-
Copyright Statement
As a registered E-materials Service user of the EBMT Annual
Meeting in Marseille March 26-29th 2017,
you have been granted permission to access a copy of the
presentation in the following pages for the
purpose of scientific education. This presentation is
copyrighted material and must not be copied,
reproduced, transferred, distributed, leased, licensed, placed
in a storage retrieval system, publicly
performed or used in any way, except as specifically permitted
in writing by the presenter or, as allowed
under the terms and conditions under which it was received or as
permitted by applicable copyright law
or rules of proper citation. Any unauthorised distribution or
use of this presentation, a subset of it or
graphics taken from the presentation may be a direct
infringement of the presenter’s rights.
-
Antonio M. Risitano, M.D., Ph.D.Head of Bone Marrow Transplantation UnitFederico II University of Naples
RACE DM training session:Immunusuppressive treatment for aplastic anemia
-
O pha disease. I ide e ates p ese t geog
aphi a iatio s. to ‐fold highe
ates i Asia tha Eu ope a
d the
U ited States
Glo al i ide e ates a ge . ‐ .
ases pe illio i ha ita ts.
Aplastic anemiaNeutrophils for Incidence, age for SCT
-
• AA: hat does it ea ?
• Ho e do the diag osis?
• Whe should e t eat?
• Ho e t eat?
Aplasti a e ia: AA
-
• AA: hat does it ea ?
• Ho e do the diag osis?
• Whe should e t eat?
• Ho e t eat?
Aplasti a e ia: AA
-
Aplastic anemia
Normal
-
Aplastic anemia
Contraction of stem cell pool
Cytopenia
Normal Marrow aplasia
Takaku et al, Blood 2010
CML
Takaku et al, Blood 2010
AA
-
AA: hat does it ea ?
(Oligo) clonal CD8+ T cells
Auto-immunity = immune disorder = idiopathic AA
-
AA: hat does it ea ?
Constitutionnal = inherited disorder (FA, dyskeratosis
congenita)
-
Hematopoietic stem cells in AAHematopoietic progenitor
cultures
-
Establishment of a CD4+ T cell clone recognizing autologous
hematopoietic progenitor cells from a patient with immune-mediated
aplastic anemia.
Experimental Hematology 23 (1995): 433
Nakao S, Takamatsu H, Yachie A, Itoh T, Yamaguchi M, Ueda M,
Shiobara S, Matsuda T.
T-cell clonality in aplastic anemiaA surrogate marker for
Ag-driven immune response
-
Hematopoietic stem cell
Pathophysiology of aplastic anemia
The immune system
-
• AA: hat does it ea ?
• Ho e do the diag osis?
• Whe should e t eat?
• Ho e t eat?
Aplasti a e ia: AA
-
Ho e do the diag osis
To eliminate something else(leukemia, lymphoma etc)
-
Full lood ou ts:
‐ Pa tope ia
‐ At least ellula li es a e de
eased
Aplastic anemiaDiagnosis
-
Ho e do the diag osis: pe iphe
al lood
-
Ho e do the diag osis: a o sa
pli g
-
Ho e do the diag osis: a o
iops
-
Aplastic anemiaSummary
Pa tope ia
Pe siste t, u e plai ed a o
aplasia
‐ He atopoiesis epla ed fat
ells
No spe ifi a ke
‐ Diag osis e lusio
Se e it eed to e defi ed
-
Aplastic anemiaCytogenetics and flow cytometry
Due to h po ellula o e a o f e ue
tl i suffi ie t etaphases
FISH fo h o oso es a d
should e o side ed
isolated del fa o a le lo g‐te out o e
A a o al toge eti lo e does
ot i pl the diag osis of MDS o
AML
C toge eti a o alities a e p ese
t i up to % of t pi
al AA patie ts
Dete tio of s all PNH lo es has i pli atio s fo defi i g the
disease.‐ A out % a e aplasti ith s all lo es a d o he ol sis.PNH
lo e size easu e e ts:
at p ese tatiose ial o ito i g should e pe fo ed at least ea
l
-
Aplastic anemiaDifferential diagnosis
Cha a te isti s AA h poplasti MDS
d se th opoiesis so eti es es
a o al eut ophil o es
d splasti egaka o tes o es
fi osis o o asio al
i eased lasts o So eti es ALIPS
CD + ells i BM
-
Aplastic anemiaDifferential diagnosis
Fa o i a e ia:‐ Positi e h o oso al
eakage test MMC o DEB
that still ep ese ts the
diag osti gold sta da d.
