Embed Size (px)
Citation preview

Pergamon Evaluation and Program Planning, Vo[. 17, No. 2, pp. 107-120, 1994
Copyright © 1994 Elsevier Science Ltd Printed in the USA. All rights reserved
0149-7189/94 $6.00 + .00
0149-7189(94)E0001-D
COST ANALYSIS OF TRAINING A N D E M P L O Y M E N T SERVICES IN M E T H A D O N E TREATMENT
MICHAEL T. FRENCH, CATHY J. BRADLEY, BRIAN CALINGAERT, MICHAEL L. DENNIS,
and GEORGIA T. KARUNTZOS
Research Triangle Institute, Research Triangle Park, North Carolina
ABSTRACT
Despite the popular belief that vocational training is an important component o f methadone treatment, little information is available on the effectiveness and cost o f various types o f ser- vices. This paper presents a cost analysis o f developing a training and employment program (TEP) at four methadone treatment programs in a quasi-experimental pilot study. We examine the cost o f establishing and operating such programs as well as the marginal cost o f a TEP component compared to standard treatment. For both standard and TEP-enhanced treatment, we also estimate the average, fixed, and variable costs o f these services and compare differ- ences across programs. Lastly, we examine the financing o f standard methadone treatment to provide additional guidanee to program directors and treatment administrators. Our main find- ings can be summarized as follows. The average annual cost o f TEP services in the pilot study was between $1,648 and $2,215 per "serviced" TEP client. The average annual cost per client for standard methadone treatment was between $3,546 and $5,104. And the marginal cost o f providing TEP services to approximately 36 clients per site in the pilot study was between 3.5 o7o and 7.2°7o o f the total annual cost o f standard methadone treatment. The cost methodology presented in this paper can be used in other research projects and by treatment providers to generate consistent and comparable cost estimates o f standard and enhanced substance abuse treatment programs.
Mill ions o f dollars are spent each year for drug abuse
t rea tment services. In 1987, the specialized drug treat-
ment sector had revenues o f $1.3 bil l ion (Institute o f
Medicine [IOM], 1990). Despite cont inued investments
in drug abuse t rea tment , few studies have evaluated the
economic merits o f these programs. Because society does
not possess the resources to suppor t all desirable treat-
ment activities, we must choose which programs and ser-
vices to support and at what level. As resource allocation
becomes more impor tan t , policy makers and p rog ram
adminis t ra tors need decis ion-making tools to evaluate
their opt ions for provid ing and funding t rea tment pro-
grams and services. Economic analysis can play a large
role in these resource a l locat ion decisions.
A cost analysis o f t reatment services is one of the most
impor t an t componen t s o f a t rea tment p rog ram evalua-
tion. Researchers, policy makers, and practit ioners have
all stressed the need for more in fo rma t ion on resource
use, cost, and f inancing o f drug abuse t rea tment ( IOM,
1990; Wallack, Larson, & Tompkins , 1990). A recent re-
view of cost and cost-effect iveness studies o f substance
abuse t rea tment programs (French, in press) found that
many existing cost studies (e.g., Caliber & Associates ,
1989; H a r w o o d , Napol i t ano , Krist iansen, & Collins,
Financial assistance for this study was provided by three grants from the National Institute on Drug Abuse (NIDA) (contract numbers 5 RI8 DA06383-02, 5 RI8 DA07262-02, and 1 P50 DA06990-01A1). The authors are entirely responsible for the research in this paper; it does not represent the position or opinions of NIDA or the Research Triangle Institute (RTI). We would like to acknowledge the numerous contributions of the former and current program directors at the four participating methadone clinics: Ken Bossert, Helen Greet, John Gyuett, Paul Ingram, Jim Nowak, Lou Mania, and Richard Weisen. Without their interest and support, this study would not have been possible. In addition, several colleagues at RTI contributed to the study, including Robert Hubbard, Valley Rachal, and Gary Zarkin.
Requests for reprints should be sent to Michael T. French, Center for Economics Research, Research Triangle Institute, 1615 M Street N.W., Washington, DC 20036.
107

108 MICHAEL T. FRENCH et al.
1984; Horgan, 1991; National Institute on Drug Abuse [NIDA], 1987; Rice, Kelman, Miller, & Dunmeyer, 1990; Wheeler, Fadel, & D'Aunno, 1990) used differ- ent methods of cost accounting and evaluation, which makes comparisons difficult. Clearly, new cost studies based on a consistent methodology are needed to assist policy makers and program administrators in determin- ing optimal resource allocation guidelines, cost account- ing rules, and ways of targeting treatment outcomes.
The research reported in this paper uses a general methodology for conducting cost studies of health care programs that was developed at the Research Triangle Institute (RTI). We have applied this cost methodology in a variety of settings including an enhanced counsel- ing regime in methadone treatment (Bradley, French, & Rachal, forthcoming) ~, quality assurance systems in substance abuse programs, (Anderson, Neighbors, French, & Phillips, 1992), and employee assistance pro- grams (French, Zarkin, & Bray, in press). The applica- tion of our cost methodology for this paper is the Training and Employment Program (TEP) pilot study (Dennis, Karuntzos, McDougal, French, & Hubbard, 1993; French, Dennis, McDougal, Karuntzos, & Hub- bard, 1992). TEP is a multiyear, randomized trial be- ing conducted by staff from RTI and the participating clinics. The data reported here are based on a quasi- experimental pilot study of the TEP protocol that was conducted by RTI at four methadone maintenance pro- grams from Fall 1990 to the end of 1991.
The TEP intervention had many objectives when RTI initiated it in 1989. One of the primary motivations for the intervention was to indirectly reduce the spread of human immunodeficiency virus (HIV) by shortening waiting lists, thus allowing more intravenous drug ad- dicts to enter treatment. If clients were able to maintain a full-time job they might be able to pay for all or some of their treatment, which would free up additional pub- licly supported slots. Increased treatment participation would then indirectly reduce the spread of HIV and a variety of other infectious diseases related to injecting drugs (e.g., hepatitis, tuberculosis, sexually transmitted diseases) (Haverkos, 1991; Haverkos & kange, 1990). This vocational rehabilitation intervention might also provide the impetus for other treatment programs to ex- pand their treatment processes to include vocational training and employment services. Finally, placing cli-
Much of the methodology and analysis plan we developed for this paper was simultaneously developed for the study by Bradley, French, and Rachal (forthcoming), which considered the annual cost of stan- dard methadone treatment and the marginal cost of an enhanced coun- seling component (Dennis, Fairbank, Bohlig, Bonito, & Rachal, 1991). Although each study considered a different intervention in methadone treatment, the methodologies were similar, and two of the methadone programs participated in both research projects. Consequently, we view these two companion studies as evidence that our methodology can be applied to different interventions and senings in methadone lreatmen!.
ents in the work force might have a positive influence on their overall recovery (Dennis et al., 1993).
Overall, the main objectives of the TEP study are as follows:
1. Investigate the availability and effectiveness of exist- ing models for addressing the vocational and em- ployment needs of clients in methadone treatment programs.
2. Assess the feasibility and resource requirements of supplementing local vocational training and employ- ment programs to meet client needs.
