Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Correlation between the cord vitamin D levels and regulatoryT cells in newborn infants
Ayşegül Güven & Ayşe Ecevit & Oktay Sözer &
Aytül Tarcan & Aylin Tarcan & Namık Özbek
Received: 25 October 2011 /Accepted: 26 January 2012 /Published online: 1 March 2012# Springer-Verlag 2012
Abstract Vitamin D is important for calcium homeostasis,muscle, and bone health. It has also immunomodulatorycapacities in vivo and in vitro. Regulatory T cells (Treg)have been found to suppress a number of T cell-mediatedimmune disorders, including allergic responses and autoim-mune diseases. This study aimed to investigate the correla-tion between 25-hydroxyvitamin D (25(OH)D) levels andthe regulatory T cells in cord blood. The study group iscomprised of 101 full-term newborn infants. Umbilical cord25(OH)D levels and number and percentage of T lympho-cyte, T helper, and Treg cells were measured. Infants were
grouped according to 25-hydroxyvitamin D levels (25(OH)D <12 ng/ml and 25(OH)D >12 ng/ml) (converting factorof 25OHD level into SI unit, 2.6). Severe vitamin D defi-ciency (25(OH)D <12 ng/ml) was observed in 32% of theinfants. There was no significant correlation between 25-hydroxyvitamin D levels and T cell number and percen-tages. There were also no significant differences in whiteblood cell, total lymphocyte count, T helper, and Treg cellpercentage and number between groups. These results sug-gest that the serum level of 25-hydroxyvitamin D is notcrucially involved in the correlation between vitamin Dstatus and T cell regulation in cord blood.
Keywords Vitamin D . Regulatory Tcells . Cord blood .
Newborn
Introduction
Over the last decade, new studies have shown that vitamin Dhas autocrine and paracrine functions and has a role in differ-ent diseases [2]. 1,25-Dihydroxyvitamin D (1,25-(OH)2D3)shows its effect via a specific vitamin D receptor (VDR) [7].VDRs exist in more than thirty tissues (e.g., intestinal cells,muscle cells, osteoblasts, distal renal cells, parathyroid cells,pancreas islet cells, epidermal cells, neurons, placenta) [7, 26].Vitamin D has anti-proliferative effects and promotes matura-tion, differentiation, and apoptosis in many different cell linesincluding malignant cells. There is evidence that enhancedsunlight exposure is associated with lower prostate, breast,and colon cancer death rates [11]. Serum 25(OH)D level isconsiderably lower in patients with tuberculosis than in healthycontrols [21]. In animal models, vitamin D administrationbefore the disease onset prevents the development of type 1diabetes [22]. Animal studies and epidemiological modelsshow that vitamin D has beneficial effects in transplantation,
A. GüvenFaculty of Medicine, Department of Pediatrics,Baskent University,Ankara, Turkey
A. EcevitFaculty of Medicine, Department of Neonatology,Baskent University,Ankara, Turkey
O. SözerAdana Teaching and Medical Research Center,Hematology Research Laboratory, Baskent University,Adana, Turkey
A. TarcanEtlik Maternity Hospital,Ankara, Turkey
A. Tarcan (*)Faculty of Medicine, Department of Neonatology,Baskent University,Ankara, Turkeye-mail: [email protected]
N. ÖzbekFaculty of Medicine, Department of Pediatric Hematology,Baskent University,Ankara, Turkey
Eur J Pediatr (2012) 171:1161–1166DOI 10.1007/s00431-012-1688-6

cardiovascular disease, rheumatoid arthritis, periodontal dis-ease, inflammatory bowel disease, etc. [16].
VDR is expressed by antigen-presenting cells such asmacrophages and dendritic cells (DCs) and is expressed bylymphocytes following activation [6]. In vitro, addition of1,25-dihydroxyvitamin is inhibited by T lymphocyte prolif-eration, cytokine secretion, and cell cycle progression [34].
