Embed Size (px)
Citation preview
CORRECTION OF SPASTIC ENTROPION 657
oval and also the fine very opaque radiate stripes, in relation to these spots, have diminished in number.
d. Circular patterns no longer predominate, but radiate patterns frequently occur; indeed, radiate canalicular and slightly tortuous stripes appear. They are strongly white because of the very heavy contrast-intensity (fig. 2) .
We may wonder if these stripes are collector channels of enlarged clefts that debouch into the orifices previously described (white spots), or if they represent a change in the direction of the trabecular clefts following a structural modification. The first hypothesis seems to us to be the more plausible.
The treatment of spastic or senile entropion, though occupying a small place in the field of ophthalmology and ophthalmic surgery, is nevertheless a perplexing, and often disappointing, challenge to the ophthalmologist. The procedure for correction of spastic entropion which is here reported, though not widely known, was first described in the fall
* From the Manhattan Eye, Ear, and Throat Hospital. Presented before the New York Academy of Ophthalmology, Section of Ophthalmology, March, 1955.
CONCLUSIONS
From our observations, we may conclude : 1. That the trabecular clefts and their
orifices at the level of the inner wall of Schlemm's canal are enlarged but only in a very poor manner.
2. That the permeability of the connective tissue, building up the trabeculae, has increased.
3. That there is no evidence that new orifices are added to those already existing, but that the passage of the contrast fluid occurs in a more direct manner.
2, Avenue Pasteur.
of 1953 and later published in June, 1954.1
On the basis of the excellent results reported, and in view of the fact that previous methods for the correction of spastic entropion have too often been disappointing, an endeavor has been made to collect a series of cases over the past 16 months which were operated by the method proposed by Dr. F. A. Wies.
Though many factors are involved in the production of senile or spastic entropion, it is reasonable to conclude as Kettesy2 pointed
REFERENCES
Bârâny, E. H. : In vitro studies of the resistance to flow through the angle of the anterior chamber. Acta Soc. Med. Upsala, 59:260-276, 1954.
Bârâny, E. H., and Scotchbrook, S.: Influence of testicular hyaluronidase on the resistance to flow through the angle of the anterior chamber. Acta Physiol. Scand., 30:240-248, 1954.
Bârâny, E. H. : Discussion to Huggert, A. : Experiments to determine the pore size in the filter of the angle of the anterior chamber. Nordic Congress Goteborg, June, 1954.
Collette, J. M. : Etude radiologique de la circulation plasmo-tissulaire par injection sous-cutanée de substance de contraste. Rev. Méd. de Liege, 8:776-787, 1953.
François, J., Collette, J. M., and Neetens, A. : Etude microradiographique de la paroi interne du canal de Schlemm. J. belge de Radiol., 38:1-15, 1955.
François, J., Neetens, A., and Collette, J. M. : Microradiographic study of the inner wall of Schlemm's canal. Am. J. Ophth., 40:491, 1955.
François, J., Rabaey, M., and Neetens, A. : Perfusion studies about the outflow of aqueous humour in human eyes. Arch. Ophth. In press.
CORRECTION O F SPASTIC ENTROPION*
BY THE METHOD PROPOSED BY W I E S
DONALD C. MCFARLANE, M.D. London, Ontario
658 DONALD C. McFARLANE
out in 1948 that the prime factor is a drawing up and accumulation of bundles of the palpebrai portion of the orbicularis muscle in the lid margin, secondary to a slackening and atrophy of the palpebrai connective tissue. The entropion occurs on contraction of the muscle and is not likely to be self-reducing, since the corneal irritation so produced often sets up a secondary spasm which may be severe.
Duke-Elder3 points out that the palpebrai orbicularis forms two arcs as it lies in its normal anatomic relationship against the lower tarsal plate. The concavity of one arc is directed posteriorly, that of the other superiorly. Contraction of the muscle, therefore, has the effect of reducing these two arcs to chords and, in the absence of normal connective tissue support, the muscle bundles accumulate in the lid margin and have a posterior direction of force.