3. Determine clients' interest and participation in voca- tional training, public service, and/or job placement programs in response to a variety of incentives.
4. Estimate the total, average, and marginal costs of standard methadone treatment and compare these es- timates with the costs associated with TEPs.
5. Estimate the effectiveness of TEPs in terms of em- ployment, earnings, drug use, criminal behavior, psy- chological functioning, and social functioning.
6. Estimate the net dollar benefits (benefits minus costs) of TEPs, and compare the cost-effectiveness of these programs as a contribution to positive treatment out- comes and as a payback mechanism for treatment.
The research is proceeding in three successive stages, with each stage focusing on two of the objectives listed above and building on the findings of the earlier stages. The first stage focused on the first two objectives and consisted of a needs assessment and a feasibility study. The second stage was a series of quasi-experimental pi- lot tests of various TEP protocols in four methadone clinics across the country and focused on the third and fourth objectives. RTI used the pilot study to develop a finalized protocol and to estimate the required re- sources and sample size for the next stage. The third and final stage of the research is just beginning. It involves a 3-year, multisite, randomized trial of the final TEP protocol and will focus on the fifth and sixth objectives. An integral part of the randomized trial is a comprehen- sive benefit-cost and cost-effectiveness analysis of the TEP intervention.
French et al. (1992) and Dennis et al. (1993) report pre- liminary findings and recommendations from the first and second stages. This paper presents findings from the resource use and cost analysis conducted later during the second stage of the pilot study. We apply our method- ology to the TEP pilot study in the following way: (a) develop a cost estimation method and data collection plan that can be implemented in any type of treatment program; (b) collect and analyze data to estimate the to- tal and average cost of enhanced training and employ- ment services in four methadone treatment programs; (c) estimate the total and average cost of standard meth- adone treatment in these programs; (d) estimate the mar- ginal resources and financial investment needed to

Cost of Job Training in Methadone Treatment 109
augment existing methadone treatment with enhanced vocational training and employment services for a se- lect number of clients; and (e) collect financing infor- mation and organize these data within categories that can be compared across programs and with national averages.
To determine the relative cost of TEP services and standard treatment, we applied our methodology at the four TEP sites located in Pittsburgh, Pennsylvania; Mil- waukee, Wisconsin; Santa Clara County, California; and Buffalo, New York. We designed our data collec- tion protocol to account for all funding sources, to separate annualized costs into fixed and operating cat- egories, and to allocate those costs over clients and interventions. We then developed a systematic, compre- hensive, cost methodology to determine total revenue, total fixed costs, total annual operating costs, average cost (per client), and incremental costs. The findings from our analysis lend insight to the financing and cost of standard and enhanced methadone treatment and of- fer guidelines for estimating future costs. In addition, we compared our findings with those of the National Drug and Alcohol Treatment Unit Survey (NDATUS), the Treatment Outcome Prospective Study (TOPS), and the Drug Services Research Survey ( D S R S ) - t h r e e na- tional studies of drug treatment programs and facilities.
METHODOLOGY
The main objective of the TEP pilot study was to deter- mine methadone clients' interest and participation in a variety of training and employment services. The re- search protocol evolved into a comprehensive vocational program that was integrated into the client's primary substance abuse treatment regimen. This section de- scribes the methodology used to select the methadone treatment programs, to recruit clients f rom the pro- grams, to develop the protocol for the pilot TEP ser- vices, and to estimate treatment costs.
Programs The methadone treatment programs were initially se- lected as part of a Congressionally mandated initiative to develop research demonstrations on the ability to ex- pand treatment capacity through public service and/or vocational training programs to help reduce the spread of AIDS. Methadone programs were selected because they primarily treat injection drug users (IDUs) and because their clients usually face more barriers to em- ployment than do those in many other treatment mo- dalities. Four programs were selected to represent a range of organizational structures (e.g., community- based, hospital-based, county health department), client demographic mixes (e.g., gender, age, race/ethnicity), labor markets, and levels of existing community voca- t ional/employment resources. Programs in the States of New York and California were specifically sought be-
cause they have large treatment populations and unique vocational and public assistance programs.
The program in Buffalo, a hospital-based program, is operated by the Sisters of Charity Hospital . The program in Pittsburgh is operated by PBA, Inc.: The Second Step, and is a freestanding nonprofit organi- zation. The program in Milwaukee was an outpatient clinic located in and operated by the Milwaukee County Mental Health Complex until it was closed on January 1, 1993. The program in Santa Clara County comprises three freestanding clinics operated by the county 's Bureau of Drugs and Alcohol (part of the Heal th Department).
As part of standard treatment, all of the programs conduct random urine tests at least once a month on av- erage, have caseloads of 35 to 40 clients per counselor, develop treatment plans within 15 to 30 days after ad- mission, and have two to three 30- to 40-minute indi- vidual counseling sessions with each client per month, as well as one to four 60- to 90-minute group counsel- ing sessions per month. In terms of methadone dosage, all average 45 to 60 mg/day, with Buffalo and Santa Clara County going up to 80 rag/day on a case-by-case basis. Although Santa Clara County allows more than half of its clients to have take-home privileges after 3 months, the other three sites provide them to fewer than 10% of their clients. All four programs maintain more than half of their clients on methadone for over 12 months after they begin the program.
Clients To get a range of clients in terms of vocational readi- ness and motivation, clients for the pilot study were re- cruited in two primary ways: (a) Each counselor was asked to recommend two clients who would benefit the most from the TEP protocol, and (b) a random sample of all remaining clients were approached about partici- pating in the study. In Santa Clara County and Milwau- kee, all people entering the program between December 1990 and June 1991 were also approached within a month of their beginning the program. The total client participation rate exceeded 80%, varying considerably by the three client samples: 90°7o of the counselor- recommended sample, 83% of the new-admission sam- ple, and 74°7o of the random sample of existing clients.
Within each client sample/site block, clients were randomly assigned to receive either standard (STD) methadone treatment or standard treatment plus TEP. Milwaukee and Pittsburgh had quasi-experimental base- line groups during the start-up (i.e., data collection but no intervention). Most clients, however, were randomly assigned to one of the two conditions. See Dennis et al. (1993) for a detailed description of the methods for as- signing clients in the randomized experiment.