S ee i g: telo e e le gth
Dyske atosis o ge ita‐ As pto ati :
‐ F e ue t asso iatio ith TE‘C, TE‘T
utatio‐ % all idiopathi fo s
‐ ‘a el , ith TINF ge e utatio‐ ‘e og iza
le phe ot pe of DC:
‐ TINF , NHP , NOP , DKC utatio
-
Aplastic anemiaSeverity
Se e e AA SAA
At least t o of the follo i g th
ee ite ia ha e to e fulfilled:
‐ ‘eti ulo tes < /L usi g a auto
ated a al ze o
-
• AA: hat does it ea ?
• Ho e do the diag osis?
• Whe should e t eat?
• Ho e t eat?
Aplasti a e ia: AA
-
Whe should e t eat?
Camitta BM et al. Blood 1976;48:63–70SAA, severe AA; VSAA, very
severe AA
SAAHypocellularity (
-
• AA: hat does it ea ?
• Ho e do the diag osis?
• Whe should e t eat?
• Ho e t eat?
Aplasti a e ia: AA
-
Treatment options for aplastic anemia
Locasciulli et al, Haematologica 2007
-
Idiopathi AA: ho e t eat?
(Oligo) clonal CD8+ T cells
Auto-immunity = immune disorder = idiopathic AA
1. Immunosuppressive treatment
-
Idiopathi AA: ho e t eat?
-
Idiopathi AA: ho e t eat?
(Oligo) clonal CD8+ T cells
Auto-immunity = immune disorder = idiopathic AA
2. Bone marrow transplantation
-
Idiopathi AA: ho e t eat?
-3 -2 -1-4-8 -7 -6 -5 +14 +40 +100 +1800
Greffon
Conditionnement
1. Reduced intensity conditioning regimen
2. Bone marrow as source of stem cells
3. No need for GvHD
4. infections
-
Age
yea s
I u osupp essi e t eat e t
No si li gsHLA‐ide ti al si li gs
BMT
Idiopathi AA: ho e t eat?
-
Constitutionnal = inherited disorder (FA, dyskeratosis
congenita)
I he ited AA: ho e t eat?
Bone marrow transplantation
-
• AA: a o e pty, othi g else
• Diag osis is e y i po ta t
• T eat e t if SAA o t as fusio s
• I u osupp essi e the apy a ui ed o
BMT a ui ed a d i he ited
Co lusio : AA
-
AA and…
… supportive care
-
n=420 (174 non-responders)Infection-related mortality from 37%
to 11%Incidence of IFIs from 49% to 8%
The most relevant breakthrough in AA treatment was the
anti-infectious supportive care: keeping AA patients alive until
they recover (IST or SCT)
CID 2011
Group 1: 12/1989-10/1986Group 2: 11/1986-10/2002Group 3:
11/2002-04/2008
Supportive careThe improvement in anti-infectious management
-
Supportive careThe role of steroids
Steroids are broadly used as ancillary therapy of SAA Based on
old data on potential therapeutic efficacy (Bacigalupo et al NEJM
1982) Drawn from empirical use (and possible efficacy) of steroids
in other immune-
mediated cytopenias (Ab-mediated)BUT No clinical evidence of
efficacy Increased risk of severe infectious complications (mostly
IFI) May mask ongoing/overt infections (including sepsis)
Short-term toxicity (cumulative with CsA): hypertension, diabetes,
fluid
retention Long-term toxicity: avascular necrosis, cataracts,
etcIn the context of SAA, steroids should be used only as
prophylaxis of serum sickness during ATG treatment, using the
lowest effective dose and the faster tapering Start with 1
mg/kg/day, eventually doubled in case of serum sickness or
other
allergic manifestations*; then taper by 25% every 2-4
days*ATG-related allergic infusion reactions should rather
considered manifestations of Complement Activation Related
Pseudo-Allergy (CARPA), which eventually derive from
massive activation of the classical pathway due to the exogenous
antibodies and their
immune-complexes
-
AA and…
… immunosuppressive treatment
-
Survival improved with years, mostly due to:Better supportive
therapy
Better salvage treatment (SCT)
OUTCOME OF IMMUNOSUPPRESSION FOR SAAImprovement over the
years
‐‐
‐
‐
EBMT Database
N=3202
Courtesy of Jakob Passweg
