Embed Size (px)
Citation preview

9/22/2014
1
Making Correct Decisions: Accurate Diagnosis and
Appropriate Test Selection
Chad Cook PT, PhD, MBA, FAAOMPTProfessor
Vice Chief of Research Duke University
Question 1
• 1. Please PICK ONLY ONE of the following choices. Pick the most appropriate choice recommendation based on the signs and symptoms of the patient. – a. Plain film radiograph of the low back
(flexion-extension views) – b. Magnetic Resonance Image of the low
back– c. Plain film radiograph of the pelvis – d. None
Question 2
• 2. Please PICK ONLY ONE of the following choices. Pick the most appropriate recommended medication choice based on the signs and symptoms of the patient. – a. Non-Steroidal Anti-Inflammatory – b. Tricyclic Anti-Depressant– c. Corticosteroid (Dose pack)– d. Short term Narcotic derivative – e. None
Question 3
• 3. Please PICK ONLY ONE of the following choices. Pick the most appropriate self-care option based on the signs and symptoms of the patient. – a. Advice to decrease activity since it
diminishes his current symptoms– b. Advice to remain active – c. Advice to perform unsupervised general
exercises such as Yoga– d. None
Question 4• 4. Please PICK ONLY ONE of the following
choices. If the patient was treated for 1 month with no improvement or worsening in the present signs or symptoms, which of the following selections is most appropriate for this patient. – a. Refer for Imaging consultation – b. Refer for Surgical consultation– c. Another round of conservative therapy– d. Recommend heavier dosages of
medication
9/22/2014
2
Course Outline• 1. Part One-The Decision Making Process• 2. Part Two-Errors and Decision Making• 3. Part Three-System 1 and System 2 Thinking• 4. Part Four-System 1 Strengths and Weaknesses• 5. Part Five-System II Thinking: Analytical Decision
Making• 6. Part Six- Which are considered the best tests for
diagnosis?• 7. Part Seven-Decision Making without a Diagnosis
Part One: The Decision Making
Process
8
Differential Diagnosis
• Differential diagnosis is a systematic process used to identify the proper diagnosis from a competing set of possible diagnoses.
• Diagnosis is one of many necessary components during the clinical decision making process
Diagnostic Process?
• The Diagnostic process involves identifying or determining the etiology of a disease or condition through evaluation of patient history, physical examination, and review of laboratory data or diagnostic imaging; and the subsequent descriptive title of that finding
Whiting et al. J Health Serv Res 2008
What’s the Best Way to Differentially Diagnosis is to use a
“Process”
• A couple of thoughts– Use a dedicated strategy– Understand the metrics of certain findings– Never rely too heavily on a single measure– Realize that diagnosis is a “process” not an
“event”
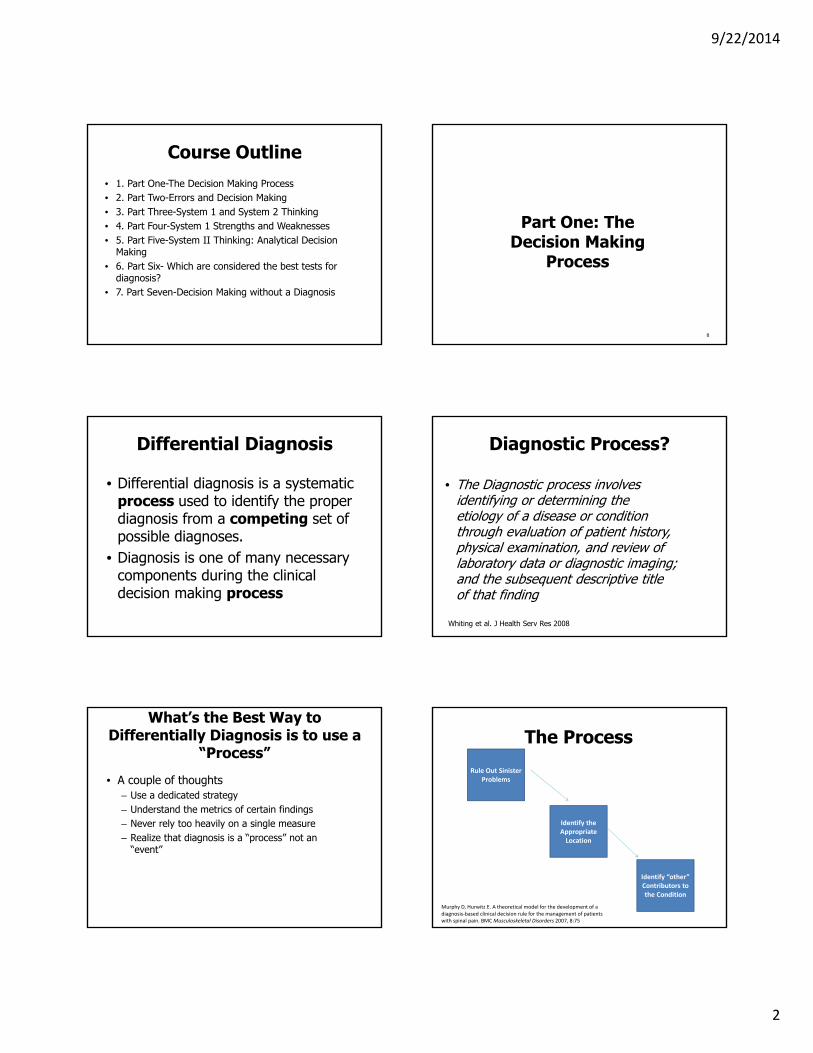
The Process
Rule Out Sinister Problems
Identify the Appropriate Location
Identify “other” Contributors to the Condition
Murphy D, Hurwitz E. A theoretical model for the development of a diagnosis‐based clinical decision rule for the management of patients with spinal pain. BMC Musculoskeletal Disorders 2007, 8:75

9/22/2014
3
Three Diagnostic Questions when Addressing a Patient
• The first question of diagnosis: Are the patient's symptoms reflective of a visceral disorder or a serious or potentially life-threatening illness?
• The second question of diagnosis: From where is the patient's pain arising?
• The third question of diagnosis: What has gone wrong with this person as a whole that would cause the pain experience to develop and persist?
Murphy D, Hurwitz E. A theoretical model for the development of a diagnosis-based clinical decision rule for the management of patients with spinal pain. BMC Musculoskeletal Disorders 2007, 8:75
Early Stages of Diagnosis
• Specific to the necessity for accuracy, is the ability to differentiate patients with symptoms that arise from non-mechanical disorders or other potentially life threatening pathology
• Tests will require high levels of sensitivity, low LR-, and reasonable reliability
Rubinstein SD, van Tulder M. A best-evidence review of diagnostic procedures for neck And low back pain. Best Practice & Research Clinical Rheum. 2008;22:471-482.
Proper Tests
• Well’s Criteria• Canadian C Spine rules• Ottawa Knee and Ankle
Rules• PERC score• Ankle Brachial Index• San Francisco Syncope Rule• CPR for myelopathy
15
Part Two of the Process
• The second question of diagnosis: From where is the patient's pain arising?
Three Possible Parameters
Ruling out a Location
Ruling in a Location (but not knowing the
diagnosis)
Confirming a Diagnosis
Ruling Out Location?
• Using tests with high sensitivity (or overpressures) to rule out a body part region as a contributor– (e.g., Using Neer’s test to rule
out the shoulder; Using a straight leg raise to rule out a disc problem; using an overpressure to the cervical spine to rule out the c-spine as a contributor)
Proper Tests
• Neers• Straight Leg Raise• Hawkins Kennedy Test• Clark’s Test for the Patella• Overpressure of movement• Palpation
18

9/22/2014
4
Ruling in a Location (but not knowing the diagnosis)
• Symptoms are Isolated to a Region
• This is Where it Gets Murky– Nonspecific low back pain– Internal Derangement of the
knee– Neck pain– Degenerative knee problems– Impingement syndrome
Confirming a Known Diagnosis
• Requires high specificity, reasonable sensitivity and a high LR+ (more on that later)
• Examples?– ACL tear– Herniated Nucleus Pulposis– Ulnar Ligament Instability
Does Imaging Fit in Here Somewhere?
• Yes, in that it can confirm some conditions were struggle to identify
• No in that it is overused • Lumbar imaging for low-back pain without indications
of serious underlying conditions does not improve clinical outcomes. Therefore, clinicians should refrain from routine, immediate lumbar imaging in patients with acute or subacute low-back pain and without features suggesting a serious underlying condition
Chou R, Fu R, Carrino JA, Deyo RA. Imaging strategies for low-back pain: a systematic review and metanalysis. Lancet. 2009;373:463-72.
Proper Tests
• Maximal Mouth Opening• Drop Arm Sign• External Rotation Lag
Sign• Reflex Testing (for hyper
or hypo-reflexia)
22
Thus for Physical Tests
Intake Patient History Observation Triage Movement Palpation/Exam MMT/Endurance Confirmatory Tests Tests
R/OHigh Sensitivity
Low LR‐
R/IHigh Specificity
High LR+
Part Three of the Process
• What has gone wrong with this person as a whole that would cause the pain experience to develop and persist?
• The social, psychosocial, and socioeconomic contextual elements

9/22/2014
5
Such As…
• Depression• Anxiety• Motivation• Litigation• Chronicity• Household Income• Habits
• Somatic perceptions• Coping Behaviors• Fear Avoidance
Behaviors• Perceptions• Employment Status• Job environment
da Costa BR, Vieira ER. Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies. Am J Ind Med. 2010;53:285-323.
Part Two: Errors in Decision Making
(Part 1) Differential Diagnosis
• Differential diagnosis is a systematic process used to identify the proper diagnosis from a competing set of possible diagnoses.
• Diagnosis is one of many necessary components during the clinical decision making process
Diagnostic Process?
• The Diagnostic process involves identifying or determining the etiology of a disease or condition through evaluation of patient history, physical examination, and review of laboratory data or diagnostic imaging; and the subsequent descriptive title of that finding
Whiting et al. J Health Serv Res 2008
Who Performs Diagnoses?
• Anyone who treats patients
• Certainly, physical therapists
PT’s and Diagnosis
• “Physical Therapists thus must establish diagnostic categories that direct their treatment prescriptions and that provide a means of communication both within the profession and with other practitioners and consumers about the conditions that require their particular expertise for effective treatment and prognostication”
Sahrmann S. Diagnosis by the physical therapist: A prerequisite for treatment. PhysTher. 1988;68:1703-6.
1988
9/22/2014
6
Now more than Ever?
• Mean physician visit duration (elderly 19.2 minutes) (Elderly and non-elderly 20.4)
• 8-10 minutes with the actual physician
• Patients are now more complex
Mechanic et al. Are Patients' Office Visits with Physicians Getting Shorter? NEJM. 2001; 344:198-204
Why it’s Important
• Failure to correctly identify an appropriate diagnosis can lead to: – Negative outcomes (Trowbridge
2008). – Delays in appropriate treatment
(Whiting et al. 2008)– Unnecessary healthcare costs
(Dohrenend and Skillings)
Can Lead to Death• 44,000 to 98,000
Americans die annually as a result of all medical errors (1999).
• 80,000 to 160,000 Americans die annually as a result of DIAGNOSTIC errors (2013).
Institute of Medicine. To err is human: building a safer health system. Kohn, Corrigan, and Donaldson (ed). Washington DC. National Academies Press, 1999Newman-Toker et al. BMJ Quality and Safety
Most Common Types and Locations?
• Most in physician offices (primary care 31%, medical specialty 21%)
• Error types: Diagnostic 36%, surgical 24%, non-surgical procedures 14%, medications 13%
Woods DM, Thomas EJ, Holl J. Ambulatory care adverse events and preventable adverse events leading to hospital admission. Qual SafHealth Care 2007;16;127-131
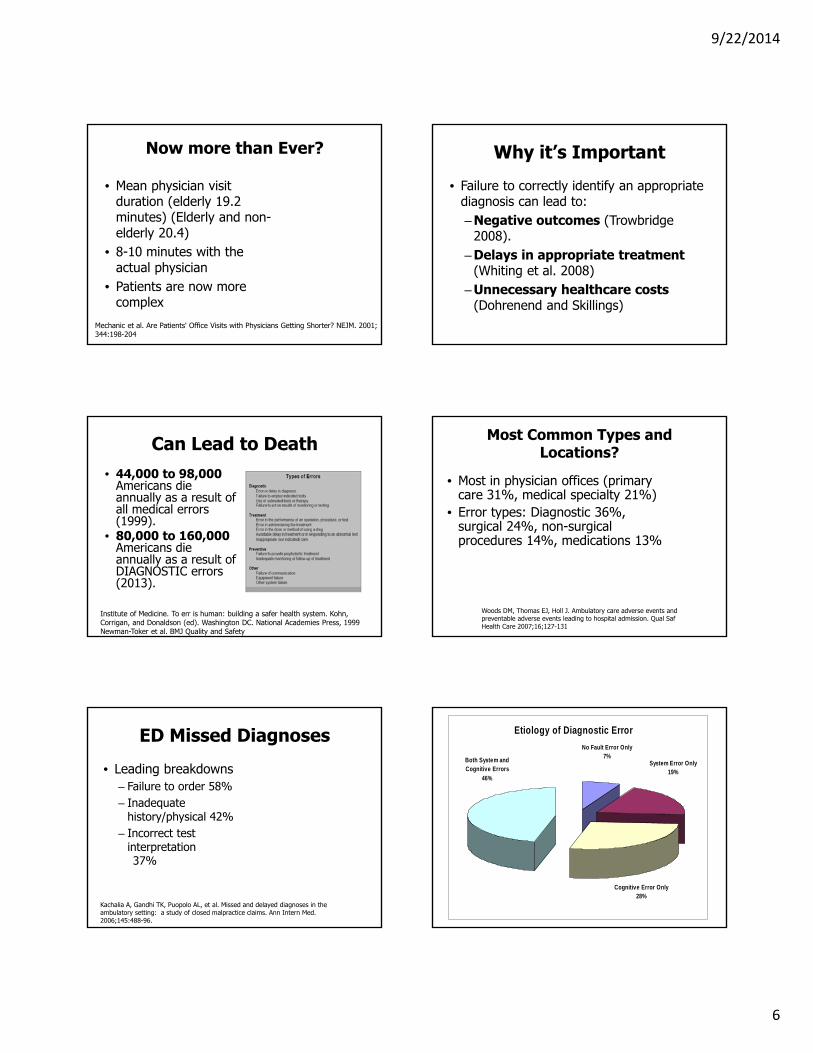
ED Missed Diagnoses
• Leading breakdowns– Failure to order 58%– Inadequate
history/physical 42%– Incorrect test
interpretation37%
Kachalia A, Gandhi TK, Puopolo AL, et al. Missed and delayed diagnoses in the ambulatory setting: a study of closed malpractice claims. Ann Intern Med. 2006;145:488-96.
Etiology of Diagnostic Error
Both System and Cognitive Errors
46%
Cognitive Error Only28%
System Error Only19%
No Fault Error Only7%

9/22/2014
7
Cognitive Errors:
Faulty Synthesis 83 %
Faulty Knowledge
3 %
Faulty Data Gathering
14 %
Diagnostic Errors• Of 350,706 paid claims, diagnostic errors were the
leading type (28.6 percent) and accounted for the highest proportion of total payments (35.2 percent).
• Diagnostic errors resulted in death or disability almost twice as often as other error categories.
• More diagnostic error claims were rooted in outpatient care than inpatient care, (68.8 percent vs. 31.2 percent) but inpatient diagnostic errors were more likely to be lethal (48.4 percent vs. 36.9 percent).
Newman‐Toker et al. BMJ Quality and Safety
Diagnosis vs. Treatment
Wilson R, Harrison B, Gibberd R, et al. An analysis of the causes of adverse events from the Quality in Australian Health Care Study. MJA 1999; 170: 411-415
• 34.8% resulted in permanent disability• 86.5% of diagnostic delays were highly preventable
Difficult, but Preventable
• Acting on Insufficient Information*– (81% High
Preventability)• Misapplication of, or
failure to apply a rule or use a bad or inadequate rule– (90.3% High
Preventability)
Wilson R, Harrison B, Gibberd R, et al. An analysis of the causes of adverse events from the Quality in Australian Health Care Study. MJA 1999; 170: 411-415
Healthcare Costs
• 50 to 53 million US dollars per million members, per year for a medical misdiagnosis.
• 6.1 to 10.4 billion dollars (adjusted) annually (for diagnostic errors)
Medical Misdiagnosis: Overlooked opportunity for meaningful health plan improvement of quality and costs. Managed Care Outlook. 2008;21(8).Institute of Medicine. To err is human: building a safer health system. Kohn, Corrigan, and Donaldson (ed). Washington DC. National Academies Press, 1999,
Malpractice Claims (Added Costs)
National Practitioner Data Bank,” BMJ Quality & Safety,
9/22/2014
8
Costs associated with Too Many Lab Tests and Imaging
• “Incorrect diagnoses may lead to incorrect and ineffective treatment or unnecessary testing, which is costly and sometimes invasive”
Reducing Errors in Health Care: Translating Research Into Practice. AHRQ Publication No. 00-PO58, April 2000. Agency for Healthcare Research and Quality, Rockville, MD. http://www.ahrq.gov/qual/errors.htm
Kerry et al. Br J Gen Pract. 2002;52:469-74.
Referral for lumbar spine radiography for first presentation of low back pain in primary care is not associated with improved physical functioning, pain or disability.
Cost Utility Analysis
• An interdisciplinary early intervention treatment model was the preferred option in over 85% of the samples within the an established range of acceptable costs.
• (most of these interventions are underutilized because of physician concerns of cost and applicability)
• Rogerson, Gatchel, & Bierner. Pain Pract. 2010;Apr 5.
Our Decisions don’t Routinely Kill People
• We are more guilty of delaying care and being an unnecessary cost
• Scare tactics are still used
Only Physicians?
• < 5% of Primary Care Physicians Routinely Examine for Red Flags during an Initial Screen
• Bishop & Wing. Spine J. 2006: 6:282-8.
• “Low rates of compliance for the assessment and documentation of yellow and red flags”
• Walsh et al. Occup Med. 2008;58:485-9.
Orthopedic Surgeons?
• “Both orthopedic surgeons and family physicians’ knowledge of treating LBP is deficient.”
• “Orthopedic surgeons are less aware of current treatment than family practitioners”
• Finestone et al. Spine. 2009;34:1600-3.

