-
Correction
ENVIRONMENTAL SCIENCESCorrection for “Assessment of the
Legionnaires’ disease out-break in Flint, Michigan,” by Sammy
Zahran, Shawn P. McElmurry,Paul E. Kilgore, David Mushinski, Jack
Press, Nancy G. Love,Richard C. Sadler, and Michele S. Swanson,
which was firstpublished February 5, 2018; 10.1073/pnas.1718679115
(Proc NatlAcad Sci USA 115:E1730–E1739).The authors wish to note,
“While we declare no conflicts of
interest, we would like to amend our original disclosure
state-ment in the interest of full transparency. We wish to
disclose thatDrs. McElmurry and Kilgore were served subpoenas by
the FlintSpecial Prosecutor, Todd Flood, to testify, under oath, at
inves-tigatory proceedings and at preliminary examinations for Mr.
LyonsandDr.Wells. Mr. Lyons is the Director of theMichigan
Departmentof Health and Human Services (MDHHS), and Dr. Wells
isChief Medical Executive for the MDHHS. MDHHS providedfunding for
this work.”
Published under the PNAS license.
Published online June 11, 2018.
www.pnas.org/cgi/doi/10.1073/pnas.1808389115
www.pnas.org PNAS | June 19, 2018 | vol. 115 | no. 25 |
E5835
CORR
ECTION
Dow
nloa
ded
by g
uest
on
June
6, 2
021
Dow
nloa
ded
by g
uest
on
June
6, 2
021
Dow
nloa
ded
by g
uest
on
June
6, 2
021
Dow
nloa
ded
by g
uest
on
June
6, 2
021
Dow
nloa
ded
by g
uest
on
June
6, 2
021
Dow
nloa
ded
by g
uest
on
June
6, 2
021
Dow
nloa
ded
by g
uest
on
June
6, 2
021
Dow
nloa
ded
by g
uest
on
June
6, 2
021
Dow
nloa
ded
by g
uest
on
June
6, 2
021
Dow
nloa
ded
by g
uest
on
June
6, 2
021
Dow
nloa
ded
by g
uest
on
June
6, 2
021
Dow
nloa
ded
by g
uest
on
June
6, 2
021
http://www.pnas.org/site/aboutpnas/licenses.xhtmlwww.pnas.org/cgi/doi/10.1073/pnas.1808389115
-
Assessment of the Legionnaires’ disease outbreak inFlint,
MichiganSammy Zahrana,b, Shawn P. McElmurryc, Paul E. Kilgored,
David Mushinskia, Jack Pressc, Nancy G. Lovee,Richard C. Sadlerf,
and Michele S. Swansong,1
aDepartment of Economics, Colorado State University, Fort
Collins, CO 80523; bDepartment of Epidemiology, Colorado School of
Public Health, Fort Collins,CO 80523; cDepartment of Civil &
Environmental Engineering, Wayne State University, Detroit, MI
48202; dDepartment of Pharmacy Practice, Wayne StateUniversity,
Detroit, MI 48201; eDepartment of Civil & Environmental
Engineering, University of Michigan, Ann Arbor, MI 48109;
fDepartment of FamilyMedicine, Michigan State University, Flint, MI
48502; and gDepartment of Microbiology and Immunology, University
of Michigan, Ann Arbor, MI 48109
Edited by Andrea Rinaldo, École Polytechnique Fédérale de
Lausanne, Lausanne, Switzerland, and approved January 5, 2018
(received for review October27, 2017)
The 2014–2015 Legionnaires’ disease (LD) outbreak in
GeneseeCounty, MI, and the outbreak resolution in 2016 coincided
withchanges in the source of drinking water to Flint’s municipal
watersystem. Following the switch in water supply from Detroit to
FlintRiver water, the odds of a Flint resident presenting with LD
in-creased 6.3-fold (95% CI: 2.5, 14.0). This risk subsided
followingboil water advisories, likely due to residents avoiding
water, andreturned to historically normal levels with the switch
back in watersupply. During the crisis, as the concentration of
free chlorine inwater delivered to Flint residents decreased, their
risk of acquiringLD increased. When the average weekly chlorine
level in a censustract was
-
water temperature, corrosion rate(s), and pipe wall effects.
Ultimately,the loss of free chlorine in a distribution system is
complex, andthe myriad of factors leading to it are commonly
referred to,collectively, as chlorine demand. With limited
historical dataavailable, it is impossible to identify which
constituents causedchlorine demand in the Flint system or had a
direct effect onbiofilm and legionellae growth. Because some of
these poten-tially confounding water quality and water system
variablespromote the growth of legionellae, the influence of free
chlorinealone on LD would likely be underestimated. Therefore,
althoughthe literature indicates insufficient chlorine is a
contributing factorto LD outbreaks (6–11), we do not attempt to
link the lack ofchlorine residual as the sole mechanistic cause of
LD. Instead, herewe use free chlorine concentration as an indicator
of the potentialfor legionellae growth. Utilities are required by
law to measure
disinfectant residual, which is an easily measured value;
there-fore, we posit that disinfectant residual concentration may
be auseful surrogate for indicating LD risk.Before the switch in
Flint’s water source, the concentration of
free chlorine (mg/L as Cl2) across eight water monitoring
loca-tions in the city was similar (Fig. 1B), as demonstrated by
thestrong between-monitor correlation in free chlorine (r >
0.70; TableS1). Within weeks of the switch, significant
fluctuations in theconcentration of free chlorine were observed
both between moni-tors (spatial variation) and at each monitor over
time (temporalvariation), with the mean between-monitor correlation
falling by∼30% and the average within monitor SD increasing from
0.200 to0.416 mg/L as Cl2. For example, throughout the postswitch
period, asustained collapse of free chlorine below 0.5 mg/L was
observed atmonitoring location 6 for all but a few weeks, the
chlorine residual
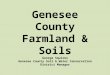
Fig. 1. Spike in LD cases coincident with switch in water supply
and increased variation observed in the Flint water distribution
system. (A) Quarterly LDincidence in Genesee County, MI, 2010
through 2016. The count of LD cases in Genesee County as compiled
in the Michigan Disease and Surveillance System atthe quarterly
time step. Bars in gray correspond to the preswitch period, bars in
maroon correspond to the postswitch period, and bars in navy
correspond tothe switch back period. (B) Free chlorine at eight
monitoring locations in Flint’s water distribution system,
2013–2016. Free chlorine (mg/L as Cl2) was reportedweekly during
the three water regime phases defined above (vertical lines) and
the periods and dates (year/week) shown at eight locations in
Flint.
