Embed Size (px)
Citation preview

Correction of Visual Impairment byCataract Surgery and Improved Survivalin Older PersonsThe Blue Mountains Eye Study Cohort
Calvin Sze-un Fong, MBBS,1 Paul Mitchell, MD, PhD,1 Elena Rochtchina, BSc, MAppStat,1
Erdahl T. Teber, BSc (Hon), PhD,1 Thomas Hong, BAppSc (Orthoptics), MScMed (ClinEpi),1
Jie Jin Wang, MMed, PhD1,2
Objective: We assessed whether correction of visual impairment (VI) by cataract surgery was associated withimproved long-term survival in an older Australian population.
Design: Population-based cohort study.Participants: In the Blue Mountains Eye Study, 354 participants, aged �49 years, had both cataract and VI
or had undergone cataract surgery before baseline examinations. They were subsequently examined after 5- and10-year follow-ups.
Methods: Associations between the mortality risk and the surgical correction of VI (visual acuity [VA] <20/40,attributable to cataract) were assessed in Cox proportional hazard regression models, after multivariate adjust-ment, using time-dependent variables for the study factor.
Main Outcome Measures: All-cause mortality.Results: The 15-year crude mortality of participants who had undergone cataract surgery at baseline with no
subsequent VI (71.8%) was relatively similar to that in participants with cataract-related VI who had not yetundergone surgery (79.4%). However, after adjusting for age and sex, participants who underwent cataractsurgery before baseline or during follow-up and no longer had VI had significantly lower long-term mortality risk(hazard ratio [HR], 0.60; 95% confidence interval [CI], 0.46e0.77) than participants with VI due to cataract whohad not undergone cataract surgery. This lower mortality risk in the group with surgically corrected VI (HR, 0.54;95% CI, 0.41e0.73) persisted after further adjustment for smoking, body mass index, home ownership, qualifi-cations, poor self-rated health, the presence of poor mobility, hypertension, diabetes, self-reported history ofangina, myocardial infarction, stroke, cancer, asthma, and arthritis. This finding remained significant (HR, 0.55;95% CI, 0.41e0.73) after additional adjustment for the number of medications taken (continuous variable) and thenumber (�5 vs. <5) of comorbid conditions (poor mobility, hypertension, diabetes, angina, myocardial infarction,stroke, cancer, asthma, or arthritis) as indicators of frailty.
Conclusions: Surgical correction of VI due to cataract was associated with significantly better long-termsurvival of older persons after accounting for known cataract and mortality risk factors, and indicators ofgeneral health. Whether some uncontrolled factors (frailty or general health) could have influenced decisions notto perform cataract surgery in some participants is unknown. However, this finding strongly supports manyprevious reports linking VI with poor survival.
Financial Disclosure(s): Proprietary or commercial disclosure may be found after the references. Ophthal-mology 2013;120:1720-1727 ª 2013 by the American Academy of Ophthalmology.
1
Visual impairment (VI), as defined in the United States asvisual acuity (VA) <20/40, has been shown to be associatedwith poor survival in older persons in a number ofstudies.2e7 Cardiovascular disease8 and physical disability,7or both,9 have been suggested to be factors on the pathwaylinking VI to increased mortality. Whether correcting VI inolder persons is associated with improved survival remainsinconclusive.10
A recent study by Blundell et al11 reported improvedsurvival in patients undergoing phacoemulsification cataractsurgery compared with people in the general population. If
1720 � 2013 by the American Academy of OphthalmologyPublished by Elsevier Inc.
VI were indeed associated with increased mortality in olderpersons,7 then its correction could be expected to beassociated with improved survival compared with that inpersons who remained visually impaired. In this report, weaimed to examine the relationship between correction ofVI by cataract surgery and long-term mortality risk ina subsample of an older Australian cohort, the BlueMountainsEyeStudy (BMES).Wecomparedmortality risk in participantswith cataract and VI: between persons who had undergonecataract surgery that corrected VI and persons who had not yetundergone surgery but who had persisting VI.