9/22/2014
9
Direct Access for Physical Therapy
• 8 articles were included. • Statistically significant and clinically
meaningful findings across studies that satisfaction and outcomes were superior, and numbers of PT visits, imaging ordered, medications prescribed, and additional non-physical therapy appointments were less in cohorts receiving PT by direct access compared with referred episodes of care.
• There was no evidence for harm.
Ojha et al. Direct access compared with referred physical therapy episodes of care: a systematic review. Phys Ther. 2014 Jan;94(1):14‐30.
Missed Diagnoses
ArchInternMed.2009;169(20):1881‐1887
While the exact prevalence of diagnostic error remains un known, data from autopsy series spanning several decades conservatively andconsistently reveal error rates of 10% to 15%
Matcher D. Chapter 1: Introduction to the Methods Guide for Medical Test Reviews. J Gen Intern Med 27(Suppl 1):S4–10
This Course
• It’s about thinking smarter
• It’s about knowing how to make better decisions
Part Three: System 1 and System 2
Thinking
54

9/22/2014
10
Dual Processing Theory
• A Careful Balance of Intuitive (Automatic) and Analytical Thoughts
Marcum JA. An integrated model of clinical reasoning: dual‐process theory of cognition and metacognition. J Eval Clin Pract.2012 Oct;18(5):954‐61.
Automatic (Intuitive) Versus Analytical
• System 1 operates automatically and quickly, with little or no effort and no sense of voluntary control”
• “System 2 allocates attention to the effortful mental activities that demand it, including complex computations”
Norman G, Monteiro S, Sherbino J Is clinical cognition binary or continuous? Acad Med. 2013 Aug;88(8):1058‐60.
Dual Processing Theory • System 1: ‘Intuitive, automatic, fast, frugal and
effortless’ process,– Involves construction of mental maps and patterns,
shortcuts and rules of thumb (heuristics), and ‘mind-lines’.
– Developed through experience and repetition, seeing what other people do, talking to local colleagues and personal experience.
• System 2: Involves a careful, rational analysis and evaluation of the available information. – This is effortful and time consuming. – Analytical and logical.
Croskerry P. A universal model of diagnostic reasoning. Acad Med. 2009 Aug; 84(8):1022‐8.Croskerry P. Context is everything or how could I have been that stupid? Healthc Q. 2009; 12 Spec No Patient():e171‐6.
Dual Processing Theory for Clinicians
• Clinical reasoning begins with system 1 processes in which the clinician assesses a patient's presenting symptoms, as well as other clinical evidence, to arrive at a differential diagnosis.
• Additional clinical evidence, if necessary, is acquired and analysed utilizing system 2 processes to assess the differential diagnosis, until a clinical decision is made diagnosing the patient's illness and then how best to proceed therapeutically
Marcum JA. An integrated model of clinical reasoning: dual‐process theory of cognition and metacognition. J Eval Clin Pract. 2012 Oct;18(5):954‐61.
System 1 Thinking (Nutshell)
• Designed to jump to conclusions form little evidence-is not designed to know the size of the jumps (Kahneman 2011)– Involves – Fast, – Automatic, – Frequent, – Emotional, – Stereotypic, – Subconscious designs
System 1 Uses Good, Quality Experiences
• Talented, well-trained clinicians make faster and better decisions.
• Factual knowledge appears to be more important than years of emergency nursing or triage experience in triage decision accuracy.
Considine J, Botti M, Thomas S Do knowledge and experience have specific roles in triage decision‐making? Acad Emerg Med. 2007 Aug;14(8):722‐6.

9/22/2014
11
Heurism• In Medicine, System 1
theory is influenced by expertise and is often called Heurism
• Heurism is knowledge derived from empirical study and practical adoption of experience (Klein J, BMJ, 2005)
• Fast and Frugal Decision Making
Heuristic Decision Making• Making quick decisions
without complete information
• Allows one to make judgments quickly.
• A frugal heuristic relies on a small fraction of the available evidence in making judgments (think ER setting).
Inductive Reasoning
• Inductive reasoning progresses from observations of individual cases to the development of a generality.
• Inductive reasoning, or induction, is the process by which a general conclusion is reached from evaluating specific observations or situations.
System 2 Thinking (Nutshell)
• Slow, • Effortful, • Infrequent, • Logical, • Calculating, • Conscious
Hypothetical Deductive Reasoning
• Proceeded by formulating a hypothesis that can be falsified by a test on observable data.
• A test that could and does run contrary to predictions of the hypothesis is taken as a falsification of the hypothesis.
• A test that could but does not run contrary to the hypothesis corroborates the hypothesis.
The Use of “Rules” or “Guidelines”

9/22/2014
12
Part Four: System 1 Strengths and Weaknesses
68
Discussion of Patient Case One
System 1 Thinking
• Designed to jump to conclusions form little evidence-is not designed to know the size of the jumps (Kahneman 2011)– Involves – Fast, – Automatic, – Frequent, – Emotional, – Stereotypic, – Subconscious designs
How Does One Obtain “Fast-Automatic” Decisions?
• Training– Depth and breadth of prior experience
• Expertise• Efficiency
– Patient Centered• Goal Oriented/Distinct view of role
– How data are used• Collaborative• Structured pattern to the decision making
model
Training
• Physical Therapy Education (CAPTE Data and Study)– Stronger academic
background and work experience
• Residency Training• Fellowship

9/22/2014
13
Expertise?
• Involves key characteristics• (1) a dynamic, multidimensional knowledge
base that is patient-centered and evolves through therapist reflection,
• (2) a clinical reasoning process that is embedded in a collaborative, problem-solving venture with the patient,
• (3) a central focus on movement assessment linked to patient function,
• (4) consistent virtues seen in caring and commitment to patients.
Jensen et al. Expert practice in physical therapy
Efficacy
• Less information was needed to make appropriate decisions
• Recognition of patterns in the care planning
• More “useful” time spent in the patient care process
• Better understanding of prognoses
Goal Oriented/Distinct View of Role
• Has ability to build and convince patient of the relationships and roles
• Knows what they want to get done
• Knows how to target useful information– Care planning – Triage and deference of
care to others
Collaborative
• Delegation• Ability to use others’ knowledge• Learning from mentors• In an environment of learning• Wherever smart people work, doors
are unlocked– Steve Wozniak
Expertise Learned through a Structured Pattern
• You miss fewer things• It is a moderator to all the other
elements we discussed• Doesn’t mean it’s needed forever
but it build the patterns
10,000 Hours Concept
• Simon and Chase’s observation—and researchers, time and again, reached the same conclusion: it takes a lot of practice to be good at complex tasks.
• Practice creates Programming
HA Simon, WG Chase ‐ Skill in chess: Experiments with chess‐playing tasks and computer simulation of skilled performance throw light on some human perceptual and memory processes American scientist, 1973

9/22/2014
14
Simple Examples of Knowledge through Programming
• 3 + 3 =• Bread and ………• Fruit Salad, ……. …….• Four score and ……..• The hills are alive ………• There once was a man from
Nantucket…..
Physical Therapists Can Determine Patient Prognosis at
Baseline• Dagfinrud H, Storheim K, Magnussen LH, et al. The predictive
validity of the Örebro Musculoskeletal Pain Questionnaire and the clinicians' prognostic assessment following manual therapy treatment of patients with LBP and neck pain. Man Ther. 2013;18(2):124-9.
• Abbott JH, Kingan EM. Accuracy of physical therapists' prognosis of low back pain from the clinical examination: a prospective cohort study. J Man Manip Ther. 2014;22:154–61.
• Hancock MJ, Maher CG, Latimer J, Herbert RD, McAuley JH. Can rate of recovery be predicted in patients with acute low back pain? Development of a clinical prediction rule. Eur J Pain. 2009 Jan;13(1):51-5.
• Cook C, Moore TJ, Learman K, Showalter C, Snodgrass S. Can Experienced Physiotherapists Identify Who Are Likely to Succeed with Physical Therapy Treatment? In Review.
System 1 Allows for Quick Accurate Discrimination
• The ability to understand when something is not consistent
• The ability to understand when subtle differences in context
• The ability to understand and classify in the absence of complex information
System 1 Allows you to Make Quick, Smart Decisions based
on Intuition
• Allows individuals to identify risk ands recognize negative consequences
• Allows clinicians to understand situations of potential harm
System 1 Allows for Fast and Frugal Decisions
• Able to process decisions even in the absence of complete information
Experience Influences use of System I
• Speed is an indicator of confidence• Comprehensiveness is also related to
Feeling of Rightness (FOR) judgments to conditional inferences and base rate problems,
• Fluency predicted the amount of deliberate processing as measured by thinking time and answer changes
Thompson et al. The role of answer fluency and perceptual fluency as metacognitive cues for initiating analytic thinking. Cognition. 2013 Aug;128(2):237‐51.
9/22/2014
15
System 1: Cognitive Biases• Characterized as the tendency to make
decisions and take action based on limited acquisition and/or processing of information or on self-interest, overconfidence, or attachment to past experience.
• Cognitive biases can result in perceptual blindness or distortion (seeing things that aren’t really there), illogical interpretation (being nonsensical), inaccurate judgments (being just plain wrong), irrationality (being out of touch with reality), and bad decisions.
drjimtaylor.com/2.0/business/cognitive‐biases‐are‐bad‐for‐business/
Bias is Subconscious-The Mind is Imperfect
• The functions associated with choice in particular are often “conducted prior to and independent of any conscious direction” (Heuer, 1999, p. 3). What spontaneously appears in our consciousness at the end of cognition is the product, not the process, of thinking. We often choose without understanding or accounting for the perceptions, intuitions, and inferences that underlie our decisions.
• Two types– Information Biases– Ego Biases
Heuer, R. (1999). Psychology of intelligence analysis. Washington: Center for the Study of Intelligence, Central Intelligence Agency.
Information Biases
• Information biases include the use of heuristics, or information-processing shortcuts, that produce fast and efficient, though occasionally inaccurate, decisions
• Priming• Context Bias• Mental Short Cuts
Driven By Priming Agents
• Such as our Experiences and Our responses to those experiences
• A good priming experience will reduce the effect of a negative finding
• A bad priming experience will reduce the effect of a positive finding
System 1 is Context Specific
The Brain will try to Organize things in the way it thinks
should be
9/22/2014
16
Ego Biases
• Ego biases include emotional motivations and social influences such as peer pressure, the desire for acceptance, and doubt that other people are as right as you are.
• Emotions• Social Influences• Arrogance (example of death
because of a machine vs. doctor)
System 1 Theory has an Emotional Component that
Drives Responses
• Emotions stimulate automatic, quick responses
• Caring is an emotion
System 1 is Driven by Stereotypes or Assumptions
• Harvard Implicit Racism Test
• Overall, despite one’s race there are inherent “preferences” toward specific races
Gender Implicit Bias Test
Arrogance• Which is most acceptable?• A regional expert physician’s protocol was able to
save the lives of 17% of children which Klotchman’s Disease who were identified within a span of 3 months. The previous life expectancy percentage was only 8%
• A computer algorithm used at Mercy Memorial in New York missed 78% of the children with Klotchman’s Disease. This resulted in the deaths of nearly 8 of out 10 children when identified within a span of 3 months. No previous algorithm was used.
How do you Improve System 1 Thinking?
• Training (good training)
• Reflection• Built in Systems
(Checks and Balances)
9/22/2014
17
Does it Work?• A default system of cognitive processes (System 1) is
responsible for cognitive biases that lead to diagnostic errors and that System 2 intervenes to correct these errors.
• The best strategy for reducing errors is to make students aware of the biases and to encourage them to rely more on System 2. However, an accumulation of evidence suggests that (a) strategies directed at increasing analytical (System 2) processing, by slowing down, reducing distractions, paying conscious attention, and (b) strategies directed at making students aware of the effect of cognitive biases, have marginal on error rates.
Monteiro SM, Norman G. Diagnostic Reasoning: Where We've Been, Where We're Going. Teach Learn Med. 2013;25 Suppl 1:S26‐32.
A Checklist for Diagnosis
Obtain YOUR OWN history Perform a focused, purposeful exam Take a “Diagnostic Time Out”Was I comprehensive ? Did I consider the inherent shortcomings
of using my intuition (heuristics) ?Was my judgment affected by bias ?Do I need to make the diagnosis now or
can it wait ?What’s the worst case scenario?
Embark on the plan, but ENSURE FOLLOW-UP & FEEDBACK
Part Five: System II Thinking
Analytical Decision Making (for Diagnosis)
System 2 Thinking (Nutshell)
• Slow, • Effortful • Infrequent • Logical • Calculating • Conscious
It’s Slower
• It can be more challenging (you have to remember the best tools)
• It can be more deliberate (if you use computers or other decision making devices)
• It fits some individuals more than others
More Focus: More Effort
• “System 2 allocates attention to the effortful mental activities that demand it, including complex computations”

