Embed Size (px)
Citation preview

Research Article
Cost Comparison of FemoralDistraction Osteogenesis WithExternal Lengthening Over a NailVersus Internal MagneticLengthening Nail
Abstract
Introduction: Femoral lengthening is performed by distractionosteogenesis via lengthening over a nail (LON) or by using amagneticlengthening nail (MLN). MLN avoids the complications of externalfixation while providing accurate and easily controlled lengthening.However, the increased cost of implants has led many to questionwhether MLN is cost-effective compared with LON.Methods: A retrospective review was performed comparingconsecutive femoral lengthenings using either LON (n = 19) or MLN(n = 39). The number of surgical procedures, time to union, andamount of lengthening were compared. Cost analysis was performedusing both hospital and surgeon payments. Costs were adjusted forinflation using the Consumer Price Index.Results: No difference was observed in the length of femoraldistraction. Patients treated with MLN underwent fewer surgeries(3.1 versus 2.1; P , 0.001) and had a shorter time to union(136.7 versus 100.2 days; P = 0.001). Total costs were similar($50,255 versus $44,449; P = 0.482), although surgeon fees werelower for MLN ($4,324 versus $2,769; P , 0.001).Discussion: Although implants are more expensive for MLNthan LON, this appears to be offset by fewer procedures. Overall,the two procedures had similar total costs, but MLN wasassociated with a decreased number of procedures and shortertime to union.Level of Evidence: III
Lengthening of the femur has beenperformed by using distraction
osteogenesis via the lengthening over anail (LON) technique,1 involving theuse of a monorail external fixator tolengthen the femur over a femoralintramedullary nail. This techniqueresults in much less time in the exter-nal fixator and fewer complicationsthan the classic technique using theexternal fixator alone,2,3 but many
drawbacks remain, including the riskof pin tract infection, pin loosening,skin traction, regenerate fracture,regenerate deformity, premature ordelayed consolidation, and kneeand/or hip stiffness.3-6 Although thistechnique results in successful out-comes for many patients,1,7 motor-ized intramedullary devices have beendeveloped with the goal of avoidingmany of these complications.
Shawn S. Richardson, MD
William W. Schairer, MD
Austin T. Fragomen, MD
S. Robert Rozbruch, MD
From the Limb Lengthening andComplex Reconstruction Service,Hospital for Special Surgery, NewYork, NY.
Correspondence to Dr. Richardson:[email protected]
Dr. Fragomen or an immediate familymember is a member of a speakers’bureau or has made paid presentationson behalf of NuVasive, Smith &Nephew, and DePuy Synthes; servesas a paid consultant to Globus Medical,NuVasive, Smith & Nephew, andDePuy Synthes; and serves as a boardmember, owner, officer, or committeemember of the Limb LengtheningResearch Society. Dr. Rozbruch or animmediate family member has receivedroyalties from Stryker; is a member of aspeakers’ bureau or has made paidpresentations on behalf of and servesas a paid consultant to NuVasive, Smith&Nephew, andStryker; and serves as aboard member, owner, officer, orcommittee member of the LimbLengthening Reconstruction Society.Neither of the following authors nor anyimmediate family member has receivedanything of value from or has stock orstock options held in a commercialcompany or institution related directly orindirectly to the subject of this article:Dr. Richardson and Dr. Schairer.
J Am Acad Orthop Surg 2018;00:1-7
DOI: 10.5435/JAAOS-D-17-00741
Copyright 2018 by the AmericanAcademy of Orthopaedic Surgeons.
