Embed Size (px)
Citation preview

7262019 Cornea 2014 p1109
httpslidepdfcomreaderfullcornea-2014-p1109 14
CASE R EPORT
Lattice Corneal Dystrophy Type 1 An Epithelial or Stromal Entity
Walter Lisch MD and Berthold Seitz MDdagger
Purpose To evaluate the question whether lattice corneal dystro-
phy type 1 (LCD1) is of epithelial or stromal origin
Methods The landmark of advanced LCD1 shows central
super 1047297cial haze and paracentral stromal lattice lines In 16 eyes of
8 affected individuals of 2 families a penetrating keratoplasty was
performed The follow-up was 8 to 16 years after penetrating
keratoplasty Slit-lamp documentation of the patients was evaluated
in direct and indirect illumination with dilated pupil to assess the
horizontal and vertical pattern of new deposits on the corneal graftThree affected patients of 2 families are demonstrated in detail A
DNA analysis was performed
Results Gene identi1047297cation revealed a transforming growth factor
beta-induced (TGFBI) Leu509Pro mutation in the 1047297rst family and
a TGFBI Arg124Cys mutation in the second family The demon-
strated 5 corneal grafts of the 3 LCD1-patients showed diffuse
opacities of distinct severity beginning 3 to 4 years postoperatively
that were often combined with corneal erosions and consecutive
pain In none of our patients we were able to detect any signs of
lattice formation in the form of gray lines that run obliquely from the
surface to the midstroma in direct illumination In retroillumination
no lattice opacity units in the form of translucent and refractile lines
were visible on the graft
Conclusions The TGFBI gene that is responsible for LCD1 is
expressed above all by the corneal epithelial cells but also by the
keratocytes We interpret the super 1047297cial diffuse LCD1 recurrences
on the graft as the product of the epithelial cells whereas the non-
occurrence of lattice lines as long as 18 years after keratoplasty an
indirect sign that the lattice lines are the product of the keratocytes
Thus LCD1 seems to represent an epithelial ndash stromal entity because
both epithelial cells and keratocytes are involved
Key Words lattice corneal dystrophy type 1 LCD1 TGFBI gene
penetrating keratoplasty recurrences epithelial ndash stromal dystrophy
(Cornea 2014331109 ndash 1112)
Lattice corneal dystrophy type 1 (LCD1) represents 1 of the5 transforming beta-induced (TGFBI )-corneal dystrophies
that are located at chromosome 5q3112 LCD1 is classi1047297ed asa stromal dystrophy in the international classi1047297cation systemof corneal dystrophies published by the International Com-mittee for Classi1047297cation of Corneal Dystrophies in 20083
Mutations in the TGFBI gene encoding for keratoepithelinwere found to be responsible for LCD112 The function of keratoepithelin is not yet understood although it is thought to
be an extracellular matrix protein mediating cell adhesion4
Keratoepithelin represents one of the major corneal proteinsLCD1 starts in the 1047297rst decade of life with 1047298eck-like opacitiesat the level of the central epithelium and subepithelium Thereare also paracentrally few and very thin lattice lines that areonly visible in retroillumination In the adult there are densediffuse opacities at the level of central epithelium and sub-epithelium Additionally a network of delicate branching lat-tice lines occurs in the stroma paracentrally in direct and indirect illumination and gives the name to this dystrophyIn LCD1 recurrence in the graft after standard penetratingkeratoplasty (PKP) is common56 These recurrences initiallytake the form of subepithelial deposits that can occur approx-imately 4 years after keratoplasty No recurrent true lattice
lines could be observed on the graft The origin of the depos-its in LCD1 has been a subject of discussion There are con-troversial reports that LCD1 is of epithelial or stromalorigin67 Our aim was to clinically investigate the recurrence
patterns of LCD1 on the graft after more than 5 years after PKP and to try to answer together with known histologicaland genetic results the question whether this entity is of epithelial or stromal source The 1047297ndings of 3 patients of the 2 families are described in detail
PATIENTS AND METHODS
Case 1
A 40-year-old male patient the older brother of case 2 presented in 1997 In both corneas dense diffuse opacities onthe super 1047297cial layers combined with paracentral stromallattice lines (Figs 1A B) His best visual acuity at this timewas 615 in the right eye and 620 in the left eye The diag-nosis was LCD1 based on the clinical appearance of cornealopacities He had been suffering from visual impairment sincethe 1047297rst decade of life and had shown symptoms of repeated extraocular in1047298ammation with photophobia and pain due torecurrent epithelial erosions A DNA analysis was performedThe patient underwent PKP on his left eye in 1997 and on hisright eye in 1999 without any intraoperative or postoperative