Operations for the correction of spastic entropion should, therefore, be directed toward preventing this upward riding of the muscle bundles over the tarsus. This can be accomplished in one of several ways :
First, by re-establishing the absent pressure of the muscle on the convexity of the lower tarsal plate, as exemplified by the Wheeler technique.
Second, by producing fibrous tissue adhesions between the muscle and the tarsal plate, which is the primary purpose of the Ziegler cautery and a secondary effect of practically all of the many methods which employ a surgical incision through the muscle.
Third, by producing an actual tissue barrier which divides the muscle, and, therefore, will not permit migration of its lower fibers into the lid margin. This is the purpose of the Wies procedure.
Other principles have been proposed, such' as increasing the tone of the tarso-orbital fascia and even complete excision of the palpebrai and part of the orbital portions of the orbicularis. These procedures do not, however, attack the problem directly or, as
WEELER [Zl CASES)
ZIEGLER ( IS CASES )
WIES [18 CASES)
SHTlSFItClORY
56 %
47 %
7β %
UNSnriSFACTORY
44%
5 3 %
22 %
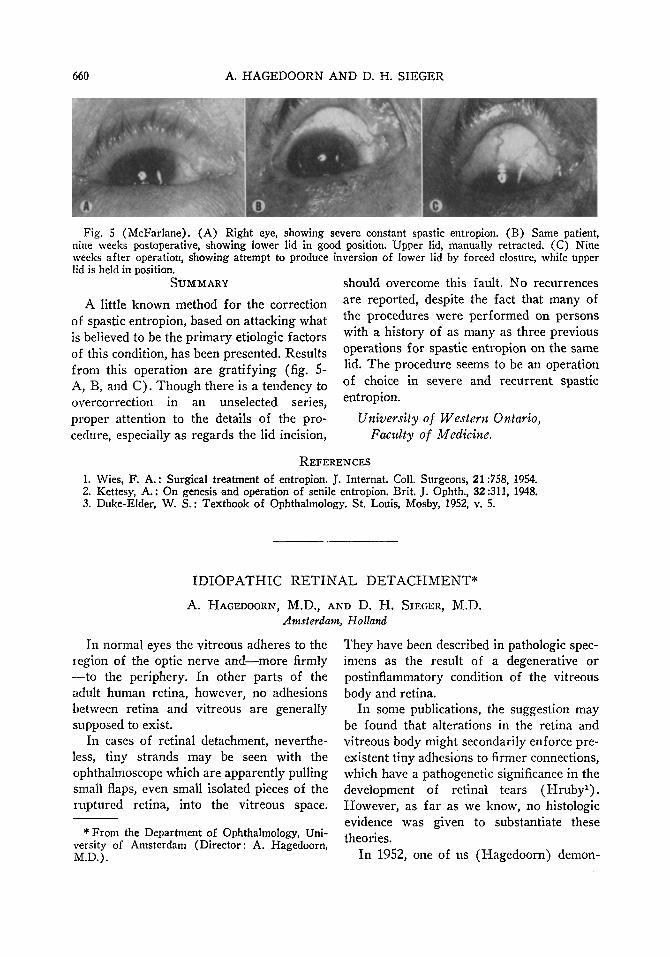
Fig. 1 (McFarlane). Postoperative results in 60 cases of spastic entropion.
in the latter technique, are more severe than is generally warranted.
In order to compare the results using the Wies method, all of the cases of spastic entropion operated on the clinical service of the Manhattan Eye, Ear, and Throat Hospital over the past five years have been reviewed. Only those cases in which the follow-up was six months or more have been recorded for comparative purposes. None of the Wies-procedure cases reported is less than three months postoperative.
This series (fig. 1) shows less than a 60 percent cure rate when the Wheeler method was used and less than 50 percent when Ziegler cautery was employed as compared to better than 75-percent cure with the Wies procedure. The relatively small number of Ziegler cauterizations is due to the fact that only those performed in the operating room are included. Undoubtedly results of many of the less severe cases treated b)r cauterization in the out-patient clinic would change this figure. I have not included procedures other than those mentioned, since only a small number of cases representing each of numerous and varied other methods of treatment could be collected.
