Embed Size (px)
DESCRIPTION
Coronary Artery Disease Clinical Trial Summary Slides. - PowerPoint PPT Presentation
Citation preview
Coronary Artery DiseaseCoronary Artery Disease
Clinical Trial Summary SlidesClinical Trial Summary Slides
www.cardiosource.com
2225
0
10
20
30
40
ACADEMIC
AZ Placebo
Adverse CVEvents
HR 0.89 (0.51-1.61)p = 0.74
Nu
mb
er o
f ev
ents
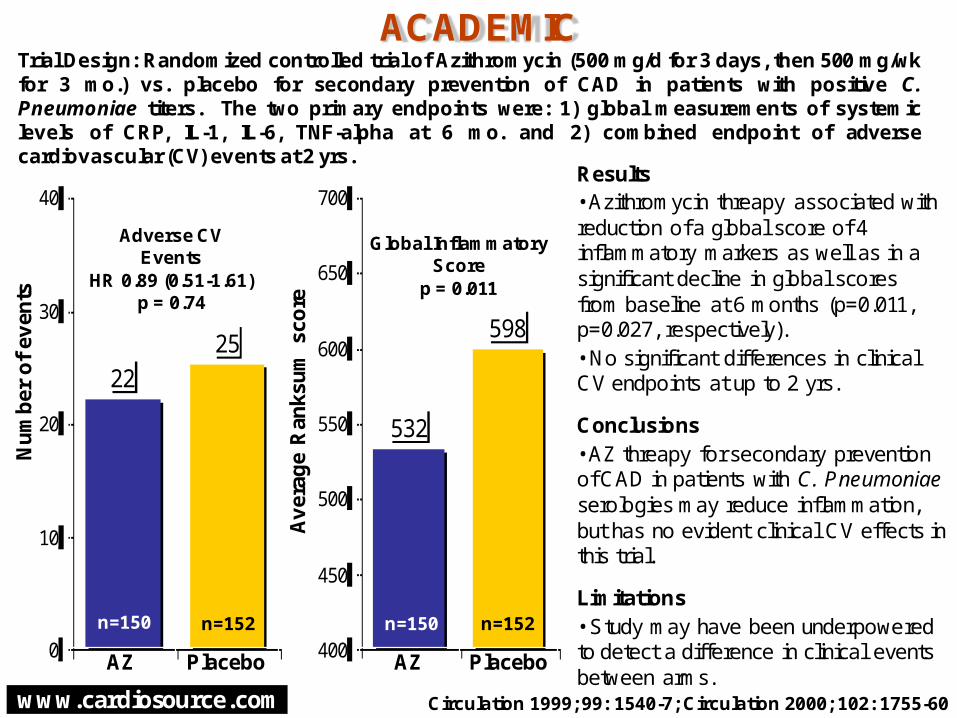
Trial Design: Randomized controlled trial of Azithromycin (500 mg/d for 3 days, then 500 mg/wkfor 3 mo.) vs. placebo for secondary prevention of CAD in patients with positive C.Pneumoniae titers. The two primary endpoints were: 1) global measurements of systemiclevels of CRP, IL-1, IL-6, TNF-alpha at 6 mo. and 2) combined endpoint of adversecardiovascular (CV) events at 2 yrs.
532
598
400
450
500
550
600
650
700
AZ Placebo
Global InflammatoryScore
p = 0.011
n=150 n=152
Av
erag
e R
anks
um
sco
re
Circulation 1999; 99: 1540-7; Circulation 2000; 102: 1755-60
Results• Azithromycin threapy associated with reduction of a global score of 4 inflammatory markers as well as in a significant decline in global scores from baseline at 6 months (p=0.011, p=0.027, respectively).• No significant differences in clinical CV endpoints at up to 2 yrs.
Conclusions• AZ threapy for secondary prevention of CAD in patients with C. Pneumoniaeserologies may reduce inflammation, but has no evident clinical CV effects in this trial.
Limitations• Study may have been underpowered to detect a difference in clinical events between arms.
n=150 n=152
www.cardiosource.com
3.2
3.7
0
1
2
3
4
5
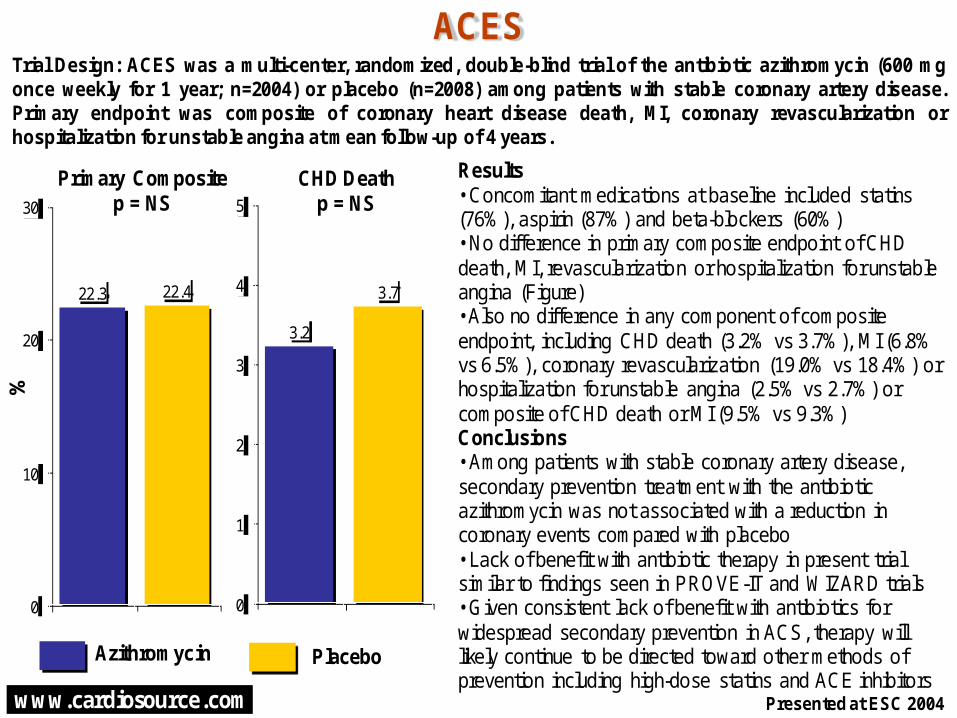
Results• Concomitant medications at baseline included statins (76%), aspirin (87%) and beta-blockers (60%)• No difference in primary composite endpoint of CHD death, MI, revascularization or hospitalization for unstable angina (Figure)• Also no difference in any component of composite endpoint, including CHD death (3.2% vs 3.7%), MI (6.8% vs 6.5%), coronary revascularization (19.0% vs 18.4%) or hospitalization for unstable angina (2.5% vs 2.7%) or composite of CHD death or MI (9.5% vs 9.3%) Conclusions• Among patients with stable coronary artery disease, secondary prevention treatment with the antibiotic azithromycin was not associated with a reduction in coronary events compared with placebo• Lack of benefit with antibiotic therapy in present trial similar to findings seen in PROVE-IT and WIZARD trials• Given consistent lack of benefit with antibiotics for widespread secondary prevention in ACS, therapy will likely continue to be directed toward other methods of prevention including high-dose statins and ACE inhibitors
22.3 22.4
0
10
20
30
ACES
Primary Compositep = NS
%
Trial Design: ACES was a multi-center, randomized, double-blind trial of the antibiotic azithromycin (600 mgonce weekly for 1 year; n=2004) or placebo (n=2008) among patients with stable coronary artery disease.Primary endpoint was composite of coronary heart disease death, MI, coronary revascularization orhospitalization for unstable angina at mean follow-up of 4 years.
Presented at ESC 2004
Azithromycin Placebo
CHD Deathp = NS
www.cardiosource.com
-5.6
-1.3
-6
-4
-2
0
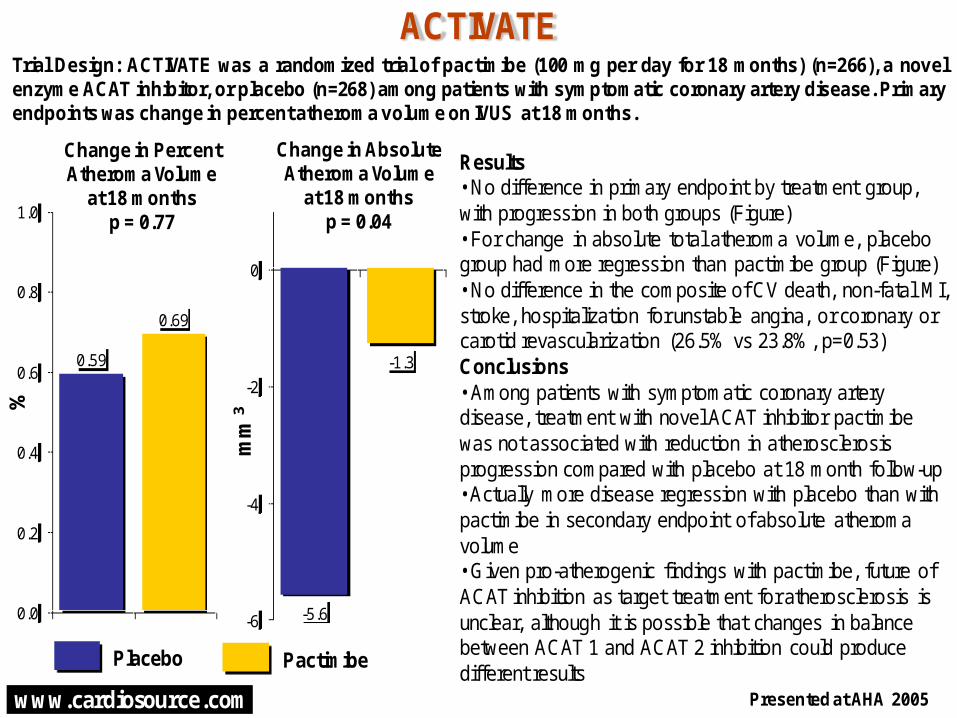
Results• No difference in primary endpoint by treatment group, with progression in both groups (Figure)• For change in absolute total atheroma volume, placebo group had more regression than pactimibe group (Figure)• No difference in the composite of CV death, non-fatal MI, stroke, hospitalization for unstable angina, or coronary or carotid revascularization (26.5% vs 23.8%, p=0.53)Conclusions• Among patients with symptomatic coronary artery disease, treatment with novel ACAT inhibitor pactimibe was not associated with reduction in atherosclerosis progression compared with placebo at 18 month follow-up• Actually more disease regression with placebo than with pactimibe in secondary endpoint of absolute atheroma volume• Given pro-atherogenic findings with pactimibe, future of ACAT inhibition as target treatment for atherosclerosis is unclear, although it is possible that changes in balance between ACAT 1 and ACAT 2 inhibition could produce different results
0.59
0.69
0.0
0.2
0.4
0.6
0.8
1.0
ACTIVATE
Change in PercentAtheroma Volume
at 18 monthsp = 0.77
%
Trial Design: ACTIVATE was a randomized trial of pactimibe (100 mg per day for 18 months) (n=266), a novelenzyme ACAT inhibitor, or placebo (n=268) among patients with symptomatic coronary artery disease. Primaryendpoints was change in percent atheroma volume on IVUS at 18 months.
Presented at AHA 2005
Placebo Pactimibe
Change in AbsoluteAtheroma Volume
at 18 monthsp = 0.04
mm
3
www.cardiosource.com
3.0
2.3
0
1
2
3 16.417.5
0
5
10
15
20
BRAVO
MortalityHR 1.33p=0.026
%
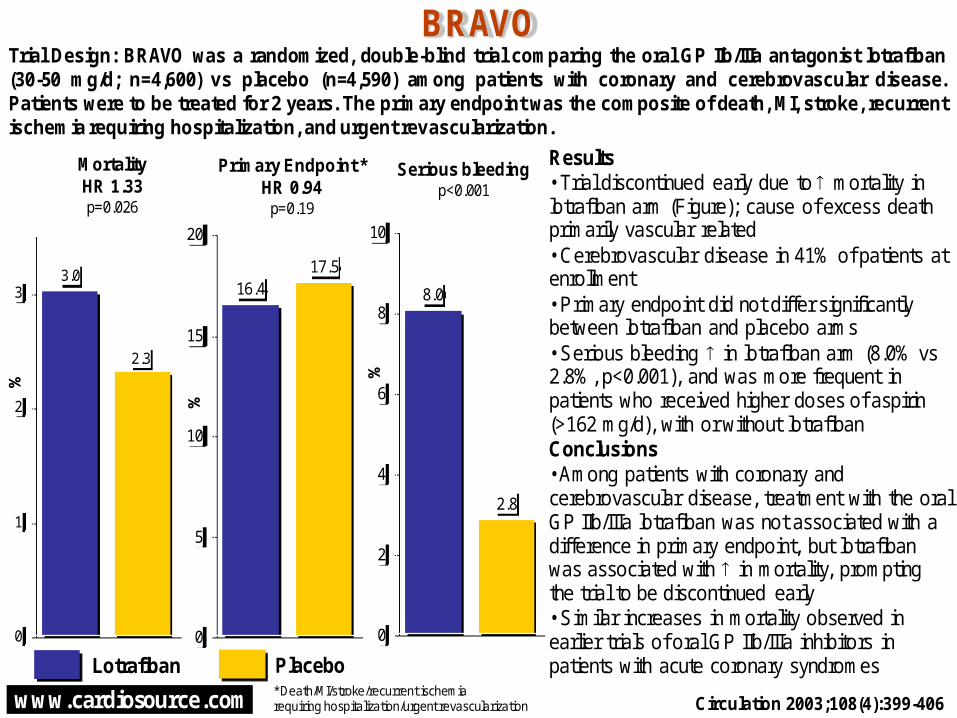
Trial Design: BRAVO was a randomized, double-blind trial comparing the oral GP IIb/IIIa antagonist lotrafiban(30-50 mg/d; n=4,600) vs placebo (n=4,590) among patients with coronary and cerebrovascular disease.Patients were to be treated for 2 years. The primary endpoint was the composite of death, MI, stroke, recurrentischemia requiring hospitalization, and urgent revascularization.
Primary Endpoint *HR 0.94
p=0.19
Circulation 2003;108(4):399-406
Results• Trial discontinued early due to mortality in lotrafiban arm (Figure); cause of excess death primarily vascular related• Cerebrovascular disease in 41% of patients at enrollment• Primary endpoint did not differ significantly between lotrafiban and placebo arms • Serious bleeding in lotrafiban arm (8.0% vs 2.8%, p<0.001), and was more frequent in patients who received higher doses of aspirin (>162 mg/d), with or without lotrafibanConclusions• Among patients with coronary and cerebrovascular disease, treatment with the oral GP IIb/IIIa lotrafiban was not associated with a difference in primary endpoint, but lotrafiban was associated with in mortality, prompting the trial to be discontinued early• Similar increases in mortality observed in earlier trials of oral GP IIb/IIIa inhibitors in patients with acute coronary syndromesLotrafiban Placebo
%
* Death/MI/stroke/recurrent ischemiarequiring hospitalization/urgent revascularization
8.0
2.8
0
2
4
6
8
10
Serious bleedingp<0.001
%