ISSN 0161-6420/13/$ - see front matterhttp://dx.doi.org/10.1016/j.ophtha.2013.02.009

Fong et al � VI Correction by Cataract Surgery and Long-term Survival
Methods
The BMES is a population-based cohort study of vision andcommon eye diseases in an older Australian population living ina suburban region west of Sydney. The study conduct adhered tothe tenets of the Declaration of Helsinki and was approved by theHuman Research Ethics Committee of the University of Sydney.All participants provided written informed consent for bothrecruitment and follow-up visits. Study procedures have beendescribed.12,13
Participants
Briefly, noninstitutionalized residents aged 49 years or older, whowere identified in a door-to-door census of the study area, wereinvited to attend detailed baseline eye examinations. Multiple call-back visits, including door-knocks, telephone reminders, andletters, were made to enhance the participation rate at baseline. Of4433 identified eligible residents of the 2 post-code areas, 3654(82.4%) participated in the baseline survey between 1992 and 1994(BMES I). All surviving participants were invited to be reexaminedafter 5 years (1997e1999, BMES II) and 10 years (2002e2004,BMES III). Participants who did not return to the 5-year visits alsowere invited to the 10-year visits. More than 75% of survivingparticipants were reexamined at each of the 5- and 10-year follow-up visits. To address our study question, we included in this reportthose BMES participants who had both cataract and VI, and thosewho had cataract surgery performed before the study baseline orduring the study follow-up period and whose VI had been cor-rected by the surgery. We excluded 32 baseline participants withlate age-related macular degeneration (AMD). Our study partici-pants had cataract surgery performed at public hospitals in NewSouth Wales, Australia, largely funded by the Medicare system,subsidized by the Australian Government, to which every taxpayer(both citizens and permanent residents) contributes a levy, or atprivate hospital/day surgery facilities, co-funded by both theparticipants and by private health insurance taken by them.
Measurements
The main outcome was deaths since the baseline examinations, upto December 31, 2007 (13e15 years), obtained via demographicdata linkage to Australian National Death Index (NDI) data.14,15 Aprobabilistic record linkage package was used to cross-match the 2datasets. Causes of death were provided by the NDI according tothe causes documented on death certificates based on the Interna-tional Classification of Diseases, 9th Revision, and the Interna-tional Statistical Classification of Diseases, 10th Revision.16,17
Australian NDI data were validated previously, with an estimatedsensitivity of 93.7% to 95% and specificity of 100% for all-causedeaths.14,15
Baseline phakic/pseudophakic status was defined by a history ofcataract surgery, confirmed at slit-lamp examination (BM900,Haag-Streit, Bern, Switzerland) and from grading slit-lamp photographs(SL-7E, Topcon Optical, Tokyo, Japan) and retroilluminationphotographs (CT-R, Neitz Instruments, Tokyo, Japan).18 Lensphotographic grading closely followed the Wisconsin cataractgrading system.19 Nuclear cataract was defined as grading level 4or 5 on a 5-level scale by comparison with 4 standard slit-lamplens photographs. Mild or substantial cortical cataract was definedas cortical opacity involving 5% to 24% or �25% of the lens area,respectively.18 Posterior subcapsular (PSC) cataract was graded asabsent or present, and then as mild (<5% of the lens area) orsubstantial (�5% of the lens area). Cataract was defined as at leastnuclear cataract standard photo 4, mild cortical cataract, or mildPSC cataract. Substantial cataract was defined to include cortical
opacity �25%, PSC cataract �5%, or nuclear cataract standardphoto 4 or greater.
Visual acuity was assessed at each visit. Presenting VA wasassessed using a logarithm of the minimum angle of resolutionchart and the participant’s habitual distance correction. Best-corrected VA was measured after subjective refraction. For eacheye, VA was recorded as the number of letters read correctly, from0 (<20/200) to 70 (20/10) letters. Presenting VI (PVI) was definedas VA <39 letters (<20/40) in the better eye, with or without thehabitual use of distance glasses, if worn. Best-corrected VI (BCVI)was defined as the same level after subjective refraction.20,21
The 2003 World Health Organization/International Society ofHypertension guidelines were used to define hypertension.22
Hypertension was defined by the use of antihypertensivemedication, a systolic blood pressure >140 mmHg, or a diastolicblood pressure >90 mmHg at baseline. Diabetes mellitus wasdefined by physician diagnosis or a fasting blood glucose level�126 mg/dl (�7.0 mmol/l) at the baseline study examination.Body mass index (BMI) at baseline was calculated as weight inkilograms divided by the square of height in meters, with a BMIless than 20 kg/m2 defined as low. Current smokers includedthose who had stopped smoking within the past year. Thepresence of difficulty in walking, termed “poor mobility,” wasdefined in participants who used a wheelchair or walking aidduring the study visit.
Home ownership, qualifications obtained, self-rated health andmedical history, were assessed using questionnaires baselineduring face-to-face interviews of all participants, performed bytrained interviewers. Higher education was defined as tertiaryqualifications after high school. Poor self-rated health was definedif participants rated their perceived health as fair or poor relativeto peers their age. Self-reported history of smoking, angina,myocardial infarction, stroke, cancer, asthma, gout, thyroiddisease, and number of regular medications used were recorded.Cardiovascular disease was defined by self-reported history ofangina or myocardial infarction. Categorized number of comorbidconditions (�5 vs. <5) included any of the following conditions:poor mobility, hypertension, diabetes, angina, myocardial infarc-tion, stroke, cancer, asthma, or arthritis.
