Embed Size (px)
Citation preview

Seediscussions,stats,andauthorprofilesforthispublicationat:http://www.researchgate.net/publication/42254932
Correlationsbetweenneurophysiological,behavioral,andcognitivefunctioninRettsyndrome
ARTICLEinEPILEPSY&BEHAVIOR·MARCH2010
ImpactFactor:2.06·DOI:10.1016/j.yebeh.2010.01.024·Source:PubMed
CITATIONS
7
DOWNLOADS
46
VIEWS
144
7AUTHORS,INCLUDING:
RosaAngelaFabio
UniversitàdegliStudidiMessina
146PUBLICATIONS83CITATIONS
SEEPROFILE
AlessandroAntonietti
CatholicUniversityoftheSacredHeart
130PUBLICATIONS441CITATIONS
SEEPROFILE
SilviaMaggiolini
CatholicUniversityoftheSacredHeart
4PUBLICATIONS8CITATIONS
SEEPROFILE
MariaPaolaCanevini
UniversityofMilan
105PUBLICATIONS1,445CITATIONS
SEEPROFILE
Availablefrom:RosaAngelaFabio
Retrievedon:22July2015

Epilepsy & Behavior 17 (2010) 489–496
Contents lists available at ScienceDirect
Epilepsy & Behavior
journal homepage: www.elsevier .com/locate /yebeh
Correlations between neurophysiological, behavioral, and cognitive functionin Rett syndrome
Aglaia Vignoli a,*, Rosa Angela Fabio b, Francesca La Briola a, Samantha Giannatiempo c,Alessandro Antonietti c, Silvia Maggiolini d, Maria Paola Canevini a
a Centro Epilessia, Azienda Ospedaliera San Paolo, Università degli Studi di Milano, Milan, Italyb Dipartimento di Psicologia e Scienze dell’Educazione, Università di Messina, Messina, Italyc Dipartimento di Psicologia, Università Cattolica Sacro Cuore, Milan, Italyd Scienze dell’Educazione, Università Cattolica Sacro Cuore, Milan, Italy
a r t i c l e i n f o
Article history:Received 13 November 2009Revised 21 January 2010Accepted 24 January 2010Available online 16 March 2010
Keywords:Rett syndromeEpilepsyElectroencephalographyCognitive performanceEye tracking
1525-5050/$ - see front matter � 2010 Elsevier Inc. Adoi:10.1016/j.yebeh.2010.01.024
* Corresponding author. Address: Centro Epilessia, Odegli Studi di Milano, Via di Rudinì, 8, 20142 Milan, I
E-mail address: [email protected] (A. V
a b s t r a c t
Rett syndrome, a neurodevelopmental disorder affecting mainly females, is caused by a mutation of theMeCP2 gene. Girls with Rett syndrome manifest diverse behavioral and cognitive phenotypes, and thereasons for this variability remain unknown. In addition, girls with Rett syndrome often have epilepticseizures and abnormal EEGs, the characteristics of which differ with the patient. The aim of the studywas to verify if neurophysiological and epileptological characteristics could be correlated with cognitivemeasures, obtained using eye tracker technology, and behavioral scores (Vineland Adaptive BehaviorScales and Rett Assessment Rating Scale) in 18 patients with Rett syndrome (mean age 13.7 years) at clin-ical stages III and IV. Age at epilepsy onset and seizure frequency were strictly correlated with neuropsy-chological outcome, as were EEG stage and distribution of paroxysmal abnormalities. Our findingsdemonstrate that neurophysiological features should be considered prognostic of cognitive and behav-ioral outcome in the clinical management of Rett syndrome.
� 2010 Elsevier Inc. All rights reserved.