www.cardiosource.com
23.1
20.2
16.6
0
10
20
30
40
CAMELOT
Adverse CVEvents
%
Trial Design: CAMELOT was a randomized, double-blinded, placebo-controlled trial (n=1991) ofthe effects of amlodipine or enalapril compared to placebo in normotensive patients withcoronary artery disease. Primary endpoint: Adverse cardiovascular events (composite of CVdeath, nonfatal MI, resuscitated cardiac arrest, coronary revascularization, hospitalization forangina or CHF, stroke/TIA, and any new diagnosis of peripheral vascular disease).
JAMA 2004;292:2217-25
Results• Mean blood pressure ↓ 4.8/2.5 mmHg in amlodipine group, ↓ 4.9/2.4 mmHg in enalapril group, and ↑ 0.7/0.6 mmHg in placebo group (p<0.001 for both treatments vs placebo)• CV events ↓ in amlodipine group compared to enalapril (HR 0.81, p=0.1) and placebo (HR 0.69, p=0.003; HR=0.85 for enalapril vs placebo, p=0.16) (Figure)• In patients undergoing IVUS, no significant change from baseline in amlodipine group (p=0.31), a trend towards progression of atheroma in enalapril group (p=0.08), and progression in placebo group (p=0.001)Conclusions• Among patients with CAD and relatively normal blood pressures, treatment with amlodipine but not enalapril was associated with a reduction in the composite primary endpoint of CV events compared to placebo, largely driven by a reduction in coronary revascularization and hospitalization from anginaPlacebo Enalapril
3.94.4
3.7
0
2
4
6
8
10Change in
%AtheromaVolume
%
p<0.003 foramlodipinevs. placebo
p=NS forcomparison
between groups
Amlodipine
www.cardiosource.com
114.3
144.0 140.3
0
40
80
120
160
91.7
115.8115.4
0
40
80
120
CARISA
Trough exercise duration
750 mg vs placebo, p=0.031000 mg vs placebo, p=0.03
seco
nd
s
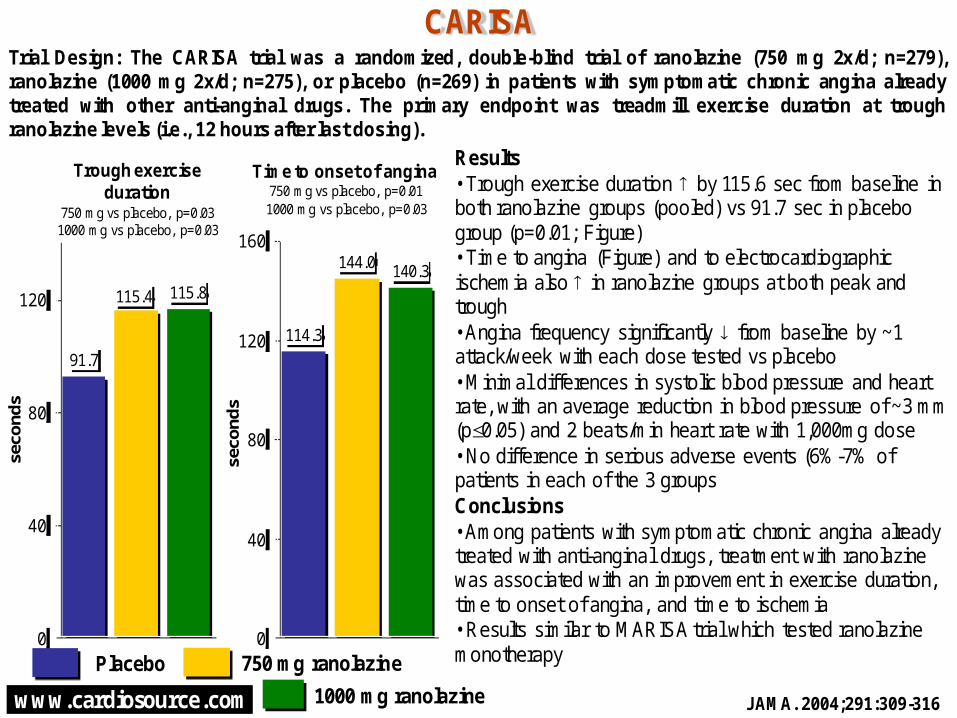
Trial Design: The CARISA trial was a randomized, double-blind trial of ranolazine (750 mg 2x/d; n=279),ranolazine (1000 mg 2x/d; n=275), or placebo (n=269) in patients with symptomatic chronic angina alreadytreated with other anti-anginal drugs. The primary endpoint was treadmill exercise duration at troughranolazine levels (i.e., 12 hours after last dosing).
Results• Trough exercise duration by 115.6 sec from baseline in both ranolazine groups (pooled) vs 91.7 sec in placebo group (p=0.01; Figure)• Time to angina (Figure) and to electrocardiographic ischemia also in ranolazine groups at both peak and trough• Angina frequency significantly from baseline by ~1 attack/week with each dose tested vs placebo• Minimal differences in systolic blood pressure and heart rate, with an average reduction in blood pressure of ~3 mm (p0.05) and 2 beats/min heart rate with 1,000mg dose• No difference in serious adverse events (6%-7% of patients in each of the 3 groupsConclusions• Among patients with symptomatic chronic angina already treated with anti-anginal drugs, treatment with ranolazine was associated with an improvement in exercise duration, time to onset of angina, and time to ischemia• Results similar to MARISA trial which tested ranolazine monotherapyPlacebo 750 mg ranolazine
Time to onset of angina 750 mg vs placebo, p=0.011000 mg vs placebo, p=0.03
seco
nd
s
1000 mg ranolazine JAMA. 2004;291:309-316

www.cardiosource.com
11.6
14.3
0
5
10
15
20
22.023.0
0
10
20
30
CARP
Mortality atfollow-up
%
Trial Design: CARP (n=510) was a multicenter, VA-based randomized trial of revascularizationvs medical management prior to elective vascular surgery in stable patients with angiographicevidence of coronary artery disease. Primary endpoint: Long-term mortality through studyperiod (median follow-up 2.7 years).
Presented at AHA Scientific Sessions 2004
Results• One third of patients were scheduled for abdominal aortic aneurysm surgery• No difference in primary endpoint of long-term mortality by study arm (Figure)• No significant differences between study groups in 30-day mortality (3.1% vs. 3.4%, p=0.82) or post-operative MI (Figure)• Delay in time to performance of vascular surgery longer in revascularization arm (54 days vs 18 days in medical therapy arm, p<0.001)Conclusions• Routine revascularization prior to elective vascular surgery not associated with improved outcomes compared to aggressive medical management• Results support current ACC/AHA guidelines which recommend revascularization in high risk/unstable patients or patients who require revascularization independent of surgery being performedRevasc Medical Therapy
PostoperativeMI
%
p=NS p=NS

www.cardiosource.com
16.717.9
0
5
10
15
20
Results• No difference in primary endpoint of CV death, MI, or stroke between clopidogrel plus aspirin group and placebo plus aspirin group (Figure)• Secondary endpoint ↓ in clopidogrel plus aspirin group (Figure) • Benefit of clopidogrel evident in symptomatic cohort for primary endpoint (6.9% vs 7.9%, RR 0.88, p=0.046) but not in asymptomatic cohort (6.6% vs 5.5%, RR 1.20, p=0.20)• In asymptomatic cohort, mortality ↑ in clopidogrel group (5.4% vs 3.8%, p=0.04) • Moderate bleeding ↑ in clopidogrel group (2.1% vs 1.3%, p<0.001)Conclusions• Among high-risk patients with stable CV disease, dual antiplatelet therapy with aspirin plus clopidogrel was not associated with a difference in CV death, MI, or stroke compared to aspirin monotherapy
6.87.3
0
2
4
6
8
10
CHARISMA
CV death, MI, or strokeRR 0.93p = 0.22
%
Trial Design: CHARISMA was a randomized, double-blind trial of clopidogrel (n=7802; 75 mg daily) or placebo(n=7801), on top of background therapy with aspirin (75-162 mg once daily) among high-risk patients withstable cardiovascular disease. Primary endpoint was composite of cardiovascular death, MI, or stroke. Medianfollow-up was 2.3 years.
N Engl J Med 2006;354:epub before print
Clopidogrel Placebo
Death, MI, stroke or hospitalization for ischemic event
RR 0.92p = 0.04
%
www.cardiosource.com
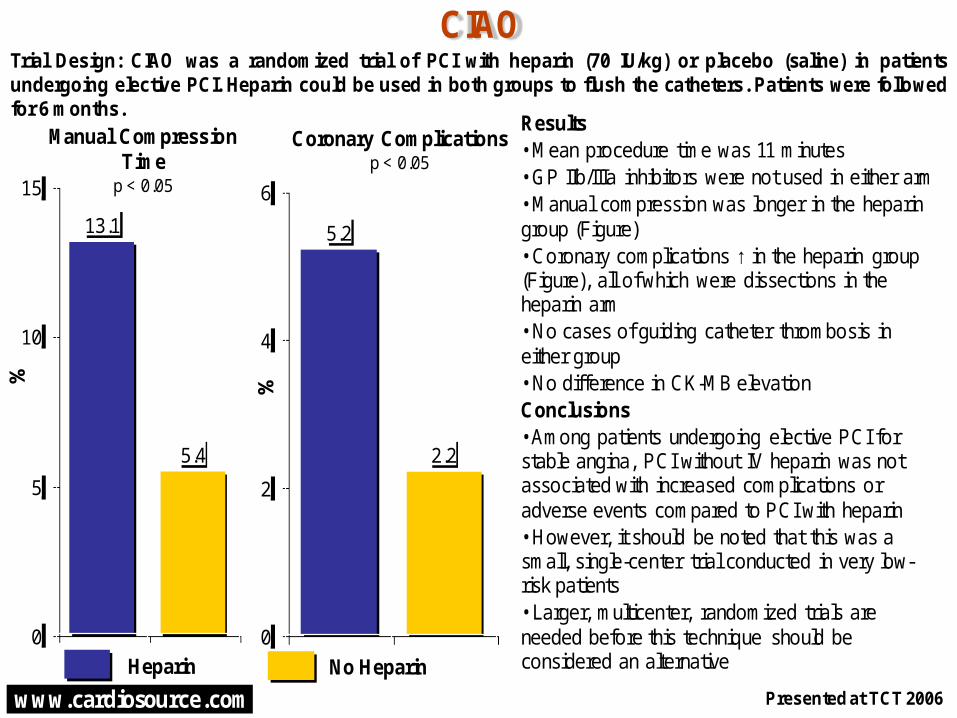
Results• Mean procedure time was 11 minutes • GP IIb/IIIa inhibitors were not used in either arm• Manual compression was longer in the heparin group (Figure)• Coronary complications ↑ in the heparin group (Figure), all of which were dissections in the heparin arm• No cases of guiding catheter thrombosis in either group• No difference in CK-MB elevationConclusions• Among patients undergoing elective PCI for stable angina, PCI without IV heparin was not associated with increased complications or adverse events compared to PCI with heparin• However, it should be noted that this was a small, single-center trial conducted in very low-risk patients• Larger, multicenter, randomized trials are needed before this technique should be considered an alternative
2.2
5.2
0
2
4
6
13.1
5.4
0
5
10
15
CIAO
Manual Compression Time
p < 0.05
%
Trial Design: CIAO was a randomized trial of PCI with heparin (70 IU/kg) or placebo (saline) in patientsundergoing elective PCI. Heparin could be used in both groups to flush the catheters. Patients were followedfor 6 months.
Presented at TCT 2006
Heparin No Heparin
Coronary Complicationsp < 0.05
%