All data were collected through client interviews un- der a Federal Certificate of Confidentiality and under

110 MICHAEL T. FRENCH et al.
TABLE 1
CLIENT DEMOGRAPHICS AT TIME OF ASSIGNMENT, BY GROUP AND PROGRAM
Methadone Program and Client Sample Type
Buffalo Pittsburgh Santa Clara Milwaukee
TEP STD TEP STD TEP STD TEP STD
Demographic (n - 40) (n - 38) (n - 40) (n - 47) (n = 45) (n - 44) (n = 28) (n = 70)
Male 62.5% 67.7% 57.5°,0 60.9% 44,4% 61.4% 56.3% 56.3% Age (average) 35 37 34 34 39 37 34 34 High school diploma/GED 52.5% 61.1 % 65.0% 55.6% 20.0% 20.9% 75.0% 77.4% Married/living as married 45.0% 43.2% 40.0% 30.4% 40.0% 50.0°.0 18.8% 32.3% White, non-Hispanic 47.5% 45.9% 72.5% 65.2% 60.5% 46.5% 73.3% 71.4% Black, non-Hispanic 35.0% 43.2% 27.5% 34.8% 18.6% 4.7% 26.7% 23.8°,4 Have health insurance 88.9% 97.2% 82.5% 88.9% 44.4% 41.9°0 46.7% 39.7% Have private health insurance 16.7% 16.7% 12.5% 6.7°0 0.0% 7.0% 13.3% 17.5% Criminal justice status 35.0% 38.9% 40.0% 50.0% 24.4% 20.5% 37.5?,o 40.6% Legally employed 25.6% 25.0% 17.5% 10.9% 36.4% 36.4% 33.3°,6 30.2% Legal earnings last year $10 ,156 $8 ,263 $12 ,159 $7 ,378 $6,921 $10,649 $5 ,970 $7 ,123 Weeks worked last year 38 29 32 32 29 29 32 33 Illegal earnings last year $10 ,070 $5,587 $18 ,415 $3 ,379 $11,464 $5 ,729 $7 ,675 $5 ,950
TEP = training and employment program group.
STD - standard treatment group.
the supervision of RTI 's Committee for the Protection of Human Subjects. Respondents were paid approxi- mately $10 per hour for participating in the interviews. Table 1 reports client demographics for TEP and con- trol groups, by site, at the time of the initial interview. The clients were approximately 50o/0 to 60°70 male, 50o/0 to 70% white, with mean ages of 34 to 37. Dennis et al. (1993) found statistically significant differences between client groups in only 2 of 24 within-site comparisons of client characteristics and in none of the 8 across-site comparisons. Elsewhere, however, we have found nu- merous differences in vocational experiences and needs by gender (French et al., 1992; Karuntzos, Caddell, & Dennis, 1993; Phillips et al., 1993). This suggests the de- sirability of blocking random assignment on gender for the main trial and conducting several additional sub- group analyses.
Pilot TEP P r o l o c o l The basic components of the pilot TEP protocol (Kar- untzos, Dennis, & Norman, 1991) included (a) perform- ing a vocational needs assessment; (b) developing a vocational treatment plan; (c) developing a resource document to locate existing basic educational, training, public service, and employment programs that can be adapted to the needs of methadone clients; (d) hiring an on-site vocational specialist at each program to work with both the counselors and clients to identify and ad- dress vocational issues; (e) training the vocational spe- cialist to recognize vocational needs and to use the initial vocational plan, resource document, and vocational services (both in-house and referral) to address them;
(f) conducting job readiness/motivational workshops focusing on personal growth, development, and job- seeking skills; and (g) providing a budget to pay for training, service stipends, treatment costs, equipment, t ransportat ion, or child care, or to facilitate in any way the placement of clients into jobs that offer $8+ per hour plus benefits. The vocational specialists at tempted to provide services to everyone assigned to TEP and to maintain weekly contact with those clients.
All three of the vocational specialists had either com- pleted or were working on their master's degrees and had training specifically related to addiction treatment. Each had 5 to 10 years of experience coordinating client ser- vices with other community agencies, and the special- ists in Pittsburgh and Santa Clara County had prior experience working in a vocational program for fami- lies of abused children and in a similar program for the chronically unemployed, respectively.
The interventions specified in the TEP protocol were conceptually similar across sites, but they were not iden- tical. It is therefore more appropriate to view them as four similar experiments rather than a single experiment with four sites. For instance, the vocational specialist in Buffalo focused on vocational counseling and network- ing with local trainers and employers. The specialist in Pittsburgh focused on job development, educational/ training program placement, job placement, and helping clients schedule interviews and services. The specialist in Santa Clara County focused on educational/training program placement and obtaining support services (e.g., t ransportat ion, child care, moving expenses, a welding license, safety equipment, eye glasses, or an automobile

Cost of Job Training in Methadone Treatment 111
starter). The varying types and levels of services provided across sites were based on different client needs and the vocational specialists' areas of expertise.
Instrumentation The TEP pilot study involved a combination of inter- views, service logs, record abstraction, and financial au- diting. To determine their employment history, current employment status, and interest in vocational services, clients were interviewed prior to randomization, and data f rom their program intake interview were ab- stracted f rom their records. The initial interview was a pilot version of the instrument being used in NIDA's Drug Abuse Treatment Outcome Study (DATOS) (Hub- bard & Jordan, 1989). This questionnaire and the sub- sequent 3-month follow-up interview draw extensively from the Treatment Outcome Prospective Study (TOPS) (Hubbard et aI., 1989) and the Addiction Severity In- dex (ASI) (McLeIlan, Luborsky, Cacciola, Griffith, McGahan, & O'Brien, 1985) and are the basis for both the Individual Assessment Profile (lAP) used in the DC Initiative (Flynn, 1991) and the Methadone Treatment Quality Assurance Study (MTQAS) (Phillips, Fountain, Hubbard, Forsyth, & Dunteman, 1992). Of the 113 core items shared between the three instruments, 71070 have test-retest reliability coefficients of .70 or higher, 13 % are between .60 and .69, 11 °7o are between .50 and .59, and only 5°70 are below .50 (Flynn et al., 1992; Phillips et al., 1992).
The vocational specialists used both general and client- specific service logs to document their activities; a na- tional coordinator reviewed these logs weekly to ensure consistency in reporting across sites. To validate the ser- vice data and assess short-term client outcomes, clients were interviewed with the previously mentioned DATOS in-treatment questionnaire 3 months after entering the program. Follow-up was attempted regardless of TEP assignment or methadone treatment status. The overall response rate was 85.1%, varying from 77.307o in Santa Clara County to 90.7°7o in Pittsburgh. The overall com- pletion rates for standard and TEP clients were not significantly different (85.607o vs. 84.7o7o) and varied by only 1.3% to 2.1°70 within sites.
We collected cost data using two different methods. The first method applies to the resource requirements and cost of TEP services. To obtain reimbursement, each program was required to submit monthly expen- diture reports to RTI that detailed TEP resource utili- zation and costs. We compiled and organized these costs into the following categories: labor, program supplies, travel, overhead and other variable, and client services. We then aggregated the values for each month to calcu- late the total cost of TEP services at each site.
In the second method of data collection, we person- ally administered RTI 's DATCAP (Drug Abuse Treat- ment Cost Analysis P r o g r a m ) - a lengthy financing and
cost w o r k s h e e t - t o program staff at their respective clinicsfl We collected information on program funding sources, resource use, and costs (both fixed and vari- able). We examined revenue sources such as public grants (e.g., federal, state, and local), private funds (e.g., donations), and types of client fees (e.g., Medic- aid, client co-pay, private insurance). We also examined fixed costs (e.g., capital and depreciation) and variable costs (e.g., personnel, supplies, utilities) for goods and services used by or for clients. We collected these data for the fiscal year 1991 (the year the TEP pilot study pro- tocol was administered to clients) from financial state- ments and through staff interviews to ensure that the data were based on actual expenditures rather than cli- ent charges or budgeted amounts. Table 2 displays the revenue and cost categories we explored. After collect- ing these data, we determined the total annual cost of standard and TEP-improved methadone treatment. We also derived average (per client) and incremental costs. We then examined the TEP costs as a percentage of to- tal treatment costs and derived similar comparisons for average and marginal costs.