1. Introduction
Rett syndrome (RS) is an X-linked dominant neurodevelopmen-tal disorder, affecting almost exclusively females, with an inci-dence ranging from 1/10,000 to 1/15,000. Clinical diagnosis ofthe classic form relies on a battery of obligatory criteria such asnormal pre-/perinatal period and normal head circumference atbirth, followed by loss of acquired skills such as communicationand purposeful hand use associated with onset of stereotypies.Additional characteristic features include deceleration of headgrowth, gait posture ataxia, breathing dysfunction, and epilepsy[1]. About 80% of females with classic RS and 25 to 75% of thosewith variant forms, depending on the criteria used for diagnosisand size and age of sampled population, have mutations in MeCP2(methyl CpG binding protein2), a transcriptional repressor genelocated on Xq28 [2].
Several studies have reported a relationship between somecharacteristics of the phenotype and the genotype, but patientswith the same MeCP2 mutation can vary greatly in phenotype, sothere may be other mechanisms modulating the clinical presenta-
ll rights reserved.
spedale San Paolo, Universitàtaly. Fax: +39 02 50323159.ignoli).
tion [3]. With respect to neurodevelopmental and behavioral phe-notypes, girls affected by RS vary, and the reason(s) for thedifferences is not well understood. Moreover, the clinical and elec-troencephalographic picture of girls with RS follows differentstages correlated with age [4,5], and electroencephalographic pat-terns vary not only between patients, but also between stages ofthe disease [6,7].
Epilepsy is very frequent in patients with RS, occurring in about80% of subjects; seizures are often difficult to treat, and in severalpatients, antiepileptic drug polytherapy is needed [8]. It is wellknown that refractory epileptic seizures can be associated withneuropsychological impairment involving different cognitive func-tions, such as memory, attention, and mental speed [9]. The aim ofour study was to delineate if and how neurological and neuro-physiological impairment reflects behavioral and neuropsycholog-ical functions, to identify prognostic factors that could beimportant in the clinical management of girls with RS.
2. Methods
2.1. Subjects
Eighteen girls with RS (mean age = 13.7 years, range = 7–21)were classified as clinical stage III (characterized by prominent

490 A. Vignoli et al. / Epilepsy & Behavior 17 (2010) 489–496
hand apraxia/dyspraxia, apparently preserved ambulation ability,and some communicative ability, mainly eye contact) or stage IV(late motor deterioration, with progressive loss of ambulation abil-ity), according to the criteria for classic RS of Hagberg et al. [10].Their demographic, developmental, clinical, behavioral, and genet-ic information, collected from all available sources (parent/care-giver reports of past history and current behavior and features,previous clinical reports, and direct observation and examinationof the girls) were entered into a database.
Neurological examination focused on epilepsy characteristics(age at seizure onset, seizure types, course of epilepsy, and antiep-ileptic drugs [AEDs]).
As for MeCP2 mutations, four patients had R306C; two patientseach had R270X, R294X, and R255X; four had C-terminal deletions;and the remaining four had T322A, R106W, R133C, and R168X.
Mean age at epilepsy onset was 5.1 years (range = 1–14); sei-zures were focal in eight patients, tonic in five, generalized to-nic–clonic in three, myoclonic in one, and atonic in one. Seizureswere controlled in four cases and occurred sporadically in five pa-tients. In the other cases, epilepsy was drug resistant, and seizurefrequency was described as monthly in two, weekly in six, and dai-ly in one patient.
Eleven girls were on AED monotherapy and six on polytherapy.In one patient, therapy was discontinued because of seizurefreedom.
Detailed clinical, neurophysiological, behavioral, and geneticfeatures of the patients are listed in Table 1.
2.2. Neurophysiological assessment
Patients underwent EEG video-polygraphic recordings duringwakefulness using a computerized EEG System (Micromed SystemPlus, Micromed s.r.l., Mogliano Veneto, TV, Italy). Scalp electrodeswere positioned according to the International 10/20 system.EMG electrodes were used for deltoid muscles and/or distal mus-cles if tremor was present. Electrocardiograms were obtained andbreathing effort was assessed. Video/EEG recording typically lasted20–30 minutes.
