Embed Size (px)
Citation preview

ACTA O P H T H A L M O L O G I C A 68 (1990) Supplementurn195
Correlations between visual acuity, grating acuity and contrast sensitivity in amblyopia
Pentti U. Koskela and Hannu 1. Alanko
Department of Ophthalmology (Head: Leila Laatikainen), University of Oulu. Oulu, Finland
Abstract. In order to obtain a large set of data to analyse correlations between different measures of vi- sion in amblyopia, we pooled the information on all 114 amblyopic patients contained in our earlier series (49 strabismic, 28 anisometropic and 37 combined strabis- miclanisometropic children).
It was found that strabismus influenced visual acuity more than did anisometropia, but anisometropia influ- enced contrast sensitivity more than strabismus.
The correlation coefficients between visual acuity and contrast sensitivity and between grating acuity and con- trast sensitivity were lowest at 1 c/deg and highest at 13 ddeg. The correlation between grating acuity and con- trast sensitivity was slightly better than between visual acuity and contrast sensitivity. The highest correlation coefficients were found in cases of combined strabismic/ anisometropic amblyopia and the lowest in anisome- tropic amblyopia, which was not expected on the basis of some earlier reports in the literature. The best corre- lation between visual acuity and grating acuity was in the cases of combined amblyopia.
Key words: visual acuity - grating acuity - contrast sensitivity - amblyopia - anisopmetropia - strabis- mus.
It is not possible to ascertain the contrast sensitivity function on the basis of visual acuity in an amblyopic eye (Hess & Howell 1977), and grating acuity is often much better than optotype acuity in amblyopia (Gstalder & Green 1971). Sjostrand (1981) sugests that the contrast sensitivity function cannot be pre- dicted from visual acuity measurements in amblyopic eyes due to strabismus, whereas a rough correaltion is observed in anisometropia. On the other hand, Rogers et al. (1987), for example, do not report any
large differences between contrast sensitivity func- tions in strabismic and anisometropic amblyopia.
The series of patients discussed in the lierature are generally rather small, and thus the aim of this retro- spective survey was to collect together all the am- blyopic patients from our earlier series (Koskela 1986 a,b, Koskela & Hyvarinen 1986 a, b) and analyse the correlations between visual acuity, grating acuity and contrast sensitivity in strabismic, anisometropic and combined amblyopia.
Patients and methods
The total number of amblyopic subjects was 114. These were consecutive cases referred to the clinic either for CAM treatment (33) or pleoptic treatment (81). They comprised 50 girls and 64 boys, with a mean age of 9 years (5-14 years).
Amblyopia was classified as anisometropic if ei- ther the spherical or the cylindrical difference in refraction between the two eyes was 1 D or more, and strabismic if any form of tropia was found irrespec- tive of the size of the angle. The patients could thus be divided into three types of amblyopia as follows: anisometropic amblyopia 28, strabismic amblyopia 49, and combined anisometropic and strabismic am- blyopia 37.
Visual acuity measured with an internally illumi- nated E chart (luminance 650 cd/m2, contrast 90%) on which the relative space between the letters be- comes gradually greater towards the lines of smaller size.
Grating acuity was measured in 38 cases using vertical gratings and the same equipment as in the contrast sensitivity measurement, from a distance of 5 m (Koskela 1986). In 76 cases grating acuity was
91

extrapolated from the contrast sensitivity function curve.
Contrast sensitivity was measured using a televi- sion screen and vertical sinusoidal gratings, the aver- age luminance being 30 cd/m2 and the maximum contrast 75%. Every measurement was started below the threshold, which was determined as the mean of four measurements (Koskela 1986). Three spatial frequencies were studied, 1,6 and 13 cldeg. These were chosen for the following reasons: 1 cldeg is the lowest frequency measured, 6 cldeg represents the medium range near the peak sensitivity, and 13 cldeg was the highest frequency which was less than the cut-off value for the most amblyopic eyes.
The statistical analyses employed a one-way analy-
Table 1. Mean values for visual acuity, grating acuity and contrast sensitiv- ity.
~
Visual Grating Contrast sensitivity acuity acuity 1 ddeg 6 ddeg 13 ddeg
Dom. eye 1.2 33.9 56.5 112.7 37.5 Mean n=114 0.19 5.4 13.6 27.4 15.1 SD AmbLeye 0.35 20.4 47.9 48.8 11.8 Mean n=114 0.17 6.3 16.1 27.9 12.4 SD Anisom. ambl. 0.44 20.9 49.3 43.4 8.9 Mean N=20 0.18 5.2 11.0 22.9 6.9 SD Strab. ambl 0.34 22.3 50.6 58.9 18.1 Mean n=49 0.16 6.6 15.8 30.6 15.2 SD Combin. ambl 0.29 17.5 43.4 39.6 5.6 Mean n=37 0.17 5.8 18.8 23.5 6.4 SD
Table 2.
Correlations between visual acuity and contrast sensitivity (V. A , ) and between grating acuity and contrast sensitivity (G. A, )
1 ddeg 6 ddeg 13 cldeg
Domeye 0.23 n=114 0.27 Ambl . eye 0.33 n=114 0.39 Anisom.ambl. -0.20 n=28 -0.04 Strab.ambl 0.21 n=49 0.21 Combin.ambl. 0.68 n=37 0.69
0.33 0.43 0.45 0.71 0.19 0.59 0.50 0.69 0.75 0.77
0.38 V.A. 0.49. G.A. 0.45 V.A. 0.73 G.A. 0.43 V.A. 0.71 G.A. 0.52 V.A. 0.73 G.A. 0.76 V.A. 0.83 G.A.
sis of variance, Student’s unpaired t-test and Pear- son’s linear correlation coefficients.
Results
The mean values and standard deviations for visual acuity, grating acuity and contrast sensitivity before treatment are shown in Table 1. All the mean values are lowest in the combined amblyopia cases. Apart from visual acuity, the highest values are found in strabismic amblyopia. One-way analysis of variance showed the visual acuity differences between the three groups to be statistically significant (p < 0.01), and paired comparison using the t-test indicated that strabismus influenced visual acuity significantly more than did anisometropia. The contrast sensitiv- ity differences between the three amblyopia groups weere statistically significant at 6 cldeg (p < 0.01) and highly significant at 13 cldeg (p < O.OOl), but not significant at 1 cldeg. Comparison between pairs of groups show anisometropia to be connected with lower contrast sensitivity, the difference being statis- tically significant in the t-test at 6 cldeg and highly significant at 13 cldeg, but again not significant at 1 cldeg.
The correlation coefficients between visual acuity and contrast sensitivity and between grating acuity and contrast sensitivity are shown in Table 2. As a general observation, it can be said that the correla- tion coefficients are lowest at 1 cldeg and highest at 13 cldeg. The correlation between grating acuity and contrast sensitivity is slightly better than that be- tween visual acuity and contrast sensitivity. The highest coefficients are found in the group with com- bined amblyopia and the lowest in that with aniso-
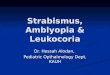
Figure I : Relationship between visual acuity and contrast sensi- tivity at 6 cldeg in the three amblyopia groups.
92