Cost Analysis Cost estimation is inherently linked to the perspective of the ana lys i s - an item may be a cost from one point of view but not f rom another. The cost analysis meth- odology and approach will vary considerably for the treatment system, treatment provider, society, govern- ment, or patient. For example, the cost of travel to and from a clinic is a legitimate cost f rom a client's perspec- tive, but it is not a cost for the treatment provider. Med- icaid payments for treatment are a cost for the paying government agency, a gain to the patient (recipient), and neither a cost nor a gain, but a transfer, to society. These examples demonstrate the importance of first defining
2DATCAP is available from the authors.
TABLE 2 REVENUE, EXPENDITURES, AND OTHER ECONOMIC
COST CATEGORIES EXAMINED a
Revenue Expenditures Other economic costs
Federal grants Fixed (capital) State grants Labor City/county grants Patient variable Other public funds (e.g., methadone, Client payment medical supplies) Private third party Other variable Public third party (e.g., utilities, Private grants and office supplies)
donations Rents Interest Other
Start-up costs Indirect costs Shared resources Donated capital
~See also Bradley et al. (forthcoming).

112 MICHAEL T. FRENCH et al.
the v iewpoin t o f the analysis and then es t imat ing costs accord ing ly .
The analysis r epor t ed in this paper adop t s the t rea t - ment p rog ram perspective. Consequent ly , we do not ex- amine ou t -o f -pocke t expenses, travel t ime, and o ther f inancia l inconveniences for clients who pa r t i c ipa ted in TEP. In add i t ion , we do not consider the admin is t ra t ive costs to federal , state, and local governments that would surely arise if a TEP- l ike p rogram was funded on a much b r o a d e r scale. A n o t h e r fact to cons ider is that each vo- ca t iona l counse lor was able to leverage some o f the ex- ist ing publ ic services that were prev ious ly avai lab le to
t r ea tment clients, but not ut i l ized. A l t h o u g h the cost o f these publ ic services represents a "social cos t" o f TEP, it is not a cost to ind iv idua l p rog rams . Several o ther ex- amples o f this type are c o m m o n features o f the T E P in- te rvent ion. A c know le dg ing that these external "cos ts" o f T E P exist is impor t a n t , but we do not fo rma l ly in- clude these items in our cost analysis given the t rea tment p r o g r a m perspect ive.
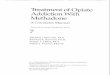
Figure 1 presents the mul t i s tage a p p r o a c h we used to collect and es t imate the total cost o f s t andard t rea tment and the incrementa l cost o f T E P services, in the first s tage o f the process , we deve loped in s t rumen ta t ion to
Determine Percentage of I Total Funding from Each I
Source; Compare to I NDA TUS |
Es t/mate A verage (per c/lent) Annual Coet for Standard Treatment
Eetlmate A verage (per cflent) Annual Cost for Enhanced Treatment
Develop Financing, Resource Use, and Cost Work.sheet with
Detailed Categories for All Items
Conduct Site Visits and Collect Data
Estimate Total and Average Funding from Various Sources
Estimate Total Annual Cost (Fixed and Variable) f~
Standard Treatment
Develop Accounting Procedures for Receiving and Processing
TEP Expense Reports
Estimate Total Annual Cost for Enhanced Treatment
Estimate Ina'emental Cost f(x TEP Services at the
Program and Client Level
Examine Cost Differentials ~ t w ~ n Programs Trealment Regimens
Treatment and Economics Literature, NDATUS, DSRS
Pittsburgh, Buffalo, San Jose, Milwaukee
Budgets, Audit Reports, Grants, Financial Statements
Budgets, Financial Statement Purchase Orders, Receipts
Research Triangle Institute Records and Billing Data
Figure I. Flow diagram of financing and cost analysis of training and employment services in methadone treatment programs. See also Bradle~ el al. (forthcoming).

Cost of Job Training in Methadone Treatment 113
collect the appropriate financial information. The instru- mentation was general enough to cover the operations at any methadone clinic, but it required precise detail on every cost element. For example, we requested infor- mation on all resources that were used in the treatment process, regardless of whether it involved a financial expense (e.g., volunteer labor). We then completed the instrument with the help of program staff during site visits to each of the four methadone clinics. Historical records such as budgets, audit reports, expense reports, and other financial statements were very helpful for es- timating the cost of most resources. We developed im- putation rules to estimate the cost of shared and "free" resources such as equipment and space. With these data, we could then estimate the total and average cost of stan- dard methadone treatment at each program.
Throughout the pilot study we were also compiling and processing the costs of TEP services. Each of the vocational counselors was asked to record all resources (including time) that were allocated to TEP activities. These activity reports were transmitted to RTI on a monthly basis where they were processed and ana- lyzed. At the end of the pilot study, we had a complete breakdown of TEP-related costs by treatment program, month, and activity. These data were used to estimate the total annual cost of TEP services and the incremen- tal cost of TEP services at the program and client levels.
also be positive (French, Zarkin, Hubbard , & Rachal, 1991; Gerstein & Harwood, 1990; Hubbard et al., 1989).
A previously published analysis of the pilot random- ized field experiment (Dennis et al., 1993) found that, relative to standard clients, TEP clients were:
• 1.5 times more likely to have been referred to some kind of class/training and over 20 times more likely to have participated in one or more classes;
• more than 5 times more likely to have been referred to job skills services, 50 times more likely to have ac- tually received job skills services, and 4 times more likely to have completed a formal vocational assess- ment;
• 2 times more likely than standard clients to have been referred to a job program, 2 to 3 times more likely to have received help or support services in their job hunt, and 8 times more likely to have received finan- cial help;
• twice as likely to have received any vocational services, and an average of 3 times as many positive vocational outcomes in the 3-month period; and
• significantly less likely to be unemployed in Pittsburgh (69.4% vs. 36.1%) with a positive trend across sites (divided between about 10°70 of the TEP clients be- coming employed and approximately 6°7o going to school).
R E S U L T S
Preliminary Outcomes of TEP Pilot Study Findings from the TEP pilot study can be summarized as follows (Dennis et al., 1993; Dennis, Karuntzos, & Rachal, 1992; French et al., 1992):
I. Methadone clients have high rates of unemployment, which has been previously linked to poor treatment outcomes.
2. Clients want vocational services, but have had a dif- ficult time accessing the traditional vocational reha- bilitation programs available in the community.
3. The TEP pilot protocol was able to successfully help clients access vocational services in the community, shorten the time to do so, and fill some of the gaps in the social service system.
4. The TEP pilot protocol appears to reduce short-term unemployment by increasing training and employ- ment participation.
The latter two findings are strengthened by the con- sistency of the patterns across different sites, different versions of the TEP protocols in these sites, and differ- ent samples of clients. The long-term outcomes on drug use, criminal activity, and health are not yet available. The previously established links between these problems and employment suggest that long-term outcomes will
The vocational specialists also arranged for 32% of the TEP clients to be reviewed by a state vocational re- habilitation agency and/or JTPA offices and were able to reduce the application time for most benefit programs by 50% to 80°7o. The specialists helped the clients move quickly through the application process by having cop- ies of all of the forms in advance, ensuring that the cli- ents had all of the necessary information, helping to collect many of the the required signatures and reports, walking the clients through the system, and following up with clients as they proceeded through the applica- tion process.