9/22/2014
18
Are You Married? (Engaged/Relationship?)
• You have 3 minutes• Write down why you continue to be
attracted to your spouse/partner
• Go!
For Diagnosis, There are Analytic Metrics
• Diagnostic accuracy– Diagnostic accuracy
relates to the ability of a test to discriminate between the target condition and health.
Diagnostic Test Metrics
• Reliability• Sensitivity• Specificity• Positive and Negative Predictive Value• Positive and Negative Likelihood Ratios• Knowing “Good” diagnostic tests can
improve both System 1 and System 2 thinking!
106
Does Reliability Matter?
The condition
is fatal
No worries, you will be fine
www.zillowblog.com
Sensitivity and Specificity
• Sensitivity: Percentage of people who test positive for a specific disease among a group of people who have the disease
• Specificity: Percentage of people who test negative for a specific disease among a group of people who do not have the disease
Sensitivity Example• 50 patients with arm pain
associated with cervical radiculopathy
• Test was positive in 40 of the 50 cases
• Sensitivity = 40/50 or 80%
• Correct 80% of the time in cases that were cervical radiculopathy
http://www.triggerpointbook.com/infrasp2.gif
9/22/2014
19
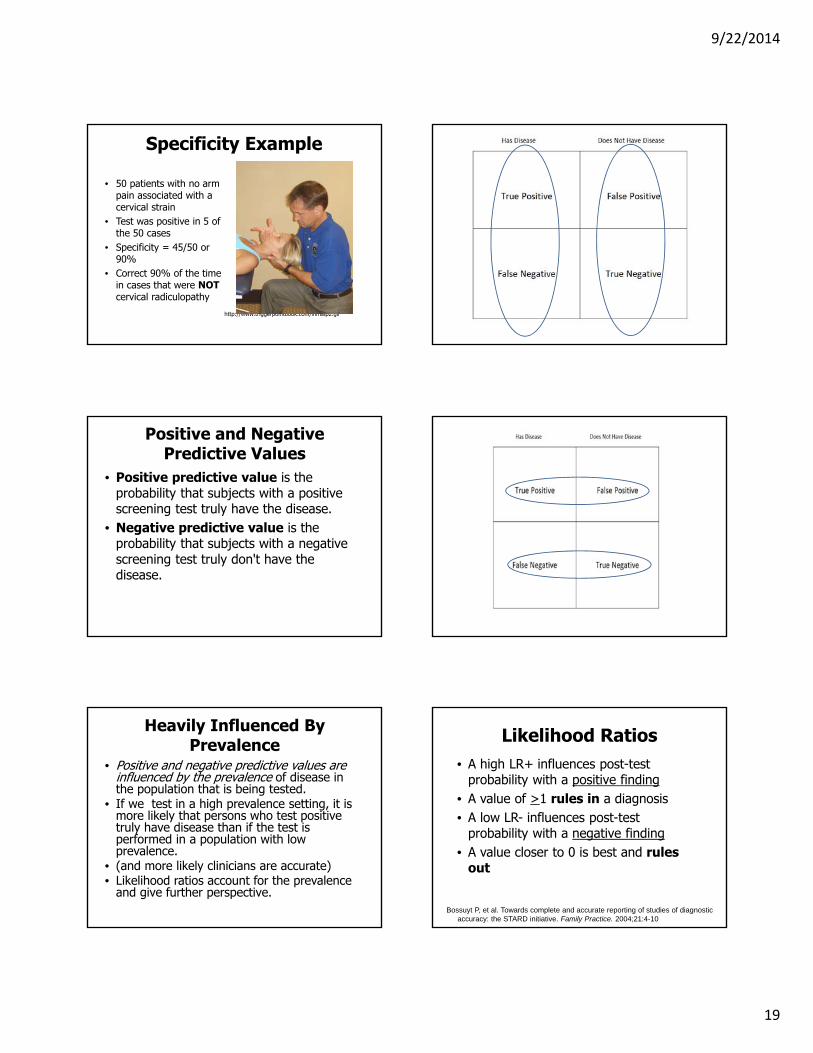
Specificity Example
• 50 patients with no arm pain associated with a cervical strain
• Test was positive in 5 of the 50 cases
• Specificity = 45/50 or 90%
• Correct 90% of the time in cases that were NOTcervical radiculopathy
http://www.triggerpointbook.com/infrasp2.gif
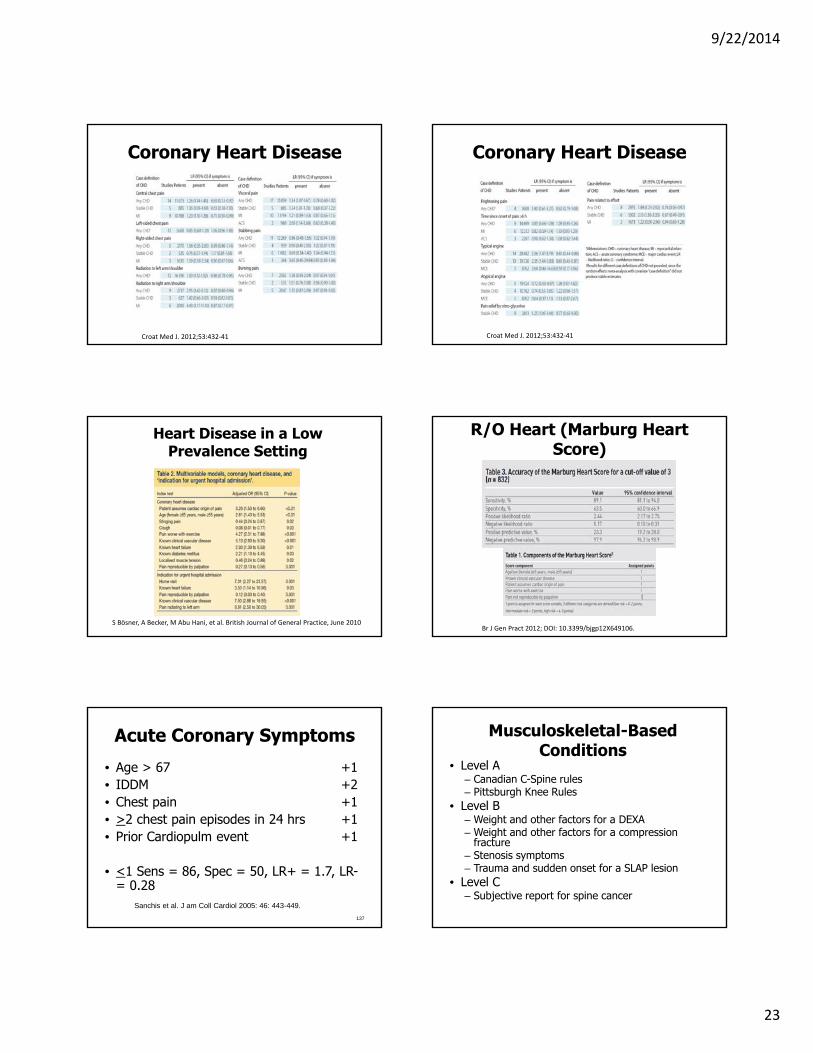
Positive and Negative Predictive Values
• Positive predictive value is the probability that subjects with a positive screening test truly have the disease.
• Negative predictive value is the probability that subjects with a negative screening test truly don't have the disease.
Heavily Influenced By Prevalence
• Positive and negative predictive values are influenced by the prevalence of disease in the population that is being tested.
• If we test in a high prevalence setting, it is more likely that persons who test positive truly have disease than if the test is performed in a population with low prevalence.
• (and more likely clinicians are accurate)• Likelihood ratios account for the prevalence
and give further perspective.
Likelihood Ratios• A high LR+ influences post-test
probability with a positive finding• A value of >1 rules in a diagnosis • A low LR- influences post-test
probability with a negative finding• A value closer to 0 is best and rules
out
Bossuyt P, et al. Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative. Family Practice. 2004;21:4-10.

9/22/2014
20
For the Math Geeks
• Positive Likelihood Ratio= (sensitivity)/(1-specificity)
• Negative Likelihood Ratio= (1-sensitivity)/(specificity)
Sound Internal Metrics
• Reliability, Sensitivity, and Specificity are measures of a tests internal metrics
• They are independent of the population of interest subjected to the test.
Lalken AG, McCluskey A. Contin Educ Anaesth Crit Care Pain (2008) 8 (6): 221‐223.
Clinical Utility
• The ability of the metrics to influence post-test probability (either in ruling out the condition or ruling it in)
• Or just improving your likelihood of being correct
Fagen’s Nomogram(LR+)
• Cervical Radic• Pretest
prob=18%• Spurling’s
LR+=4.8• Post test prob
of a positive finding= 52%
Fagen’s Nomogram(LR-)
• Cervical Radic• Pretest
prob=18%• ULTT (LR- =
0.14)• Post test prob
of a negative finding = 2.98%
Confidence Intervals?
• Wainner’s CPR for CTS
• 34% pre-test prob• <4/5 of the tests• LR+ = 4.6 (95%CI
2.5, 8.7)• Post-test
probability = 70% (56.3%, 81.7%)
•

9/22/2014
21
121
Influencing Decision Making
Cook C. Orthopedic Manual Therapy. An Evidence Based Approach. Prentice Hall; Upper Saddle River, NJ: 2007.
Summary
• Internal Test Metrics
• Sensitivity• Specificity
• External Decision Making Influence
• Positive Likelihood ratio
• Negative Likelihood ratio
Improving your knowledge of test metrics can improve both System 1 and System 2 decision making
Analytics Tend to Do Best in Highly Complex Decision
Making Situations
Because the Environment Influences Results
• This is a significant limitation of using predictive values and/or post-test probabilities.
• Each pair of predictive values or post-test probabilities is associated with a single pre-test probability. Changing the pre-test probability changes the predictive value in non-linear ways (remember, we use the complicated, non-linear Bayes formula to calculate the post-test probability of disease).
• The same test result may therefore give you one post-test probability in the emergency room, and a different one in your office, if the pre-test probabilities differ.
125
Because Tests Should be Used in Proper Order
• Some tests should typically be used early– E.g., SLR, ULTT,
Hawkins Kennedy,
• Some late in the examination– Spurlings, Hoffmann’s
test, Well leg Raise
OTHERWISE YOUR RESULTS WILL BE BIASED
• Chad add Matcher’s work here Table

9/22/2014
22
Part Six: Which are considered the best tests
for diagnosis (Medical, Neuro, and Ortho)?
127
Best Tests, Based on What?
• Evidence• Appropriate
Design• Quality• Metrics• Decision Making
Power
128
Guidelines
• No fatal flaws in design• LR+ of 5.0 or higher• LR- of 0.2 or lower• Sensitivity of .90 or higher• QUADAS of 10 or higher• A test that matters
129
Patient History/Subjective Examination
Heart Related Conditions
• Level A– Various clinical findings
• Level B– Marburg heart score
9/22/2014
23
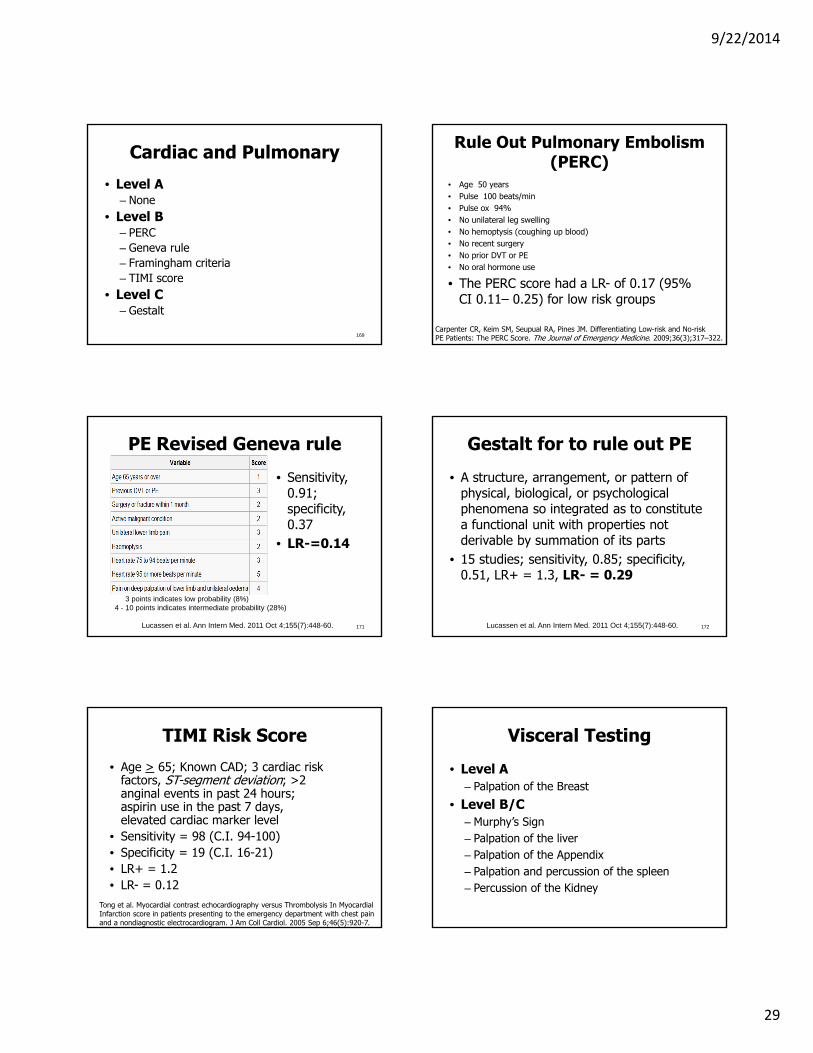
Coronary Heart Disease
Croat Med J. 2012;53:432‐41
Coronary Heart Disease
Croat Med J. 2012;53:432‐41
Heart Disease in a Low Prevalence Setting
S Bösner, A Becker, M Abu Hani, et al. British Journal of General Practice, June 2010
R/O Heart (Marburg Heart Score)
Br J Gen Pract 2012; DOI: 10.3399/bjgp12X649106.
Acute Coronary Symptoms
• Age > 67 +1• IDDM +2• Chest pain +1• >2 chest pain episodes in 24 hrs +1• Prior Cardiopulm event +1
• <1 Sens = 86, Spec = 50, LR+ = 1.7, LR-= 0.28
137
Sanchis et al. J am Coll Cardiol 2005: 46: 443-449.
Musculoskeletal-Based Conditions
• Level A– Canadian C-Spine rules– Pittsburgh Knee Rules
• Level B– Weight and other factors for a DEXA– Weight and other factors for a compression
fracture– Stenosis symptoms– Trauma and sudden onset for a SLAP lesion
• Level C– Subjective report for spine cancer

9/22/2014
24
139
Canadian C-Spine Rules
Sensitivity = 99
Stiell et al. Canadian CT head rule study for patients with minor head injury: methodology for phase II (validation and economic analysis). Ann Emerg Med. 2001;38(3):317-22.
Cervical Closed Fracture
140
Cook CE, Sizer PS, Isaacs RE, Wright A. Pain Pract. 2013 Apr 23. doi: 10.1111/papr.12061. [Epub ahead of print]
Clinical Examination in Cervical Spine
Injuries in Awake and Alert Blunt Trauma Patients
• The sensitivity and specificity of the clinical examination were 80% and 73.98%
Hussian et al. Asian Spine Journal. 2011;5, No. 1, pp 10~14, 142
Spine Cancer• History sensitivity specificity
– Age > 50 0.77 0.71– previous history 0.31 0.98
of cancer– failure to improve 0.31 0.90
in 1 mo. of therapy– no relief -bed rest >0.90 0.46– duration > 1 mo 0.50 0.81– age >50 or cancer hx or 1.00 0.60
unexplained wt loss or failure of conservative tx.
Deyo RA, Jarvik JG. Diagnostic evaluation of low back pain with emphasis on imaging. Ann Intern Med. 2002;137:586-97.
Spine Malignancy
Henschke N, Maher CG, Ostelo RWJG, de Vet HCW, Macaskill P, Irwig L. Red flags to screen for malignancy in patients with low‐back pain. Cochrane Database of Systematic Reviews 2013, Issue 2. Art. No.: CD008686. DOI:10.1002/14651858.CD008686.pub2.
Spine Malignancy
Henschke N, Maher CG, Ostelo RWJG, de Vet HCW, Macaskill P, Irwig L. Red flags to screen for malignancy in patients with low‐back pain. Cochrane Database of Systematic Reviews 2013, Issue 2. Art. No.: CD008686. DOI:10.1002/14651858.CD008686.pub2.

9/22/2014
25
145
Ankylosing Spondylitis
• History sensitivity specificity– age at onset <40 1.00 0.07– pain not relieved by supine 0.80 0.49– morning back stiffness 0.64 0.59– pain duration >3 months 0.71 0.54– 4 of 5 questions above positive 0.23 0.82
also: improved by exercise
+LR = 1.27
Deyo RA, Jarvik JG. Diagnostic evaluation of low back pain with emphasis on imaging. Ann Intern Med. 2002;137:586-97.
Who Needs a DEXA
• (Weight in KG – age in years) X 0.2
• Example (115 pound women (52 KG) who is 67 years of age) Value = -3
• OST = < -1 a DEXA is recommended
146
SCORE test for a DEXA
– Patient is not black +5– Patient has RA +4– Hx of fracture from minor trauma– +4 for each fracture up to 12 0-12– Estrogen therapy (never) +1– Weight in LBs divided by 10
• > 6 a DEXA is recommended
147
Vertebral Compression Fracture
• Female sex• Age >70 years• Significant trauma• Prolonged use of corticosteroids • 1 of 4 Sens = 88, Spec = 50, LR+ = 1.8• 3 of 4 Sens = 38, Spec = 100, LR+ = 218
Henschke et al. Prevalence of and screening for serious spinal pathology in patients presenting to primary care settings with acute low back pain.Arthritis Rheum. 2009 Oct;60(10):3072-80.
Compression Fracture
Clustered ResultsSensitivity
(95% CI)
Specificity (95%
CI)
PositiveLikelihood Ratio
(95% CI)
NegativeLikelihood
Ratio (95% CI)
1 of 5 positive tests .97 (.89-.99) .06 (.06-.07) 1.04 (.92-1.1) 0.39 (0.07-2.1)
2 of 5 positive tests .95 (.83-.99) .34 (.33–.34) 1.4 (1.3-1.8) 0.16 (0.04-.51)
3 of 5 positive tests .76 (.61-.87) .68 (.68-.69) 2.5 (1.9-2.8) 0.34 (.19-.46)
4 of 5 positive tests .37 (.24-.51) .96 (.95-.97) 9.6 (3.7-14.9) 0.65 (0.50-0.79)
5 of 5 positive tests .03 (.01-.08) .99 (.98-.99) 9.3 (1.4-60.2) 0.97 (0.92-0.99)
NOTE. Five findings are included in the rule: (1) age > 52 years; (2) no presence of leg pain; (3) body mass index < 22; (4) does not exercise regularly; and (5) female gender.
Roman M, Brown C, Richardson W, Isaacs R, Howes C, Cook C. The development of a clinical decision making algorithm for detection of osteoporotic vertebral compression fracture or wedge deformity. JMMT 2010;81:45-50. 150
Lumbar Compression fracture
• History sensitivity specificity– age >50 0.84 0.61– age >70 0.22 0.96– trauma 0.30 0.85– corticosteroid use 0.06 0.995
– in elderly trauma can be minor
Deyo RA, Jarvik JG. Diagnostic evaluation of low back pain with emphasis on imaging. Ann Intern Med. 2002;137:586-97..