www.cardiosource.com
Results• Multivessel disease present in 69% of patients at entry• No difference in primary endpoint of death or MI for PCI group vs. medical therapy group (Figure), components of composite, or hospitalization for ACS (12.4% for PCI vs. 11.8% for medical therapy, HR 1.07, p = 0.56)• Angina significantly ↓ in both groups during follow-up, with no difference between PCI and medical therapy at 5 years (Figure), but slightly ↑ rates of freedom from angina in early time frame with PCI• PCI costs averaged $5,295 ↑ than medical therapy through 3 years (p < 0.0001)• In cost-effectiveness analysis, PCI was estimated at $217,000 per quality-adjusted life-year gained; $50,000 often used as benchmark for acceptable C/E therapiesConclusions• Among patients with stable but severe coronary artery disease, treatment with PCI was not associated with a difference in death or MI compared with medical therapy through 5 years of follow-up, but was associated with much higher costs
7274
0
20
40
60
80
100
19.0 18.5
0
5
10
15
20
25
COURAGE
Freedom From Angina at 5 Years(p = 0.35)
%
Trial Design: COURAGE was a randomized trial of optimal medical therapy alone (n = 1,138) or PCI in additionto optimal medical therapy (n = 1,149) in patients with stable but severe coronary artery disease. Primaryendpoint was composite of death or nonfatal MI through median 4.6-year follow-up.
N Engl J Med 2007;356:1503-1516
Optimal Medical Therapy + PCI
Optimal Medical Therapy Alone
Death or MI(HR 1.05,p = 0.62)
%
www.cardiosource.com
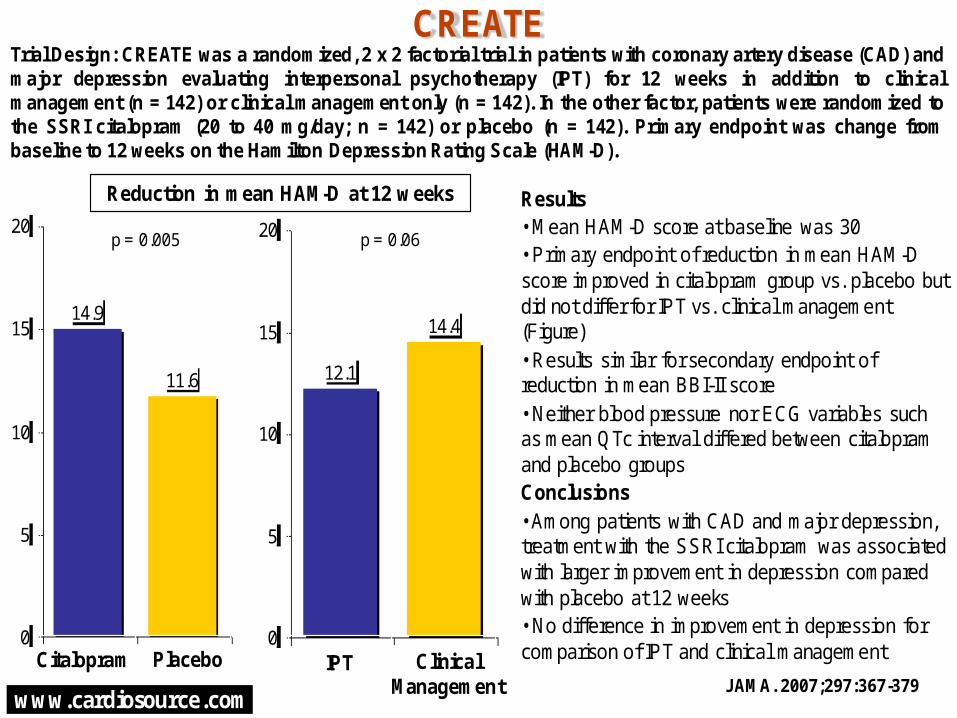
Results• Mean HAM-D score at baseline was 30• Primary endpoint of reduction in mean HAM-D score improved in citalopram group vs. placebo but did not differ for IPT vs. clinical management (Figure)• Results similar for secondary endpoint of reduction in mean BBI-II score • Neither blood pressure nor ECG variables such as mean QTc interval differed between citalopram and placebo groupsConclusions• Among patients with CAD and major depression, treatment with the SSRI citalopram was associated with larger improvement in depression compared with placebo at 12 weeks• No difference in improvement in depression for comparison of IPT and clinical management
14.4
12.1
0
5
10
15
20
14.9
11.6
0
5
10
15
20
CREATE
Reduction in mean HAM-D at 12 weeks
Trial Design: CREATE was a randomized, 2 x 2 factorial trial in patients with coronary artery disease (CAD) andmajor depression evaluating interpersonal psychotherapy (IPT) for 12 weeks in addition to clinicalmanagement (n = 142) or clinical management only (n = 142). In the other factor, patients were randomized tothe SSRI citalopram (20 to 40 mg/day; n = 142) or placebo (n = 142). Primary endpoint was change frombaseline to 12 weeks on the Hamilton Depression Rating Scale (HAM-D).
JAMA. 2007;297:367-379Citalopram Placebo
p = 0.06p = 0.005
IPT ClinicalManagement

www.cardiosource.com
-0.10
-0.06
-0.20
-0.15
-0.10
-0.05
0.00
DAIS
MinimumLumen
Diameter
mm
Trial Design: DAIS was a randomized placebo-controlled trial (n=418) designed to assesswhether correcting lipoprotein abnormalities with fenofibrate (200 mg/day) in patients with type2 diabetes would decrease the rate of angiographic progression of coronary artery disease.Primary endpoint: Change in mean coronary artery segment diameter (mm).
Lancet 2001; 357: 905-10
Results• Half of study patients had history of prior CAD.• Total cholesterol, LDL, and triglycerides significantly and HDL significantly in fenofibrate arm compared to placebo (p<0.001 for each).• Fenofibrate was associated with smaller decrease in minimum lumen diameter (-0.06 vs. -0.10 mm, p=0.029), smaller increase in % diameter stenosis (2.11 vs. 3.65%, p=0.02), and a nonsignificantly smaller decrease in primary endpoint of mean segment diameter (-0.06 vs. -0.08 mm, p=0.171).• There was a mild correlation between angiographic changes and changes in lipid profiles; effect of fenofibrate was similar in all subgroups.
Conclusions• Although the primary endpoint was not significantly different between groups, the reduced rates of disease progression measured by parameters of focal disease including % diameter stenosis and min lumen diameter suggests that lipid-lowering therapy in diabetics can result in the slowing of focal coronary atherosclerotic disease.
Placebo Fenofibrate
-0.08
-0.06
-0.20
-0.15
-0.10
-0.05
0.00
MeanSegmentDiameter
P=0.029 P=0.171
mm
www.cardiosource.com
94 9593
86
91 91
72
81
89
60
70
80
90
100
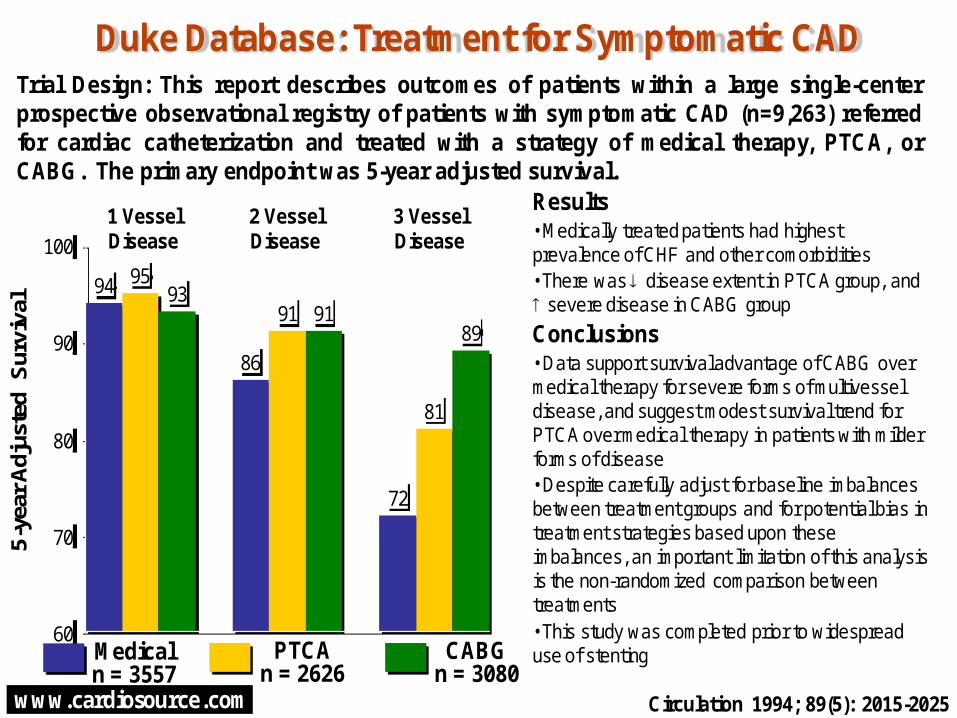
Duke Database: Treatment for Symptomatic CAD
1 VesselDisease
5-y
ear
Adj
uste
d S
urvi
val
Trial Design: This report describes outcomes of patients within a large single-centerprospective observational registry of patients with symptomatic CAD (n=9,263) referredfor cardiac catheterization and treated with a strategy of medical therapy, PTCA, orCABG. The primary endpoint was 5-year adjusted survival.
2 VesselDisease
Circulation 1994; 89(5): 2015-2025
Results• Medically treated patients had highest prevalence of CHF and other comorbidities• There was disease extent in PTCA group, and severe disease in CABG group
Conclusions• Data support survival advantage of CABG over medical therapy for severe forms of multivessel disease, and suggest modest survival trend for PTCA over medical therapy in patients with milder forms of disease• Despite carefully adjust for baseline imbalances between treatment groups and for potential bias in treatment strategies based upon these imbalances, an important limitation of this analysis is the non-randomized comparison between treatments• This study was completed prior to widespread use of stentingMedical
n = 3557
3 VesselDisease
PTCAn = 2626
CABGn = 3080

www.cardiosource.com
ENCORE-I
10.0
18.8
11.112.9
0
10
20
30 Change in acetylcholine-inducedvasoconstriction
%
Trial Design: ENCORE-I was a multicenter randomized trial of nifedipine 30-60 mg/d (n=84), cerivastatin0.4 mg/d (n=85), and their combination (n=89) vs placebo (n=85) in patients with coronary artery disease(CAD) undergoing PCI. The primary endpoint was change in acetylcholine-induced coronary vascularresponse at the highest dose of acetylcholine on the most constricted segment at 6 month follow-up.
Circulation. 2003;107:422-428
Results• Change in mean luminal diameter in most constricted segment from baseline in response to acetylcholine larger in nifedipine arm vs placebo but not cerivastatin or combo arm• Change in all segments improved in nifedipine arm and in combo arm vs placebo but not cerivastatin arm• Smaller improvement in patients not taking ACE-I in placebo group vs those taking ACE-I (6.0+/-3.6% vs 21.2+/-8.0%, p=0.11)Conclusions• Among patients with CAD undergoing PCI, treatment with nifedipine but not cerivastatin improved coronary endothelial function in the most constricted segment at 6 month follow-up • ENCORE-II underway to detect effects of nifedipine on coronary morphology Limitations• Cerivastatin withdrawn from market due to possible cases of fatal rhabdomyolysis
p=0.04
p=NS p=NS
Placebo Nifedipine Cerivastatin Cerivastatin+Nifedipine

