Embed Size (px)
Citation preview

Cost analysis of large-scaleimplementation of the ‘Helping Babies
Breathe’ newborn resuscitation-training program in Tanzania
The Harvard community has made thisarticle openly available. Please share howthis access benefits you. Your story matters
Citation Chaudhury, Sumona, Lauren Arlington, Shelby Brenan, AllanKaijunga Kairuki, Amunga Robson Meda, Kahabi G. Isangula, VictorMponzi, et al. 2016. “Cost Analysis of Large-Scale Implementationof the ‘Helping Babies Breathe’ Newborn Resuscitation-TrainingProgram in Tanzania.” BMC Health Services Research 16 (1)(December). doi:10.1186/s12913-016-1924-2.
Published Version doi:10.1186/s12913-016-1924-2
Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:33732141
Terms of Use This article was downloaded from Harvard University’s DASHrepository, and is made available under the terms and conditionsapplicable to Open Access Policy Articles, as set forth at http://nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of-use#OAP
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by Harvard University - DASH

1
Costanalysisoflarge-scaleimplementationofthe‘HelpingBabiesBreathe’newborn
resuscitation-trainingprograminTanzania
Authors:
SumonaChaudhury,MRCP,MPHa
LaurenArlington,MPHb
ShelbyBrenan,MD,MPHa
AllanKaijungaKairuki,MD,MPHb
AmungaRobsonMeda,MDb
KahabiG.Isangula,MD,MPH,CPHb
VictorMponzi,PgDM&Ec
DunstanBishanga,MD,Mscc
EricaThomas,MD,Mmedc
GeorginaMsemo,MD,Mmedd
MaryAzayo,MD,Mmedd
AliceMolinier,MBA,MSce
BrettD.Nelson,MD,MPH,DTM&Hb,f,g
Institutions:
a.HarvardT.H.ChanSchoolofPublicHealth,Boston,MA02115,USA
b.DivisionofGlobalHealth,MassGeneralHospitalforChildren,Boston,MA02114,USA
c.Jhpiego,DaresSalaam,Tanzania
d.MinistryofHealthandSocialWelfare,DaresSalaam,Tanzania
e.Children’sInvestmentFundFoundation,LondonW1S2FT,UK
f.DepartmentsofPediatricsandEmergencyMedicine,MassachusettsGeneralHospital,Boston,
MA02114,USA
2
g.HarvardMedicalSchool,Boston,MA02115,USA
Emailaddresses:
Correspondingauthor:
SumonaChaudhuryBMBS,MRCP(UK),MPH,MSc
DepartmentsofEpidemiologyandGlobalHealth
HarvardT.H.ChanSchoolofPublicHealth,Boston,MA02115,USA
mobile+1.617.642.4451

3
Abstract
Background:HelpingBabiesBreathe(HBB)hasbecomethegoldstandardgloballyfortraining
birth-attendantsinneonatalresuscitationinlow-resourcesettingsineffortstoreduceearly
newbornasphyxiaandmortality.Thepurposeofthisstudywastodoafirst-everactivity-based
cost-analysisofat-scaleHBBprogramimplementationandinitialfollow-upinalargeregionof
Tanzaniaandevaluatecostsofnationalscale-upasonecomponentofamulti-methodexternal
evaluationoftheimplementationofHBBatscaleinTanzania.
Methods:Weusedactivity-basedcostingtoexaminebudgetexpensedataduringthetwo-
monthimplementationandfollow-upofHBBinoneofthetargetregions.Activity-costcenters
includedadministrative,initialtraining(includingresuscitationequipment),andfollow-up
trainingexpenses.Sensitivityanalysiswasutilizedtoprojectcostscenariosincurredtoachieve
countrywideexpansionoftheprogramacrossallmainlandregionsofTanzaniaandtomodel
costsofprogrammaintenanceoveroneandfiveyearsfollowinginitiation.
Results:TotalcostsfortheMbeyaRegionwere$202,240,withthehighestproportiondueto
initialtrainingandequipment(45.2%),followedbycentralprogramadministration(37.2%),and
follow-upvisits(17.6%).WithinMbeya,49trainingsessionswereundertaken,involvingthe
trainingof1,341healthprovidersfrom336healthfacilitiesineightdistricts.Tosimilarlyexpand
theHBBprogramacrossthe25regionsofmainlandTanzania,thetotaleconomiccostis
projectedtobearound$4,000,000(around$600perfacility).Followingsensitivityanalyses,the
estimatedtotalforallTanzaniainitialrolloutliesbetween$2,934,793to$4,309,595.Inorderto
maintaintheprogramnationallyunderthecurrentmodel,itisestimateditwouldcost
$2,019,115forafurtheroneyearand$5,640,794forafurtherfiveyearsofongoingprogram
support.

4
Conclusion:HBBimplementationisarelativelylow-costinterventionwithpotentialforhigh
impactonperinatalmortalityinresource-poorsettings.Itisshownherethatnationwide
expansionofthisprogramacrosstherangeofhealthprovisionlevelsandregionsofTanzania
wouldbefeasible.Thisstudyprovidespolicymakersandinvestorswiththerelevantcost-
estimationfornationalrolloutofthispotentiallyneonatallife-savingintervention.
Keywords:
Activity-basedcosting,Cost-analysis,HelpingBabiesBreathe,newbornresuscitation,
resuscitation-training,low-incomecountries,Tanzania,low-resourcesetting,resource-poor
setting

5
Background
Anestimated2.9millionneonatallives(frombirththroughday28)arestillbeinglosteachyear
globally,withthepersistinghighestrisksofdeathoccurringinAfricancountriesandwithinthe
first24hoursoflife[1].Addressingglobalstandardsofcareforneonatestoreducethesedeaths
isofincreasingimportanceinacceleratingprogresstowardthefulfillmentofglobalchild
mortalityreductiontargets[2].Neonataldeathsaredueinparttoalackoftrainedbirth
attendantswithbasicrequisiteskillsfornewbornresuscitation[2].‘HelpingBabiesBreathe’
(HBB)isanevidence-basedcurriculumdevisedtomeetthetrainingneedsoflargegroupsof
birthattendantstobecomeskilledintheessentialsofneonatalresuscitation,withafocuson
achievingadequateventilationofapneicnewbornswithinthefirstminuteoflife–theso-called
“GoldenMinute”[3].
TheAmericanAcademyofPediatricsdevelopedHBB,inpartnershipwithUSAID,Savethe
Children,andUNICEF,amongstothers[4].AsHBBbecomesthegoldstandardofcarefor
minimumnewbornresuscitationtrainingofallbirthattendantsglobally,bothgovernmentand
non-governmentalentitiesareincreasinglyfocusingoncostsandimpactsofimplementation.
Althoughsomestudieshaveinvestigatedthecost-effectivenessofEssentialNewbornCare(ENC)
andintegratednewborncarepackagesincorporatingresuscitationtoreducenewbornmortality,
veryfewattemptshavebeenmadetodatetoquantifythecostsandeffectsofnewborn
resuscitationatscaleinresource-poorsettingswherethepotentialcost-effectivenessmaybe
invaluable[5-13].AlthoughENCexpansionaloneinresource-poorsettingshasbeen
investigated,withManayasanetal.reportinga41%reductioninneonatalmortality(RR0.59
95%CI0.48-0.77),furtherinvestigationofasphyxia-relateddeathsandthosepotentially
preventablethroughneonatalresuscitationcapacity-buildingwarrantfurtherinvestigation