metropic amblyopia. the relationship between visual acuity and contrast sensitivity at 6 c/deg in the three amblyopia groups is shown graphically in Fig. 1.
the correlations between visual acuity and grating acuity are shown in Table 3. The best correlation is observed in the group with combined amblyopia.
Discussion
The assessment of both contrast sensitivity and grat- ing acuity in this series is based on the same kind of grating detection task, whereas recognition of an optotype represents a different kind of psychophys- ical test (Mayer 1986). It is thus understandable that the correlations between grating acuity and contrast sensitivity are better than those between visual acuity and contrast sensitivity.
Since visual acuity, grating acuity and contrast sen- sitivity at high spatial frequencies depict subject’s ability to process detailed visual information, it is not surprising that the correlation between visual acuity or grating acuity and contrast sensitivity improves towards higher spatial frequencies.
the better correlation observed here between vi- sual acuity and contrast sensitivity in strabismic am- blyopia than in anisometropic amblyopia is not in agreement with the results of Sjostrand (1981) or Abrahamsson & Sjostrand (1988). The reason for this is unclear. The correlation would be better if amblyopia were based on both strabismus and aniso- metropia, and that between visual acuity and grating acuity would similarly be better if both factors, stra- bismus and anisometropia, were present.
The results show that, strabismus has more influ- ence on visual acuity and anisometropia on contrast sensitivity at intermediate and high spatial frequen- cies. This points to different amblyopiogenic mecha- nisms for strabismus and anisometropia. Sjostrand (1981) and Campos et.al. (1984) suggest that aniso- metropia influences contrast sensitivity over the whole frequency range and strabismus mainly at high spatial frequencies. This difference was not apparent at 1 c/deg in our material. Abnormal binocular inter- action with incorrect sptial coding is typical of stra- bismus, while anisometropia is characterised by vi- sual deprivation (von Noorden 1985). It may be thought that the detrimental influences are better balanced in combined amblyopia, and thus the corre- lation between the different measures of vision is better in these cases.
Table 3.
Correlations between visual acuity and grating acuity.
Domin. eyes 0.47 Amblyopic eyes 0.56 Anisometropic ambl. 0.44 Strabismic ambl. 0.52 Combined ambl. 0.72
References
Abrahamsson M & Sjostrand J (1988): Contrast sensitivity and acuity relationship in strabismic and anisometropic amblyo- pia. Br. J Ophthalmol72:44-49.
Campos EC, Prampolini ML & Gulli R (1984): Contrast sensi- tivity differences between strabismic and anisometropic am- blyopia: objective correlate by means of visual evoked re- sponses. Doc Ophthalmol58:45-50.
Gstalder RJ - Green DG (1971): Laser interferometric acuity in amblyopia. J Pediatr Ophthalmol8:251-256.
Hess RF & Howell ER (1977): the threshold contrast sensitivity function in strabismic amblyopia: evidence for a two type classification. Vision Res 17:1049-1055.
Koskela PU (1986a): Contrast sensitivity in amblyopia. I. Changes during CAM treatment. Acta Ophthalmol (Copenh)
Koskela PU (1986b): conrast sensitivity in amblyopia. 11. Changes during pleoptic treatment. Acta Ophthalmol (Co- penh) 64563-569.
Koskela PU & Huvarinen L (1986a): Contrast sensitivity in amblyopia 111. Effect of occlusion. Acta Ophthalmol (Co- penh) 64:386-390
Koskela PU & Hyvarinen L (1986b): Contrast sensitivity in amblyopia IV. Assessment of vision using vertical and hori- zontal gratings and optotypes at different contrast levels. Acta Ophthalmol (Copenh) 64570-577.
von Noorden GK (1985): Amblyopia: A multidisciplinary ap- proach. Proctor Lecture. Invest Ophthalmol Vis Sci 26:1704- 1716.
Rogers GL, Bremer DL & Leguire LE (1987): the contrast sensitivity function and childhood amblyopia. Am J Ophthal- mol 10454-68.
Sjostrand J (1981): Contrast sensitivity in children with strabis- mic and anisometropic amblyopia. A study of the effect of treatment. Acta Ophthalmol (Copenh) 59:25-33.
64:344-351.
Author’s address: Pentti U. Koskela Department of Ophthalmology, University of Oulu
SF-90220 Oulu, Finland.
93