Received for publication March 18 2014 revision received April 22 2014accepted June 10 2014 Published online ahead of print July 22 2014
From the Department of Ophthalmology Johannes Gutenberg UniversityMainz Mainz Germany and daggerDepartment of Ophthalmology UniversityMedical Center UKS Saarland Germany
The authors have no funding or con1047298icts of interest to discloseW Lisch and B Seitz contributed equally to this studyReprints Walter Lisch MD Kurt-Blaum-Platz 8 Hanau 63450 Germany
(e-mail profdrlischaugenklinik-hanaude)Copyright copy 2014 by Lippincott Williams amp Wilkins
Cornea
Volume 33 Number 10 October 2014 wwwcorneajrnlcom |
1109
7262019 Cornea 2014 p1109
httpslidepdfcomreaderfullcornea-2014-p1109 24
problems The follow-up consists of regular 3-month slit-lamp examinations in direct and indirect illumination bydilated pupil until today
Case 2
A 39-year-old female patient the younger sister of case 1 presented in 1997 with very dense diffuse opacitieson the super 1047297cial layers mostly masquerading the para-central stromal lattice lines (Fig 2A) Her best visual acuityat this time was 630 in the right eye and 620 in the left eye
The diagnosis was LCD1 based on the clinical appearance of corneal opacities and on the family history She also had recurrent painful attacks due to epithelial erosions and slowly diminishing visual acuity for many years Her 16-year-old daughter showed very 1047297ne paracentral latticelines that were only visible by retroillumination (Fig 2B)A DNA analysis was performed Case 2 underwent PKP onher right eye in 1998 and on her left eye in 1999 without anyintraoperative or postoperative problems The follow-upconsisted of annual slit-lamp examination in direct and indi-rect illumination by dilated pupil because the patient is stillliving abroad
Case 3A 43-year-old female patient not related to cases 1
and 2 presented in 1996 with dense diffuse opacities on thesuper 1047297cial layers combined with paracentral stromal latticelines Her best visual acuity at this time was 620 in the right eye and 612 in the left eye The diagnosis was LCD1 based on the clinical appearance of corneal opacities and on thefamily history She had been suffering from visual impair-ment since the beginning of the second decade of life and had shown recurrent painful attacks due to epithelialerosions A DNA analysis was performed The patient underwent right PKP in 2000 without any intraoperative or
postoperative problems The follow-up consisted of irregular
slit-lamp examinations in direct and indirect illumination bydilated pupil because the patient lives far away from our of 1047297ces
RESULTS
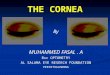
The gene identi1047297cation of family 1 (cases 1 and 2)revealed a TGFBI Leu509Pro mutation In 2002 both graftsof case 1 were clear and the best visual acuity was 67 in theright eye and 68 in the left eye (Fig 1C) In 2005 1047297rst signsof recurrence could be observed in the left graft in the form of moderate diffuse super 1047297cial opacities of the central cornea In2008 1047297rst signs of recurrences could be observed in the right graft similar to those of the left eye No lattice lines were
revealed on either graft in direct and indirect illumination In2013 bilateral diffuse super 1047297cial opacities of the graft werevisible centrally and paracentrally (Fig 1D) No lattice linescould be observed The best visual acuity was 612 in theright eye and 624 in the left eye The beginning of the recur-rence was after 10 years on the right graft and after 8 years onthe left
In case 2 both grafts were clear in 2003 The best visualacuity was 66 in the right eye and 610 in the left eye becauseof a higher astigmatism In 2006 the right graft did not showany signs of recurrence However the left graft showed moderate diffuse super 1047297cial haze on the paracentral nasal area
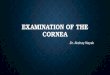
FIGURE 1 Lattice corneal dystrophy type 1 (TGFBI Leu509Pro) A A 40-year-old male patient with diffuse opacities of the sub-epithelial cornea in direct illumination B The same eye showingparacentral stromal lattice lines in retroillumination C The sameeye 9 years after PKP revealing diffuse opacities but no latticelines on the graft