Sakaguchi et al. [31, 33] described a subpopulation set ofperipheral CD4+ T cells in normal healthy mice, which were5–10% of the total peripheral CD4+ T cell population. TheseCD4+ T cells expressed CD25 and were critical in controllingautoimmune diseases [31, 33]. CD4+CD25+ T cells (Treg)effectively suppress the proliferation and cytokine productionof CD4+ and CD8+ T cells [36]. They also inhibit the
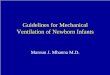
Fig. 1 Flow cytometricanalysis of the subgroup oflymphocytes. Gating strategyfor Treg cells identification andquantification: a Lymphocyteswere selected from CD45/SSplot for analysis (A gate).b Cells from the CD3/SS plotwere examined for theexpression of T lymphocytes(B gate). c CD4/CD25 doublepositive cells were selected forthe expression of TREG cells(C2 gate)
1162 Eur J Pediatr (2012) 171:1161–1166

proliferation and antibody production of B cells [4]. Naturallyarising Treg cells play a key role in the maintenance of periph-eral tolerance to self-antigen and alloantigen in vivo [19]. Tregcells have been found to suppress several T cell-mediatedimmune diseases, including allergic responses and autoim-mune diseases such as type 1 diabetes, gastritis, colitis, poly-arteritis, as well as allograft rejection and graft versus hostdisease [6, 10]. Allergen specific regulatory T cells play animportant role in controlling the development of allergy andasthma [6]. Vitamin D induces dendritic cells to modulateregulatory T cells in immune tolerance. 1,25-(OH)2D3 and itsanalogues induce DCs with tolerogenic properties in vivo, asdemonstrated in models of allograft rejection by oral adminis-tration or by adoptive transfer of in vitro-treated DCs [12, 13].
Low 25-hydroxyvitamin D levels are common in newborncord blood [3, 28, 29]. However, the effect of vitamin Ddeficiency on Treg has not been studied previously. In thispresent study, we aimed to investigate the correlation betweenthe 25-hydroxyvitamin D levels with the count and percentageof regulatory T cells.
Materials and methods
One hundred one term infants born in two hospitals (BaskentUniversity Faculty of Medicine, Maternity Department andEtlik Maternity Hospital) between February and March 2008were included in this study. Ethical committees of two hospi-tals approved the research proposal. Informed consent wasobtained from the mothers of babies in the study. A detailedquestionnaire was prepared to the mothers recruited, collect-ing information on their sociodemographic characteristics.Sociodemographic factors were place of residence and mater-nal age, education, occupation, number of pregnancies, andrelationship with her husband. Special interest was given tothe mother’s dietary practices during pregnancy regardingcalcium and vitamin D intake in particular milk (number ofglasses per day). Mothers were also asked about vitamin Dand calcium supplement consumption during pregnancy. Ma-ternal poor obstetric history and systemic illness, intrauterinegrowth retardation, and perinatal asphyxia were exclusioncriteria. Immediately after clamping the umbilical cord, 9 ccof blood was obtained.
Serum 25(OH)D levels were determined in the laboratoriesof Baskent University by radioimmunoassay using reagent kitfor HPLC analysis (parameters: injection volume 50 μl, flowrate 1.6 ml/min, determined wavelength 265 nm, columntemperature ambient; specifications: linearity 5–500μg/l, limitof detection 2.5 μg/l, recovery >85% (Vc 4%), run time7.5 min; CHROMSYSTEMS Instruments & ChemicalGmbH, München). Severe vitamin D deficiency in whichumbilical cord 25(OH)D levels are below 12 ng/ml wasaccepted [8, 18].
Flow cytometry
The following antibodies were used for phenotypic charac-terization of Tregs: anti-CD45 PC5, CD3 ECD, CD4 PE,and CD25 FITC. Cells were incubated with antibodies for20 min at room temperature in the dark. Cells were washedin DPBS, and data were acquired on a Coulter Epics XL-MCL (Beckman Coulter Inc., Miami, FL, USA). Flowcytometric data (Fig. 1) were analyzed using EXPO 32ADC software (Beckman Coulter Inc., Marseille, France).All monoclonal antibodies were obtained from BeckmanCoulter (Marseille, France). Fluorescence histograms wereobtained by recording 200,000 cells/sample at a flow rate ofapproximately 200 cell events/s.
Statistics
For statistical evaluation, SPSS for Windows SPSS software(Statistical Package for Social Sciences, version 14.0, SPSSInc.; Chicago, IL, USA) was used. χ2 and Fisher’s exacttests were used for categorized data. Normal distributionand homogeneity of the variances were evaluated usingShapiro–Wilk test. The data were distributed normally; thus,to compare the continuous data, student t test was used.Relations between 25-hydroxyvitamin D levels and T cellsubtypes were assessed by Pearson’s correlation analysis.P values <0.05 were considered statistically significant.