www.cardiosource.com
3.2
5.4
0
2
4
6
Results• Primary endpoint of percent change in MLD in response to acetylcholine in nifedipine arm vs control (Figure)• In the subset of patients enrolled after cerivastatin use was discontinued, difference in primary endpoint was larger (17.5% for nifedipine vs 0.95% for control, p<0.0001)• No difference in atheroma volume on IVUS by treatment group (Figure) or in absolute change in atheroma volume (-2.1 vs 3.0 mm3, p=NS)Conclusions• Among patients with coronary heart disease, treatment with nifedipine plus statin therapy was associated with improvement in primary endpoint of coronary endothelium function at 18-24 months compared with statin therapy alone but was not associated with plaque size on IVUS• These data confirm results in ENCORE I, which also showed improvement in endothelial function associated with nifedipine plus statin therapy
18.3
6.9
0
5
10
15
20
25
ENCORE II
Change in MLDin response to acetylcholine
p = 0.0007
%
Trial Design: ENCORE II was a randomized trial of the calcium antagonist nifedipine (30-60 mg) plus statintherapy on coronary endothelial function compared with statin therapy alone among patients with coronaryheart disease. Primary endpoint was change in minimum lumen diameter (MLD) in response to acetylcholineat 18-24 month follow-up.
Presented at ESC 2004
Nifedipine Control
Atheroma volumeon IVUSp = 0.594
www.cardiosource.com
-0.0017-0.0013
0.0134
-0.0019 -0.0016
0.0036
-0.002
0.000
0.002
0.004
0.006
0.008
0.010
0.012
0.014
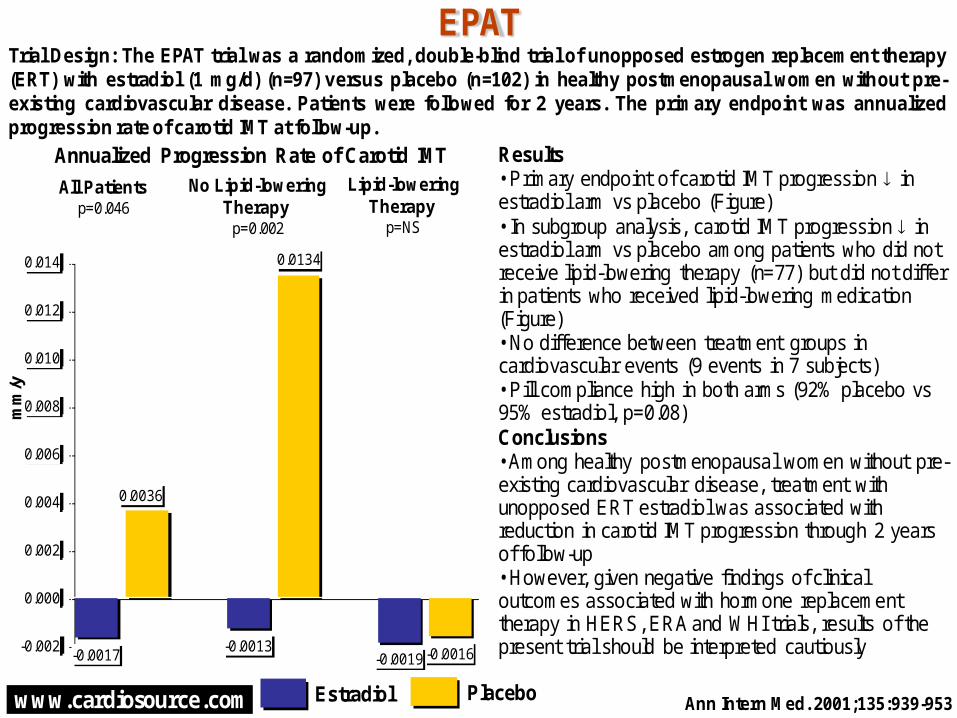
EPAT
All Patientsp=0.046
mm
/y
Trial Design: The EPAT trial was a randomized, double-blind trial of unopposed estrogen replacement therapy(ERT) with estradiol (1 mg/d) (n=97) versus placebo (n=102) in healthy postmenopausal women without pre-existing cardiovascular disease. Patients were followed for 2 years. The primary endpoint was annualizedprogression rate of carotid IMT at follow-up.
No Lipid-loweringTherapy
p=0.002
Ann Intern Med. 2001;135:939-953
Results• Primary endpoint of carotid IMT progression in estradiol arm vs placebo (Figure)• In subgroup analysis, carotid IMT progression in estradiol arm vs placebo among patients who did not receive lipid-lowering therapy (n=77) but did not differ in patients who received lipid-lowering medication (Figure)• No difference between treatment groups in cardiovascular events (9 events in 7 subjects)• Pill compliance high in both arms (92% placebo vs 95% estradiol, p=0.08)Conclusions• Among healthy postmenopausal women without pre-existing cardiovascular disease, treatment with unopposed ERT estradiol was associated with reduction in carotid IMT progression through 2 years of follow-up• However, given negative findings of clinical outcomes associated with hormone replacement therapy in HERS, ERA and WHI trials, results of the present trial should be interpreted cautiously
Estradiol Placebo
Lipid-loweringTherapy
p=NS
Annualized Progression Rate of Carotid IMT

www.cardiosource.com
Results• More patients in the intervention group met recommended fruit and vegetable intake guidelines (Figure) as did their partners• Other improvements with intervention group included reduced consumption of saturated fat to <10% of caloric intake, increased consumption of oily fish, increased physical activity targets, and increased blood pressure targets Conclusions• Among patients with or at high risk for coronary heart disease and their partners, use of nurse-led prevention intervention program was associated with improvements in lifestyle modifications compared with usual care• Present trial is one of first large-scale behavior modification/risk reduction studies to target not only coronary heart disease patients, but also partners of these patients
39
78
0
20
40
60
80
100
72
35
0
20
40
60
80
100
EUROACTION
Coronary Disease Cohort
%
Trial Design: EUROACTION was a randomized trial of usual care (n = 2,613 patients and 1,634 partners) orEuroAction intervention program (n = 2,778 patients and 1,632 partners) in patients with or at high risk forcoronary heart disease and their partners. Patients were followed for 1 year to assess adherence to lifestyle,risk factor, and therapeutic goals for CV disease prevention of the Joint European Societies’ Guidelines.
Presented at ESC 2006
Intervention Usual Care
High-Risk Cohort
Met Recommended Fruit and Vegetable Intake Guidelines

www.cardiosource.com
3.5
4.1
0
1
2
3
4
5
8.0
9.9
0
4
8
12
EUROPA
CV death/non-fatal MI/cardiac arrest
p=0.0003
%
Trial Design: EUROPA was a randomized, double-blind trial of the ACE-inhibitor perindopril (8 mg/day, n=6,110)vs placebo (n=6,108) among low-risk patients with stable coronary artery disease. Patients were followed for amean of 3.4 years. The primary endpoint was cardiovascular mortality, non-fatal MI, and cardiac arrest.
Presented at ESC 2003; Lancet 2003 362: 782-88
Results• 80% of patients remained on treatment at 3 years• Systolic blood pressure 5 mm Hg and diastolic blood pressure 2 mm Hg in the perindopril arm• Primary composite endpoint of cardiovascular mortality, non-fatal MI, and cardiac arrest in perindopril arm vs control (Figure)• Among the components of composite, CV death (Figure) and cardiac arrest (0.1% vs 0.2%) were not significantly reduced but nonfatal MI with perindopril (4.8% vs 6.2%, p=0.001)Conclusions• Among patients with stable coronary artery disease,treatment with the ACE-I perindopril was associatedwith a reduction in the primary endpoint ofcardiovascular mortality, non-fatal MI, and cardiacarrest compared with placebo• ACE inhibitors previously shown to be effective inother patient populations, including heart failure, leftventricular dysfunction, and high-risk coronary arterydisease (CAD) patients• Present trial largest to show benefit in stable, low-risk CAD patientsPerindopril Placebo
CV Mortalityp=0.107
%
www.cardiosource.com
6.78.0
9.4
12.1
0
5
10
15
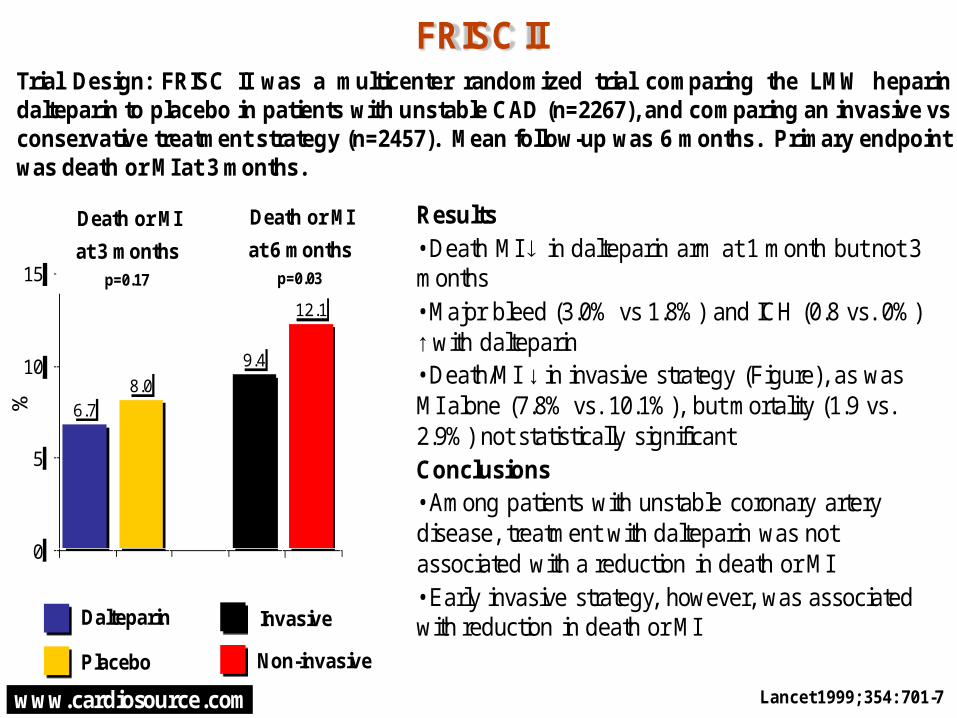
FRISC II
Lancet 1999; 354: 701-7
n=
Results• Death MI in dalteparin arm at 1 month but not 3 months• Major bleed (3.0% vs 1.8%) and ICH (0.8 vs. 0%) ↑ with dalteparin• Death/MI ↓ in invasive strategy (Figure), as was MI alone (7.8% vs. 10.1%), but mortality (1.9 vs. 2.9%) not statistically significant Conclusions• Among patients with unstable coronary artery disease, treatment with dalteparin was not associated with a reduction in death or MI • Early invasive strategy, however, was associated with reduction in death or MI
Trial Design: FRISC II was a multicenter randomized trial comparing the LMW heparindalteparin to placebo in patients with unstable CAD (n=2267), and comparing an invasive vsconservative treatment strategy (n=2457). Mean follow-up was 6 months. Primary endpointwas death or MI at 3 months.
%
Dalteparin
Placebo
Invasive
Non-invasive
Death or MI
at 6 monthsp=0.03
Death or MI
at 3 monthsp=0.17
www.cardiosource.com
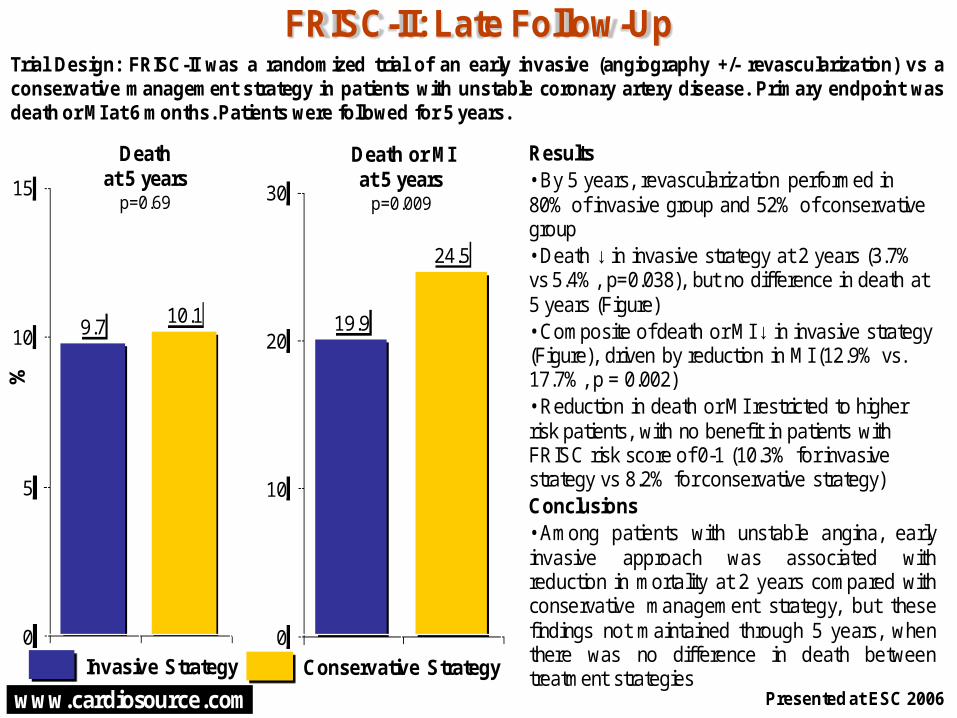
Results• By 5 years, revascularization performed in 80% of invasive group and 52% of conservative group• Death ↓ in invasive strategy at 2 years (3.7% vs 5.4%, p=0.038), but no difference in death at 5 years (Figure)• Composite of death or MI ↓ in invasive strategy (Figure), driven by reduction in MI (12.9% vs. 17.7%, p = 0.002)• Reduction in death or MI restricted to higher risk patients, with no benefit in patients with FRISC risk score of 0-1 (10.3% for invasive strategy vs 8.2% for conservative strategy)Conclusions• Among patients with unstable angina, earlyinvasive approach was associated withreduction in mortality at 2 years compared withconservative management strategy, but thesefindings not maintained through 5 years, whenthere was no difference in death betweentreatment strategies
24.5
19.9
0
10
20
30
9.710.1
0
5
10
15
FRISC-II: Late Follow-Up
Death or MIat 5 years
p=0.009
%
Trial Design: FRISC-II was a randomized trial of an early invasive (angiography +/- revascularization) vs aconservative management strategy in patients with unstable coronary artery disease. Primary endpoint wasdeath or MI at 6 months. Patients were followed for 5 years.
Presented at ESC 2006
Invasive Strategy Conservative Strategy
Deathat 5 years
p=0.69

