Embed Size (px)
Citation preview
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2020
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1644
Coronary angiography after out-of-hospital cardiac arrest
RICKARD LAGEDAL
ISSN 1651-6206ISBN 978-91-513-0888-3urn:nbn:se:uu:diva-406036

Dissertation presented at Uppsala University to be publicly examined in H:sonHolmdahlsalen, Ingång 100, Akademiska sjukhuset, Uppsala, Friday, 4 September 2020at 09:00 for the degree of Doctor of Philosophy (Faculty of Medicine). The examinationwill be conducted in Swedish. Faculty examiner: Professor Markus Skrifvars (Helsingforsuniversitet).
AbstractLagedal, R. 2020. Coronary angiography after out-of-hospital cardiac arrest. DigitalComprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 1644.60 pp. Uppsala: Acta Universitatis Upsaliensis. ISBN 978-91-513-0888-3.
Out-of-hospital cardiac arrest (OHCA) is a common cause of death with a survival rate of 10%in Sweden. The chance of survival depends on rapid recognition, high quality cardiopulmonaryresuscitation and post-resuscitation care including searching and treating the cause of the arrest.Ischaemic cardiac disease including acute coronary artery occlusions is the most commoncause of OHCA. Acute coronary artery lesions can be diagnosed and treated with coronaryangiography and subsequent PCI. This thesis analyses various aspects of coronary angiographyafter OHCA. Paper I+II describes the rational, protocol and the results from the pilot phase(n=117) of a randomized multicentre clinical trial. We compared a strategy of immediatecoronary angiography in patients successfully resuscitated after OHCA with a strategy withoutimmediate coronary angiography. We did not reach the stipulated time of 120 minutes from firstmedical contact to angiography, but our study strategy was feasible. No major unexpected safetyissues were reported. The main phase of the study could therefore be started with only minorchanges from the pilot phase protocol. In a registry study of 1133 patients (Paper III) coronaryangiographic findings were compared with ECG and comorbidities in unconscious patients afterOHCA. In patients without ST-elevation, the rate of PCI attempts was higher in patients withST-depression (47%) and in patients with ECG classified as “other findings” (45%) comparedto patients with normal ECG (33%), OR 1.78 (CI 1.13-2.82) and OR 1.65 (CI 1.04-2.61),respectively. When analysing patients without ST-elevation, no difference in PCI rates werefound between the comorbidity groups and neither between patients with shockable comparedto non-shockable initial ECG rhythm. Paper IV is a registry study (n=3906) analysing theimpact of patient income on the probability to receive early coronary angiography after OHCA.When dividing patients into income quarters and adjusting for confounders, increasing incomewas associated with higher rates of early coronary angiography. Thirty-six percent of patientsin the highest income quarter received early angiography compared to fifteen percent in thelowest income quarter, OR 1.64 (1.27-2.11). Adding potential mediators to explain this findinggradually decreased the difference, and the main explanatory factor for this difference was thathigher income is associated with higher rates of shockable ECG rhythm. 30-day survival wasalso higher in the highest income quarter compared to the lowest income group in the fullyadjusted analysis, OR 1.51 (CI 1.22-1.89).
Keywords: Cardiac arrest, OHCA, coronary angiography, PCI, percutaneous coronaryintervention, socioeconomy
Rickard Lagedal, Department of Surgical Sciences, Anaesthesiology and Intensive Care,Akademiska sjukhuset, Uppsala University, SE-75185 Uppsala, Sweden.
© Rickard Lagedal 2020
ISSN 1651-6206ISBN 978-91-513-0888-3urn:nbn:se:uu:diva-406036 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-406036)

“The problem with the world is that the intelligent people are full of doubts, while the stupid ones are full of confidence”
Charles Bukowski
To Ebba, Agnes and Pernilla

List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Lagedal, R., Elfwén, L., James, S., Oldgren, J., Erlinge, D., Öst-
lund, O., Wallin, E., Larsson I-M., Lilja, G., Cronberg, T., Ru-bertsson, S., Nordberg, P. (2018). Design of DISCO - Direct or Subacute Coronary Angiography in Out-of-Hospital Cardiac Arrest Study. American heart journal. 197:53-61
II Elfwén, L., Lagedal, R., Nordberg, P., James, S., Oldgren, J., Böhm, F., Lundgren P., Rylander C., van der Linden J., Hollen-berg, J., Erlinge, D., Cronberg, T., Jensen, U., Friberg, H., Lilja, G., Larsson, I-M., Wallin, E., Rubertsson, S., Svensson, L. (2019) Direct or Subacute Coronary Angiography in Out-of-Hospital Cardiac Arrest (DISCO)– an initial feasibility study of a randomized clinical trial. Resuscitation. 139:253-261
III Lagedal R., Elfwén L., Jonsson M., Lindgren E., Smekal D., Svensson L., James S., Nordberg P., Rubertsson S. (2020) Cor-onary angiographic findings after cardiac arrest in relation to ECG and comorbidity. Resuscitation. 146:213-219
IV Lagedal R., Jonsson, M., Elfwén, L., Smekal, D., Nordberg, P., James, S., Rubertsson, S. Income is associated with the proba-bility to receive early coronary angiography after out-of-hos-pital cardiac arrest. In manuscript
Reprints were made with permission from the respective publishers.

Contents
Introduction ................................................................................................... 11 History ...................................................................................................... 11 Cardiac arrest ............................................................................................ 12
Incidence and outcome ........................................................................ 12 Factors affecting outcome .................................................................... 13 Post-resuscitation care ......................................................................... 13 Initial ECG rhythm .............................................................................. 14 Causes of cardiac arrest ....................................................................... 15 Coronary angiography ......................................................................... 15 Socioeconomic status in cardiac arrest ................................................ 19 Neurologic outcomes, prognostication and follow-up ......................... 19
Aims .............................................................................................................. 22 Paper I and II ............................................................................................ 22 Paper III .................................................................................................... 22 Paper IV ................................................................................................... 22
Material and methods .................................................................................... 23 Paper I and II ............................................................................................ 23
Study enrolment and randomization .................................................... 23 Inclusion / exclusion criteria ................................................................ 23 Coronary angiography ......................................................................... 25 Post resuscitation care and withdrawal of life-sustaining therapy ....... 25 Statistical analyses ............................................................................... 25 Patient consent ..................................................................................... 26 Safety and feasibility evaluation .......................................................... 26
Paper III .................................................................................................... 26 Population and data sources ................................................................. 26 Statistics ............................................................................................... 27
Paper IV ................................................................................................... 28 Population and data sources ................................................................. 28 Statistics ............................................................................................... 28
Ethical approvals and considerations ....................................................... 28 Ethical approvals ................................................................................. 28 Ethical considerations .......................................................................... 29
Results ........................................................................................................... 31
Paper I and II – The DISCO study ........................................................... 31 Main results ......................................................................................... 32 Coronary angiography and PCI ........................................................... 32 Safety aspects ...................................................................................... 34
Paper III .................................................................................................... 36 Main results ......................................................................................... 36
Paper IV ................................................................................................... 38 Main results ......................................................................................... 38
Discussion ..................................................................................................... 41 Main findings ........................................................................................... 41
Paper I and II ....................................................................................... 41 Paper III ............................................................................................... 41 Paper IV ............................................................................................... 41
Paper I and II ............................................................................................ 42 Paper III .................................................................................................... 43 Paper IV ................................................................................................... 44
Summary/Conclusion .................................................................................... 47 Paper I and II ............................................................................................ 47 Paper III .................................................................................................... 47 Paper IV ................................................................................................... 47
Future perspectives ....................................................................................... 48
Summary in Swedish – Sammanfattning på svenska .................................... 50
Acknowledgements ....................................................................................... 53
References ..................................................................................................... 55
Abbreviations
COPD Chronic Obstructive Pulmonary Disease
CPC Cerebral Performance Category CPR Cardiopulmonary Resuscitation DES Drug Eluting Stents ECG Electrocardiogram EEG Electroencephalography EMS Emergency Medical Services GCS Glasgow Coma Scale ICU Intensive Care Unit LBBB Left Bundle Branch Block MAP Mean Arterial Pressure MI Myocardial Infarction NSTEMI Non-ST-Elevation Myocardial
Infarction OHCA Out-of-Hospital Cardiac Arrest PCAS Post Cardiac Arrest Syndrome PCI Percutaneous Coronary Intervention PEA Pulseless Electrical Activity PTCA Percutaneous Transluminal Coronary
Angioplasty ROSC Return Of Spontaneous Circulation SES Socioeconomic Status SRCR Swedish Register for Cardiopulmo-
nary Resuscitation STEMI ST-Elevation Myocardial Infarction TTM Targeted Temperature Management VF Ventricular Fibrillation VT Ventricular Tachycardia


11
Introduction
History Sudden cardiac arrest is one of the most dramatic situations in the field of medicine and a condition associated with a high mortality and morbidity. Out-of-hospital cardiac arrest (OHCA) is defined as the sudden absence of cardiac mechanical contractility with loss of signs of circulation that occurs within a community setting1. In parallel with other fields of medicine, early cardiopul-monary resuscitation (CPR) methods relied more on guesses and beliefs than empiric research and physiologic knowledge. However, early descriptions, e.g. in the old testament, describes events similar to mouth-to-mouth resusci-tation2 but it was not until the 18th century that the first known society for resuscitation was formed: The Society for the Recovery of Drowned Persons.3 This was established due to problems with drowning accidents in the Dutch canals. The evolution of modern intensive care in the middle of the 20th cen-tury enabled more advanced post resuscitation care and thus an opportunity to treat patients successfully resuscitated after cardiac arrest.
The possibility to treat unconscious survivors after successful CPR led to an increased interest in cardiac arrest research with an initial focus on CPR.4 Various compression/ventilation techniques, mechanical devices for chest compressions, pharmacological treatment during CPR and improvements in the education and equipment for first responders were developed. The intro-duction of modern mouth-to-mouth ventilation by James Elam and Peter Safar in 1956 is by many seen as the birth of modern CPR practice.5 The gradual improvement in the “chain of survival”, i.e. early recognition and early CPR with good quality, led to an increasing number of patients with return of spon-taneous circulation (ROSC) admitted to hospital. Early recognition and imme-diate high-quality CPR with timely defibrillation remains cornerstones of suc-cessful cardiac arrest care.6 However, mortality remained high in the increas-ing number of patients admitted after OHCA, highlighting the need for opti-mizing the post-resuscitation care.

12
Cardiac arrest
Incidence and outcome It might seem peculiar to describe the incidence of cardiac arrest since almost everyone eventually dies due to loss of cardiac activity. However, when we talk about cardiac arrests in the field of medicine, we generally describe the condition of a sudden (unexpected) cardiac arrest described in the first section. This thesis focuses on OHCA, i.e. not cardiac arrest that patients suffer when already admitted and cared for in hospital. Incidence rates varies between dif-ferent countries due to demography and the variation of important comorbid-ities, but also due to the quality of registration. Nevertheless, OHCA is com-mon and an important cause of death, at least in developed countries. During 2018, in Sweden, cardiopulmonary resuscitation was started in 6129 cases, and this is roughly in half of all cases of OHCA. In the USA, there are an estimated 350 000 OHCA annually, with an overall survival rate of 5.5%.7,8 Many countries, including Sweden, have reliable reports on the number of patients with ROSC where CPR is started, due to validated national registries. The uncertainty in the total number of OHCA is largely due to those where no CPR is performed since these cases are not reported in the CPR registers. Due to the uncertainty in the cause of death in many patients with unwitnessed death and the rather low number of autopsies carried out, both the true number of OHCA and the actual mortality rates therefor remains uncertain.
Despite improvements in all links of the “chain of survival”, mortality rates after OHCA remains high. Outcome data varies widely due to several factors. Different studies report outcome from different populations, e.g. all presumed cardiac arrests, all cases treated by the EMS, only patients with ventricular fibrillation (VF), only cases with a presumed cardiac cause etc. Therefore, during the last two decades, studies can be found with survival rates from 3.3% to 40.5%!8-10 In the Swedish register for cardiopulmonary resuscitation (SRCR), 30-day survival in patients with OHCA treated by the EMS was 10.3% in 2018. During the last decade, survival rates have remained between 10%-11.3%.11 One important factor that is hard to study, but is likely to influ-ence survival rates significantly and might explain some of the national and regional differences in outcome, is the selection of patients for CPR. Reports that only includes patients where CPR is started by the EMS, is highly affected by local guidelines on when CPR should be initiated. If many older patients with a high burden of comorbidities, e.g. institutionalized elderly, have a do-not-resuscitate decision, CPR will not be given, and they will thus not be in-cluded in the CPR registers reports. This will improve survival rates in that region/country regardless if the cardiac arrest care has developed or not.