WHEEIER
ZIEGISR
WIES
SATISFACTORY
AND COSMCly" RUS-'U
M
5
u
GCGD rUNCnuNAL
RESULT
;
2
3
lAISfttlSfACTOFY.
tlCCUHF-.ENCE
./;
7
0
OVERCORRIXTION
MILLI SEVCRC
I
1
I
0
0
3
Fig. 2 (McFarlane). Postoperative analysis of 60 cases of spastic entropion.
CORRECTION OF SPASTIC ENTROPION 659
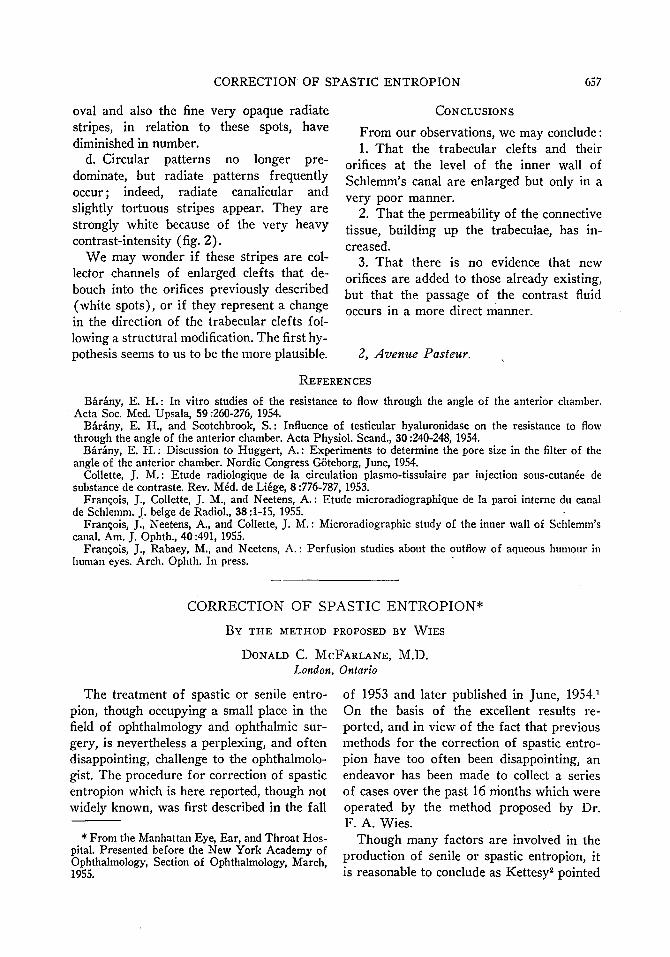
Fig. 3 (McFarlane). (A) Conjunctival incision made the length of the lower lid. No fixation clamp or ocular protector is shown. (B) Cross section of lid following incision no more than four mm. below the lid margin. Artist's conception of tarsus below incision is exaggerated.
A more detailed analysis of the cases (fig. 2) demonstrates one point clearly. Cases treated by both the Wheeler and Zielger methods show a marked tendency to recurrence, even after several months, while those treated by the Wies method do not. The Wies method, on the other hand, shows a tendency toward overcorrection in an un-selected series, a difficulty which I feel can be largely eliminated by attention to the technique.
METHOD OF OPERATION
The technique recommended by Dr. Wies, and the one which has been followed, can be done as an office procedure if adequate assistance is available.