www.cardiosource.com
HERS
JAMA 1998;280(7):605-13
# of
eve
nts
Results• No difference in CHD events between groups (Figure)• Patients in HRT arm had 11% LDL and 10% HDL (p<0.001 each)• Venous thromboembolic events in HRT group, as was gallbladder disease (Figure)Conclusions• Among post-menopausal women with established CHF, use of HRT was not associated with CHD events was associated with risk of VTE and gallbladder disease• Based on findings of no overall cardiovascular benefit and possible increased adverse events, HRT for secondary prevention of CHD not recommended
Trial Design: HERS was a multicenter randomized trial of estrogen + progestin (n=1,380) compared toplacebo (n=1,383) in prevention of coronary heart disease (CHD) events in postmenopausal womenwith established CHD. Average follow up was 4.1 years. Primary endpoint was CHD death or nonfatalMI.
172 176
34
12
84
62
0
50
100
150
200
HRT Placebo
CHD events
GallbladderDisease
HR 1.38 (1.0-1.92)
VTEHR 2.89 (1.5-5.58)
HR 0.99 (0.8-1.22)
www.cardiosource.com
21.7
17.3
0
5
10
15
20
25
30
HIT
Nonfatal MI or Death from CAD
%
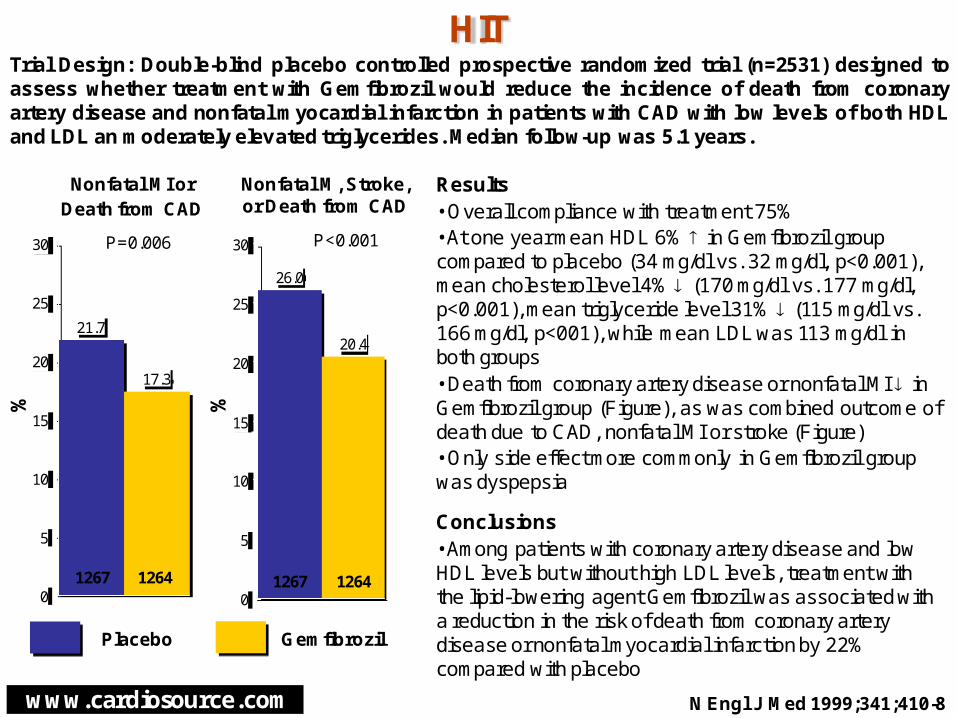
Trial Design: Double-blind placebo controlled prospective randomized trial (n=2531) designed toassess whether treatment with Gemfibrozil would reduce the incidence of death from coronaryartery disease and nonfatal myocardial infarction in patients with CAD with low levels of both HDLand LDL an moderately elevated triglycerides. Median follow-up was 5.1 years.
N Engl J Med 1999;341;410-8
Results• Overall compliance with treatment 75%• At one year mean HDL 6% in Gemfibrozil group compared to placebo (34 mg/dl vs. 32 mg/dl, p<0.001), mean cholesterol level 4% (170 mg/dl vs. 177 mg/dl, p<0.001), mean triglyceride level 31% (115 mg/dl vs. 166 mg/dl, p<001), while mean LDL was 113 mg/dl in both groups• Death from coronary artery disease or nonfatal MI in Gemfibrozil group (Figure), as was combined outcome of death due to CAD, nonfatal MI or stroke (Figure)• Only side effect more commonly in Gemfibrozil group was dyspepsia
Conclusions• Among patients with coronary artery disease and low HDL levels but without high LDL levels, treatment with the lipid-lowering agent Gemfibrozil was associated with a reduction in the risk of death from coronary artery disease or nonfatal myocardial infarction by 22% compared with placebo
Placebo Gemfibrozil
26.0
20.4
0
5
10
15
20
25
30
Nonfatal M, Stroke,or Death from CAD
12641267 1267 1264
P=0.006 P<0.001%

www.cardiosource.com
4.0
5.3
0
2
4
6
Results• Baseline homocysteine levels 12.2 µmol/L; ↓ to 9.9 µmol/L at 2 years in folic group• No difference in primary endpoint of CV death, MI, or stroke between folic group and placebo plus aspirin group (Figure)• Stroke ↓ in folic group (Figure)• No difference in cancer (13.0% vs. 12.3%, RR 1.06, p = 0.47) or cancer death (3.4% each) between treatment groupsConclusions• Among patients with pre-existing CV disease or diabetes, treatment with homocysteine lowering vitamins folic acid and vitamin B were not associated with reduction in composite of death, MI, or stroke at 5-year follow-up compared with placebo• Despite reducing homocysteine concentrations by ~25%, there was no apparent clinical benefit with folic acid and vitamin B treatment on CV events, with the exception of reduction in stroke
18.819.8
0
5
10
15
20
25
HOPE-2
CV Death, MI, or Stroke(RR 0.95p = 0.41)
%
Trial Design: HOPE-2 was a randomized, double-blind trial of treatment with folic acid 2.5 mg, vitamins B6 50mg and B12 1 mg (n = 2,758), or placebo (n = 2,764) among patients with pre-existing cardiovascular (CV)disease or diabetes. Primary endpoint was composite of CV death, MI, or stroke. Mean follow-up was 5 years.
N Engl J Med 2006;354:1567-77
Folic Vitamin Placebo
Stroke(RR 0.75p = 0.03)
%

www.cardiosource.com
Results• HDL at follow-up ↑ in torcetrapib group vs. atorvastatin alone group (72.1 mg/dl vs. 43.9 mg/dl, p < 0.001)• BP ↑ in torcetrapib group by 6.5/2.8 mm Hg• No difference in primary endpoint of change in percent atheroma volume (Figure)• Mortality was 1.4% in torcetrapib group and 1.0% in atorvastatin alone group• Clinical composite endpoint did not differ between groups (Figure)• Blood pressure-related adverse events ↑ in torcetrapib group (23.7% vs. 10.6%)Conclusions• Among patients with coronary disease, treatment with CETP inhibitor torcetrapib in addition to atorvastatin was not associated with a difference in change in percent atheroma volume compared with atorvastatin alone at 24-month follow-up• No effect on atherosclerosis progression, despite having expected impact on ↑ HDL and ↓ LDL• Commercial development of torcetrapib recently halted after large trial showed ↑ in mortality with torcetrapib
0.12
0.19
0.0
0.1
0.2
0.3
ILLUSTRATE%
Trial Design: ILLUSTRATE was a randomized, double-blind trial of torcetrapib (60 mg; n = 591), a cholesterylester transfer protein (CETP) inhibitor, in addition to atorvastatin vs. atorvastatin alone (n = 597) in patientswith coronary disease. Patients underwent IVUS at baseline and 24 months. Primary endpoint was change inpercent atheroma volume.
N Engl J Med 2007;356:1304-16
Torcetrapib Control
Change in Percent Atheroma Volume
(p = 0.72)
21.019.6
0
10
20
30
CHD Death, MI, Stroke, Hospitalization for UA,
or Coronary Revascularization
(p = NS)