Month 2018, Vol 00, No 00 1
Copyright � the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

The introduction of the magneticlengthening nail (MLN)has graduallyled some surgeons to shift their prac-tices toward internal lengtheningtechniques.8,9 Initial internal length-ening nail designs had many of theirown complications, including diffi-culty controlling lengthening rate,mechanical device failure, prema-ture consolidation, and insufficientbone regenerate.10-14 Some studieseven found that early devices hadmore complications than LON tech-niques.7 However, as the implantdesign and function has improvedover time, more recent studies ofimproved designs have shown thatfemoral lengthening via MLN maybe performed reliably with excellentprecision.15-17
Recent comparative clinical stud-ies have shown that internal length-ening via MLN may reduce many ofthe complications associated withLON, such as pin tract infection,
skin traction, knee stiffness, andregenerate fracture.5,15,18-20 Fur-thermore, patients treated withMLN have been shown to have ashorter mean healing index, allowingearlier weight bearing, as well asimproved patient satisfaction andperception of the cosmetic result oftheir surgery.5 These studies haveonly reinforced patient and surgeonenthusiasm for the technique.Although advances in the implant
technology have led to improvedpatient outcomes with fewer compli-cations, the high implant costs associ-atedwithMLNmay exceed the clinicalbenefits. The purpose of this studywasto determine whether there is a differ-ence in the hospital, surgeon, and totalcost between femoral osteogenesis viaLON or MLN. Furthermore, combin-ing clinical and cost data, we sought toanalyze whether there is a difference inthe relative cost-effectiveness of LONandMLN.
Methods
Patient SelectionAll patients who underwent femorallengthening via distraction osteo-genesis at a single institution between2005 and 2014 were included in thestudy. All surgical procedures wereperformed by the two senior authorsof the study (S.R.R., A.T.F.). Allpatients had a minimum of 2-yearfollow-up. Because of a change inpractice preference of the treatingsurgeons, patients in the earlier sec-tion of our period underwent LON(n = 19; 2005 to 2009), whereasthose later in the period underwentMLN (n = 39; 2012 to 2014). LONwas performed with an expectationof three procedures: osteotomy withthe insertion of the intramedullarynail and application of the externalfixation, removal of the externalfixator, and eventual removal of the
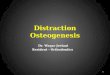
Figure 1
Radiographs depicting treatment with LON and MLN. A through C depict LON: lengthening of the femur using an externalfixator and intramedullary nail (A), consolidation of the regenerate after removal of the external fixator (B), and the ultimateremoval of the intramedullary nail after union (C). D through F depict MLN: insertion of the MLN (D), consolidation of theregenerate after lengthening was completed (E), and the final result after removal of the nail (F). LON = lengthening over anail, MLN = magnetic lengthening nail
Cost of Femoral Lengthening: Lengthening Over a Nail Versus Magnetic Lengthening Nail
2 Journal of the American Academy of Orthopaedic Surgeons
Copyright � the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

intramedullary nail. MLN was per-formed using the PRECICE nail(NuVasive) with an expectation oftwo surgical procedures: osteotomywith insertion of the MLN andremoval of the MLN. The typicaltreatment protocols, as demon-strated by serial radiographs, may beseen in Figure 1.
OutcomesPatient clinical records were retro-spectively reviewed, includingdemographics, the number of inpa-tient and outpatient surgical proce-dures performed, total distractionlength, and time to bony union. Bonyunion was determined based on con-tinuity of three of four cortices on APand lateral radiographs as well as theability to fully weight bear withoutassistance or discomfort.Cost analysis was performed from
the payer perspective.We compiled thetotal payments received by the hospitalfor all care related to femoral length-ening, including surgical, inpatient,and outpatient visits. This total wasincluded as the total hospital cost paidby the payer. For each surgical proce-dure performed, the Current Proce-dural Terminology (CPT) codes billedwere recorded and used to calculate anexpected surgeon fee using the Medi-care Physician Fee Schedule (https://www.cms.gov/apps/physician-fee-schedule/), represented as the surgeoncost. A list of the included CPT codescan be found in Appendix 1. Thesetwo components were summed tocalculate the total cost. To allow dol-lar values to be accurately comparedover the study period, costs wereinflation adjusted to be recorded in2015 dollars using the chained Con-sumer Price Index (https://data.bls.gov/pdq/SurveyOutputServlet).