Statistical Analysis
Statistical software (SAS version 9.2; SAS Inc, Cary, NC) wasused to perform survival analyses. The treatment group consistedof participants who underwent cataract surgery before baselineexaminations or during the study follow-up period, and in whomno VI (VA �20/40) was present at subsequent visits. Thenontreatment group consisted of participants who still had cataractand were visually impaired at follow-up examinations. The treat-ment state was a time-dependent variable and incorporated time-to-event from successful treatment (cataract surgery with no VI) to thecensored date, which was the date of death, survival until the endof 2007, or when they were found to have VI again at any follow-up examination. Participants found to have been deceased using theNDI linkage, but had no confirmed date of death (n¼4), wereexcluded from analyses.
Cox proportional hazard regression models were conducted toassess mortality risk over 13 to 15 years between the treatment andnontreatment groups. Co-variables were checked for violations ofthe proportional hazard ratio (HR) assumption using 2 methods:Schoenfeld residuals and Pearson correlation coefficients, andinteractions between log-survival time and the co-variable. In allanalyses, P values of �0.05 were used to identify assumptionviolation. Because age and sex were found to violate theassumption, both age and sex strata were used in Cox regressionmodels. Three Cox survival models were generated. The first
1721

Ophthalmology Volume 120, Number 9, September 2013
model adjusted for baseline age and sex. The second model alsoadjusted for individual potential confounding factors: smokingstatus, BMI, home ownership, qualifications, poor self-rated health,presence of poor mobility, hypertension, diabetes, self-reportedhistory of angina, myocardial infarction, stroke, cancer, asthma,and arthritis. The third model adjusted for all variables contained inthe second model plus known indicators of poor general health andfrailty: the number of medications taken (as a continuous variable)and the number (�5 vs. <5) of comorbid conditions.23 MortalityHRs are presented with 95% confidence intervals (CIs).Statistical significance was defined as a P value <0.01.
Fifteen-year crude mortality rates were calculated for both thebaseline treatment and nontreatment groups. Survival curves ofbaseline participants, who had cataract surgery performed beforetheir baseline with no residual VI (�20/40) or who still had cata-ract with persisting VI at baseline, were plotted using estimatesfrom the second model, using the method by Zhang et al.24
Supplementary analyses were conducted using (1) best-correctedVA to define VI, in addition to PVI; and (2) analyses confined toparticipants with substantial cataract, rather than any cataract.
Results
There were 170 participants who had undergone cataract surgerybefore baseline and who had no residual VI at baseline, and 184participants who still had both cataract and VI due to cataract atthis time. Among these 184 subjects, 21 had cataract surgeryduring the follow-up period from BMES I to BMES III (endingSeptember 2004). These increased the number who had cataractsurgery with no residual VI from 170 to 191 and reduced thenumber who still had both cataract with VI due to cataract over thefollow-up period from 184 to 163 (Fig 1). Of these 354 (170þ184)baseline participants, 154 (72.3% of 213 survivors) survived untilthe 5-year examinations (BMES II) and 87 (61.7% of 141 survi-vors) survived until the 10-year examinations (BMES III)(Table 1).
The 5-year follow-up rate was 61.8% (n ¼ 105) among the 170participants who had previous cataract surgery with no residual VIat baseline and 26.6% (n ¼ 49) among the 184 participants whohad both cataract and VI due to cataract at baseline. There were anadditional 20 subjects who were still alive but who did not return toeither the 5- or 10-year examinations. Figure 1 shows the numbersof participants who did or did not attend the baseline and follow-upvisits.
Of the 184 participants with unoperated cataract and VI atbaseline, 113 (61%) had substantial cataract. Table 2 shows thatthere were more female than male participants in the group withboth cataract and persisting VI than the group with cataractsurgery with no residual VI (P ¼ 0.037).
By late 2007, 268 (76%) of the 354 participants had died. Themean follow-up period among the 86 survivors was 13.2 years(standard deviation, 3.6). Apart from a slightly higher proportionwith home ownership among surviving participants who returned(98%) compared with those who were lost to follow-up (85%,P ¼ 0.012), there was no difference in baseline characteristicsbetween the 2 groups (Table 3).
The 15-year crude mortality of the baseline treatment group(participants who had cataract surgery with no residual PVI)(71.8%; 95% CI, 64.4e78.4) was relatively similar to that of thebaseline nontreatment group (those who had cataract causing PVIbut who had not yet had surgery) (79.4%; 95% CI, 72.8e85.0).However, after adjusting for age, sex, smoking, BMI, homeownership, qualifications, poor self-rated health, the presence ofpoor mobility, hypertension, diabetes, self-reported history of
1722
angina, myocardial infarction, stroke, cancer, asthma, and arthritis,compared with the treatment group who had undergone cataractsurgery before baseline, subjects in the nontreatment group atbaseline had progressively poorer long-term survival (Fig 2).