www.cardiosource.com
Results• Time from surgery to randomization 4 days• No significant difference in primary composite endpoint by treatment group, but was directionally ↑ in quinapril group (HR 1.15, p=0.21)• No difference in any component of composite endpoint, including CV death or resuscitated cardiac arrest (Figure)• Primary endpoint showed ↑ risk in quinapril group vs placebo during first 3 months following CABG (HR 1.52, p=0.04), but no difference after 3 months (HR 1.08, p=0.52)Conclusions• Among patients undergoing CABG, initiation of ACE inhibitor quinapril early post-surgery was not associated with difference in primary composite endpoint compared with placebo at median 3 year follow-up, with data suggesting possible increased risk during first 3 months following surgery
1.6
1.3
0
1
2
IMAGINE
CV death orresuscitated cardiac arrest
p=NS
Trial Design: IMAGINE was a randomized trial of the ACE-inhibitor quinapril (up to 40 mg daily) (n=1,280) orplacebo (n=1,273) in patients early (within 7 days) following coronary bypass surgery. Primary endpoint wasComposite of CV death or resuscitated cardiac arrest, nonfatal MI, coronary revascularization, hospitalizationfor unstable angina, documented angina not requiring hospitalization, stroke, or heart failure requiringhospitalization at median 3 year follow-up.
Presented at ESC 2005
Quinapril Placebo
%
www.cardiosource.com
9.9 10.2
7.8 7.9
1.2 1.3
0
2
4
6
8
10
12
INVEST
Death/MI/StrokeRR 0.98p=0.57
%
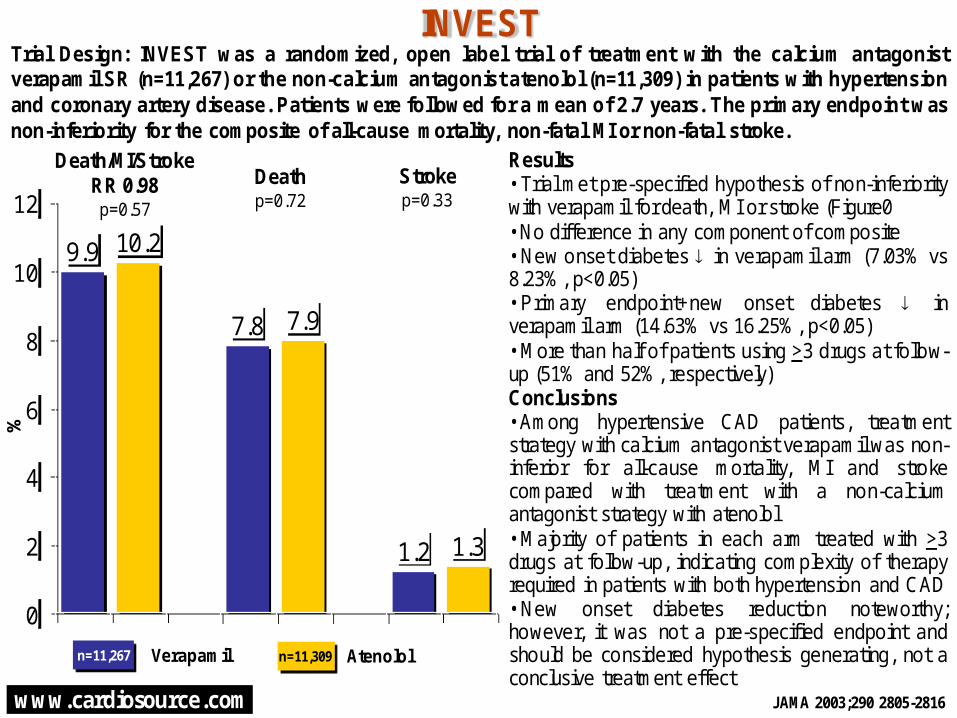
Trial Design: INVEST was a randomized, open label trial of treatment with the calcium antagonistverapamil SR (n=11,267) or the non-calcium antagonist atenolol (n=11,309) in patients with hypertensionand coronary artery disease. Patients were followed for a mean of 2.7 years. The primary endpoint wasnon-inferiority for the composite of all-cause mortality, non-fatal MI or non-fatal stroke.
Deathp=0.72
Results• Trial met pre-specified hypothesis of non-inferioritywith verapamil for death, MI or stroke (Figure0• No difference in any component of composite• New onset diabetes in verapamil arm (7.03% vs8.23%, p<0.05)• Primary endpoint+new onset diabetes inverapamil arm (14.63% vs 16.25%, p<0.05)• More than half of patients using >3 drugs at follow-up (51% and 52%, respectively)Conclusions• Among hypertensive CAD patients, treatmentstrategy with calcium antagonist verapamil was non-inferior for all-cause mortality, MI and strokecompared with treatment with a non-calciumantagonist strategy with atenolol• Majority of patients in each arm treated with >3drugs at follow-up, indicating complexity of therapyrequired in patients with both hypertension and CAD• New onset diabetes reduction noteworthy;however, it was not a pre-specified endpoint andshould be considered hypothesis generating, not aconclusive treatment effect
Strokep=0.33
Verapamil Atenolol n=11,267 n=11,309
JAMA 2003;290 2805-2816

www.cardiosource.com
HR Through 3 Years
Any CV Event 0.61
Stroke 0.60
HF Hosp. 0.54
Angina Hosp. 0.35
Results• Trial discontinued early due to evidence of benefit• Blood pressure ↓ at follow-up by 8.2 mm Hg/4.7 mm Hg in valsartan group and 7.2 mm Hg/3.7 mm Hg in control group• Primary endpoint of any CV event ↓ in valsartan group vs. control group (Figure, p = 0.00021)• Stroke ↓ in valsartan group (p = 0.028), as was heart failure hospitalizations (p = 0.029) and angina hospitalizations (p < 0.0001) • No difference in death or MIConclusions• Among Japanese patients with heart failure, ischemic heart disease, or hypertension, addition of valsartan to usual care was associated with reduction in primary endpoint of any CV event compared with usual care alone at median 3-year follow-up• Benefit in CV events in valsartan group not fully explained by blood pressure reduction
JIKEI Heart StudyTrial Design: JIKEI was a randomized trial of usual care plus valsartan (80 mg/d, titrated to 40-160 mg/d) (n =1,541) or usual care alone (n = 1,540) in Japanese patients with heart failure, ischemic heart disease, orhypertension. Primary endpoint was any cardiovascular (CV) event at 3-year follow-up.
Presented at ESC 2006
Valsartan Better Control Better
1.00.5 1.5

www.cardiosource.com
Results• At baseline, mean CIMT 1.15 mm in rosuvastatin group and 1.17 mm in placebo group• LDL levels ↓ to greater extent in rosuvastatin group vs placebo group (-48.8% vs. -0.3%, p < 0.001) and HDL levels ↑ to greater extent in rosuvastatin group • Change in CIMT showed nonsignificant regression in rosuvastatin group and progression in placebo group (Figure)• Myalgia occurred in 12.7% of rosuvastatin group and 12.1% of placebo groupConclusions• Among asymptomatic patients at low risk for cardiovascular disease, treatment with rosuvastatin was associated with reduction in CIMT compared with placebo at 2 years• ASTEROID trial previously showed regression in atherosclerosis disease, as assessed by intravascular ultrasound with rosuvastatin, but did not have comparator arm• Impact of aggressive lipid lowering on clinical events not evaluated in this trial, particularly given low risk population• Larger JUPITER trial will evaluate impact of rosuvastatin therapy on clinical events in patients with low to normal LDL, but elevated CRP
-0.0014
0.0131
-0.01
0.00
0.01
0.02
METEORm
m/y
ear
Trial Design: METEOR was a randomized (5:2), double-blind trial of rosuvastatin (40 mg; n = 702) or placebo (n= 282) in patients at low risk for cardiovascular disease. Patients underwent carotid ultrasound prior torandomization and at 6, 12, 18, and 24 months. Primary endpoint was annualized rate of change in maximumcarotid intima-media thickness (CIMT).
JAMA 2007;297:1344-53
Rosuvastatin Placebo
Annual change in CIMT for 12 carotid
artery sites p < 0.001
90
20
0
20
40
60
80
100
120115
60
0
20
40
60
80
100
120
NICE
All patients at 12 weeks
p = 0.087
Sec
on
ds
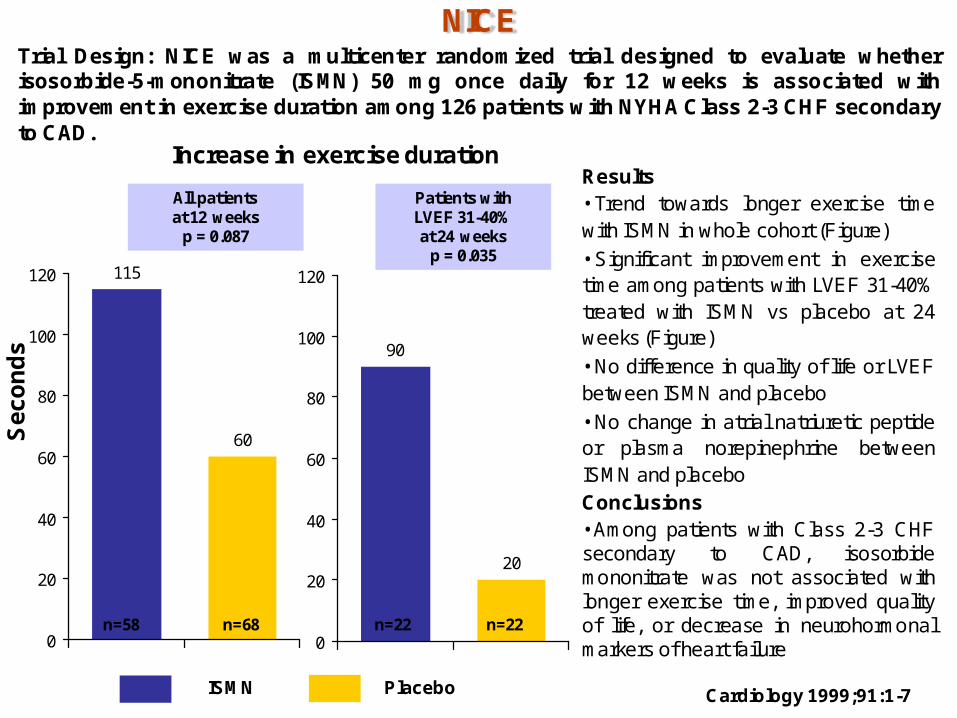
Trial Design: NICE was a multicenter randomized trial designed to evaluate whetherisosorbide-5-mononitrate (ISMN) 50 mg once daily for 12 weeks is associated withimprovement in exercise duration among 126 patients with NYHA Class 2-3 CHF secondaryto CAD.
Cardiology 1999;91:1-7
Results• Trend towards longer exercise timewith ISMN in whole cohort (Figure)
• Significant improvement in exercisetime among patients with LVEF 31-40%treated with ISMN vs placebo at 24weeks (Figure)
• No difference in quality of life or LVEFbetween ISMN and placebo
• No change in atrial natriuretic peptideor plasma norepinephrine betweenISMN and placeboConclusions• Among patients with Class 2-3 CHFsecondary to CAD, isosorbidemononitrate was not associated withlonger exercise time, improved qualityof life, or decrease in neurohormonalmarkers of heart failure
ISMN Placebo
Patients with LVEF 31-40% at 24 weeks
p = 0.035
n=68n=58 n=22 n=22
Increase in exercise duration