Statistical AnalysisClinical and cost data were comparedbetween the LON and MLN groups,using chi-squared tests for categorical
data and t-tests for continuous data.Analyseswere performed using STATA(version 14.2; StataCorp).
Results
DemographicsA total of 58 patients were included inthe study, 19 of which had undergoneLON and 39 who had undergoneMLN (Table 1). Most patients weremale, with an average age in thefourth decade. No notable differencewas observed in demographics be-tween the MLN and LON cohorts.
Clinical ResultsThe total length distracted was similarbetween groups (LON, 41.4 versusMLN, 38.5 mm; P = 0.595). The pa-tients treated with MLN had a shorteroverall total time to union (136.7versus 100.2 days; P = 0.001). Inaddition, the time from distractioncompletion to final union was shorterfor patients treated with MLN (85.6versus 57.9 days; P = 0.008). The pa-
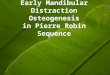
tients treated withMLNunderwent onaverage one fewer surgical procedure(3.1 versus 2.1; P , 0.001), whichresulted from both fewer inpatient andoutpatient procedures (Figure 2).
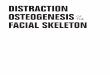
CostsThe total hospital costs paid weresimilar between the groups ($45,913versus $41,680; P = 0.875). Surgeonpayments were markedly lower forpatients treated with MLN ($4,324versus $2,769; P , 0.001). No nota-ble difference was observed in the totalpayments between the two groups($50,255 versus $44,449; P = 0.482).A comparison of costs is shown inFigure 3.
Discussion
In this retrospective comparison of pa-tients undergoing femoral distractionosteogenesis via LON orMLN techni-ques, treatment with MLN resulted inlower surgeon costs with no differencein total or hospital costs. Furthermore,
Table 1
Demographic, Clinical, and Cost Comparison Between Patients WhoUnderwent Treatment With LON Versus MLN
Parameters LON MLN P Value
Number 19 39 —
Female 10.5% 23.1% 0.260
Age (yr) 32.4 6 14.6 29.26 13.4 0.412
Length distracted (mm) 41.4 6 23.2 38.56 16.7 0.595
Time to union (d, total) 136.76 50.4 100.2 6 29.7 0.001a
Time to union(d, postdistraction)
85.6 6 42.8 57.96 31.7 0.008a
Total procedures 3.1 6 0.8 2.1 6 0.5 ,0.001a
Inpatient procedures 1.9 6 1.0 1.3 6 0.4 0.002a
Outpatient procedures 1.2 6 0.5 0.8 6 0.5 0.005a
Outpatient office visits 9.3 6 5.8 6.3 6 3.1 0.021a
Total hospital costs ($) 45,913 6 35,094 41,680 6 22,345 0.875
Total surgeon costs ($) 4,342 6 830 2,7696 768 ,0.001a
Total cost(hospital 1 surgeon, $)
50,255 6 35,103 44,449 6 22,358 0.482
LON = lengthening over a nail, MLN = magnetic lengthening naila Signifies P , 0.05.