The EEGs were evaluated independently by two of the authors(A.V. and F.L.) and were classified according to Glaze et al. [4] asEEG stage III (moderate to marked slowing of background activitywith dominant theta and delta activity) or IV (no occipital domi-nant rhythm and marked slowing of background activity). More-over, we identified four subgroups of EEG abnormalities (1) thetaslow activity over the frontal and central regions (eight cases)(Fig. 1); (2) frontocentroparietal spikes (eight cases) (Fig. 2); (3)generalized spike and waves (one case) (Fig. 3); (4) diffuse subcon-tinuous spike and waves suggestive of epileptic encephalopathy(one case) (Fig. 4).
2.3. Behavioral measures
2.3.1. Vineland Adaptive Behavior ScalesThe Vineland Adaptive Behavior Scales [11] are designed to sup-
port the diagnosis of intellectual and developmental disabilities.The Scales are organized in four domains: Communication (Recep-tive, Expressive, Written); Daily Living (Personal, Domestic, Com-munity); Socialization (Interpersonal Relationships, Play andLeisure Time, Coping Skills); and Motor Skills (Gross, Fine). Thereliability of the Scales was established as follows: split-half,0.73–0.93 for the Communication domain, 0.83–0.92 for Daily Liv-ing Skills, 0.78–0.94 for Socialization, 0.70–0.95 for Motor Skills,0.84–0.98 for Adaptive Behavior Composite, 0.77–0.88 for Mal-adaptive Behavior (Survey Form) (0.80s and 0.90s for the SurveyForm). Note that interrater reliability coefficients for the Surveyand Expanded forms ranged from 0.62 to 0.75. SEM ranged from
3.4 to 8.2 over the four domains, and from 2.2 to 4.9 for the Adap-tive Behavior Composite, on the Survey Form.
2.3.2. Rett Assessment Rating ScaleThe Rett Assessment Rating Scale (RARS) is used to evaluate
subjects with Rett syndrome [12]. The structure of RARS is similarto that of the Childhood Autism Rating Scale (CARS) [13], GilliamAutism Rating Scale (GARS) [14], and Asperger Syndrome Diagnos-tic Scale (ASDS) [15], well-known instruments devised to assessthe presence/absence of symptoms characterizing the pervasivedevelopmental disorders included in the same nosographic cate-gory as RS [16]. The items in RARS were constructed followingthe diagnostic criteria for RS proposed by DSM-IV-TR [16] and re-cent research and clinical experience. A total of 31 items were gen-erated as representative of the profile of RS. Each item concerns aspecific phenotypic characteristic and describes four increasinglevels of its severity. Each item is provided with a brief glossaryexplaining its meaning in a few words.
Each item is rated on a 4-point scale, where 1 = within normallimits, 2 = infrequent or low abnormality, 3 = frequent or med-ium-high abnormality, and 4 = strong abnormality. Intermediateratings are possible; for example, an answer between 2 3 pointsis rated as 2.5 [12]. For each item, the evaluator circles the numbercorresponding to the best description of the patient. After a patienthas been rated on all 31 items, a Total score is computed by sum-ming the individual ratings. This Total score allows the evaluator toidentify the level of severity of RS, conceptualized as a continuumranging from mild symptoms to heavy deficits.
The RARS was established by a standardization procedure,involving a sample of 220 patients with RS, proving that the instru-ment is statistically valid and reliable. More precisely, normal dis-tribution analyses of the scores were computed, and the meanscores of the scale were similar to the median and the mode. Skew-ness and kurtosis values, calculated for the distribution of the Totalscore, were 0.110 and 0.352, respectively. The distribution wasfound to be normal. Cronbach’s a was used to determine the inter-nal consistency for the whole scale and subscales. Total a was0.912, and the internal consistency of the subscales was high(0.811–0.934).