Results
Median birth weight was 3,450.00 (ranges 1,800–4,450) g,and duration of gestation was 39 (38–42) weeks. Median andranges of the number and percentage of T lymphocyte,T helper, and Treg are reported in Table 1. There was nocorrelation between 25-hydroxyvitamin D levels and the num-ber and percentage of T lymphocyte, T helper, and Treg(Table 2).
Table 1 Median and ranges of the number and percentage of leucocyte,total lymphocyte, T lymphocyte, T helper, and Treg
Leucocyte (/μl) 12,400 (5,000–22,200)
% Total lymphocyte 29.2 (14.2–49.3)
Total lymphocyte (/μl) 3,697 (1,020–7,630)
T lymphocyte (%) 69.1 (40.5–89.5)
T lymphocyte (/μl) 2,582 (657–5264)
T helper (%) 70.1 (51.8–87.2)
T helper (/μl) 1,814 (469–3,659)
T regulatory (%) 6.1(3.5–10.1)
T regulatory (/μl) 153 (40–303)
Eur J Pediatr (2012) 171:1161–1166 1163

Newborn babies were divided into two groups according to25-hydroxyvitamin D levels (25(OH)D <12 ng/ml and 25(OH)D >12 ng/ml). Median and ranges of birth weight in 25(OH)D <12 ng/ml and 25(OH)D >12 ng/ml groups were3,500.00 (1,800–4,450) and 3,300.00 (1,800–4,350) g, re-spectively. Median gestational ages were 39 (38–42) and 39(38–42) weeks in each group. The median and ranges of birthweight and gestational age of the groups were not differentsignificantly. The median and ranges of 25-hydroxyvitamin Dlevels and the number and percentage of T lymphocyte, Thelper, and Treg in the two groups are shown in Table 3. Therewas no significant difference in 25-hydroxyvitamin D levels,white blood cell, total lymphocyte counts, T helper, and Tregcell percentage and numbers between the groups (Table 3).
Dıscussion
itamin D has an important role in the control of inflamma-tory responses. Regulatory T cells mediate this control. Theadult and animal studies have shown that some autoimmune
and infectious diseases occur due to dysfunction of regula-tory T cells related to vitamin D deficiency [9, 20, 27].Treg’s role in the inflammatory disease of the neonatal andinfancy period has been shown in different clinical trials tobe strongly related to vitamin D deficiency (e.g., atopiceczema, cow’s milk allergy, asthma, and wheezy infant)[1, 17]. There was no significant difference in Treg’s per-centage and count in the newborn infant groups whose 25-hydroxyvitamin D levels were below or above 12 ng/ml.
In most studies, the cutoff for vitamin D deficiency variesbetween 10 and 12 ng/ml [8, 18], whereas in others, hypo-vitaminosis D is defined by 25(OH)D levels beyond whichparathyroid hormone levels rise above the normal range.This level of 25(OH)D was 22 or 25 ng/ml in differentstudies [8, 30]. In our study population, only 7 of the 101infant’s 25-hydroxyvitamin D levels were above 25 ng/ml.Severe vitamin D deficiency (25(OH)D <12 ng/ml) wasobserved in 32 patients (32%). In an Indian study, mean25-hydroxyvitamin D levels were 8.4±5.7 ng/ml in cordblood samples of neonates, and the rate of vitamin D hypo-vitaminosis (serum 25(OH)D <20 ng/ml) was 95.7% [30].In that study, contrary to expectations, women both in ruraland urban regions had equal frequency of vitamin D defi-ciency (84%). In a Greek study, 19.5% of mothers and 8.1%of neonates had hypovitaminosis D (25(OH)D <10 ng/ml),and strong correlation was found between maternal andinfant vitamin D concentrations [24]. Taken together, simplesunlight exposure, even in geographical regions like Greeceand Turkey, is not sufficient to cover the vitamin D needs inthe perinatal period.