By using time-dependent variables for VI and cataract surgicalstatus to include incident cataract surgical cases in which VI wassurgically corrected over the follow-up period, and after adjustmentfor age and sex in the Cox models, the treatment group had a 40%reduction in mortality risk using PVI or BCVI measures. Forcorrection of PVI, the HR was 0.60 (95% CI, 0.46e0.77), and forcorrection of BCVI, the HR was 0.57 (95% CI, 0.39e0.83)compared with the nontreatment group.
Age, sex, smoking, poor self-reported health, poor mobility,diabetes, and history of stroke were significantly associated withmortality (P< 0.05) in the second model, and other remaining co-variables were not significant but forced into the model. Thelower mortality risk association with the surgical correction of VIpersisted after further adjustment for all the individual co-variablesin the second model. For correction of PVI, the HR was 0.54(95% CI, 0.41e0.73). For correction of BCVI, the HR was 0.55(95% CI, 0.35e0.87), shown in Table 4. Likewise, the samevariables (age, sex, smoking, poor self-reported health, poormobility, diabetes, and history of stroke) plus number of medicationsused were the significant co-variables (P< 0.05) in the third model.After adjusting for all the individual and grouped indicators ofgeneral health and frailty in the third model, the lower mortality riskin the treatment group remained significant. For PVI that wassurgically corrected, the HR was 0.55 (95% CI, 0.41e0.73), whereasfor BCVI that was surgically corrected, the HR was 0.55 (95% CI,0.35e0.86) compared with the nontreatment group.
Analyses confined to participants with substantial cataractshowed that the protective association of cataract surgery withreduced mortality remained significant in all 3 Cox models(Table 4).
Discussion
In light of the consistent evidence showing that olderpersons with VI are likely to have greater mortality thantheir age peers without VI,3e7,25,26 we aimed to address thecritical question of whether cataract surgery to correct VI isassociated with improved survival among older persons withVI. We found that, after adjusting for factors that wereassociated with mortality, older persons who had VI due tocataract that was corrected by cataract surgery had anapproximately 40% lower mortality risk over the long-term(15 years), compared with that in older persons whoremained visually impaired because of cataract. The asso-ciation was independent of indicators of general health andfrailty, including poor self-rated health, number of medica-tions, and number of comorbid conditions.23,27 Our findingsprovide further support to the VIemortality associationpreviously observed in multiple studies.3e7 The exactmechanisms explaining this observed association remain tobe understood, although they are highly likely to be indirectvia other factors or pathways.7,9,28,29 Plausible factors orpathways may include physical and emotional well-being,optimism, and improved confidence associated with inde-pendent living after correcting cataract-related VI.
Walker et al30 previously reported that cataract surgeryimproved not only visual function but also the domains of

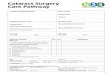
Figure 1. Participants included in this study: participants with both cataract and visual impairment (VI) (n ¼ 163) and those with cataract surgeryperformed before the study baseline (n ¼ 170) or during the study follow-up period (n ¼ 21) and who had no VI after surgery (total n ¼ 191) in the BlueMountains Eye Study (BMES). AMD ¼ age-related macular degeneration.
Fong et al � VI Correction by Cataract Surgery and Long-term Survival
disability and dependency. However, findings linkingcataract surgery to subsequent mortality have beeninconsistent.3,31e35 All previous studies compared subjectswho had cataract surgery with subjects in the general pop-ulation31e33 or patients who had not had cataract surgery forcataract that might or might not be visually impairing.3,34,35
These previous studies addressed the question of whethercataract surgery was associated with better survival in the
Table 1. Numbers and Proportions of Surviving Baseline ParticipantsWhose Cataract and Visual Impairment Were Present at Both Baselin
Eye Stu
BMES Baseline (1992e1n (%)
Participants with cataract surgery and no VI 170 (48.0)Participants with both cataract and VI 184 (52.0)Total 354 (100)
BMES ¼ Blue Mountains Eye Study; VI ¼ visual impairment.*Numbers exclude 20 participants who were alive but did not return to the 5-
older population, whereas we address a slightly differentquestion in the current study, which is whether correction ofVI (likely due to cataract) via cataract surgery is associatedwith better survival among older persons with both VI andcataract. Therefore, our study findings are not directlycomparable to findings from previous studies.3,31e35
In a prospective study by McGwin et al10 of 384participants aged �55 years, 98 were cataract-free with no
Who Had Cataract Surgery and No Visual Impairment and Thosee and Last Known Follow-up Examinations of the Blue Mountainsdy
994) BMES 5-Yr Follow-up*n (%)
BMES 10-Yr Follow-up*n (%)
105 (68.2) 67 (77.0)49 (31.8) 20 (23.0)154 (100) 87 (100)
or 10-yr examinations.