2.4. Neuropsychological measures
Eye tracker technology was used to measure recognition,matching of pairs (the same), and semantic categorization (thesimilar). Three tasks were designed: (1) response to verbal instruc-tion (look at the dog, etc.); (2) recognition and matching of pairs(look at the one that is the same), and (3) semantic categorization(look at the one that is similar). The images used were of objectsfamiliar to the children, according to their parents. Nine differentpictures were divided into three groups: fruit—apple, orange, andbanana; animals—dog, cat, and horse; and emotions—happy, sad,and angry. Each item was presented for 5 seconds. The parameterwas the length (seconds) of fixation.
An Eyegaze device was used to record the subject’s visual scan-ning response to visual computer screen stimulation. This devicerecords ocular movements such as the location and duration ofocular fixations (i.e., pause of eye movement on an object of inter-est) and saccadic movements (i.e., rapid movements between fixa-tions) (Salvucci and Goldberg [17] movements between fixations).EyeGaze was used in a microcomputer with a 15-in. LCD monitorand a Matrox-like video plaque, which captures the signals sentfrom a video camera equipped with lenses sensitive to high-speedinfrared light. The camera also has a LED that emits low-intensityinfrared light directly on the retina of the person sitting in frontof the monitor. The direction of the gaze is determined accordingto the Pupil Center/Corneal Reflection Method. The software Pas-

Table 1Clinical, EEG and behavioral characteristics of the patients.
Patient Age(years)
Age at epilepsyonset (years)
Seizure type Seizure frequency AED Clinicalstage
EEGstage
EEG pattern VABSa RARS (Totalscore)
MECP2mutation
Totalscore
Communication DailyAbility
Socialization MotorAbility
1 7 4 Myoclonic Sporadic VPA III III Theta activity 118 36 30 41 11 47 C terminaldeletion
2 8 1 Tonic Controlled - III III Theta activity 110 25 29 30 26 64 R133C3 8 4 Tonic Controlled (single
seizure)VPA III III FCP spikes 121 38 24 31 28 49 R306C
4 10 8 Focal Monthly VPA III III Theta activity 89 26 14 26 23 70.5 R294X5 10 3 Atonic Weekly LEV III III FCP spikes 169 32 34 48 55 56.5 C terminal
deletion6 10 4 Focal Sporadic VPA III III Theta activity 84 24 22 31 7 74 R270X7 11 8 Focal Sporadic VPA +
LEVIII III FCP spikes 123 35 28 49 11 64.5 R306C
8 11 2 Focal Weekly VPA IV IV FCP spikes 34 15 1 16 2 85 R168X9 12 6 Focal Weekly TPM +
PBIII III FCP spikes 107 43 17 34 13 66.5 R255X
10 14 6 Tonic Weekly VPA +LTG
IV IV Theta activity 92 31 15 39 7 77 R106W
11 16 3 Generalizedtonic–clonic
Monthly VPA +LTG
III III FCP spikes 113 43 15 36 19 64 R255X
12 16 2 Tonic Weekly LTG IV IV Diffuse spike–waves
134 49 30 35 20 60 T322A
13 17 14 Generalizedtonic–clonic
Controlled (singleseizure)
LTG IV IV Theta activity 113 41 27 12 33 71 R306C
14 18 3 Focal Sporadic VPA +LTG
IV IV FCP spikes 58 20 0 33 5 55 C terminaldeletion
15 19 5 Tonic Weekly VPA IV IV Theta activity 142 49 37 46 10 63.5 R306C16 19 8 Focal Daily CBZ +
ZNSIV IV Multifocal
spikes83 30 8 18 27 66 R294X
17 21 2 Focal Controlled CBZ IV IV FCP spikes 131 34 33 42 22 61.5 C terminaldeletion
18 21 9 Generalizedtonic–clonic
Sporadic LTG IV IV Theta activity 110 24 10 26 50 61.5 R270X
a VABS, Vineland Adaptive Behavior Scales; RARS, Rett Assessment Rating Scale; VPA, valproic acid; LEV, levetiracetam; CBZ, carbamazepine; LTG, lamotrigine; TPM, topiramate; PB, phenobarbital; ZNS, zonisamide; FCP,frontocentroparietal.