Zahran et al. PNAS | Published online February 5, 2018 |
E1731
ENVIRONMEN
TAL
SCIENCE
SPN
ASPL
US
http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplemental
-
measured at monitoring location 8 was persistently >1.5 mg/L,
andthat at monitoring location 7 varied greatly. With the switch
back toDWSD-supplied water, the extreme variation in free chlorine
be-tween locations subsided, with the exception of location
6.During the period that treated Flint River water was distrib-
uted to Flint residents, poor water quality and extended
periodsof low chlorine residual may have enabled legionellae growth
inthe distribution system (4, 12). Residual chlorine is maintained
inwater distribution systems to inhibit the growth of
pathogens,including L. pneumophila (6, 7). Free-living L.
pneumophila areinactivated within 15 min of exposure to 0.4 mg
Cl2/L (8).However, this pathogen also resides in biofilms attached
to pipewalls and replicates within predatory free-living protozoa
(13,14), two habitats that require higher doses of chlorine to
killlegionellae (9–11). To reduce the risk associated with
bacterialgrowth in water distribution systems, regulatory agencies
rec-ommend a minimum free chlorine residual of 0.2–0.5 mg/L
(15–17). The effectiveness of chlorine disinfection depends on
systemconditions and chemistry; for example, iron and assimilable
or-ganic carbon can both consume chlorine and support L.
pneu-mophila growth (18). However, because chlorine residual is
oneof the most common measurements of water conditions
withindistribution systems, here we exploit the chlorine residual
valuesreported in Flint from 2013 to 2016 to investigate how
theselevels associated with the occurrence of LD.Analytically, the
timing of changes in Flint’s source water and
treatment, the accompanying spatiotemporal variations in
freechlorine, and the enhanced level of monitoring allow us to
sta-
tistically calculate the effect of water disinfection on LD risk
atthe scale of a municipal water system. To evaluate the
hypothesisthat changes in Flint’s source water and treatment
resulted in theGenesee County LD outbreak, we develop a series of
statisticaltests that exploit spatiotemporal details for the
complete in-ventory of LD cases that occurred from 2010 to 2016 in
Geneseeand neighboring Wayne and Oakland Counties. LD case
dataobtained from the Michigan Department of Health and
HumanServices (MDHHS) included relevant epidemiological
informa-tion on dates of symptom onset and referral to the
MichiganDisease Surveillance System, as well as residence of LD
cases bycensus tract. In analyses that follow, we construct a
series of re-gression models that capture the variation in LD risk
attributableto four distinct phases of exposure to water regimes in
Flint’smunicipal water system. Using these models, we derive the
in-cidence of human LD as a function of residual chlorine
concen-tration in a full-scale municipal water distribution system.
Weassess the robustness of our models by excluding all likely
hospital-acquired LD cases and by ascertaining if the risk of LD in
censustracts adjacent to Flint increased as a function of commuter
flowinto Flint. Results of this analysis can inform the management
ofwater systems dependent on chlorine disinfection.
Water Exposure RiskTo capture the effects of changes in source
water and treatment,we constructed a series of
difference-in-differences regressionmodels that exploit spatial
variation (in Flint versus outside ofFlint) and four distinct
phases of water-related LD exposure
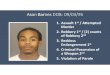
Fig. 2. Probability of observing a case of LD in Genesee County
during four phases of the Flint water crisis. (A) The four phases
of water exposure risk aredefined. Phase A is the period before
switch with water supplied by the DWSD from Lake Huron. Phase B is
the period after switch to Flint River water treatedby the City of
Flint and before water boil advisories. Phase C is the period after
switch to treated Flint River water and after boil advisories.
Phase D is theperiod after switch back to water derived from Lake
Huron. Start and end dates for each phase are indicated. (B) The
probability of observing a case of LD inFlint and non-Flint census
tracts by phases in the Flint water crisis. The estimated
probability (with 95% confidence intervals) of observing a case of
LD in acensus tract in each of the four phases of water regime
exposure risk in Oakland and Wayne census tracts (control group,
non-Flint tracts, navy) and in Flintcensus tracts (treatment group,
Flint, maroon) are shown. Estimated probabilities are derived with
all other model covariates (i.e., meteorological and de-mographic)
fixed at sample means.
E1732 | www.pnas.org/cgi/doi/10.1073/pnas.1718679115 Zahran et
al.
www.pnas.org/cgi/doi/10.1073/pnas.1718679115
-
risk during the Flint water crisis (Fig. 2A and Table S2).
