Embed Size (px)
Citation preview
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Head and Facial ConditionsHead and Facial Conditions
Chapter 10
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
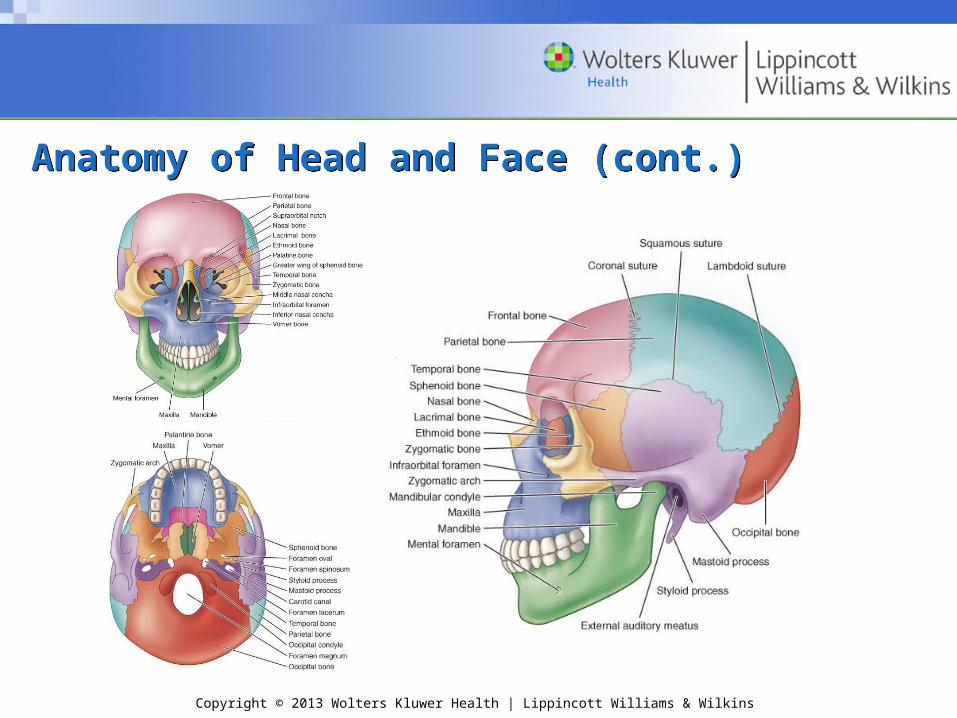
Anatomy of Head and FaceAnatomy of Head and Face• Bones of skull
– Cranium
• Protects the brain
– Facial
• Provide the structure of the face
• Form the sinuses, orbits of the eyes, nasal cavity, and the mouth
• Scalp
– Protective function
– Extensive blood supply
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy of Head and Face (cont.)Anatomy of Head and Face (cont.)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy of Head and Face (cont.)Anatomy of Head and Face (cont.)
• Brain– Major regions
• Cerebral hemispheres• Diencephalon• Brainstem• Cerebellum
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy of Head and Face (cont.)Anatomy of Head and Face (cont.)