Lisch and Seitz Cornea Volume 33 Number 10 October 2014
1110 |
wwwcorneajrnlcom
2014 Lippincott Williams amp Wilkins
7262019 Cornea 2014 p1109
httpslidepdfcomreaderfullcornea-2014-p1109 34
of the graft No lattice lines were seen in direct and indirect illumination The best visual acuity was unchanged on bothand identical to that of 2003 In 2013 there were diffusecentral and paracentral opacities on the super 1047297cial layers of the graft on both eyes left more than right (Fig 2C) How-ever no lattice lines were visible on the graft but on the host
cornea in indirect illumination (Fig 2D) The best visualacuity was 675 right eye and 620 left eye The beginningof the recurrence was 7 years after PKP on the left graft and later on the right without exact determination
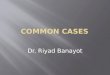
The gene identi1047297cation of case 3 (family 2) revealed a TGFBI Arg124Cys mutation In 2002 the graft on the right eye was clear The best visual acuity on the right was 68 In2004 the 1047297rst recurrence in the form of 1047297ne diffuse super 1047297cialhaze of the central cornea could be revealed The best visualacuity was the same as in 2002 In 2013 there were super 1047297cialdense but irregular diffuse opacities throughout the graft (Fig 3A) No lattice lines were revealed in direct and indirect illumination (Fig 3B) The best visual acuity was 630 The
beginning of the recurrence was 4 years after PKP
DISCUSSION
In 1979 Witschel and Sundmacher pointed out that granular corneal dystrophy and LCD1 may eventually evolveas primarily epithelial diseases78 In 1997 the TGFBI gene of LCD1 was identi1047297ed2 The most frequent mutation in LCD1is the Arg124Cys mutation To date many other independent mutations have been reported regarding LCD1 Recently wehave been able to 1047297nd a new Leu509Pro mutation regardingour second family The precise molecular functions of TGFBI in vivo are unknown but it has been proposed that it may act as a cell adhesion molecule and as a bifunctional linker pro-
tein interconnecting different matrix molecules to reach other cells The TGFBI gene is expressed above all by the cornealepithelial cells but also by the keratocytes9 It is a very impor-tant fact regarding the pathomorphology of the TGFBI cor-neal dystrophies that both epithelial cells and keratocytes areinvolved in the pathological process In LCD1 the diffuseopacities are located at the level of epitheliumsubepitheliumwhereas the lattice lines run through the whole stroma Bothopacity patterns start in the 1047297rst decade of life However wecan see a difference in the distribution of the 2 LCD1 opacity
patterns when the disease recurs after PKP Snead and Math-ews10 postulate that the reason for this difference may be that donor keratocytes survive long enough in the transplanted cornea to prevent building up of abnormal keratoepithelin
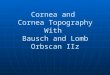
FIGURE 2 Lattice corneal dystrophy type 1 (TGFBI Leu509-Pro) A A 39-year-old female patient (sister of the patient of Fig 1) with dense superficial opacities mostly masqueradingthe stromal lattice lines (arrow) in direct illumination B A 16-
year-old daughter of (A) revealing fine paracentral lattice linesin retroillumination C The same eye as in (A) 15 years after PKP with diffuse opacities on the graft but without lattice linesin direct illumination D The same eye disclosing no latticelines on the graft but on the host cornea in retroillumination(arrow)
Cornea Volume 33 Number 10 October 2014 Lattice Corneal Dystrophy Type 1
2014 Lippincott Williams amp Wilkins wwwcorneajrnlcom
|
1111
7262019 Cornea 2014 p1109
httpslidepdfcomreaderfullcornea-2014-p1109 44
the product of the mutated gene in LCD1 By contrast theepithelium being replaced by host epithelium shortly after grafting is still producing abnormal protein The 1047297ndingssuggest different corneal cell types may repopulate at differ-ent speeds The repeat corneal grafts performed 24 years later on both eyes of Snead rsquos patient showed histologically exten-sive amyloid deposits between the epithelium and Bowman
layer10 There was relative sparing of the stroma in bothcorneas
The theory of differential expression based on the presence of host epithelial cells with a paucity of keratocytesseems to have validity but proof awaits better understandingof how keratocytes or 1047297 broblasts might form refractile lines in
the undisturbed dystrophy The theory could be further endorsed if there was evidence in reoperated grafts of thelocation of TGFBI in the epithelial cells as opposed tokeratocytes