1723

Table 2. Baseline Demographic and Health Characteristics of the Blue Mountains Eye Study Subsamples by Participants Who HadCataract and Visual Impairment and Those Who Had Prior Cataract Surgery with No Visual Impairment
Characteristic n*
Cataract Status, n (%)
Unadjusted P ValueUnoperated Cataract N ¼ 184 Prior Cataract Surgery N ¼ 170
Age, mean � SD, yrs 354 76.6�8.4 75.1�8.7 0.10Female 354 119 (64.7) 90 (52.9) 0.037y
Current smokerz 331 15 (8.7) 19 (12.0) 0.51BMI <20 kg/m2 333 21 (11.9) 15 (9.6) 0.83Hypertension 349 140 (76.5) 134 (80.7) 0.19Diabetes mellitus 354 15 (8.2) 27 (15.9) 0.079Cardiovascular disease 354 48 (26.1) 36 (21.2) 0.21Stroke 352 16 (8.7) 13 (7.7) 0.64Cancer 354 23 (12.5) 18 (10.6) 0.60Poor mobilityx 354 38 (20.7) 27 (15.9) 0.52Fair or poor self-rated health 341 54 (30.3) 51 (31.3) 0.82Home ownership 354 150 (81.5) 148 (87.1) 0.24Higher education 316 75 (44.9) 79 (53.0) 0.23�5 comorbid conditionsk 354 12 (6.5) 7 (4.1) 0.32�8 regular medications 354 23 (12.5) 15 (8.8) 0.28
BMI ¼ body mass index; SD ¼ standard deviation.*Excludes missing data.yAdjusted for age for comparison of female proportion.zIncluding participants who gave up smoking <1 yr before the baseline examinations.xExaminer assessed.kComorbid conditions included poor mobility, hypertension, diabetes, angina, myocardial infarction, stroke, cancer, asthma, and arthritis.
Ophthalmology Volume 120, Number 9, September 2013
VI (VA >20/40) and 286 had cataract with VA �20/40. Ofthe 286 participants with cataract, 200 and 86 elected to haveor not to have cataract surgery, respectively. The authorsfound that participants with cataract and VI who did not electto have cataract surgery had a 3-fold greater mortality riskover 6 years compared with those who were cataract-freewith no VI, after adjusting for age, sex, race, education,chronic medical conditions, smoking, drinking, depression,and cognitive status.10 Participants with cataract and VI whodid not elect to have cataract surgery could have had otherhealth problems that prevented them from undergoing
Table 3. Comparison of Baseline Characteristics of the Surviving SubsThose Who Were Followed and Tho
Characteristics n*
Follo
Returned to the 5- or 10-YrExamination, N ¼ 66
Age, mean � SD, yrs 86 68.3�7.8Female 86 43 (65)PVI (VA <20/40) 86 28 (42)Diabetes mellitus 86 6 (9)Cardiovascular disease 86 9 (14)Poor mobilityy 86 2 (3)Fair or poor self-rated health 85 13 (20)Home ownership 86 65 (98)Higher education 79 34 (53)
PVI ¼ presenting visual impairment; SD ¼ standard deviation; VA ¼ visual a*Excludes missing data.yExaminer assessed.
1724
surgery, and these other health problems could also explainthe poorer survival in this group. The study by McGwinet al10 did not demonstrate improved survival amongparticipants who had cataract and low vision who elected tohave cataract surgery.
Strengths of our study include its long-term follow-up ofa well-documented older cohort, the standardized methodsused to measure VA and to document cataract and cataractsurgery, the use of time-dependent variables for cataractsurgical status, and the control for a large number ofpotential confounders in multivariate Cox regression
ample (n ¼ 86) of Blue Mountains Eye Study Participants betweense Who Were Lost to Follow-up
w-up Status, n (%)
Unadjusted P ValueDid Not Return to Either of the 2
Examinations, N ¼ 20
70.8�9.0 0.2317 (85) 0.09010 (50) 0.551 (5) 0.563 (15) 0.882 (10) 0.195 (25) 0.6317 (85) 0.0125 (33) 0.17
cuity.

Figure 2. Survival curves by baseline participants who had prior cataractsurgery and no visual impairment (VI) and those who had both cataractand VI present (not treated), after adjustment for age, sex, smoking, bodymass index (BMI), home ownership, qualifications, poor self-rated health,presence of poor mobility, hypertension, diabetes, self-reported history ofangina, myocardial infarction, stroke, cancer, asthma, and arthritis.