-
n=112 hATG x 4 (40mg/kg) + CsA x 6 m
Hematological response is the
main predictor for outcome
3m survivors
OS 55% @7y; OR 60% @ 3m, 61% @ 6m, 58% @ 1y
2003
3m survivors
-
IMPROVING ATG-BASED IMMUNOSUPPRESSIONThe benefit of combining
ATG and cyclosporine A
CyA speed hematological response without affecting survival
Blood 2003
Treatment of aplastic anemia with antilymphocyte globulin and
methylprednisolone with or without cyclosporine. The German
Aplastic Anemia Study GroupN Frickhofen, JP Kaltwasser, H
Schrezenmeier, A Raghavachar, HG Vogt, F
Herrmann, M Freund, P Meusers, A Salama, and H Heimpel
NEJM 1991
CyA reduces early treatment failure but not long-term relapse
rate
-
RELAPSES AFTER ISTThe role of maintenance CyA therapy
Frickhofen N. Blood. 2003 (101). 1236-1242
Maintenance CyA is required to sustain blood counts after
initial response to IST
-
REASONS FOR TREATMENT FAILURE
•Pathophysiology other than immune-mediated
•Irreversible stem cell deficit
•Insufficient immunosuppression
Improve front line immunosuppressive
therapies
-
Improving IST for AA: chronicle of a failure
-
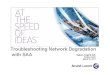
APC (HLA+Ag) triggering
Naive
T-cellAPC
Cytokine release (IL-1, IL-6)Cell-cell contact
TCR
AutoantigenHLA
T-cell activationActivated
T-cell
IL-2
releaseIL-2 signaling
T-cell differentiation
Effector
T-cell
Second signals
(IL-2, IL-12, IL-23,
IL-4, IL-6, IL-17)
Proliferation
Expanded
effector T-cell
pool
T-cell expansion
Marrow damage
Haematopoietic nicheHaematopoietic stem cells
Effector mechanisms
Inflammation
TNF-αIFN-γ
Perforine/
granzymeFas-L
Cell-cell contactInhibitory cytokines
Anergy inductors
•CTLA4-Ig•Anti-CD154
CNIs•CyA•FK506
IL-2 R blockers•Daclizumab•Basiliximab
MToR inhibitors•Sirolimus•Everolimus
Anti-lymphocyte agentsBiologicals Cytostatics
•CTX•MMF•MTX•AZA
Selective•Rituximab•Visilizumab•Zanolimumab•Apolizumab•Alefacept•Efalizumab
Broad•ATGs•Alemtuzumab
Anti-cytokines
TNF-α•Etanercept•Infliximab•AdalimumabIFN-γ•Fontolizumab
Steroids
?
STRATEGIES OF IMMUNOSUPPRESSION (Risitano, BJH 2010)
-
IMPROVING IMMUNOSUPPRSSIVE TREATMENT FOR AAThe history of a
failure
1. No benefit from the addition of a third drug over the
hATG-CsA platform Mycophenolate mofetil (randomized NIH trial)
Rapamicine (open-label NIH trial)
2. No benefit from using non-hATG based regimens Rabbit ATG
(NIH, EBMT, etc) Alemtuzumab (NIH, Naples) Cyclophosphamide (John
Hopkins, NIH)
3. Novel immunosuppressive strategies Anti-cytokine mAbs (TNF,
IFN, IL2/IL23, etc) Daclizumab (anti-IL2R), alefacept (anti-LFA-3),
efalizumab (anti-
LFA-1) Mesenchimal stem cells Anti-CD26 (Begedina®): in
development for aGvHD
Scheinberg et al BJH 2006; Scheinberg et al Haematologica 2009;
Risitano et al BJH 2009; Scheinberg et al NEJM 2011; Marsh et al
Blood 2013; Scheinberg et al Blood 2012
-
rATG is inferior to hATG in first line treatment of SAA, as
indicated by hematological response and survival
NEJM 2011
Phase III prospective randomized study, first-line treatment
hATG + CyA (n=60) vs rATG + CyA (n=60)OR @ 6m 68% vs 37% (p
-
Blood 2012
rATG is inferior to hATG in first line treatment of SAA, as
indicated by hematological response and survival
Phase II pilot study rATG + CyA (n=35) Retrospective matched
comparison (pair-matched) with hATG + CyA (n=105)Pilot rATG + CyA
study: OR 40% @ 6m (CR 3%, PR 37%)
-
REASONS FOR TREATMENT FAILURE
•Pathophysiology other than immune-mediated
•Irreversible stem cell deficit
•Insufficient immunosuppression
Eltrombopag???