Vitamin D-deficient rickets is reported to be associatedwith increased risk of infection and some changes in theimmune system [23]. Camak et al. [5] have found that thenumber and percentage of CD4+ and CD8+ T cells, CD4+/CD8+ ratios, were significantly higher in infants with vita-min D-deficient rickets compared to the control group. We
Table 3 The median and ranges of 25(OH)D levels and number and percentage of leucocyte, total lymphocyte, T lymphocyte, T helper, and Tregaccording to groups
Group 1 (n069) (25(OH)D >12 ng/mla) Group 2 (n032) (25(OH)D <12 ng/mla) P value
Leucocytes (/ml) 12,700 (5,000–21,000) 11,850 (6,500–22,200) 0.18
Total lymphocytes (%) 29.3 (19.0–48.60) 29.1 (14.2–49.3) 0.73
Total lymphocytes (/μl) 3,760 (1,020–7,630) 3,604 (1,961–7,095) 0.09
T lymphocytes (%) 67.6 (40.5–88.3) 69.9 (54.1–89.5) 0.72
T lymphocytes (/μl) 2,603 (657–5,264) 2,490 (1,389–4,858) 0.11
T helper (%) 70.5 (51.8–87.2) 68.7 (55.7–83.7) 0.11
T helper (/μl) 1,825 (469–3,659) 1,653 (983–3,173) 0.06
T regulatory (%) 6.1 (3.6–9.6) 6 (3.5–10.1) 0.71
T regulatory (/μl) 156 (40–303) 148 (52–224) 0.28
a Converting factor of 25(OH)D level into SI unit, 2.6
Table 2 Correlationbetween 25-hydroxyvitamin Dlevels and numberand percentage ofleucocyte, totallymphocyte, Tlymphocyte, Thelper, and Treg
NS not siginficant
25-hydroxyvitaminD levels
Leucocyte (/μl) −0.135 (NS)
Total lymphocyte(%)
0.051 (NS)
Total lymphocyte(/μl)
−0.078 (NS)
T lymphocyte (%) −0.009 (NS)
T lymphocyte (/μl) −0.058 (NS)
T helper (%) 0.253 (NS)
T helper (/μl) 0.010 (NS)
T regulatory (%) 0.051 (NS)
1164 Eur J Pediatr (2012) 171:1161–1166

could not support this finding in white blood cell number,total lymphocyte, and CD4+ T cell number and percentages.However, our population consisted of term neonates, andany of them had congenital rickets. Gysemans et al. [14]reported that CD4+CD25+ T cells were low in spleen,mesenteric lymph nodes, and thymus of vitamin Dreceptor-deficient diabetic mice. In our study group, almostall 25-hydroxyvitamin D levels were <25 ng/ml; this may bethe reason of the lack of difference between groups.
In our study, according to our questionnaire, the 79% ofmothers were living in a sunny house, 71% of them had usedvitamin D supplements and 61% of them had drunk >1 cup ofmilk everyday. But there was no significant difference be-tween 25(OH)D levels <12 or >12 ng/ml groups regardingmother’s education, occupation, whether taking vitamin Dsupplements or not, nutrition habits, dressing style, houselocation, number of pregnancies, and sex of newborns. Also,we did not find any difference according to using vitamin Dsupplements in 25(OH)D levels <12 or >12 ng/ml groups.Since the foods in Turkey are not vitamin D-fortified, we didnot find any statistically difference in newborn’s 25(OH)Dlevels according to milk consumption.
In our study, the amount of cord blood Treg was 6.23±1.33%. In literature, it is reported that natural Tregs repre-sent 1–5% of circulating CD4+ T cells [32]. In a study ofnewborn infants, about 5% to 15% of CD4+ cells expressedCD25 in umbilical venous blood has been found [25]. Inanother study, the amount of CD4+CD25+ Treg cells incord blood was 3.86±1.63% [35]. There are few studies inadult that examine the relationship between vitamin Dlevels and regulatory Tcells. Hamzaoui et al. designed a studyto investigate disease variables associated with vitamin Dlevels in patients with Behçet’s disease and its interaction withinflammatory responses. They concluded that active Behçet’sdisease was associated with lower serum vitamin D levels.Their result also showed that low levels of vitamin D wereassociated with a decrease in Treg cells [15]. Prietly et al.investigated whether vitamin D supplementation increasesTreg frequency (Treg %) within circulating CD4 T cells, andthey found that vitamin D supplementation was associatedwith significantly increased percent Tregs in healthy individ-uals [29]. In our study, we did not aim to find a correlationbetween vitamin D levels and clinical significance. On theother hand, this is the first study to investigate the relationshipbetween vitamin D levels and regulatory T cells in newborninfants.
In conclusion, the vitamin D deficiency was very high inour study group, with almost all having 25(OH)D concentra-tions in the deficiency range. The rate of severe deficiencywas32%, but Treg numbers and percentages did not differ be-tween those with and without severe vitamin D deficiency. Inaddition, there was no relationship between vitamin D statusand Tregs. The effects of vitamin D deficiency on Treg cells
and mortality and morbidity of neonatal and early infancyperiod should be investigated in the presence of antenataland perinatal risk factors. Long-term consequences of theseinfants may reveal the clinical impact of vitamin D deficiency.Further studies will also imply the relationship between clin-ical significance of autoimmune, allergic, infectious, inflam-matory diseases and vitamin D.