The clinical and histological results of penetratingLCD1 grafts show together with the characteristics of theTGFBI gene that LCD1 represents not an isolated epithelial or isolated stromal dystrophy but a common epithelial ndash stromalentity This assessment has important clinical implicationsregarding the treatment of graft LCD1 recurrence performing
phototherapeutic keratectomy 1047297rst may postpone PKP
REFERENCES
1 Stone EM Mathers WD Rosenwasser GO et al Three autosomal dom-inant corneal dystrophies map to chromosome 5q Nat Genet 1994647 ndash 51
2 Munier FL Korvatska E Djemaiuml A et al Kerato-epithelin mutations infour 5q31-linked corneal dystrophies Nat Genet 199715247 ndash 251
3 Weiss JS Moslashller HU Lisch W et al The IC3D classi1047297cation of thecorneal dystrophies Cornea 200827(suppl 2)S1 ndash S83
4 Skonier J Neubauer M Madisen L et al cDNA cloning and sequenceanalysis of beta ig-h3 a novel gene induced in human adenocarcinomacell line after treatment with transforming growth factor-beta DNA Cell Biol 199211511 ndash 522
5 Klintworth GK Ferry AP Sugar A et al Recurrence of lattice cornealdystrophy type 1 in the corneal grafts of two siblings Am J Ophthalmol198294540 ndash 546
6 Meisler DM Fine M Recurrence of the clinical signs of lattice cornealdystrophy (type 1) in corneal transplants Am J Ophthalmol 198497210 ndash 214
7 Witschel H Sundmacher R Bilateral recurrence of granular cornealdystrophy in the grafts A clinic-pathological study Albrecht VonGraefes Arch Klin Exp Ophthalmol 1979209179 ndash 188
8 Witschel H Epithelial origin of ldquostromalrdquo corneal dystrophies ArchOphthalmol 2002120101 ndash 102
9 Wang MX Flattem NL Munier FL Molecular genetics of corneal dys-trophies In Wang MX ed Corneal Dystrophies and Degenerations(Chapter 1) American Academy of Ophthalmology New York Oxford University Press 2003161 ndash 17
10 Snead DRJ Mathews BN Differences in amyloid deposition in primaryand recurrent corneal lattice dystrophy type 1 Cornea 200221308 ndash 311
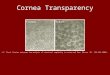
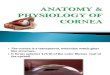
FIGURE 3 Lattice corneal dystrophy type 1 (TGFBI Arg124Cys) A A 60-year-old female patient with superficial irregular diffuse opacities on the graft 13 years after PKP in direct
illumination B The same eye showing no lattice lines on thegraft in retroillumination
Lisch and Seitz Cornea Volume 33 Number 10 October 2014
1112 |
wwwcorneajrnlcom
2014 Lippincott Williams amp Wilkins

7262019 Cornea 2014 p1109
httpslidepdfcomreaderfullcornea-2014-p1109 24
problems The follow-up consists of regular 3-month slit-lamp examinations in direct and indirect illumination bydilated pupil until today
Case 2
A 39-year-old female patient the younger sister of case 1 presented in 1997 with very dense diffuse opacitieson the super 1047297cial layers mostly masquerading the para-central stromal lattice lines (Fig 2A) Her best visual acuityat this time was 630 in the right eye and 620 in the left eye
The diagnosis was LCD1 based on the clinical appearance of corneal opacities and on the family history She also had recurrent painful attacks due to epithelial erosions and slowly diminishing visual acuity for many years Her 16-year-old daughter showed very 1047297ne paracentral latticelines that were only visible by retroillumination (Fig 2B)A DNA analysis was performed Case 2 underwent PKP onher right eye in 1998 and on her left eye in 1999 without anyintraoperative or postoperative problems The follow-upconsisted of annual slit-lamp examination in direct and indi-rect illumination by dilated pupil because the patient is stillliving abroad
Case 3A 43-year-old female patient not related to cases 1
and 2 presented in 1996 with dense diffuse opacities on thesuper 1047297cial layers combined with paracentral stromal latticelines Her best visual acuity at this time was 620 in the right eye and 612 in the left eye The diagnosis was LCD1 based on the clinical appearance of corneal opacities and on thefamily history She had been suffering from visual impair-ment since the beginning of the second decade of life and had shown recurrent painful attacks due to epithelialerosions A DNA analysis was performed The patient underwent right PKP in 2000 without any intraoperative or
postoperative problems The follow-up consisted of irregular
slit-lamp examinations in direct and indirect illumination bydilated pupil because the patient lives far away from our of 1047297ces
RESULTS