6
[9].
Althoughlarge-scaleformalcost-effectivenessanalyseshavebeenplannedtoaddressexpansion
ofsuchHBBprogramsinresource-poorsettings[13],ourstudyisthefirsttofullydescribethe
costsofimplementingtheHBBprogramataregionalandnationalscale.Priortothisstudy,cost
analysisofHBBintroductionhadbeenlimitedtoamissionaryhospitalinTanzania,inwhichHBB
wasfoundtobeahighlycost-effectiveintervention[6].Byaccountingforcostsataregionaland
nationalscaleinTanzania,weattempttoaccountforthediversescopeofserviceprovisionand
potentialforachievingeconomiesofscaleforgovernmentsconsideringexpansionin
comparableresource-limitedsettingsascalledforbyMsemoetal[7].
InSeptember2009,theTanzanianMinistryofHealthandSocialWelfare(MOHSW)launcheda
nationalHBBtrainingprogram.Since2012,throughthefundingsupportoftheChildren’s
InvestmentFundFoundationandimplementationpartnerJhpiego,HBBhasbeenimplemented
atscalein16regionsthroughoutTanzaniainaphasedregion-by-regionrolloutamonga
targeted14,000facility-basedproviders.Initialone-dayHBBtrainingsessionswereheld
centrallywithinseveraldistrictsineachtargetregionwithprovidersfromalllevelsofthehealth
caresystem.Fourtosixweekspost-training,follow-upvisitswereconductedatallofthe
facilitiesforprogrammonitoring,equipmentassessment,andfollow-upappraisalofthe
trainees’skillsthroughobjectivestructuredclinicalexaminations(OSCEs)[16].Additional
subsequentfollow-upandsupportivesupervisionvisitswerealsoprovidedlongitudinally.The
TanzaniaMOHSWhasplansinprogresstointegrateHBBexpansionwithENC,toachieve
economiesofscaleanddemonstrateglobalstandardsofnewborncare.

7
Thepurposeofthisstudywastoconductacostanalysisasonecomponentofamulti-method
externalevaluationoftheimplementationofanHBBprogramatscaleinTanzania.Thiscost
analysisaimedtodeterminethefullcostsofinitialprogramimplementationinonegenerally
representativeregionofTanzania.AnydifferencesinthisregionwithotherregionsofTanzania
wereaccountedforinadditionalscale-upandsensitivityanalysestomodelwhattheprojected
costswouldbeforprogramimplementationthroughoutnationalmainlandTanzania.Further
sensitivityanalysesarealsopresentedforappraisalofpotentialmaintenancecostsoveraone-
andfive-yearperiod,accordingtothecostsofconductingrepeatedrefreshertrainingsusingthe
currentmodel.AsHBBisfurtherexpandedacrossTanzaniaandacrosstheglobe,thesecostdata
willhelptoinformstakeholdersonthehumanandfinancialresourcesneededtoaccelerate
reductionsinneonatalmortalityandestablishglobalstandardsofnewborncare[5-12,17].
Methods
Aim
Theprimaryobjectiveofthisstudywastodoafirst-everactivity-basedcost-analysisofat-scale
HBBprogramimplementationandinitialfollow-upinalargeregionofTanzaniaandevaluate
costsofnationalscale-upasonecomponentofamulti-methodexternalevaluationofthe
implementationofHBBatscaleinTanzania.
StudyDesign
Theactivity-basedcost-analysisstudyutilizedreal-timecostdatacollectionduringatwo-month
periodofprogramadministrationinacross-sectionaldesigninaselectedregionofTanzania.
Sensitivityanalyseswereutilizedtoestimatenationalcostsofscale-up.
8
StudySetting
ThestudywaspurposivelyconductedinMbeyaRegion,whichislocatedinthesouthwest
mainlandofTanzania,islargelyrural,andissurroundedbyhighlands.Theregionalcapitalis
MbeyaCity.MbeyaRegionisoneofTanzania’s25mainlandregions,coveringanareaof
62,420km2withapopulationof2,707,410accordingto2012censusfindings[18].Withinthe
MbeyaRegion,thereareatotalof407healthfacilities(386ofwhichareoperational),the
majoritybeingdispensaries,followedbyhealthcenters,andhospitals[19].TheMbeyaRegion
waspurposelyselectedforregional-levelprogramcostanalysisasisthoughttobehighly
representativeoftheoverallvariationofurbanandruralproviderswithinthemainland
Tanzanianhealthcareproviderlandscape.Scale-upanalysisisconductedtoextrapolatefindings
totheotherregionswhereHBBisbeingimplemented.Scale-upandsensitivityanalysesconsider
theeffectsofvariationinregioncharacteristics,includinggeographicalareaandpopulation
densitytocapturepotentialcostdifferencesbetweenregionsuponnationalscaleup.
Datacollectionandcostanalysis
Thecostdatarelatedtotrainingimplementationandfacility-levelfollow-upwerecollected
betweenFebruaryandMarch2014.Cost-analysisoftheprogramusedamicro-costing,bottom-
upapproachcombiningactivity-basedcosting(ABC),usingreal-timebudgetexpensedata[21-
24].Activity-basedcostingisapreferredmethodinthecontextofprogramexpansion[24-25].
Expendituredatawerecollectedfromthecentral,DaresSalaam-based,Jhpiegoprogramoffice
todetermineexpensesattributabletotheHBBprograminMbeya.Costdataforthisstudywere
collectedusingaseriesofquestionnaires.Staffattheimplementingorganizationheadquarters
filledoutstandardizedstructuredformstoobtainreal-timecostdataonofficecosts,personnel
costs,initialtrainingsessions,refreshertrainings,andmonitoringvisits.Itemizationofall

9
individualinputactivitiesperformedaspartoftheHBBprogram(e.g.,theinitialtraining
sessions,equipmentdistribution,monitoringvisits)wascompletedusingthesestandardized
datacollectioninstruments.
Threecategoriesofcostswereconsideredinthisstudy:(1)program-specificcosts,(2)personnel
costs,and(3)capitalcosts.Theactivitycostcenterswithinthesecostcategorieswereitemized
as:(1)initialtrainingsessionandequipment,(2)facility-basedfollow-upvisits4-6weekspost-
training,and(3)centraladministrationoftheprogram(Tables1and2).Sensitivityanalyses
accountforgeographicalandeconomicsourcesofvariationincostandforcostsofmaintenance
oftheprogramaccordingtorepetitionofthefollow-upvisitsthatwouldberequiredoveraone-
yearperiodtosustaintheprogramandaccordingtotherefreshertrainingsandproject
continuedadministrationandequipmentcostsoverafive-yearperiod(Tables3and4).
Personnelcosts
Centraladministrationpersonnelcostswerelimitedtostaffoftheimplementingpartner,
Jhpiego.Thesearepartiallyrecurringcostsandrefertocost-activitycenterA:central
administration.PersonnelemployedbyJhpiegoinTanzaniaareinvolvedinmanydifferent
programsasidefromHBB,therefore,theirexpenseswereadjustedtoreflecttheproportionof
personneltimeattributabletoHBBinMbeyaRegionduringthetwo-monthimplementation
period.Personnelincludedprogramleadership,implementationstaff,monitoringstaff,and
administrativesupport.Furtherrolesofcentraladministrationstaffwereitemizedinthecost
analyses,sub-dividedintoauditandfinance,communications,humanresources,operations,
procurement,programstaff,andtransportstaff(Tables1and2),withabreakdownofexact
costsandtheirrespectiveproportionsfortheMbeyainitiationpresented(Table2).Further