www.cardiosource.com
54.063.0
0
25
50
75
100
PATCH
Placebo EDTA
Time to ischemiap = 0.69
JAMA 2002; 287 (4):481-6
n=43 n=41
Sec
onds
Results• Mean time to ischemia by average of 54 seconds (95% CI 23 to 84, p<0.001) in placebo group vs 63 seconds (95% CI 29 to 95, p<0.001) in EDTA group • Mean difference between two groups not statistically significant at 9 seconds (95% CI -36 to 53, p=0.69; Figure)• No significant difference between two groups in VO2
time to anaerobic threshold, Duke Activity Status Index, Seattle Angina Questionnaire, or Health Status Survey Short FormConclusions• Among patients with coronary artery disease and stable angina, chelation therapy with EDTA was not associated with a significant improvement in quality of life or exercise capacity compared to placebo• These findings suggest that chelation therapy with EDTA is not effective in patients with chronic, stable, ischemic heart disease
Trial Design: PATCH was a multi-center randomized trial of chelation therapy with EDTA compared withplacebo in patients with stable ischemic heart disease. Patients were followed for 27 weeks. Theprimary endpoint was the change in time required in order to achieve a minimum of 1 mm ST segmentdepression on a treadmill test 27 weeks after randomization.
www.cardiosource.com
9.8
11.5
0
5
10
15
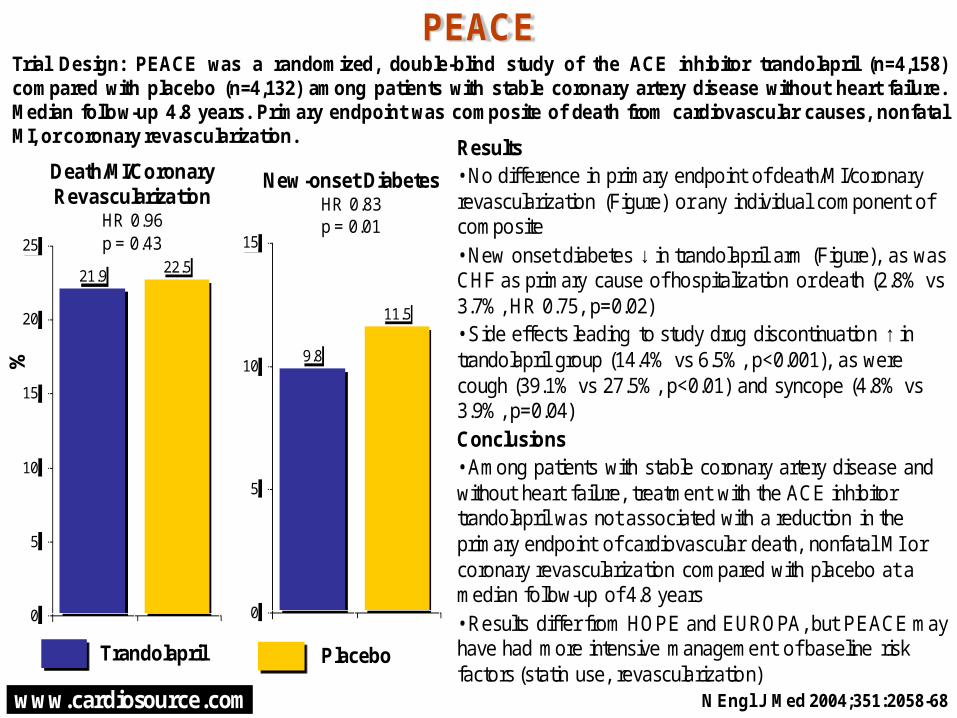
Results• No difference in primary endpoint of death/MI/coronary revascularization (Figure) or any individual component of composite• New onset diabetes ↓ in trandolapril arm (Figure), as was CHF as primary cause of hospitalization or death (2.8% vs 3.7%, HR 0.75, p=0.02) • Side effects leading to study drug discontinuation ↑ in trandolapril group (14.4% vs 6.5%, p<0.001), as were cough (39.1% vs 27.5%, p<0.01) and syncope (4.8% vs 3.9%, p=0.04)Conclusions• Among patients with stable coronary artery disease and without heart failure, treatment with the ACE inhibitor trandolapril was not associated with a reduction in the primary endpoint of cardiovascular death, nonfatal MI or coronary revascularization compared with placebo at a median follow-up of 4.8 years• Results differ from HOPE and EUROPA, but PEACE may have had more intensive management of baseline risk factors (statin use, revascularization)
21.922.5
0
5
10
15
20
25
PEACE
New-onset DiabetesHR 0.83p = 0.01
Trial Design: PEACE was a randomized, double-blind study of the ACE inhibitor trandolapril (n=4,158)compared with placebo (n=4,132) among patients with stable coronary artery disease without heart failure.Median follow-up 4.8 years. Primary endpoint was composite of death from cardiovascular causes, nonfatalMI, or coronary revascularization.
N Engl J Med 2004;351:2058-68
Trandolapril Placebo
Death/MI/CoronaryRevascularization
HR 0.96p = 0.43
%
www.cardiosource.com
3.3
2.9
0
1
2
3
4
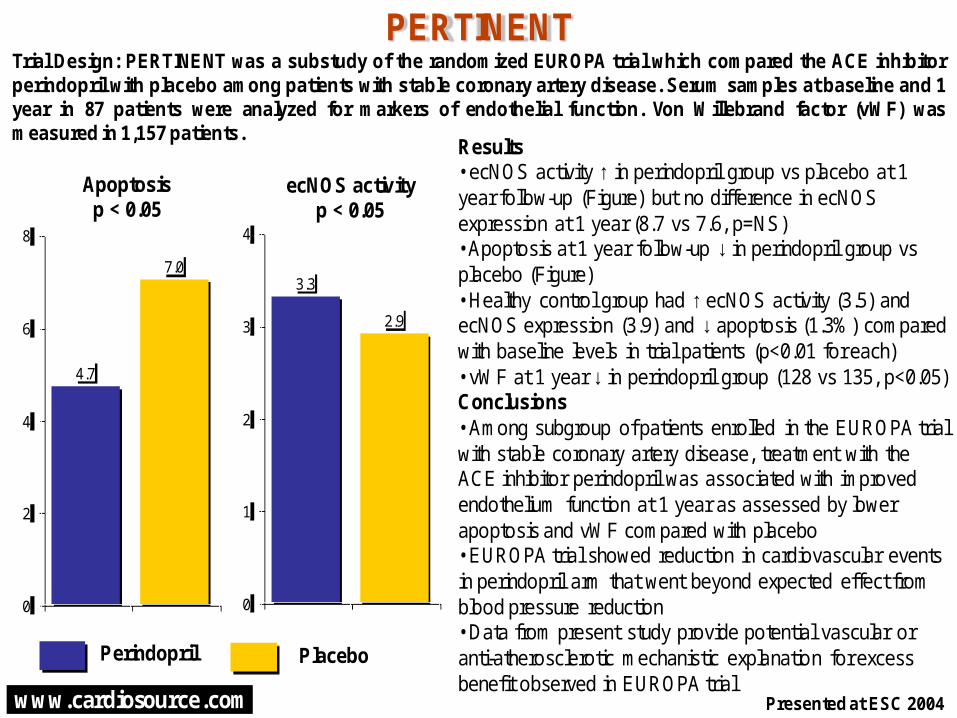
Results• ecNOS activity ↑ in perindopril group vs placebo at 1 year follow-up (Figure) but no difference in ecNOS expression at 1 year (8.7 vs 7.6, p=NS)• Apoptosis at 1 year follow-up ↓ in perindopril group vs placebo (Figure)• Healthy control group had ↑ ecNOS activity (3.5) and ecNOS expression (3.9) and ↓ apoptosis (1.3%) compared with baseline levels in trial patients (p<0.01 for each)• vWF at 1 year ↓ in perindopril group (128 vs 135, p<0.05)Conclusions• Among subgroup of patients enrolled in the EUROPA trial with stable coronary artery disease, treatment with the ACE inhibitor perindopril was associated with improved endothelium function at 1 year as assessed by lower apoptosis and vWF compared with placebo• EUROPA trial showed reduction in cardiovascular events in perindopril arm that went beyond expected effect from blood pressure reduction• Data from present study provide potential vascular or anti-atherosclerotic mechanistic explanation for excess benefit observed in EUROPA trial
4.7
7.0
0
2
4
6
8
PERTINENT
ecNOS activityp < 0.05
Trial Design: PERTINENT was a substudy of the randomized EUROPA trial which compared the ACE inhibitorperindopril with placebo among patients with stable coronary artery disease. Serum samples at baseline and 1year in 87 patients were analyzed for markers of endothelial function. Von Willebrand factor (vWF) wasmeasured in 1,157 patients.
Presented at ESC 2004
Perindopril Placebo
Apoptosisp < 0.05

www.cardiosource.com
Results• Hs-CRP at 12 weeks was reduced from baseline in all three treatment groups, but to a greater degree with combination therapy (from 3.49 mg/L to 2.06 mg/L, p < 0.001) than pioglitazone and simvastatin monotherapy groups (3.64 mg/L to 2.48 mg/L and 3.26 mg/L to 2.81 mg/L)• No change in LDL cholesterol from baseline to 12 weeks in pioglitazone group (from 3.50 to 3.56 mmol/L) but LDL was reduced from baseline in simvastatin group (from 3.60 to 2.32 mmol/L) and combination group (from 3.68 to 2.40 mmol/L)• Peripheral edema was highest in combination group (Figure)Conclusions• Among nondiabetic patients with CV disease and elevated hs-CRP, treatment with combination of pioglitazone and simvastatin was associated with greater reduction in hs-CRP at 12 weeks compared with monotherapy• Pioglitazone was shown to reduce composite of death, MI, or stroke by 3 years in PROactive trial in type 2 diabetics, but as with the present study, was associated with excess of edema• Data from present study extend observations of pioglitazone in nondiabetic patients to show reduction in inflammatory parameters
7.0
11.4
22.2
0
5
10
15
20
25
PIOSTAT
Peripheral Edema
%
Trial Design: PIOSTAT was a randomized, double-blind trial of 12 weeks of treatment with simvastatin plusplacebo (40 mg; n = 43), pioglitazone plus placebo (45 mg; n = 39), or simvastatin plus pioglitazonecombination (n = 43) in nondiabetic patients with CV disease and elevated hs-CRP. Primary endpoint waschange in hs-CRP from baseline to 12-week follow-up.
J Am Coll Cardiol 2007;49:290-7
Simvastatin Pioglitazone
Combination

www.cardiosource.com
14.1
16.2
10.1
12.2
3.34.2
0
5
10
15
20
PROSPER Trial
Prava-statin
Placebo
Dth / MI / strokep = 0.014
%
Trial Design: The PROSPECT trial was a multi-center randomized trial of pravastatincompared with placebo in 5,804 elderly patients with or at high-risk for cardiovasculardisease. Follow-up averaged 3.2 years. The primary endpoint was CV death / MI / stroke.
Dth / MIp = 0.006
Deathp = 0.043
Lancet 2002; 360: 1623–30
Results• Primary endpoint significantly reducedin the pravastatin arm• All components of the endpoint except
stroke showed a benefit with pravastatin
Conclusions• PROSPER was the first major trial toshow a benefit with a lipid-lowering agentspecifically in high-risk elderly patients
Limitations•The major safety concern was the rateof any cancer in the pravastatin arm(8.5% vs 6.8%), which was not confirmedin a meta-analysis
Prava-statin
Placebo Prava-statin
Placebo

www.cardiosource.com
Results• Mean number of injections 14.6/patient, with mean procedural time of 152 minutes• At 6 month follow-up, primary endpoint of exercise time improved in BMC group but did not differ in control group (Figure)• No sustained ventricular tachycardias on Holter and no symptomatic arrhythmias• One patient in control group and no patients in BMC group died during follow-upConclusions• Among patients with severe CAD who have failed conventional therapies, endomyocardial implantation of autologous bone marrow mononuclear cells associated with longer exercise duration at 6 month follow-up compared with baseline but no difference in control group, although direct head-to-head comparison between BMC and control group was not made• Larger trials would be needed to validate findings• No dose response observed between low and high dose groups
392
439464
404
0
200
400
600
PROTECT-CAD
Exercise Treadmill Time at Baseline and Follow-up
p < 0.05 for BMCp = NS for control
sec
Trial Design: PROTECT-CAD was a randomized trial of bone marrow mononuclear cells (BM MNC) (1x106 or2x106 cells/0.1 ml, n=19) or control (n=9) via catheter-based direct endomyocardial injection using guidedelectromechanical mapping among patients with severe coronary artery disease who have failed conventionaltherapies. Primary endpoint was exercise treadmill time at 6 months.
Presented at ACC 2006
BMC; Follow-up Control; Follow-up
BMC; Baseline Control; Baseline
www.cardiosource.com
38 38
0
20
40
60
80
QUIET
Frequencyof Cardiac
Events
%
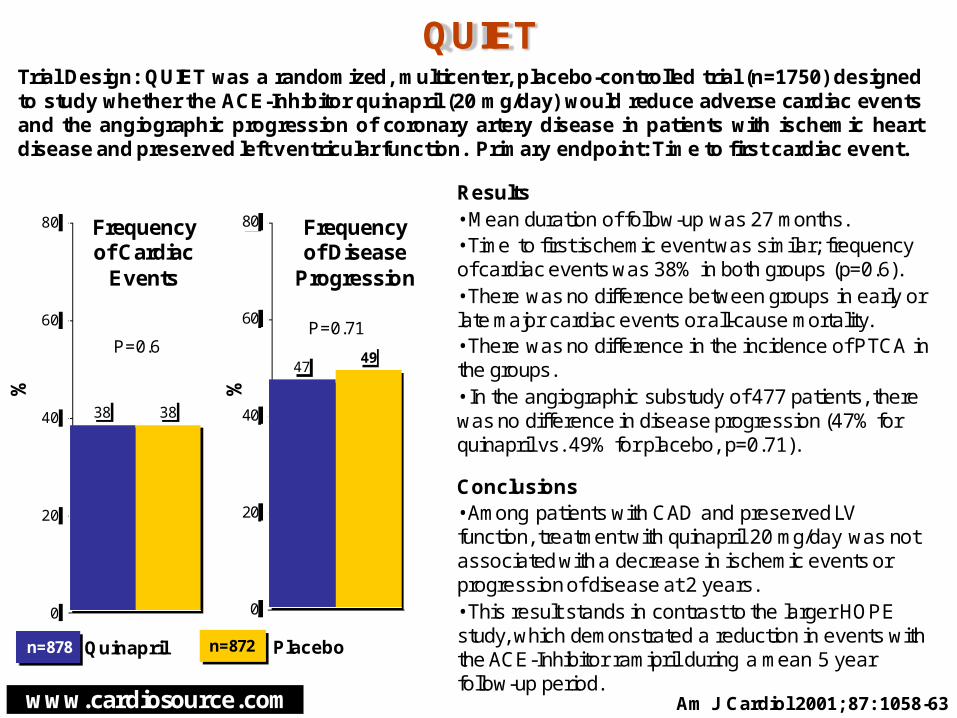
Trial Design: QUIET was a randomized, multicenter, placebo-controlled trial (n=1750) designedto study whether the ACE-Inhibitor quinapril (20 mg/day) would reduce adverse cardiac eventsand the angiographic progression of coronary artery disease in patients with ischemic heartdisease and preserved left ventricular function. Primary endpoint: Time to first cardiac event.
Am J Cardiol 2001; 87: 1058-63
Results• Mean duration of follow-up was 27 months.• Time to first ischemic event was similar; frequency of cardiac events was 38% in both groups (p=0.6).• There was no difference between groups in early or late major cardiac events or all-cause mortality.• There was no difference in the incidence of PTCA in the groups.• In the angiographic substudy of 477 patients, there was no difference in disease progression (47% for quinapril vs. 49% for placebo, p=0.71).
Conclusions• Among patients with CAD and preserved LV function, treatment with quinapril 20 mg/day was not associated with a decrease in ischemic events or progression of disease at 2 years.• This result stands in contrast to the larger HOPE study, which demonstrated a reduction in events with the ACE-Inhibitor ramipril during a mean 5 year follow-up period.
Quinapril Placebo
4749
0
20
40
60
80 Frequencyof Disease
Progression
n=872n=878
P=0.6P=0.71
%