The gene identi1047297cation of family 1 (cases 1 and 2)revealed a TGFBI Leu509Pro mutation In 2002 both graftsof case 1 were clear and the best visual acuity was 67 in theright eye and 68 in the left eye (Fig 1C) In 2005 1047297rst signsof recurrence could be observed in the left graft in the form of moderate diffuse super 1047297cial opacities of the central cornea In2008 1047297rst signs of recurrences could be observed in the right graft similar to those of the left eye No lattice lines were
revealed on either graft in direct and indirect illumination In2013 bilateral diffuse super 1047297cial opacities of the graft werevisible centrally and paracentrally (Fig 1D) No lattice linescould be observed The best visual acuity was 612 in theright eye and 624 in the left eye The beginning of the recur-rence was after 10 years on the right graft and after 8 years onthe left
In case 2 both grafts were clear in 2003 The best visualacuity was 66 in the right eye and 610 in the left eye becauseof a higher astigmatism In 2006 the right graft did not showany signs of recurrence However the left graft showed moderate diffuse super 1047297cial haze on the paracentral nasal area
FIGURE 1 Lattice corneal dystrophy type 1 (TGFBI Leu509Pro) A A 40-year-old male patient with diffuse opacities of the sub-epithelial cornea in direct illumination B The same eye showingparacentral stromal lattice lines in retroillumination C The sameeye 9 years after PKP revealing diffuse opacities but no latticelines on the graft
Lisch and Seitz Cornea Volume 33 Number 10 October 2014
1110 |
wwwcorneajrnlcom
2014 Lippincott Williams amp Wilkins
7262019 Cornea 2014 p1109
httpslidepdfcomreaderfullcornea-2014-p1109 34
of the graft No lattice lines were seen in direct and indirect illumination The best visual acuity was unchanged on bothand identical to that of 2003 In 2013 there were diffusecentral and paracentral opacities on the super 1047297cial layers of the graft on both eyes left more than right (Fig 2C) How-ever no lattice lines were visible on the graft but on the host
cornea in indirect illumination (Fig 2D) The best visualacuity was 675 right eye and 620 left eye The beginningof the recurrence was 7 years after PKP on the left graft and later on the right without exact determination
The gene identi1047297cation of case 3 (family 2) revealed a TGFBI Arg124Cys mutation In 2002 the graft on the right eye was clear The best visual acuity on the right was 68 In2004 the 1047297rst recurrence in the form of 1047297ne diffuse super 1047297cialhaze of the central cornea could be revealed The best visualacuity was the same as in 2002 In 2013 there were super 1047297cialdense but irregular diffuse opacities throughout the graft (Fig 3A) No lattice lines were revealed in direct and indirect illumination (Fig 3B) The best visual acuity was 630 The
beginning of the recurrence was 4 years after PKP
DISCUSSION
In 1979 Witschel and Sundmacher pointed out that granular corneal dystrophy and LCD1 may eventually evolveas primarily epithelial diseases78 In 1997 the TGFBI gene of LCD1 was identi1047297ed2 The most frequent mutation in LCD1is the Arg124Cys mutation To date many other independent mutations have been reported regarding LCD1 Recently wehave been able to 1047297nd a new Leu509Pro mutation regardingour second family The precise molecular functions of TGFBI in vivo are unknown but it has been proposed that it may act as a cell adhesion molecule and as a bifunctional linker pro-
tein interconnecting different matrix molecules to reach other cells The TGFBI gene is expressed above all by the cornealepithelial cells but also by the keratocytes9 It is a very impor-tant fact regarding the pathomorphology of the TGFBI cor-neal dystrophies that both epithelial cells and keratocytes areinvolved in the pathological process In LCD1 the diffuseopacities are located at the level of epitheliumsubepitheliumwhereas the lattice lines run through the whole stroma Bothopacity patterns start in the 1047297rst decade of life However wecan see a difference in the distribution of the 2 LCD1 opacity
patterns when the disease recurs after PKP Snead and Math-ews10 postulate that the reason for this difference may be that donor keratocytes survive long enough in the transplanted cornea to prevent building up of abnormal keratoepithelin
FIGURE 2 Lattice corneal dystrophy type 1 (TGFBI Leu509-Pro) A A 39-year-old female patient (sister of the patient of Fig 1) with dense superficial opacities mostly masqueradingthe stromal lattice lines (arrow) in direct illumination B A 16-
year-old daughter of (A) revealing fine paracentral lattice linesin retroillumination C The same eye as in (A) 15 years after PKP with diffuse opacities on the graft but without lattice linesin direct illumination D The same eye disclosing no latticelines on the graft but on the host cornea in retroillumination(arrow)
