel data methods in estimating the cost function. First, as noted above,pooling across the three years was rejected by a likelihood ratio test. Second, while panel data methodscan sidestep some of the shortcomings of stochastic frontier analysis (Kumbhakar and Lovell, 2000),standard panel methods such as fixed or random effects assume that a given hospital’s inefficiency isunchanged over time, which does not appear to be the case for this data set, and panel methods forallowing inefficiency to vary over time require a specification for the pattern of change (Jacobs et al.,2006). Finally, data in this study span only three years.
The residuals that we use as a measure of a hospital’s relative inefficiency in a given year are notestimated directly. Rather they are calculated using the coefficient estimates from the cost functions andthe two parameters l and s; the formula used to calculate the inefficiency residuals, as given in Jondrowet al. (1982), and adjusted for a cost function, is
Eðmi jmi þ viÞ ¼sl
1þ l2
f�eils
� �
1� F�eils
� �þ ðeiÞls
2664
3775
N. L. MCKAY AND M. E. DEILY846
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

where ei ¼ Yi � X 0b; l ¼ sm=sn;s ¼ ðs2m þ s2nÞ1=2;f is the density of the standard normal distribution
and F is the standard normal cumulative distribution function.
ACKNOWLEDGEMENTS
We gratefully acknowledge the data provided by Solucient, LLC, and the assistance of David A. Foster,Chief Scientist, Solucient. We also received valuable comments and suggestions from Michael D. Roskoand Larry W. Taylor. The Martindale Center for the Study of Private Enterprise and the College ofBusiness and Economics Research Fund, Lehigh University, provided financial support. Neither authorhas financial or personal relationships that might bias this study. No institutional ethical committeeapproval was necessary for this study.
REFERENCES
Bartels L. 1991. Instrumental and ‘quasi-instrumental’ variables. American Journal of Political Science 35: 777–800.Birkmeyer J, Siewers A, Finlayson E, Stukel T, Lucas F, Batista I, Welch H, Wennberg D. 2002. Hospital volume
and surgical mortality in the United States. New England Journal Medicine 346: 1128–1137.Bound J, Jaeger D, Baker R. 1995. Problems with instrumental variables estimation when the correlation between
the instruments and the endogenous explanatory variable is weak. Journal of the American Statistical Association90: 443–450.
Carey K, Burgess J. 1999. On measuring the hospital cost/quality trade-off. Health Economics 8: 509–520.Chirikos T. 1998/1999. Further evidence that hospital production is inefficient. Inquiry 35: 408–416.Chirikos T. 1998. Identifying efficiently and economically operated hospitals: the prospects and pitfalls of applying
frontier regression techniques. Journal of Health Politics Policy and Law 23: 879–904.Deily M, McKay N. 2006. Cost inefficiency and mortality rates in Florida hospitals. Health Economics 15: 419–431.Donabedian A. 1980. Explorations in Quality Assessment and Monitoring, Volume I: The Definition of Quality and
Approaches to its Assessment. Health Administration Press: Ann Arbor, MI.Dudley R, Johansen K, Brand R, Rennie D, Milstein A. 2000. Selective referral to high-volume hospitals. Journal of
the American Medical Association 283: 1159–1166.Encinosa W, Bernard D. 2005. Hospital finances and patient safety outcomes. Inquiry 42: 60–72.Fleming S. 1991. The relationship between quality and cost: pure and simple? Inquiry 28: 29–38.Folland S, Hofler R. 2001. How reliable are hospital efficiency estimates? Exploiting the dual to homothetic
production. Health Economics 10: 683–698.Grannemann T, Brown R, Pauly M. 1986. Estimating hospital costs: a multiple-output analysis. Journal of Health
Economics 5: 107–127.Griffith J, Alexander J, Foster D. 2006. Is anybody managing the store? National trends in hospital performance.
Journal of Healthcare Management 51: 392–405.Hartz A, Gottlieb M, Kuhn E, Rimm A. 1993. The relationship between adjusted hospital mortality and the results
of peer review. Health Services Research 27: 765–777.Jacobs J, Smith P, Street A. 2006. Measuring Efficiency in Health Care: Analytic Techniques and Health Policy.