-
ELTROMBOPAGA Tpo-mimetic agent
-
ELTROMBOPAG IN REFRACTORY SAAThe status of art
Phase II studyn=25Refractory SAAEltrombopag 50-150 mg,
orally, for 12 weeks
44% hematological response (at least 1 lineage)
Plt response 36% Hb response 24% ANC response 36%
Increased marrow cellularity (resp.)Minimal toxicity (liver?),
no fibrosis
-
ELTROMBOPAG IN REFRACTORY SAAThe status of art
Out 11 responders 7 still on eltrombopag, showing
further improvement 4 discontinued (2 ANC responders
and 2 toxicities)
-
ELTROMBOPAG IN REFRACTORY SAAThe risk of clonal evolution
Additional 18 patients (n=43), OR 17/43 (40%)Long-term follow
up
Eltrombopag discontinued in 5 robust VGPR, with sustained
responseClonal evolution in 8/43 (18%), mostly in non-responders
(6/8); no RAEB/AML
• NR: 7-/del(7) [n=5], +8 [n=1] • R: del(13) [n=2]
CGH(SNP-based)
-
n=112
In all recent studies, the incidence of clonal evolution is
about 10-15%,
regardless the specific treatment
2003Clonal evolution (3y)•11% MDS (especially 7-)•10% PNH
Evolution to MDS (3y)•21% hATG•14% rATG
hATG x 4 (40mg/kg)
+ CsA x 6 m
NEJM 2011Blood 2012
-
ELTROMBOPAG IN SAAThe status of art
-
ELTROMBOPAG ADDED TO STANDARD IMMUNOSUPPRESSION AS FIRST
TREATMENT IN APLASTIC ANEMIA
Danielle Townsley, MDBogdan Dumitriu, MD, Phillip Scheinberg,
MD, Ronan Desmond, MD,
FRCPath, Xingmin Feng, PhD, Olga Rios, RN, Barbara Weinstein,
RN, Janet Valdez, PA-C, Thomas Winkler, MD, Marie Desierto, BS,
Harshraj Leuva,
MBBS, Colin Wu, PhD, Katherine R. Calvo, MD, PhD, Andre
Larochelle, MD, PhD, Cynthia E. Dunbar, MD and Neal S. Young,
MD
National Heart, Lung, and Blood Institute
American Society for Hematology 2015 Annual MeetingDecember 8,
2015
Courtesy of Danielle Townsley
-
STUDY DESIGNELTROMBOPAG ADDED TO IST
h-ATGDay 1 to 4
EPAG 150 mgDay 14 to 6 months
Hematologic response
EPAG 150 mgDay 14 to 3 months
CSA x 6 monthsCohort
5 yearfollow-up
EPAG 150 mgDay 1 to 6 months
clinicaltrials.gov NCT01623167
3 mo 6 mo
Courtesy of Danielle Townsley
-
57SAAWP London, 5 November 2015
EBMT studies for AAmoderate AA (EMAA) vSAA / SAA (RACE)
Primary objective PR + CR at 6 months CR at 3 months
Inclusion criteria - age > 18 years- Treatment requiring
MAA(transfusion dependency or ANC < 1G/l or Thrombo < 30G/l
or Hb < 8,5g/dl & Reti < 60G/l)
- age > 15 years- SAA/ vSAA- No primary allo-SCT
Treatment CsA + Eltrombopagversus CsA + Placebo
hATG (ATGAM) + CsA + Eltrombopagversus h ATG + CsA
EltrombopagDosage
150 mg (225 mg) 150 mg
Design Placebo controlled Open lable
Patient number 2 x 58 2 x 100
Sponsor University hospital Ulm EBMT
-
58SAAWP London, 5 November 2015
THE RACE trialA prospective Randomized multicenter study
comparing horse
Antithymocyte globuline (hATG) + Cyclosporine A (CsA)
±Eltrombopag as front-line therapy for severe aplastic anemia
patients.