10
administrationcostswereattributabletoofficespacerent,officeutilitiesandsupplies,andstaff
benefits.Whenconsideringthemaintenanceoftheprogramperrefreshertrainingconducted,a
proportionofthesecostswouldberequisite.Itisestimatedherethatapproximately20%ofthe
initiationcentraladministrationcostswouldberequiredperrefreshertraining(Table4).
Programimplementationadministrationcostswereagainattributabletoimplementation
partnerJhpiegostaffwithadditionalassistanceofregionalanddistrict-levelMOHSWleadership.
Thesearepartiallyrecurringcostsreferringtocost-activitycentersBandC:initial-trainingand
follow-uptraining.Rolesofprogramimplementationstaffareagainitemized,sub-dividedinto
perdiemsfortrainers,trainees,implementingpartnerstaff,andministryofhealthstaff(Tables
1and2),withabreakdownofexactcostandtheirrespectiveproportionsfortheMbeyaRegion
initiationpresented(Table2).Cost-activitycenterCrepresentsafullyrecurringcostand
providesthebasisfortheprogrammaintenance-costanalysis,asongoingprogramsupportis
basedonconductingrepeatedfollow-uptrainingsintheformofrefreshertrainingswitha
proportionofcost-activitycentersAandBcoststoaccountfortherepeatedcentral
administrationandresuscitationequipmentcostsrequired(Table4).
HBBprogram-specificcosts
TheseincludedcostsincurredexclusivelyintheimplementationoftheHBBprograminthe
MbeyaRegion.Thesearepartiallyrecurringcostsandrefertocost-activitycentersBandC:
initialtrainingandfollow-uptraining(withcost-activitycenterC:follow-uptraining,
representingafullyrecurringcostasabove).TheseincludeallexpensesattributabletoHBB
trainingsessionsandfacility-basedfollow-upvisits,specifically,costsrelatedtotraining
equipment,rentalofatrainingvenue,food,transportation,andaccommodations.Program-

11
specificcostsweredifferentiatedfrompersonnelandcapital-costs,bothofwhichmaybe
sharedwithJhpiegoprogramsotherthanHBBand,therefore,representedaproportionoftheir
centralofficecosts.Thesignificanceofprogram-specificcoststodecision-makersliesinthat
theymustberegularlyrenewedasareaccountedforinthemaintenanceanalysispresented
below(e.g.,intheformofrefreshertrainingsandequipmentreplacement).Equipment
replacementwasfactoredintotheanalysisofmaintenancecosts,assumingupto20%of
equipmentwouldrequirereplacingperyearfollowinginitiation(Table4).
Capitalcosts
Capitalcostswereitemizedwithincost-activitycenterA:centraladministration.Thisincluded
vehicles,officeinfrastructure,computers,officefurniture,andotherassetsrequiredforthe
functioningofJhpiego’scentralofficeinDaresSalaamandproportionallyattributabletothe
two-monthimplementationofHBBinMbeya.
Equipmentcosts
Equipmentcostswereitemizedwithincost-centerB:initialtraining,asingeneralthesecostsare
notanticipatedtoberecurring,butaproportionofreplacementcostsareaccountedforin
programmaintenancecostprojections.ResuscitationequipmentincludedLaerdalNeoNatalie
mannequinsandmultiplesetsofreusablebag-maskandsuctiondevices,accordingtothesizeof
thefacility.Trainingmaterials(e.g.,HBBlearner’smanuals,HBBwallposter,largeHBBflipchart,
etc.)werealsoprovided.
Sensitivityanalyses

12
Finally,sensitivityanalyseswereconductedtodemonstratehowpotentialvariationsinvariables
acrosssettingsmightimpactoverallcosts(Table3).Sourcesofvariationinprogram-specificand
administrativecostsareanticipatedaccordingtodifferencesinregionaleconomicvariation,
distancebetweentheregionandcentraladministration,populationcoverage,and
implementationbylocalministryofhealthoraninternationalnon-governmentalorganization.
Equipmentcostsareanticipatedtovaryacrosssettings,througheconomiesofscale,andmay
reduceovertimeasadvancesaremadeinproduction.
Maintenancecosts
Additionalsensitivityanalyseswereundertakentoestimatethosecoststhatwouldbeincurred
forsustainingthetrainingthroughrepeatedrefreshertrainingsandtheattendant
administrationandequipmentcostsoveraone-andfive-yearperiod(Table4).Aprojected20%
oftheprograminitiationcostswasestimatedaseffortneededforcentraladministrationto
deliverrefreshertraining.Allcentraladministrationcostswerebaseduponthecostsneededof
thenon-governmentalimplementationpartnertoconductwork.Allcentraladministrationcosts
andmaintenanceadministrationcostsare,therefore,proportionallyattributabletotheduration
ofactivityneededbyacentralsupportmechanism.Aprojected20%ofinitialequipmentcostsis
usedtoestimatetheannualcostofreplacingequipmentinmaintainingtheprogram,assuming
alossoffunctioninsomeofthematerialsovertime.
Results
Costanalysis
ThetotalcostforimplementationoftheHBBtrainingprogramintheMbeyaRegionoveratwo-
monthperiodin2014was$202,240.Thisincludedtotalinitialtrainingcostsof$91,425,total

