Embed Size (px)
Citation preview

BRIEF REPORT
Correlation between cystatin C- and renal scan-determinedglomerular filtration rate in children with spina bifida
Catherine Morgan & Ambikaipakan Senthilselvan &
Fiona Bamforth & Michael Hoskinson &
Manjula Gowrishankar
Received: 26 February 2007 /Revised: 9 August 2007 /Accepted: 10 August 2007 / Published online: 9 October 2007# IPNA 2007
Abstract We report on the relationships between serumcystatin C level, glomerular filtration rate (GFR) estimatedfrom a cystatin C-based prediction equation (that of Fillerand Lepage), GFR calculated by the Schwartz formula andtechnetium 99m-diethylene triamine penta-acetic acid(99Tc-DTPA)-determined GFR in 28 children with spinabifida. All children underwent measurement of height,weight, serum cystatin C level, and serum creatinine levelat the time of their renal scan. The relationship betweenvariables was assessed by Pearson correlation. Pearsoncorrelation for the relationship between 99Tc-DTPA GFRand GFR calculated by the cystatin C-based equation wassignificant and higher than that of the relationship between99Tc-DTPA GFR and GFR calculated by the Schwartz
equation, which was not statistically significant. Thecorrelation for Filler GFR was 0.42 (P=0.03) and forSchwartz GFR was 0.21 (P=0.28). Although we use renalscan determination of GFR as the best measure, and acreatinine-based formula as the most practical measure,perhaps a formula such as that published by Filler andLepage, which is not dependent on anthropometric data,might be a more useful (and accurate) tool for establishingGFR in children with spina bifida.
Keywords Renal function . Prediction equations .
Biomarkers . Monitoring . Spinal dysraphism
Introduction
Children with spina bifida are at risk of developing renalimpairment due to the structural and or functional abnor-malities of their urinary tracts [1], and, therefore, accuratemonitoring of glomerular filtration rate (GFR) is of greatimportance. In paediatric clinical practice, GFR hastraditionally been estimated by serum or urine creatinine-based methods. These methods, utilizing creatinine as afiltration marker, have well recognized inherent problems[2, 3], which are amplified in children with spina bifida.
A more effective alternative for screening and continu-ous monitoring for change in GFR in these children isneeded. Serum cystatin C level is evolving as a standardmarker of GFR in children [2, 4–6]. It has been previouslyshown in children with spina bifida that cystatin C is asuperior marker to estimate GFR when compared with thecreatinine-based Schwartz estimation [7]. In addition, asmore data emerge regarding serum cystatin C level as amarker of GFR, investigators are deriving cystatin C-based
Pediatr Nephrol (2008) 23:329–332DOI 10.1007/s00467-007-0613-0
C. Morgan :M. Gowrishankar (*)Pediatric Nephrology, Department of Pediatrics,University of Alberta,2B2-42 Walter Mac Kenzie Health Science Centre,Edmonton T6G 2R7, AB, Canadae-mail: [email protected]
A. SenthilselvanDepartment of Public Sciences, School of Public Health,University of Alberta,13-106 B Clinical Science Building,Edmonton T6G 2G3, AB, Canada
F. BamforthClinical Laboratory Medicine and Pathology Services,University of Alberta,4B4-02 Walter Mac Kenzie Health Sciences Centre,Edmonton T6G 2R7, AB, Canada
M. HoskinsonDepartment of Radiology and Diagnostic Imaging,University of Alberta,2A3-22 Walter Mac Kenzie Health Sciences Centre,Edmonton T6G 2R7, AB, Canada

prediction equations for paediatric GFR, with the goal ofuse in clinical practice [2, 8].
Here, we report on the relationships between serumcystatin C level, GFR estimated from a cystatin C-basedprediction equation (that of Filler and Lepage) [8], GFRcalculated by the Schwartz formula, and technetium 99m-diethylene triamine penta-acetic acid (99Tc-DTPA)-determinedGFR, in children with spina bifida.
Materials and methods
We report findings from 28 children with spina bifida. Thestudy received full approval by the local Human ResearchEthics Board. Laboratory and radiological investigationswere performed at the Stollery Children’s Hospital,Edmonton, Alberta, Canada. Blood was drawn forcystatin C and creatinine measurement at the time ofradionucleotide scanning for determination of GFR. Heightand weight were also measured at this time. For childrenwho were wheelchair bound, supine length was measuredand used as a surrogate for height.