Cambridge University Press: Cambridge.Jiang J, Friedman B, Begun J. 2006. Factors associated with high-quality/low-cost hospital performance. Journal of
Health Care Finance 32: 39–52.Jondrow J, Lovell K, Materov I, Schmidt P. 1982. On the estimation of technical inefficiency in the stochastic
frontier production function model. Journal of Economics 19: 233–238.Keeler E, Rubenstein L, Kahn K, Draper D, Harrison E, McGinty M, Rogers W, Brook R. 1992. Hospital
characteristics and quality of care. Journal of the American Medical Association 268: 1709–1714.Kovner C, Jones C, Zhan C, Gergen P, Basu J. 2002. Nurse staffing and postsurgical adverse events: an analysis of
administrative data from a sample of U.S. hospitals, 1990–1996. Health Services Research 37: 611–627.Kumbhakar S, Lovell C. 2000. Stochastic Frontier Analysis. Cambridge University Press: Cambridge, UK.Manheim L, Feinglass J, Shortell S, Hughes E. 1992. Regional variation in Medicare hospital mortality. Inquiry 29:
55–66.Mark B, Harless D, McCue M, Xu Y. 2004. A longitudinal examination of hospital registered nursing staffing and
quality of care. Health Services Research 39: 279–300.
COST INEFFICIENCY AND HOSPITAL HEALTH OUTCOMES 847
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec

McKay N, Deily M. 2005. Comparing high- and low-performing hospitals using risk-adjusted excess mortality andcost inefficiency. Health Care Management Review 30: 347–360.
McKay N, Deily M, Dorner F. 2002/2003. Ownership and changes in hospital inefficiency, 1986–1991. Inquiry 39:388–399.
Morey R, Fine D, Loree S, Retzlaff-Roberts D, Tsubakitani S. 1992. The trade-off between hospital cost andquality of care: an exploratory empirical analysis. Medical Care 30: 677–698.
Mukamel D, Zwanziger J, Tomaszewski K. 2001. HMO penetration, competition, and risk-adjusted hospitalmortality. Health Services Research 36: 1019–1035.
Needleman J, Buerhaus P, Mattke S, Stewart M. 2002. Nurse-staffing levels and the quality of care in hospitals.New England Journal of Medicine 346: 1715–1722.
Newhouse J. 1994. Frontier estimation: how useful a tool for health economics? Journal of Health Economics 13:317–322.
Rosko M. 2001. Cost efficiency of U.S. hospitals: a stochastic frontier approach. Health Economics 10: 539–551.Seshamani M, Schwartz J, Volpp K. 2006. The effect of cuts in Medicare reimbursement on hospital mortality.
Health Services Research 43: 683–700.Skinner J. 1994. What do stochastic frontier cost functions tell us about inefficiency? Journal of Health Economics
13: 323–328.Smith C, Cowan C, Heffler S, Catlin A, National Health Accounts Teams. 2006. National health spending in 2004:
recent slowdown led by prescription drug spending. Health Affairs 25: 186–196.Street A. 2003. How much confidence should we place in efficiency estimates? Health Economics 12: 895–907.Thornlow D, Stukenborg G. 2006. The association between hospital characteristics and rates of preventable
complications and adverse events. Medical Care 44: 265–269.Vitaliano D, Toren M. 1994. Frontier analysis: a reply to Skinner, Dor and Newhouse. Journal of Health Economics
13: 341–343.Wagstaff A. 1989. Estimating efficiency in the hospital sector: a comparison of three statistical cost frontier models.
Applied Economics 21: 659–672.Zuckerman S, Hadley J, Iezzoni I. 1994. Measuring hospital efficiency with frontier cost functions. Journal of
Health Economics 13: 255–280.
N. L. MCKAY AND M. E. DEILY848
Copyright # 2007 John Wiley & Sons, Ltd. Health Econ. 17: 833–848 (2008)
DOI: 10.1002/hec