9/22/2014
26
151
Stenosis (N=1448) Cook et al.Clustered Results
Sensitivity (95% CI)
Specificity (95% CI)
LR+ (95% CI) LR- (95% CI)Posttest Prob of CTS (%)
1 of 5 positive tests
.96 (.94-.97) .20 (.19-21) 1.2 (1.1-1.2)0.19 (0.12-
0.29)44
2 of 5 positive tests
.68 (.65-.71) .62 (.60–.64) 1.8 (1.6-2.0) 0.51 (0.45-.58)
55
3 of 5 positive tests
.29 (.27-.31) .88 (.87–.90) 2.5 (2.0-3.1)0.80
(.76-.85) 63
4 of 5 positive tests
.06 (.05-.07) 98 (.98-.99) 4.6 (2.4-8.9)0.95
(0.94-0.97)76
5 of 5 positive tests
<.01 (.001-.003)
1.0 (.99-1.0) Inf (.77-Inf)0.99 (0.99-
1.0)99+
Five findings are included in the rule: (1) Bilateral symptoms; (2) Leg pain more than back pain; (3) Pain during walking/standing; (4) pain relief upon sitting; and (5) age >48 years. Pretest probability of 40.3%. 152
ICD-10 Criteria for Concussion• Require a history of TBI and the presence of
three or more of the following eight symptoms:
• 1) headache,• 2) dizziness, • 3) fatigue, • 4) irritability, • 5) insomnia, • 6) concentration• 7) memory difficulty, • 8) intolerance of stress, emotion, or alcohol.
World Health Organization: The ICD-10 Classification of Mental and BehaviouralDisorders: Clinical Descriptions and Diagnostic Guidelines. Geneva, World Health Organization, 1992
ICD-10 Criteria for Concussion
• Optimal threshold of 5 symptoms present• Sens = 72.7, Spec = 61, LR+ = 1.9, LR- =
0.45• To assess delayed recovery or
Postconcussion syndrome (PCS) symptoms
153Kashluba S, Casey JE, Paniak C. J Int Neuropsychol Soc. 2006 Jan;12(1):111
Type I SLAP lesion
Michener et al. Journal of Athletic Training 2011:46(4):343–348
Type II-IV SLAP lesion
Michener et al. Journal of Athletic Training 2011:46(4):343–348
Acromioclavicular Joint
Cadogan et al. BMC Musculoskeletal Disorders 2013, 14:156

9/22/2014
27
157
Pittsburgh (Knee) Rule(s)
Sn = .99
Sp = .60
+LR = 2.48
-- LR = .025 !Seaberg DC, Yealy DM, Lukens T, Auble T, Mathias S. Multicenter comparison of two clinical decision rules for the use of radiography in acute, high-risk knee injuries. Ann Emerg Med 1998;32:8-13
A knee radiograph is indicated when:
1.There is a history of fall or blunt trauma and at least one of the following:
+2. Patient age more than 50
or less than 12 years 3. Inability to bear weight for
four steps at the time of injury and when examined
Criteria for the Pittsburgh Knee Rule
ACL
Wakemakers et al. Arch Phys Med Rehabil 2010;91:1452‐9.
Knee Meniscus Injury
Yan et al. Swiss Med Wkly. 2011;141:w13314
Best Tests for Medical Screening
160
Influenza
• Level 1– None
• Level 2– Myalgia– Fever– Cough
Flu Models, 1, 2, and 3
Ebell et al. J Am Board Fam Med 2012;25:55– 62.

9/22/2014
28
Flu Models 4 and 5
Ebell et al. J Am Board Fam Med 2012;25:55– 62.
Fall Risks
• Level A– None
• Level B– Fall Risk for Hospitalization– Fall Risk for Peripheral Neuropathy– Fall Risk Post Stroke– Fall Risk in a nursing Home
164
Fall Risk (Hospitalization)• St. Thomas Risk Assessment
Tool in Falling elderly inpatients
165
Meta-analysisSN = 67SP = 57LR+ = 1.56LR-= 0.57
17 studies
Billington et al. BMC Fam Pract2012:13:76
Fall Risk Peripheral Neuropathy
• Dynamic Gait Index cut of <22 – Sens=90, Spec=84.6, LR+ =5.9,
LR- = 0.10
• Timed up and Go cut of >10.7 seconds– Sens=90, Spec=88.5, LR+ =7.8,
LR- = 0.10
166Jernigan et al. Phys Ther. 2012
Fall Risk-Post Stroke (Community)
• 12 month, multiple or injurious falls post stroke (LEAPS trial)
• Berg Balance Scale score ≤ 42/56 • Sensitivity =73% Specificity=53%,
LR+ =1.53, LR- = 0.51
167Tilson et al. Stroke. 2012; 43:446-452.
Fall Risk in Nursing Home
• Staff judgment of fall risk and Presence of previous falls (remembered)
• Sensitivity varied from 65% to 72%, Specificity from 69% to 75%
168Bentzen et al. Aging Clin Exp Res. 2011 Jun;23(3):187-95.
9/22/2014
29
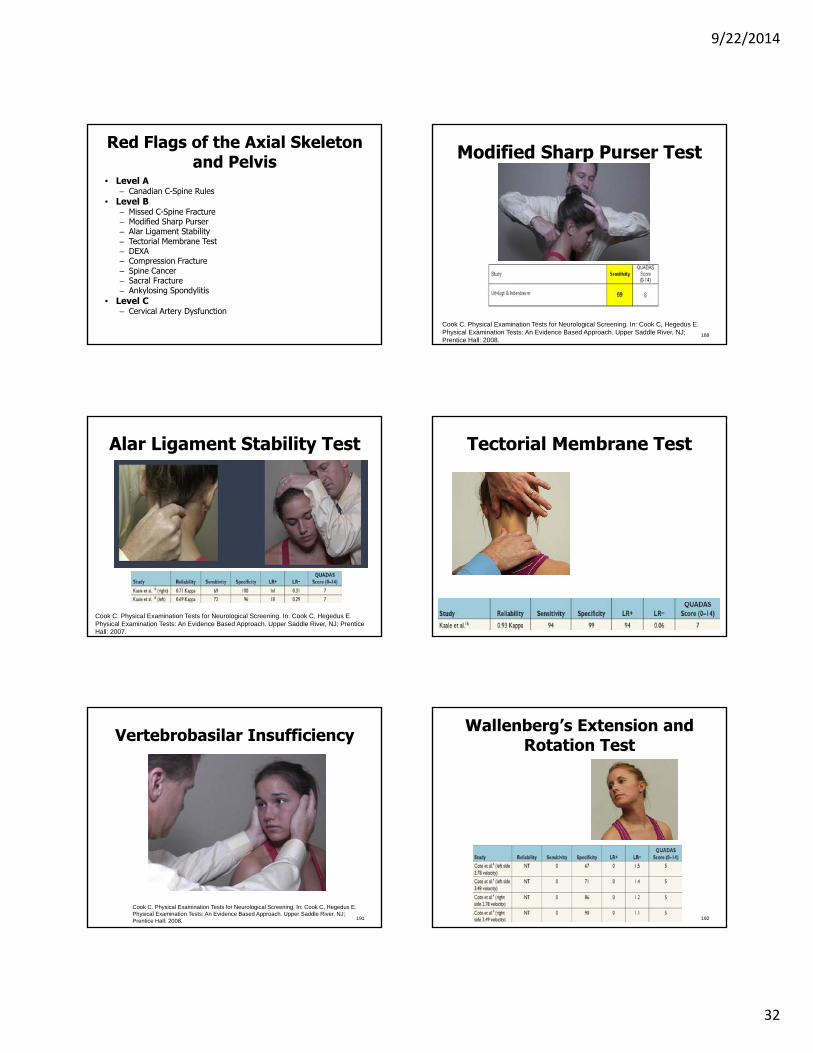
Cardiac and Pulmonary
• Level A– None
• Level B– PERC– Geneva rule– Framingham criteria– TIMI score
• Level C– Gestalt
169
Rule Out Pulmonary Embolism (PERC)
• Age 50 years• Pulse 100 beats/min• Pulse ox 94%• No unilateral leg swelling• No hemoptysis (coughing up blood)• No recent surgery• No prior DVT or PE• No oral hormone use
• The PERC score had a LR- of 0.17 (95% CI 0.11– 0.25) for low risk groups
Carpenter CR, Keim SM, Seupual RA, Pines JM. Differentiating Low-risk and No-risk PE Patients: The PERC Score. The Journal of Emergency Medicine. 2009;36(3);317–322.
PE Revised Geneva rule
• Sensitivity, 0.91; specificity, 0.37
• LR-=0.14
171
0 - 3 points indicates low probability (8%)4 - 10 points indicates intermediate probability (28%)11 points or more indicates high probability (74%)
Lucassen et al. Ann Intern Med. 2011 Oct 4;155(7):448-60.
Gestalt for to rule out PE
• A structure, arrangement, or pattern of physical, biological, or psychological phenomena so integrated as to constitute a functional unit with properties not derivable by summation of its parts
• 15 studies; sensitivity, 0.85; specificity, 0.51, LR+ = 1.3, LR- = 0.29
172Lucassen et al. Ann Intern Med. 2011 Oct 4;155(7):448-60.
TIMI Risk Score
• Age > 65; Known CAD; 3 cardiac risk factors, ST-segment deviation; >2 anginal events in past 24 hours; aspirin use in the past 7 days, elevated cardiac marker level
• Sensitivity = 98 (C.I. 94-100)• Specificity = 19 (C.I. 16-21)• LR+ = 1.2• LR- = 0.12
Tong et al. Myocardial contrast echocardiography versus Thrombolysis In Myocardial Infarction score in patients presenting to the emergency department with chest pain and a nondiagnostic electrocardiogram. J Am Coll Cardiol. 2005 Sep 6;46(5):920-7.
Visceral Testing
• Level A– Palpation of the Breast
• Level B/C– Murphy’s Sign– Palpation of the liver– Palpation of the Appendix– Palpation and percussion of the spleen– Percussion of the Kidney

9/22/2014
30
175
Visceral Referred Pain Clinical Breast Examination (Cancer) Initial Screen
176
Test Values
Palpatory Breast Exam
Mammogram
CBE + Mammogram
SN 26.7 90.1 94.9
SP 98 95.4 93.7
LR+ 13.3 18 15.1
LR‐ 0.74 0.10 0.05
Chiarelli et al. J Natl Cancer Inst. 2009 Sep 16;101(18):1236-43.
Conclusion
• Annual mammography in women aged 40-59 does not reduce mortality from breast cancer beyond that of physical examination or usual care when adjuvant therapy for breast cancer is freely available.
• Overall, 22% (106/484) of screen detected invasive breast cancers were over-diagnosed, representing one over-diagnosed breast cancer for every 424 women who received mammography screening in the trial.
Murphy’s Sign for Cholecystitis
• Sensitivity = 97• Specificity = 48• LR+ = 1.9• LR- = .06
179
Singer et al. Ann Emerg Med. 1996;28:267-272.
Acute Abdominal Pain
180Laurell et al. Scand J Gastroenterol. 2006 Oct;41(10):1126-31.

9/22/2014
31
Palpation Liver
181
Palpation Aorta
182
Palpation Appendix
183
Nixon’s Percussion Spleen
184
Palpation and Middleton’s Man
• Barkun et al. Sens = 46, Spec = 97, LR+ = 15.3, LR- = 0.56.
185
Kidney Palpation/Percussion
9/22/2014
32
Red Flags of the Axial Skeleton and Pelvis
• Level A– Canadian C-Spine Rules
• Level B– Missed C-Spine Fracture– Modified Sharp Purser– Alar Ligament Stability– Tectorial Membrane Test– DEXA– Compression Fracture– Spine Cancer– Sacral Fracture– Ankylosing Spondylitis
• Level C– Cervical Artery Dysfunction
188
Modified Sharp Purser Test
Cook C. Physical Examination Tests for Neurological Screening. In: Cook C, Hegedus E.Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008.
Alar Ligament Stability Test
Cook C. Physical Examination Tests for Neurological Screening. In: Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
Tectorial Membrane Test
190
191
Vertebrobasilar Insufficiency
Cook C. Physical Examination Tests for Neurological Screening. In: Cook C, Hegedus E.Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008.
Wallenberg’s Extension and Rotation Test
192

9/22/2014
33
Other CAD Symptoms
• Other potential symptoms associated with VBI are: (1) visual disturbances (diplopia), (2) auditory phenomena (sudden sensorineural hearing loss), (3) facial numbness or paresthesias, (4) dysphagia, (5) dysarthria, and (6) syncope (drop attacks).
193Sizer, Brismee, Cook. Pain Practice. 2007;7:53-71 194
Non-Mechanical, Meta-Static Pain
• Pain that cannot be produced, changed, or reduced during your mechanical examination.
• Pain that has an origin outside our practice capabilities.
http://images.craveonline.com/article_imgs/Image/arthritis_pain.jpg
Non-Mechanical Spinal Pain
Cook C, Ross MD, Isaacs R, Hegedus E. Investigation of Nonmechanical Findings during Spinal Movement Screening for Identifying and/or Ruling Out Metastatic Cancer. Pain Pract. 2011 Nov 22. [Epub ahead of print].
Non-Mechanical Pain-Cont.
Cook C, Ross MD, Isaacs R, Hegedus E. Investigation of Nonmechanical Findings during Spinal Movement Screening for Identifying and/or Ruling Out Metastatic Cancer. Pain Pract. 2011 Nov 22. [Epub ahead of print]
197
Ruling Out Pelvic Fractures(Negative findings of)
• Trauma +– Posterior Inflammation
(sacral ala fracture)– Pain with Hip ROM– Pain during rectal
examination– Pain during
compression
Sauerland et al. (2004) Reliability of clinical examination in detecting pelvic fractures In blunt trauma patients: a meta-analysis. Arch Orthop Trauma Surg. 124:123-128.
Clinical Examination-Sacral Fracture
• CE SN = 96.4, SP =50.25 • XRAY SN=79.2, SP =99.7• CE findings age (OR, 1.025), hip pain (OR,
4.971) internal rotation of the leg (OR, 4.880), tenderness to palpation over the sacrum (OR, 2,297) tenderness over the right or left hip (OR, 3.626) diffuse pain throughout the pelvis (OR, 16.445)
198Duane et al. Am Surg. 2008 Jun;74(6):476-9; discussion 479-80.

9/22/2014
34
Red Flags of the Upper Quarter
• Level A– None
• Level B– Upper extremity DVT– Elbow Fracture– Clavicular Fracture (Auscultation)
Upper Extremity DVT• Sens = 96; Spec = 48, LR+ = 1.5; LR- = 0.12
• 1 The presence of venous material (catheter, venous access, or pacemaker) 1
• 2 Upper extremity, unilateral pitting edema 1• 3 Localized upper extremity pain 1• 4 Another diagnosis is reasonably plausible −1
– Scoring is as follows: score ≤ 0 low risk for DVT; score = 1
intermediate risk; and score ≥ 2 =higher risk for UEDVT
200Constans et al. Thromb Haemost. 2008;99:202-207.
201
Shoulder (upper Arm) Specific Red Flags
• Category I Findings– Paget-Schroetter
Syndrome
Hegedus E, Cooper L, Cook C. Differential diagnosis of a female weight lifter with Paget’s Schroetter Syndrome. J OrthopSports Phys Ther. 2006;36:882-6.
Clavicular or Humeral Fracture
202
Bony Apprehension Test
• Abduct the arm then ER
• + Test is apprehension
203
Elbow Extension Test
• Sensitivity=100 • Specificity=100 • LR+ =NA • LR-=NA

9/22/2014
35
Elbow Supination Test
• Sensitivity=43• Specificity= 97 • LR+ =14.3 • LR- =0.58
Joshi et al. ACADEMIC EMERGENCY MEDICINE 2013; 20:1–15
Red Flags of the Lower Quarter
• Level A– Pubic Percussion Test– Ottawa Knee Rules– Pittsburgh Knee Rules– Ottawa Ankle Rules– Wells Criteria for DVT– Auscultation of the Fibula– Ankle/Brachial Index
• Level B– Hip Flexion test– Infection with a total joint replacement
208
Ruling Out Hip Fractures(Negative findings of)
• + Pubic Percussion Test (LR+ = 9 to 313)
• ER of one limb versus the other
Reiman MP, Goode AP, Hegedus EJ, Cook CE, Wright AA. Diagnostic accuracy of clinical tests of the hip: a systematic review with meta-analysis. Br J Sports Med. 2012 Jul 7.
209
Hip Flexion Test
• Sensitivity = 90, LR-= 0.10
• Helps rule out presence of a pelvis fracture
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008. 210
Clinical Findings for Infection in THR
Type Acute Subacute Later Stages
Pain 100% 100% 96%
Swelling 100% ? 77%
High WBC ? 100% 27%
Drainage 100% ? 27%
Fever 100% ? ?
Windsor et al JBJS; 1990

