Embed Size (px)
Citation preview

Electrophysiology
Coronary artery involvement early and late after radiofrequency current application in young pigs
Thomas Paul, MD, a Regina BSkenkamp, MD, a Br i t t a Mahner t , MD, a
and Hans-Joach im Trappe, MD b Hannover, Germany
Radiofrequency current (500 kHz) was delivered by temper- ature guidance (75 ° C) over a 30-second period in 10 young piglets with a steerable 6F electrode catheter equipped with a thermistor at the 4 mm tip electrode. Lesions were created at the right atrial aspect of the tricuspid valve anulus, at the left ventricular myocardium under the lateral mitral valve anulus, and at the left ventricular apex. After 48 hours, five animals were randomly sacrificed. Lesions in the five ani- mals appeared as transmural gray-white coagulation necro- sis. Lymphocytic infiltration around the right atrial lesions extended into the layers of the right coronary artery in four of five animals. After 6 months, lesions consisted of com- pact fibrous tissue in the remaining five animals. Right atrial lesions extended to the layers of the right coronary artery in four of five pigs. In two animals the lumen of the right cor- onary artery was narrowed because of intimal thickening by 25% and 40%, respectively. No increase in the lesion size was observed with the growth of the animals. Effects on the right coronary artery as a late sequela after radiofrequency current application may also be possible in human beings and should be considered when radi0frequency current ab- lation procedures are proposed in infants and young chil- dren. (Am Heart J 1997;133:436-40.)
Cathe te r ablat ion of accessory a t r iovent r icular path- ways by radiofrequency cur ren t applicat ion has be- come a rout ine procedure in adul t pa t ients 1, 2 as well as in children and adolescents. 3-5 Data concerning lesion format ion induced by radiofrequency cur ren t discharge in i m m a t u r e myocard ium are sparse. Af- t e r radiofrequency cur ren t application in developing sheep myocardium, lesion format ion was associated wi th la te lesion en la rgement and fibrous t issue
From the Departments of aPediatric Cardiology and bCardiology, Hannover Medical School.
Supported by Deutsche Forschungsgemeinschaft grant PA 352/2-1, Bonn- Bad Godesberg, Germany.
Reprint requests: Thomas Patti, MD, Pediatric Cardiology, Children's Hos- pital, Hannover Medical School, D-30623 Hannover, Germany.
Copyright © 1997 by Mosby Year Book, Inc. 0002-8703/97/$5.00 + 0 4/1/80079
invasion of normal myocardium. 6 Lesions were often found to be poorly demarca ted from sur rounding tis- sue. However, lesion size was not measu red exactly by vo lumet ry bu t only es t imated by measur ing width and depth. S ta tus of the coronary sinus and the cor- onary ar ter ies was also not ment ioned in detail. G
Late sequelae af ter radiofrequency cur ren t appli- cation at the a t r iovent r icular groove m ay theoret i- cally include an eu ry sm format ion of the lesions and occurrence of a t r ia l or vent r icu la r dysrhythmias ; the coronary ar ter ies m ay also be affected.
The purpose of this s tudy was to systemat ical ly assess morphologic sequelae af ter radiofrequency cur ren t application in young pigs.
METHODS
Ten young German Landrace pigs with a mean age of 6 weeks and a mean body weight of 12.5 _+ 0.8 kg were used. The experimental study was approved by the local author- ity (Bezirksregierung Hannover) on Jan. 18, 1993 (ref. no. 504-42502-92/582).
Animals were orally intubated and ventilated under general anesthesia (fentanyl 5 ~g/kg and midazolam 0.1 mg/kg repeatedly). Vascular access to the femoral artery and vein was accomplished by the cutdown technique. A steerable 6F electrode catheter equipped with an inte- grated thermistor at the 4 mm tip electrode (Cerablate 630, Dr. Osypka GmbH, Grenzach-Wyhlen, Germany) was in- troduced into the right atrium under fluoroscopic control. The tip of the electrode catheter was positioned at the lat- eral atrial aspect of the tricuspid anulus. After registration of a bipolar atrial, and ventricular electrogram of equal amplitude, radiofrequency current (500 kHz, generator HAT 200 S, Dr. Osypka) was delivered by temperature guidance at 75 ° C for 30 seconds in the unipolar mode against a plate electrode placed under the back of the an- imal.