Cornea Volume 33 Number 10 October 2014 Lattice Corneal Dystrophy Type 1
2014 Lippincott Williams amp Wilkins wwwcorneajrnlcom
|
1111
7262019 Cornea 2014 p1109
httpslidepdfcomreaderfullcornea-2014-p1109 44
the product of the mutated gene in LCD1 By contrast theepithelium being replaced by host epithelium shortly after grafting is still producing abnormal protein The 1047297ndingssuggest different corneal cell types may repopulate at differ-ent speeds The repeat corneal grafts performed 24 years later on both eyes of Snead rsquos patient showed histologically exten-sive amyloid deposits between the epithelium and Bowman
layer10 There was relative sparing of the stroma in bothcorneas
The theory of differential expression based on the presence of host epithelial cells with a paucity of keratocytesseems to have validity but proof awaits better understandingof how keratocytes or 1047297 broblasts might form refractile lines in
the undisturbed dystrophy The theory could be further endorsed if there was evidence in reoperated grafts of thelocation of TGFBI in the epithelial cells as opposed tokeratocytes
The clinical and histological results of penetratingLCD1 grafts show together with the characteristics of theTGFBI gene that LCD1 represents not an isolated epithelial or isolated stromal dystrophy but a common epithelial ndash stromalentity This assessment has important clinical implicationsregarding the treatment of graft LCD1 recurrence performing
phototherapeutic keratectomy 1047297rst may postpone PKP
REFERENCES
1 Stone EM Mathers WD Rosenwasser GO et al Three autosomal dom-inant corneal dystrophies map to chromosome 5q Nat Genet 1994647 ndash 51
2 Munier FL Korvatska E Djemaiuml A et al Kerato-epithelin mutations infour 5q31-linked corneal dystrophies Nat Genet 199715247 ndash 251
3 Weiss JS Moslashller HU Lisch W et al The IC3D classi1047297cation of thecorneal dystrophies Cornea 200827(suppl 2)S1 ndash S83
4 Skonier J Neubauer M Madisen L et al cDNA cloning and sequenceanalysis of beta ig-h3 a novel gene induced in human adenocarcinomacell line after treatment with transforming growth factor-beta DNA Cell Biol 199211511 ndash 522
5 Klintworth GK Ferry AP Sugar A et al Recurrence of lattice cornealdystrophy type 1 in the corneal grafts of two siblings Am J Ophthalmol198294540 ndash 546
6 Meisler DM Fine M Recurrence of the clinical signs of lattice cornealdystrophy (type 1) in corneal transplants Am J Ophthalmol 198497210 ndash 214
7 Witschel H Sundmacher R Bilateral recurrence of granular cornealdystrophy in the grafts A clinic-pathological study Albrecht VonGraefes Arch Klin Exp Ophthalmol 1979209179 ndash 188
8 Witschel H Epithelial origin of ldquostromalrdquo corneal dystrophies ArchOphthalmol 2002120101 ndash 102
9 Wang MX Flattem NL Munier FL Molecular genetics of corneal dys-trophies In Wang MX ed Corneal Dystrophies and Degenerations(Chapter 1) American Academy of Ophthalmology New York Oxford University Press 2003161 ndash 17
10 Snead DRJ Mathews BN Differences in amyloid deposition in primaryand recurrent corneal lattice dystrophy type 1 Cornea 200221308 ndash 311
FIGURE 3 Lattice corneal dystrophy type 1 (TGFBI Arg124Cys) A A 60-year-old female patient with superficial irregular diffuse opacities on the graft 13 years after PKP in direct
illumination B The same eye showing no lattice lines on thegraft in retroillumination
Lisch and Seitz Cornea Volume 33 Number 10 October 2014
1112 |
wwwcorneajrnlcom
2014 Lippincott Williams amp Wilkins

7262019 Cornea 2014 p1109
httpslidepdfcomreaderfullcornea-2014-p1109 34
of the graft No lattice lines were seen in direct and indirect illumination The best visual acuity was unchanged on bothand identical to that of 2003 In 2013 there were diffusecentral and paracentral opacities on the super 1047297cial layers of the graft on both eyes left more than right (Fig 2C) How-ever no lattice lines were visible on the graft but on the host
cornea in indirect illumination (Fig 2D) The best visualacuity was 675 right eye and 620 left eye The beginningof the recurrence was 7 years after PKP on the left graft and later on the right without exact determination
The gene identi1047297cation of case 3 (family 2) revealed a TGFBI Arg124Cys mutation In 2002 the graft on the right eye was clear The best visual acuity on the right was 68 In2004 the 1047297rst recurrence in the form of 1047297ne diffuse super 1047297cialhaze of the central cornea could be revealed The best visualacuity was the same as in 2002 In 2013 there were super 1047297cialdense but irregular diffuse opacities throughout the graft (Fig 3A) No lattice lines were revealed in direct and indirect illumination (Fig 3B) The best visual acuity was 630 The