Thedifference-in-differences method infers an exposure risk effect
bycomparing the difference between periods on the outcome
ofinterest (the presence of an LD case in a census tract in a
givenweek) for treated census tracts relative to not treated
censustracts (Table S2). In the preswitch period, LD risk in Flint
andnon-Flint census tracts was similar (Fig. S1). Thus, the
difference-in-differences method posits that the LD risk in
non-Flint census tractsrepresents what would have occurred in Flint
census tracts if not forthe switch in source water and
treatment.The association between a census tract in Flint
presenting with
an LD case and the switch in water supply from DWSD to theFlint
River is measured in weekly periods as an odds ratio
(OR).Throughout, the estimated treatment effect is the coefficient
ofthe interaction between space and time. In Table 1, models 1,
2,and 3 contrast Flint × postswitch, phase B vs. C vs. A, and
phaseD vs. A, respectively, as defined in Fig. 2. In model 1,
thepostswitch period combines phases B and C. Other factors
heldequal, model 1 of Table 1 shows that the switch in source
waterand treatment increased the odds of a census tract in Flint
havinga case of LD by factor 7.3 [95% confidence interval (CI):
3.5–15.0]. When the non-Flint Genesee County census tracts
areincluded in our control group (Table S3, model 1), the switch
inwater regime increased the risk of LD incidence in Flint by
440%(OR = 5.4, 95% CI: 2.7–11.2).Next, we test whether boil water
advisories issued by author-
ities in Flint attenuated the risk of LD. After positive tests
forEscherichia coli contamination, public boil water advisories
in-creased water avoidance by residents across the city (19,
20).Indeed, the odds of an LD case in a Flint census tract
increasedby a factor of 10 (OR = 10.0, 95% CI: 4.2–23.8) in the
postswitchpreadvisory period compared with a 6 factor increase (OR
= 5.9,95% CI: 2.6–13.2) in the postswitch postadvisory period
(Table1, model 2). Although the difference in LD risk in Flint
between
the preadvisory versus postadvisory periods is
epidemiologicallysubstantive, it is not statistically
significant.In October 2015, the MDHHS and the Genesee County
Health
Department jointly announced a state of emergency and
instruc-ted residents to avoid drinking the water. On October 16,
Flintreconnected to the DWSD water system. This switch back in
watersource and treatment provides another test of the water
systemhypothesis. In particular, we compare LD risk in the switch
backphase D versus phase A both in Flint (Table 1, model 3) and
incontrol neighborhoods of Oakland and Wayne Counties (Table
S3,model 3). In both models, the risk of an LD case appearing in
aFlint census tract during the switch back period is
indistinguishablefrom the preswitch period, indicating that the
switch back in watersupply ended the LD outbreak in Flint.The
estimated probabilities of observing an LD case in a
census tract inside or outside Flint through the four phases
ofwater exposure risk (Fig. 2A) is plotted in Fig. 2B. Before
theswitch to the Flint River water source, there is only
negligibledifference in the estimated probabilities of LD incidence
be-tween Flint and non-Flint census tracts. In contrast, the LD
riskin Flint increases significantly in the postswitch water
regimeperiod and then lessens somewhat following water
advisories.After the switch back to the DWSD water source, the LD
risk inFlint returns to the level before the regime switch. These
distinctshifts in estimated probabilities in Flint versus non-Flint
neighbor-hoods between each water exposure phase support the
hypothesisthat changes in Flint’s municipal water system were
responsible forthe outbreak and subsidence of LD incidence.
Free ChlorineThe extreme temporal and spatial variation in free
chlorine in-duced by the switch in Flint’s water supply (Fig. 1B
and Table S1)provides an unprecedented opportunity to analyze the
relation-ship between a water quality parameter and LD incidence in
a
Table 1. Odds ratios of tract presenting with case of
Legionnaires’ disease: water regime exposure effects
Variables
Model 1: phases B and C vs.A non-Flint Geneseecensus tracts
excludedfrom control group
Model 2: phase B vs. C vs.A non-Flint Geneseecensus tracts
excludedfrom control group
Model 3: phase D vs.A non-Flint Geneseecensus tracts
excludedfrom control group
Flint 0.603 0.603 0.584*[0.325, 1.118] [0.325, 1.118] [0.314,
1.085]
Postswitch 0.822*[0.674, 1.002]
Flint × postswitch 7.245***[3.504, 14.979]
Postswitch/preadvise 0.779[0.567, 1.071]
Postswitch/postadvise 0.844[0.670, 1.063]
Flint × postswitch/preadvise 10.007***[4.211, 23.782]
Flint × after switch/postadvise 5.854***[2.595, 13.204]
Switch back 1.381***[1.135, 1.680]
Flint × switch back 0.990[0.310, 3.165]
N 309,192 309,192 277,480Ntracts 991 991 991Log likelihood
−3,930.58 −3,929.78 −3,784.70Wald χ2 286.79 293.15 279.08
Notes: 95% confidence intervals in braces, ***P < 0.01, **P
< 0.05, *P < 0.1. Models 1 through 3 control for average
temperature, average humidity,average precipitation, percent of
households in a census tract receiving public assistance, and
percent of population ≥50 y of age and include a census tractrandom
effect.
Zahran et al. PNAS | Published online February 5, 2018 |
E1733
ENVIRONMEN
TAL
SCIENCE
SPN
ASPL
US
http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplemental
-
full-scale municipal water distribution system. For this
purpose,we develop a monitor-to-parcel assignment algorithm that
le-verages best available information on parcel
occupancy/vacancy,residence time of water (i.e., water age), and
the Flint waterdistribution system pipe network (Fig. S2).Table 2
reports ORs of a census tract in Flint presenting with
an LD case by the estimated chlorine residual in water
deliveredto residents. In addition to controlling for demographic
andmeteorological factors that influence LD outcomes, this
modelcaptures other factors that may contribute to
neighborhoodvariation in LD risk, including socioeconomic status
and age >50 y.Model 1 shows results where free chlorine is
measured as a con-tinuous variable. We find that a unit increase in
free chlorine(1 mg/L) reduced the odds (OR = 0.21, 95% CI:
0.07–0.62) of anLD case being reported by about 80%. Models 2 and 3
show resultswhere the concentration of free chlorine is measured
categoricallyas
-
Flint after the city switched to the Flint River as its
municipal watersource but not before (Fig. 4). This statistical
relationship indicatesthat exposure to Flint water partially
accounts for the observed in-crease in LD in neighboring
municipalities.