Serum cystatin C was analysed with the Dade Behring NLatex cystatin C assay, automated on the Dade Behring BNSystem (Dade Behring Diagnostics, Marburg, Germany).The method was a fully automated, particle-enhanced,nephelometric immunoassay. Serum creatinine was ana-lysed by the kinetics Jaffe reaction method with a BeckmanSyncron LX analyser.
Glomerular filtration rate was measured by a single-injection technique using 99Tc-DTPA with a multipleplasma sample method [9]. Correction was made for bodysurface area (BSA), calculated from the Haycock formula[10], and the result was expressed as millilitres per minuteper 1.73 square metres BSA.
Estimated GFR was calculated from both the Schwartzformula and a cystatin C-based formula previously derivedby Filler and Lepage [8] (herein referred to as the Fillerequation). The Schwartz formula for estimating GFR isgiven by the equation, GFR=k x ht/Scr, where k is aconstant, ht is the height of the child (in centimetres) andScr is the serum creatinine concentration (in micromolesper litre) [11]. In the Schwartz equation, the constant k usedfor adolescent boys (13 years of age or older) was 62, andfor all other children was 49 [11]. The cystatin C-basedformula for estimating GFR is given by the equation,log GFRð Þ ¼ 1:962þ 1:23* log 1=cystatin Cð Þ, where cystatin Cis measured in milligrammes per litre. GFR is obtainedfrom the equation by taking the anti-logarithm. Thisformula was derived using the same cystatin C assay asours and, the same gold standard for determination of GFR.Therefore, we used the published coefficients for calculat-ing the GFRs.
Statistical analysis
We used Stata 9.2 for Windows to conduct the statisticalanalysis [12]. Glomerular filtration rate determined by theSchwartz formula and the Filler formula were comparedwith the 99Tc-DTPA GFR using paired t-tests. Pearsoncorrelation was compared between GFR measured by 99Tc-DTPA renal scan and GFR calculated from the Schwartzand Filler formulae. The Pearson correlation was alsodetermined for measured GFR and 1/cystatin C. In order tolook for a possible modification of the effect, of thepatient’s being in a wheelchair or not on the prediction ofthe 99Tc-DTPA GFR by Schwartz GFR and Filler GFR,respectively, we applied a linear regression model, whichincluded an interaction term for such an effect. A P value of<0.05 was considered to be statistically significant in allanalyses.
Results
In total, 28 children were studied, 16 of whom were boysand all of whom had myelomeningocele. Two children hada thoracic lesion, with the remainder having a lumbar orlumbosacral lesion. Nine children were wheelchair bound.The children ranged in age from 4 years to 15 years, with amean age for the group of 9.4 years. Mean ± standarddeviation (SD) for body mass index (BMI) was 0.97±0.29(kg/m2), with a minimum of 0.62 (kg/m2) and a maximumof 1.75 (kg/m2). Serum cystatin C ranged from 0.61 mg/l to1.24 mg/l, with a mean of 0.81 mg/l and a median of0.76 mg/l.
The mean ± SD for 99Tc-DTPA GFR, Schwartz GFR,and Filler GFR was 112±26 ml/min per 1.73 m2 BSA,170±50 ml/min per 1.73 m2, and 120±22 ml/min per1.73 m2, respectively. The mean difference betweenSchwartz GFR and 99Tc-DTPA GFR was significant(P<0.0001) and was equal to 58 ml/min per 1.73 m2
BSA [95% confidence interval (CI) 39 ml/min per 1.73 m2
to 78 ml/min per 1.73 m2]. Mean values of Filler GFR and99Tc-DTPA GFR were not significantly different, with thedifference being equal to 7 ml/min per 1.73 m2 (95% CI3 ml/min per 1.73 m2 to 17 ml/min per 1.73 m2).
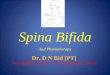
The results of correlation analysis are illustrated inFig. 1. In this group of children with spina bifida, Pearsoncorrelation for the relationship between 99Tc-DTPA GFRand Filler GFR was significant and greater than that for therelationship between 99Tc-DTPA GFR and Schwartz GFR,which was not statistically significant. The correlationbetween 99Tc-DTPA GFR and Filler GFR was 0.42 (95%CI 0.06 to 0.70, P=0.03), and between 99Tc-DTPA GFRand Schwartz GFR it was 0.21 (95% CI −0.18 to 0.61,P=0.28). There was a significant correlation between 99Tc-
24 Pediatr Nephrol (2008) 23:329–332

DTPA GFR and 1/cystatin C; Pearson correlation 0.42;95% CI 0.06 to 0.70, P=0.03.