13
Factors affecting outcome There are several factors in the treatment of patients with cardiac arrest known to affect outcome. Several patient factors are also important for the prognoses after the arrest. When the heart stops, circulation to the body immediately ceases, and within seconds the patient loses consciousness. The brain is par-ticularly sensitive to the cessation of oxygen delivery, and within minutes, irreversible neuronal death begins. The period between the cardiac arrest and the start of CPR is thus called the no-flow period and it is crucial to the out-come that this period is as short as possible, and early recognition and initia-tion of CPR are thus of utmost importance for a good outcome. To address this critical part of treatment, many countries have rolled out massive educa-tion programmes in CPR for laymen. Bystander CPR has been shown to im-prove outcome and there has been a gradual increase in bystander CPR in Sweden where today around 75% of OHCA patients receives bystander CPR before ambulance arrival.11-13 During good quality CPR, only around 20-30% of normal cardiac output can be sustained, and the period of CPR before the heart hopefully starts pumping on its own again, is called the “low-flow” pe-riod.14,15 This low-flow state can buy time and prolongs the period before or-gan damage becomes too severe to survive but is not sufficient for longer pe-riods. The quality of CPR is crucial and so is the length of the low-flow phase.16,17 For patients with shockable rhythms, most often VF, where an elec-trical chaos in the myocardium creates a no flow-situation (pulseless ventric-ular tachycardia is also included), early defibrillation is the treatment that can “restart” the heart.18 Early defibrillation has been shown to increase survival rates and is perhaps best illustrated by patients with VF in coronary care units where excellent survival rates are seen after defibrillation almost immediately after the arrest.19 For patients with other ECG rhythms, high quality CPR, adrenaline (shown to increase ROSC rates but maybe not survival with good neurologic outcome) and sometimes treatment of the underlying cause of the arrest are cornerstones in the treatment.20-22
Post-resuscitation care For patients with ROSC, that are usually unconscious, the period of post-re-suscitation care begins. The initial care in the ICU focuses on limiting further organ damage by stabilizing respiration and circulation and initiating neuro-protective treatment. Initial care also focuses on searching and treating poten-tial causes for the arrest (e.g. myocardial infarction, pulmonary embolism, electrolyte disturbances etc.) and evaluate the potential damage the patient has suffered during the cardiac arrest.21 To limit the neurologic damage, target temperature management, i.e. keeping the body temperature at either 33 or 36◦
C is recommended for the first 24 h.21,23-25 The treatment of patients after ROSC is often complicated by a clinical picture called “post cardiac arrest

14
syndrome” (PCAS) in addition to the potential organ dysfunctions following the cause of the arrest, e.g. cardiac dysfunction after myocardial infarction. The features of PCAS includes a systemic inflammatory response (including capillary leakage and vasodilation), brain injury and myocardial stunning and is probably caused both by the generalized ischaemia-reperfusion injury caused by the cardiac arrest and might be affected by some of the treatments, e.g. adrenaline.26 Treatment is mainly supportive, and the cardiovascular in-stability usually resolves within days. However, many fields of cardiac arrest care, in particular post-resuscitation care, relies on retrospective studies and extrapolation from research in other parts of intensive care. The optimal tar-gets of cornerstones in intensive care medicine, e.g. mean arterial pressure (MAP), PaCO2 and PaO2-levels are yet to be determined for the cardiac arrest patients. Retrospective studies have suggested that some patients might bene-fit from a higher than standard MAP as well as higher than normal PaCO2-levels.27-30 It is also likely that there exists an optimal PaO2-level in the post-resuscitation phase (and perhaps also during CPR).31 The evidence to support a new strategy for the individual patient, i.e. aiming for higher MAP and/or PaCO2 is currently too weak though. High quality, randomized trials on car-diac arrest patients are in many cases yet to be performed or published.32
Initial ECG rhythm As mentioned, several factors regarding the patient and the cardiac arrest af-fects the chance of a good outcome. As in almost all fields of medicine, ad-vanced age and comorbidities, negatively affect the chance to survive a car-diac arrest. That witnessed cardiac arrest has a better prognosis than unwit-nessed is clear, due to both the possibility for early bystander CPR and earlier arrival of EMS personnel starting advanced life support.19 One of the most important prognostic factors though, are the initial ECG rhythm registered. Historically, this has been divided into shockable (VF or VT) or non-shocka-ble (asystole or pulseless electrical activity, PEA). Shockable rhythms carry a far better prognosis due to a number of reasons; they are in general causes by an abrupt cardiac event, e.g. a thrombotic occlusion in a coronary artery or a primary arrhythmia, which means that the blood and brain are normally oxy-genated and the blood volume intact at the time of the arrest.33-35 Thus, the brain (and other organs) has some time before cell death ensues, and CPR is as effective as possible when initiated. For non-shockable rhythms, the causes for the arrest are more heterogeneous, including e.g. hypovolemia and as-phyxia. In severe hypovolemia, e.g. after bleeding, CPR is ineffective since there is no volume to pump. In asphyctic cardiac arrest, the brain has already suffered a period of hypoxia before the heart stops leading to more neurologic damage even if effective CPR is started early. Furthermore, some of the pa-tients that presents with asystole, initially has had a shockable rhythm (all

15
rhythms eventually progress into asystole if the patient is not successfully re-suscitated). That means that some patients with asystole are merely patients with initial VF/VT with long no-flow and low-flow times before the first rhythm registration, leading to worse prognoses. In many countries, including Sweden, a gradual decrease of initial shockable rhythms has been noticed dur-ing the last decades despite increased rates of bystander CPR.36 The explana-tion of this is likely multifactorial and a combination of older population, im-proved interventional and medical treatment of both ischaemic heart disease and chronic heart failure, increased use of implantable cardiac devises etc. might have an impact.37-39 Of interest, more recent research has shown, that PEA carries a better prognosis than asystole and it is reasonable that future research divides patients into three distinct groups, separating patients with asystole from PEA patients when evaluating new treatment options.40
Causes of cardiac arrest In OHCA, cardiac causes are the most common aetiology.34 Several studies have identified ischaemic cardiac disease, in itself a broad group of diseases, as the major underlying factor for cardiac caused OHCA. The fact that is-chaemic heart disease is a common cause for cardiac arrests does not neces-sarily imply that an acute ischaemic insult is the direct cause of the cardiac arrest. This is an area that is hard to study. Changes in primary and secondary prevention of heart disease limits the generalizability of older studies. Low rates of clinical autopsies, differences in diagnostic routines between countries and hospitals and regional differences in cardiac arrest causes limits the value of single centre studies. In patients without an obvious non-cardiac cause after OHCA, significant coronary artery stenoses are common but the findings of acute coronary lesions are considerably lower. In patients with initial shocka-ble rhythm and ST-elevation, acute ischaemic coronary artery events are very common, but these patients are a rather small part of the OHCA group.41 Pri-mary arrythmias, congenital heart disease, respiratory failure, pulmonary em-bolism, cerebrovascular events (especially bleeding) and intoxications are other diagnoses frequently found when analysing groups with OHCA and no obvious non-cardiac cause.42 After ROSC, successful post-resuscitation care necessitates stabilizing and supporting vital functions and in parallel diagnos-ing and treating potential causes for the arrest. Finding the right diagnostic tools for the right patients with optimal timing, is likely to improve outcome both by optimizing treatment and avoiding potentially dangerous treatments.
Coronary angiography After the proposal that coronary artery occlusion was associated with myocar-dial infarction (MI) already in 1880, it took several decades to establish its

16
causative role. During the first half of the 20th century, many scientists be-lieved that the occlusions observed at autopsies was caused by the MI and not the opposite. Due to the lack of pathophysiologic understanding, treatment options were limited. Bed rest sometimes combined with oxygen and intrave-nous fluids was standard treatment. During the 1970s and 1980s, autopsy and coronary angiography studies could demonstrate the likely causative role of coronary artery thrombus for MI and also the tendency for spontaneous throm-bolysis by the finding of lower rates of total artery occlusion if coronary angi-ography was performed between 12-24 h rather than the first 12 h after debut of symptoms.43 This also showed that coronary angiography was feasible and safe even in the acute setting of an ongoing MI. These and similar findings from other studies led the way to introduce therapies to enable revasculariza-tion of the coronary arteries. Streptokinase, extracted already 1933, was the first thrombolytic agent used and its introduction revolutionized the care of MI patients. Initial studies where streptokinase was administered intracoro-nary were followed by others showing that intravenous administration was feasible which enabled treatment to be started earlier and in centres without angiography facilities. Even if thrombolytic therapy improved care substan-tially, it was not perfect. In many patients, revascularization could not be achieved, others had contraindications to the treatment (e.g. recent surgery) and the complications, especially bleeding including intracerebral haemor-rhage were problematic.
In 1977, the first successful percutaneous transluminal coronary angio-plasty (PTCA) was performed in a patient with stable angina pectoris. This was followed by successful treatment of patients with MI.44 Initial trials with PTCA performed after thrombolytic therapy failed to show additional benefit. However, performing primary PTCA, showed superior results compared to thrombolytic therapy.45 Even if PTCA increased the rates of revascularization and had fewer severe complications than thrombolysis, problems with stenotic re-coil and restenosis remained. The introduction of stents, initially bare metal stents, in the 1990s were shown to reduce the problems after PTCA and soon became the standard treatment, now called percutaneous coronary interven-tion (PCI).46 Due to problems with intimal hyperplasia and thus a risk of reste-nosis at the site of the stent, drug eluting stents (DES) were developed. These stents, covered with drugs with anti-proliferative properties, where introduced in 2003. DES has been further developed and are now standard treatment when PCI is performed with low rates of restenosis and stent occlusion. How-ever, medical treatment with anti-thrombotic agents, are needed to prevent both early and late complications.47
The relative safety and impressing results when treating patients with ST-elevation myocardial infarction (STEMI) with immediate PCI has of course in-creased the interest to treat other patient groups. Even if coronary angiography with the possibility to perform PCI is an important part even in the care for patients with non-ST-elevation myocardial infarction (NSTEMI), the benefit of
17
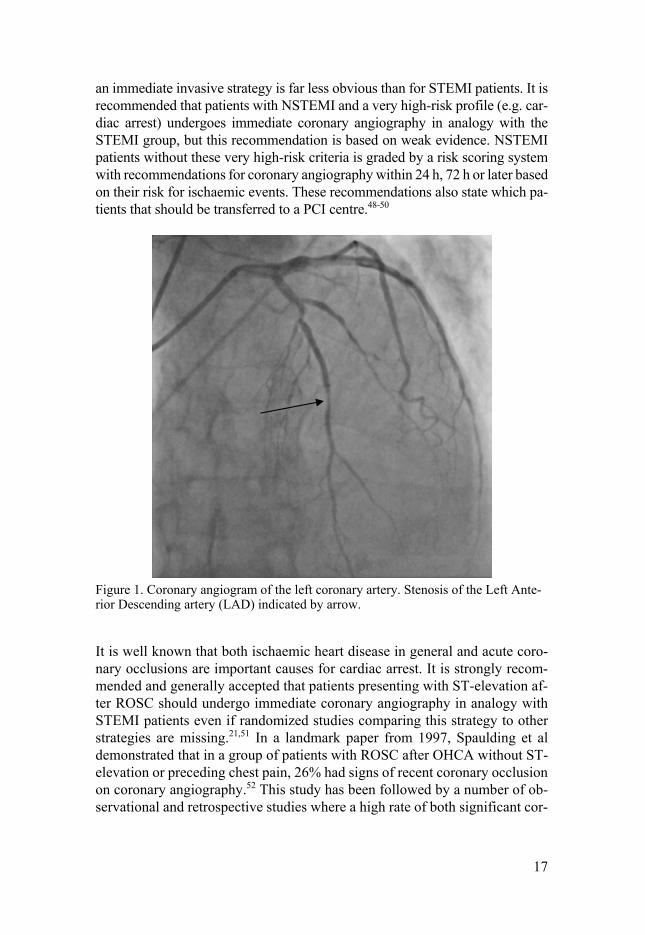
an immediate invasive strategy is far less obvious than for STEMI patients. It is recommended that patients with NSTEMI and a very high-risk profile (e.g. car-diac arrest) undergoes immediate coronary angiography in analogy with the STEMI group, but this recommendation is based on weak evidence. NSTEMI patients without these very high-risk criteria is graded by a risk scoring system with recommendations for coronary angiography within 24 h, 72 h or later based on their risk for ischaemic events. These recommendations also state which pa-tients that should be transferred to a PCI centre.48-50
Figure 1. Coronary angiogram of the left coronary artery. Stenosis of the Left Ante-rior Descending artery (LAD) indicated by arrow.
It is well known that both ischaemic heart disease in general and acute coro-nary occlusions are important causes for cardiac arrest. It is strongly recom-mended and generally accepted that patients presenting with ST-elevation af-ter ROSC should undergo immediate coronary angiography in analogy with STEMI patients even if randomized studies comparing this strategy to other strategies are missing.21,51 In a landmark paper from 1997, Spaulding et al demonstrated that in a group of patients with ROSC after OHCA without ST-elevation or preceding chest pain, 26% had signs of recent coronary occlusion on coronary angiography.52 This study has been followed by a number of ob-servational and retrospective studies where a high rate of both significant cor-

18
onary artery stenosis and acute coronary artery lesions are described in pa-tients without ST-elevation after ROSC.41,53-55 These findings have led to a shift in the care of patients after cardiac arrest, with many centres advocating an early invasive strategy with immediate coronary angiography in some, or all, patients with suspected cardiac cause for the cardiac arrest, despite the absence of ST-elevation. The findings described above, raises several ques-tions: Firstly, is ECG sensitive enough to detect myocardial ischaemia after cardiac arrest and CPR? Troponin levels are usually elevated after cardiac ar-rest and thus of limited use for determining which patients that presents with ongoing ischaemia. The troponin elevation can have several causes: An acute coronary artery occlusion and myocardial ischaemia is a common cause of the cardiac arrest. The cardiac arrest itself creates a no-flow or low-flow state even in the coronary vessels causing ischaemia to the myocardium with subsequent troponin release. Finally, chest compressions have the potential to damage the myocardium and cause troponin release.56 Secondly, is it possible to develop a risk scoring system for patients without ST-elevation after ROSC, similar to NSTEMI patients, thereby enabling a selection of patients with the highest risk for acute coronary artery insults that might benefit the most from an im-mediate coronary angiography? and thirdly, could outcome after OHCA be improved by immediate coronary angiography in all OHCA patients without an obvious non-cardiac cause for the arrest? Several studies have reported rates of acute occlusions similar to that in Spaulding’s material, and signifi-cant stenoses in more than 60% of patients without ST-elevation thereby chal-lenging ECG as a tool for selecting patients for an early invasive strategy. Many of these studies have been relatively small and retrospective, limiting subgroup analyses, e.g. comparing coronary angiographic findings with spe-cific ECG changes in the non-ST elevation group.57 Other important patient characteristics, e.g. comorbidity are often missing or of poor quality. Some well performed retrospective studies on outcome in relation to early angi-ography showed promising results with higher survival rates in patient that had undergone immediate or early angiography compared to later or no angi-ography. These findings have not though, been consistent in other studies where no survival benefit could be found.41,58-62 Retrospective trials in general have some limitations, e.g. the risk of selection bias. In these studies, what is considered “early angiography” also varies and no control regarding other parts of the care were possible due to the retrospective design.
In 2019, the first study randomizing patients with ROSC after OHCA and no ST-elevation to a strategy of immediate coronary angiography or a strategy with a more conservative approach without immediate angiography was pre-sented.63 This well performed study only included patients with shockable rhythms to select patients with high risk of cardiac cause. However, the rate of acute occlusions was lower than expected and no difference in either total survival or survival with good neurologic outcome were found. Unfortunately,