13
follow-upvisitcostsof$35,659,andtotalcentraladministrationcostsof$75,156.Intotal,49
trainingsessionswereundertaken,involvingthetrainingof1,341healthprovidersfrom336
healthfacilitiesinMbeyaRegion,suchthatthecostofdeliveringHBBtrainingattheregional
levelwas$4,128pertrainingsession,costing$151pertraineeand$602perhealthfacility.
CoverageoftheHBBtrainingprogram
Atotalof336of407(82.6%)healthfacilitiesintheMbeyaRegionparticipatedinthetrainings,
withanaverageoffourprovidersfromeachfacility,rangingfromonetonine,dependingonthe
leveloffacility.Duringthefacility-basedfollow-upvisits,theJhpiegoprogramassessedatotalof
1,001healthprovidersfrom322ofthese336trainedhealthfacilities(95.8%).Tenofthe11
(90.9%)districtcouncilswerealsovisited.
Costdistribution
OftheoveralltotalprogramcostsforimplementingHBBinMbeyaRegion,thehighest
proportionofcostswasspentoninitialtrainingcosts(45.2%),followedbycentral
administrationcosts(37.2%),andlastlyfollow-upvisitcosts(17.6%)forprograminitiation.
Scale-upcosts
Allscale-upestimateswerebasedonthebest-availablenationaldataforscalingtothe25
Tanzanianmainlandregions.ThefiveadditionalregionsofZanzibarareundertheleadershipof
aseparateministryofhealthand,asislandregions,wereconsideredtohaveuniquecosting
issuesand,therefore,arenotincludedintheanalyses.However,theestimatespresentedhere
relyonassumptions,whichareexploredfurtherinthesensitivityanalysesanddiscussedas
limitationstothisstudybelow.
14
Perhealthfacility
Accordingtonationaldata,thereareatotalof7,537healthfacilities(6,640ofwhichare
operational)withintheTanzanianmainland.7Usingper-facilitycostscalculatedinthisstudy,
scale-upto6,226(82.6%coverage,aswithMbeyaRegion)ofthesefacilitieswouldcostan
estimated$3,747,429.
Pertrainingsession
Forty-ninetrainingswererequiredtoreach336healthfacilities.Coverageof82.6%ofthetotal
nationalnumberofhealthfacilitieswouldrequireanestimated908trainingsessions,costinga
projected$3,747,579.
Pertrainee
AssumingroughlyfourhealthcareproviderstrainedinHBBperhealthfacility,andassuming
82.6%coverage,thecostofscaling-uptrainingtoreach24,904providerswouldbe$3,755,772.
Calculationsofnationalcostsbasedonper-facility,per-training,andper-traineecostsinMbeya
Regionwerefairlyconsistent.Theoverallrangeinthesevariousper-itemestimatessuggestsa
minimumpotentialcostof$3,747,429andamaximumpotentialcostof$3,755,772tocover
approximately82.6%ofmainlandTanzania.Theeffectsofpossiblesourcesofvariationare
exploredinbriefinthefollowingsensitivityanalyses.
Sensitivityanalyses

15
Extensionindurationofinitialtrainingwouldincurthegreatestpotentialimpactonoverall
nationalrolloutcosts.Withinregionalcostofinitialtraining(cost-centerB;Table1and2),
57.3%ofthecostswerecalculatedtoberecurring(personnel,venue,foodandhousing;Table
2).Hence,costsforextendeddurationofinitialtrainingwouldcosttothenationalrolloutan
estimatedadditionof$970,470peradditionaldayofinitialtraining(Table3).Variationin
programcostsandpersonnelcostsbetweenregions–forexample,asaresultofattainable
populationcoverageanddistancebetweentheregionandthenationalcapital–may
additionallyincursignificantimpactsonnationalscale-up(Table3).Themajorityofoverall
personnelcosts,includingcentraladministrationandprogram-specificpersonnel,were
attributabletoprogramimplementationstaff,withafurther28.9%toadministrativesupport,
2.0%toleadership,1.7%tomonitoringandevaluationstaff,andtheremaining10.0%tofringe
benefits.
Economicvariation,includingalterationsininterestratesandthevalueofthecurrency
(estimatedwithintherangeof-5%to+5%ofcurrent),mayincurchangestoallelementsofthe
programcosts,suchthatoverallcostsofnationalrolloutmayvaryfrombetween$3,560,051to
$3,934,793.TheextenttowhichexpansionofHBBtrainingisachieved,intermsofthenumber
ofregionalfacilitiessuppliedwithtrainedbirthattendantsandtheconsequentcoverageofthe
populationwithHBBservices,influencesallelementsofprogramcosts.Variationofthis
coveragefrom65%to95%ofthetotalpopulationmayleadtoavariationinthetotalcostof
nationalrolloutoftherangeof$2,948,702to$4,309,595.Changesinthedistancebetweena
regionandcentraladministration,aswellasthepopulationdensityoftheregion,mayimpact
costsoftransportation,program-specificpersonnelastheymayneedtotravelformoredays,as
wellasthecostsofthevenue,food,andhousing.Variationinregionaldistancefromcentral

16
administrationmayincurvariationinallTanzaniaprogramrolloutcostsintherangeof
$3,582,678to$3,912,166.Variationinequipmentcostsrangingfrom-20%to+20%–depending
on,forexample,economyofscale,wouldbeexpectedtoincurimpactsonprogramsupply
costs,suchthatthetotalTanzaniaprogramcostmayvaryfrombetween$3,605,951to
$3,888,893.
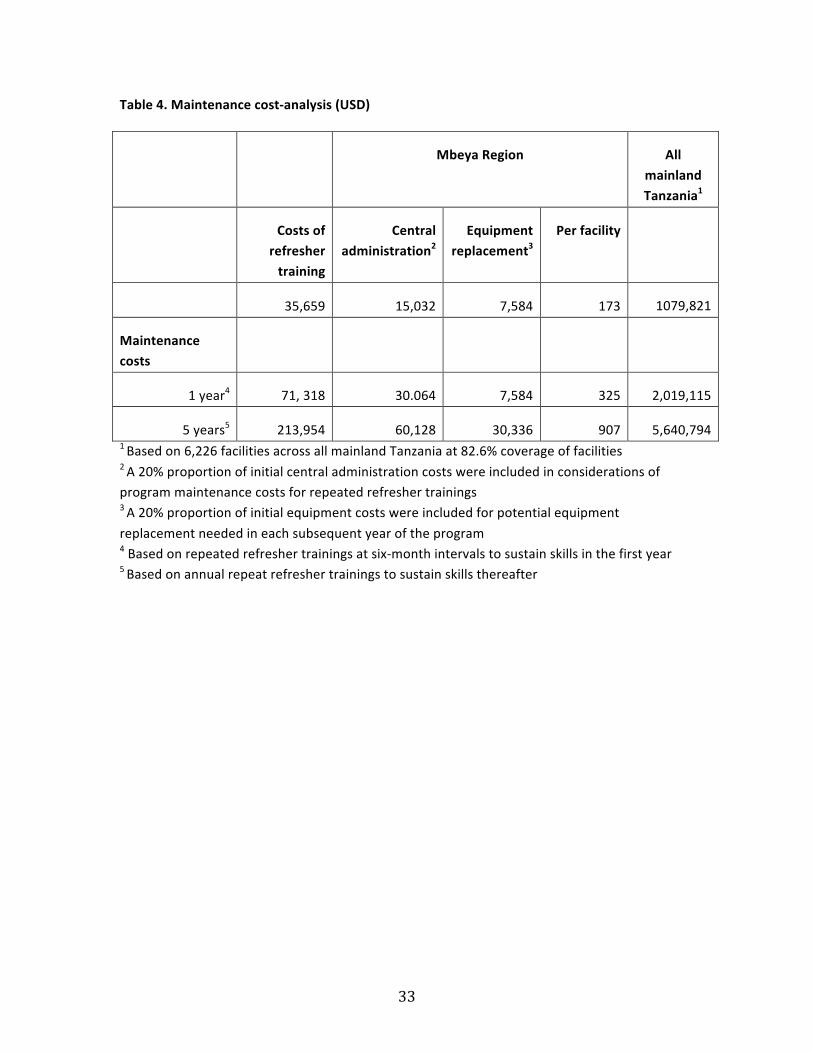
Maintenancecosts
Analysesarepresentedforcostsofrepeatedrefreshertrainingsoveraone-yearandfive-year
durationfollowingHBBprograminitiation.Costsofrepeatedrefreshertrainingareassumedto
beconsistentwithfollow-uptrainingcostsduringtheinitiation.Overthisperiod,itisanticipated
thatthein-countryMinistryofHealthwouldassumeresponsibilityfortheprogramtoachieve
economiesofscaleresultinginareducedregularinvestmentof20%oftheinitialcentral
administrationcostsforeachrefresher-training.Twentypercentofinitialequipmentcostsare
anticipatedforreplacementsforeachyearfollowinginitiation.Itis,thus,estimatedthatit
wouldcostaround$173perfacilityforasinglerefreshertrainingsession($1,079,821forall
Tanzania)andhence$2,019,115tosustaintheprogramnationallyforoneyearbasedontwice
yearlyrefreshervisitsinthefirstyear,and$5,640,794tosustaintheprogramnationallyforfive
yearsbasedonannualrefreshertrainingsthereafter.
Discussion
HBBisconsideredoneoftheleadinginterventionsforimprovinghealthoutcomesinlow-and
middle-incomecountries[26].AsHBBisfurtherexpandedacrosstheglobe,theseat-scalecost
datawillbeanessentialtoolprovidingstakeholderswithcriticalinformationonthehumanand
financialresourcesneededtodeliverreductionsinperinatalmortality.Ourcalculationsprojecta