Linear regression of 99Tc-DTPA GFR on Schwartz GFRand 99Tc-DTPA GFR on Filler GFR, with an interactionterm for wheelchair use in both models, resulted in aP=0.62 and P=0.13 for the interaction term in each model,respectively. Therefore, wheelchair use was not a signifi-cant modifier of either of these relationships.
Discussion
The results of this study show that, in children with spinabifida, GFR determined by a cystatin C-based estimationequation is a better measure of GFR than that estimated bythe Schwartz formula, which is commonly used for serialmonitoring of GFR in high-risk populations. That GFRestimated from the Schwartz formula showed no significantcorrelation with 99Tc-DTPA GFR confirms that, in childrenwith spina bifida, currently used surrogate markers of GFRare not accurate. We report that the GFR determined by theSchwartz formula significantly overestimates that deter-mined by radioisotope scan. We did not use locally derivedproportionality constants (k) for the Schwartz formula, and,hence, the difference between a potentially less biasedestimation by Schwartz- and radioisotope-determined GFRscannot be inferred. However, given that the constants werederived by a method similar to that performed locally,Schwartz GFR estimates are likely to be reasonablyaccurate.
Serum cystatin C has been examined in a number ofpatient populations, including healthy children [13], renaltransplant recipients [14] and patients with glomerulone-phritis/various renal diseases [4, 7, 15–17]. In many studies,serum cystatin C-derived GFR was equivalent to radioiso-tope (125-I iothalamate) determination of GFR and 24 hurine for creatinine clearance and was superior to serumcreatinine for monitoring renal impairment [18]. Ourfindings are in agreement with those previous studies, aswell as the investigation of serum cystatin C as a marker ofGFR in patients with spinal cord injury [19] and the priorinvestigation of the use of cystatin C to estimate GFR inpatients with spina bifida [7].
Although our results suggest that the prediction of GFRby Filler and Schwartz equations is not modified by thepatients’ being wheelchair-bound or not, our study was notinitially powered to detect this interaction. It is of interestthat the correlation seen between 99Tc- DTPA GFR andFiller GFR as well as the correlation between 99Tc- DTPAGFR and the inverse of cystatin C in this study group islower than that shown in studies including children withoutspina bifida [8]. In comparison with that in a previous studyof children with spina bifida [7], the Pearson correlation forthe relationship between 99Tc- DTPA GFR and the inverseof cystatin C study is similar (0.45 in the previous studycompared with 0.42 in our study). An explanation for thedifference in strength of association between these studiesis the difference in the range of GFR of the studyparticipants; the weaker association in the present andprevious study of children with spina bifida may reflect that
5010
015
020
0T
c99
GF
R (
mls
/min
/sq
m)
80 100 120 140 160Filler GFR (mls/min/1.73 sq m)
5010
015
020
0T
c99
GF
R (
mls
/min
/sq
m)
.8 1 1.2 1.4 1.61/cystatin C (L/mg)
5010
015
020
0T
c99
GF
R (
mls
/min
/sq
m)
100 150 200 250 300 350Schwartz GFR (mls/min/1.73 sq m)
ρ=0.42 ρ=0.21
ρ=0.42
Fig. 1 Correlation between esti-mates of glomerular filtrationrate and glomerular filtrationrate determined by 99Tc-DTPA.The straight line indicates thefitted line, and the shaded arearepresents the 95% confidenceinterval for the fitted line. ρ=Pearson correlation
Pediatr Nephrol (2008) 23:329–332 25

the majority of participants had a relatively normal GFR.An alternate hypothesis is that this may reflect measure-ment error in terms of GFR by 99Tc- DTPA renal scan inthe population of children with spina bifida, due to thedependence on anthropometric data. It may illustrate theinaccuracy of BSA measurement in these children, who areoften wheelchair bound and/or have scoliosis, lower limbdeformities, and abnormal body morphology. Although weuse the renal scan determination of GFR as the bestmeasure, perhaps a formula such as that published by Fillerand Lepage, which is not dependant on anthropometricdata, might be a more useful (and accurate) tool forestablishing GFR in children with spina bifida.