9/22/2014
36
211
Ottawa Knee RulesCriteria for the Ottawa Knee Rule
A knee x-ray is indicated after trauma only and when at least one of the following is present:
1. Patient age > 55 2. Isolated tenderness of the patella 3. Tenderness over the fibular head 4. Inability to flex the knee to 90°5. Inability to bear weight for four
steps at the time of injury and when examined
Sn = 1.0 !
Sp = .49
+LR = 1.96
-- LR = .11 !Jackson et al, Annals Int Med, 2003
212
Deep Vein Thrombosis Clinical Exam
213
The Problem:
• “Overall, no single sign or symptom can be used to predict the presence of DVT”-Dunn & McGinn, J Amer Ger Soc, March 2002
• The majority of patients with venous thromboembolism will have no symptoms-Stuart & Bussey, AJHP, January 1997
214
History
215
Combining History with Exam:The Wells et al Clinical Tool-DVT
Wells et al. JAMA 2006
Clinical Variable Score Active cancer (treatment ongoing or within previous 6 months or palliative) 1 Paralysis, paresis, or recent plaster immobilization of the lower extremities 1 Recently bedridden for 3 days or more, or major surgery within the previous 12 weeks requiring general or regional anesthesia 1 Localized tenderness along the distribution of the deep venous system 1 Entire leg swelling 1 Calf swelling at least 3 cm larger than that on the asymptomatic leg (measured 10 cm below the tibial tuberosity)† 1 Pitting edema confined to the symptomatic leg 1 Collateral superficial veins (nonvaricose) 1 Previously documented DVT 1 Alternative diagnosis at least as likely as DVT −2 TOTAL
216
Pre-test Probability of a DVT
Score Probability of a DVT
< 0 LOW
1-2 MODERATE
> 3 HIGH
9/22/2014
37
Fracture of the Fibula
217 218
Sn = 1.0 for Foot Fx and Ankle Fx Sp = .50 ankle, .77 foot: Steill et al, JAMA, 1994
Ankle-Brachial Index• Assessment of
Peripheral Vascular Disease
• Lower ratio suggests blockage in leg
• Measure blood pressure at the ankle and at the arm (Systolic) while a person is at rest.
• Ankle / Arm Guo et al. Sensitivity and Specificity of Ankle-Brachial Index for Detecting AngiographicStenosis of Peripheral Arteries. Circ J 2008; 72: 605 –610
Ankle-Brachial Index• Normal: 0.9 to 1.3. • Abnormal: Less than 0.9 is abnormal.
Sensitivity = 76, Specificity = 90, LR+ = 7.6
• If the ABI is:– 0.41 to 0.9, you likely have mild to
moderate peripheral arterial disease.
– 0.4 or below, you likely have severe peripheral arterial disease.
Guo et al. Sensitivity and Specificity of Ankle-Brachial Index for Detecting AngiographicStenosis of Peripheral Arteries. Circ J 2008; 72: 605 –610
Best Tests for Neurological Screening
Neurological Testing
• Level A– Straight Leg Raise (*)
• Level B– Protracted recovery from concussion– Monohemispheric tumor testing– Syncope– Myelopathic testing– Cervical Radiculopathy testing– Cauda Equina Testing

9/22/2014
38
Protracted Concussion Recovery
• Overall, 80% sensitivity for IMPaCT for Protracted recovery – Migraine symptom cluster 18 or greater – Cognitive symptom cluster 19 or greater – Visual memory 46 or less– Processing speed 23.46 or less
223Lau et al. Neurosurgery. 2012 Feb;70(2):371-9; discussion 379.
Finger Tap Test Monohemispheric Dysfunction-
Tumor• Sens = 73.3• Spec = 87.5• LR+ = 5.9• LR- = 0.31• Tap the tip of the
index finger to the IP joint of the thumb as many time as possible in 10 seconds
224Teitelbaum et al. Can J Neurol Sci. 2002;29:337-44.
Pronator Drift Test Monohemispheric Dysfunction-
Tumor
• Sens = 92.2• Spec = 90• LR+ = 9.2• LR- = 0.09• Palms up, elbow
extended (pronation drift is positive finding)
225Teitelbaum et al. Can J Neurol Sci. 2002;29:337-44.
Finger Rolling Test-Monohemispheric Dysfunction-
Tumor
• Sensitivity =41• Specificity=93 • LR+ =5.86 • LR-=0.63
Maranhao et al. J Neurologic Phys Ther. 2010;34:145-49.
Finger Rolling Test-Monohemispheric Dysfunction-
Tumor
• Sensitivity=16 • Specificity=100• LR+= Inf • LR- =0.84
Maranhao et al. J Neurologic Phys Ther. 2010;34:145-49. 228

9/22/2014
39
San Francisco Syncope Rule• Identifies patients with serious short
term adverse outcomes after partial or complete loss of consciousness with interruption of awareness of oneself and ones surroundings
• Abnormal ECG, a complaint of shortness of breath, hematocrit less than 30%, systolic blood pressure less than 90 mm Hg, or a history of CHF
• Sensitivity = 96%• Specificity = 62% LR+ = 2.52, LR- =
0.06
Quinn et al. Derivation of the San Francisco Syncope Rule to predict patients with short-term serious outcomes. Ann Emerg Med. 2004 Feb;43(2):224-32.
230
Myelopathy Tests Reliability•
• κ• < 0 No agreement• 0.0 — 0.20 Very low agreement• 0.21 — 0.40 Low agreement• 0.41 — 0.60 Moderate agreement• 0.61 — 0.80 full agreement• 0.81 — 1.00 Almost perfect agreement
• Hoffmann's test= Kappa = 0.73 (% agreement = 0.88) (95% CI= .54-.92) SE=0.096 p<0.01
• Deep Tendon reflexes =Kappa=0.76 (%agreement=0.88) (95%CI=0.56-.93) SE=0.09 p<0.01
• Inverted suppinator sign =Kappa=0.56 (%agreement=0.78) (95%CI=.35-.77) SE=0.11 p<0.01
• Suprapatellar Quads (Isaacs Sign)=Kappa=0.65 (%agreement=0.83) (95% CI=.46-.84) SE=0.1 p<0.01
• Hand withdrawal =Kappa=0.59 (%agreement=.8) (95%CI=.38-.79) SE=0.11 p<0.01
• Babinski = Kappa=0.57 (%agreement=.92) (95%CI=.25-.89) SE=0.16 p<0.05
• Clonus = Kappa = 0.79 (%agreement=.98) (95%CI=.39-.99) SE=0.20 p<0.01
Cook et al. Diagnostic accuracy of tests for myelopathy. JOSPT 2009.
231
Hoffmann’s Test
Cook C. Physical Examination Tests for Neurological Screening. In: Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008.
232
Inverted Suppinator Sign
• Look for finger flexion and elbow extension
• Cook et al. Sensitivity = 67
• Most sensitive tool for CSM available
Cook et al. Reliability and Diagnostic Accuracy of Clinical Special Tests for Myelopathy in Patients seen for Cervical Dysfunction. 2009 JOSPT.
233
Myelopathy (Babinski and Clonus)
http://academic.uofs.edu/faculty/kosmahle1/courses/pt351/lab351/babinski.htm
Cook C. Physical Examination Tests for Neurological Screening. In: Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008.
Cook et al. found clonus sensitivity = 14 and Babinski = 24
Clinical Prediction Rule-Myelopathy
N = 249 patients with cervical pain: 88 with CSM– Age >45 years– + Hoffmann’s Sign– + Inverted Supinator Sign– + Babinski Test– + Gait Abnormality
Cook et al. JMMT. 2010;18(4).

9/22/2014
40
Cervical Myelopathy Cluster
NOTE. Five tests are included in the rule: (1) Gait deviation; (2) +Hoffmann’s test; (3) Hyperreflexia of the brachioradialis; (4) +Babinski test; and (5) age >45 years. The associated posttest probability values are based on a pretest probability of 35%. 236
Upper Limb Tension Test (Median Nerve Bias)
• Sensitivity = 97, LR- = 0.14
• Helps rule out the presence of cervical radiculopathy when performed early in the examination
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
237
Cervical Distraction Test
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
238
Spurlings Test
Specificity = 92, LR+ = 4.87Rules in presence of cervical radiculopathy
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
239
Cervical Radiculopathy• Spurlings,
ROM<60 degrees, Distraction test, and ULTT
• Sens = 24, Spec = 99, LR+ = 30.3 (all 4 tests positive)
• QUADAS = 10
Wainner et al. Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy. Spine. 2003;28(1):52-62.
12
3 4
240
Lumbar Category III Findings
• Bilateral lower extremity weakness or numbness
• The Straight leg raise

9/22/2014
41
241
Cauda Equina
Jalloh & Minhas. Emerg Med. 2007;24:33-4Shapiro S. Spine. 2000;25:248-52.Small et al. Orthopedic pitfalls. Am J Em Med. 2005;23:159-63.
Rapid symptoms within 24 hours 89% sensitivityHistory of back pain 94% sensitivityUrinary retention 90% sensitivityLoss of sphincter tone 80% sensitivitySacral sensation loss 85% sensitivityLower extremity weakness or gait loss 84% sensitivityCombined bilateral sciatica, motor loss, sacral sensory loss, and sphincter disturbance (19% sensitivity)
Patient Case Number Two
Best Tests for Orthopedics
Best Tests for the Temporomandibular Joint
• Level A• Level B
– Maximal Mouth Opening– Pain during active assistive opening– Pain during palpation– Lateral Glide– Auscultation (but not a click)
• Only 3 studies presented in this literature review were of high quality. Because all of the included studies assessed diagnostic accuracy among subclassifications of individuals suspected of having TMD, the ability of any of these tests to distinguish between patients with TMD versus patients without TMD remains unknown.
Maximal Mouth Opening
• Sensitivity = 22• Specificity = 98• LR+ = 11• LR- = .80
Dworkin et al. (maximal mouth opening of <35mm for men and <30mm for women)
9/22/2014
42
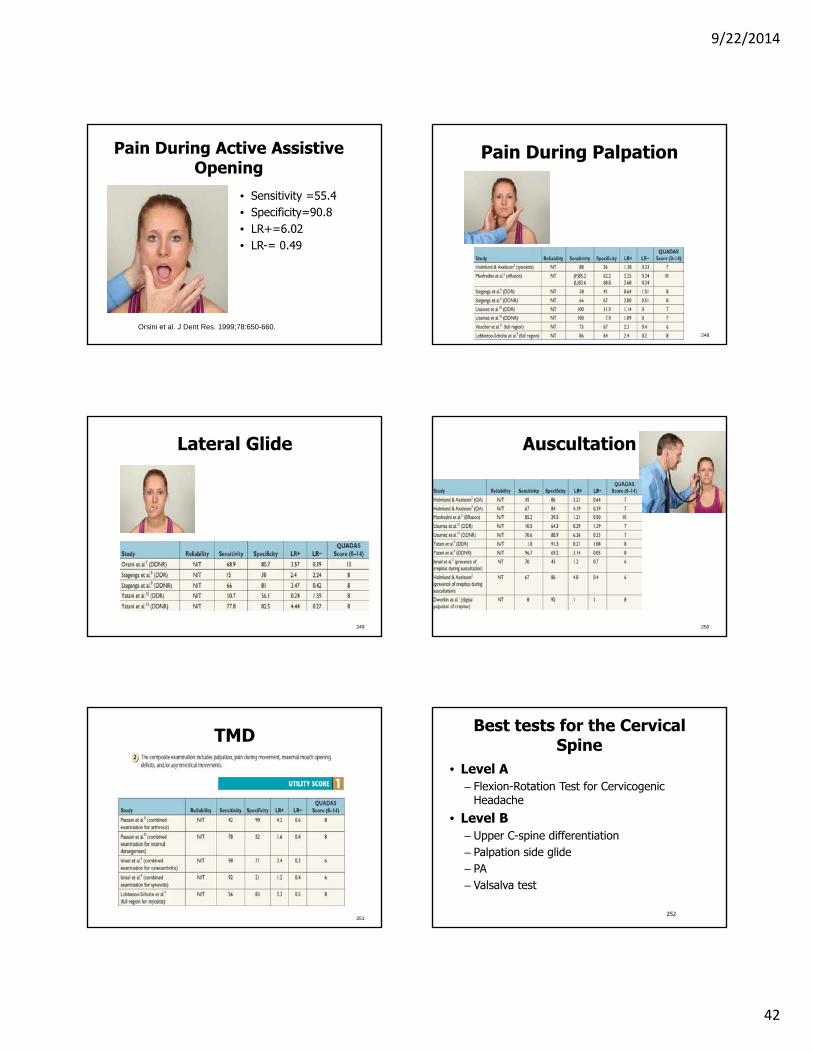
Pain During Active Assistive Opening
• Sensitivity =55.4 • Specificity=90.8 • LR+=6.02• LR-= 0.49
Orsini et al. J Dent Res. 1999;78:650-660.
Pain During Palpation
248
Lateral Glide
249
Auscultation
250
TMD
251
Best tests for the Cervical Spine
• Level A– Flexion-Rotation Test for Cervicogenic
Headache
• Level B– Upper C-spine differentiation– Palpation side glide– PA– Valsalva test
252

9/22/2014
43
C0/1-C1/2-C2/3 Differentiation
• Sensitivity=62• Specificity= 87 • LR+=4.9 • LR-=0.43
254
Palpation Side Glide• C2-3 only• Sensitivity =98,
LR- = 0.02; LR+ = 10.9
• Helps rule out presence of block or restriction
Humphreys et al. An investigation into the validity of cervical spine motion palpation using subjects with congenital block vertebrae as a 'gold standard'. BMC MusculoskeletDisord. 2004;5:19.
255
Flexion-Rotation test
• Sensitivity = 86%• Specificity = 100,
LR+ = ~18+• Rules in and out
the presence of a cervicogenicheadache with an origin at C1-2
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007. 256
Posterior Anterior
• 100% Sensitivity at identifying a lesion of any sort
• Helps rule out presence of cervical pain on any origin
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
257
Valsalva Test
• Specificity = 94, LR+ = 3.7
• Used to rule in presence of cervical radiculopathy
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
Best Tests for Shoulder Problems
• Level A– Hawkins Kennedy*
• Level B– Rent– Surprise Test– External Rotation Lag
Sign– Bear Hug Test– Belly Press Test– Internal Rotation
Strength test– Lateral Jobe Sign– Internal rotation lag sign
• Level B (cont.)– Infraspinatus test– Supine impingement test– Sulcus sign– Upper cut test– Resisted AC extension
test– Cross body adduction
test– AC joint palpation
• Level C– Biceps II load test– Hyperabduction test
9/22/2014
44
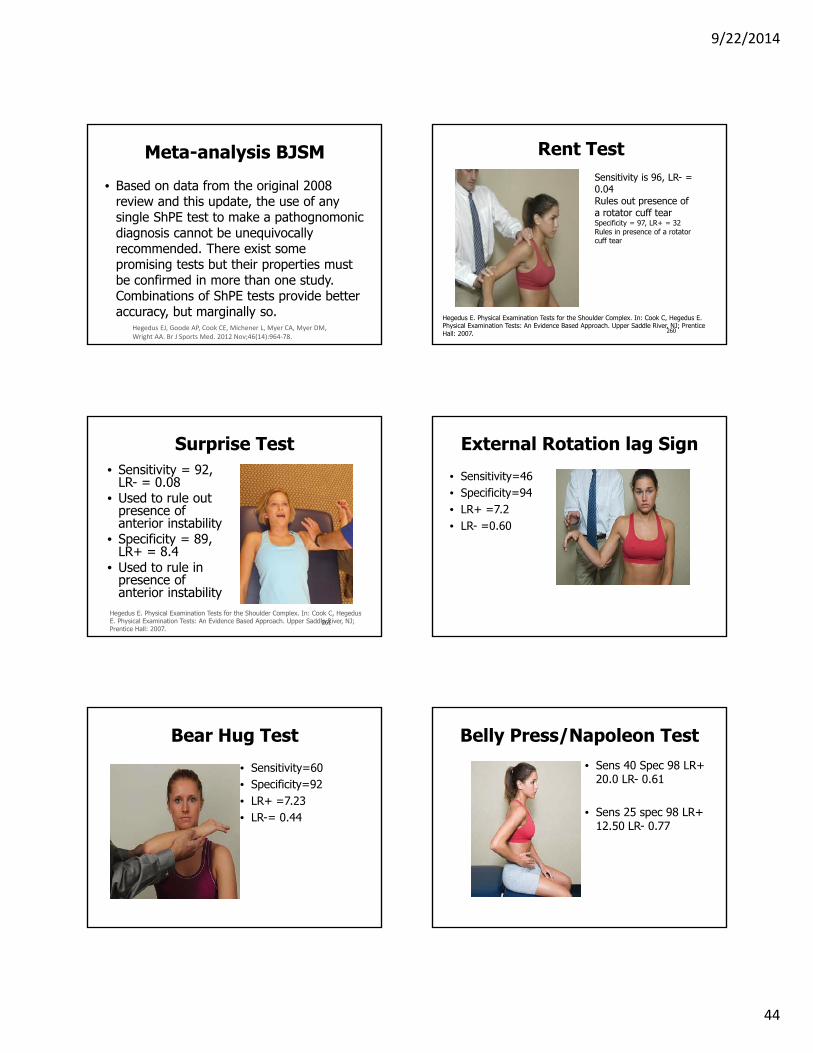
Meta-analysis BJSM
• Based on data from the original 2008 review and this update, the use of any single ShPE test to make a pathognomonic diagnosis cannot be unequivocally recommended. There exist some promising tests but their properties must be confirmed in more than one study. Combinations of ShPE tests provide better accuracy, but marginally so.
Hegedus EJ, Goode AP, Cook CE, Michener L, Myer CA, Myer DM, Wright AA. Br J Sports Med. 2012 Nov;46(14):964‐78.
260
Rent Test
Hegedus E. Physical Examination Tests for the Shoulder Complex. In: Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
Sensitivity is 96, LR- = 0.04Rules out presence of a rotator cuff tear Specificity = 97, LR+ = 32Rules in presence of a rotator cuff tear
261
Surprise Test• Sensitivity = 92,
LR- = 0.08• Used to rule out
presence of anterior instability
• Specificity = 89, LR+ = 8.4
• Used to rule in presence of anterior instability
Hegedus E. Physical Examination Tests for the Shoulder Complex. In: Cook C, HegedusE. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
External Rotation lag Sign
• Sensitivity=46 • Specificity=94 • LR+ =7.2 • LR- =0.60
Bear Hug Test
• Sensitivity=60 • Specificity=92 • LR+ =7.23• LR-= 0.44
Belly Press/Napoleon Test• Sens 40 Spec 98 LR+
20.0 LR- 0.61
• Sens 25 spec 98 LR+ 12.50 LR- 0.77

9/22/2014
45
265
Internal Rotation Strength Test
Hegedus E. Physical Examination Tests for the Shoulder Complex. In: Cook C, HegedusE. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
Sensitivity = 88, LR- = 0.12. Rules out presence of impingement of the shoulder
Lateral Jobe Test
• Sensitivity =81 • Specificity=89 • LR+=7.36 • LR-=0.10
267
Hawkins-Kennedy Test
• Sensitivity = 92, and LR- = 0.18
• Rules out the presence of impingement
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007. 268
Biceps Load Test II
Hegedus E. Physical Examination Tests for the Shoulder Complex. In: Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
Sensitivity = 90, LR- = 0.11. Rules out the presence of a SLAP lesion
269
Hyperabduction Test
Hegedus E. Physical Examination Tests for the Shoulder Complex. In: Cook C, HegedusE. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007. 270
Internal Rotation Lag Sign
• Specificity = 96, LR+ = 24.3.
• Use caution, QUADAS = 8
• Used to rule in presence of subscapularis tear
Cook C. Orthopedic Manual Therapy: An Evidence Based Approach. Upper Saddle River NJ; Prentice Hall: 2007.