17
costtoimplementinganHBBtrainingprogramat$4,128attheregionallevel,servingaround
sevenhealthfacilitiesatacostapproximating$602perhealthfacility.Weestimateeachre-
trainingtocost$1,211forsevenhealthfacilities($173perfacility).Voissusetal.foundina
singlehospitalsiteinTanzaniathatinitialtrainingcost$2,084andre-trainingcost$1,515[6].
Ourcostdatacapturecost-influentialfactorsinvolvedinrollingoutanHBBprogramata
regionallevel,weexpectthesedatatobeareasonableestimateofregionalcostsofscale-upin
regionscomparabletoMbeyaRegion.Ournationalestimateof$4,000,000isfurtherexamined
insensitivityanalysestoconsidertheeffectsofvariationsincost-influentialvariablesacrossthe
differingregionsofTanzania,givingboundstothisestimateof$2,934,793to$4,309,595.Our
costestimatesarebasedonaone-dayinitialtrainingperiod.Furtherestimationoftheimpactof
extendeddurationtotheinitialtrainingisconsideredtohavethegreatestoverallimpacton
potentialcosts,atanexcessofjustunder$1,000,000perday.Additionalcost,therefore,isa
considerationindecisionsregardingtheoptimaldurationoftheinitialtrainingperiodin
resource-limitedsettings.
Resuscitationtrainingofbirthattendantswithinintegratednewborncarepackagesalongwith
otherevidence-basedmeasurestosaveliveshaveresultedinsignificantreductionsinneonatal
mortality[5-12].Carloetal.didnotfindareductioninmortalityfollowingintroductionof
newbornresuscitationtraining,however,theresuscitationtrainingwasconductedafterENC
trainingthatincludedelementsofresuscitationtraining,dilutinganypotentialeffects[12].Bang
etal.reportedsignificantreductionsinneonatalcase-fatalityduetosevereasphyxia(by45%,
from39to20%(p<0.07))andasphyxia-relatedneonatalmortality(by65%,from11to4%
(p<0.02))inastudyofcommunityhealthworkersinIndiatrainedinbothnewborncareand
resuscitationskills[14].TheFIRSTBREATHtrialestimatedreductionstobeashighasa30to

18
40%[12].Similarly,Sabinetal.estimateda45%reductionfromacombinedprogram(RR0.55
95%CI0.33to0.90)[5].CountriesimplementingHBBandnewborncareprogramsare
anticipatedtobenefitfromthesystemsapproachtotraining,suchthatexpansionofHBBmay
beconvenientlyundertakeninconjunctionwithENCandotherinterventionsforfullpotential
neonatalmortalityimpactsandcost-savingstoberealized[15].
ThisstudyinTanzaniarepresentsafirst-evercost-analysisofimplementingtheHBBtraining
programatscale.Regionalcostswerecalculatedtoprojectcostestimatesfornationalrolloutof
theprogram.Datawerecapturedinareal-timeefforttoexpandHBBacrossMbeyaRegion.This
isthefirstreportofaregionalcost-analysisinalow-incomecountrysetting.Activity-based
costingmethodology,usedincombinationwiththebottom-upcostingandingredients
approachgivesanaccuratemeasureofthecostsinvolvedattheregionallevel,aswellasavalid
basisfromwhichtoestimatenationalinitiationandmaintenancecostsfortheHBBprogram.
CostsfortheHBBprogramweredividedintothreeactivity-costcenters–initialtrainingand
equipment,facility-basedfollow-upvisits,andcentraladministration–andintothreecost
categories–program-specificcosts,personnelcosts,andcapitalcosts.Ofthese,initialtraining
costswerefoundtobethehighest,andcapitalcostswerethelowest.Withinthetrainingcosts,
personnelcostswerethehighest,followedbythecostofHBBtraining-relatedequipment.
Limitations
Costswithinthisstudyareestimatedundertheassumptionsofamodelofimplementation
largelyadministratedbynon-governmentalorganizationsand,hence,reflecthigher
organizationalpersonnelandadministrationcosts.Althoughthereislittleavailabledataonthe
comparativecostsofgovernmentalversusnon-governmentalexpenditureinsuchprograms,

19
nationalministriesofhealthwouldbeinapositiontoachievesignificantcostsavingsthanare
achievableworkingwithanon-governmentalimplementationpartner,toreducethecostsof
programexpansionascomparedtowhatispresentedhere.Additionaleconomiesofscalecould
beachievedonlargerbulk-purchaseofequipment.Inthecurrentanalysis,theaveragecostof
equipmentwas$350perfacilityinordertoprovidefacilitieswithmultiplesetsoftraining
materials,includingaLaerdalNeoNataliemannequin,HBBlearner’smanuals,wallposters,and
multiplesetsofHBBnewbornresuscitationequipment(e.g.reusablebag-maskdevice,reusable
suctiondevice,etc.)accordingtothesizeoftheregionalfacility[20].Furthermore,integration
ofHBBwithinapackageofENCandotheressentialneonatalserviceswouldlikelyfurther
reduceoverallcentraladministrationcosts,whilstincreasinghealthgainsandconsolidatinga
systemsbasedapproachtoneonatalhealthcare[15].Empiricaldataontheextentofcost-
savingsachievablethroughgovernmentadministrated,integrateddeliveryofcareathigh
volume,suchthateconomiesofscalecouldbefullyrealized,withinresource-limitedsettingsare
warranted.Suchsourcesofpotentialcost-savingsonoverallnationalHBBprogramrolloutand
sustainabilitycostswerenotimmediatelyestimablewithinthelimitsofthecurrentstudy.
ForthisanalysisitwasnecessarytoextrapolaterealtimecostdatafromMbeyaRegioninorder
tomakeestimatesforscale-uptoalloftheothermainlandregions.Whilesensitivityanalyses
servedtoapplythisregionalinformationtoprojectednationalimplementation,these
projectionsnecessarilyrelyonassumptionsthatthecostofprogramimplementationinMbeya
RegionisrepresentativeofotherregionswithinTanzaniaandatdifferenttimes.Effortsto
accountformajorsourcesofpotentialvariationincostsregionallyandovertimearepresented
inthesensitivityanalyses.Thefindingsofthesensitivityanalysis,suggestthatthenational
estimateforprograminitiationweprojectofaround$4,000,000ispotentiallyrobusttoseveral