Under local infiltration anesthesia, a hori-
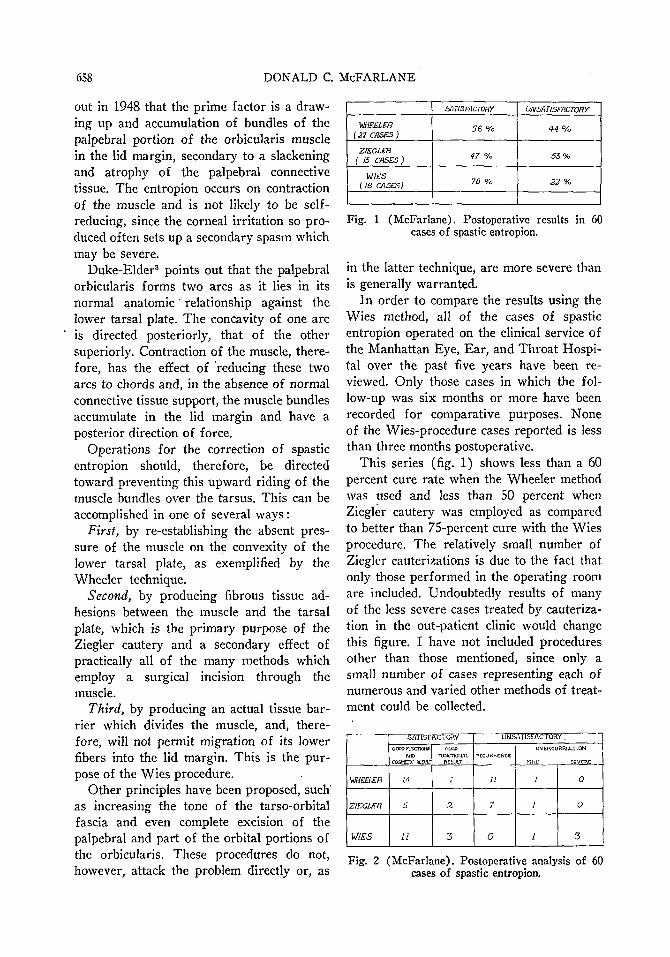
Fig. 4 (McFarlane). (C) Showing double-armed, 4-0 black-silk suture passed through conjunctiva of the lower part of incision and emerging through skin of the upper part. (D) Deep sutures in position and secured over rubber pegs. Skin closure with interrupted 6-0 silk.
zontal through-and-through incision, to include skin, muscle, tarsus, and conjunctiva, is made the length of the lower lid and four mm. below its margin (fig. 3). Hemo-stasis is readily achieved by pressure. Three 4-0 black silk, double-armed sutures are placed in the free margin of the conjunctiva (fig. 4) at the lower edge of the incision and brought out through the skin of the upper part, where they are tied over rubber pegs or a continuous rubber strip. The skin edges are then closed with interrupted 6-0 silk sutures. This effectively incarcerates a tongue of conjunctiva within the wound and above the major portion of the lower palpebrai orbicularis fibers.
Experience has taught that the most important part of the procedure is the lid incision. This should be made perpendicular to the lid and no more than four mm. below its margin, after first outlining the incision with marking fluid. If local anesthesia is used, it is best to block the lid rather than infiltrate directly into the area of the incision. To facilitate an incision perpendicular to the surface of the lid, a fixation device, such as the Erhardt clamp, is extremely helpful. Practically all of the overcorrections encountered have been attributed to an incision which is either too far below the lid margin, or is slanted downward and posteriorly into the lower fornix.
It has not been found necessary to undermine the conjunctiva which is to be incarcerated in the wound. The deep sutures are usually removed on the third or fourth day and the skin sutures on the fifth or sixth. Several of our successful cases have shown an apparent early overcorrection which persists as long as two or even three weeks. The overcorrections regress, however, without treatment or, if pronounced, it may be advisable to remove the offending deep suture or sutures at the first dressing. In the event that overcorrection occurs, application of the cautery to the conjunctival surface of the lid, as recommended by Wies, should be sufficient to control the ectropion.