PRINCIPAL INVESTIGATORS
Regis Peffault de Latour (Paris) Antonio M Risitano (Naples)
-
59Marleen van Os, Clinical Trials Coordinator, CTO Leiden, The
Netherlands [email protected] +31 71 526 1183
A prospective Randomized multicenter study comparing horse
Antithymocyte globuline (hATG) + Cyclosporine A (CsA) with or
without Eltrombopag as front-line therapy for severe aplastic
anemia patients – RACE STUDY(1)
Working party
Principal investigators Trial Coordinator
SAA-WP
Antonio M Risitano / Regis Peffault de Latour
Marleen van Os
To investigate whether Eltrombopag (Revolade,GSK) added to
standard immune-suppressivetreatment, CsA + hATG (ATGAM, Pfizer)
increasesthe rate of early complete response in untreated
AApatients*
* Patients will be stratified by age and disease severity
Participating countries
-
60
THE EBMT RACE STUDYStudy design
An EBMT Severe Aplastic Anemia Working Party study (approved by
the CTO), entirely funded by Novartis and Pfizer
Aim of the study: to improve the current standard treatment for
SAA To improve the robustness of hematological response of SAA
patients
receiving IST
Prospective, open label, phase III randomized study Control arm:
horse ATG (40 mg/kg x 4dd, iv) + cyclosporine (5 mg/kg, os)
Investigational arm: horse ATG + cyclosporine + eltrombopag
(150
mg/die, os)
Type B trial, because eltrombopag may theoretically result in a
somewhat higher risk (mostly clonal evolution) in comparison to
standard medical care
Participating centers: 30 sites from 7 EU Countries (France,
Italy, UK, Germany, Spain, Netherlands, Switzerland)
-
61
THE EBMT RACE STUDYStatistical design
Superiority studySample size calculation
Aiming to increase the 3m CR rate from 7% (Scheinberg,
Haematologica 2010)to 21% (current NIH data)
Sample size to reject the null hypothesis at 5% significance
level (alpha-error) and with 80% power (two-sided test) is n=96
patients for treatment arm
Sample size increased by 4% to compensate for possibly not
evaluable patients: total number of 200 patients (100 each arm)
Randomization 1:1 randomization, including a stratified block
design Stratification according to:
• Disease severity:− Severe aplastic anemia (SAA)− Very severe
aplastic anemia (VSAA: SAA plus ANC =15 and =40 year old
No stopping rules (study continuation led to discretion of the
DMSB)No interim analysis
-
62Marleen van Os, Clinical Trials Coordinator, CTO Leiden, The
Netherlands [email protected] +31 71 526 1183
RACE STUDY (2)SAA-WP
TREATMENT Scheme
Ste oids
Cyclosporin A
hATG
‘a do isatio
+1 // +14 // +3m +24m
Eltrombopag
Ste oids
Cyclosporin A
hATG
No CR
stop
continue
Primary endpoint 3m CR
CR
-
63
THE EBMT RACE STUDYStudy flow-chart
Initial treatment
3 month evaluation: primary endpoint
6 month evaluation: stop eltrombopag
Possible cross-over
(standard arm only)
12 month evaluation:
Relapse: possible eltrombopag
re-starting (investigational arm only)
24 month evaluation: end of the study
Randomisation
ARM A (hATG + CsA)
ARM B (hATG + CsA + Eltrombopag)
3m evaluation
6m evaluation
CR PR or NR
Stop Eltrombopag
Continue Eltrombopag
Stop Eltrombopag
Observation
CR or PR NR
Observation Salvagetreatment
CR PR or NR
Observation
Observation
Observation
Relapse (
-
64
RACE trial – participating sites
RACE trial, 11 March 2016
Country # sitesFrance 6 (6 open) +2Germany 5 (on hold)Italy 6 (2
open) +3Netherlands 4 (3 open)Spain 5 (1 open)Switzerland 1 (0
open) +1United Kingdom 5Total 32 (up to 40)
Brazil Back up site?
-
65
• 46 patients, 16 sites open (10 sites recruiting) out of 27
sites (not DE)
• Target of 50 patients (milestone Novartis) by end Oct – on
track(September 14 patients, October 10 so far)
Patient recruitment (October 10, 2016)
Patient recruitment is excellent for the
number of sites
Delays are in site opening (contracts
and regulatory hurdles) –improving
-
66
RACE trial – ancillary biological study (King’s College)
RACE trial, 11 March 2016
-
PNH MDS AML
7 8
Fixation of neutral mutation (founder effect)
vs true clonal complication
Consider oligoclonal hematopoiesis in AA due to HSC
reduction
Pre-existing vs subsequent?
CLONAL EVOLUTIONA matter of definition
-
The actual meaning of somatic mutations in hematologyDo all
mutations imply cancer (especially in marrow failure)?
-
SOMATIC MUTATION IN HSCThe lesson from ageing
17,182 individuals unselected for hematologic phenotypes
detectable mutations in 746 persons (4.3%)
Most common variants in three genes: DNMT3A, TET2, and ASXL1
The presence of a somatic mutation was associated with increased
risk:
− hematologic cancer (hazard ratio, 11.1; 95% CI 3.9-32.6)
− all-cause mortality (HR 1.4; 95% CI 1.1-1.8)
− incident coronary heart disease (HR 2.0; 95% CI 1.2-3.4)
− ischemic stroke (HR 2.6; 95% CI 1.4-4.8) Siddhartha Jaiswal et
al, Dec 2014
-
ACKNOWLEDGEMENTS
The EBMT RACE team