Acknowledgments We thank Dr. Berkan Gürakan for the helpfulcomments for this study. We also thank Ömer Keleş, Ayşegül Haberal,and Ilknur Kozanoğlu for the technical support and for providing us thelaboratory data during the study period.
Conflicts of interest Authors declare no financial interests with theorganization that sponsored the research.
References
1. Borrego LM, Arroz MJ, Videira P, Martins C, Guimaraes H, NunesG, Papoila AL, Trindade H (2009) Regulatory cells, cytokinepattern and clinical risk factors for asthma in infants and youngchildren with recurrent wheeze. Clin Exp Allergy 39:1160–1169
2. Bouillon R, Carmeliet G, Daci E, Segaert S, Verstuyf A (1998)Vitamin D metabolism and action. Osteoporos Int 8:S13–S19
3. Bowyer L, Catling-Paull C, Diamond T, Homer C, Davis G, CraigME (2009) Vitamin D, PTH and calcium levels in pregnant womenand their neonates. Clin Endocrinol (Oxf) 70:372–377
4. Bystry RS, Aluvihare V, Welch KA, Kallikourdis M, Betz AG(2001) B cells and professional APCs recruit regulatory T cells viaCCL4. Nat Immunol 2:1126–1132
5. Cakmak FN, Erol M, Ergül P, Yalcyner A (1997) T lymphocytesand vitamins. J Pediatr 130:77–85
6. Cohen JL, Trenado A, Vasey D, Klatzmann D, Salomon BL (2002)CD4(+)CD25(+) immunoregulatory T cells: new therapeutics forgraft-versus-host disease. J Exp Med 196:401–406
7. DeLuca HF, Cantorna MT (2001) Vitamin D: its role and uses inimmunology. FASEB J 15:2579–2585
8. DeLucia M, Carpenter T (2000) Rickets in the sunshine? Nutrition8:97–98
9. Ellman P, Anderson KH (1948) Calciferol in tuberculous peritonitiswith disseminated tuberculosis. BMJ 1:394
10. Furtado GC, Olivares-Villagomez D, Curotto de Lafaille MA,Wensky AK, Latkowski JA, Lafaille JJ (2001) Regulatory T cellsin spontaneous autoimmune encephalomyelitis. Immunol Rev182:122–134
11. Garland CF, Garland FC, Gorham ED (1991) Can colon cancerincidence and death rates be reduced with calcium and vitamin D?Am J Clin Nutr 54:193S–201S
12. Gregori S, Casorati M, Amuchastegui S, Smiroldo S, Davalli MA,Adorini L (2001) Regulatory T cells induced by 1α,25-dihydroxyvitamin D3 and mycophenolate mofetil treatment mediate trans-plantation tolerance. J Immunol 167:1945–1953
13. Griffin MD, Lutz W, Phan WA, Bachman LA, McKean DJ, KumarR (2001) Dendritic cell modulation by 1α,25 dihydroxyvitamin D3
and its analogs: a vitamin D receptor-dependent pathway thatpromotes a persistent state of immaturity in vitro and in vivo. ProcNatl Acad Sci U S A 98:6800–6805
14. Gysemans C, van Etten E, Overbergh L, Giulietti A, Eelen A, WaerM, VerstuyfA BR, Mathieu C (2008) Unaltered diabetes presentationin NOD mice lacking the vitamin D receptor. Diabetes 57:269–275
Eur J Pediatr (2012) 171:1161–1166 1165

15. Hamzaoui K, Ben Dhifallah I, Karray E, Sassi FH, Hamzaoui A(2010) Vitamin D modulates peripheral immunity in patients withBehçet’s disease. Clin Exp Rheumatol 28(4 Supppl 60):s50–s57
16. Holick MF (2004) Sunlight and vitamin D for bone health andprevention of autoimmune diseases, cancers, and cardiovasculardisease. Am J Clin Nutr 80(8 Suppl):1678s–1679s
17. Karlsson MR, Rugtveit J, Brand Zaeg P (2004) Allergen responsiveCD4+CD25+ regulatory T cells in children who have outgrowncow’s milk allergy. J Exp Med 199:1679–1688
18. Lapatsanis D, Moulas A, Cholevas V, Soukakos P, PapadopoulouZL, Challa A (2005) Vitamin D: a necessity for children andadolescents in Greece. Calcif Tissue Int 77:348–355