660 A. HAGEDOORN AND D. H. SIEGER
i 'λι·.·
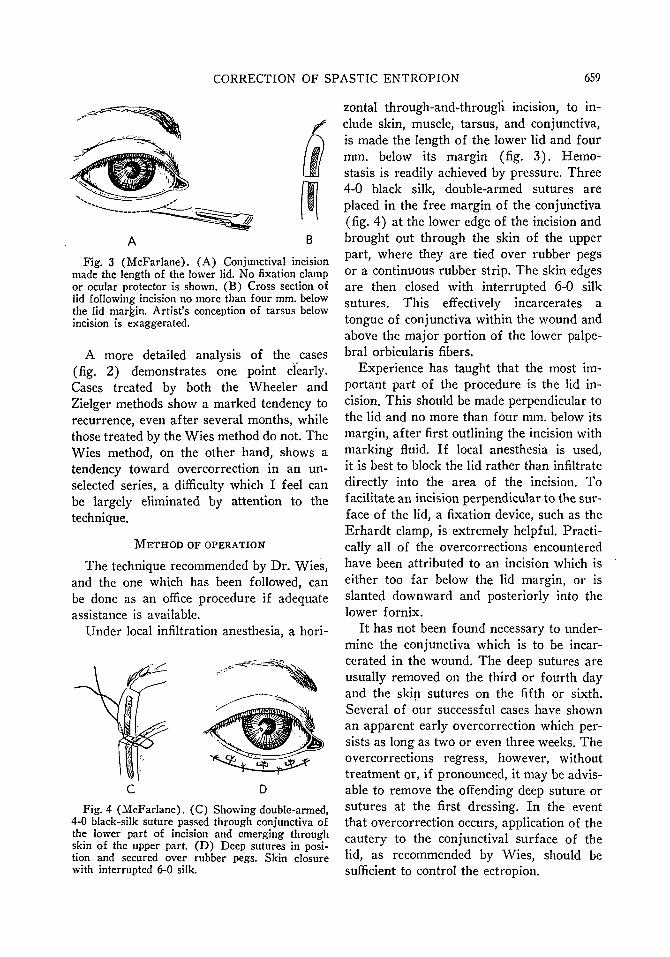
Fig. S (McFarlane). (A) Right eye, showing severe constant spastic entropion. (B) Same patient, nine weeks postoperative, showing lower lid in good position. Upper lid, manually retracted. (C) Nine weeks after operation, showing attempt to produce inversion of lower lid by forced closure, while upper lid is held in position.
SUMMARY
A little known method for the correction of spastic entropion, based on attacking what is believed to be the primary etiologic factors of this condition, has been presented. Results from this operation are gratifying (fig. 5-A, B, and C). Though there is a tendency to overcorrection in an unselected series, proper attention to the details of the procedure, especially as regards the lid incision,
should overcome this fault. No recurrences are reported, despite the fact that many of the procedures were performed on persons with a history of as many as three previous operations for spastic entropion on the same lid. The procedure seems to be an operation of choice in severe and recurrent spastic entropion.
University of Western Ontario, Faculty of Medicine.
REFERENCES
1. Wies, F. A.: Surgical treatment of entropion. J. Internat. Coll. Surgeons, 21:758, 19S4. 2. Kettesy, A.: On genesis and operation of senile entropion. Brit. J. Ophth., 32:311, 1948. 3. Duke-Elder, W. S. : Textbook of Ophthalmology. St. Louis, Mosby, 1952, v. 5.
IDIOPATHIC RETINAL DETACHMENT*
A. HAGEDOORN, M.D., AND D. H. SIEGER, M.D. Amsterdam, Holland
In normal eyes the vitreous adheres to the region of the optic nerve and—more firmly —to the periphery. In other parts of the adult human retina, however, no adhesions between retina and vitreous are generally supposed to exist.
In cases of retinal detachment, nevertheless, tiny strands may be seen with the ophthalmoscope which are apparently pulling small flaps, even small isolated pieces of the ruptured retina, into the vitreous space.
* From the Department of Ophthalmology, University of Amsterdam (Director: A. Hagedoorn, M.D.).
They have been described in pathologic specimens as the result of a degenerative or postinflammatory condition of the vitreous body and retina.
In some publications, the suggestion may be found that alterations in the retina and vitreous body might secondarily enforce préexistent tiny adhesions to firmer connections, which have a pathogenetic significance in the development of retinal tears (Hruby1). However, as far as we know, no histologie evidence was given to substantiate these theories.
In 1952, one of us (Hagedoorn) demon-





