DiscussionThat a sustained and widespread inability to maintain
adequatefree chlorine residuals in Flint’s municipal water system
wasresponsible for the LD outbreak in Genesee County in 2014
and2015 is supported by this ensemble of causal inference
tests,integration of multiple datasets, and repeated substantiation
ofhypotheses. The odds of a neighborhood (i.e., census tract)
inFlint reporting a case of LD increased by a factor of 7.3 in
theperiod after the switch to the Flint River water source (Table
1,model 1a). The relative risk between Flint and non-Flint
censustracts in this postswitch period was over 6–1, with an
estimated80% of LD cases in Flint attributable to the change in
watersource and treatment. When boil water advisories
increasedwater avoidance by residents, the odds of an LD case
reportingfrom a Flint neighborhood subsided from an OR of
10.0–5.9(Table 1, model 2). The advisories, along with General
MotorsCorporation’s statement that the water was too corrosive to
useat their engine plant, likely confirmed residents’ suspicions
thatthe water was unsafe and resulted in behavior change that
re-duced their exposure. Furthermore, the risk of LD returned
topre-Flint water crisis levels after the switch back to the
LakeHuron water supply (Table 1, model 3).During the period when
water was drawn from the Flint River,
the free chlorine residual that associated with mitigation of
LDrisk was nearly five times greater than it was before the switch
inwater supply (1.4 versus 0.3 mg/L; Fig. 3). This response in
ourmodel is indicative of an increase in free chlorine demand that
isconsistent with reports during this period of enhanced levels
ofiron and assimilable organic matter, both of which
promotelegionellae growth and react chemically with free
chlorine,thereby reducing its availability for disinfection
reactions.Exploiting the extraordinary variation in water quality
in the
Flint distribution system, we developed an analysis of human
LD
incidence as a function of free chlorine residual in a
community-scale distribution system. When water was supplied by the
FlintRiver, a 1 mg/L increase in free chlorine reduced the risk of
anLD case in a neighborhood by about 80% (Table 2, model
1).Conversely, the odds of an LD case increased by factors of2.9
and 3.9 when the average weekly chlorine levels in a censustract
were
-
municipal water systems similar to that in Flint, increasing
theamount of free chlorine residual above trace levels at all
points inthe distribution network is likely to reduce LD risk. The
optimallevel of chlorine residuals must take into account
potentially det-rimental effects, such as formation of disinfection
by-products andincreased rates of corrosion. However, our analyses
establish thatother things held equal, maintaining disinfectant
residual at allpoints within water distribution systems can
substantially minimizethe risk of Legionnaires’ disease.
Materials and MethodsData. Deidentified data on LD cases from
2010 to 2016 were obtained fromthe MDHHS by Data Use and
Confidentiality Agreements following approvalfrom the Institutional
Review Board for the Protection of Human ResearchSubjects (MDHHS
IRB 201608-01-EA, Wayne State University IRB 067016B3E).Data
represent a complete inventory of LD cases in Genesee, Oakland,
andWayne Counties over this 6-y period. Each case is time-stamped
with dates ofsymptom onset, patient diagnosis, and referral to the
Michigan DiseaseSurveillance System (MDSS). The precise date of
referral to the MDSS isavailable for all LD cases. Only 623 of the
833 (25.2% missing) LD cases inGenesee, Oakland, and Wayne Counties
have a recorded diagnosis date.Although MDHHS staff generously
provided enhanced onset date datacollected from case
investigations, only 694 cases (16.7% missing) had averified date
of symptom onset. In consultation with scientific personnel
atMDHHS, the date of the referral is the most reliable and valid
indication oftiming. Median difference in elapsed time between
referral and diagnosisdates is 1 d, and 5 d between referral and
symptom onset dates. These lagsinform our use of referral timing
data in chlorine analyses. Given the veryhigh correlation between
referral and onset date (R2 = 0.9973), using referraldate with a
time lag adjustment in chlorine models resolves the timing errorand
preserves maximum information (limiting themissing information bias
thatarises with use of onset date). MDHHS data are also referenced
geographicallyby the residence of the LD case at the census tract
scale. Of the 833 LD casesobserved over this time period, all but
27 cases included a verifiable address(or census tract residential
indicator), including 3 in Genesee, 2 in Oakland, and22 in Wayne
County.
To test the water regime hypotheses, we exploited the temporal
andspatial properties of MDHHS case data to develop an outcome
variable, LDincidence, that is observable in time (before and after
the switch in waterregime) and space (in and outside regime and
chlorine-treated neighbor-hoods). LD incidence is a binary variable
equal to 1 if a confirmed case of LD isobserved in census tract i
in week t and 0 otherwise.
To estimate LD effects from the switch in water source and
treatment, andthe ensuing variability in chlorine residuals, we
also collected a suite ofdemographic and meteorological control
variables. With respect to neigh-borhood (census tract) demography,
two variables from the US Census Bu-reau are used: percent of
population receiving public assistance and percentof population ≥50
y of age. Both socioeconomic status and age (≥50 y) areknown
correlates of LD risk. Three county-level meteorological variables
areused: average weekly temperature, average weekly humidity, and
averageweekly precipitation. The thermal forces of temperature,
humidity, andprecipitation are known to govern the observed
seasonality of LD incidencerates through growth effects on
legionellae bacteria (25–27).
Capturing Water Regime Effects. To capture effects of changes to
source waterand treatment, or water regime, we deployed a
quasi-experimental methodcalled difference-in-differences. An
illustration of the method is summarizedin Table S2. Our first
difference is spatial, corresponding to whether a censustract is
located inside Flint (F), and therefore treated by the shift in
waterregime, or not in Flint (NF). Our second difference is
period-based, corre-sponding to whether a census tract is observed
before (A) or after (B) theswitch in water regime. The
difference-in-differences method infers a causaleffect by comparing
the difference between A and B on the outcome ofinterest (LD
incidence) for treated census tracts (F) relative to not
treatedcensus tracts (NF).