9/22/2014
46
271
Infraspinatus Test
• Specificity = 90, LR+ = 4.2
• Used to rule in the presence of impingement
Cook C. Orthopedic Manual Therapy: An Evidence Based Approach. Upper Saddle River NJ; Prentice Hall: 2007.
Supine Impingement Test
272
Sulcus Sign
• Finger width sulcus is considered positive
273
Upper Cut Test (Biceps Tendinopathy)
• SN = 73• SP = 78• LR+ = 3.38• LR-= 0.34
274Kibler et al. Am J Sports Med 2009;37:1840-1847.
275
AC Resisted Extension Test
• Specificity = 85, LR+ = 4.8
• Used to rule in presence of AC joint
Cook C. Orthopedic Manual Therapy: An Evidence Based Approach. Upper Saddle River NJ; Prentice Hall: 2007.
Cross Body Adduction Test
276
9/22/2014
47
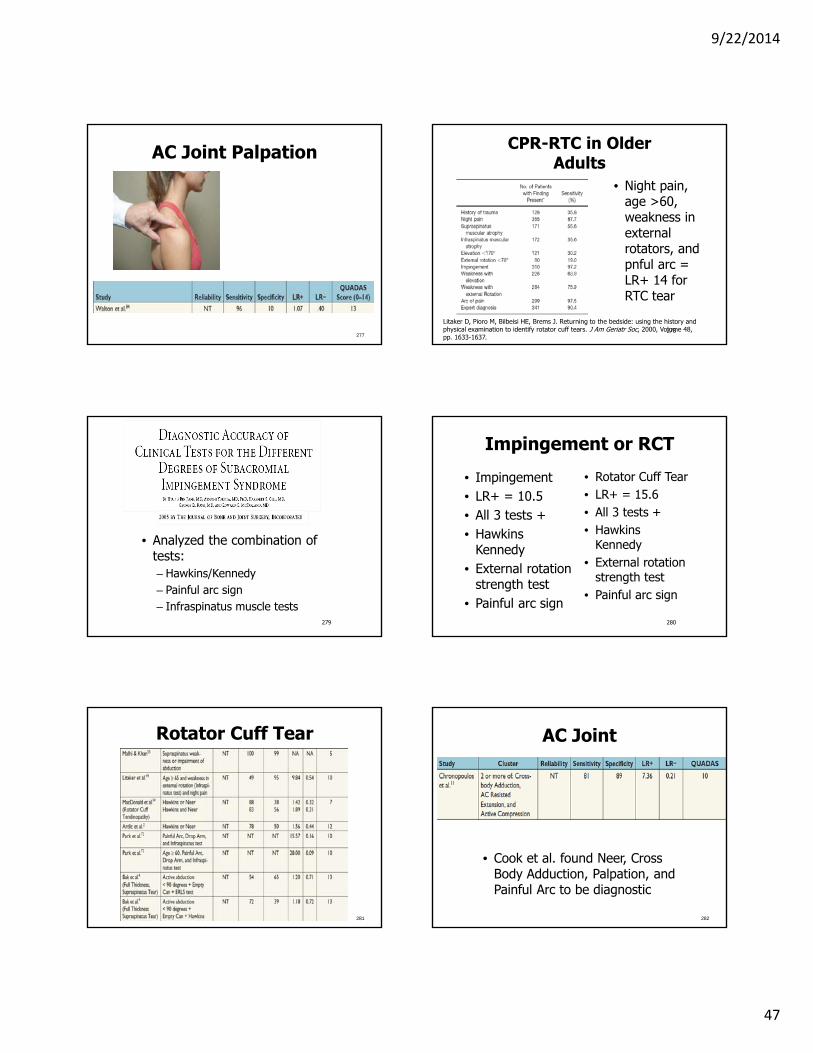
AC Joint Palpation
277278
CPR-RTC in Older Adults
Litaker D, Pioro M, Bilbeisi HE, Brems J. Returning to the bedside: using the history and physical examination to identify rotator cuff tears. J Am Geriatr Soc, 2000, Volume 48, pp. 1633-1637.
• Night pain, age >60, weakness in external rotators, and pnful arc = LR+ 14 for RTC tear
279
• Analyzed the combination of tests:– Hawkins/Kennedy– Painful arc sign– Infraspinatus muscle tests
280
Impingement or RCT
• Impingement• LR+ = 10.5• All 3 tests +• Hawkins
Kennedy• External rotation
strength test• Painful arc sign
• Rotator Cuff Tear• LR+ = 15.6• All 3 tests +• Hawkins
Kennedy• External rotation
strength test• Painful arc sign
Rotator Cuff Tear
281
AC Joint
• Cook et al. found Neer, Cross Body Adduction, Palpation, and Painful Arc to be diagnostic
282
9/22/2014
48
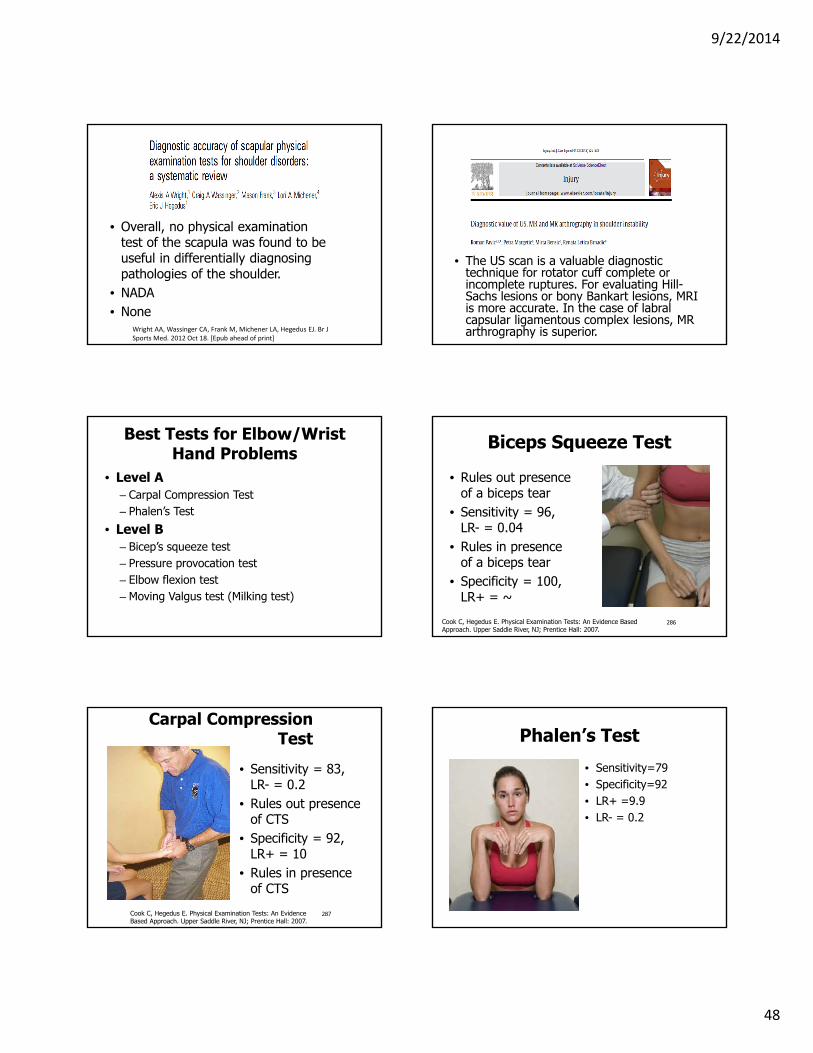
• Overall, no physical examination test of the scapula was found to be useful in differentially diagnosing pathologies of the shoulder.
• NADA• None
Wright AA, Wassinger CA, Frank M, Michener LA, Hegedus EJ. Br J Sports Med. 2012 Oct 18. [Epub ahead of print]
• The US scan is a valuable diagnostic technique for rotator cuff complete or incomplete ruptures. For evaluating Hill-Sachs lesions or bony Bankart lesions, MRI is more accurate. In the case of labralcapsular ligamentous complex lesions, MR arthrography is superior.
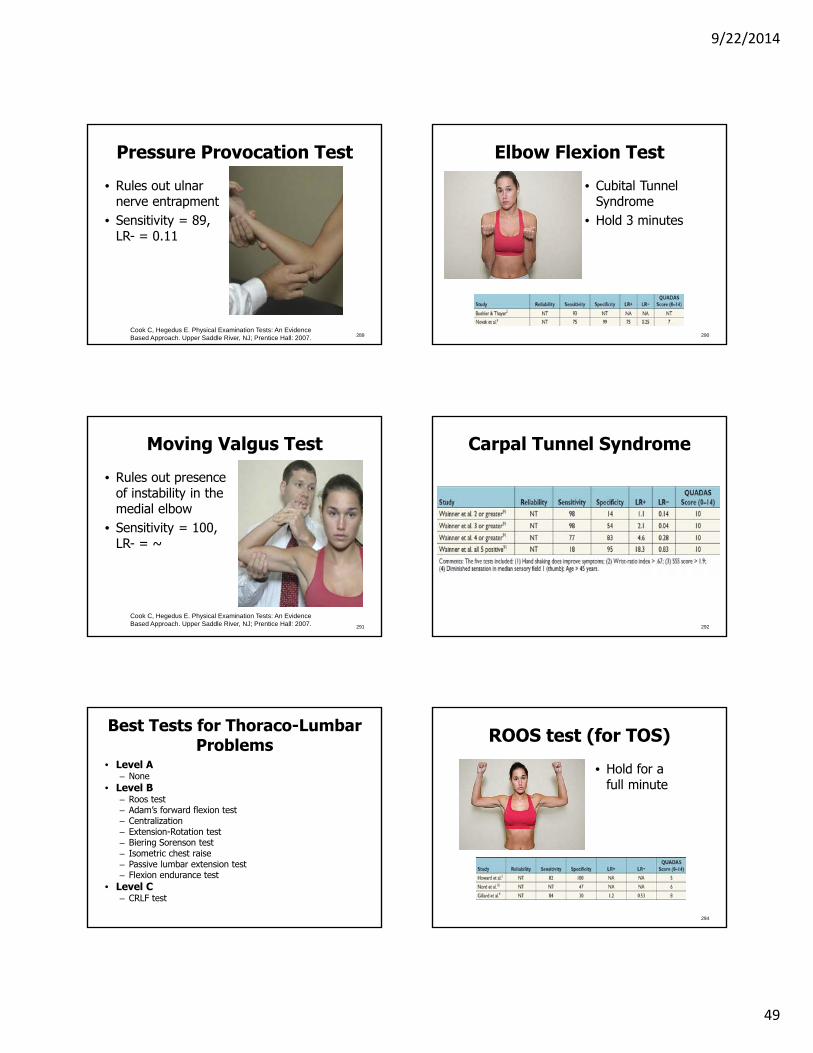
Best Tests for Elbow/Wrist Hand Problems
• Level A– Carpal Compression Test– Phalen’s Test
• Level B– Bicep’s squeeze test– Pressure provocation test– Elbow flexion test– Moving Valgus test (Milking test)
286
Biceps Squeeze Test
• Rules out presence of a biceps tear
• Sensitivity = 96, LR- = 0.04
• Rules in presence of a biceps tear
• Specificity = 100, LR+ = ~
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
287
Carpal Compression Test
• Sensitivity = 83, LR- = 0.2
• Rules out presence of CTS
• Specificity = 92, LR+ = 10
• Rules in presence of CTS
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
Phalen’s Test
• Sensitivity=79 • Specificity=92 • LR+ =9.9• LR- = 0.2
9/22/2014
49
289
Pressure Provocation Test
• Rules out ulnar nerve entrapment
• Sensitivity = 89, LR- = 0.11
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
Elbow Flexion Test
• Cubital Tunnel Syndrome
• Hold 3 minutes
290
291
Moving Valgus Test
• Rules out presence of instability in the medial elbow
• Sensitivity = 100, LR- = ~
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2007.
Carpal Tunnel Syndrome
292
Best Tests for Thoraco-Lumbar Problems
• Level A– None
• Level B– Roos test– Adam’s forward flexion test– Centralization– Extension-Rotation test– Biering Sorenson test– Isometric chest raise– Passive lumbar extension test– Flexion endurance test
• Level C– CRLF test
ROOS test (for TOS)
• Hold for a full minute
294

9/22/2014
50
Cervical Rotation, Lateral Flexion
• Testing left side in photo
• Rotation and SB are opposite
295
Adam’s Forward Flexion
• Tests for scoliosis
296
297
Centralization
Specificity = 94, +LR = 6.7; LR- = .12; Used to rule in and out the presence of Lumbar Radiculopathy
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008.
Extension Rotation Test
• Sensitivity=100 • Specificity=22 • LR+=1.28 • LR- =0.00
Biering Sorenson Test
• Make sure chin is tucked too
299
Isometric Chest Raise
300