The catheter was then introduced retrogradely into the left ventricle and positioned under the lateral aspect of the mitral valve anulus. Radiofrequency current was delivered as previously described if a ventricular and atrial electro-
436
Volume 133, Number 4
American Heart Journal Paul et al. 437
Table I. Lesion characteristics
Wall Energy thickness Volume
(Ws) (ram) Transmural (mm 3)
RA 48 hours 414.7 -- 176.8 2 ± 0.3 5/5 48.9 ± 13.5 6 mon ths 356.1 ± 131.5 2.1 ± 0.6 5/5 27.8 ± 4.7
MV 48 hours 268.7 -+ 211.8 7.6 ± 0.5 5/5 150.2 ± 15.2 6 m o n t h s 154.4 _+ 64 16.5 ± 0.8 0/5 96.7 ± 18.6
LV 48 hours 296.4 _+ 186.1 5.4 _+ 1.1 5/5 161.7 ± 14 48 hours 292.9 ± 234.5 7.2 _+ 1.3 5/5 164.2 + 19.9
RA, Right atrial lesions; MV, lesions under mitral valve anulus; LV, lesions at left ventricular apex.
gram of equal amplitude could be recorded. The procedure was performed the same as described for children and adults.l, 2, 4
Finally, radiofrequency current was delivered in the same way at the left ventricular apex. Data concerning temperature at the catheter tip, power output, and imped- ance were stored on a personal computer as previously de- scribed. 2
Five of the 10 animals were randomly sacrificed afte r 48 hours; the remaining five animals were examined at the age of 6 months. Under deep general anesthesia (fentanyl 30 pg/kg), the hearts were removed after median sternot- omy. Atria and ventricles were opened for macroscopic study of the lesions.
For microscopic study and exact volumetry, blocks con- taining whole lesions with the adherent tissue of the atri- oventricular groove were removed and processed in mi- croseries with a section thickness of 5 ~m. Staining was performed with hematoxylin-eosin and alcian blue by standard procedures. At every fortieth section, maximal area of the lesion was measured by planimetry with a computerized analysis system (Ernst Leitz Wetzlar, Wet- zlar, Germany). Lesion volumes were calculated according to the equation Ei = (Areai x Thicknessi), where i is the number of sections performed per lesion.
Statistical evaluation. Comparison of the lesion volumes at the different locations was performed by analysis of variance (ANOVA). If the ANOVA was statistically signif- icant, Bonferroni's modification of the t test was subse- quently used for pairwise comparisons. 7 Statistical signif- icance was inferred if the probability of a difference occur- ring by chance was <0.05.