A key assumption of the difference-in-differences method, known
as theparallel paths requirement, posits that the average period
difference (A − B)in control group (NF) census tracts constitutes
the counterfactual averagedifference between A and B in F census
tracts if not for the treatment orswitch in water regime. In this
analysis, the preperiod parallel paths re-quirement is satisfied
(Supporting Information). The differential behavior ofLD incidence
rates in post-water regime switch period of Fig. S1 is indicativeof
a powerful place-specific period effect. Note in Fig. S1 the
extraordinaryincrease in the LD incidence rate in Genesee County.
Although it is analyt-ically tempting to conclude that the switch
in water regime governs the LDspike in Genesee, our analysis plan
aimed to rule out forces coincidental withthe regime switch,
evaluate plausible alternative explanations, and identifya
potential causal mechanism for the observed increase in LD in
GeneseeCounty.
Our analysis begins by identifying regime effects. In the regime
effectequations detailed below, our first difference is always
geographic, corre-sponding to whether a census tract is located in
Flint (and is therefore arecipient of Flint water) or is not in
Flint (either located in Oakland,Wayne, orparts of Genesee County
not in Flint). Our second difference is a period in-dicator that is
variously defined by whether or not parameters from a given
Fig. 4. LD incident risk in non-Flint census tracts by commuter
flow to Flint. LD incident risk is shown as a function of the
number of commuters from GeneseeCounty locations other than Flint
either before (navy) or after (maroon) the switch to the Flint
River as the Flint municipal water source. Probabilities
areestimated with all other model covariates fixed at their sample
means, and bars indicate 95% confidence intervals.
E1736 | www.pnas.org/cgi/doi/10.1073/pnas.1718679115 Zahran et
al.
http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalwww.pnas.org/cgi/doi/10.1073/pnas.1718679115
-
census tract are observed before the first switch in water
source (phase A),after the switch to the Flint River but before the
issuance of water qualityalerts (phase B), after the switch and
after the issuance of water qualityalerts (phase C), and after the
switch back to the DSWDwater supply (phaseD). Fig. 2A summarizes
the precise timing of each phase. Expectations ofparameter behavior
involving various statistical comparisons by phase aredescribed
below.
Water Regime Effects: Preswitch vs. Postswitch. We begin with a
more globaltest of a water regime effect, estimating a baseline
census tract randomeffects logistic equation for the probability of
census i in week t presentingwith a case of LD (1 = yes, and 0 =
no):
ProbðLDit = 1jFi , Pt ,Rit ,XiÞ
=Λ ½ β0 + β1Fi + β2Pt + δðFi × PtÞ+Γ1Rit +Γ2Xit + ζi �, [1]
where Λ½ · � is the cumulative distribution function (CDF) of
the logistic dis-tribution; Rit is a vector of temperature,
precipitation, and humidity mea-sures (from Weather Underground);
Xit is a vector of census tract controlvariables including
percentage of population ≥50 y of age and percent ofhouseholds
receiving public assistance (from US Census Bureau); ζi is
therandom effect of census tract i; Fi is an indicator variable = 1
if the censustract is in Flint; and Pt = 1 if the census tract is
observed in the postswitchperiod (combining phases B and C detailed
in Fig. 2A), with the treatmenteffect of the regime switch captured
by the estimated coefficient ðδÞ, con-stituting our
difference-in-differences of F and P. In the presentation of
logitmodel results below we exponentiate the estimated coefficient
δ to derivean odds ratio, with the expectation that expδ > 1
indicating that the switchfrom Detroit to Flint River water caused
an increase the risk of a census tractin Flint presenting with an
LD case.
Water Regime Effects: Division of the Postswitch Period. Next,
we test whetherboil water advisories issued by authorities in Flint
attenuated the risk of LD,providing an additional probe of whether
the switch in water regime causedthe observed spike in LD incidence
in Flint. We divide the postswitch periodinto two phases, B and C
(as detailed in Fig. 2A); compare LD outcomes incensus tracts in
phase B (after switch, before advisories) and phase C (afterswitch,
after advisories) to phase A (before the switch in water regime);
andthen compare outcomes in phase C to B. These comparisons assume
that theissuance of boil water advisories induced a meaningful
reduction in wateruse by residents. Boil advisories were not issued
to address the presence oflegionellae in the Flint water supply:
authorities issued advisories afterpositive tests for E. coli
contamination. However, the advisories may haveconfirmed suspicion
among residents that the drinking water was unsafe,thereby
unintentionally increasing water avoidance by residents. Twosources
indicate that the advisories meaningfully affected residential
waterexposure. First, Google Trend search interest data on water
contaminationin the Flint–Saginaw–Bay City metropolitan area
increased measurablyaround boil advisory dates, indicating
awareness of the official warningsamong the local population (see
ref. 19). Second, a large, statistically sig-nificant, and
sustained increase in sales of bottled water in Genesee
Countycorresponded with the issuance of advisories (18).
To examine whether advisories reduced LD risk (through a water
avoid-ance pathway), we estimate a census tract random effects
logistic equationfor the probability of census i in week t
presenting with an incidence of LD(1 = yes, and 0 = no):
ProbðLDit = 1jGCi , PBt , PCt ,Rit ,XiÞ
=Λ ½ β0 + β1Fi + β2PBt + β3PCt + δ1ðFi ×PBtÞ+ δ2ðFi ×PCtÞ+Γ1Rit
+Γ2Xit + ζi �,[2]
where all terms carry from Eq. 1, with the exception of PBt,
which is equal to1 if the census tract is observed in the
postperiod but before boil wateradvisories, and PCt, which assumes
a value of 1 if the census tract is observedin the postperiod and
after boil water advisories. The comparison of esti-mated
coefficients δ1 and δ2 indicates whether water avoidance behavior
ofresidents in Flint helped attenuate the LD outbreak and provides
support forthe water regime hypothesis. Insofar as waterborne
exposure to legionellaein Flint is linked to LD risk in a given
census tract in time, and boil wateradvisories helped to reduce LD
risk in Flint by inducing water avoidance inresident population, it
is expected that expδ1 > 1, expδ2 > 1, and expδ1 > expδ2
.