20
sourcesofcross-regionaldifferencesincost-influentialvariables.Weconsidertheinfluenceof
economicvariationssuchasinterestrateandcurrencyvaluationchanges,populationcoverage
achievableacrossregionsaccordingtogeographicalareaandpopulationdensity,distanceofthe
regionfromthesiteofcentraladministration,aswellaspotentialvariationsinthecostsof
equipment.However,ourchoiceofcost-influentialvariableswarrantfurtherinvestigation,as
thereisuncertaintyregardingthetrueeffectsofvariationacrossregionsuponnational
expansionoftheprogram.
Regionalexpansionpresentedhereachieved82.6%coverageoffacilitiesand74.6%coverageof
providers.Thisrepresentsahighlysatisfactoryproportionofcoverageforanat-scale
interventioninareal-worldlow-incomecountrysetting,consideringthevariationinhealth-
servicesanticipatedacrossregionsandourchoicetorepresentallfacilities(totalversus
operational).Forinstance,intypicallower-levelfacilitiessuchasdispensaries,theremaybeonly
1-2skilledbirthattendantsonstaffsuchthatreleasingstafftoattendacentralizedtrainingat
thedistricthospitalcanbedifficultinconjunctionwithcontinueddeliveryofclinicalcare.
Additionally,HBB-trainedproviderscanberotatedtonewdepartments,andnewstaffarehired.
Theseresultinadilutionofthetrainingcoverage.
Thisstudydidnotattempttoaccountforprogramplanningandstart-upcosts,suchasthe
trainingoftheMOHSWmastertrainerswhoconductedtheregionaltrainingsessions.MOHSW
leadershipcontributionswerealsonotincluded.Furthermore,scale-upanalysisisbasedupon
thenumberofnationalhealthfacilitiesinformationfromtheTanzanianMOHSW.Wechoseto
usetotalfacilities,asopposedtooperationalfacilities,toprovideaconservativeestimatefor
nationalrollout.

21
Intheabsenceofaformalcost-effectivenessanalysisatscale,andrandomizedcontroltrialdata
todemonstratetheinterventioneffectsizeinthiscontext,itischallengingtoreliablycompare
thecostsandimpactstosimilarneonatalcareprograms.Additionally,therearenoreliable
baselinemeasurementsofmortalityconcurrentwiththesecostmeasurements.Dataare
neededonmortalityindicatorsassociatedwithHBBimplementationatscale,suchasnumberof
livessavedornumberofresuscitationsconducted,withoutwhichitisnotpossibletoestimate
thecostperneonataldeathavertedordisability-adjustedlifeyeargained.
Sustainability
MaintenancecostsarisingfromsustainingtheHBBprogramfollowinginitialrollouthavebeen
previouslyestimatedtobesignificantlylowerthaninitialrolloutcosts–approximatelyone-third
thecostsofimplementationperyear[6].Theconsiderationofmaintenancecostshereis
essentialtoensurefurtheruptakeandretentionofskillsovertime,throughactivitiessuchas
refreshertrainings.Theactivity-basedcostingmethodologyallowsforefficentcalculationsof
validmaintenancecosts,however,someassumptionsarenecessaryforconsideringthe
proportionofadministrationandequipmentreplacementcosting.These,unfortunately,are
untestableassumptionsbutareinkeepingwithexpectationsestablishedfrompriorstudies[5-
12].
OurcostdatademonstratethefinancialfeasibilityofHBBregionalandnationalexpansionand
maintenanceoveroneandfiveyearsinlow-incomecountrysettings.Forcontextualizationof
themagnitudeofthecosts,weconsiderthatthelatestnationalhealthbudgetinTanzaniawas
approximately$800million[27].Therefore,countrywideimplantationofa$4millionHBB

22
programwouldaccountforroughlyonehalfpercentofthecountry’sannualhealthsystem
budget.Givenanapproximateprojected$2millioncostforone-yearprogrammaintenanceand
$6millioncostforfive-yearprogrammaintenance,thecountrywideexpansionandsustenance
ofsuchnewbornstandardofcarepracticesishighlycost-feasible.
Furthereffortstoquantifythecostsandimpactsofintegratedpackagesofneonatalcare
involvingessentialcarearecalledfor.Althoughestimationoftheseisbeyondthescopeofthis
work,thiscostanalysisdoesprovideausefulframeworkforpolicymakerstoestimatethe
potentialcostsinvovledinexpandingprogramsofnewborncare,basedonsimilarmodelsof
trainingasHBBisdesignedtobeeasilyammendedwithadditionaltrainingelementsandis
intendedtoprovideaplatformfortrainingthatenhancesasystems-approachtodeliveryofcare
[3-15].
Conclusion
NationalrolloutoftheHBBprograminTanzaniaisfinanciallyfeasible.Stakeholderscanusethe
currentstudyasaguideforcostingouttheexpansionofthispotentiallylife-savingneonatal
resuscitationprograminotherresource-limitedsettings.Formalcost-effectivenessanalysesare
warrantedtoassesspotentialcost-savingsperneonataldeathaverted.
Declarations
Listofabbreviations
HBB–HelpingBabiesBreathe;OSCE–objectivestructuredclinicalexamination;USAID–United
StatesAgencyforInternationalDevelopment;UNICEF–UnitedNationsChildren’sFund;ENC–
EssentialNewbornCare;MOHSW–MinistryofHealthandSocialWork;ABC–activity-based
costing.