A.V
ignoliet
al./Epilepsy&
Behavior17
(2010)489–
496491

Fig. 1. Rhythmic theta activity recorded mainly in the frontal and central regions.
Fig. 2. Asynchronous focal epileptiform activity over both frontotemporal regions.
492 A. Vignoli et al. / Epilepsy & Behavior 17 (2010) 489–496
sive Gaze Tracing (LC Technologies, Inc., Sao Paulo, Brazil) was usedto generate eye found flag, gaze point, pupil diameter during visualscanning, and eyeball position. The girls sat on their parent’s lap,about 20 cm away from the monitor.
2.5. Procedure
Each girl underwent, on the same day and in direct succession,EEG video-polygraphic recording during wakefulness and neuro-

Fig. 3. Generalized spike–wave activity.
Fig. 4. Diffuse subcontinuous paroxysmal discharges in wakefulness.
A. Vignoli et al. / Epilepsy & Behavior 17 (2010) 489–496 493
psychological assessment with the EyeGaze. Behavioral measureswere collected through interviews with parents in a separate ses-sion. Informed consent to participate in the study was obtainedfrom parents.
2.6. Data analysis
Total scores were calculated for each neuropsychological andbehavioral scale and for each subject. Pearson correlations were

494 A. Vignoli et al. / Epilepsy & Behavior 17 (2010) 489–496
used to assess the relationship of each neurophysiological measureto neuropsychological and behavioral scales. The P value was set at<0.05.
3. Results
Results are presented with respect to each of the neurophysio-logical measures presented above.
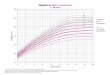
Fig. 6. Correlation between seizure frequency and time of fixation of the correctstimuli in semantic categorization of animals.
3.1. Relationship between age at epilepsy onset andneuropsychological measures
Age at epilepsy onset was positively correlated with the abilityof the girls with RS to reply to verbal instructions, to recognize andmatch pairs, and to semantically categorize animals: r = +0.43,P < 0.05, r = +0.43, P < 0.05, and r = +0.41, P < 0.07, respectively. Inaddition, age at epilepsy onset was positively correlated with theability of the girls with RS to reply to verbal instructions relatedto emotions: r = +0.64, P < 0.01. According to this result, the laterthe onset of seizures, the greater the ability to recognize and asso-ciate animals and emotions (Fig. 5).
Fig. 7. Correlation between EEG stages and time of fixation of the correct stimuli insemantic categorization of animals.
3.2. Relationship between seizure frequency and neuropsychological/behavioral measures
Seizure frequency was negatively correlated with the ability ofthe girls with RS to reply to verbal instructions, to recognize andmatch pairs, and to semantically categorize animals: r = �0.45,P < 0.05, r = �0.54, P < 0.02, and r = �0.47, P < 0.05, respectively(Fig. 6). Also, seizure frequency was negatively correlated withthe Vineland Adaptive Behavior Scales (r = �0.49, P < 0.03). Thus,as seizure frequency increased, Vineland Scales Total scores andability to recognize and associate animals decreased.
3.3. Relationship between EEG stage and neuropsychological/behavioral measures
EEG stage was negatively correlated with the ability of the girlswith RS to reply to verbal instructions, to recognize and matchpairs, and to semantically categorize animals: r = �0.47, P < 0.05,r = �0.43, P < 0.06, and r = �0.47, P < 0.05, respectively (Fig. 7). Inaddition, EEG stage was negatively correlated with Vineland ScalesDaily Living (r = �0.55, P < 0.02) and Total (r = �0.47, P < 0.05)scores. Thus, as EEG stage increased, ability to recognize and asso-ciate animals and Vineland Scales scores decreased.
Fig. 5. Correlation between age at epilepsy onset and time of fixation on correctemotional stimuli.