Cost of TEP Services The programs were reimbursed for all allowable ex- penses required to implement the TEP protocol. Table 3 presents a detailed financial breakdown of TEP services provided to clients at each site. These data highlight the diverse array of services purchased across programs. The differences in type and amount of services reflect the diversity of client needs and the availability of existing resources and services. We allowed each vocational spe- cialist to draw on his or her unique understanding of the treatment population, community demographics, and available resources to design a specialized protocol.
Table 4 lists the cost categories, total annual TEP cost, and average annual expenses (per TEP client and per ser- viced TEP client) incurred above the cost for standard

114 MICHAEL T. FRENCH et al.
TABLE 3 TEP SERVICES AND COSTS, BY SITE
Buffalo Pittsburgh Santa Clara Milwaukee ($) ($) ($) ($)
Training/education stipend 239 3,525 5,900 1,513 Training/books/supplies - 278 - 510 Work related equip./tools 32 310 972 238 Training related equip/tools 8 3,419 Transportation 35 499 1,981 1,020 Child care 38 - 147 Clothing 539 150 308 - Medical/eye 131 770 195 Vocational evaluation 348 - 480 - Fee waiver 2,072 - 975 846 Total other services 2,886 992 2,174 695
placement agencies (2,000) (19) (695) meals (5) {273} - - bad debt payment (881) - - - incentives (650) (124) criminal status check (50) -- -- housing -- -- (2,050) --
Total 6,320 6,532 16,551 4,822
Note. Costs were taken from expense logs kept by the vocational specialist, reporting dollars spent for client services.
methadone treatment at each program. Some of the dif- ferences in TEP costs between sites are due to geograph- ical differences in the costs of identical resources and not necessarily to a difference in the type or amount of re- sources. For example, the vocational specialist in Santa Clara County received a higher salary than the other vo- cational specialists due to higher wage scales in that lo- cal labor market. Similar examples exist where the cost of services do not correspond directly with the amount of services received. Unfortunately, these distortions will
always be present in geographical comparisons of pro- gram costs. Lastly, some of the differences in total TEP cost are due to the number of clients actually assigned and serviced, which varied across sites.
To estimate the average cost per TEP client, we di- vided the total annual costs of TEP by the number of clients who were assigned to the TEP protocol. For a variety of reasons (e.g., gainfully employed, ineligible due to disability, heavy drug users, declined services, not ready for training), not all TEP-assigned clients actu-
TABLE 4 ANNUAL TOTAL AND AVERAGE COSTS OF ADDING TEP SERVICES
Program (December 1990-November 1991 )
Buffalo Pittsburgh Santa Clara Milwaukee a
Labor $38,402 65% $41,681 57% $49,762 69% $50,981 82% Client services b $8,671 15% $12,926 18% $16,500 23% $6,443 10% Program supplies $3,298 6% $1,541 2 % $ 553 1% _ c _ c Travel $1,211 2% $3,035 4% $2,625 4% $1,870 3% Overhead & other variable $7,736 13% $14,033 19% $2,619 4% $2,728 4% Total annual TEP cost $59,318 100% $73,217 100% $72,060 100% $62,022 100%
TEP clients assigned 40 40 45 28 Cost per assigned client $1,483 $1,830 $1,601 $2,215
TEP clients serviced 36 38 43 28 Cost per serviced client $1,648 $1,927 $1,676 $2,215
aCOsts are from April 1991 January 1992 and represent partial implementation, prorated to 12 months. bClient services include indirect overhead expenses and indirect operating costs for the vocational specialist in Pittsburgh, Buffalo, and
Milwaukee. Clncluded in client services.

Cost of Job Training in Methadone Treatment 115
ally received services. Therefore, we also calculated the average effective cost per client for each site by divid- ing the total cost of TEP by the total number of clients who actually received some services. Although both measures of the average cost per client vary widely across sites, we cannot conclude that one program is more cost- effective than another without examining program out- comes (e.g., employment, earnings, retention, drug use, criminality). Furthermore, to derive the total annual cost of TEP-enhanced treatment, we must add the total an- nual cost of standard treatment to the cost estimates in Table 4.
Cost of Standard Methadone Treatment To put the cost of TEP services into the proper perspec- tive, it is useful to compare the cost of TEP-enhanced treatment with the cost of standard methadone treat- ment. In addition to estimating the total annual cost of standard methadone treatment, we disaggregated total cost into five categories-building and equipment, rent and maintenance, labor, other variable, and contracted services. Assigning costs to certain categories can be somewhat arbitrary, but we found that these five cate- gories effectively illustrated the operations of the metha- done clinics in our study. Table 5 presents the results of our cost analysis for standard treatment. Not surpris- ingly, labor (particularly medical personnel, nurses, and physicians) was the most costly resource at each pro- gram. Labor 's share in total cost hovered around 50% at each program, with a high of 59% at the Pittsburgh clinic and a low of 43% at the Milwaukee clinic. The other cost categories displayed considerable variability across programs. Contracted services (i.e., physicians, attorneys, and accountants) was the next highest expense
at Pittsburgh and Milwaukee, but it was much lower in Buffalo because this program received most of these ser- vices from the host hospital.
Given the diversity in services and size at these four programs, average cost estimates may be a more mean- ingful financial description than total cost. The most common way to calculate average cost is to divide total cost by some measure of caseflow. But caseflows are so erratic at methadone clinics that the average cost esti- mates would be highly sensitive to external factors (e.g., seasonal variation, staffing changes). To develop an ob- jective and comparable measure of average cost, we first calculated the static caseload for each program. We de- fine static caseload as the typical number of clients re- ceiving treatment at any point in time over the course of a year. The static caseload measure is preferable to a dynamic measure of caseflow because it avoids distor- tions due to treatment completions or dropouts, seasonal variations, and other episodes that occur sporadically during the year. It should be noted that all four pro- grams had significantly higher actual admissions com- pared to the static caseload. As shown in Table 5, the average annual treatment cost per client in our study was between $3,546 and $5,104, with a mean treatment cost per client of $4,002 ($5,934,783/1,483).
Program administrators and evaluators are often re- quired to document the marginal cost and benefit of an ancillary service(s). In Table 4, we reported the total and average cost of the TEP services provided at each clinic. It is natural to ask how the relative cost of TEP com- pares with standard treatment. At the bottom of Table 5, we report two ratios that help answer this question. The first measure is the ratio of total annualized cost of TEP services to total annualized cost of standard treatment.