Shawn S. Richardson, MD, et al
Month 2018, Vol 00, No 00 3
Copyright � the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

theMLN technique resulted in a fastertime to final bony union with fewersurgical procedures.In addition to similar, if not lower,
cost of treatment, our data show thattreatment with MLN may providea better clinical experience for thepatient. As has been described in past
studies, MLN has many advantagesover LON, including avoiding the useof external fixators. External fixatorshave many disadvantages, such asincreased pain, skin traction due to pintravel, increased hip and knee stiffness,risk of pin-site infections, and socialstigma.3-6 Furthermore, despite a sim-
ilar amount of lengthening betweenthe cohorts, our data show that MLNleads to a faster time to union, thusallowing a shorter total treatment timeand faster return toweight bearing andactivity. These findings echo those ofLaubscher et al,5 who found similarlyfaster time to union for MLN com-pared to a monorail external fixatorsystem. Furthermore, our data showthat patients treated with MLNunderwent on average one fewer sur-gical procedure, thus lowering thenumber of anesthesia episodes andrisks associated therein. This discrep-ancy in the number of surgical proce-dures is inherent in the treatmentprotocols followed for each form oflengthening, as patients undergoingLON were expected to undergo threeprocedures compared with two pro-cedures for MLN, and was not a re-sult of an increased number ofcomplication-related procedures.The hospital cost data used in this
study were a sum of all paymentsmade to the hospital by the payer,which is a more accurate assessmentof cost than total billings, as it reflectswhat the patient or insurance com-pany actually paid for the treatmentreceived, and thus the direct cost to thehealthcare system.The surgeonbillingdata were calculated based on theMedicare PhysicianFee Schedule inanattempt to standardize surgeon fees,as these may vary based on a patient’sinsurance plan and the reimburse-ment schedules for each patient’scorresponding insurance plan werenot available for use in this study.Costs of prolonged treatment with
LON exist that we were not able tomeasure but are important toconsider.Patients undergoing LON requiredadditional procedures and prolongedconsolidation time compared withthose undergoing MLN, which likelyresulted in additional time awayfrom work or other activities. Al-though not accounted for in thisstudy, nevertheless, these indirect costsincrease the treatment cost to society.
Figure 3
Chart showing the comparison of the total, hospital, and surgeon costs forpatients treated with LON versus MLN. *Signifies P , 0.05. LON = lengtheningover a nail, MLN = magnetic lengthening nail
Figure 2
Chart showing the comparison of the number of procedures performed forpatients treated with LON versus MLN. *Signifies P , 0.05. LON = lengtheningover a nail, MLN = magnetic lengthening nail
Cost of Femoral Lengthening: Lengthening Over a Nail Versus Magnetic Lengthening Nail
4 Journal of the American Academy of Orthopaedic Surgeons
Copyright � the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

This studydoes have limitations.Theexact cost of various components ofthe treatment, such as the cost of theindividual implants, was not available.The price paid for implants varies frominstitution to institution, and ourinstitution could be paying less thanothers for the MLN implant. How-ever, the idea that the price would below enough to offset the measureddifference in total cost is unlikely.Furthermore, we were only able
to measure direct costs paid by thepayer; indirect or opportunity costsare not captured in our study. Thesurgeon cost was calculated based onthe reimbursement rates provided byMedicare for thebilledCPTcodesandthus may differ from and not be ap-plicable to patients with private payerinsurance. Additionally, inherent biasmay be observed between the twogroups as they underwent treatmentat different periods and with variablelengths of follow-up.
Conclusions
The results of this study indicate thatsimilar distraction canbe achievedwiththeMLN technique comparedwith theLON technique, but with few surgicalprocedures and with a faster time tofinal bony union. Despite the increasedcost of implants for the MLN tech-nique, the total payments were similarbetween the twogroups, likely from theadditionalproceduresandhospital carerequired in the LON technique.
References
Evidence-based Medicine: Levels ofevidence are described in the table of
contents. In this article, reference 11is a level II study. References 3, 5, 7,and 18 are level III studies. Refer-ences 1-2, 4, 6, 8-10, 12-16, 20 arelevel IV studies. References 17 and19 are level V expert opinion.
References printed in bold type arethose publishedwithin the past 5 years.
1. Kim HJ, Fragomen AT, Reinhardt K,Hutson JJ Jr, Rozbruch SR: Lengtheningof the femur over an existing intramedullarynail. J Orthop Trauma 2011;25:681-684.
2. Sangkaew C: Distraction osteogenesis ofthe femur using conventional monolateralexternal fixator. Arch Orthop Trauma Surg2008;128:889-899.
3. Wan J, Ling L, Zhang XS, Li ZH: Femoralbone transport by a monolateral externalfixator with or without the use ofintramedullary nail: A single-departmentretrospective study. Eur J Orthop SurgTraumatol 2013;23:457-464.
4. Gordon JE, Manske MC, Lewis TR,O’Donnell JC, Schoenecker PL, KeelerKA: Femoral lengthening over apediatric femoral nail: Results andcomplications. J Pediatr Orthop 2013;33:730-736.