Water Regime Effects: Switch Back in Water Supply. We analyze
whether theswitch back in water supply on October 16, 2015, caused
a reduction in LD
incidence by estimating a census tract randomeffects logistic
equation for theprobability of census i in week t presenting with
an incidence of LD (1 = yes,and 0 = no):
ProbðLDit = 1jFi , PDt ,Rit ,XiÞ
=Λ ½ β0 + β1Fi + β2PDt + δ1ðFi × PDtÞ+Γ1Rit +Γ2Xit + ζi
�,[3]
where all terms carry from Eq. 1, with the exception of PDt
which is equal to1 if the census tract is observed in the switch
back period (phase D in Fig. 2A)and 0 if observed in the preswitch
period (phase A in Fig. 2A). The causaleffect of the switch back in
water regime is captured by the estimated co-efficient ðδÞ. Insofar
as the rise and fall of LD incidence in Flint was caused bya
city-wide failure in water treatment, this test is expected to
yield anexpδ ≈ 1, indicating that the switch back to Detroit water
returned the risk ofa census tract in Flint presenting with an LD
case to precrisis levels.
Chlorine Residual. Free chlorine (mg/L as Cl2) measurements at
eight moni-toring locations in Flint from 2013 to 2016 were
obtained from the MonthlyOperating Reports provided by the Flint
Water Department (SupportingInformation). Chlorine was measured at
each location two to three times perweek. Fig. 1B illustrates the
behavior of average free chlorine at the weeklytime step at each
monitor site. Vertical lines bisecting the space correspondto water
regime switch moments. Note the high between-monitor agreementin
the level of free chlorine in the preswitch period, indicating
negligiblespatial variation in water quality across the City of
Flint. In the postswitchperiod, we observe extraordinary temporal
(or within monitor) and spatial(or between monitor) variation in
the level of free chlorine.
Table S1 summarizes the statistical behavior of free chlorine
within andbetween monitors in time illustrated in Fig. 1B.
Analytically, the un-precedented exogenous variation in free
chlorine levels observed in Fig. 1Band Table S1 is what we exploit
to identify statistically the effect of changesin water quality on
LD incidence in Flint, MI.
Free Chlorine Data Assignment. To test the chlorine residual
hypothesis, weneeded to select a method for associating a location
in the City of Flint mapwith chlorine residual monitoring points.
Although a number of approachescould be used, we choose to develop
a physically relevant monitor-to-parcelassignment algorithm that
leverages best available information on parceloccupancy/vacancy,
residence time of water, and the Flint water distributionsystem
pipe network. We tried a number of common approaches,
includingvarious proximity and Thiessen polygon-based methods that
deliveredquantitatively similar results. A hydraulic-based chemical
transport model ofthe water distribution system could be used to
estimate free chlorine re-sidual. However, it is unclear if this
will have a meaningful effect on theresults given the spatial and
epidemiologic limitations of surveillance data.The algorithm begins
by finding the shortest path (or spine) from the cen-troid of each
parcel to the Flint Water Plant (FWP) via the pipe networkobeying
the water age gradient. The water age gradient used is
correlatedwith spatial variation in blood lead levels during the
switch in water supply(28), demonstrating the utility of this
metric to account for physical vari-ability within the water
distribution system. Water age is dynamic and likelyvaried
spatially during the study period. Utilizing the water age
gradienthelps to incorporate major hydraulic constraints that
proximity-basedmethods fail to accommodate (e.g., flow restrictions
due to pipe size). Thisresults in 41,286 parcel to FWP spines.
Next, the algorithm finds the shortestpath of each monitor to each
spine, again obeying the water age gradient.Each parcel is then
assigned the (weekly average) chlorine value of themonitor with a
spine juncture nearest to the parcel. Because LD incidencedata are
organized at the census tract scale, we average parcel chlorine
tothe census tract to generate 8,000 fully observed census tract
(i) by week (t)observations in Flint from 2013 to 2016. The outcome
of the monitor-to-parcel assignment algorithm is provided in Fig.
S2.
Effect of Free Chlorine. At adequate levels (commonly assumed to
be con-centrations ≥0.2 mg/L as Cl2), chlorine effectively
suppresses legionellaegrowth. Under normal circumstances, it is
near impossible to identify sta-tistically a chlorine residual →
legionellae → LD incidence pathway becauseof insufficient time and
space variation in chlorine within water distributionsystems. As
observed in Fig. 1B, the switch in water regime in Flint
inducedstriking temporal and spatial variation of free chlorine in
the Flint waterdistribution system. Our estimation strategy
analytically leverages this quasi-random behavior in free chlorine
throughout the city. We estimate a census
Zahran et al. PNAS | Published online February 5, 2018 |
E1737
ENVIRONMEN
TAL
SCIENCE
SPN
ASPL
US
http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1718679115/-/DCSupplemental
-
tract random effects logistic equation for the probability of a
census i inweek t presenting with an incidence of LD (1 = yes, and
0 = no):
ProbðLDit = 1jCit−1, Pt , PDt ,Rit ,XiÞ
=Λ ½ β0 + β1Cit−1 +Γ1Pt +Γ2PDt +Γ3Rit +Γ4Xit + ζi �, [4]
where all terms carry from Eqs. 1 and 3 with the exception Cit−1
denotingthe average weekly free chlorine (mg Cl2/L) at census tract
i in time t − 1. The1-wk lag in free chlorine is included to
account for the difference betweensymptom onset and referral date
information in MDHSS case data. Recall theuse of referral date
information was necessitated due to missing and im-precise data for
symptom onset date. In addition to a continuous measure offree
chlorine, we examine threshold effects of free chlorine, with Cit−1
=1 if < 0.5 mg/L or 1 in threshold models.