beginning of the recurrence was 4 years after PKP
DISCUSSION
In 1979 Witschel and Sundmacher pointed out that granular corneal dystrophy and LCD1 may eventually evolveas primarily epithelial diseases78 In 1997 the TGFBI gene of LCD1 was identi1047297ed2 The most frequent mutation in LCD1is the Arg124Cys mutation To date many other independent mutations have been reported regarding LCD1 Recently wehave been able to 1047297nd a new Leu509Pro mutation regardingour second family The precise molecular functions of TGFBI in vivo are unknown but it has been proposed that it may act as a cell adhesion molecule and as a bifunctional linker pro-
tein interconnecting different matrix molecules to reach other cells The TGFBI gene is expressed above all by the cornealepithelial cells but also by the keratocytes9 It is a very impor-tant fact regarding the pathomorphology of the TGFBI cor-neal dystrophies that both epithelial cells and keratocytes areinvolved in the pathological process In LCD1 the diffuseopacities are located at the level of epitheliumsubepitheliumwhereas the lattice lines run through the whole stroma Bothopacity patterns start in the 1047297rst decade of life However wecan see a difference in the distribution of the 2 LCD1 opacity
patterns when the disease recurs after PKP Snead and Math-ews10 postulate that the reason for this difference may be that donor keratocytes survive long enough in the transplanted cornea to prevent building up of abnormal keratoepithelin
FIGURE 2 Lattice corneal dystrophy type 1 (TGFBI Leu509-Pro) A A 39-year-old female patient (sister of the patient of Fig 1) with dense superficial opacities mostly masqueradingthe stromal lattice lines (arrow) in direct illumination B A 16-
year-old daughter of (A) revealing fine paracentral lattice linesin retroillumination C The same eye as in (A) 15 years after PKP with diffuse opacities on the graft but without lattice linesin direct illumination D The same eye disclosing no latticelines on the graft but on the host cornea in retroillumination(arrow)
Cornea Volume 33 Number 10 October 2014 Lattice Corneal Dystrophy Type 1
2014 Lippincott Williams amp Wilkins wwwcorneajrnlcom
|
1111
7262019 Cornea 2014 p1109
httpslidepdfcomreaderfullcornea-2014-p1109 44
the product of the mutated gene in LCD1 By contrast theepithelium being replaced by host epithelium shortly after grafting is still producing abnormal protein The 1047297ndingssuggest different corneal cell types may repopulate at differ-ent speeds The repeat corneal grafts performed 24 years later on both eyes of Snead rsquos patient showed histologically exten-sive amyloid deposits between the epithelium and Bowman
layer10 There was relative sparing of the stroma in bothcorneas
The theory of differential expression based on the presence of host epithelial cells with a paucity of keratocytesseems to have validity but proof awaits better understandingof how keratocytes or 1047297 broblasts might form refractile lines in
the undisturbed dystrophy The theory could be further endorsed if there was evidence in reoperated grafts of thelocation of TGFBI in the epithelial cells as opposed tokeratocytes
The clinical and histological results of penetratingLCD1 grafts show together with the characteristics of theTGFBI gene that LCD1 represents not an isolated epithelial or isolated stromal dystrophy but a common epithelial ndash stromalentity This assessment has important clinical implicationsregarding the treatment of graft LCD1 recurrence performing
phototherapeutic keratectomy 1047297rst may postpone PKP
REFERENCES
1 Stone EM Mathers WD Rosenwasser GO et al Three autosomal dom-inant corneal dystrophies map to chromosome 5q Nat Genet 1994647 ndash 51
2 Munier FL Korvatska E Djemaiuml A et al Kerato-epithelin mutations infour 5q31-linked corneal dystrophies Nat Genet 199715247 ndash 251
3 Weiss JS Moslashller HU Lisch W et al The IC3D classi1047297cation of thecorneal dystrophies Cornea 200827(suppl 2)S1 ndash S83
4 Skonier J Neubauer M Madisen L et al cDNA cloning and sequenceanalysis of beta ig-h3 a novel gene induced in human adenocarcinomacell line after treatment with transforming growth factor-beta DNA Cell Biol 199211511 ndash 522
5 Klintworth GK Ferry AP Sugar A et al Recurrence of lattice cornealdystrophy type 1 in the corneal grafts of two siblings Am J Ophthalmol198294540 ndash 546