RESULTS Morphometric and volumetric results 48 hours after
radiofrequency current delivery. I n al l f ive animals ra- diofrequency cu r ren t lesions a p p e a r e d as a t r ans - m u r a l g ray-whi te coagula t ion necrosis wi th perifocal h e m o r r h a g e in all t h ree locations 48 hours a f te r en- e rgy discharge. M e a n wall th ickness of the r igh t a t r ia l wall was 2 m m , 7.6 m m unde r the mi t r a l va lve
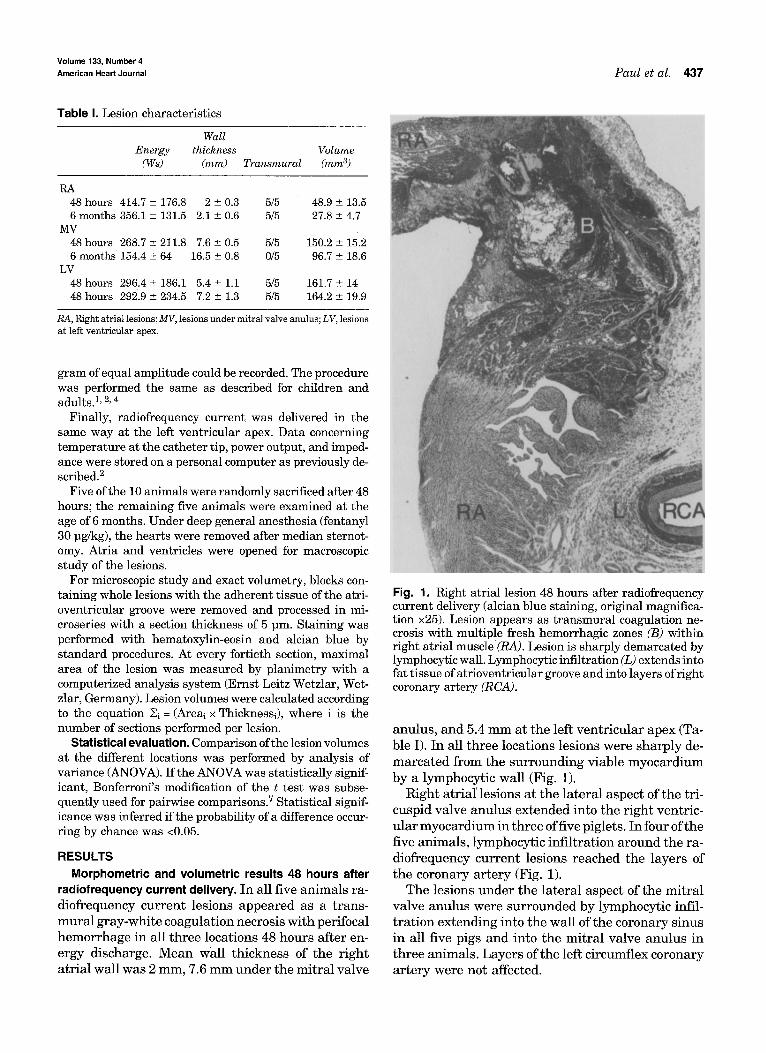
Fig. 1. Right atrial lesion 48 hours after radiofrequency current delivery (alcian blue staining, original magnifica- tion ×25). Lesion appears as transmural coagulation ne- crosis with multiple fresh hemorrhagic zones (B) within right atrial muscle (RA). Lesion is sharply demarcated by lymphocytic wall. Lymphocytic infiltration (L) extends into fat tissue of atrioventricular groove and into layers of right coronary artery (RCA).
anulus , and 5.4 m m a t the left ven t r i cu la r apex (Ta- ble I). In all th ree locations lesions were sha rp ly de- m a r c a t e d f rom the su r round ing viable m y o c a r d i u m by a lymphocyt ic wall (Fig. 1).
Right a t r i a l lesions a t t:he la te ra l aspec t of the tri- cuspid valve anu lus ex tended into the r igh t ventr ic- u la r m y o c a r d i u m in th ree of five piglets. In four of the five an imals , lymphocyt ic inf i l t ra t ion a round the ra- diofrequency cu r ren t lesions reached the layers of the coronary a r t e ry (Fig. 1).
The lesions unde r the la te ra l aspect of the mi t r a l va lve anu lus were su r rounded by lymphocyt ic infil- t r a t ion ex tending into the wal l of the coronary s inus in all five pigs and into the mi t r a l valve anu lus in th ree animals . Laye r s of the left c i rcumflex coronary a r t e r y were not affected.
April 1997 438 Paul et al. American Heart Journal
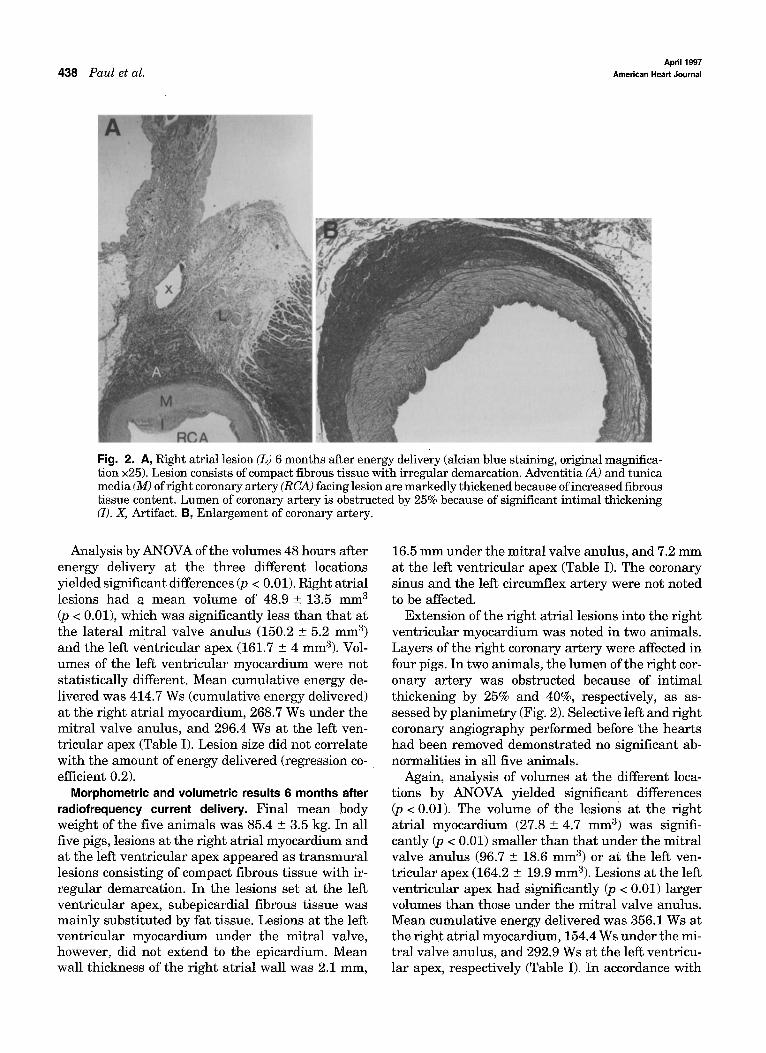
Fig. 2. A, Right atrial lesion (L) 6 months after energy delivery (alcian blue staining, original magnifica- tion ×25). Lesion consists of compact fibrous tissue with irregular demarcation. Adventitia (A) and tunica media (M) of right coronary artery (RCA) facing lesion are markedly thickened because of increased fibrous tissue content. Lumen of coronary artery is obstructed by 25% because of significant intimal thickening (I). X, Artifact. B, Enlargement of coronary artery.