19
the study was underpowered and designed with an estimated 40% relative in-crease in survival for the immediate angiography group, which must be con-sidered a bit optimistic. Also, no long-term effect of the intervention on car-diac function has been presented.
Socioeconomic status in cardiac arrest It is well known that socioeconomic status (SES), in study settings often lim-ited to economic status and educational level, affects both the risk of develop-ing certain diseases but also the outcome following certain diagnoses.64 This is affected by several factors, e.g. nutritional intake, tobacco and alcohol con-sumption, occupational environment and exercise, but also the tendency to seek healthcare and adherence to prescribed drugs or recommended lifestyle changes. It has also been shown that SES might impact access to certain ther-apies such as PCI in patients without cardiac arrest and other treatment choices.65-69 In cardiac arrest patients, SES seems to have an impact both on the risk for cardiac arrest, rate of bystander CPR and outcome.70-73 No studies have investigated if the care offered to patients with ROSC is associated with SES.
SES is a difficult area to study since the term SES is in itself unclear. In-come and education are common factors when addressing this field but other factors, e.g. marital status, type of employment etc. are also part of a person’s SES. In many countries, large, registry-based studies measuring individual SES are almost impossible. Therefore, the majority of SES studies in the car-diac arrest field are based either on the general SES level in the area the car-diac arrest victim lives or the SES level in the area where the cardiac arrest occurred. This is a major limitation and does not allow for adjustments be-tween different components of SES, e.g. income and education level.70 Comorbidity data are also often missing. The limitations of many studies make it hard to establish why low SES is correlated with worse outcome after car-diac arrest. The main explanatory factors have traditionally been low rates of bystander CPR, possibly lower quality of bystander CPR, and more severe comorbidities. It is obvious that these factors are important, but if these are the only explanatory variables or if other factors, e.g. in-hospital treatment, might impact differences in outcome are unknown.
Neurologic outcomes, prognostication and follow-up For patients successfully resuscitated after cardiac arrest, mortality is still high. Even if the major cause of early deaths (occurring the first days after the arrest), are cardiovascular events, the most common cause of death is caused by the ischemic injury to the brain.74 The neurons are especially susceptible to ischemia and the process of irreversible cell death starts within minutes after cessation of circulation. The obvious lack of oxygen and energy in the brain

20
caused by the cardiac arrest initiates the process of neuronal damage and, if left untreated, this rapidly leads to non-survivable brain damage. However, further damage is caused by the reperfusion of previously ischemic organs, when blood flow is restored. Furthermore, the process of cell death through apoptosis might continue for hours or days after the cardiac arrest caused by processes initiated either during the hypoperfusion phase during the arrest or by the reperfusion process.75 This leads to two conclusions: firstly, it is hard to prognosticate the severity of neurologic sequele during the first days after the cardiac arrest and secondly, the process of reperfusion and ongoing cell death provides a window where therapeutic interventions might improve neu-rologic outcome.
Neurologic prognostication, in itself a vast research area, provides several important aspects both in the patient care and in the study setting. The ability to determine if a patient has suffered too severe neurologic damage to survive with an acceptable quality of life, makes it possible to withdraw life sustaining therapy rather early (usually during the first week) after the cardiac arrest. This protects the patient and relatives from meaningless, prolonged, intensive care which is also important from a justice perspective, where limited resources and ICU beds can be provided to other patients. Even more important, this limits the number of patients that survives the intensive care period with very severe brain damage and ends up in a vegetative state. Many countries with a tradition of neurologic prognostication and withdrawal of life sustaining ther-apy have very low rates of survivors after cardiac arrest with severe brain damage. In general, patients with good neurologic outcome exceeds 90% in the survivor group.76,77 On the other hand, if withdrawal of life sustaining ther-apy is done too early or based on doubtful methods, there is a risk that patients that could have survived with good outcome, dies. In fact, the direct cause of death, for the majority of patients dying after successful resuscitation, is with-drawal of life support due to poor neurologic prognoses, highlighting the ex-treme importance of robust prognostication tools.78 Even if most comatose survivors that eventually survives, wakes up during the first 3 days after the arrest, a large group of patients (in one study around half of the survivors), unconscious on day three, survives with good neurologic function and thus, too early prognostication might lead to catastrophic decisions.79 Apart from the obvious need of good prognostication for the best patient care, this is also important for clinical studies. Several recent or ongoing cardiac arrest studies, including the DISCO study, are not blinded. It is therefore of great importance, that participating sites uses a common and optimally a conservative prognos-tication strategy for prognostication and withdrawal of life sustaining therapy to prevent criticism that the results could be affected by early withdrawal of life support in combination with the non-blinded study setting.
The field of neurologic prognostication has gradually evolved, and the sen-sitivity and specificity in several clinical, laboratory, neurophysiological and radiological methods have been evaluated. The problems with many early

21
studies in the field is the tendency for a self-fulfilling prophecy, where life sustaining therapy has been withdrawn in case of specific findings, e.g. a cer-tain EEG pattern, and thus no patients with this specific EEG pattern has sur-vived. To shortly summon this complex field, no method alone is sufficient to state with certainty that an individual patient will have a poor neurologic out-come. International guidelines states that withdrawal of care should not be done too early (i.e. at least not before 72 hours apart from in some very special circumstances) and that clinical evaluation should be combined with one or several other methods. In case of uncertainty, care should be continued, and the examinations repeated. Even if this field still is under evaluation, current guidelines provides a robust and evidence-based support in these ethically challenging decisions.21
Due to the vulnerability of the brain to ischemic insults it has become clear that merely looking at survival, e.g. 30-day survival, when evaluating or com-paring treatment strategies in cardiac arrest patients is insufficient. Increasing survival at the cost of worsening neurologic outcome is not desired. The cer-ebral performance category (CPC) has been widely used in cardiac arrest stud-ies to evaluate neurologic status in survivors where CPC 1-2 are considered good outcomes and 3-4(5) bad outcomes.80 The CPC is rather easy to use and has the advantage of being widely used but certainly has limitations. Several studies have shown that patients recovering from cardiac arrest can present with a number of problems not easily detected by CPC, that nevertheless affect their daily lives, e.g. problems with memory and executive functions, depres-sion, anxiety, and fatigue.76,81-83 When evaluating the effects of a new inter-vention, improvements in some of these parameters might be of utmost im-portance for the individual patient and will not be detected by a 30-day sur-vival rate or the CPC-scale. A broader follow-up using instruments to address these potential problems is therefore important both when designing cardiac arrest trials and to implement in clinical follow-up programs. There is no in-strument specifically designed for cardiac arrest patients and work is currently done to validate various follow-up instruments, that is usually designed for stroke patients or neuro-trauma care, against cardiac arrest patients. It is im-portant to remember, that the global hypoperfusion that cardiac arrest patients suffer, is very different from the pathophysiology in a stroke patient. Different parts of the brain have varying sensibility to ischemic insults, making different parts recovering at different pace, and providing a pathophysiologic back-ground to some of the characteristic long-term problems that survivors might encounter.84,85 Improvement in neurocognitive function during the first months is common and evaluating neurocognitive effects of a specific treat-ment should thus not be done too early.86
22
Aims
Paper I and II To investigate the feasibility and safety of a strategy of immediate coronary angiography compared to a strategy with no immediate coronary angiography in patients resuscitated after OHCA without ST-elevation on ECG.
Paper III To describe coronary angiographic findings after cardiac arrest in relation to ECG changes and comorbidities.
Paper IV To investigate if patients´ income influences the probability to receive early coronary angiography in patients successfully resuscitated after OHCA.

23
Material and methods
Paper I and II
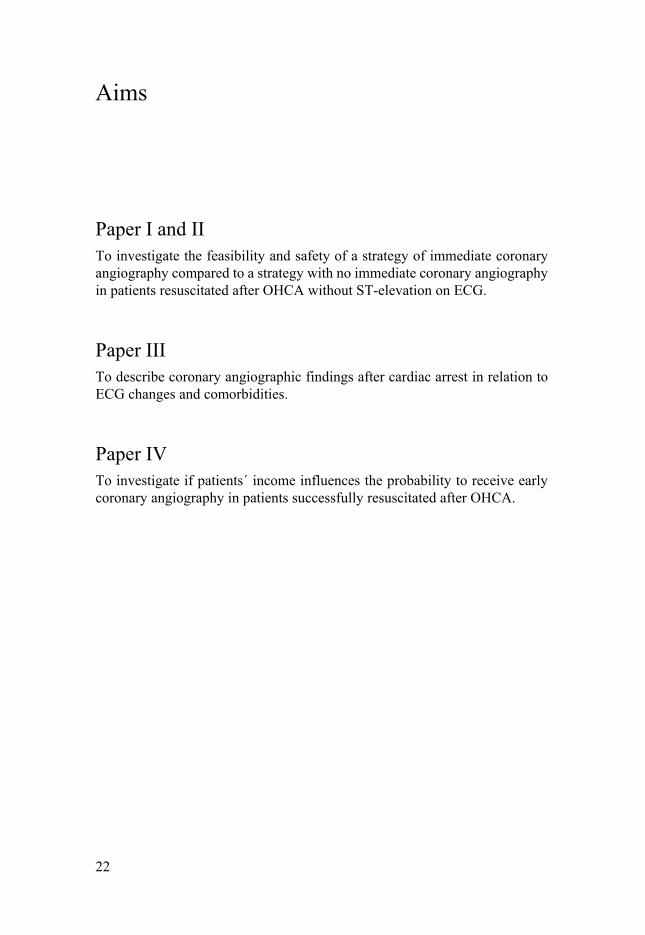
Study enrolment and randomization The DISCO study is a randomized multicentre study, initiated by Uppsala University. It is funded by institutional grants from Uppsala University and the Swedish research council (Vetenskapsrådet). The pilot phase started in January 2015 at two sites and was gradually expanded to in total 10 Swedish hospitals, mainly university hospitals. The last patient in the pilot phase was included in October 2017. There was a possibility to include patients prehospi-tally or in the emergency department. Eligible patients were randomized in a 1:1 ratio via a web-based randomization module with separate randomization blocks per each study site. (Figure 2)
Inclusion / exclusion criteria Eligible patients for the study were patients with witnessed OHCA with sus-tained ROSC after resuscitation and the possibility to perform coronary angi-ography within 120 minutes from prehospital personnel’s arrival to the pa-tient. Exclusion criteria were: 1. Obvious non-cardiac causes. 2. Terminally ill patients with a life expectancy less than one year. 3. Known pregnancy. 4. ST-elevation on ECG and 5. Patient not unconscious (GCS>8)
24
Figure 2. DISCO study flowchart
25
Coronary angiography Patients randomized to immediate coronary angiography should undergo cor-onary angiography as soon as possible. After initial assessment of the vessels, PCI against suspected culprit lesion should be performed. In the pilot phase, other significant stenoses should also be treated with PCI if the operator con-sidered them accessible for PCI. Stenoses were considered significant if they were >50%. Other treatment, e.g. vasoactive medication and anti-platelet drugs, were given according to local routine and not stated in the protocol.
Patient not randomized to immediate coronary angiography were taken to the ICU and treated according to local routine. Coronary angiography in this group should not be performed during the first three days. Coronary angi-ography could be performed after three days at the discretion of the treating physician but was not mandatory. However, if patients in this group developed severe cardiovascular instability, e.g. cardiogenic chock, signs of ongoing is-chemia on ECG or severe ventricular arrhythmias, coronary angiography could be performed during the first three days.
Post resuscitation care and withdrawal of life-sustaining therapy Apart from the randomized intervention (coronary angiography), treatment should follow international guidelines and local routines and were not speci-fied in the protocol. However, the protocol stated how neurologic prognosti-cation and potential withdrawal of life-sustaining therapy should be under-taken. This was in line with international guidelines but highlighted in the protocol due to its importance.
Statistical analyses The statistical analyses plan, power calculation and data analyses from the pilot phase were coordinated by Uppsala Clinical Research Center, Uppsala, Sweden. Data were either entered directly into the electronic Clinical Report Form (e-CRF) or written on paper CRF and then transferred to the e-CRF.
Power calculation and statistical methods The power calculation was based on survival rates from a post hoc analyses from the TTM-trial and the Swedish register for cardiopulmonary resuscita-tion. Primary endpoint for the main study is 30-day survival. Assuming a sur-vival rate of 45% in the group not receiving immediate coronary angiography, inclusion of 1006 patients was calculated to be necessary to detect a 20% im-proved survival rate (from 45% to 54%) in those receiving immediate angi-ography (with 80% power). To avoid needing to adjust for multiple analyses, no hypothesis testing for outcome data planned to be presented after closing the main study were done after the pilot phase was completed.
26
The sample size for the pilot phase were predefined to 80 randomized pa-tients. 40 patients with ST-elevation were also planned to be included, but not randomized, and was followed in the study for comparison reason. No com-parative statistics were performed in paper II due to reasons mentioned above and the limited number of patients included.
Patient consent Patients were included and randomized prior to informed consent due to the nature of the study and in accordance with the ethical permission. Oral and written informed consent were thereafter obtained from the patients´ next-of-kin as soon as possible. For surviving patients who regained sufficient mental capacity, informed consent was obtained directly from the patients.
Safety and feasibility evaluation Several safety parameters were included in the pilot phase analyses, including bleeding, procedure related cardiac arrests, presence of renal failure and need for renal replacement therapy. The feasibility analyses focused on pre- and in-hospital timeframes, adherence to protocol (cross over), logistical problems regarding randomization and informed consent and if presenting ECG were correctly interpreted.
Paper III
Population and data sources This retrospective registry study included patients with OHCA registered in The Swedish Register for Cardiopulmonary Resuscitation between 2008-2013. Eligible patients were comatose survivors after OHCA admitted to Swe-dish hospitals over the age of 18 years. Data from three different registers were used:
• The Swedish Register for Cardiopulmonary Resuscitation – All Swedish
EMS services reports cardiac arrest cases to the registry. It mainly con-tains prehospital parameters but also 30-day survival. This was used to identify the patients used in the study.
• The Swedeheart Registry – This registry is an “umbrella” registry contain-ing several national registers in the cardiovascular field, e.g. the Swedish Coronary Angiography and Angioplasty Register (SCAAR). All patients undergoing coronary angiography in Sweden should be registered and many parameters are mandatory.