TABLE 5 ANNUAL COSTS OF STANDARD METHADONE TREATMENT
Program
Source of Revenue Buffalo a Pittsburgh a Santa Clara Milwaukee
Fixed (building/equipment) b $105,340 $83,107 Rent & maintenance (buildings) $6,955 $93,783 Labor $456,072 $911,139 Other variable $215,971 $226,546 Contracted services $34,864 $238,241 Total annual cost $819,202 $1,552,816
Static caseload 210 400 Total annual cost per client $3,901 $3,882
Total TEP cost/total standard cost 7.2 % 4.7 % Average TEP cost/average standard cost 42.2% 49.6%
$374,030 $43,734
$1,153,136 $301,192 $159,606
$2,031,698
573 $3,546
3.5% 47.3%
$5,262 $333,591 $661,826 $130,665 $399,723 c
$1,531,067
30O $5,104
4.1% d 43.4% d
aStandard treatment costs for these two sites are also reported in Bradley et al. (forthcoming). bAverage across two or more years. Clncludes salaries and fringe benefits for five counselors and three urine tests per week per client. dCosts are from April 1991 -January 1992 and represent partial implementation, prorated to 12 months.

116 M I C H A E L T. F R E N C H et al.
This ratio ranged from a low of approximately 3.5% at Santa Clara County to a high of 7.2% at Buffalo. 3
The second ratio in Table 5 divides the average annu- alized cost per serviced TEP client by the average an- nualized cost per client in standard treatment. This measure may be more meaningful from a programmatic perspective, and it is more comparable across programs because it adjusts for program size and TEP caseloads. Buffalo had the lowest ratio of average cost for stan- dard and TEP services and Pittsburgh had the highest. Although concluding that Buffalo provided TEP ser- vices more efficiently than the other three sites may be tempting, such judgments are unwarranted without sys- tematic and comparable information on service deliv- ery and effectiveness.
Financing To generalize findings across the four programs, we also considered the programs' varied financing sources. We identified the primary payment sources for methadone treatment as self/family (out-of-pocket), private insur- ance, Medicaid/Medi-Cal/Medicare, charity, and other sources (e.g., MCHCP). Table 6 shows the percentage of clients in each program who relied on these payment sources for treatment. The bottom line of Table 6 is the percentage of total revenue dollars that came from cli-
3These estimates require at least two qualifications. First, the total cost estimates are sensitive to the number of" clients assigned and served at each program. Thus, it would be misleading to view the marginal cost estimates as representative of the costs to implement TEP program- wide. Second, recall that the TEP protocol was similar but not identical across sites. Consequently, these estimates highlight some differences in the cost of administering TEP, but they do not conclusively dem- onstrate differences in resource efficiency of cost-effectiveness,
TABLE 6
P E R C E N T A G E OF CL IENTS BY PRIMARY P A Y M E N T S O U R C E
Prog ram
Source of Buf fa lo a P i t tsburgh a Santa Clara M i lwaukee
Paymen t (%) (%) (%) (%)
Sel f / fami ly 2 8 18 6 5 2 8
Pr ivate insurance - 6 2 17
Medica id 6 6 76 - 17
Med ica re 4 - 8
Medi -Cal -- - 3 3 -
Char i ty 1 - -- --
M C H C P b -- 3 0
No pay 1 1 -- --
Cl ient f ees as
pe rcen tage of
total p rogram
paymen ts 9 4 41 8 51
aClient in format ion for these two si tes is also repor ted in Brad ley
et al. ( fo r thcoming) .
bMi lwaukee Coun ty Heal th Care Program.
ent fees. As shown in the table, Santa Clara County had a significantly smaller percentage of total revenue from client fees. The other programs rely heavily on client fees and reimbursement for treatment from public sources (e.g., Medicaid).
Table 7 contains the distribution of revenue by program and funding source. The three nonhospital p r o g r a m s - Pittsburgh, Milwaukee, and Santa Clara C o u n t y - r e - ported greater dependence on public grants than the hospital-based program in Buffalo. These three pro- grams relied on public grants to subsidize program ac- tivities that were not covered by client fees. We believe this difference is based primarily on the relationship be- tween the host hospital and the methadone treatment program (i.e., the treatment program sometimes has the opportunity to benefit from shared resources with the hospital). For example, if the Buffalo program had ex- cess demand for treatment services due to limited space, the host hospital may agree to subsidize operations by donating existing space at the hospital to use for treat- ment services. While the free-standing programs usually have to seek external funding for this situation, the hospital-based program can also explore internal fund- ing sources within the hospital.
Another way to describe treatment financing at these programs is to compare the funding percentages to national averages. The National Drug Abuse Treatment Unit Survey (NDATUS) asks treatment directors to re- port funding levels for the following categories- federal grants, state grants, other public sources, private sources, and all other sources. Results from the 1988 survey show that 4,403 drug abuse treatment programs (including outpatient methadone, residential, and outpatient drug- free) received total annual funding of $1.31 billion (NIDA, 1989). While the NDATUS categories are not exactly comparable to our categories, Table 8 shows that the funding profile at the Milwaukee clinic is similar to national averages, but the other three programs have moderate to extreme differences. For example, Pitts- burgh and Santa Clara both have a much larger share of funding from federal grants and a much smaller share of funding from private sources compared to the NDATUS averages. In addition, Buffalo received about two-thirds of its total funding from other public sources (i.e., Medicaid), which is considerably higher than the national average of 14 percent. Although some of these differences are dramatic, they should not be interpreted as a measure of program efficiency or effectiveness.
D I S C U S S I O N
The TEP pilot study and current TEP randomized trial represent ambitious attempts to improve drug abuse treatment. Research has shown that drug abuse treat- ment can effectively improve the employability and in- crease the earnings of drug abusers in methadone and residential clinics (French et al., 1991; French & Zarkin,

Cost of Job Training in Methadone Treatment 117
TABLE 7
DISTRIBUTION OF R E V E N U E BY P R O G R A M AND S O U R C E
Program
Source of Revenue Buf fa lo a Pi t tsburgh a Santa Clara M i lwaukee
Federal grants - 2 1 % 6 0 % -
State grants . . . .
O ther state funds - -- 1 2 % 4 9 %
Coun ty grants - 3 7 % - -
O ther coun ty funds - 2 % 1 4 % --
Other publ ic funds -- - - 6 % --
Cl ient paymen t 2 7 % 5 % 7 % 2 1 %
Private insurance -- 2 % _ b 1 3 %
Med ica id 6 3 % 3 3 % - 1 2 %
Med icare 4 % - - 5 %
Donat ions 6 % - - -
Interest _ _ b _ _ b __ b
Other - -
Total annual revenue $ 8 5 5 , 6 6 4 $ 1 , 6 3 4 , 3 7 0 $ 2 , 3 2 0 , 9 9 8 $ 1 , 5 1 5 , 6 4 2
aFinancing informat ion for these two si tes is also repor ted in Bradley et al. ( fo r thcoming) .
bLess than 0 . 5 % .
1992). Dennis et al. (1991) reported that vocational and educational counseling is associated with lower drug in- jecting rates of heroin, cocaine, speedballs, and drugs in general. French et al. (1992) showed that positive em- ployment outcomes also enhanced other treatment out- comes such as reduced drug use and criminality. Despite these encouraging signs, many programs have reduced or eliminated vocational services in treatment due to changes in the therapeutic process and/or financial pres- sure. The findings of this study will help decision mak- ers explore the feasibility of a renewed emphasis on vocational services in treatment.