3.4. Relationship between EEG abnormalities and neuropsychological/behavioral measures
EEG abnormalities were negatively correlated with the ability ofthe girls with RS to reply to verbal instructions, to recognize andmatch pairs, and to semantically categorize fruit: r = �0.469,P < 0.05, r = �0.43, P < 0.06, and r = �0.48, P < 0.05, respectively.Also, EEG abnormalities were negatively correlated with VinelandScales General scores (r = �0.49, P < 0.05) (Fig. 8) and positivelycorrelated with RARS scores (r = 0.64, P < 0.01). Therefore, as EEGabnormalities become more diffuse and multifocal, Vineland Totalscores and the ability to recognize and associate fruit decreasedand RARS scores increased.
4. Discussion
Cognitive performance and behavioral features in persons withRS have scarcely been investigated. Most studies on cognitive func-tions and behavioral features in RS are based on information sup-plied by the parents and professionals who take care of thepatients [18,19]. Few studies have explored cognitive performancedirectly in subjects with RS: in 2006, Baptista et al. [20] demon-strated that intentional gaze is a measurable parameter in girlswith RS and can be used to explore their cognitive performance.More recently, the same authors recommended reevaluation ofthe method because a small group of 10 girls with RS (aged4–12 years) did not manifest recognition of the solicited conceptswithin a fixation time of 4 seconds, even if they argued that thelow age of the sample and the brief fixation span could have inter-fered with the results [21]. Although it is well known that girls

Fig. 8. Correlation between EEG abnormalities and Vineland Adaptive BehaviorScales.
A. Vignoli et al. / Epilepsy & Behavior 17 (2010) 489–496 495
with RS have good visual attention [22], it has recently been shownthat they are able to learn to discriminate complex stimuli [23];however, they have a specific deficit in the ability to attend selec-tively to relevant sources of information while ignoring irrelevantones [24].
To our knowledge this is the first study that has demonstrated astrict correlation between neurophysiological features andneuropsychological impairment, using eye tracker technology, inpatients with RS. The results of our study demonstrate that bothepilepsy features (age at seizure onset and seizure frequency)and EEG characteristics (EEG stage and EEG abnormality pattern)are correlated with the ability to recognize and match pairs andsemantically categorize with respect to animals and behavioralfeatures, as assessed with the Vineland Scales and RARS. The signif-icant ability to recognize and categorize animals, but not the otherobjects proposed in the task, may be explained by these girls’ bet-ter knowledge of animals as compared with fruits and emotions.
Our findings are coherent both within neurophysiologicalparameters and within neuropsychological and behavioral mea-sures (as Vineland Scales scores decrease, RARS scores and eyetracking-derived measures increase).
Regarding the relationship between age at epilepsy onset andcognitive impairment, our study shows that also in girls with RS,epilepsy plays a crucial role in future cognitive performance, asdemonstrated by recent studies supporting the assumption thatthe epileptic process underlying seizures could interfere with cog-nitive development [25]. In addition, in our group of patients withRS, age at seizure onset was inversely correlated with the ability torecognize emotions, as it has been exhaustively shown in patientswith temporal lobe epilepsy, in whom early onset of seizures/epi-lepsy is a key factor leading to severe impairment in recognition ofemotions, involving the temporomedial structures and especiallythe amygdala [26]. This is also supported by the recent finding ina mouse model in which specific deletion of MeCP2 in the basolat-eral amygdala mediated behavioral phenotypes associated with RSimpacting selective forms of learning and memory [27].
With respect to seizure frequency, factors influencing thecourse of epilepsy in RS are not yet well understood. It has beenshown that compared with later onset, early epilepsy onset tendsto be associated with more severe epilepsy, including more seizuretypes, more frequent intractable epilepsy, and status epilepticus[28]. Moreover, children with RS with early developmental prob-lems as well as those with greater motor disability have a higherseizure frequency [29].