27
• The National Patient Register – National registry containing ICD coding of diagnoses set in the specialist care including date of the diagnosis. En-abled us to identify comorbidities present prior to the cardiac arrest.
If ECG data were missing in the registry data, this was completed with ECG from the patients´ health records. The ECG´s were interpreted by a specialist in cardiology prior to the analyses and thus blinded for the coronary angi-ography results. Coronary angiography was classified as “early” if it was done the same date as the cardiac arrest. (Figure 3)
Figure 3. Participant flow (Coronary angiographic findings after cardiac arrest in relation to ECG and comorbidity)
Statistics No imputation was needed since all angiographic data presented has been mandatory to register in the Swedeheart registry minimizing the problem with missing data. ECG groups and the rate of PCI attempts were analyzed with logistic regression and presented as odds ratios with 95% confidence intervals. Significance testing for categorical data were made with chi-square test and for continuous data with the Mann-Whitney test. Statistical analyses were per-formed using IBM SPSS Statistics, Version 25, Armonk, NY: IBM Corp.
28
Paper IV
Population and data sources Paper IV is, like paper III, a retrospective registry study including patients with OHCA registered in The Swedish Register for Cardiopulmonary Resus-citation. Patients registered as OHCA admitted to Swedish hospitals after ROSC between 2008-2013 were identified. Patients under 18 years and those with crew witnessed arrests were excluded leaving 3906 patients for the anal-ysis. Data from four different registries were used. • The Swedish Register for Cardiopulmonary Resuscitation – This was used
to identify the patients used in the study and provided prehospital data for the adjusted analyses and survival data.
• The Swedeheart Registry and The National Patient Register – Described under paper III
• Statistics Sweden – National registry containing data on income and edu-cational level for every inhabitant in Sweden with a Swedish personal number.
Coronary angiography was classified as early if it was performed the same date as the cardiac arrest.
Statistics Missing data were handled by multiple imputations and missing were assumed to be missing at random. Early angiography was analyzed using logistic re-gression analysis. As a sensitivity analysis the relationship between income and early angiography were analyzed using multiple logistic regression with restricted cubic splines for the continuous income variable. P-values below 0.05 were regarded as statistically significant. All analyses were performed using R version 3.6.2 (R Foundation for Statistical Computing, Vienna, Aus-tria).
Ethical approvals and considerations
Ethical approvals Ethical approval for the studies included in this thesis were given by the re-gional ethical boards in Sweden:

29
Paper I and II – Regional ethical board of Stockholm, Sweden (Reg no: 2014/1170-31/1) Paper III - Regional ethical board of Stockholm, Sweden (Reg no: 2014/1139-31/2, 2016/361-32) Paper IV - Regional ethical board of Stockholm, Sweden (Reg no: 2018/951-32)
Ethical considerations This thesis contains two distinct types of studies with very different, but im-portant, ethical considerations. Medical research in general, and intensive care research in particular, demands the highest ethical standards possible from the researchers. This is important from several aspects: Firstly, patients should feel totally assured that the care given is in their best interest. Secondly, future medical research relies on the fact that patients in general trusts in researchers and are willing to participate in studies. If the reputation of medical research deteriorates, future research might be impossible to carry out. Thirdly, it is of great importance that study results are handled and presented with high qual-ity. Otherwise, study participants have volunteered in vain. Finally, it is es-sential to follow internationally accepted ethical standards to gain general ac-ceptance for the study results.
Paper I and II The ground principle for medical research is that the patient has the chance to choose whether or not to participate in the study in the process of informed consent. In special circumstances, e.g. if patients are unconscious or critically ill, obtaining informed consent would be impossible or unethical. Most car-diac arrest studies suffer this common problem, whether a new resuscitation algorithm is tested, and the patient has a circulatory arrest or a new strategy in post-resuscitation care is evaluated when most patients has not regained con-sciousness. To avoid unnecessary clinical trials, randomizing patients without prior consent, other studies, e.g. animal or retrospective studies can be made. However, in many cases these can only be hypothesis generating and need to be confirmed in large scale, randomized trials. The declaration of Helsinki admits such an exception from its ground principle of informed consent in article 28 and 30.87 Many countries have a system of legal representatives that can consent to study participation if the patient is too ill to give informed con-sent. In Sweden, we have no system of legal representatives which provides further limitations to intensive care research. Furthermore, in cardiac arrest studies, time might be too limited to receive consent even in a system with legal representatives. This leaves us with two options, either include patients without consent in studies or not perform randomized trials in critically ill

30
patients. In the DISCO study, we have chosen, and received ethical approval for, to randomize patients without consent and as soon as possible inform pa-tients´ next-of-kin who then get the role of legal representative after random-ization. Patients that regain enough mental capacity then gets information about the study and the possibility not to participate in further follow-up. This system poses a great responsibility on the study group to conduct a high-qual-ity study without exposing the study participants for unnecessary risks or dis-comfort.
The alternative, not to conduct studies in these patients would, in my opin-ion, be more unethical for two major reasons. Firstly, this would limit medical progress in caring for the most severely ill patients that cannot express their own will to participate in studies. Secondly, from a Swedish perspective, we would certainly “import” research results from other countries where these studies could be made. It would be hard to justify that we can use research results from studies that we ourselves do not want to perform for ethical rea-sons. Furthermore, questions about study generalizability might arise.
Paper III and IV Patients registered in Swedish medical registries, e.g. the Swedish Register for Cardiopulmonary Resuscitation (SRCR), are informed about their right to have their information removed. Therefore, in general, the ethical boards in Sweden allows research on registry data without informed consent from the patients. This was the case in the papers in this thesis. After merging data from the SRCR and Swedeheart, the data file was sent to Statistics Sweden and the National Patient Register to be completed with socioeconomic and comorbid-ity data respectively. Since these parameters contains sensitive information, the files were sent back to us anonymized, without personal numbers, thus making it impossible for us in the research group to identify the individual patients. Thus, the privacy of the participating patients was protected as far as possible.
31
Results
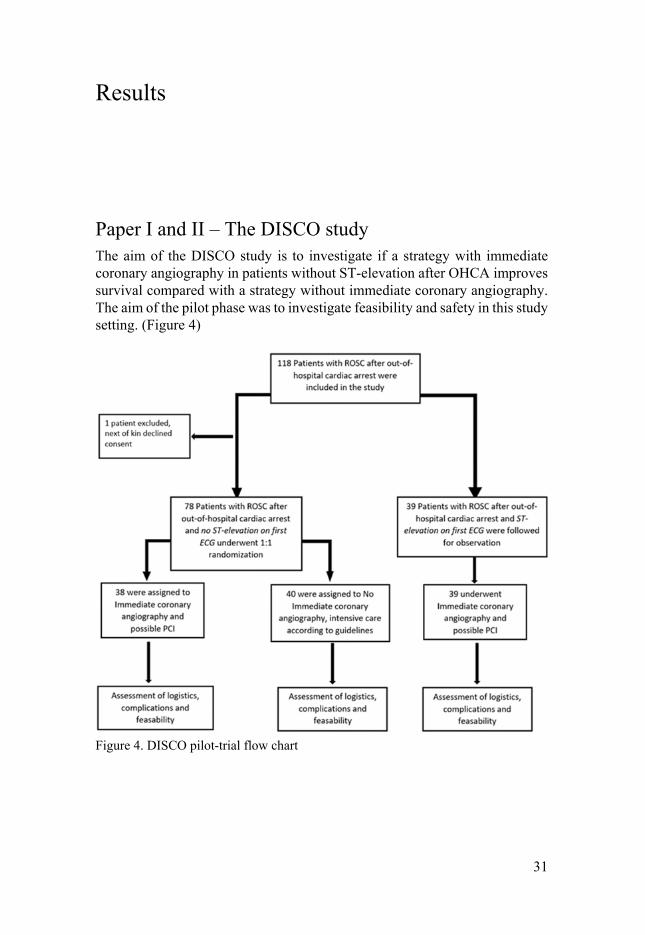
Paper I and II – The DISCO study The aim of the DISCO study is to investigate if a strategy with immediate coronary angiography in patients without ST-elevation after OHCA improves survival compared with a strategy without immediate coronary angiography. The aim of the pilot phase was to investigate feasibility and safety in this study setting. (Figure 4)
Figure 4. DISCO pilot-trial flow chart
32
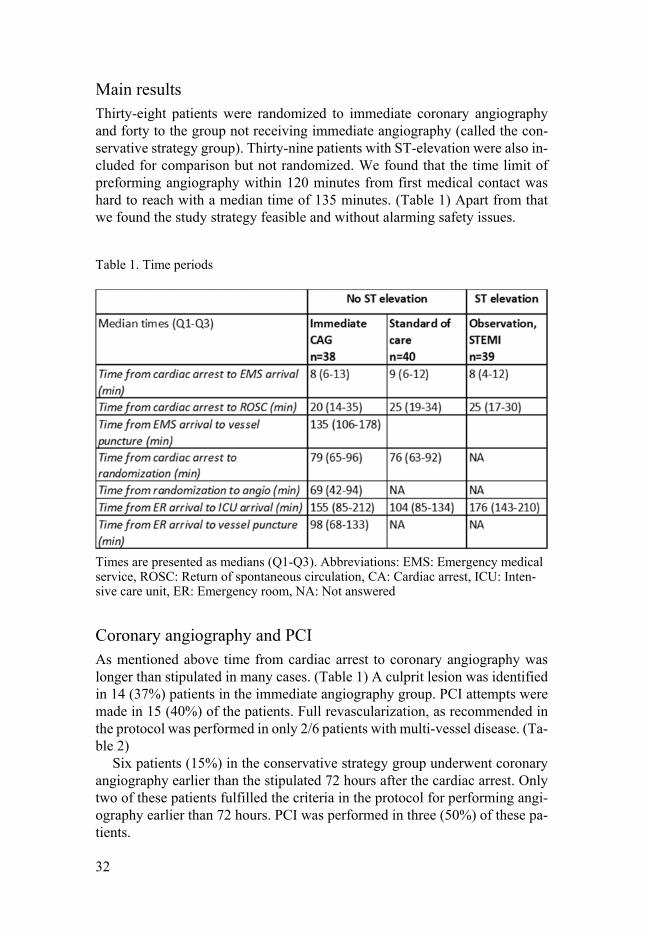
Main results Thirty-eight patients were randomized to immediate coronary angiography and forty to the group not receiving immediate angiography (called the con-servative strategy group). Thirty-nine patients with ST-elevation were also in-cluded for comparison but not randomized. We found that the time limit of preforming angiography within 120 minutes from first medical contact was hard to reach with a median time of 135 minutes. (Table 1) Apart from that we found the study strategy feasible and without alarming safety issues.
Table 1. Time periods
Times are presented as medians (Q1-Q3). Abbreviations: EMS: Emergency medical service, ROSC: Return of spontaneous circulation, CA: Cardiac arrest, ICU: Inten-sive care unit, ER: Emergency room, NA: Not answered
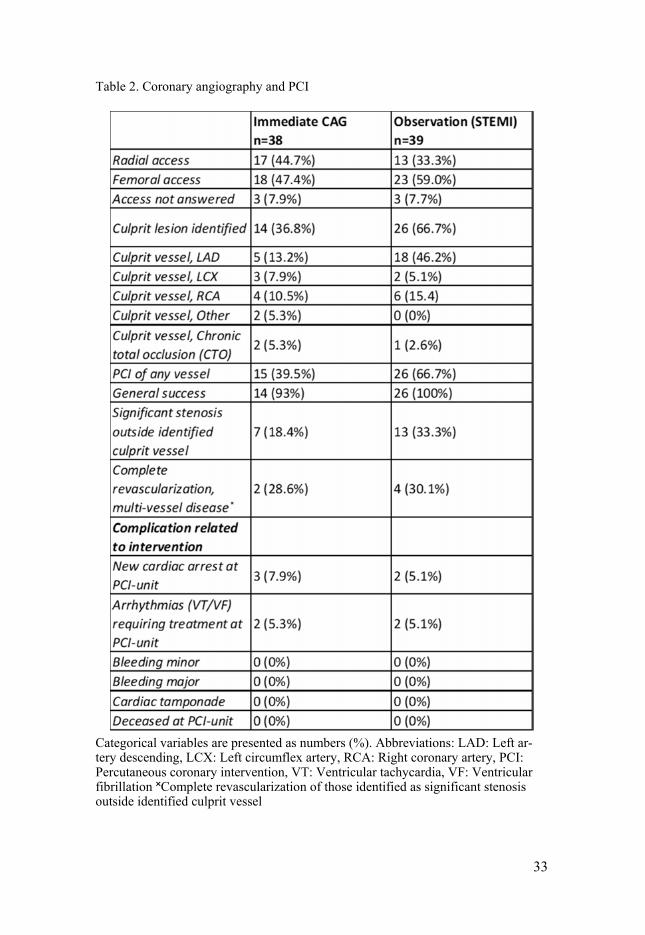
Coronary angiography and PCI As mentioned above time from cardiac arrest to coronary angiography was longer than stipulated in many cases. (Table 1) A culprit lesion was identified in 14 (37%) patients in the immediate angiography group. PCI attempts were made in 15 (40%) of the patients. Full revascularization, as recommended in the protocol was performed in only 2/6 patients with multi-vessel disease. (Ta-ble 2)
Six patients (15%) in the conservative strategy group underwent coronary angiography earlier than the stipulated 72 hours after the cardiac arrest. Only two of these patients fulfilled the criteria in the protocol for performing angi-ography earlier than 72 hours. PCI was performed in three (50%) of these pa-tients.
33
Table 2. Coronary angiography and PCI
Categorical variables are presented as numbers (%). Abbreviations: LAD: Left ar-tery descending, LCX: Left circumflex artery, RCA: Right coronary artery, PCI: Percutaneous coronary intervention, VT: Ventricular tachycardia, VF: Ventricular fibrillation ˟Complete revascularization of those identified as significant stenosis outside identified culprit vessel
34
Safety aspects Seven patients (18%) were transported to another hospital for coronary angi-ography after inclusion. No adverse events during transportation to coronary angiography was reported. However, one patient that was transported back to the admitting hospital after angiography had a new cardiac arrest during trans-portation. This transport was due to shortage of ICU beds and not in line with local recommendations or the study protocol.
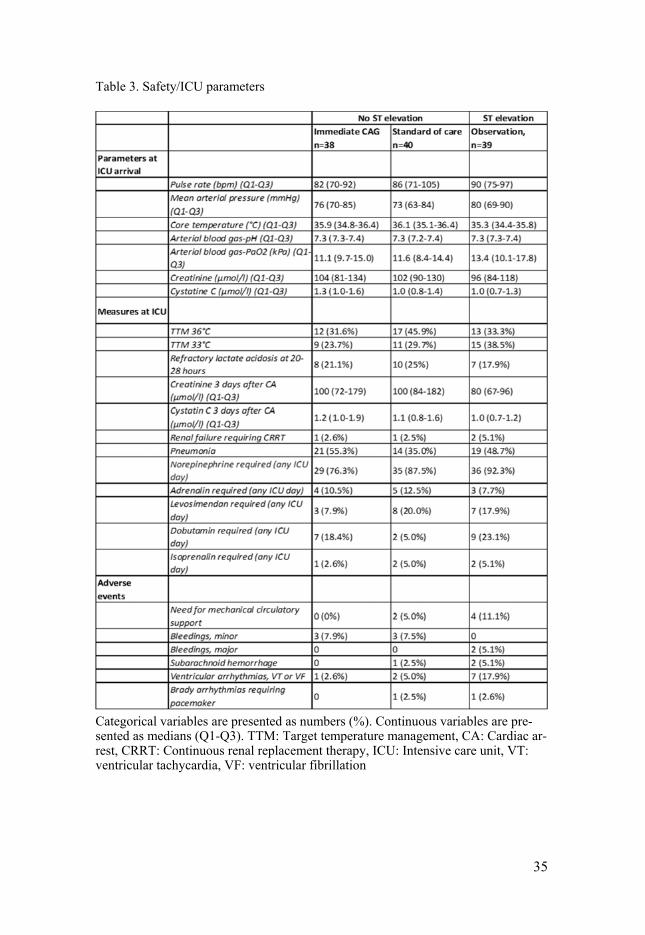
Three patients in the immediate coronary angiography group had a new cardiac arrest during the procedure but no patient suffered from a procedure related death. No major bleeding was reported in the randomized groups and the incidence of minor bleeding was similar between the groups. Kidney func-tion and the need for renal replacement therapy was also similar between the groups. (Table 3)
35
Table 3. Safety/ICU parameters
Categorical variables are presented as numbers (%). Continuous variables are pre-sented as medians (Q1-Q3). TTM: Target temperature management, CA: Cardiac ar-rest, CRRT: Continuous renal replacement therapy, ICU: Intensive care unit, VT: ventricular tachycardia, VF: ventricular fibrillation