19. Maloy KJ, Powrie F (2001) Regulatory T cells in the control ofimmune pathology. Nat Immunol 2:816–822
20. Manolagas SC, Hustmyer FG, Yu XP (1990) Immunomodulatingproperties of 1,25-dihydroxyvitamin D3. Kidney Int 38:S9–S16
21. Mathieu C, Adorini L (2002) The coming of age 1,25-dihydroxyvitamin D3 analogs as immunomodulator agents. Trends MolMed 8:174–179
22. Mathieu C, Waer M, Casteels K, Laureys J, Bouillon R (1995)Prevention of type 1 diabetes in NOD mice by non hypercalcemicdoses of an new structural analog of 1,25-dihydroxyvitamin D3,KH1060. Endocrinology 3:866–872
23. Najada AS, Habashneh MS, Khader M (2004) The frequency ofnutritional rickets among hospitalized infants and its relation torespiratory diseases. J Trop Pediatr 50:364–368
24. Nemere I, Farach-Carson MC (1998) Membrane receptors forsteroid hormones: a case for specific cell surface binding sites forvitaminDmetabolites and estrogens. BiochemBiophys Res Commun248:442–449
25. Ng WF, Duggan PJ, Ponchel F, Matarese G, Lombardi G, EdwardsAD, Isaacs JD, Lechler RI (2001) Human CD4+CD25+ cells: anaturally occuring population of regulatory T cells. Blood98:2736–2744
26. Norman AW (1998) Receptors for 1α-25(OH)2D3: past, presentand future. J Bone Res 13:1360–1369
27. Pozzilli P, Manfrini S, Crino A, Picardi A, Leomanni C, Cherubini V(2005) Vitamin D3 and type 1 diabetes. HormMetab Res 37:680–683
28. Prietl B, Pilz S, Wolf M, Tomaschitz A, Obermayer-Pietsch B,Graninger W, Pieber TR (2010) Vitamin D supplementation andregulatory T cells in apparently healthy subjects: vitamin D treat-ment for autoimmune diseases? Isr Med Assoc J 12:136–139
29. Read S, Malmstrom V, Powrie F (2000) Cytotoxic T lymphocyte-associated antigen 4 plays an essential role in the function of CD25(+)CD4(+) regulatory cells that control intestinal inflammation. JExp Med 192:295–302
30. Sachan A, Gupta R, Das V, Agarwal A, Awasthi PK, Bhatia V(2005) High prevalence of vitamin D deficiency among pregnantwomen and their newborns in northern India. Am J Clin Nutr81:1060–1064
31. Sakaguchi S, Sakaguchi N, Asano M, Itoh M, Toda M (1995)Immunologic self-tolerance maintained by activated T cellsexpressing IL-2 receptor α-chains (CD25). Breakdown of a singlemechanism of self-tolerance causes various autoimmune diseases.J Immunol 155:1151–1164
32. Sakaguchi S, Sakaguchi N, Shimizu J, Yamazaki S, SakihamaT, Itoh M, Kuniyasu Y, Nomura T, Toda M, Takahashi T(2001) Immunologic tolerance maintained by CD25+CD4+regulatory T cells: their common role in controlling autoimmu-nity, tumor immunity, and transplantation tolerance. ImmunolRev 182:18–32
33. Takahashi T, Tagami T, Yamazaki S, Uede T, Shimizu J, SakaguchiN, Mak TW, Sakaguchi S (2000) Immunologic self-tolerancemaintained by CD25(+)CD4(+) regulatory T cells constitutivelyexpressing cytotoxic T lymphocyte-associated antigen 4. J ExpMed 192:303–310
34. Takeuchi A, Reddy GS, Kobayashi T, Okano T, Park J, Sharma S(1998) Nuclear factor of activated T cells (NFAT) as a moleculartarget for 1α,25-dihydroxyvitamin D3-mediated effects. J Immunol160:209–218
35. Tang J, Li BQ, Ruan J, Zhang LJ (2008) Expression of Foxp3 inCD4CD25(high) Treg cells of neonatal cord blood. Xi Bao Yu FenZi Mian Yi Xue Za Zhi 24:365–367
36. Thornton AM, Shevach EM (2000) Suppressor effector function ofCD4+CD25+ immunoregulatory T cells is antigen nonspecific. JImmunol 164:183–190
1166 Eur J Pediatr (2012) 171:1161–1166