23
EthicsapprovalandconsenttoparticipateThisstudywasapprovedbytheinstitutionalreviewboardatMassachusettsGeneralHospital(Boston,MA,USA),theNationalInstituteforMedicalResearch(DaresSalaam,Tanzania),andtheMinistryofHealthandSocialWelfare(DaresSalaam,Tanzania).Alldatawerede-identified.AvailabilityofdataandmaterialsAllstudydatahavebeenmadeavailablewithinthetablesofthemanuscript.
Competinginterests
Theauthorsdeclarenottohaveanyfinancialandnon-financialcompetinginterests.
FundingTheChildren’sInvestmentFundFoundation,London,UnitedKingdomAuthors'contributionsSCdesignedthestudyandundertooktheanalysis.SCdrafted,reviewedandrevisedthe
manuscript.LKrevisedtheregionalanalysistoincorporateallavailabledataandsupportedthe
overallanalysisandrevisions.AKK,ARM,KGI,WM,DB,ET,GMandMAdesignedthedata
collectionandoversawandconductedthedatacollectionprocedureswithinnon-governmental
andministryofhealthpartnerorganizations.AMprovidedsupporttooverallfundingand
administrationofthestudyfromwithinourfundingpartnerorganization.BNoversawall
aspectsofthestudy,criticallyreviewedthemanuscript,andapprovedthefinalmanuscriptas
submitted.Allauthorsapprovedthefinalmanuscriptassubmittedandagreedtobeaccountable
forallaspectsofthework.
Acknowledgements

24
Wewouldliketothankourfundersfortheirsupportofthisstudy,ourimplementingpartners
Jhpiego,andtheMinistryofHealthandSocialWelfareofTanzaniafortheirleadershipand
partnershipinimprovingneonatalhealthservices.
References
1. UNICEF,WHO,TheWorldBank,UnitedNations.Levelsandtrendsinchildmortality:report
2013.NewYork,USA:UNICEF,2013.
2. LawnJE,BlencoweH,OzaS,etal.,forTheLancetEveryNewbornStudyGroup.Progress,
priorities,andpotentialbeyondsurvival.Lancet2014.
3. TomekS,Newbornresuscitation:thegoldenminute.EMSWorld.2011Jun;40(6):45-50.
4. AmericanAcademyofPediatrics.HBBImplementationGuide.2010.Accessed6August
2015.
<http://www.helpingbabiesbreathe.org/docs/IG_pdfs/Impl.%20guide%2022%20december%
202011.pdf>
5. SabinLL,KnappAB,MacLeodWB,Phiri-MazalaG,KasimbaJ,etal.(2012)CostsandCost-
EffectivenessofTrainingTraditionalBirthAttendantstoReduceNeonatalMortalityinthe
LufwanyamaNeonatalSurvivalStudy(LUNESP).PLoSONE7(4):e35560.
6. VossiusC,LottoE,LyangaS,MdumaE,MsemoG,PerlmanJ,etal.Cost-effectivenessofthe
"HelpingBabiesBreathe"programinamissionaryhospitalinruralTanzania.PLoSOne.2014
Jul9;9(7):e102080.
7. MsemoG,MassaweA,MmbandoD,RusibamayilaN,ManjiK,KidantoHL,etal.Newborn
mortalityandfreshstillbirthratesinTanzaniaafterHelpingBabiesBreathetraining.
Pediatrics.2013Feb;131(2):e353-60
8. GoudarSS,SomannavarMS,ClarkR,LockyerJM,RevankarAP,FidlerHM,etal.Stillbirthand

25
newbornmortalityinIndiaafterHelpingBabiesBreathetraining.Pediatrics.2013;
131(2):e344-e52.
9. ManasyanA,ChombaE,McClureEM,etal.Cost-effectivenessofEssentialNewbornCare
Traininginurbanfirst-levelfacilities.Pediatrics.2011;127(5):e1176-e1181.
10. CarloWA,McClureEM,ChombaE,etal.Newborn-caretrainingformidwivesandneonatal
andperinatalmortalityratesinadevelopingcountry.Pediatrics.2010;126(5):e1064–e1071.
11. CarloWA,GoudarSS,JehanI,etal.;FirstBreathStudyGroup.Highmortalityratesofvery
lowbirthweightinfantsindevelopingcountriesdespitetraining.Pediatrics.2010;126(5):
e1072–e1080.
12. CarloWA,GoudarSS,JehanI,etal.;FirstBreathStudyGroup.Newborn-caretrainingand
perinatalmortalityindevelopingcountries.NEnglJMed.2010;362(7):614–623.
13. BangA,BelladR,GisoreP,etal.ImplementationandevaluationoftheHelpingBabies
Breathecurriculuminthreeresourcelimitedsettings:doesHelpingBabiesBreathesave
lives?Astudyprotocol.BMCPregnancyandChildbirth.2014;14:116.
14. BangAT,BangRA,BaituleSB,ReddyHM,DeshmukhMD:Managementofbirthasphyxiain
homedeliveriesinruralGadchiroli:theeffectoftwotypesofbirthattendantsandof
resuscitationwithmouth-to-mouth,tube-maskorbag-mask.JPerinatol.2005;25(Suppl
1):S82–S91.
15. CarnellMA,DoughertyL,PomeroyAM,KarimA,MekonnenYM,MulliganBE.Effectiveness
ofscalingupthe‘ThreePillars’approachtoacceleratingMDG4progressinEthiopia.J
HealthPopulNutr.2014Dec;32(4):549-563.
16. ReismanJ,MartineauN,KairukiA,MponziV,MedaAR,IsangulaKG,etal.Developmentand
validationofatoolforassessingnewbornresuscitationskillsamonghealthcareproviders
26
trainedintheHelpingBabiesBreatheprograminTanzania.InternationalJournalof
GynecologyandObstetrics(inpress).
17. LittleG,NiermeyerS,SinghalN,LawnJ,KeenanW.Neonatalresuscitation:Aglobal
challenge.Pediatrics.2010;126(5):e1259-e60.
18. NationalBureauofStatistics(NBS)andOfficeofChiefGovernmentStatistician(OCGS),
Zanzibar.2013.2012PopulationandHousingCensus:PopulationDistributionby
AdministrativeUnits;KeyFindings.DaresSalaam,Tanzania:NBSandOCGS.
19. TheUnitedRepublicofTanzania,MinistryofHealthandSocialWelfare.“OnlineHealth
FacilityRegistry.”Accessed6August2015.
<http://ehealth.go.tz/mfl/index.php?page=report_geo_count>
20. LaerdalMedical.NeoNatalie.Accessed6August2015.
<http://www.laerdalglobalhealth.com/doc/2528/NeoNatalie>
21. MogyorosyZ,SmithP.Themainmethodologicalissuesincostinghealthcareservices:a
literaturereview.UK:CentreforHealthEconomics,UniversityofYork;2005.
22. ContehL.Costandunitcostcalculationsusingstep-downaccounting.HealthPolicyPlan.
2004;19:127–135.
23. Tan-TorresEdejerT,BaltussenR,AdamT,etal.(eds)2003.Makingchoicesinhealth:WHO
guidetocost-effectivenessanalysis.Geneva:WorldHealthOrganization.
24. DrummondMF,SculpherMJ,TorranceGW,O’BrienBJ,StoddartGL,editors.Methodsfor
theeconomicevaluationofhealthcareprogrammes.3rdedition.OxfordUniversityPress.
2005.
25. FiedlerJL,VillalobosCA,DeMattosAC. Anactivity-basedcostanalysisoftheHonduras
Community-Based,IntegratedChildCare(AIN-C)programme.HealthPolicyandPlanning.
2008;23:408–427.