Although some national surveys of the treatment sys- tem have included a cost component (NIDA, 1989; Hor- gan, 1991; Hubbard et al., 1989), our study is one of the first to rigorously analyze the cost of standard and TEP- enhanced methadone treatment at the program level (see also Bradley et al., forthcoming). Our economic model is more appropriate than accounting methods for pro-
gram evaluation because it estimates the opportunity costs of both fixed and operating resources. The most useful documents for assessing these costs are financial audit reports compiled by external auditors, grant ap- plications and awards, invoices, and contract agree- ments. We found that these documents were available at the program sites but often lacked organization and required further explanation from the program director, administrative staff, and auditors. Indirect costs, how- ever, were often elusive and difficult to calculate. To es- timate these indirect costs, we met directly with program directors and financial officers and developed imputa- tion rules to value "free" or shared resources.
We summarize our research findings for the four treat- ment programs as follows:
• The total annual cost of TEP services ranged from $59,318 to $73,217, the average annual cost per as- signed TEP client ranged from $1,483 to $2,215, and
T A B L E 8
C O M P A R I S O N OF FUNDING S O U R C E S TO N D A T U S FINDINGS
Program N D A T U S
Source of Buf fa lo a Pi t tsburgh a Santa Clara M i lwaukee 1 9 8 9
Revenue (%) (%) (%) (%) (%)
Federa l grants -- 2 0 . 8 5 9 . 5 -- 3.1
State/ local - 3 8 . 7 2 6 . 4 4 8 . 5 3 4 . 8
O the r publ ic 6 6 . 6 3 2 . 8 6 . 4 17.1 1 4 . 3
Pr ivate th i rd-party 3 3 . 4 7 .7 7 .4 3 4 . 4 4 2 . 4
O the r . . . . 5 . 4
aFinancing in format ion for these two si tes is also repor ted in Bradley et al. ( fo r thcoming) .

118 MICHAEL T. FRENCH el al.
the average annual cost per serviced TEP client ranged from $1,648 to $2,215.
• The total annual cost of standard methadone treat- ment ranged from $819,202 to $2,031,698, and the av- erage annual cost per client ranged from $3,546 to $5,104.
• The marginal cost of providing TEP-enhanced treat- ment to a select number of clients was between 3.5% and 7.2% of the total annual cost of standard treat- ment and between 42.2°70 and 49.6% of the average cost per treatment client.
Looking first at standard methadone treatment, the total annual cost varied considerably depending on the level of treatment services offered and the number of cli- ents served. For example, Milwaukee, the most costly (on a per-patient basis) of the four programs, had a more stringent regiment of urine monitoring (2 times per week versus 8 to 12 times per year in most programs) offered clients a much fuller range of ancillary services. In gen- eral, ancillary services varied considerably by site and included such services as adult day care, child care, re- ferral services, aftercare, AIDS education seminars, fre- quent medical check-ups, and psychological testing. Similarly, Santa Clara County had the highest annual cost estimate, but this program also provided treatment to significantly more individuals than the other pro- grams. When we converted the total cost estimates to a common unit (i.e., the cost to treat one client for one year), we found that the average cost estimates were more consistent. The average annual standard treatment cost was between $3,546 and $5,104 at the four programs studied, which is slightly higher than estimates from ear- lier studies, most likely due to our opportunity cost ap- proach. For example, DSRS reported median per-slot cost, for all types of programs, at $4,600 (Horgan, 1991). The 17 methadone treatment programs that par- ticipated in TOPS had an average annual cost of $1,945 per client in 1980 (equivalent to $3,085 in 1990 dollars) (Hubbard et al., 1989).
Across-program differences in TEP costs were not as pronounced as the cost differentials for standard treat- ment. As mentioned earlier, the structural components of TEP-enhanced treatment were designed to provide on-site vocational services, vocational/educational as- sessments, increased vocational counseling, and place- ment into training and jobs at each site. However, the individual protocols varied somewhat across sites due to counselor styles, client needs, local labor markets, and other factors. Consequently, the marginal cost of pro- viding TEP services ranged from a low of approximately 4% of total treatment costs at the freestanding sites to a high of approximately 7% of total treatment costs at the hospital-based program. Santa Clara County, the TEP program with the largest number of serviced cli-
ents (43), had one of the lowest per-client costs ($1,676), and Milwaukee, the TEP program with the smallest number of serviced clients (28), had the highest per-client cost ($2,215). As suggested earlier, these differences in cost per TEP client can be attributed to differences in caseloads, areas of expertise of the vocational special- ists, and the type and intensity of client services.
The cost methodology presented in this paper is more rigorous than the methods used in earlier substance abuse studies and the results are informative. However, we must caution the reader to avoid using these esti- mates for national policy purposes given the small num- ber of programs in our study. We feel confident that we accurately described the financing and operations at the four programs that participated in the TEP pilot study. And the estimates can be reviewed by other methadone programs to see how they compare across different financing and cost categories. But the primary contri- butions of the paper lie in the cost methodology itself, the DATCAP instrument, and a demonstration of how it can be applied to a substance abuse intervention. Future analyses of the TEP trials will combine cost in- formation with data on treatment effectiveness to assess the cost-effectiveness of standard and TEP-enhanced methadone treatment.
To further improve program success and cost-effec- tiveness, several changes have been made to the TEP pilot protocol for the current randomized trial. First, the services provided by the vocational specialist will be in- tegrated into the client's primary treatment plan and co- ordinated with the primary counselors. This feature leads to more comprehensive care for the client and al- lows the vocational specialist to service a higher case- load. Second, the vocational specialists will use a case management model to target services that can be funded and/or leveraged from existing community resources. This will increase the likelihood that client services can be maintained beyond the duration of the study and that TEP can be generalized to other standard treatment pro- grams. Third, each client assigned to the TEP interven- tion will be categorized into a vocational readiness group (i.e., prevocational, training ready, job ready) deter- mined by the information given in the Individual Assess- ment Profile (lAP) and other vocational screeners. This will enable the vocational specialists to target specific ser- vices based on individual needs and will help the primary counselor develop a short- and long-term treatment plan. Fourth, an on-site vocational research assistant will work with the vocational specialist to help coordinate client services and develop contacts and resources. Finally, the vocational specialists and research assistants will use a computerized integrated control system to track general and client-level services. Monthly reports summarizing services and activities will be generated and distributed to the vocational specialists, the primary counselors, and

Cost of Job Training in Methadone Treatment 119
the RTI research staff as a tool for providing ongoing program direction. Further information on current re- search plans and protocol is available from the authors.
R E F E R E N C E S
ANDERSON, D.W., NEIGHBORS, D.M., FRENCH, M.T., & PHIL- LIPS, C.D. (1992). Quality assurance in drug abuse treatment: Esti- mating quality assurance program operating costs. Report prepared for Office of Applied Studies, Substance Abuse Mental Health Ser- vices Administration.
BRADLEY, C.J., FRENCH, M.T., & RACHAL, J.g. (forthcoming). Costs and financing of standard and enhanced methadone treatment. Journal o f Substance Abuse Treatment.
CALIBER & ASSOCIATES. (1989). Cost benefit study of the Navy's level 1H alcohol rehabilitation program. Final Report. Fairfax, VA: Author.