Analysis by ANOVA of the volumes 48 hours after energy delivery at the three different locations yielded significant differences (p < 0.01). Right atrial lesions had a mean volume of 48.9 __ 13.5 mm 3 (p < 0.01), which was significantly less than that at the lateral mitral valve anulus (150.2 _+ 5.2 mm 3) and the left ventricular apex (161.7 _+ 4 mm3). Vol- umes of the left ventricular myocardium were not statistically different. Mean cumulative energy de- livered was 414.7 Ws (cumulative energy delivered) at the right atrial myocardium, 268.7 Ws under the mitral valve anulus, and 296.4 Ws at the left ven- tricular apex (Table I). Lesion size did not correlate with the amount of energy delivered (regression co- efficient 0.2).
Morphometric and volumetric results 6 months after radiofrequency current delivery. Final mean body weight of the five animals was 85.4 _+ 3.5 kg. In all five pigs, lesions at the right atrial myocardium and at the left ventricular apex appeared as t ransmural lesions consisting of compact fibrous tissue with ir- regular demarcation. In the lesions set at the left ventricular apex, subepicardial fibrous tissue was mainly substituted by fat tissue. Lesions at the left ventricular myocardium under the mitral valve, however, did not extend to the epicardium. Mean wall thickness of the right atrial wall was 2.1 mm,
16.5 mm under the mitral valve anulus, and 7.2 mm at the left ventricular apex (Table I). The coronary sinus and the left circumflex artery were not noted to be affected.
Extension of the right atrial lesions into the right ventricular myocardium was noted in two animals. Layers of the right coronary artery were affected in four pigs. In two animals, the lumen of the right cor- onary artery was obstructed because of intimal thickening by 25% and 40%, respectively, as as- sessed by planimetry (Fig. 2). Selective left and right coronary angiography performed before the hearts had been removed demonstrated no significant ab- normalities in all five animals.
Again, analysis of volumes at the different loca- tions by ANOVA yielded significant differences (p < 0.01). The volume of the lesions at the right atrial myocardium (27.8 _+ 4.7 mm 3) was signifi- cantly (p < 0.01) smaller than that under the mitral valve anulus (96.7 +_ 18.6 mm 3) or at the left ven- tricular apex (164.2 _+ 19.9 mm3). Lesions at the left ventricular apex had significantly (p < 0.01) larger volumes than those under the mitral valve anulus. Mean cumulative energy delivered was 356.1 Ws at the right atrial myocardium, 154.4 Ws under the mi- tral valve anulus, and 292.9 Ws at the left ventricu- lar apex, respectively (Table I). In accordance with

Volume 133, Number 4
American Heart Journal PGUl et al. 439
the findings 48 hours after radiofrequency current discharge, lesion size did not correlate with mount of delivered energy (regression coefficient 0.014).
Comparison of volumetric results 48 hours and 6 months after radiofrequency current delivery. No evi- dence of increase in lesion size with growth of the animals was observed. By group comparison, vol- umes of the right atrial lesions and of the left ventricular myocardium under the mitral valve an- ulus were significantly smaller 6 months after en- ergy discharge compared with those after 48 hours. Lesion size at the left ventricular apex had not sig- nificantly differed with growth of the animals (Table I).