9/22/2014
51
Flexion Endurance Test
301
The Passive Lumbar Extension Test
• Sensitivity=84.2 • Specificity=90.4 • LR+ =8.78 • LR- =0.17
Thoracic Outlet Syndrome
303
Best Tests for the Pelvis/SIJ
• Level A• Level B
– Thigh Thrust– Sacral Thrust– Sit to Stand– Pubic Symphysis Palpation
• Level C
Use Caution
• The PSIS distraction test showed a sensitivity of 100% and a specificity of 89% for SIJ pathology. The positive predictive value (PPV) was 90% and the negative predictive value (NPV) was 100%.
• Diagnostic odds ratio of the PSIS distraction test was infinite. Werner et al. BMC Surgery. 2013 Oct 31;13:52.
Case Control QUADAS = 5/14
Sacral Thrust
• Sensitivity=45 • Specificity=89 • LR+=4.39 • LR-=0.60
9/22/2014
52
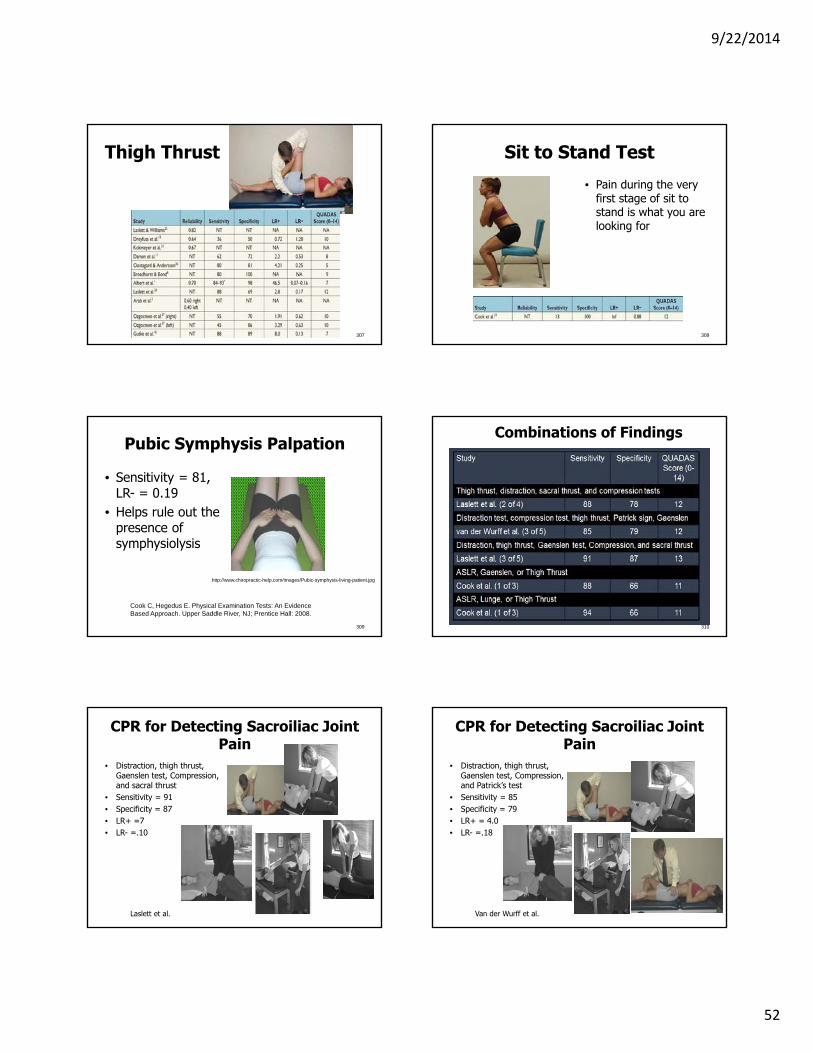
Thigh Thrust
307
Sit to Stand Test
• Pain during the very first stage of sit to stand is what you are looking for
308
309
Pubic Symphysis Palpation
• Sensitivity = 81, LR- = 0.19
• Helps rule out the presence of symphysiolysis
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008.
http://www.chiropractic-help.com/images/Pubic-symphysis-living-patient.jpg
310
Combinations of Findings
CPR for Detecting Sacroiliac Joint Pain
• Distraction, thigh thrust, Gaenslen test, Compression, and sacral thrust
• Sensitivity = 91• Specificity = 87• LR+ =7• LR- =.10
Laslett et al.
CPR for Detecting Sacroiliac Joint Pain
• Distraction, thigh thrust, Gaenslen test, Compression, and Patrick’s test
• Sensitivity = 85• Specificity = 79• LR+ = 4.0• LR- =.18
Van der Wurff et al.
9/22/2014
53
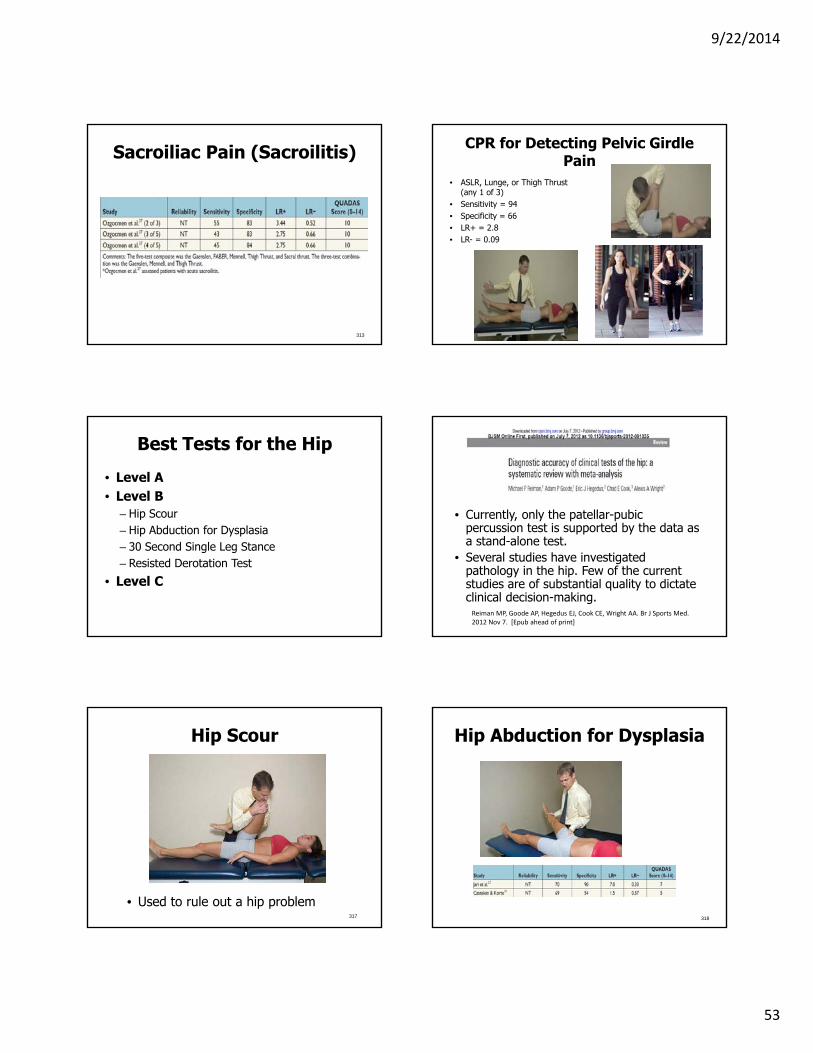
Sacroiliac Pain (Sacroilitis)
313
CPR for Detecting Pelvic Girdle Pain
• ASLR, Lunge, or Thigh Thrust (any 1 of 3)
• Sensitivity = 94• Specificity = 66• LR+ = 2.8• LR- = 0.09
Cook et al. JMPT 2007
Best Tests for the Hip
• Level A• Level B
– Hip Scour– Hip Abduction for Dysplasia– 30 Second Single Leg Stance– Resisted Derotation Test
• Level C
• Currently, only the patellar-pubic percussion test is supported by the data as a stand-alone test.
• Several studies have investigated pathology in the hip. Few of the current studies are of substantial quality to dictate clinical decision-making.Reiman MP, Goode AP, Hegedus EJ, Cook CE, Wright AA. Br J Sports Med. 2012 Nov 7. [Epub ahead of print]
Hip Scour
• Used to rule out a hip problem317
Hip Abduction for Dysplasia
318

9/22/2014
54
30 Second Single Leg Stance for Trochanteric Bursitis
• Sensitivity=100 • Specificity=97.3 • LR+=37 • LR- =0.0
Resisted Derotation Test
• Sensitivity =88 • Specificity=97.3 • LR+=32.6 • LR-=0.12
Hip Osteoarthritis
• Self report of pain during squatting• Active hip flexion causes lateral pain• Passive Extension causes pain• IR less 25 degrees• Pain during Scour and FABER
• <1 factor present Sens = 95, Spec = 18, LR+ = 1.2, LR- = 0.27
321322
Composite Test for Arthritis
• Sensitivity = 86, LR- = 0.19
• Includes test for 1) hip pain, 2) IR<15 degrees, 3) pain with IR, 4) morning stiffness up to 60 minutes, and 5) age>50 years
• Helps rule out the presence of osteoarthritis at the hip
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008.
Composite Test for Arthritis
323
Best Tests for the Knee• Level A
– Lachmans– Anterior Drawer Test– Pivot Shift
• Level B– Thessaly’s test– Dynamic test– Ege’s test– Loss of extension test– Posterior drawer– Functional tests of the patella– MPP Test for Plica
• Level C– McMurray’s test
9/22/2014
55
325
Thessaly Test at 20 Degrees
• 4 studies
• 3 of the 4 have LR+ of 6.2 to 30.0 for the lateral meniscus
And 1.8 to 23 for the medial meniscus
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008. 326
Dynamic Test
• Sensitivity = 85, LR- = 0.17
• Helps rule out the presence of a meniscus tear
• Specificity = 90, • +LR = 8.5• Use to rule in
presence of a meniscus tear
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008.
McMurray’s Test
• Sensitivity=51 • Specificity=91 • LR+=6.3 • LR- =0.53
Ege’s Test
328
Anterior Drawer Test
• Sensitivity=91
• Specificity=89
• LR+=8.3 • LR-=0.10
Meta-Analysis (Anterior Drawer
• Without anesthesia the sensitivity was 0.38 and the specificity 0.81. The positive likelihood ratio was 4.52 and the negative likelihood ratio was 0.67.
• With anesthesia, the sensitivity was 0.63 and the specificity 0.91. The positive likelihood ratio was 8.01 and the negative likelihood ratio 0.33.
Knee Surg Sports Traumatol Arthrosc (2013) 21:1895–1903
9/22/2014
56
331
Lachman’s Test
• Sensitivity = 96, LR- = ~ (specificity is 100)
• Helps rule out the presence of an ACL tear
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008.
Meta-Analysis (Lachman)
• The overall sensitivity of the Lachman test without anesthesia was 0.81 and the specificity 0.81. The positive likelihood ratio was 4.50 and the negative likelihood ratio was 0.22.
• With anesthesia, the sensitivity of the Lachman test was 0.91 and the specificity 0.78. The positive likelihood ratio was 10.07 and the negative likelihood ratio 0.06.
Knee Surg Sports Traumatol Arthrosc (2013) 21:1895–1903
Pivot Shift Test
333
Meta-analysis (Pivot shift)
• The sensitivity of the pivot shift test was 0.28 without anaesthesia and the specificity 0.81. The positive likelihood ratio 5.35 and negative likelihood ratio 0.84.
• With anaesthesia, the sensitivity was 0.73 and the specificity 0.98. The positive likelihood ratio 86.23 and negative likelihood ratio 0.27.
Knee Surg Sports Traumatol Arthrosc (2013) 21:1895–1903
Loss of Extension Test• ACL• Versus other Knee• Sensitivity was
77.6 %, specificity was 94.7 %, its positive predictive value was 95.9 %, and its negative predictive value was 72.4 %
J Orthopaed Traumatol 2013 DOI 10.1007/s10195‐013‐0238‐y 336
Posterior Drawer Test
• Sensitivity = 90, LR- = 0.10
• Helps rule out the presence of a torn posterior cruciate ligament
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008.
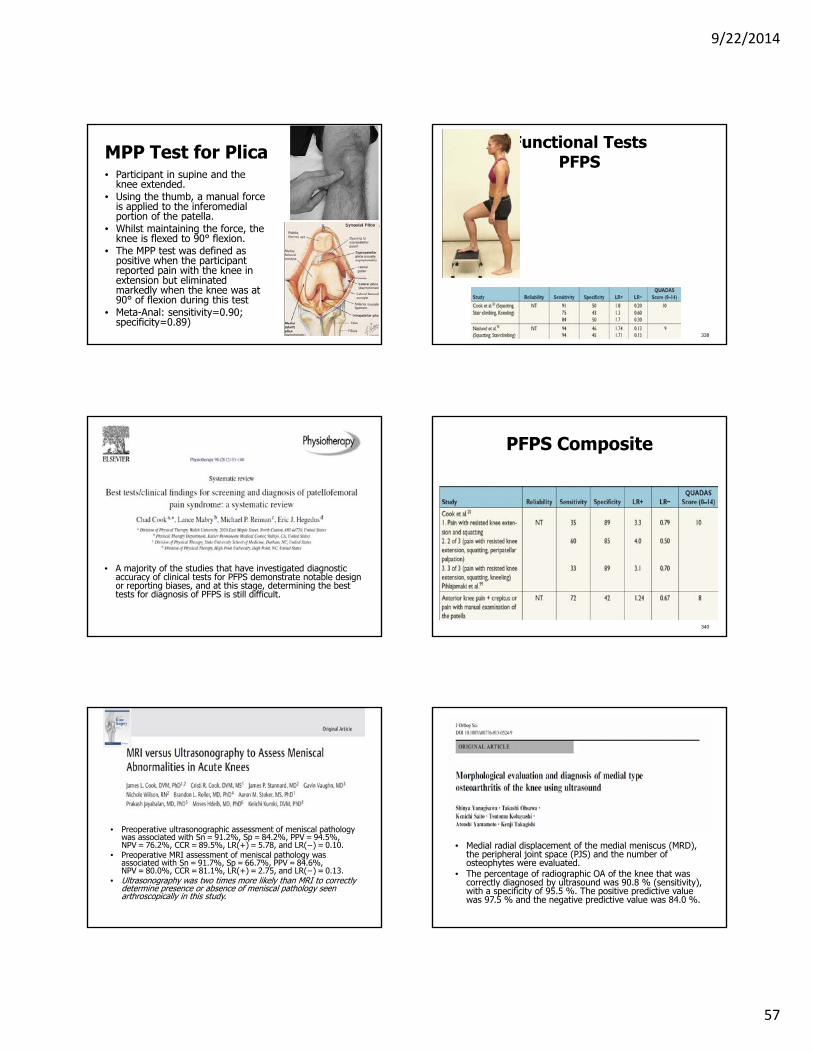
9/22/2014
57
MPP Test for Plica• Participant in supine and the
knee extended. • Using the thumb, a manual force
is applied to the inferomedialportion of the patella.
• Whilst maintaining the force, the knee is flexed to 90° flexion.
• The MPP test was defined as positive when the participant reported pain with the knee in extension but eliminated markedly when the knee was at 90° of flexion during this test
• Meta-Anal: sensitivity=0.90; specificity=0.89)
Functional TestsPFPS
338
• A majority of the studies that have investigated diagnostic accuracy of clinical tests for PFPS demonstrate notable design or reporting biases, and at this stage, determining the best tests for diagnosis of PFPS is still difficult.
PFPS Composite
340
• Preoperative ultrasonographic assessment of meniscal pathology was associated with Sn = 91.2%, Sp = 84.2%, PPV = 94.5%, NPV = 76.2%, CCR = 89.5%, LR(+) = 5.78, and LR(−) = 0.10.
• Preoperative MRI assessment of meniscal pathology was associated with Sn = 91.7%, Sp = 66.7%, PPV = 84.6%, NPV = 80.0%, CCR = 81.1%, LR(+) = 2.75, and LR(−) = 0.13.
• Ultrasonography was two times more likely than MRI to correctly determine presence or absence of meniscal pathology seen arthroscopically in this study.
• Medial radial displacement of the medial meniscus (MRD), the peripheral joint space (PJS) and the number of osteophytes were evaluated.
• The percentage of radiographic OA of the knee that was correctly diagnosed by ultrasound was 90.8 % (sensitivity), with a specificity of 95.5 %. The positive predictive value was 97.5 % and the negative predictive value was 84.0 %.

9/22/2014
58
Best Tests for the Ankle
• Level A– None
• Level B– Anterior Drawer test– Lateral Impingement Test– Forced Dorisflexion Test
• Level C
None are Great
• There is need for future research with more stringent study design criteria so that more accurate diagnostic power of ankle/lower leg special tests can be determined.
Anterior Drawer Test
345
Lateral Impingement Test
346
347
Forced Dorsiflexion Test
• Sensitivity = 95, LR- = 0.06
• Helps rule out the presence of impingement at the ankle.
Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008.
Ankle Impingement
348

9/22/2014
59
Patient Case Number ThreePart Seven: Decision Making
without a Diagnosis
Chad Cook PT, PhD, MBA, FAAOMPTProfessor
Duke University
All Models
• All models use tests and measures to come to a decision point
• Tests and measures are used to influence one’s post-test decision making (probability)
• Diagnostic• Prognostic• Prescriptive
Definitions and Examples• Diagnostic: The test assists in determining a
specific medical diagnosis (e.g., Rotator cuff tear) (test example, Hoffmann’s test for myelopathy)
• Prognostic: The test assists in determining an expected outcome for a patient regardless of treatment provided (test example, Babinski is associated with very poor outcomes)
• Prescriptive: The test when positive and linked with a dedicated intervention will lead to a better outcome then if the test is positive and the intervention is not provided (test example, the prone instability test or Centralization)
Treatment By Diagnosis
• Using a medical diagnosis to drive clinical treatment
• Of obvious importance for selected conditions– Cancer– Heart Disease
• Of dubious importance in other conditions– Shoulder pain– Low back pain
Non-Specific Diagnoses are Prevalent
• Non-specific low back pain• Non-specific abdominal pain• Non-specific neck pain• Non-specific, anterior knee pain• Non-specific shoulder pain
(Impingement syndrome)
9/22/2014
60
Non-specific Low back pain
• Not attributable to a recognizable, known specific pathology
• 85% of LBP• Not life threatening• Should be treated by guidelines• Should not be overly imaged• Should not be treated by surgery
Balaque, Mannion, Pelise, Cedraschi. Non‐specific low back pain. Lancet. Oct 7, 2011
Quibbling over Non Threatening Diagnoses
• Stop trying to differentiate one form of non-sinister pain from another and, instead, focus on the determinants of success or failure.
Dinant GJ, Buntinx FF, Butler CC. The necessary shift from diagnostic to prognosticresearch. BMC Fam Pract. 2007;8:53.
Even the Same Diagnoses are Not Similar
• Severity affects testing and accuracy
• Life cycle of the disease affects accuracy
• Clarity of the concept of the disease affects accuracy (syndromes)
• Stage of the disease affects accuracy (shoulder labrum)
Spinal Myelopathy
• Grade 0: signs or symptoms of root involvement but without evidence of spinal cord disease
• Grade 1: signs of spinal cord disease but no difficulty in walking. • Grade 2: slight difficulty in walking which does not prevent full-
time employment • Grade 3: difficulty in walking which prevented full time
employment or the ability to do all housework, but which was not so severe as to require someone else's help to walk
• Grade 4: able to walk only with someone else's help or with the aid of a frame.
• Grade 5 : chair bound or bedridden.
Nurick S. The pathogenesis of the spinal cord disorder associated with cervical spondylosis. Brain. 95:87-100 (1972)
Snyder’s Criteria for SLAP• Type I: Degenerative changes to the glenoid labrum but
an attached labrum • Type II: Degenerative changes and fraying as well as
complete detachment of the labrum from the glenoid rim and instability of the biceps tendon attachment.
• Type III lesions involved a displaced free-margin of the labrum into the joint and an attached biceps tendon.
• Type IV lesions were categorized as a displaced labrum into the joint and an affected long biceps tendon injury (e.g., partial rupture).
Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy 1990;6:274-9.
SLAP Differences