Acknowledgements This work was supported by a grant from theStollery Children’s Hospital Foundation (G599000602).
References
1. Muller T, Arbeiter K, Aufricht C (2002) Renal function inmeningomyelocele: risk factors, chronic renal failure, renalreplacement therapy and transplantation. Curr Opin Urol12:479–484
2. Schwartz G, Furth S (2007) Glomerular filtration rate measure-ment and estimation in chronic kidney disease. Pediatr NephrolDOI 10.1007/s00467-006-0358-1
3. Gretz N, Schock D, Sadick M, Pill J (2007) Bias and precision ofestimated glomerular filtration rate in children. Pediatr Nephrol22:167–169
4. Foster J, Reisman W, Lepage N, Filler G (2006) Influence ofcommonly used drugs on the accuracy of cystatin C-derivedglomerular filtration rate. Pediatr Nephrol 21:235–238
5. Mitsnefes M, Kathman T, Mishra J, Kartal J, Khoury P, NickolasT, Barasch J, Devarajan P (2007) Serum neutrophil gelatinase-associated lipocalin as a marker of renal function in children withchronic kidney disease. Pediatr Nephrol 22:101–108
6. Bouvet Y, Bouissou F, Coulais Y, Séronie-Vivien S, Tafani M,Decramer S, Chatelut E (2006) GFR is better estimated by
considering both serum cystatin C and creatinine levels. PediatrNephrol 21:1299–1306
7. Pham-Huy A, Leonard M, Lepage N, Halton J, Filler G (2003)Measuring glomerular filtration rate with cystatin C and beta-traceprotein in children with spina bifida. J Urol 169:2312–2315
8. Filler G, Lepage N (2003) Should the Schwartz formula forestimation of GFR be replaced by cystatin C formula? PediatrNephrol 18:981–985
9. Piepsz A, Colarinha P, Gordon I, Hahn K, Olivier P, Sixt R, vanVelzen J, Paediatric Committee of the European Association ofNuclear Medicine (2001) Guidelines for glomerular filtration ratedetermination in children. Eur J Nucl Med 28:BP31–BP36
10. Haycock G, Schwartz G, Wisotsky D (1978) Geometric methodfor measuring body surface area: a height-weight formulavalidated in infants, children, and adults. J Pediatr 93:62–66
11. Schwartz G, Brion L, Spitzer A (1987) The use of plasmacreatinine concentration for estimating glomerular filtration rate ininfants, children and adolescents. Pediatr Clin North Am 34:571–590
12. StataCorp (2005) Stata statistical software: release 9. CollegeStation, TX: StataCorp LP
13. Filler G, Witt I, Priem F, Ehrich JHH, Jung K (1997) Arecystatin C and beta2-microglobulin better markers than serumcreatinine for prediction of a normal glomerular filtration rate inpediatric subjects? Clin Chem 43:1077–1078
14. White C, Akbari A, Hussain N, Dinh L, Filler G, Lepage N, KnollGA (2005) Estimating glomerular filtration rate in kidneytransplantation: a comparison between serum creatinine andcystatin C-based methods. J Am Soc Nephrol 16:3763–3770
15. Wasilewska A, Zoch-Zwierz W, Jadeszko I, Porowski T,Biernacka A, Niewiarowska A, Korzeniecka-Kozerska A (2006)Assessment of serum cystatin C in children with congenitalsolitary kidney. Pediatr Nephrol 21:688–693
16. Alvarez O, Zilleruelo G, Wright D, Montane B, Lopez-Mitnik G(2006) Serum cystatin C levels in children with sickle cell disease.Pediatr Nephrol 21:533–537
17. Bokenkamp A, Herget-Rosenthal S, Bokenkamp R (2006)Cystatin C, kidney function and cardiovascular disease. PediatrNephrol 21:1223–1230
18. Dharnidharka VR, Kwon C, Stevens G (2002) Serum cystatin C issuperior to serum creatinine as a marker of kidney function: ameta-analysis. Am J Kidney Dis 40:221–226
19. Thomassen S, Johannesen I, Erlandsen E, Abrahamsen J, RandersE (2002) Serum cystatin C as a marker of the renal function inpatients with spinal cord injury. Spinal Cord 40:524–528
26 Pediatr Nephrol (2008) 23:329–332