Fong et al � VI Correction by Cataract Surgery and Long-term Survival
models. Late AMD is an alternative cause of VI in partici-pants with cataract. To reduce the confounding effect ofAMD-related VI in our analysis, 32 baseline participantswith late AMD were excluded. The survival benefit ofcataract surgery with no subsequent VI was similar before orafter adjustment for factors known to be associated withpoor survival. These results may suggest that the benefit ofimproved survival from correcting VI via cataract surgerymay be independent of these known mortality risk factors.However, there are likely to be many other factors associ-ated with poor survival that we did not measure and
Table 4. Mortality Hazard Ratios of Participants Who Had Prior CCataract and Visual Impairm
Participants, n* Deceased, n (%)
PVI Any cataractx
Cataract surgery and no PVI 191 130 (68.1)Cataract and PVI 163 138 (84.7)Substantial cataractx
Cataract surgery and no PVI 183 127 (69.4)Substantial cataract and PVI 100 91 (91)
BCVI Any cataractx
Cataract surgery and no BCVI 191 138 (72.3)Cataract and BCVI 45 42 (93)Substantial cataractx
Cataract surgery and no BCVI 190 137 (72.1)Substantial cataract and BCVI 33 32 (97)
BCVI ¼ best-corrected visual impairment; BMI ¼ body mass index; CI ¼ conpresenting visual impairment; VI ¼ visual impairment.*Numbers reflect cataract surgery status before baseline or over the follow-up pySecond model adjusted for baseline age, sex, smoking status, BMI, home owhypertension, diabetes, self-reported histories of angina, myocardial infarction,zThird model adjusted for all the variables in the second model plus number ofcomorbid conditions (poor mobility, hypertension, diabetes, angina, myocardiaxAny cataract was defined as one or more of the following: (1) nuclear cataractcortical cataract �5% of the lens area involved, (3) PSC cataract of any lensopacity �25%, PSC cataract �5%, or nuclear cataract standard photo 4 or gre
therefore have not adjusted for. Visual impairment couldhave been a surrogate of these unknown factors.
Study Limitations
Our study has a number of limitations, including the rela-tively small number of subjects. Of the 354 participants atbaseline, 6% (n ¼ 20) were lost to follow-up without furtherinformation about cataract surgical status since baseline,although information about the date of death was availablefor all but 4 baseline participants. Potential misclassificationin the death data is highly unlikely. We noticed that a higherproportion of subjects returned to the 5-year follow-up visitsamong those who had undergone surgery (61.8%) thanthose who had VI and still had not undergone surgery(26.6%). This suggests some differential in the follow-uprates between participants who had and those who had notundergone cataract surgery. Nevertheless, we obtainedmortality information (the study outcome) from theAustralian NDI, a reliable linked dataset, which coversdeath information for all Australians, regardless of whetherthe participant was followed in our study or their domicile inAustralia. Differential follow-up rates between participantswho had and those who had not yet undergone cataractsurgery at baseline may have potentially biased our findings,but this would have likely been toward the null. This isbecause some participants who did not return to follow-upvisits could have had cataract surgery performed else-where but were classified as nonsurgical cases because wewere not aware of their surgical status. This could havemisclassified both surgical (surgical vs. nonsurgical) casesand VI (VI vs. no VI) groups.
ataract Surgery and No Visual Impairment versus Those Whoseent Were Both Present
Age- and Sex-AdjustedHR (95% CI)
Multivariate-AdjustedHR (95% CI)y
Multivariate-AdjustedHR (95% CI)z
0.60 (0.46e0.77) 0.54 (0.41e0.73) 0.55 (0.41e0.73)
0.58 (0.43e0.77) 0.53 (0.38e0.74) 0.53 (0.38e0.75)
0.57 (0.39e0.83) 0.55 (0.35e0.87) 0.55 (0.35e0.86)
0.52 (0.34e0.80) 0.53 (0.32e0.89) 0.53 (0.32e0.88)
fidence interval; HR ¼ hazard ratio; PSC = posterior subcapsular; PVI ¼
eriod.nership, qualifications, poor self-rated health, presence of poor mobility,stroke, cancer, asthma, and arthritis.medications taken (as a continuous variable) and number (�5 vs. <5) ofl infarction, stroke, cancer, asthma, or arthritis).standard photo 4 or greater of the Wisconsin cataract grading system, (2)area involvement; substantial cataract was defined as presence of corticalater.