www.cardiosource.com
3.53.9
1.7
0
5
10
REACH Registry
CV Death/ MI / Strokeat 1 Year
%
Results• At baseline, diabetes present in 44.1% of subjects, hypercholesterolemia in 72.1%, and multiple risk factors in 18.3%• At 1 year, composite of CV death, MI or stroke ↑ in symptomatic patients than asymptomatic patients (Figure)• Among cohort with single arterial disease (CAD, CVD, or PAD), CV death, MI or stroke occurred in 3.4% of population vs 6.0% in patients with polyvascular disease• Highest event rates were in patients with CAD, CVD and PVD (7.4%)Conclusions• Among patients with stable or at high-risk for atherothrombosis, CV event rates were relatively high and increased with number of symptomatic arterial diseases compared with patients with risk factors only• Geographic variation existed in event rates, as did variation in age group and less so by gender
Trial Design: The REACH Registry followed patients with stable atherothrombosis toevaluate risk factors and cardiovascular event rates. Patients were followed for 1 year.
Presented at ACC 2006
All patients
Symptomatic patients
Asymptomatic patients
www.cardiosource.com
89
81
0
20
40
60
80
100
-0.10
-0.06
-0.12
-0.10
-0.08
-0.06
-0.04
-0.02
0.00
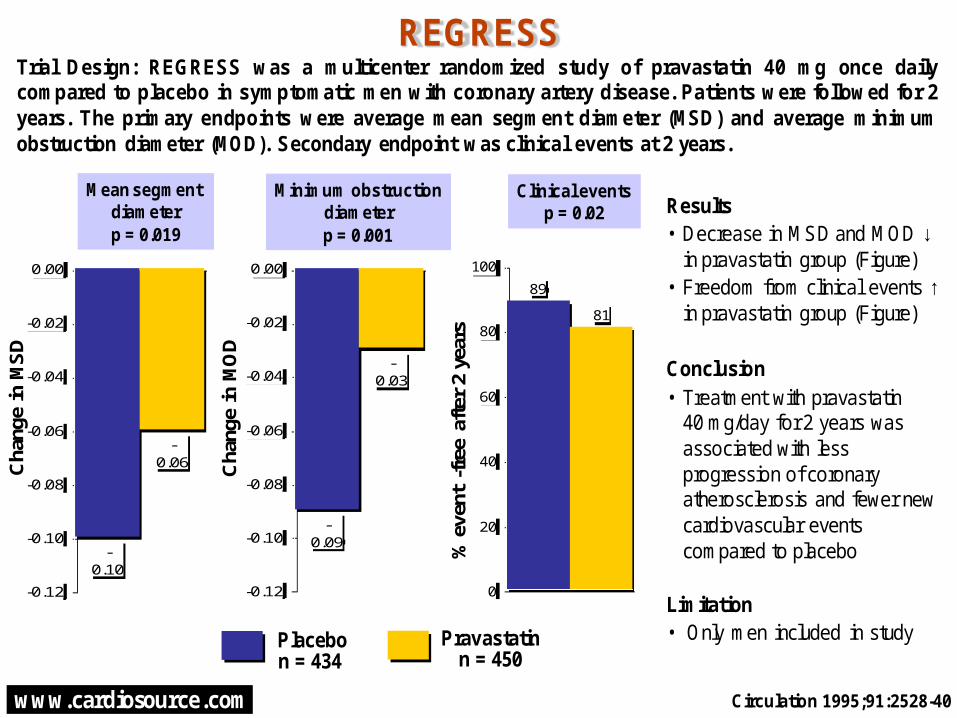
REGRESS
Mean segment diameterp = 0.019
Cha
nge
in M
SD
Trial Design: REGRESS was a multicenter randomized study of pravastatin 40 mg once dailycompared to placebo in symptomatic men with coronary artery disease. Patients were followed for 2years. The primary endpoints were average mean segment diameter (MSD) and average minimumobstruction diameter (MOD). Secondary endpoint was clinical events at 2 years.
Minimum obstructiondiameterp = 0.001
Circulation 1995;91:2528-40
Results• Decrease in MSD and MOD ↓
in pravastatin group (Figure)• Freedom from clinical events ↑
in pravastatin group (Figure)
Conclusion• Treatment with pravastatin
40 mg/day for 2 years was associated with less progression of coronary atherosclerosis and fewer new cardiovascular events compared to placebo
Limitation• Only men included in studyPlacebo
n = 434
Clinical eventsp = 0.02
Pravastatinn = 450
Cha
nge
in M
OD
% e
vent
-fre
e af
ter
2 ye
ars
-0.09
-0.03
-0.12
-0.10
-0.08
-0.06
-0.04
-0.02
0.00

www.cardiosource.com
0.4
1.1
0.0
0.5
1.0
1.5
REVASC
* P-values for changefrom baseline time
Min
utes
to
1mm
S
T d
epre
ssio
nTrial Design: REVASC was a multi-center randomized trial of AdVEGF121, an angiogenic growth factor(n=27) delivered via a minithoracotomy with direct intramyocardial injections throughout the free wallof the left ventricle vs control (n=29) in patients with severely symptomatic CAD who were notcandidates for conventional revascularization. Patients were followed for 26 weeks. The primaryendpoint was exercise treadmill time to additional 1-mm ST depression at 12 weeks.
AHA 2002, Late Breaking Trials
Results• 1 endpoint of change in time to 1 mm ST depression from baseline on ETT was not improved at 12 weeks (p=0.36), but was improved at 26 weeks (p=0.024)• Total exercise duration improved at both 12 weeks (p=0.011) and 26 weeks (p=0.014), as did time to level 2 angina (p=0.006 at 12 weeks, p=0.002 at 26 weeks)• Angina frequency, stability and disease perception score from Seattle Angina Questionnaire all improved from baseline to 6, 12, and 26 weeks in the AdVEGF arm (p<0.001 for each) but not in the medical care arm • No difference in SAEs between the 2 armsConclusions• First randomized trial to deliver angiogenic genes by direct intramyocardial injections• 1 endpoint negative; many 2 endpoints favored AdVEGF armLimitations• No blinding to therapy received; placebo effect cannot be discounted• Lack of benefit with 1 endpoint and small sample size do not support clinical application of therapy; additional blinded study may be warranted
AdVEGFn = 27
12 Weeksp = 0.36*
26 Weeksp = 0.024*

www.cardiosource.com
18.6
34.3
0
10
20
30
40
SPACE
Vit E Placebo
Primary EndpointRR 0.54
p = 0.016
n=97 n=99
%
Trial design: SPACE was a multi-center, randomized, double-blind, placebo-controlled trialof high-dose vitamin E supplementation (800 IU/day) in hemodialysis patients with pre-existing cardiovascular disease. 198 patients were followed for a median time of 519 days.Primary end-point was composite of cardiovascular events (MI, PVD, Stroke, UA, orsudden death).
8.2
18.2
0
5
10
15
20
Vit E Placebo
Myocardial InfarctionRR 0.45p=0.04
Lancet 2000;356:1213-18
Results• Primary endpoint ↓ in vitamin E group (Figure)• MI ↓ in vitamin E group (Figure)• Total mortality did not differ between groups (31.2% vitamin E vs 29.3% placbeo)Conclusions• Among hemodialysis patients with pre-existing CV disease, high-dose vitamin E supplementation was associated with a significant reduction in composite cardiovascular disease endpoint and myocardial infarctionLimitations• Insufficient power to detect differences in primary endpoint components
n=97 n=99

www.cardiosource.com
3.2
8.6
10.5
14.1
0
5
10
15
20
584
142
0
200
400
600
800
St. Francis Heart Study
p<0.0001
n=122
Mea
n B
asel
ine
Cal
cific
atio
n S
core
Trial Design: The St. Francis Heart Study was a prospective study of the use of coronary calcificationassessed by electron-beam computed tomography (EBCT) for risk stratification in patients with noprior history, symptoms, or signs of atherosclerotic CVD. Patients (n=5585) were followed for 4.3 yearsto assess the development of atherosclerotic cardiovascular disease (ASCVD) events.
Presented at ACC 2003
Results• Mean calcification score in patientswho subsequently developed ASCVDevent• Presence of baseline score >100associated with incidence of anyASCVD (RR 9.5, 95% CI 6.5-13.8), allcoronary events (8.6% event rate, RR10.7, 95% CI 7.1-16.3), and MI orcoronary death (RR 9.9, 95% CI 5.2-18.9)Conclusions• Among patients with no prior history,symptoms, or signs of ASCVD,development of an ASCVD event wasassociated with baseline calcium score• Association independent of standardrisk factors in MV model and providedadditional risk stratification withinFramingham risk score
CV event NoCV event
Calcium ScoreThresholds
Pos
itive
Pre
dict
ive
Val
ue
>0
Score Threshold
>100 >200 >600
www.cardiosource.com
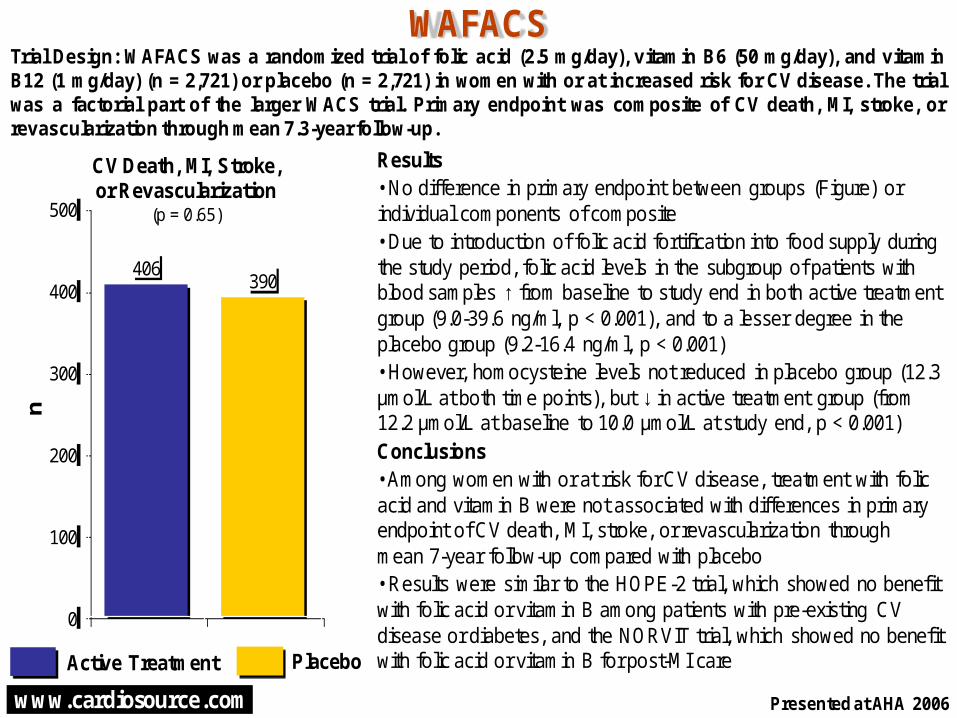
Results• No difference in primary endpoint between groups (Figure) or individual components of composite• Due to introduction of folic acid fortification into food supply during the study period, folic acid levels in the subgroup of patients with blood samples ↑ from baseline to study end in both active treatment group (9.0-39.6 ng/ml, p < 0.001), and to a lesser degree in the placebo group (9.2-16.4 ng/ml, p < 0.001)• However, homocysteine levels not reduced in placebo group (12.3 µmol/L at both time points), but ↓ in active treatment group (from 12.2 µmol/L at baseline to 10.0 µmol/L at study end, p < 0.001)Conclusions• Among women with or at risk for CV disease, treatment with folic acid and vitamin B were not associated with differences in primary endpoint of CV death, MI, stroke, or revascularization through mean 7-year follow-up compared with placebo• Results were similar to the HOPE-2 trial, which showed no benefit with folic acid or vitamin B among patients with pre-existing CV disease or diabetes, and the NORVIT trial, which showed no benefit with folic acid or vitamin B for post-MI care
406390
0
100
200
300
400
500
WAFACSn
Trial Design: WAFACS was a randomized trial of folic acid (2.5 mg/day), vitamin B6 (50 mg/day), and vitaminB12 (1 mg/day) (n = 2,721) or placebo (n = 2,721) in women with or at increased risk for CV disease. The trialwas a factorial part of the larger WACS trial. Primary endpoint was composite of CV death, MI, stroke, orrevascularization through mean 7.3-year follow-up.
Presented at AHA 2006
Active Treatment Placebo
CV Death, MI, Stroke, or Revascularization
(p = 0.65)




