5. Laubscher M, Mitchell C, Timms A,Goodier D, Calder P: Outcomesfollowing femoral lengthening: An initialcomparison of the Precice intramedullarylengthening nail and the LRS externalfixator monorail system. Bone Joint J2016;98-B:1382-1388.
6. Song HR, Oh CW, Mattoo R, et al:Femoral lengthening over anintramedullary nail using the externalfixator: Risk of infection and knee problemsin 22 patients with a follow-up of 2 years ormore. Acta Orthop 2005;76:245-252.
7. Mahboubian S, Seah M, Fragomen AT,Rozbruch SR: Femoral lengthening withlengthening over a nail has fewercomplications than intramedullary skeletalkinetic distraction. Clin Orthop Relat Res2012;470:1221-1231.
8. Fragomen AT, Rozbruch SR: Lengtheningof the femur with a remote-controlledmagnetic intramedullary nail: Retrogradetechnique. JBJS Essent Surg Tech 2016;6:1-15.
9. Rozbruch SR, Fragomen AT: Lengthening ofthe femur with a remote-controlled magneticintramedullary nail: Antegrade technique.JBJS Essent Surg Tech 2016;6:1-11.
10. Burghardt RD, Herzenberg JE, Specht SC,Paley D: Mechanical failure of theintramedullary skeletal kinetic distractor inlimb lengthening. J Bone Joint Surg Br2011;93:639-643.
11. Kenawey M, Krettek C, Liodakis E, Meller R,Hankemeier S: Insufficient bone regenerateafter intramedullary femoral lengthening: Riskfactors and classification system. Clin OrthopRelat Res 2011;469:264-273.
12. Kenawey M, Krettek C, Liodakis E,Wiebking U, Hankemeier S: Leglengthening using intramedullay skeletalkinetic distractor: Results of 57 consecutiveapplications. Injury 2011;42:150-155.
13. Lee DH, Ryu KJ, Song HR, Han SH:Complications of the intramedullaryskeletal kinetic distractor (ISKD) indistraction osteogenesis. Clin Orthop RelatRes 2014;472:3852-3859.
14. Schiedel FM, Pip S, Wacker S, et al:Intramedullary limb lengthening with theintramedullary skeletal kinetic distractor inthe lower limb. J Bone Joint Surg Br 2011;93:788-792.
15. Kirane YM, Fragomen AT, Rozbruch SR:Precision of the PRECICE internal bonelengthening nail. Clin Orthop Relat Res2014;472:3869-3878.
16. Schiedel FM, Vogt B, Tretow HL, et al: Howprecise is the PRECICE compared to theISKD in intramedullary limb lengthening?Reliability and safety in 26 procedures. ActaOrthop 2014;85:293-298.
17. Rozbruch SR, Birch JG, Dahl MT,Herzenberg JE: Motorized intramedullarynail for management of limb-lengthdiscrepancy and deformity. J Am AcadOrthop Surgeons 2014;22:403-409.
18. Horn J, Grimsrud O, Dagsgard AH,Huhnstock S, Steen H: Femoral lengtheningwith a motorized intramedullary nail. ActaOrthop 2015;86:248-256.
19. Paley D: PRECICE intramedullary limblengthening system. Expert Rev MedDevices 2015;12:231-249.
20. WiebkingU, Liodakis E, KenaweyM, KrettekC: Limb lengthening using the PRECICETMnail system: Complications and results. ArchTrauma Res 2016;5:e36273.
Shawn S. Richardson, MD, et al
Month 2018, Vol 00, No 00 5
Copyright � the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

Appendix 1
A Listing of the CPT Codes Used in the Calculation of Surgeon Fees.