DISCUSSION Morphologic observations Right atrial lesions. Extension of the lymphocytic
infiltration to the fat tissue of the atrioventricular groove and the layers of the right coronary artery, which was evident in four of the five pigs in this study, has not been described before early after ra- diofrequency current application. Data are lacking concerning long-term effects of radiofrequency cur- rent application at right atrial myocardium regard- ing the adjacent right coronary artery. In contrast to findings after energy discharge at the right atrial wall in adult dogs, s, 9 involvement of the layers of the right coronary artery with narrowing of the lumen of the vessel was evident in the majority of our animals.
Left ventricular lesions. Left ventricular lesions 48 hours after energy discharge had a t ransmural extension as previously reported in young sheep 6 and in dogs 1°-12 with a comparable experimental setting. All animals exhibited lymphocytic infiltration in the layers of the coronary sinus. In accordance with findings after radiofrequency current application within the coronary sinus or after energy discharge in a bipolar mode between the coronary sinus and the left ventricle, 13, 14 no major abnormalities such as rupture, perforation, or stricture of the coronary si- nus were evident.
Lesions under the mitral valve anulus examined 6 months after energy discharge extended into the mi- tral valve anulus without any significant alterations of the mitral valve leaflets, 15, 10 the coronary sinus, or the left circumflex artery. 13, 16
Morphometric findings. In the majority of studies concerning morphometric evaluation of radiofre- quency current lesions, lesion volume had been extrapolated from the endocardial diameter and the depth of the lesions. 11-13, 17-20 Volume size 6 months after radiofrequency current application had signif- icantly decreased in the lesions at the right atrial
myocardium and at the left ventricular myocardium under the mitral valve anulus: These results are in contrast with the findings in young sheep with lesion growth and myocardial tissue loss over time. 6 Exact volumetric evaluation of the lesions, however, was not performed in that study. Findings with regres- sion of lesion growth over a period of time are in ac- cordance with previous reports in adult animals. 12, 21 Lesions under the mitral valve anulus 6 months af- ter energy discharge were significantly smaller than those at the left ventricular apex. The hypothesis of different reactions of left ventricular myocardium at different locations against thermal injury 12 is sup- ported by these findings.
Clinical implications. Shrinkage or unchanged le- sion size after radiofrequency current application in the young animals of this study may support safety of radiofrequency current ablation procedures in in- fants and children. A study of the North American Pediatric Electrophysiology Society 15 revealed a mor- tality rate of 4% in infants and children <4 years of age after radiofrequency current application. Acute coronary occlusion caused by radiofrequency cathe- ter ablation of a left lateral accessory pathway has recently been reported in an adult patient. 22 Previ- ous studies in adult patients, including preablation and postablation coronary angiography, did not show any vessel lesions or permanent alteration of coro- nary anatomy. 23, 24
In this study the coronary arteries were influenced in the majority of the animals. Consequences of these alterations over long-term follow-up (years or de- cades) are still unknown, Potential risk of the coro- nary artery being affected, that is intimal thickening that may provide a nidus for shear forces and plaque formation over years of development, at an early age has to be considered when radiofrequency current ablation is planned in infhnts and children.
REFERENCES
1. Calkins H, Sousa J, E1-Atassi R, Roseneck S, de Buitleir M, Kou WH, et al. Diagnosis and cure of the Wolff-Parkinson-White syndrome or paroxysmal supraventricular tachycardia during a single electrophys- iologic test. N Engl J Med 1991;324:1612-8.
2. Kuck KH, Schliiter M, Geiger M, Siebels J, Duckeck W. Radiofrequency current catheter ablation of accessory pathways. Lancet 1991;337:1557- 61.
3. Saul JP, Hulse JE, De W, Weber AT, Rhodes LA, Lock JE, et al. Cath- eter ablation of accessory atrioventricular pathways in young patients: use of long vascular sheaths, the transseptal approach and a retrograde left posterior parallel approach. J Am Coll Cardiol 1993;21:571-83.
4. Van Hare GF, Lesh MD, Scheinman M, Langberg JJ. Percutaneous radiofrequency catheter ablation for supraventricular arrhythmias in children. J Am Coll Cardiol 1991;17:1613-20.
5. Langberg JJ, Chin MC, Rosenquist M, Cockrell J, DuIlet N, Van Hare G, et al. Catheter ablation of the atrioventricular junction with radio- frequency energy. Circulation 1989;80:1527-35.