36
Paper III
Main results 1133 patients who were successfully resuscitated after OHCA and comatose when admitted were included in the analyses. 897 (79%) had a shockable rhythm on first ECG analyses and 562 patients (50%) had other ECG findings than ST-elevation or LBBB.
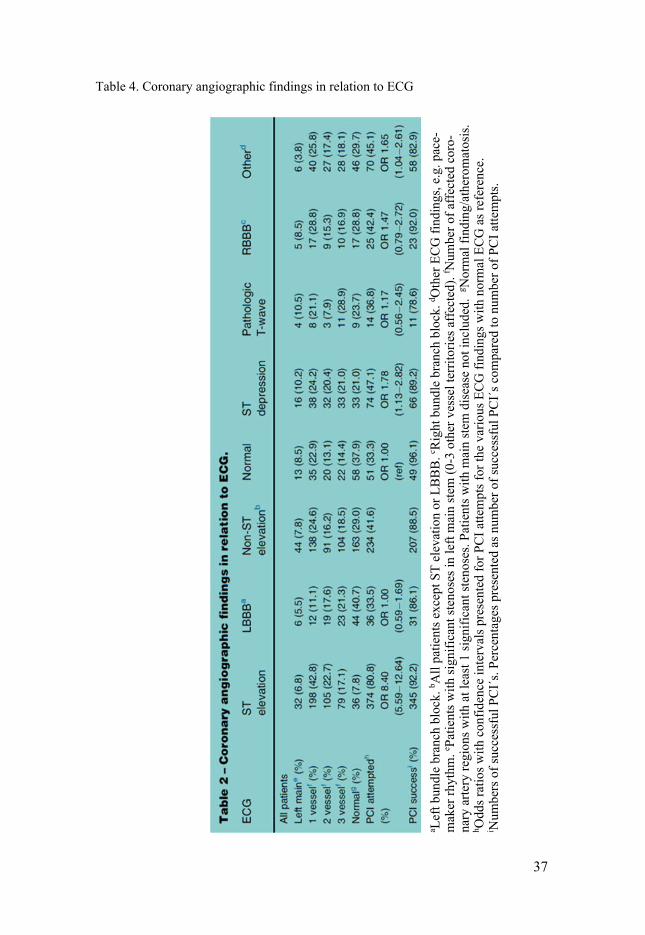
In patients without ST-elevation or LBBB, 71% had at least one significant stenosis, and PCI attempts were made in 41.6%. The rate of PCI attempts was higher in patients with ST-depression (47%) and those classified as “Other” (45%) compared to those with normal ECG where PCI attempts were made in 33% (OR 1.78, CI 1.13-2.82 and 1.65, CI 1.04-2.61 respectively). (Table 4)
37
Table 4. Coronary angiographic findings in relation to ECG
a Lef
t bun
dle
bran
ch b
lock
. b All
patie
nts e
xcep
t ST
elev
atio
n or
LBB
B. c R
ight
bun
dle
bran
ch b
lock
. d Oth
er E
CG fi
ndin
gs, e
.g. p
ace-
mak
er rh
ythm
. e Pat
ient
s with
sign
ifica
nt st
enos
es in
left
mai
n ste
m (0
-3 o
ther
ves
sel t
errit
orie
s affe
cted
). f N
umbe
r of a
ffect
ed c
oro-
nary
arte
ry re
gion
s with
at l
east
1 sig
nific
ant s
teno
ses.
Patie
nts w
ith m
ain
stem
dise
ase
not i
nclu
ded.
g Nor
mal
find
ing/
athe
rom
atos
is.
h Odd
s rat
ios w
ith c
onfid
ence
inte
rval
s pre
sent
ed fo
r PCI
atte
mpt
s for
the
vario
us E
CG fi
ndin
gs w
ith n
orm
al E
CG a
s ref
eren
ce.
i Num
bers
of s
ucce
ssfu
l PCI
´s. P
erce
ntag
es p
rese
nted
as n
umbe
r of s
ucce
ssfu
l PCI
´s c
ompa
red
to n
umbe
r of P
CI a
ttem
pts.

38
Patients in the non-ST-elevation group with diabetes mellitus or ischaemic heart disease prior to the cardiac arrest had higher rates of significant coronary artery disease compared to those with COPD or kidney disease, but also com-pared to the total population. The rate of PCI attempts, however, were similar between the comorbidity groups as well as compared to the total population.
In the group with an initial non-shockable rhythm without ST-elevation or LBBB, a PCI attempt was made in 44 patients (41%). This is similar to the PCI rate in those with initial shockable rhythm were PCI attempts were made in 42% of the patients.
Paper IV
Main results Patients admitted to Swedish hospitals after OHCA between 2008-2013 were eligible for inclusion. After exclusion of crew-witnessed cardiac arrests, 3906 patients were included. Of these, 50% had shockable rhythm and 71% re-ceived bystander CPR.
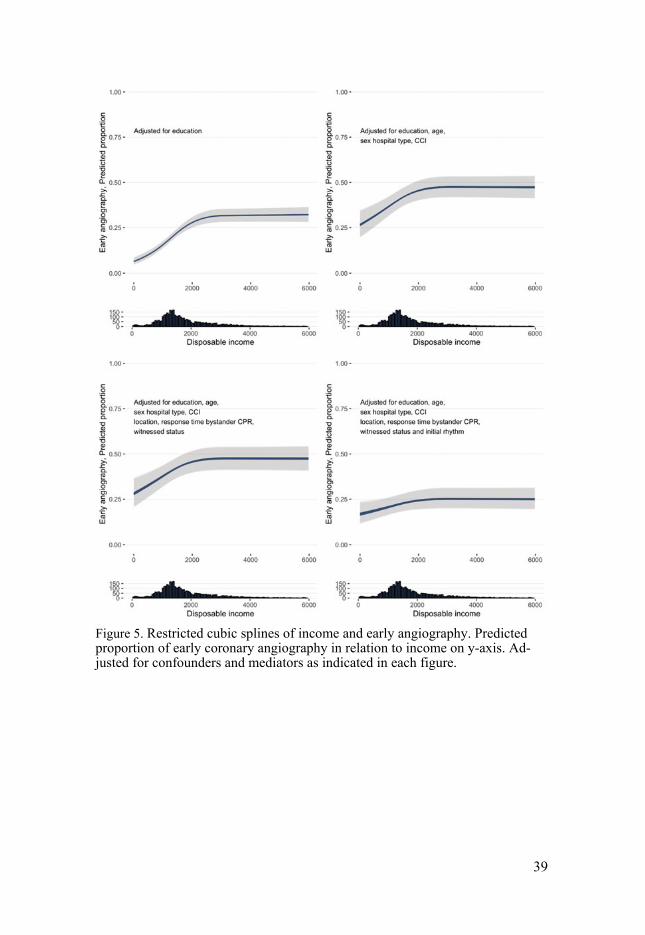
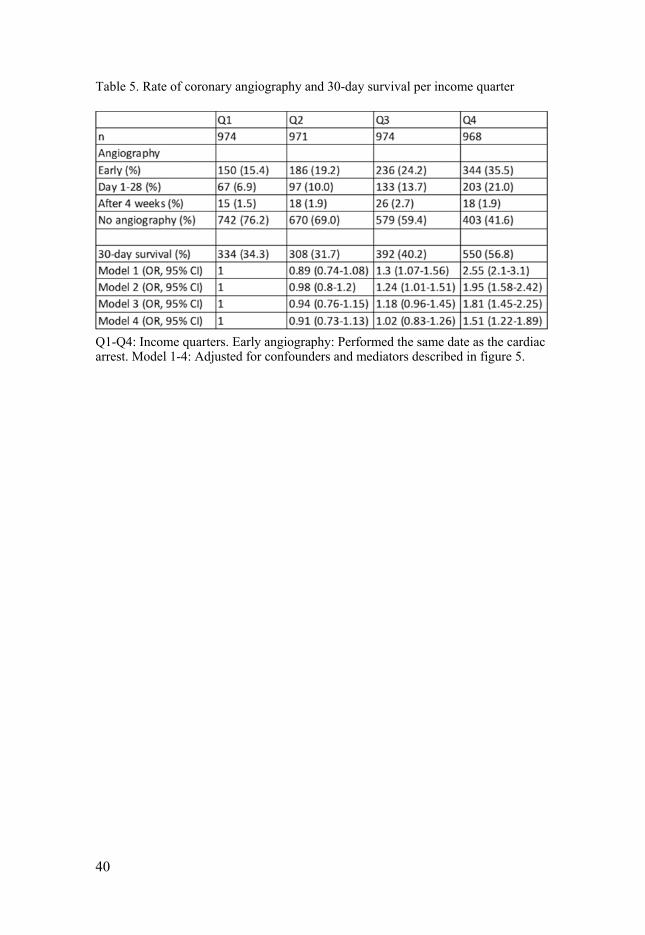
Dividing patients in quarters, based on income, showed a clear association between income and early coronary angiography. 35.5% of patients in the highest income quarter received early coronary angiography compared to 15.4% in the lowest quarter. There was also an association between education level and early angiography but not as strong as income level. These results were consistent when comparing different hospital types. When adjusting for potential confounders, (education, age, hospital type, sex and comorbidity), the association between income and early angiography remained. When also adjusting for prehospital factors that could influence outcome (location, re-sponse time, if bystander CPR was given and if the arrest was witnessed) the association became weaker but still significant. When finally adjusting also for initial rhythm, no significant association remained. When performing a similar analysis but with income as a continuous variable, the same pattern was present, i.e. a clear association between income and early coronary angi-ography that disappeared when adjusting for initial rhythm. (Figure 5)
We also performed a secondary analysis (not prespecified), analysing 30-day survival in relation to income after OHCA. In the fully adjusted model described above, patients in the highest income quarter had a higher survival rate than the lowest income quarter, OR 1.51 (CI 1.22-1.89) (Table 5)
39
Figure 5. Restricted cubic splines of income and early angiography. Predicted proportion of early coronary angiography in relation to income on y-axis. Ad-justed for confounders and mediators as indicated in each figure.
40
Table 5. Rate of coronary angiography and 30-day survival per income quarter
Q1-Q4: Income quarters. Early angiography: Performed the same date as the cardiac arrest. Model 1-4: Adjusted for confounders and mediators described in figure 5.