9/22/2014
61
Unnecessary Labeling
• There is evidence that telling patients that they have an “imaging abnormality” has negative effects related to labeling
• Individuals who are told they have a structural pathology identified on an MRI had lower reported health statuses 1 year later (versus a randomized comparator)
Flynn TW, Smith B, Chou R. Appropriate use of diagnostic imaging in low back pain: a reminder that unnecessary imaging may do as much harm as good. J Orthop Sports Phys Ther. 2011 Nov;41(11):838‐46.
An MRI for Diagnosis of HNP• MRI studies identified 22–40% of
adults with herniated disk, who are asymptomatic and pain free; one study found 81% of such asymptomatic individuals with a bulging disk
Jarvik J, Deyo R. Diagnostic evaluation of low back pain with emphasis on imaging. Ann Intern Med. 2002;137:586–95.
Weaknesses
• We typically don’t treat the diagnosis, we treat the patient
• Diagnosing everyone with certainty can get expensive
• Some diagnoses overlap a lot
Prescriptive Tests and Measures
The test when positive and linked with a dedicated intervention will lead to a better outcome then if the test is positive and the intervention is not provided
Patient Response Method
• Maitland• McKenzie• Mulligan• Treatment is born
from patient response to assessment and results, not from diagnosis
Patient Response Method allows Real-Time Follow up
• Patient centered• Targets reproduction/reduction of
symptoms as a measure of success• Can be performed in absence of a
diagnosis• Appears very sensitive• Ample literature that demonstrates short
term success

9/22/2014
62
Key Terms: Within Sessions Change
• Changes in pain or range of motion (ROM) during a single visit are termed within-session changes
Maitland GD, Hengenveld L, Banks K, English K. Maitland’s vertebral manipulation. 6th ed. Oxford: Butterworth Heinemann; 2001.
Key Terms: Between Session Changes
• Changes in pain or ROM that carry over to a succeeding visit is known as a between-session change
Maitland GD, Hengenveld L, Banks K, English K. Maitland’s vertebral manipulation. 6th ed. Oxford: Butterworth Heinemann; 2001.
Fairly Strong Evidence for Use
• Both of these types of changes have been studied and reported on for neck and low back pain13-16 and hip and shoulder pain.17,18
• Evidence of benefit in utilizing within- and between-session approaches are strongest in the spine.13-16
• There is evidence that within-session changes are predictive of between-session changes for neck pain;however, within-session changes do not appear to be predictive of long-term functional improvement.13
• Currently, within- and between-session analyses have poor support within the periphery.
• Garrison JC, Shanley E, Thigpen C, Hegedus E, Cook C. Between-session changes predict overall perception of improvement but not functional improvement in patients with shoulder impingement syndrome seen for physical therapy: an observational study. Physiother Theory Pract 2011;27:137e45
• Hahne AJ, Keating JL, Wilson SC. Do within-session changes in pain intensity and range of motion predict between-session changes in patients with low back pain? Aust J Physiother 2004;50:17e23.
• Tuttle N. Do changes within a manual therapy treatment session predict betweensession changes for patients with cervical spine pain? Aust J Physiother2005; 51:43e8.
• Tuttle N, Laasko L, Barrett R. Change in impairments in the first two treatments predicts outcome in impairments, but not in activity limitations, in subacute neck pain: an observational study. Aust J Physiother 2006;52:281e5.
• Tuttle N. Is it reasonable to use an individual patient’s progress after treatment as a guide to ongoing clinical reasoning? J Manip Physiol Ther 2009;32: 396e403.
• Wright AA, Abbott JH, Baxter D, Cook C. The ability of a sustained within-session finding of pain reduction during traction to dictate improved outcomes from a manual therapy approach on patients with osteoarthritis of the hip. J Man ManipTher 2010;18:166e72.
Key Terms: Directional Preference
• Moderate evidence was identified that DPM was significantly more effective than a number of comparison treatments for pain, function and work participation at short, intermediate and long-term follow-up.
• No trials found that DPM was significantly less effective than comparison treatments.
Surkitt et al. Efficacy of Directional Preference Management for Low Back Pain: ASystematic Review. Phys Ther. 2012; Jan 12 {E-pub ahead of print]
“The McKenzie Approach”• 11 trials of mostly high quality were included. McKenzie
reduced pain (weighted mean difference [WMD] on a 0- to 100-point scale, -4.16 points; 95% confidence interval, -7.12 to -1.20) and disability (WMD on a 0- to 100-point scale, -5.22 points; 95% confidence interval, -8.28 to -2.16) at 1 week follow-up when compared with passive therapy for acute LBP.
• When McKenzie was compared with advice to stay active, a reduction in disability favored advice (WMD on a 0- to 100-point scale, 3.85 points; 95% confidence interval, 0.30 to 7.39) at 12 weeks of follow-up.
• There is some evidence that the McKenzie method is more effective than passive therapy for acute LBP; however, the magnitude of the difference suggests the absence of clinically worthwhile effects.
Machado LA, de Souza Mv, Ferreira PH, Ferreira ML. Spine (Phila Pa 1976). 2006 Apr 20;31(9):E254‐62.

9/22/2014
63
Requires Re-assessment of Function
• “A methodical approach that considers change in parameters such as patient impairments is likely to be a useful guide for decision making during ongoing patient management but only when the change being reassessed can be directly linked to functional goals.”
Tuttle N. Is it reasonable to use an individual patient’s progress after treatment as a guideTo ongoing clinical reasoning? J Manipulative Physiol Ther. 2009;32:396-403.
Weaknesses of the Patient Response Method
• Over-focus on symptoms of the patient• Requires that the patient play a role in the
treatment process• Requires really good communication
between the clinician and the patient
Cook C. Orthopedic Manual Therapy: An Evidence Based Approach. 2nd edition. Upper Saddle River NJ; Prentice Hall: 2012.
How about the Periphery?
• Classification• Guidelines• Acquired knowledge
from evidence
Prescriptive CPRs
• Prescriptive CPRs are more difficult to design and publish
• Are more difficult to find significance because the outcome measure is malleable (and different among studies)
• Frequently inappropriately derived (single arm studies), and the results are prognostic, versus prescriptive
• Bottom Line: There is trouble here. Kent P, Hancock M, Petersen DH, Mjøsund HL. Clinimetrics corner: choosing appropriate study designs for particular questions about treatment subgroups. J Man Manip Ther. 2010 Sep;18(3):147‐52.
The Outcome Measure is Malleable
– OMERACT-OARSI Criteria– PASS (Patient Acceptable Symptom State)– GRoC (change of 5)– No Surgery (versus went to surgery)– MCID’s
• Results suggested that different “CPRs” were developed from same sample using different outcomes measures!!!
Wright A, et al. Predictors of response to physical therapy intervention in patients with primary hip osteoarthritis: a comparison of predictive modeling based on varying response criterion.IFOMPT Submission, 2012.
When Different Outcomes are UsedModel Variables Individual
P valueCoefficientT value
Model F value
Model Adjusted R2
Model Pvalue
ODI Change Score
Lower initial ODIMet CPRHEP complianceShorter duration sxsYounger age
<0.010.040.070.01<0.01
9.7‐2.1‐1.8‐2.5‐3.6 24.0 46.2 P<0.01
NPRS ChangeScore
Lower initial NPRSLower initial ODIMet CPRShorter duration SxsHEP complianceDiagnosis
<0.010.01<0.01<0.010.06<0.01
14.9‐2.4‐3.5‐3.9‐1.8‐2.6 46.6 67 P<0.01
Total Visits Met CPR <0.01 2.8 8.3 0.5 P<0.01
Rate of Recovery (0 to 100%)
Lower initial NPRSMet CPRNo irritabilityShorter duration Sxs
0.090.010.03<0.01
1.7‐2.62.3‐3.8 7.7 16.7 P<0.01

9/22/2014
64
• Different rules for different outcomes measures.
• Hope we pick the right one!!!Schwind et al. J Man Manip Ther. 2013;21:71‐78.
Different CPRs for different MCID’s. Hope we pick the right one!!
When Different MCID’s are Used Why is this a Problem?• We don’t all use the same
outcome measure.• We should use more than one
outcome measure• We don’t all use the same cut
point and know the best cut point per outcome measure
• Yet we are telling people they HAVE to do a particular treatment if a person meets a particular rule
Using Derivation Studies for Treatment Decision Making
• Single arm derivation studies are likely to capture prognostic variables that demonstrate improvement regardless of whether the intervention is used or not
Hancock M, Herbert RD, Maher CG. A guide to interpretation of studies investigating subgroups of responders to physical therapy interventions. Phys Ther. 2009 Jul;89(7):698‐704.
Prescriptive Concerns
• Some (Beattie and Nelson 2006; Chaitow, 2010) have expressed concern regarding the indiscriminate use of CPRs and the potential undermining of clinical reasoning during the care of a patient.

9/22/2014
65
We didn’t find that
Learman K, Showalter C, Cook C. Does the Use of a Prescriptive Clinical Prediction Rule Increase the Likelihood of Applying Inappropriate Treatments? Man Ther. 2012;
To date, 4 Have Critically Appraised (Systematically) CPRs
Thus Far• Beneciuk JM, Bishop MD, George SZ. Clinical prediction rules
for physical therapy interventions: a systematic review. PhysTher. 2009 Feb;89(2):114-24. Epub 2008 Dec 18.
• Haskins R, Rivett DA, Osmotherly PG. Clinical prediction rules in the physiotherapy management of low back pain: A systematic review. Man Ther. 2011 Jun 3. [Epub ahead of print]
• Stanton TR, Hancock MJ, Maher CG, Koes BW. Critical appraisal of clinical prediction rules that aim to optimize treatment selection for musculoskeletal conditions. 2010 Jun;90(6):843-54. Epub 2010 Apr 22.
• May S, Rosedale R. Prescriptive clinical prediction rules in back pain research: a systematic review. J Man Manip Ther. 2009;17(1):36-45.
The verdict so far: Limited support for current CPRs that have been published for PT
Prognostic Tests and Measures
The test assists in determining an expected outcome for a patient regardless of treatment provided
Stratified Treatment Approach
• Risk stratification to determine resource allocation of services
• Potentially, resource stratification based on projected prognosis (insurance rates for unhealthy lifestyles)
How is this Determined• Prognostic models generalize best to
populations that have similar ranges of predictor values to those in the development population
• Application of prognostic models requires unambiguous definitions of predictors and outcomes and reproducible measurements using methods available in clinical practice
• Impact studies quantify the effect of using a prognostic model on physicians’ behavior, patient outcome, or cost effectiveness of care compared with usual care without the model
• Impact studies require different design, outcome, analysis, and reporting from validation studies
Moons, KG.; Altman, DG.; Vergouwe, Y.; Royston, P. “Prognosis and prognostic research: application and impact of prognostic models in clinical practice.” BMJ: v. 338, 2009, p. b606.
STarT• This tool classifies patients into 3 categories for
targeted treatment, based on the presence of potentially modifiable physical and psychological prognostic indicators for persistent, disabling symptoms, identified through 9 questions.
• Patients are classified as "low risk" of future disabling LBP if they score positively on fewer than 4 questions. The remainder are then subdivided into "medium risk" (physical and psychosocial indicators for poor outcome, but without high levels of psychological indicators) and "high risk" (high levels of psychological prognostic indicators with or without physical indicators).
Hill J et al. Eur J Pain. Jan 2010; 14(1): 83–89.

9/22/2014
66
Weaknesses• Getting clinicians to agree on the
stratification models• Getting patients to agree on less or more
care• We still can’t agree upon a defined
outcome measure• There aren’t many of these in
conventional MSK literature
Prognostic CPRs• Prognostic is prediction of success in
the future. • Not to be confused with prescriptive • Often there are interactions in the
findings (a variable can be both prescriptive and prognostic, or prognostic only (Kent et al)
• Bottom line: Not difficult to do when designed correctly
Kent P, Keating JL, Leboeuf‐Yde C. Research methods for subgrouping low back pain. BMC MedRes Methodol. 2010 Jul 3;10:62.
Synthesizing the Information: Making Complete Decisions

9/22/2014
67
Classification Systems• Allows “pooling” of decision making by
identifying pertinent features• Evidence Supports This
Outside of Low Back Pain?
• Let’s just say it’s early on the evolutionary scale
Classification
• Considered the “Holy Grail” for treatment of LBP
• May have credence for shoulder problems too
• Clustering probable groups (which is best?)
399
Classification Systems
• Three types of classification• Status Indices (defined by patient
description: e.g., ICD-9 Code)• Prognostic indices (defined by statistical
prediction of projected outcome)• Clinical Guideline indices (clinical
examination findings drives the treatment provided)
Riddle DL. Classification and low back pain: a review of the literature and critical analysis of selected systems. Phys Ther. 1998;78: 708‐737.
Treatment Based Classification
• Manipulation• Stabilization• Traction• Specific Exercise
Stanton and Colleagues1
• Treatment Based Classification• 25.2% (95% confidence interval
[CI]=19.8%–30.6%) of the participants did not meet the criteria for any subgroup
• 49.6% (95% CI=43.4%–55.8%) of the participants met the criteria for only one subgroup,
• 25.2% (95% CI=19.8%–30.6%) of the participants met the criteria for more than one subgroup.

9/22/2014
68
Stanton and Colleagues2
• Who did not have a clear classification?• Greater odds of being older (odds ratio [OR]=1.01,
95% confidence interval [CI]=1.003-1.033), • Having a longer duration of LBP (OR=1.001, 95%
CI=1.000-1.001), • Having had a previous episode(s) of LBP (OR=1.61,
95% CI=1.04-2.49), • Having fewer fear-avoidance beliefs related to both
work (OR=0.98, 95% CI=0.96-0.99) and physical activity (OR=0.98, 95% CI=0.96-0.996),
• Having less LBP-related disability (OR=0.98, 95% CI=0.96-0.99) than people with clear classifications.
Which one is the Best?
pursuingmeaningfulwork.com
The Classifications vary tremendously
• “There is, as yet, a long way to go so be cautious of subgrouping approaches without robust evidence. The potential for this research to produce misleading results is high and attention to careful design issues is critical.”
405
Weaknesses of Classification Models
• Different models don’t always agree• Some “conditions” are left out• Models to support philosophies• Models that provide only marginal effect• Poorly studied• Limited for systems outside low back pain
Treatment Based Guidelines
• Treatment based guidelines are "evidence-based clinical practice guidelines," which are created following a rigorous development process and are based on the highest quality scientific evidence.
Use Caution: Guidelines are Not Infallible
Let’s consider how these are made• 1. Expert consensus.• 2. Outcomes based• 3. Preference based
(Outcomes based combined with patient based)
• 4. Evidence Based (what we are used to)
Scazitti D. Evidence‐based guidelines: application to clinical practice. Phys Ther. 2001 Oct;81(10):1622‐8.
9/22/2014
69
The Primary Care Provider as the Economic Gatekeeper
• All guidelines are geared toward initiation of care from a primary care provider (Dagenais et al., Spine J, 2010).
• That role takes different forms in different countries and cultures and a primary care provider doesn’t know a lot about MSK injuries
Economic Factors
• Rarely, are cost effectiveness components considered in LBP guidelines development (Koes et al., Eur Spine J, 2010 )
• Many create guidelines as a mechanism to adapt to societal, cultural, legal, or economic realities of their countries. (Dagenais et al., Spine J, 2010)
Mono-Disciplinary Guidelines
• Clinical guidelines created by a specific group (e.g., physical therapists)
• Mono-disciplinary guidelines are more likely to be consensus-based as well as biased, especially in areas where evidence is weak and discipline self interest is strong
Breen et al. Eur J Spine. 2006;15:641‐647.
Conflicts of interest
• 62% of guidelines creators had a vested interest in the diagnostic or interventional guidelines they advocate
• Some guidelines involve findings as high as 87-90% (Jones et al., Ann Intern Med, 2012)
• Top deficient findings in the Agree II guidelines
Examples• Physical Therapist
Guidelines (Manipulation)
• Thrust manipulative and non-thrust mobilization procedures can also be used to improve spine and hip mobility and reduce pain and disability in patients with subacuteand chronic low back and back-related lower extremity pain. A
• Chiropractic Guidelines (Manipulation)
• There was little evidence for the use of manipulation for other conditions affecting the low back, and very few papers to support a higher rating (Rating: C).
Delitto et al. JOSPT. 2012;42(4):A1‐A57. http://www.ccgpp.org/delphi.pdf
• Osteopathic Guidelines (Manipulation)
• Other areas……what??
http://www.ccgpp.org/delphi.pdf
More Examples (CPRs)?• Physical
Therapy• Discussion of 2
pages dedicated to this
• Osteopathic
• Not even mentioned
• Chiropractic
• Not even mentioned
9/22/2014
70
Weaknesses of Guidelines
• By their nature they are always outdated• Designed to improve outcomes to be
“better than average care”• Rarely used• Information is not dispensed well
Turner et al. Development of evidence‐based clinical practice guidelines (CPGs): comparing approaches Implementation Science 2008, 3:45
So Final Advice: How do you Make “Correct” Decisions?
• Train and use your experiences the best you can• Recognize your biases and try to compensate
for these• Know the best tests• Know the guidelines and classification
approaches (if available)• Be thorough, be diligent, care, realize the
patient is also responsible, and know there will never be perfection
Patient Case Number Four