1725

Ophthalmology Volume 120, Number 9, September 2013
Differential access to health care services is mitigated tosome extent in Australia, where all citizens and permanentresidents are covered by Medicare. Causation is not impliedin our findings, rather, the observed association could relateto some unmeasured confounding variables in addition tothe many variables already adjusted for.
Presenting VI in the better eye was used in our studybecause it is considered the habitual vision that participantshave in daily life. When BCVI was used, the significantfinding of lower mortality among those with VI correctionvia cataract surgery was unaltered. Although trained inter-viewers ensured uniformity in asking questions during theface-to-face interview, self-reported medical history datawithout validation from medical records could have reducedreliability and accuracy.
In conclusion, data from a subsample of a population-based older cohort not only strongly support previouslydocumented significant associations between VI andincreased mortality among older persons but also strengthenthis association by showing that the correction of VI viacataract surgery seems to be associated with lower long-termmortality risk by 40% among older persons who had VI dueto cataract. Further prospective studies to confirm thisbenefit from correcting VI among older persons are needed.If confirmed, this has an important message to ophthal-mologists that correcting VI in their daily practice likelyresults in better outcomes for patients beyond the eye andvision. It would confirm the focus on cataract surgery by theVision 2020 initiative and justify an expansion of eye healthcare provision to the older sector of the population. Furtherstudies are needed to explore the underlying mechanisms forthis effect, if demonstrated in other studies.
References
1. Eye Diseases Prevalence Research Group. Causes and preva-lence of visual impairment among adults in the United States.Arch Ophthalmol 2004;122:477–85.
2. Appollonio I, Carabellese C, Frattola L, Trabucchi M. Effectsof sensory aids on the quality of life and mortality of elderlypeople: a multivariate analysis. Age Ageing 1996;25:89–96.
3. Wang JJ, Mitchell P, Simpson JM, et al. Visual impairment,age-related cataract, and mortality. Arch Ophthalmol2001;119:1186–90.
4. McCarty CA, Nanjan MB, Taylor HR. Vision impairmentpredicts 5 year mortality. Br J Ophthalmol 2001;85:322–6.
5. AREDS Research Group. Associations of mortality withocular disorders and an intervention of high-dose antioxidantsand zinc in the Age-Related Eye Disease Study: AREDSreport no. 13. Arch Ophthalmol 2004;122:716–26.
6. Knudtson MD, Klein BE, Klein R. Age-related eye disease,visual impairment, and survival: the Beaver Dam Eye Study.Arch Ophthalmol 2006;124:243–9.
7. Karpa MJ, Mitchell P, Beath K, et al. Direct and indirecteffects of visual impairment on mortality risk in older persons:the Blue Mountains Eye Study. Arch Ophthalmol 2009;127:1347–53.
8. Thiagarajan M, Evans JR, Smeeth L, et al. Cause-specificvisual impairment and mortality: results from a population-based study of older people in the United Kingdom. ArchOphthalmol 2005;123:1397–403.
1726
9. Kulmala J, Era P, Tormakangas T, et al. Visual acuity andmortality in older people and factors on the pathway.Ophthalmic Epidemiol 2008;15:128–34.
10. McGwin G Jr, Owsley C, Gauthreaux S. The associationbetween cataract and mortality among older adults.Ophthalmic Epidemiol 2003;10:107–19.
11. Blundell MS, Hunt LP, Mayer EJ, et al. Reduced mortalitycompared to national averages following phacoemulsificationcataract surgery: a retrospective observational study. Br JOphthalmol 2009;93:290–5.
12. Mitchell P, Smith W, Attebo K, Wang JJ. Prevalence of age-related maculopathy in Australia. The Blue Mountains EyeStudy. Ophthalmology 1995;102:1450–60.
13. Attebo K, Mitchell P, Smith W. Visual acuity and the causesof visual loss in Australia. The Blue Mountains Eye Study.Ophthalmology 1996;103:357–64.
14. Powers J, Ball J, Adamson L, Dobson A. Effectiveness of theNational Death Index for establishing the vital status of olderwomen in the Australian Longitudinal Study on Women’sHealth. Aust N Z J Public Health 2000;24:526–8.
15. Magliano D, Liew D, Pater H, et al. Accuracy of the AustralianNational Death Index: comparison with adjudicated fataloutcomes among Australian participants in the Long-termIntervention with Pravastatin in Ischaemic Disease (LIPID)study. Aust N Z J Public Health 2003;27:649–53.
16. ICD-9-CM: International Classification of Diseases, ClinicalModification. 4th ed. 9th rev. Geneva: World Health Organi-zation; 1991.
17. ICD-10: International Statistical Classification of Diseases andRelated Health Problems. 10th rev. Geneva: World HealthOrganization; 1992.