Our results in girls with RS with drug-resistant seizures are inaccordance with data from the literature demonstrating that re-peated seizures are associated with increased intellectual impair-ment [9].
Looking at EEG features, we found that as soon as EEG abnor-malities became more diffuse and multifocal, cognitive perfor-mance decreased. This finding could be explained by presumingthat epileptiform EEG discharges could have additional effects oncognitive processes (alertness, mental speed) that might accumu-late over time, resulting in stable effects [30].
Adverse cognitive side effects, mainly on attention, vigilance,memory, and psychomotor speed, have been reported with AEDs[31,32]. All but one patient in our sample were on AEDs, but wecould not find a close relationship between cognitive impairmentand the use of a specific AED.
Our preliminary findings on a limited number of patients indi-cate that in the clinical management of RS, epilepsy characteristicsand EEG patterns suggestive of epileptic encephalopathy should beconsidered prognostic factors in neuropsychological outcome.
Future investigations focused on the correlation betweenneurophysiological features and definite phases of informationprocessing, attention, memory, and logic relationships in RS areneeded to correlate in more depth the exact stage of informationprocessing impairment with neurophysiological features. Findingthat this relationship is strongest in the input phase (i.e., attentionprocess), we could focus on cognitive empowerment in this precisephase. With reference to the severity of the disease and to the dif-ficulty in distinguishing the different phases of information pro-cessing, we know that new paradigms could allow us to attributedisease to one specific phase [23,24].
Acknowledgments
We thank all the RTT patients and their families for their activeparticipation in the study.
References
[1] Hagberg B, Hanefeld F, Percy A, Skjeldal O. An update on clinically appli-cable diagnostic criteria in Rett syndrome. Eur J Pediatr Neurol 2002;6:293–7.
[2] Shahbazian MD, Zoghbi HY. Molecular genetics of Rett syndrome and clinicalspectrum of MECP2 mutations. Curr Opin Neurobiol 2001;14:171–6.
[3] Weaving LS, Ellaway CJ, Gecz J, Christodoulou J. Rett syndrome: clinical reviewand genetic update. J Med Genet 2005;42:1–7.
[4] Glaze DG, Frost Jr JD, Zoghbi HY, Percy AK. Rett’s syndrome: correlation ofelectroencephalographic characteristics with clinical staging. Arch Neurol1987;44:1053–6.
[5] Glaze DG. Neurophysiology of Rett syndrome. Ment Retard Dev Disabil Res Rev2002;8:66–71.
[6] Moser SJ, Weber P, Lütschg J. Rett syndrome: clinical and electrophysiologicaspects. Pediatr Neurol 2007;36:95–100.
[7] Buoni S, Zannolli R, De Felice C, et al. Drug-resistant epilepsy and epilepticphenotype–EEG association in MECP2 mutated Rett syndrome. ClinNeurophysiol 2008;119:2455–8.
[8] Huppke P, Köhler K, Brockmann K, Stettner GM, Gärtner J. Treatment ofepilepsy in Rett syndrome. Eur J Paediatr Neurol 2007;11:10–6.
[9] Aldenkamp AP, Bodde N. Behaviour, cognition and epilepsy. Acta Neurol Scand2005;112(Suppl. 182):19–25.
[10] Hagberg B. Clinical manifestations and stages of Rett syndrome. Ment RetardDev Disabil Res Rev 2002;8:61–5.
[11] Sparrow S, Balla DA, Cicchetti DV. Vineland adaptive behavior scales. CircePines, MN: American Guidance Service; 1984.
[12] Fabio RA, Martinazzoli C, Antonietti A. Costruzione e standardizzazione dellostrumento ‘‘R.A.R.S.” (Rett Assessment Rating Scale). Ciclo Evol Disabil2005;8:257–81.
[13] Schopler E, Reichler RJ, Devellis RF, Daly K. Toward objective classification ofchildhood autism: Childhood Autism Rating Scale (CARS). J Autism Dev Disord1980;10:91–3.