DENNIS, M.L., FAIRBANK, J.A., BOHLIG, E.M., BONITO, A.J., & RACHAL, J.V. (1991). Reducing injection drug use through meth- adone assisted rehabilitation: Factors other than methadone dosage. Paper presented at NIDA's Third Annual National AIDS Research Demonstrations Conference, Washington, DC.
DENNIS, M.L., KARUNTZOS, G.T., & RACHAL, J.V. (1992). Ac- cessing community resources through case management to meet the needs of methadone clients. In R. Ashery (Ed.), Progress and issues in case management (NIDA Research Monograph 127, pp. 54-78). Rockville, MD: National Institute on Drug Abuse.
DENNIS, M.L., KARUNTZOS, G., McDOUGAL, G., FRENCH, M., & HUBBARD, R. (1993). Developing training and employment pro- grams to meet the needs of methadone treatment clients. Evaluation and Program Planning, 16, 73-86.
FLYNN, P.M. (1991). D.C. Initiative instrumentation (Subcontract under NIDA Grant No. DA07082-01). Research Triangle Park, NC: Research Triangle Institute.
FLYNN, P.M., HUBBARD, R.L., FORSYTH, B.H., FOUNTAIN, D.L., SMITH, T.K., & HOFFMAN, J.A. (1992, August). Individual Assessment Profile (IA P): Standardizing the assessment of substance abusers. Paper presented at the 100th Annual Meeting of the Ameri- can Psychological Association, Washington, DC.
FRENCH, M.T. (in press). Economic evaluation of drug abuse treat- ment programs: Methodology and findings. American Journal of Drug and Alcohol Abuse.
FRENCH, M.T., DENNIS, M.L., McDOUGAL, G.L., KARUN- TZOS, G.T., & HUBBARD, R.L. (1992). Training and employment programs in methadone treatment: Client needs and desires. Journal of Substance Abuse Treatment, 9, 293-303.
FRENCH, M.T., ZARKIN, G.A., & BRAY, J.W. (in press). A meth- odology for evaluating the costs and benefits of employee assistance programs. Journal o f Drug Issues.
FRENCH, M.T., ZARKIN, G.A., HUBBARD, R.L., & RACHAL, J.V. (1991). The impact of time in treatment on the employment and earnings of drug abusers. American Journal o f Public Health, 81, 904-907.
FRENCH, M.T., & ZARKIN, G.A. (1992). The effects of drug abuse treatment on legal and illegal earnings. Contemporary Policy Issues, 10, 98-110.
GERSTEIN, D.R., & HARWOOD, H.J. (Eds.). (1991). Treating drug problems: Vol. 1. A study o f the evolution, effectiveness, and financ- ing of public and private drug treatment systems (Reprint). Washing- ton, DC: U.S. Government Printing Office. (Original work published in 1990 by National Academy Press).
HARWOOD, H.J., NAPOLITANO, D.M., KRISTIANSEN, P.L., & COLLINS, J.J. (1984). Economic costs to society of alcohol and drug abuse and mental illness: 1980. Final report prepared for the Al- cohol, Drug Abuse, and Mental Health Administration (RT1 2734/00- 01FR). Research Triangle Park, NC: Research Triangle Institute.
HAVERKOS, H.(1991). Infectious diseases and drug abuser. Jour- nal of Substance Abuse Treatment, 8, 269-272.
HAVERKOS, H., & LANGE, R. (1990). Serious infection other than human immunodeficiency virus among intravenous drug abusers. Jour- nal o f Infectious Diseases, 161, 894-902.
HORGAN, C. (1991, January). Cost of drug treatment programs: Pre- liminary findings from the 1990 drug services research survey. Pre- sented at the NIDA National Conference on Drug Abuse Research and Practice, Washington, DC. Rockville, MD: US Department of Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration.
HUBBARD, R.L., & JORDAN, B.K. (1989). Drug abuse treatment outcome study (DATOS) (NIDA Contract No. 271-89-8233). Research Triangle Park, NC: Research Triangle institute.
HUBBARD, R.L., MARSDEN, M.E., RACHAL, J.V., HARWOOD, H.J., CAVANAUGH, E.R., & G1NZBURG, H.M. (1989). Drugabuse treatment: A national study of effectiveness. Chapel Hill, NC: The University of North Carolina Press.
INSTITUTE OF MEDICINE (IOM). (1990). Treating drug problems. Washington, DC: National Academy Press.
KARUNTZOS, G.T., CADDELL, J.M., & DENNIS, M.L. (1993, June). Gender differences in vocational needs and outcomes for meth- adone treatment clients. Paper presented at the Fourth Biennial APA Society for Community Research and Action Conference. Williams- burg, VA.
KARUNTZOS, G.T., DENNIS, M.L., & NORMAN, H. (1991). Voca- tional protocol for methadone treatment clients (NIDA Grant No. 5-R18-DA06383-02). Research Triangle Park, NC: Research Trian- gle Institute.
McLELLAN, A.T., LUBORSKY, L., CACCIOLA, J., GRIFFITH, J., McGAHAN, P., & O'BRIEN, C.P. (1985). Guide to the Addic- tion Severity Index." Background, administration, and field testing re- sults (DHHS Publication No. ADM 85-1419). Rockville, MD: National Institute on Drug Abuse.
NATIONAL INSTITUTE ON DRUG ABUSE (NIDA). (1987). Na- tional drug and alcoholism treatment unit survey (NDATUS). Final Report, Publication No. (ADM) 89-1626. Rockville, MD: Author.
NATIONAL INSTITUTE ON DRUG ABUSE (NIDA). (1989). Na- tional drug and alcoholism treatment unit survey (NDATUS). Final Report. Rockville, MD: Author.

120 M I C H A E L T. FRENCH et al.
PHILLIPS, C., FOUNTAIN, D., HUBBARD, R., FORSYTH, B., & DUNTEMAN, G. (1992). Methadone Treatment Quality Assurance System (MTQA S)feasibility study: Results f r o m part one o f the f ie ld test (NIDA Contract No. 271271-8%8532). Research Triangle Park, NC: Research Triangle Institute.
PHILLIPS, C., FOUNTAIN, D., HUBBARD, R., FORSYTH, B., DUNTEMAN, G., & WECHSBERG, W.M. (1993, June). GenderdiJL jerences among those entering drug abuse treatment: Traditional, clas- sical, and current issues. Paper presented at the Fourth Biennial APA Society for Community Research and Action Conference, Williams- burg, VA.
RICE, D., KELMAN, S., MILKER, L.S., & DUNMEYER, S. (1990). The economic costs o f alcohol and drug abuse and mental illness: 1985. San Francisco: Institute for Health and Aging, University of California.
WALLACK, S.S., LARSON, M.J., & TOMPKINS, C. (1990). Issues" in the financing, delivery, and costs o f drug abuse services'. Waltham, MA: Center for Drug Abuse Services Research, Bigel Institute for Health Policy, Brandeis Universily.
WHEELER, J.R.C., FADEL, H., & D'AUNNO, T.A. (1990). Own- ership and perJormance in outpatient substance abuse treatment cen- ters. Ann Arbor: University of Michigan, Institute for Social Research and School of Public Healtt~.