18. Mitchell P, Cumming RG, Attebo K, Panchapakesan J. Prev-alence of cataract in Australia: the Blue Mountains Eye Study.Ophthalmology 1997;104:581–8.
19. Klein BE, Klein R, Linton KL, et al. Assessment of cataractsfrom photographs in the Beaver Dam Eye Study. Ophthal-mology 1990;97:1428–33.
20. Correctable visual impairment among persons with dia-beteseUnited States, 1999-2004. MMWR Morb Mortal WklyRep 2006;55:1169–72.
21. Kuang TM, Tsai SY, Hsu WM, et al. Correctable visualimpairment in an elderly Chinese population in Taiwan: theShihpai Eye Study. Invest Ophthalmol Vis Sci 2007;48:1032–7.
22. World Health Organization, International Society of Hyperten-sion Writing Group. 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement onmanagement of hypertension. J Hypertens 2003;21:1983–92.
23. Klein BE, Klein R, Knudtson MD, Lee KE. Frailty, morbidityand survival. Arch Gerontol Geriatr 2005;41:141–9.
24. Zhang X, Loberiza FR, Klein JP, Zhang MJ. A SAS macro forestimation of direct adjusted survival curves based on a strati-fied Cox regression model. Comput Methods Programs Bio-med 2007;88:95–101.
25. Reuben DB, Mui S, Damesyn M, et al. The prognostic value ofsensory impairment in older persons. J Am Geriatr Soc1999;47:930–5.
26. Klein R, Klein BE, Moss SE. Age-related eye disease andsurvival. The Beaver Dam Eye Study. Arch Ophthalmol1995;113:333–9.
27. Bharucha AJ, Pandav R, Shen C, et al. Predictors of nursingfacility admission: a 12-year epidemiological study in theUnited States. J Am Geriatr Soc 2004;52:434–9.
28. Lam BL, Christ SL, Lee DJ, et al. Reported visual impairmentand risk of suicide: the 1986-1996 national health interviewsurveys. Arch Ophthalmol 2008;126:975–80.

Fong et al � VI Correction by Cataract Surgery and Long-term Survival
29. Christ SL, Lee DJ, Lam BL, et al. Assessment of the effect ofvisual impairment on mortality through multiple health path-ways: structural equation modeling. Invest Ophthalmol Vis Sci2008;49:3318–23.
30. Walker JG, Anstey KJ, Hennessy MP, et al. The impact ofcataract surgery on visual functioning, vision-related disabilityand psychological distress: a randomized controlled trial. ClinExperiment Ophthalmol 2006;34:734–42.
31. Ninn-Pedersen K, Stenevi U. Cataract patients in a definedSwedish population 1986e90: VII Inpatient and outpatientstandardised mortality ratios. Br J Ophthalmol 1995;79:1115–9.
32. Meddings DR, Marion SA, Barer ML, et al. Mortality ratesafter cataract extraction. Epidemiology 1999;10:288–93.
33. McKibbin M, Mohammed M, James TE, Atkinson PL. Short-term mortality among middle-aged cataract surgery patients.Eye (Lond) 2001;15:209–12.
34. Klein R, Klein BE, Moss SE, Cruickshanks KJ. Association ofocular disease and mortality in a diabetic population. ArchOphthalmol 1999;117:1487–95.
35. Borger PH, van Leeuwen R, Hulsman CA, et al. Is there a directassociation between age-related eye diseases and mortality? TheRotterdam Study. Ophthalmology 2003;110:1292–6.
Footnotes and Financial Disclosures
Originally received: September 5, 2012.Final revision: January 10, 2013.Accepted: February 11, 2013.Available online: May 9, 2013. Manuscript no. 2012-1362.1 Centre for Vision Research, Department of Ophthalmology and West-mead Millennium Institute, University of Sydney, Sydney, Australia.2 Centre for Eye Research Australia, University of Melbourne, Melbourne,Australia.
Financial Disclosure(s):The author(s) have made the following disclosure(s): C.S.F. has receiveda travel fellowship grant from the Centre for Eye Research Australia (2010);P.M. serves on Advisory Boards for Novartis and Bayer, receiving
consultancy fees and payment for lectures from these companies; J.J.W. isfunded by a National Health & Medical Research Council Senior ResearchFellowship (2005e2014); the rest of the authors have no conflicts ofinterest to disclose.
Supported by the National Health & Medical Research Council, Canberra,Australia (Grants 932085, 974159, 211069, and 457349). The fundingorganization had no role in the design or conduct of this research.
Correspondence:Jie Jin Wang, MMed, PhD, Centre for Vision Research, WestmeadMillennium Institute (University of Sydney), Westmead Hospital, Haw-kesbury Road, Westmead, NSW Australia, 2145. E-mail: [email protected].
1727