27
26. PATH.Breakthroughinnovationsthatcansavewomenandchildrennow.Accessed6August
2015.<https://unicefstories.files.wordpress.com/2013/09/unga-innovations2015_final-
091213.pdf>
27. TheUnitedRepublicofTanzania,MinistryofFinance.GovernmentbudgetforFinancialYear
2014/15:Citizens’budgetedition.Accessed6August2015.<http://www.policyforum-
tz.org/sites/default/files/citizensbudget201415.pdf>

28
Table1.Cost-activitiesofnationalHBBtrainingprogramimplementationandfollow-up
PERSONNELANDCAPITALCOSTS Comments
Cost-activitycenterA:
Centraladministration
Leadership
Implementation
Monitoring
Administration
Officesupport
Internationalhires,in-countryleadership
Inclusiveofaudit,finance,communications,human
resources,operations,procurement,programstaff,and
transportcosts
Officespace,supplies
PROGRAM-SPECIFICCOSTS
Cost-activitycenterB:
Initialtraining
Trainingofbirthattendants
DistributionofHBBequipment
Ensuringcompetence(OSCEs)
MinistryofHealthandimplementationpartnercosts
Trainerandtraineeperdiems
LaerdalNeoNataliemannequin,andmultiplesetsofHBB
newbornresuscitationequipment(e.g.,reusablebag-mask
device,reusablesuctiondevice,etc.)[20]
Trainingmaterials(e.g.,HBBlearner’smanuals,HBBwall
poster,HBBflipchart,etc.)
Printedmaterial
Administration(inclusiveofvenuecosts,associated
accommodation,transportation)
Cost-activitycenterC:
Follow-upvisits
Sustainingtraining
Ensuringskillretention(OSCEs)
VerifyingpresenceofHBB
equipment
MinistryofHealthandimplementationpartnercosts
Providerandtrainerperdiems
Printedmaterial
Administration(inclusiveofassociatedaccommodation,
transportation)

29
Table2.MbeyaRegionHBBtrainingprogramactivity-basedcosts
Activitycostcenters CostinUSD (Percent)
Cost-centerA:Centraladministration
Personnel
Leadership
Internationalhires 446 (0.2)
In-countryleadership 2,201 (1.1)
Implementationstaff 16,174 (8.0)
Monitoringteam 2,281 (1.1)
Administrativestaff
Auditandfinance 14,961 (7.4)
Communications 3,157 (1.6)
Humanresources 5,409 (2.7)
Operationsdepartment 7,156 (3.5)
Procurementdepartment 3,693 (1.8)
Programstaff 2,358 (1.2)
Transportdepartment 2,115 (1.0)
Benefits 13,408 (6.6)
Officespaceandsupplies
Officespacerent 747 (0.4)
Utilities 150 (0.1)
Othercontractualcosts* 598 (0.3)
Officesupplies** 302 (0.1)
Total 75,156 (37.2)
Cost-centerB:InitialHBBtraining
Personnel
Perdiemfortrainers 9,694 (4.8)
Perdiemfortrainees 32,066 (15.9)
Perdiemforimplementingpartner 1,725 (0.9)
Perdiemforministryofhealthstaff 203 (0.1)

30
Equipment[20]
Mannequins(70USDeach) 24,104 (11.9)
Bag-maskdevices(15USDeach) 10,407 (5.1)
Penguinsuckers(3USDeach) 2,848 (1.4)
Learnerworkbooks 13 (0.0)
Trainingforms(registration,OSCE) 505 (0.2)
Other(communication,stationary) 44 (0.0)
Venue 1,569 (0.8)
Food 5,648 (2.8)
Transportation 1,134 (0.6)
Housing 1,465 (0.7)
Total 91,425 (45.2)
Cost-centerC:Follow-uptraining
Personnel
Perdiemfortrainers 13,857 (6.9)
Perdiemforproviders 369 (0.2)
Perdiemforimplementingpartner 2,744 (1.4)
Perdiemforministryofhealthstaff 450 (0.2)
Supplies(photocopying) 253 (0.1)
Transportation 14,111 (7.0)
Housing 3,875 (1.9)
Total 35,659 (17.6)
TotalCostsforMbeyaRegion 202,240 (100.0)
*Othercontractualcostsincludedeliveryservices,wasteremoval,contractcleaning,etc.
**Officesuppliesincludecomputersoftware,printingandphotocopying,furniture,etc.

31
Table3.Sensitivityanalysis:variationincostperfacilityandforallTanzaniarolloutgiven
varianceinselectedcost-influentialvariables
Program-specific:distance
Program-specific:
equipment
Centraladministration
Perfacility AllTanzania
MbeyaRegion $88,908 $38,174 $75,156 $602
Nationalestimates* 1,647,444 707,355 1,392,623 602 3,747,422
Initialtrainingduration
- - - -
+1day - - - 758 4,717,826
+2days - - - 914 5,688,230
Economicvariation:
-5% 1,565,072 671,987 1,322,992 572 3,560,051
-3% 1,598,021 686,134 1,350,844 584 3,634,999
+3% 1,696,867 728,576 1,434,402 620 3,859,845

32
+5% 1,729,816 742,723 1,462,254 632 3,934,793
Populationcoverage:
65% 1,296,310 556,590 1,095,801 602 2,948,702
75% 1,495,824 642,255 1,264,455 602 3,402,534
90% 1,794,830 770,637 1,517,212 602 4,082,680
95% 1,894,587 813,470 1,601,539 602 4,309,595
Distancefromcentraladministration:
-10% 1,482,700 707,355 1,392,623 575 3,582,678
-5% 1,565,072 707,355 1,392,623 589 3,665,050
+5% 1,729,816 707,355 1,392,623 615 3,829,794
+10% 1,812,188 707,355 1,392,623 628 3,912,166
Equipmentcosts:
-20% 1,647,444 565,884 1,392,623 579 3,605,951
-10% 1,647,444 636,620 1,392,623 591 3,676,687
+10% 1,647,444 778,091 1,392,623 613 3,818,158
+20% 1,647,444 848,826 1,392,623 625 3,888,893*Basedona1-dayinitialtrainingduration
33
Table4.Maintenancecost-analysis(USD)
MbeyaRegion All
mainlandTanzania1
Costsof
refreshertraining
Centraladministration2
Equipmentreplacement3
Perfacility
35,659 15,032 7,584 173 1079,821
Maintenancecosts
1year4 71,318 30.064 7,584 325 2,019,115
5years5 213,954 60,128 30,336 907 5,640,7941Basedon6,226facilitiesacrossallmainlandTanzaniaat82.6%coverageoffacilities2A20%proportionofinitialcentraladministrationcostswereincludedinconsiderationsofprogrammaintenancecostsforrepeatedrefreshertrainings3A20%proportionofinitialequipmentcostswereincludedforpotentialequipmentreplacementneededineachsubsequentyearoftheprogram4Basedonrepeatedrefreshertrainingsatsix-monthintervalstosustainskillsinthefirstyear5Basedonannualrepeatrefreshertrainingstosustainskillsthereafter





