6. Saul JP, Hulse JE, Papagiannis J, Van Praagh R, Walsh EP. Late en-

April 1997 440 Paul et al. American Heart Journal
largement of radiofrequency lesions in infant lambs. Implications for ablation procedures in small children. Circulation 1994;90:492-9.
7. Wallenstein S, Zucker C, Fleiss JL. Some statistical methods useful in circulation research. Circ Res 1980;47:1-9.
8. Franklin JO, Langberg JJ, OeffM, Finkbeiner WE, Herre JM, Griffin JC, et al. Catheter ablation of canine myocardium with radiofrequency energy. PACE 1989;12:170-6.
9. Huang SK. Radio-frequency catheter ablation of cardiac arrhythmias: appraisal of an evolving therapeutic modality. Am Heart J 1989; 118:1317-23.
10. Huang SK, Graham AR, Hoyt RH, Odell RC. Transcatheter desiccation of the canine left ventricle using radio-frequency energy: a pilot study. Am Heart J 1987;114:42-8.
11. Huang SKS, Graham AR, Wharton K. Radiofrequency catheter abla- tion of the left and right ventricles: anatomic and electrophysiologic observations. PACE 1988;11:449-59.
12. Simmers T, Wittkamp FH, Hauer RaN, Robles de Medina E. In vivo ventricular lesion growth in radiofrequency catheter ablation. PACE 1994;17:523-31.
13. Huang SK, Graham AR, Bharati S, Lee MAi German G, Lev M. Short- and long-term effects oftranscatheter ablation of the coronary sinus by radiofrequency energy. Circulation 1988;78:416-27.
14. Jackman WM, Kuck KH, Naccarelli GV, Carmen L, Pitha J. Radiofre- quency current directed across the mitral anulus with a bipolar epicar- dial~endocardial catheter electrode configuration in dogs. Circulation 1988;78:1288-98.
15. Kugler JD, Danford DA, Deal BJ, Gillette PC, Perry JC, Silka M J, et al., for the Pediatric Electrophysiolog~ Society. Radiofrequency cathe- ter ablation for tachyarrhythmias in children and adolescents. N Engl J Med 1994;330:1481-7.
16. Chin MC, Schuenemyer T, Finkebeiner WE, Stern RA, Scheinman
MM, Langberg JJ. Histepathology of monopolar transcatheter radio- frequency ablation at the mitral valve anulus. PACE 1991;14:1956- 60.
17. Chang RJ, Stevenson WG, Saxon LA, Parker J. Increasing catheter ablation lesion size by simultaneous application of radiofrequency cur- rent to two adjacent sites. Am Heart J 1993;125:1276-84.
18. Huang SKS, Graham AR, Lee MA, Ring ME, German GD, Shiffman R. Comparison of catheter ablation using radiofrequency versus direct current energy: biophysical, electrophysiological and pathological ob- servations. J Am Cell Cardiol 1991;18:1091-7.
19. Kongsgaard E, Foerster A, Aass H, Amlie JP. The effect oftemperature- guided radiofrequency ablation of ventricular myocardium. Eur Heart J 1993;14:852-8.
20. Hindricks G, Haverkamp W, Gtilker H, Rissel U, Budde T, Richter KD, et al. Radiofrequency coagulation efventricular myocardium: improved prediction of lesion size by monitoring catheter tip temperature. Eur Heart J 1989;10:972-84.
21. Bakker PF, Vermeulen FIE, Boo JA, Elbers HR, ri~veel I, Beyeren I, et aI. Extensive cryoablation of the left ventricular posterior papillary muscle and subjacent ventricular wall. Impact on mitral valve function and hemodynamics. J Thorac Cardiovasc Surg 1993;105:327-36.
22. Chatelaln P, Zimmermann M, Weber R, Campanini C, Adamec R. Acute coronary occlusion secondary to radiofrequency catheter ablation of a left lateral accessory pathway. Eur Heart J 1995;16:859-61.
23. Strickberger SA, Okishige K, Meyerovitz M, Shea J, Friedman PL. Evaluation of possible long-term adverse consequences of radiofre- qnency ablation of accessory pathways. Am J Cardiol 1993;71:473-5.
24. Solomon AJ, Tracy CM, Swartz JF, Reagan KM, Kamsik PE, Fletcher RD. Effect on coronary artery anatomy of radiofrequency catheter ab- lation of atrial insertion sites of accessory pathways. J Am Cell Cardiol 1993;21:1440-4.





