Techniques Encounter CPT Code Patients Description
MLN Surgery #1 27466 39 Osteoplasty, femur; lengthening
— 27495 39 Prophylactic treatment (nailing, pinning, plating, orwiring) with or without methyl methacrylate, femur
Surgery #2 20680 33 Removal of implant; deep (eg, buried wire, pin, screw,metal band, nail, rod or plate)
Other codes 11044 1 Débridement, bone (includes epidermis, dermis,subcutaneous tissue, muscle and/or fascia, ifperformed); first 20 sq cm or less
— 20902 1 Bone graft, any donor area; major or large
— 27005 1 Tenotomy, hip flexor(s), open (separate procedure)
— 27062 1 Excision; trochanteric bursa or calcification
— 27305 4 Fasciotomy, iliotibial (tenotomy), open
— 27334 1 Arthrotomy, with synovectomy, knee; anterior ORposterior
— 27360 1 Partial excision (craterization, saucerization, ordiaphysectomy) bone, femur, proximal tibia and/orfibula (eg, osteomyelitis or bone abscess)
— 27430 1 Quadricepsplasty (eg, Bennett or Thompson type)
— 27450 3 Osteotomy, femur, shaft or supracondylar; with fixation
— 27470 1 Repair, nonunion or malunion, femur, distal to headand neck; without graft (eg, compression technique)
— 27570 1 Manipulation of knee joint under general anesthesia(includes application of traction or other fixationdevices)
— 27687 1 Gastrocnemius recession (eg, Strayer procedure)
LON Surgery #1 27466 19 Osteoplasty, femur; lengthening
— 20692 19 Application of amultiplane (pins or wires inmore than 1plane), unilateral, external fixation system (eg,Ilizarov, Monticelli type)
Surgery #2 27495 18 Prophylactic treatment (nailing, pinning, plating, orwiring) with or without methyl methacrylate, femur
— 20694 18 Removal, under anesthesia, of external fixation system
Surgery #3 20680 16 Removal of implant; deep (eg, buried wire, pin, screw,metal band, nail, rod or plate)
Other codes 11044 1 Débridement, bone (includes epidermis, dermis,subcutaneous tissue, muscle and/or fascia, ifperformed); first 20 sq cm or less
— 14020 2 Adjacent tissue transfer or rearrangement, scalp, armsand/or legs; defect 10 sq cm or less
— 14021 1 Adjacent tissue transfer or rearrangement, scalp, armsand/or legs; defect 10.1 sq cm to 30.0 sq cm
— 20693 1 Adjustment or revision of external fixation systemrequiring anesthesia (eg, new pin[s] or wire[s] and/ornew ring[s] or bar[s])
— 20902 9 Bone graft, any donor area; major or large
— 27005 1 Tenotomy, hip flexor(s), open (separate procedure)
— 27334 1 Arthrotomy, with synovectomy, knee; anterior ORposterior
(continued )
CPT = Current Procedural Terminology, LON = lengthening over a nail, MLN = magnetic lengthening nailThe typical codes used at each planned surgery throughout the two treatment protocols are delineated, followed by a listing of other codes included inthe study.
Cost of Femoral Lengthening: Lengthening Over a Nail Versus Magnetic Lengthening Nail
6 Journal of the American Academy of Orthopaedic Surgeons
Copyright � the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

Appendix 1 (continued )
A Listing of the CPT Codes Used in the Calculation of Surgeon Fees.
Techniques Encounter CPT Code Patients Description
— 27430 2 Quadricepsplasty (eg, Bennett or Thompson type)
— 27472 5 Repair, nonunion or malunion, femur, distal to headand neck; with iliac or other autogenous bone graft(includes obtaining graft)
— 27479 1 Arrest, epiphyseal, any method (eg, epiphysiodesis);combined distal femur, proximal tibia and fibula
— 38220 1 Bone marrow; aspiration only
CPT = Current Procedural Terminology, LON = lengthening over a nail, MLN = magnetic lengthening nailThe typical codes used at each planned surgery throughout the two treatment protocols are delineated, followed by a listing of other codes included inthe study.
Shawn S. Richardson, MD, et al
Month 2018, Vol 00, No 00 7
Copyright � the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.