The census tract-specific residual, ζi, in the random effects
model is meantto capture the combined effect of all omitted census
tract-specific covariatesthat cause neighborhood variation in LD
susceptibility. Omitted variablesmay include the underlying health
frailty of residents or other sources ofwater chemistry parameters
that affect legionellae growth, such as iron, pH,water temperature,
or assimilable organic carbon. The census tract-specificrandom
effect measures the difference in LD risk in a given census
tractversus LD risk across all tracts in the City of Flint. Results
from a Hausmanspecification test (χ2 = 2.54,p= 0.96) indicate that
model coefficients areefficiently estimated by random as opposed to
census tract fixed effects.
Robustness Test: Hospital Hypothesis. To test the plausibility
of the hospital-based outbreak hypothesis, we recapitulate Eq. 1
through Eq. 4 but limitanalysis to non-hospital A-related LD cases.
Potential hospital A-related casesare identified by screening (i)
all cases in the MDHSS case file indicatingadmission to hospital A
and LD between 2014 and 2016 and/or whetherMDHHS staff, on the
basis of case analysis, override the reported admissionindication
and assign the case as a hospital A admission (n = 64) and (ii)
allnon-hospital A hospitalized cases with epidemiological
investigation notesindicating a prior admission to hospital A
between 2014 and 2016 (n = 19).All 19 cases in screen ii appear in
screen i, giving a total of 64 cases poten-tially related to
hospital A. Granting the hospital outbreak hypothesismaximum
explanatory power, we assume that all 19 cases with a prior
ad-mission to hospital A contracted LD at hospital A. Of the 45
cases remainingfrom screen i, all but 6 were returned to our
analysis pool because the recordedsymptom onset date was before the
hospital admission date. Adding 6 and 19gives 25 cases plausibly
resulting from a hospital-based outbreak.
By limiting the analysis to non-hospital A-related cases, we
test whetherestimated water regime and free chlorine suppression
effects appreciablychange. If hospital A-related cases fully govern
LD outcomes in Flint, then ourstatistical results pertaining to
water regime and loss of free chlorine effectsought to disappear.
However, if water regime and chlorine coefficients donot
appreciably change with the exclusion of hospital A-related LD
cases,
then it is highly unlikely that the LD spike in Flint resulted
from a hospital-based outbreak only. Although the hospital exposure
thesis is not incom-patible with our water regime/chlorine
hypothesis—the hospital is similarlydrawing water from a portion of
Flint’s water distribution system wherechlorine residual was often
very low—our case exclusion tests allow one torule out an
exclusively hospital-based argument.
The Genesee County (Outside of Flint) Epidemic. To test the
hypothesis that thesizeable increase in LD incidence in
neighborhoods (or census tracts) adjacent toFlint, in Genesee
County, were due to water exposure in Flint, we utilized
theLongitudinal Employer-Household Dynamics Employment Statistics
dataset(https://lehd.ces.census.gov/data/). This dataset estimates
that 15,857 workersflow into Flint every day, with 12,843 of them
residing in neighboring areas inGenesee County, constituting a
remarkable 61.7% of all employed personsworking inside Flint.
Although commuting data capture inflows for the pur-poses of work,
it is reasonable to assume exposure to the Flint water
distri-bution system through leisure and other activities as
well.
Restricting to not-Flint Genesee County census tracts, we test
the com-muter flow hypothesis by estimating the following census
tract randomeffects logistic equation for the probability of census
tract i in week t pre-senting with a case of LD (1 = yes, and 0 =
no):
ProbðLDit = 1jGCi , Pt ,Rit ,XiÞ
=Λ ½ β0 + β1GCi + β2Pt + δðGCi ×PtÞ+Γ1Rit +Γ2Xit + ζi �,[5]
where all terms carry from Eq. 1, with the exception of GC which
is equal tothe observed count of daily commuters to Flint
originating in non-FlintGenesee County census tract i. Insofar as
exposure to Flint water is thesource of the non-Flint outbreak, it
is expected that δ increases mono-tonically in GC.
ACKNOWLEDGMENTS. We are grateful for the assistance of all
members ofthe Flint Area Community Health and Environment
Partnership whichhelped guide the development of this manuscript.
Specifically, Marcus Zervos(Henry Ford) provided guidance on
epidemiologic surveillance and LD patho-genesis. Lead investigators
of this group not already identified include
(listedalphabetically): Carol Miller [Wayne State University
(WSU)], Jessica Robbins-Ruszkowski (WSU), Joanne Smith-Darden
(WSU), Judith Moldenhauer (WSU),Lara Treemore-Spears (WSU), Ben
Pauli (Kettering), Joanne Sobeck (WSU),Poco Kernsmith (WSU), Susan
Lebold (WSU), Tam E. Perry (WSU), Yongli Zhang(WSU), Matt Seeger
(WSU), and Laura Sullivan (Kettering). Mariana Runho andMohammed
Dardona (WSU) assisted in compiling the chlorine dataset. Thework
reported was supported by MDHHS under Contract 20163753-00
andNational Institute of Environmental Health Sciences of the
National Institutesof Health (NIH) under Award R21 ES027199-01. As
contractually mandated, themanuscript was submitted to the MDHHS
for review more than 30 d in ad-vance of being submitted for
publication. The content is solely the responsi-bility of the
authors and does not necessarily represent the official views of
theMDHHS or NIH.
1. Beer KD, et al. (2015) Surveillance for waterborne disease
outbreaks associated withdrinking water—United States, 2011–2012.
MMWR Morb Mortal Wkly Rep 64:842–848.
2. Collier SA, et al. (2012) Direct healthcare costs of selected
diseases primarily or par-tially transmitted by water. Epidemiol
Infect 140:2003–2013.