6 Meisler DM Fine M Recurrence of the clinical signs of lattice cornealdystrophy (type 1) in corneal transplants Am J Ophthalmol 198497210 ndash 214
7 Witschel H Sundmacher R Bilateral recurrence of granular cornealdystrophy in the grafts A clinic-pathological study Albrecht VonGraefes Arch Klin Exp Ophthalmol 1979209179 ndash 188
8 Witschel H Epithelial origin of ldquostromalrdquo corneal dystrophies ArchOphthalmol 2002120101 ndash 102
9 Wang MX Flattem NL Munier FL Molecular genetics of corneal dys-trophies In Wang MX ed Corneal Dystrophies and Degenerations(Chapter 1) American Academy of Ophthalmology New York Oxford University Press 2003161 ndash 17
10 Snead DRJ Mathews BN Differences in amyloid deposition in primaryand recurrent corneal lattice dystrophy type 1 Cornea 200221308 ndash 311
FIGURE 3 Lattice corneal dystrophy type 1 (TGFBI Arg124Cys) A A 60-year-old female patient with superficial irregular diffuse opacities on the graft 13 years after PKP in direct
illumination B The same eye showing no lattice lines on thegraft in retroillumination
Lisch and Seitz Cornea Volume 33 Number 10 October 2014
1112 |
wwwcorneajrnlcom
2014 Lippincott Williams amp Wilkins

7262019 Cornea 2014 p1109
httpslidepdfcomreaderfullcornea-2014-p1109 44
the product of the mutated gene in LCD1 By contrast theepithelium being replaced by host epithelium shortly after grafting is still producing abnormal protein The 1047297ndingssuggest different corneal cell types may repopulate at differ-ent speeds The repeat corneal grafts performed 24 years later on both eyes of Snead rsquos patient showed histologically exten-sive amyloid deposits between the epithelium and Bowman
layer10 There was relative sparing of the stroma in bothcorneas
The theory of differential expression based on the presence of host epithelial cells with a paucity of keratocytesseems to have validity but proof awaits better understandingof how keratocytes or 1047297 broblasts might form refractile lines in
the undisturbed dystrophy The theory could be further endorsed if there was evidence in reoperated grafts of thelocation of TGFBI in the epithelial cells as opposed tokeratocytes
The clinical and histological results of penetratingLCD1 grafts show together with the characteristics of theTGFBI gene that LCD1 represents not an isolated epithelial or isolated stromal dystrophy but a common epithelial ndash stromalentity This assessment has important clinical implicationsregarding the treatment of graft LCD1 recurrence performing
phototherapeutic keratectomy 1047297rst may postpone PKP
REFERENCES
1 Stone EM Mathers WD Rosenwasser GO et al Three autosomal dom-inant corneal dystrophies map to chromosome 5q Nat Genet 1994647 ndash 51
2 Munier FL Korvatska E Djemaiuml A et al Kerato-epithelin mutations infour 5q31-linked corneal dystrophies Nat Genet 199715247 ndash 251
3 Weiss JS Moslashller HU Lisch W et al The IC3D classi1047297cation of thecorneal dystrophies Cornea 200827(suppl 2)S1 ndash S83
4 Skonier J Neubauer M Madisen L et al cDNA cloning and sequenceanalysis of beta ig-h3 a novel gene induced in human adenocarcinomacell line after treatment with transforming growth factor-beta DNA Cell Biol 199211511 ndash 522
5 Klintworth GK Ferry AP Sugar A et al Recurrence of lattice cornealdystrophy type 1 in the corneal grafts of two siblings Am J Ophthalmol198294540 ndash 546
6 Meisler DM Fine M Recurrence of the clinical signs of lattice cornealdystrophy (type 1) in corneal transplants Am J Ophthalmol 198497210 ndash 214
7 Witschel H Sundmacher R Bilateral recurrence of granular cornealdystrophy in the grafts A clinic-pathological study Albrecht VonGraefes Arch Klin Exp Ophthalmol 1979209179 ndash 188
8 Witschel H Epithelial origin of ldquostromalrdquo corneal dystrophies ArchOphthalmol 2002120101 ndash 102
9 Wang MX Flattem NL Munier FL Molecular genetics of corneal dys-trophies In Wang MX ed Corneal Dystrophies and Degenerations(Chapter 1) American Academy of Ophthalmology New York Oxford University Press 2003161 ndash 17
10 Snead DRJ Mathews BN Differences in amyloid deposition in primaryand recurrent corneal lattice dystrophy type 1 Cornea 200221308 ndash 311
FIGURE 3 Lattice corneal dystrophy type 1 (TGFBI Arg124Cys) A A 60-year-old female patient with superficial irregular diffuse opacities on the graft 13 years after PKP in direct
illumination B The same eye showing no lattice lines on thegraft in retroillumination
Lisch and Seitz Cornea Volume 33 Number 10 October 2014
1112 |
wwwcorneajrnlcom
2014 Lippincott Williams amp Wilkins