[14] Gilliam JE. Gilliam Autism Rating Scale (GARS). Austin, TX: Pro-Ed; 1995.[15] Myles BS, Bock SJ, Simpson RL. Asperger Syndrome Diagnostic Scale
(ASDS). Austin, TX: Pro-Ed; 2001.[16] Diagnostic and statistical manual of mental disorders, 4th ed., text revision
(DSM-IV-TR). Washington, DC: American Psychiatry Assoc.; 2000.[17] Salvucci DD, Goldberg JH. Identifying fixations and saccades in eye-tracking
protocols. In: Proceedings of the eye tracking research and applicationssymposium. New York: ACM Press; 2000. p. 71–8.
[18] Fontanesi J, Haas RH. Cognitive profile of Rett syndrome. J Child Neurol1988;3:S20–4.

496 A. Vignoli et al. / Epilepsy & Behavior 17 (2010) 489–496
[19] Mount RH, Charman T, Hastings RP, Reilly S, Cass H. The Rett SyndromeBehaviour Questionnaire (RSBQ): refining the behavioural phenotype of Rettsyndrome. J Child Psychol Psychiatry 2002;43(Suppl. 182):1099–110.
[20] Baptista PM, Mercadante MT, Macedo EC, Schwartzman JS. Cognitiveperformance in Rett syndrome girls: a pilot study using eyetrackingtechnology. J Intellect Disabil Res 2006;50:662–6.
[21] De Lima Velloso R, Alves de Araùjo C, Schwartzman JS. Concepts of color,shape, size and position in ten children with Rett syndrome. ArqNeuropsiquiatr 2009;67:50–4.
[22] Perry A, Sarlo-McGravy N, Haddad C. Cognitive and adaptive functioning in 28girls with Rett Syndrome. J Autism Dev Disord 1991;21:551–6.
[23] Fabio RA, Giannatiempo S, Antonietti A, Budden S. The role of stereotypiesin overselectivity process in Rett syndrome. Res Dev Disabil 2009;30:136–45.
[24] Fabio RA, Antonietti A, Castelli I, Marchetti A. Attention and communication inRett syndrome. Res Autism Spectr Disord 2009;3:329–35.
[25] Kaaden S, Helmstaedter C. Age at onset of epilepsy as a determinant ofintellectual impairment in temporal lobe epilepsy. Epilepsy Behav2009;15:213–7.
[26] Meletti S, Benuzzi F, Cantalupo G, Rubboli G, Tassinari CA, Nichelli P. Facialemotion recognition impairment in chronic temporal lobe epilepsy. Epilepsia2009;50:1547–59.
[27] Adachi M, Autry AE, Herb EC, Monteggia LM. MeCP2-mediated transcriptionrepression in the basolateral amygdala may underlie heightened anxiety in amouse model of Rett syndrome. J Neurosci 2009;29:4218–27.
[28] Steffenburg U, Hagberg G, Hagberg B. Epilepsy in a representative series of Rettsyndrome. Acta Paediatr 2001;90:34–9.
[29] Jian L, Nagarajan L, de Klerk N, Ravine D, Christodoulou J, Leonard H. Seizuresin Rett syndrome: an overview from a 1-year calendar study. Eur J PaediatrNeurol 2007;11:310–7.
[30] Aldenkamp AP, Arends J. Effects of epileptiform EEG discharges on cognitivefunction: is the concept of ‘‘transient cognitive impairment” still valid?Epilepsy Behav 2004;5(Suppl. 1):S25–34.
[31] Aldekamp AP. Effects of antiepiletic drugs on cognition. Epilepsia2001;42(Suppl. 1):S46–9.
[32] Meador KJ. Cognitive effects of epilepsy and of antiepileptic medications. In:Wyllie E, editor. The treatment of epilepsy: principles andpractice. Philadelphia: Lippincott Williams & Wilkins; 2001. p. 1215–25.