3. Liu G, et al. (2017) Potential impacts of changing
supply-water quality on drinkingwater distribution: A review. Water
Res 116:135–148.
4. Rosen MB, Pokhrel LR, Weir MH (2017) A discussion about
public health, lead andLegionella pneumophila in drinking water
supplies in the United States. Sci TotalEnviron
590–591:843–852.
5. Fonger R (October 13, 2014) General Motors shutting off Flint
River water at engineplant over corrosion worries. MLive. Available
at
www.mlive.com/news/flint/index.ssf/2014/10/general_motors_wont_use_flint.html.
Accessed December 6, 2017.
6. Muraca P, Stout JE, Yu VL (1987) Comparative assessment of
chlorine, heat, ozone,and UV light for killing Legionella
pneumophila within a model plumbing system.Appl Environ Microbiol
53:447–453.
7. Zhang Z, et al. (2009) Legionella control by chlorine dioxide
in hospital water systems.J Am Water Works Assoc 101:117–127.
8. Yabuuchi E, et al. (1995) An outbreak of Pontiac fever due to
Legionella pneumophilaserogroup 7. II. Epidemiological aspects.
Kansenshogaku Zasshi 69:654–665.
9. Ashbolt NJ (2015) Environmental (saprozoic) pathogens of
engineered watersystems: Understanding their ecology for risk
assessment and management. Pathogens4:390–405.
10. Cervero-Aragó S, Rodríguez-Martínez S, Puertas-Bennasar A,
Araujo RM (2015) Effectof common drinking water disinfectants,
chlorine and heat, on free Legionella andamoebae-associated
Legionella. PLoS One 10:e0134726.
11. Thomas V, et al. (2004) Amoebae in domestic water systems:
Resistance to disin-fection treatments and implication in
Legionella persistence. J Appl Microbiol 97:950–963.
12. Craun GF, et al. (2010) Causes of outbreaks associated with
drinking water in theUnited States from 1971 to 2006. Clin
Microbiol Rev 23:507–528.
13. Falkinham JO, 3rd, Hilborn ED, Arduino MJ, Pruden A, Edwards
MA (2015) Epidemi-ology and ecology of opportunistic premise
plumbing pathogens: Legionella pneu-mophila, Mycobacterium avium,
and Pseudomonas aeruginosa. Environ HealthPerspect 123:749–758.
14. Taylor M, Ross K, Bentham R (2009) Legionella, protozoa, and
biofilms: Interactionswithin complex microbial systems. Microb Ecol
58:538–547.
15. Davis ML (2010) Water and Wastewater Engineering: Design
Principles and Practice.Professional Edition (McGraw-Hill, New
York).
16. Great Lakes – Upper Mississippi River Board of State and
Provincial Public Health andEnvironmental Managers (2012)
Recommended Standards for Water Works (HealthResearch Inc, Albany,
NY).
17. World Health Organization (2014) Water Safety in
Distribution Systems (WHO, Geneva).18. Manske C, Hilbi H (2014)
Metabolism of the vacuolar pathogen Legionella and im-
plications for virulence. Front Cell Infect Microbiol 4:125.19.
Christensen P, Keiser DA, Lade GE (2017) Economic effects of
environmental crisis:
Evidence from Flint, Michigan (Iowa State University, Ames, IA),
Mimeo.20. Zahran S, McElmurry SP, Sadler RC (2017) Four phases of
the Flint water crisis: Evi-
dence from blood lead levels in children. Environ Res
157:160–172.21. American Water Works Association Disinfection
Systems Committee (2008) Commit-
tee report: Disinfection survey, Part 1-Recent changes, current
practices, and waterquality. J Am Water Works Assoc 100:76–90.
E1738 | www.pnas.org/cgi/doi/10.1073/pnas.1718679115 Zahran et
al.
https://lehd.ces.census.gov/data/http://www.mlive.com/news/flint/index.ssf/2014/10/general_motors_wont_use_flint.htmlhttp://www.mlive.com/news/flint/index.ssf/2014/10/general_motors_wont_use_flint.htmlwww.pnas.org/cgi/doi/10.1073/pnas.1718679115
-
22. Fonger R (February 16, 2017) CDC finds first genetic link
between Legionnaires’outbreak, Flint water. M Live. Available at
www.mlive.com/news/flint/index.ssf/2017/02/cdc_finds_first_genetic_link_b.html.
Accessed January 18, 2018.
23. AWWA Disinfection Systems Committee (2008) Committee report:
Disinfectionsurvey, Part 2-Alternatives, experiences, and future
plans. J Am Water WorksAssoc 100:110–124.
24. US Environmental Protection Agency (2008) FACTOIDS: Drinking
water and groundwater statistics for 2007 (US Environmental
Protection Agency, Office of Water,Washington, DC), EPA
816-K-07-004.
25. Garcia-Vidal C, et al. (2013) Rainfall is a risk factor for
sporadic cases of Legionellapneumophila pneumonia. PLoS One
8:e61036.
26. Garrison LE, et al. (2016) Vital signs: Deficiencies in
environmental control identifiedin outbreaks of Legionnaires’
disease–North America, 2000–2014. MMWR MorbMortal Wkly Rep
65:576–584.
27. Hicks LA, et al. (2007) Increased rainfall is associated
with increased risk for legion-ellosis. Epidemiol Infect
135:811–817.
28. Sadler RC, LaChance J, Hanna-Attisha M (2017) Social and
built environmental correlatesof predicted blood lead levels in the
Flint water crisis. Am J Public Health 107:763–769.
Zahran et al. PNAS | Published online February 5, 2018 |
E1739
ENVIRONMEN
TAL
SCIENCE
SPN
ASPL
US
http://www.mlive.com/news/flint/index.ssf/2017/02/cdc_finds_first_genetic_link_b.htmlhttp://www.mlive.com/news/flint/index.ssf/2017/02/cdc_finds_first_genetic_link_b.html