41
Discussion
Main findings The main findings in the papers included in my thesis were:
Paper I and II The strategy of the DISCO study, randomizing patients with ROSC after OHCA without ST elevation to a strategy with immediate coronary angi-ography vs a strategy with no immediate coronary angiography is feasible. The main feasibility problem was that median time from first medical contact to coronary angiography was longer than the 120 minutes stated in the proto-col. The number of patients included in the pilot phase was rather low, but no immediate safety concerns were obvious. This led to the start of the main, now ongoing, DISCO study with an adjusted protocol, stating that coronary angi-ography should be performed within 120 minutes from randomization.
Paper III In a large cohort of patients with ROSC after OHCA, the rate of coronary artery stenoses were high, despite the absence of ST elevation. Subgroup anal-yses of specific ECG findings within the group without ST elevation showed that the rate of PCI attempts varied between the groups, suggesting that ECG might be used as an adjunct when trying to identify patients with high risk for culprit coronary artery lesions. Certain comorbidities (previous ischaemic heart disease and diabetes) are risk factors for significant coronary artery ste-noses but these patients did not receive more PCI, suggesting comorbidity do not confer more information when identifying high risk patients for culprit lesions. Patients with non-shockable ECG rhythm without ST elevation re-ceived PCI in a similar proportion as patients with shockable rhythm when undergoing coronary angiography after ROSC.
Paper IV High patient income is associated with higher rates of early coronary angi-ography. This seems to be mediated through a higher rate of shockable ECG

42
rhythm in the higher income groups. In a secondary, not pre-specified anal-yses, we found that patients in the highest income quarter, had higher survival rate than patients in the lowest income quarter, even after adjusting for several prognostic factors.
Paper I and II At the time of designing and starting the pilot phase of the DISCO study, this was the first study randomizing patients after cardiac arrest to either immedi-ate coronary angiography or a more conventional strategy without immediate angiography. This led to a difficult power calculation. In common with most randomized studies in intensive care medicine, the power calculation becomes a balance between uncertain retrospective data, how big treatment effect that would be clinically relevant and how many patients that it is feasible to include within a reasonable time limit. We were aware, that it could be hard to reach our goal of including more than 1000 patients, and that our power calculation could be too optimistic. Therefore, already before starting the study, we initi-ated collaboration with two other research groups planning similar studies in other countries, trying to harmonize our protocols to enable us to pool data after study completion.88 The low rate of inclusion in several of the ongoing studies in the field (including DISCO), as well as the optimistic power calcu-lation and negative result of the otherwise impressing COACT trial, has strengthened our opinion that future randomized studies in intensive care med-icine in general and cardiac arrest in particular, need more international col-laboration to conduct large enough trials.63
The choice to have 30-day survival as primary endpoint might seem con-troversial in the scope of the current interest in neurologic outcome after car-diac arrest. However, 30-day survival has at least two advantages: Firstly, we anticipate very few, if any, missing patients in this particular endpoint. Fol-low-up visits for neurologic assessment carries a much higher risk of missing data. Secondly, it is easy to compare our findings with other studies, for in-stance when pooling data with other similar studies. The neurologic outcome is indeed of great importance in cardiac arrest research. It is well described that significant neurologic recovery might take months after a cardiac arrest.86 Thus, we have included an ambitious, 6-month follow-up into our secondary analyses, including several neurocognitive tests but also questionnaires meas-uring e.g. depression and anxiety. This extended follow-up might also help us to validate some of the outcome scores for the cardiac arrest population, since there are no tests specifically targeting this population.
In the pilot phase, the coronary angiography protocol included a rather ag-gressive PCI strategy, recommending PCI not only against the presumed cul-prit lesion, but also a full revascularisation, i.e. PCI against all significant ste-noses accessible for PCI. This was based on retrospective data from patients

43
in cardiogenic shock (without cardiac arrest) that suggested a benefit from an aggressive PCI strategy.89 After the publishing of the CULPRIT-SHOCK trial, including patients with ST elevation and cardiogenic shock (both patients after cardiac arrest and no cardiac arrest), where a full revascularisation strategy increased mortality and the need for renal replacement therapy, our protocol for the main study was adjusted to recommend culprit only-PCI.90 Only two patients in the pilot phase received full revascularisation and changing the pro-tocol during the study will thus not affect the final result.
The finding that we did not reach our rather ambitious timeline with 120 minutes from first medical contact to coronary angiography led us to change the protocol to the main study to count 120 minutes from randomization. The aim both in the pilot and the main study phase is that patients randomized to immediate coronary angiography should be taken to angiography as fast as possible. This small change in the protocol has not the intention to change the study strategy but instead adjusting the protocol to the clinical reality. We will thus include the outcome data from patients included during the pilot phase in the final analyses when closing the main study.
Studying safety aspects in intensive care is notoriously hard. Potential ad-verse events occur every day in the critically ill patient and its frequency are basically limited only by how hard you look for them. In the pilot phase of DISCO, we chose to focus on events likely to be affected by the intervention, but this obviously is a limitation since it is impossible to know which events that is a consequence of a certain intervention. The low number of randomized patients (79) is however the major limitation. A much larger sample size is needed to conclude that a certain strategy is equally safe as another. Out inter-pretation of our results, however, is that the pilot study did not present such major safety issues that the main study phase should be stopped. Ultimately, it is the potential benefits from immediate coronary angiography vs the poten-tial risks of this strategy in this critically ill population that needs to be studied in a large-scale randomized study.
Paper III As far as we know, this is the largest material presented, were coronary angi-ography findings in relation to ECG and comorbidity is presented. The strength, and also the aim of the study, was to include enough patients to be able to describe angiographic findings not only in relation to ST elevation and non-ST elevation patients that has been common in previous studies, but to divide the heterogenous non-ST elevation group into specified ECG findings. This has been done before, but in smaller populations.57 The finding of a slightly higher incidence of coronary artery stenoses in this material than in previous retrospective studies might be a consequence of the study’s major limitation.41 The patients included are those that have been selected, on some

44
grounds, for coronary angiography, and are thus not representative for the whole cardiac arrest population. Important anamnestic and clinical infor-mation available for the clinician when deciding to take the patient to a coro-nary angiography, are missing. Thus, it is likely that the patients included had a higher risk for coronary artery disease than the general cardiac arrest popu-lation. This obviously limits the generalizability. This kind of registry study can, in general, only be hypothesis generating. It is however possible, that the ongoing randomized studies, like DISCO, might turn out to be negative, just like the COACT trial. If that is the case we need to find strategies to better identify those likely to benefit from early coronary angiography and PCI since as clinicians, we have all seen cases that certainly have benefited from PCI after cardiac arrest, despite absence of ST elevation, in terms of improved he-modynamic stability. Negative results in large randomized trials, might thus represent either too optimistic power calculations, or the fact that some pa-tients benefits, and some are harmed by early coronary angiography. This study suggests, that ECG might have the possibility, at least as an adjunct, to select patients with higher risk of having lesions suitable for revascularisation. This highlights the need for pooling data from the ongoing randomized trials to create subgroups large enough to compare e.g. ECG findings and outcome.
The finding that the patients with non-shockable ECG rhythm, often inter-preted as having lower risk of a cardiac cause of the arrest, received PCI in a similar rate as those with shockable rhythm is interesting. Once again, in this study, we are looking at a selected material and this finding needs confirma-tion. It raises several questions though. In many countries, e.g. Sweden, the rate of patients with shockable rhythm is decreasing for unknown reasons.36 One theory is that more aggressive preventive medication for cardiac disease lowers the risk of both cardiac arrest but even more for shockable rhythms. If that is the case, patients with non-shockable rhythms might be misinterpreted as non-cardiac, thereby lowering the chances for optimal treatment. Another fact is that all cardiac arrest eventually switches from shockable to non-shock-able rhythm if ROSC is not achieved, and this develops faster if no CPR is performed or CPR quality is poor. Thus, patients that has received no or poor bystander CPR might present with a non-shockable rhythm when EMS ar-rives, even if the initial rhythm in fact was shockable. This might be one rea-son why patients with lower income receives lower rates of early coronary angiography, that is further discussed in the next section.
Paper IV The right to health is one of the human rights and it is well known that low socioeconomic status, e.g. income or education level, is associated with higher risk for cardiovascular disease and shorter life expectancy.64 It is therefore important to study socioeconomic aspects both in potential differences in the

45
care given, as well as its impact on outcome. Since low socioeconomic status has been associated with worse outcomes after cardiac arrest, we wanted to investigate, if income was associated with differences in the treatment of pa-tients, in our case early coronary angiography.70 These types of studies are hard to perform with good quality, since data on important confounders often are missing. Studies with individual income data is also uncommon. In Swe-den, the individual personal numbers, making individual patients traceable, combined with high quality registries containing both prehospital parameters, coronary angiography findings, medical diagnoses and individual income data, we have a unique possibility to perform high quality registry studies in the socioeconomic field. Of course, this study has limitations. There can al-ways be unknown confounders, the diagnoses used to calculate Charlson comorbidity index (CCI) do not provide information about the severity of the disease and patients might have undeclared incomes not covered by the regis-try.91 However, compared to other studies in this field, these limitations must be considered minor.
After adjusting for confounders, there was still a clear association between high income and higher rate of early coronary angiography. We wanted to understand the cause for this finding and performed further adjustments in our analyses for potential mediators, i.e. factors causing the difference in early coronary angiography. We found that higher income was associated with higher rates of shockable ECG rhythm, which seem to be the most important factor to explain our initial finding. This is indeed interesting and should be investigated further. We do not know the cause for this difference and several factors might be involved. Low income level is associated with lower rates of bystander CPR, and perhaps CPR with poorer quality, thus increasing the risk that an initial shockable rhythm has transformed to a non-shockable rhythm when the EMS arrives.70,73 Even if we adjusted for comorbidity, there might be differences in comorbidity that impacts the rate of shockable/non-shocka-ble rhythm but gives similar CCI-score. Finally, low socioeconomic status probably increases the risk of cardiac arrest due to non-cardiac causes, e.g. intoxications and traumatic cardiac arrests.92 Luckily, our study presents ex-planatory findings to the higher rate of early angiography in high income pa-tients and it does not seem that patients are chosen by physicians to more ac-tive treatment based on their socioeconomic status.
The finding in paper III, that patients with non-shockable rhythms had sim-ilar rates of PCI attempts when undergoing coronary angiography as patients with shockable rhythms, together with the findings in this paper, that low in-come groups has higher rates of non-shockable rhythm needs more attention. Future studies need to address the increasing group of patients with non-shockable rhythms and investigate the risk for ischaemic cardiac events in this group that are often treated as “non-cardiac” causes solely based on initial ECG rhythm.

46
The finding that patients in the highest income quarter had higher survival rates than the lowest income group is a secondary, not pre-specified finding. This obviously limits the importance of the findings. One could also argue, that the difference in outcome after cardiac arrest based on socioeconomic status is well described previously.70-72 However, few, if any prior study in this field, has been conducted with such high-quality data. Usually, socioeconomic data is based on the area either where the patient lives or where the cardiac arrest occurs and not as in our case individual data. Our study, where we could adjust our analyses for so many prognostic factors, including comorbidity and hospital type, is in our opinion conducted with enough quality to present even a result not prespecified. Furthermore, it is an important finding, since we have adjusted for the factors usually used to explain the difference in outcome, e.g. initial ECG rhythm, bystander CPR and comorbidity. Obviously, this finding needs to be confirmed in a study designed with this question as the study aim.
47
Summary/Conclusion
Paper I and II • In unconscious patients with ROSC after OHCA and no ST-elevation
on their ECG, a study strategy of randomization to either immediate coronary angiography or to a more conservative strategy of no imme-diate coronary angiography is feasible and without major safety con-cerns.
• The major feasibility concern from the pilot phase of the DISCO study was difficulties reaching our goal of 120 minutes from first medical contact to coronary angiography. Thus, the time target for the main study phase has been adjusted to 120 minutes from randomization to coronary angiography.
Paper III • In a population with OHCA-patients without ST-elevation, selected
to undergo coronary angiography, there are differences in the rate of PCI attempts based on their initial ECG findings.
• Comorbidities present prior to the cardiac arrest affected the rate of significant coronary artery disease but the rate of PCI attempts did not differ between the various comorbidity groups.
• In this selected population, patients with non-shockable rhythm re-ceived PCI to a similar extent as patients with shockable rhythm, when comparing patients without ST-elevation.
Paper IV • Patients with higher income is more likely to receive early coronary
angiography after OHCA even after adjusting for confounders. • The main explanatory factor for this finding in our study is that higher
income is associated with a higher rate of shockable ECG rhythm. • In an analysis that was not prespecified, patients in the highest income
quarter had higher 30-day survival than patients in the lowest income quarter

48
Future perspectives
Research in modern medicine in general, and intensive care in particular, poses many opportunities, but also some obstacles. Thanks to advances in the treatment of many diagnoses, mortality and morbidity rates has gradually fallen which obviously is good. On the other hand, this makes it harder to show statistically significant improvements when testing new treatment strat-egies and therapies in clinical studies. In intensive care, where the number of patients with a certain diagnose is rather limited, there is also a tendency to have to broad inclusion criteria in the study setting, e.g. all patients with septic shock or all cardiac arrest patients, with the risk of “blurring” the results. Some of the larger studies presented the last decade in the field of intensive care that presented a negative result, have likely been affected by either too small sam-ple size, too broad inclusion criteria, or both. This creates an obvious risk, that effective treatments are discarded due to poor trial design or type II errors. A finding could be clinically relevant, e.g. reducing mortality with a minor in-tervention from 50% to 48% in a certain condition but would need a huge trial to prove. This problem is often “solved” by starting the study with an optimis-tic power calculation and ends up with a negative result. Thus, there is a risk that effective treatments are abandoned due to poor trial design.
There are ways to handle this problem. Creating multicentre trials, national or international, as we have done in the DISCO trial, enables more rapid in-clusion of patients and thus a chance for a realistic power calculation without broadening inclusion criteria. Changing primary outcome measures, from e.g. survival to either physiologic endpoints, e.g. cardiac function or composite endpoints, might make it easier to present a positive result, but also in general makes the study result harder to interpret. Finally, to do classical meta-anal-yses or pooling of data from several similar studies, is a way to find smaller but important differences in outcome. It also enables analyses of subgroups to find those patients that actually benefits from a treatment in case of a negative result in the whole study group.
Already prior to starting the DISCO trial, contact was taken with research-ers internationally conducting similar studies. The aim was to prepare for a common pooling of data after all the ongoing studies have presented their re-sults. This has led us to be able to some extent, to harmonize our study proto-cols. We are currently planning to conduct a pooling of data from the DISCO trial and at least three other studies. The need for this was highlighted by the result presented last year from the COACT trial.

49
It is likely (and from a clinical perspective obvious) that some patients ben-efit from immediate coronary angiography after OHCA but for some patients the risks probably outweigh the benefits. The results from COACT and some of the results presented in this thesis, implies that future studies need to iden-tify those patients that might benefit the most from an early invasive strategy.
Another field that needs further investigation is how antithrombotic treat-ment after stenting in OHCA patients are and should be managed. Current treatment is developed in non-cardiac arrest patients and some studies have implied that cardiac arrest patients might have an increased risk of stent throm-bosis. Uptake of enterally administered drugs in post cardiac arrest patients and the effect on the treatment by therapeutic hypothermia is largely unknown and deserves attention.
The finding that low income is associated with lower rates of shockable ECG rhythms needs both confirmation and explanation. If the cause is due to lower rates/poorer quality of bystander CPR, a general discussion on how the CPR training in society should be managed. If this is the case, a discussion regarding treatment strategies (e.g. coronary angiography) based solely on in-itial rhythm needs to be initiated. The finding of high rates of PCI attempts in patients without shockable rhythm in this thesis, highlights this issue. In gen-eral, what factors that influences many of the critical decisions in intensive care medicine, e.g. admitting patients to ICU and withdrawal of care, are poorly studied and needs more attention.
50
Summary in Swedish – Sammanfattning på svenska
Plötsligt hjärtstopp utanför sjukhus är en vanlig orsak till plötsligt död. Varje år inleds hjärt-lungräddning (HLR) på ca 6000 personer i Sverige pga hjärt-stopp utanför sjukhus och av dessa räddas endast drygt 600 till livet. Chansen till överlevnad påverkas förstås av faktorer vi inte kan påverka, tex ålder och samtidiga svåra sjukdomar. Bland påverkbara faktorer, alla av stor vikt för att öka överlevnadschanserna, finns tidig upptäckt av hjärtstoppet, tidig HLR av god kvalitet och tidig behandling med s.k. hjärtstartare där en stark elektrisk ström genom hjärtat kan återstarta hjärtat vid vissa typer av hjärtstopp, de med s.k. defibrillerbar rytm (eng. shockable rhythm). För de patienter där man fått igång hjärtat, krävs också optimal efterbehandling på sjukhus, i de flesta fall med intensivvård. Vården består både av att understödja vitala funktioner som ofta är påverkade efter ett hjärtstopp och att leta och behandla orsaken till hjärtstoppet. De flesta patienter är tex medvetslösa, behöver andningsstöd i respirator och olika typer av stöd för sviktande funktion i hjärta samt lågt blod-tryck.
En de vanligaste orsakerna till hjärtstopp är att det bildats en blodpropp i ett kranskärl, hjärtats egna blodkärl. Hos de flesta patienter ger detta upphov till en hjärtinfarkt men kan också ge en rubbning i hjärtats elektriska signalsy-stem, orsaka ett elektriskt kaos och hjärtstopp. I vissa fall ger detta ett typiskt utseende på EKG, sk ST-höjning, som talar starkt för att det bildats en propp i ett kranskärl. Om patienter som återfått egen cirkulation efter ett hjärtstopp har ST-höjning på EKG får de i normalfallet direkt genomgå en kranskärls-röntgen (där man via ett blodkärl i handleden eller ljumsken för in en tunn slang upp till kranskärlen för att ge kontrastmedel direkt i kärlet) där eventu-ella proppar och förträngningar i kranskärlen kan ses. I samband med krans-kärlsröntgen kan man också öppna upp stängda kärl med en uppblåsbar bal-long (ballongvidgning) och för att förhindra att kärlet åter blir trångt lägger man in ett metallnät (stent) som spänns upp över ballongen och expanderas vid ballongvidgningen. Hos dessa patienter är akut kranskärlsröntgen en eta-blerad strategi.
Det har visat sig att relativt många patienter, i flera studier ca 30%, som efter hjärtstopp inte har en ST-höjning på EKG, trots allt har en propp i ett kranskärl. Därför argumenterar vissa för att alla patienter som inte har någon

51
uppenbar annan förklaring till hjärtstoppet borde genomgå akut kranskärls-röntgen. Detta är dock omdiskuterat då det både finns potentiella risker med detta och inte heller något starkt vetenskapligt stöd för att en sådan strategi ökar överlevnaden. Denna avhandling består av fyra arbeten som fokuserar på kranskärlsröntgen efter hjärtstopp.
Arbete I och II beskriver protokollet för DISCO-studien samt genomföran-det av en inledande, pilot-fas av studien. I DISCO-studien lottas patienter som inkommer till akutmottagningen efter hjärtstopp och inte har ST-höjning på EKG till att antingen genomgå akut kranskärlsröntgen med möjlighet till bal-longvidgning av eventuella kranskärlsförändringar eller att tas direkt till IVA utan kranskärlsröntgen. Vi kommer därefter att följa patienterna upp till sex månader och undersöka om det finns några skillnader mellan de två grupperna vad gäller överlevnad, hjärtfunktion samt hur hjärnan återhämtat sig. För att kunna ingå i studien ska patienterna vara vuxna, medvetslösa efter hjärtstop-pet, inte vara gravida och inte ha några uppenbara, icke hjärtrelaterade, andra orsaker till hjärtstoppet (tex olycksfall med stora blödningar, kvävning etc.). I pilot-fasen av studien som nu är avslutad, undersöktes om det gick att genom-föra studien enligt den plan vi lagt upp och om det fanns några uppenbara säkerhetsrisker med studiestrategin. 78 patienter utan ST-höjning inkluderas. Vi upptäckte att det var svårt att hålla den tidsgräns vi tänkt oss, 120 minuter från ambulansens ankomst till kranskärlsröntgen, men i övrigt fann vi inga större problem med genomförandet av studien. Vi kunde inte heller se några uppenbara säkerhetsproblem, dvs förekomsten av allvarliga patienthändelser var inte större än förväntat. Dessa fynd gjorde att vi kunde initiera fortsätt-ningsdelen av studien som nu pågår där totalt över 1000 patienter ska inklud-eras.
I arbete III samlades data in från flera svenska register för att kunna jämföra EKG-fynd samt tidigare sjukdomar hos patienter som haft hjärtstopp med fynd vid kranskärlsröntgen. Bakgrunden till studien var att vi ville undersöka om man kunde hitta de patienter som inte har ST-höjning efter hjärtstopp som har högst risk för proppar i kranskärlen genom EKG-analys och sjukdomshistoria. Dessa patienter borde vara de som har mest att vinna på en akut kranskärls-röntgen. 1133 patienter inkluderades i analysen. Vi kunde visa att patienter med vissa EKG-förändringar genomgick ballongvidgning i större utsträckning än andra som ett tecken på högre förekomst av proppar i kranskärlen. Däremot sågs ingen sådan skillnad när man jämförde olika bakomliggande sjukdomar. Detta skulle kunna tala för att EKG kan användas för att identifiera de patien-terna med högst risk för akut kranskärlssjukdom efter hjärtstopp. Dessa fynd måste dock bekräftas i en annan typ av studie som inte baseras på registerdata.
I arbete IV har vi undersökt om patienters inkomst påverkar sannolikheten för att man gör en tidig kranskärlsröntgen. Även i denna studie samlades data in från flera olika register. 3906 patienter med hjärtstopp analyserades. Det har tidigare visats i studier att patienter med högre utbildning och inkomst har högre överlevnad efter hjärtstopp. Detta har förklarat med att patienter med

52
lägre socioekonomisk status har fler och svårare sjukdomar sedan tidigare men också i lägre utsträckning får HLR innan ambulansens ankomst. Vi ville un-dersöka om även behandling på sjukhus påverkas av inkomstnivå. Vi kunde visa att patienter med högre inkomst i större utsträckning genomgår tidig kranskärlsröntgen efter hjärtstopp. Detta verkar lyckligtvis inte bero på att pa-tienter selekteras utifrån inkomstnivå utan förklaras till största delen av att patienter med högre inkomst i större utsträckning har s.k. defibrillerbar rytm. Denna EKG-rytm vid hjärtstopp anses tala starkt för att hjärtstoppet beror på ett primärt hjärtproblem och ökar därför sannolikheten för att en kranskärls-röntgen utförs. Varför patienter med högre inkomst har högre förekomst av defibrillerbar rytm är oklart. När vi delade in patienterna i fjärdedelar utifrån inkomstnivå kunde vi också se att de med de högsta inkomsterna hade större chans att överleva jämfört med gruppen med lägst inkomst. Detta kunde inte förklaras av olika grad av tidigare sjukdomar eller andelen som fått HLR innan ambulansens ankomst. Orsaken till denna skillnad är oklar och behöver stude-ras ytterligare.
53
Acknowledgements
The work with this thesis has always been interesting, often fun and some-times a struggle. Its content and completion would not have been possible without the help and support from brilliant colleagues and fantastic friends. Thank you all! A special thanks to:
My supervisor, professor Sten Rubertsson for constant support, the introduc-tion to the academic world and many laughs. Your combination of scientific knowledge, clinical expertise and warm humanity are impressing!
Professor Stefan James, my co-supervisor. It is an honour to have had the chance to get your always enriching input in everything from trial design to scientific English. Always clever, always kind.
My co-supervisor David Smekal. Thank you for all the tips and tricks in in-tensive care, article writing and thesis production and for always having the door open and a cup of coffee ready. Our research colleagues at Södersjukhuset, Ludwig Elfwén, Per Nordberg, Martin Jonsson and Leif Svensson for your impressive contribution to our common projects. Ollie Östlund, for all statistical input and a mind that works faster than ours. Ing-Marie Larsson and Eva Wallin for sharing your expertise and introducing me to the field of cardiac arrest outcome and follow-up. Erik Lindgren, for all the support in statistics, cardiac arrest epidemiology and for the fantastic morning reports in CIVA. Micael Taavo and Jennifer Fridman. To have some of your best friends as colleagues is a luxury. I know that. And I am grateful. Joanna Wessberg and Elin Söderman, the best research nurses possible. Pro-fessional, kind and fun, the optimal combination.
54
Katja Andersson for always having time for a chat, and the ability to be able to help with small and big things even when it is someone else’s problem. To the intensive care section at Akademiska sjukhuset and Rafael Kawati, for defending and enabling clinical research despite a heavy clinical responsibil-ity. To all my fantastic colleagues at AnOpIva who have trained me, worked with me, helped me and laughed with me. I cannot mention you all by name, but I am grateful to be surrounded by so many talented people. To my parents, Pär and Birgitta, for your constant support, encouragement and love. To my daughters, Agnes and Ebba. I am sorry for all the hours at the hospital and by the computer. You have been more than patient. You always make me glad and proud, and are a constant reminder of what is important in life. I love You! And finally, to my wife Pernilla. Even your extreme patience has been tested during the work with this thesis. I am so grateful for your understanding, sup-port and help but most of all for sharing my life with you. You are fantastic. I love you!
55
References
1. Jacobs I, Nadkarni V, Bahr J, et al. Cardiac arrest and cardiopulmonary resusci-tation outcome reports: update and simplification of the Utstein templates for re-suscitation registries. A statement for healthcare professionals from a task force of the international liaison committee on resuscitation (American Heart Associa-tion, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterA-merican Heart Foundation, Resuscitation Council of Southern Africa). Resusci-tation 2004;63:233-49.
2. Bible. I Kings 17, v. 21, II Kings, 4 v. 34. 3. Hurt R. Modern cardiopulmonary resuscitation--not so new after all. Journal of
the Royal Society of Medicine 2005;98:327-31. 4. Kouwenhoven WB, Jude JR, Knickerbocker GG. Closed-chest cardiac massage.
Jama 1960;173:1064-7. 5. Safar P, Escarraga LA, Elam JO. A comparison of the mouth-to-mouth and
mouth-to-airway methods of artificial respiration with the chest-pressure arm-lift methods. The New England journal of medicine 1958;258:671-7.
6. Perkins GD, Handley AJ, Koster RW, et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 2. Adult basic life support and auto-mated external defibrillation. Resuscitation 2015;95:81-99.
7. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation 2016;133:e38-360.
8. Committee on the Treatment of Cardiac Arrest: Current S, Future D, Board on Health Sciences P, Institute of M. The National Academies Collection: Reports funded by National Institutes of Health. In: Graham R, McCoy MA, Schultz AM, eds. Strategies to Improve Cardiac Arrest Survival: A Time to Act. Washington (DC): National Academies Press (US) Copyright 2015 by the National Academy of Sciences. All rights reserved.; 2015.
9. Grasner JT, Wnent J, Herlitz J, et al. Survival after out-of-hospital cardiac arrest in Europe - Results of the EuReCa TWO study. Resuscitation 2020;148:218-26.
10. Berdowski J, Berg RA, Tijssen JG, Koster RW. Global incidences of out-of-hos-pital cardiac arrest and survival rates: Systematic review of 67 prospective stud-ies. Resuscitation 2010;81:1479-87.
11. https://www.hlr.nu/hjart-lungraddningsregistrets-arsrapport-2018/2019. 12. Hasselqvist-Ax I, Riva G, Herlitz J, et al. Early cardiopulmonary resuscitation in
out-of-hospital cardiac arrest. The New England journal of medicine 2015;372:2307-15.
13. Waalewijn RA, Nijpels MA, Tijssen JG, Koster RW. Prevention of deterioration of ventricular fibrillation by basic life support during out-of-hospital cardiac ar-rest. Resuscitation 2002;54:31-6.
14. Weil MH, Bisera J, Trevino RP, Rackow EC. Cardiac output and end-tidal carbon dioxide. Critical care medicine 1985;13:907-9.
56
15. Rubertsson S, Grenvik A, Zemgulis V, Wiklund L. Systemic perfusion pressure and blood flow before and after administration of epinephrine during experi-mental cardiopulmonary resuscitation. Critical care medicine 1995;23:1984-96.
16. Funada A, Goto Y, Tada H, et al. Duration of cardiopulmonary resuscitation in patients without prehospital return of spontaneous circulation after out-of-hospi-tal cardiac arrest: Results from a severity stratification analysis. Resuscitation 2018;124:69-75.
17. Wallace SK, Abella BS, Becker LB. Quantifying the effect of cardiopulmonary resuscitation quality on cardiac arrest outcome: a systematic review and meta-analysis. Circulation Cardiovascular quality and outcomes 2013;6:148-56.
18. Surawicz B. Ventricular fibrillation. Journal of the American College of Cardiol-ogy 1985;5:43b-54b.
19. Herlitz J, Engdahl J, Svensson L, Angquist KA, Young M, Holmberg S. Factors associated with an increased chance of survival among patients suffering from an out-of-hospital cardiac arrest in a national perspective in Sweden. American heart journal 2005;149:61-6.
20. Soar J, Nolan JP, Bottiger BW, et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 3. Adult advanced life support. Resuscitation 2015;95:100-47.
21. Nolan JP, Soar J, Cariou A, et al. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines for Post-resuscitation Care 2015: Section 5 of the European Resuscitation Council Guidelines for Resuscitation 2015. Resuscitation 2015;95:202-22.
22. Perkins GD, Ji C, Deakin CD, et al. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. The New England journal of medicine 2018;379:711-21.
23. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. The New England journal of medicine 2002;346:549-56.
24. Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. The New England journal of medicine 2002;346:557-63.
25. Nielsen N, Wetterslev J, Cronberg T, et al. Targeted temperature management at 33 degrees C versus 36 degrees C after cardiac arrest. The New England journal of medicine 2013;369:2197-206.
26. Nolan JP, Neumar RW, Adrie C, et al. Post-cardiac arrest syndrome: epidemiol-ogy, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardio-vascular Surgery and Anesthesia; the Council on Cardiopulmonary, Periopera-tive, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation 2008;79:350-79.
27. Eastwood GM, Schneider AG, Suzuki S, et al. Targeted therapeutic mild hyper-capnia after cardiac arrest: A phase II multi-centre randomised controlled trial (the CCC trial). Resuscitation 2016;104:83-90.
28. Vaahersalo J, Bendel S, Reinikainen M, et al. Arterial blood gas tensions after resuscitation from out-of-hospital cardiac arrest: associations with long-term neu-rologic outcome. Critical care medicine 2014;42:1463-70.
29. Beylin ME, Perman SM, Abella BS, et al. Higher mean arterial pressure with or without vasoactive agents is associated with increased survival and better neuro-logical outcomes in comatose survivors of cardiac arrest. Intensive care medicine 2013;39:1981-8.
57
30. Kilgannon JH, Roberts BW, Jones AE, et al. Arterial blood pressure and neuro-logic outcome after resuscitation from cardiac arrest*. Critical care medicine 2014;42:2083-91.
31. Wang CH, Chang WT, Huang CH, et al. The effect of hyperoxia on survival fol-lowing adult cardiac arrest: a systematic review and meta-analysis of observa-tional studies. Resuscitation 2014;85:1142-8.
32. Jakkula P, Reinikainen M, Hastbacka J, et al. Targeting low- or high-normal Car-bon dioxide, Oxygen, and Mean arterial pressure After Cardiac Arrest and RE-suscitation: study protocol for a randomized pilot trial. Trials 2017;18:507.
33. Granfeldt A, Wissenberg M, Hansen SM, et al. Clinical predictors of shockable versus non-shockable rhythms in patients with out-of-hospital cardiac arrest. Re-suscitation 2016;108:40-7.
34. Geri G, Passouant O, Dumas F, et al. Etiological diagnoses of out-of-hospital cardiac arrest survivors admitted to the intensive care unit: Insights from a French registry. Resuscitation 2017;117:66-72.
35. Andrew E, Nehme Z, Lijovic M, Bernard S, Smith K. Outcomes following out-of-hospital cardiac arrest with an initial cardiac rhythm of asystole or pulseless electrical activity in Victoria, Australia. Resuscitation 2014;85:1633-9.
36. Hulleman M, Zijlstra JA, Beesems SG, et al. Causes for the declining proportion of ventricular fibrillation in out-of-hospital cardiac arrest. Resuscitation 2015;96:23-9.
37. Bunch TJ, White RD, Friedman PA, Kottke TE, Wu LA, Packer DL. Trends in treated ventricular fibrillation out-of-hospital cardiac arrest: a 17-year popula-tion-based study. Heart rhythm 2004;1:255-9.
38. Youngquist ST, Kaji AH, Niemann JT. Beta-blocker use and the changing epide-miology of out-of-hospital cardiac arrest rhythms. Resuscitation 2008;76:376-80.
39. Cobb LA, Fahrenbruch CE, Olsufka M, Copass MK. Changing incidence of out-of-hospital ventricular fibrillation, 1980-2000. Jama 2002;288:3008-13.
40. Bergstrom M, Schmidbauer S, Herlitz J, Rawshani A, Friberg H. Pulseless elec-trical activity is associated with improved survival in out-of-hospital cardiac ar-rest with initial non-shockable rhythm. Resuscitation 2018;133:147-52.
41. Dumas F, Cariou A, Manzo-Silberman S, et al. Immediate percutaneous coronary intervention is associated with better survival after out-of-hospital cardiac arrest: insights from the PROCAT (Parisian Region Out of hospital Cardiac ArresT) registry. Circulation Cardiovascular interventions 2010;3:200-7.
42. Chen N, Callaway CW, Guyette FX, et al. Arrest etiology among patients resus-citated from cardiac arrest. Resuscitation 2018;130:33-40.
43. Smilowitz NR, Feit F. The History of Primary Angioplasty and Stenting for Acute Myocardial Infarction. Current cardiology reports 2016;18:5.
44. Gruntzig AR, Senning A, Siegenthaler WE. Nonoperative dilatation of coronary-artery stenosis: percutaneous transluminal coronary angioplasty. The New Eng-land journal of medicine 1979;301:61-8.
45. Grines CL, Browne KF, Marco J, et al. A comparison of immediate angioplasty with thrombolytic therapy for acute myocardial infarction. The Primary Angio-plasty in Myocardial Infarction Study Group. The New England journal of med-icine 1993;328:673-9.
46. Grines CL, Cox DA, Stone GW, et al. Coronary angioplasty with or without stent implantation for acute myocardial infarction. Stent Primary Angioplasty in Myo-cardial Infarction Study Group. The New England journal of medicine 1999;341:1949-56.

58
47. Bangalore S, Kumar S, Fusaro M, et al. Short- and long-term outcomes with drug-eluting and bare-metal coronary stents: a mixed-treatment comparison analysis of 117 762 patient-years of follow-up from randomized trials. Circulation 2012;125:2873-91.
48. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). European heart journal 2018;39:119-77.
49. Roffi M, Patrono C, Collet JP, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-seg-ment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). European heart journal 2016;37:267-315.
50. Rasmussen MB, Stengaard C, Sorensen JT, et al. Comparison of Acute Versus Subacute Coronary Angiography in Patients With NON-ST-Elevation Myocar-dial Infarction (from the NONSTEMI Trial). The American journal of cardiology 2019;124:825-32.
51. Pareek N, Kordis P, Webb I, Noc M, MacCarthy P, Byrne J. Contemporary Man-agement of Out-of-hospital Cardiac Arrest in the Cardiac Catheterisation Labor-atory: Current Status and Future Directions. Interventional cardiology (London, England) 2019;14:113-23.
52. Spaulding CM, Joly LM, Rosenberg A, et al. Immediate coronary angiography in survivors of out-of-hospital cardiac arrest. The New England journal of medicine 1997;336:1629-33.
53. Anyfantakis ZA, Baron G, Aubry P, et al. Acute coronary angiographic findings in survivors of out-of-hospital cardiac arrest. American heart journal 2009;157:312-8.
54. Radsel P, Knafelj R, Kocjancic S, Noc M. Angiographic characteristics of coro-nary disease and postresuscitation electrocardiograms in patients with aborted cardiac arrest outside a hospital. The American journal of cardiology 2011;108:634-8.
55. Zanuttini D, Armellini I, Nucifora G, et al. Predictive value of electrocardiogram in diagnosing acute coronary artery lesions among patients with out-of-hospital-cardiac-arrest. Resuscitation 2013;84:1250-4.
56. Dumas F, Manzo-Silberman S, Fichet J, et al. Can early cardiac troponin I meas-urement help to predict recent coronary occlusion in out-of-hospital cardiac arrest survivors? Critical care medicine 2012;40:1777-84.
57. Staer-Jensen H, Nakstad ER, Fossum E, et al. Post-Resuscitation ECG for Selec-tion of Patients for Immediate Coronary Angiography in Out-of-Hospital Cardiac Arrest. Circulation Cardiovascular interventions 2015;8.
58. Dumas F, White L, Stubbs BA, Cariou A, Rea TD. Long-term prognosis follow-ing resuscitation from out of hospital cardiac arrest: role of percutaneous coro-nary intervention and therapeutic hypothermia. Journal of the American College of Cardiology 2012;60:21-7.
59. Hollenbeck RD, McPherson JA, Mooney MR, et al. Early cardiac catheterization is associated with improved survival in comatose survivors of cardiac arrest with-out STEMI. Resuscitation 2014;85:88-95.
60. Dankiewicz J, Nielsen N, Annborn M, et al. Survival in patients without acute ST elevation after cardiac arrest and association with early coronary angiography: a post hoc analysis from the TTM trial. Intensive care medicine 2015;41:856-64.
59
61. Millin MG, Comer AC, Nable JV, et al. Patients without ST elevation after return of spontaneous circulation may benefit from emergent percutaneous intervention: A systematic review and meta-analysis. Resuscitation 2016;108:54-60.
62. Elfwen L, Lagedal R, James S, et al. Coronary angiography in out-of-hospital cardiac arrest without ST elevation on ECG-Short- and long-term survival. Amer-ican heart journal 2018;200:90-5.
63. Lemkes JS, Janssens GN, van der Hoeven NW, et al. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. The New England journal of med-icine 2019.
64. Mackenbach JP, Stirbu I, Roskam AJ, et al. Socioeconomic inequalities in health in 22 European countries. The New England journal of medicine 2008;358:2468-81.
65. Alter DA, Naylor CD, Austin P, Tu JV. Effects of socioeconomic status on access to invasive cardiac procedures and on mortality after acute myocardial infarction. The New England journal of medicine 1999;341:1359-67.
66. Udell JA, Juurlink DN, Kopp A, Lee DS, Tu JV, Mamdani MM. Inequitable dis-tribution of implantable cardioverter defibrillators in Ontario. Int J Technol As-sess Health Care 2007;23:354-61.
67. Guan J, Karsy M, Couldwell WT, et al. Factors influencing management of un-ruptured intracranial aneurysms: an analysis of 424 consecutive patients. J Neu-rosurg 2016:1-6.
68. Schnegelsberg A, Mackenhauer J, Nibro HL, Dreyer P, Koch K, Kirkegaard H. Impact of socioeconomic status on mortality and unplanned readmission in septic intensive care unit patients. Acta Anaesthesiol Scand 2016;60:465-75.
69. Schroder SL, Richter M, Schroder J, Frantz S, Fink A. Socioeconomic inequali-ties in access to treatment for coronary heart disease: A systematic review. Inter-national journal of cardiology 2016;219:70-8.
70. van Nieuwenhuizen BP, Oving I, Kunst AE, et al. Socio-economic differences in incidence, bystander cardiopulmonary resuscitation and survival from out-of-hospital cardiac arrest: A systematic review. Resuscitation 2019;141:44-62.
71. Jonsson M, Harkonen J, Ljungman P, et al. Survival after out-of-hospital cardiac arrest is associated with area-level socioeconomic status. Heart (British Cardiac Society) 2019;105:632-8.
72. Wells DM, White LL, Fahrenbruch CE, Rea TD. Socioeconomic status and sur-vival from ventricular fibrillation out-of-hospital cardiac arrest. Ann Epidemiol 2016;26:418-23.e1.
73. Moncur L, Ainsborough N, Ghose R, Kendal SP, Salvatori M, Wright J. Does the level of socioeconomic deprivation at the location of cardiac arrest in an English region influence the likelihood of receiving bystander-initiated cardiopulmonary resuscitation? Emerg Med J 2016;33:105-8.
74. Lemiale V, Dumas F, Mongardon N, et al. Intensive care unit mortality after car-diac arrest: the relative contribution of shock and brain injury in a large cohort. Intensive care medicine 2013;39:1972-80.
75. Sekhon MS, Ainslie PN, Griesdale DE. Clinical pathophysiology of hypoxic is-chemic brain injury after cardiac arrest: a "two-hit" model. Critical care (London, England) 2017;21:90.
76. Lilja G, Nielsen N, Friberg H, et al. Cognitive function in survivors of out-of-hospital cardiac arrest after target temperature management at 33 degrees C ver-sus 36 degrees C. Circulation 2015;131:1340-9.
77. Kragholm K, Wissenberg M, Mortensen RN, et al. Return to Work in Out-of-Hospital Cardiac Arrest Survivors: A Nationwide Register-Based Follow-Up Study. Circulation 2015;131:1682-90.
60
78. Dragancea I, Rundgren M, Englund E, Friberg H, Cronberg T. The influence of induced hypothermia and delayed prognostication on the mode of death after car-diac arrest. Resuscitation 2013;84:337-42.
79. Dragancea I, Horn J, Kuiper M, et al. Neurological prognostication after cardiac arrest and targeted temperature management 33 degrees C versus 36 degrees C: Results from a randomised controlled clinical trial. Resuscitation 2015;93:164-70.
80. Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet (London, England) 1975;1:480-4.
81. Wallin E, Larsson IM, Rubertsson S, Kristofferzon ML. Cardiac arrest and hypo-thermia treatment--function and life satisfaction among survivors in the first 6 months. Resuscitation 2014;85:538-43.
82. Cronberg T, Lilja G, Horn J, et al. Neurologic Function and Health-Related Qual-ity of Life in Patients Following Targeted Temperature Management at 33 de-grees C vs 36 degrees C After Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA Neurol 2015;72:634-41.
83. Wilder Schaaf KP, Artman LK, Peberdy MA, et al. Anxiety, depression, and PTSD following cardiac arrest: a systematic review of the literature. Resuscita-tion 2013;84:873-7.
84. Moulaert VR, Verbunt JA, van Heugten CM, Wade DT. Cognitive impairments in survivors of out-of-hospital cardiac arrest: a systematic review. Resuscitation 2009;80:297-305.
85. Petito CK, Feldmann E, Pulsinelli WA, Plum F. Delayed hippocampal damage in humans following cardiorespiratory arrest. Neurology 1987;37:1281-6.
86. Tong JT, Eyngorn I, Mlynash M, Albers GW, Hirsch KG. Functional Neurologic Outcomes Change Over the First 6 Months After Cardiac Arrest. Critical care medicine 2016;44:e1202-e7.
87. World Medical Association Declaration of Helsinki: ethical principles for medi-cal research involving human subjects. Jama 2013;310:2191-4.
88. Hauw-Berlemont C, Lamhaut L, Diehl JL, et al. EMERGEncy versus delayed coronary angiogram in survivors of out-of-hospital cardiac arrest with no obvious non-cardiac cause of arrest: Design of the EMERGE trial. American heart journal 2020;222:131-8.
89. Windecker S, Kolh P, Alfonso F, et al. 2014 ESC/EACTS Guidelines on myo-cardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the Euro-pean Association of Percutaneous Cardiovascular Interventions (EAPCI). Euro-pean heart journal 2014;35:2541-619.
90. Thiele H, Akin I, Sandri M, et al. PCI Strategies in Patients with Acute Myocar-dial Infarction and Cardiogenic Shock. The New England journal of medicine 2017.
91. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. Jour-nal of chronic diseases 1987;40:373-83.
92. Brattstrom O, Eriksson M, Larsson E, Oldner A. Socio-economic status and co-morbidity as risk factors for trauma. European journal of epidemiology 2015;30:151-7.


Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1644
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-406036
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2020





