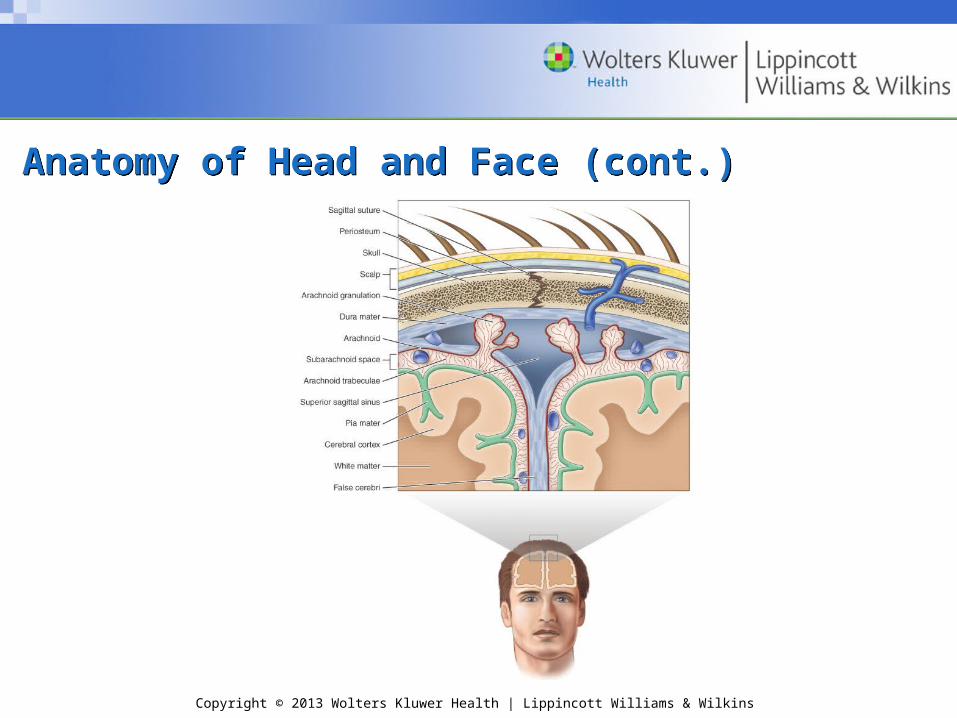
• Meninges
• Protective tissue that encloses brain and spinal cord
• Dura mater; arachnoid mater; pia mater
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy of Head and Face (cont.)Anatomy of Head and Face (cont.)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy of Head and Face (cont.)Anatomy of Head and Face (cont.)
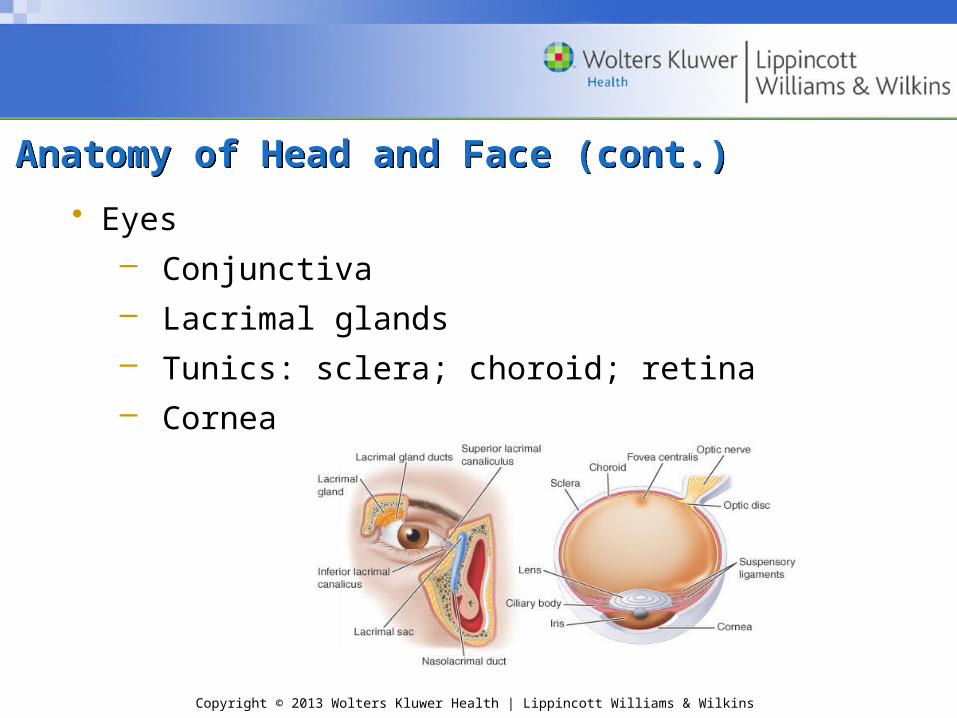
• Eyes– Conjunctiva– Lacrimal glands– Tunics: sclera; choroid; retina– Cornea
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy of Head and Face (cont.)Anatomy of Head and Face (cont.)
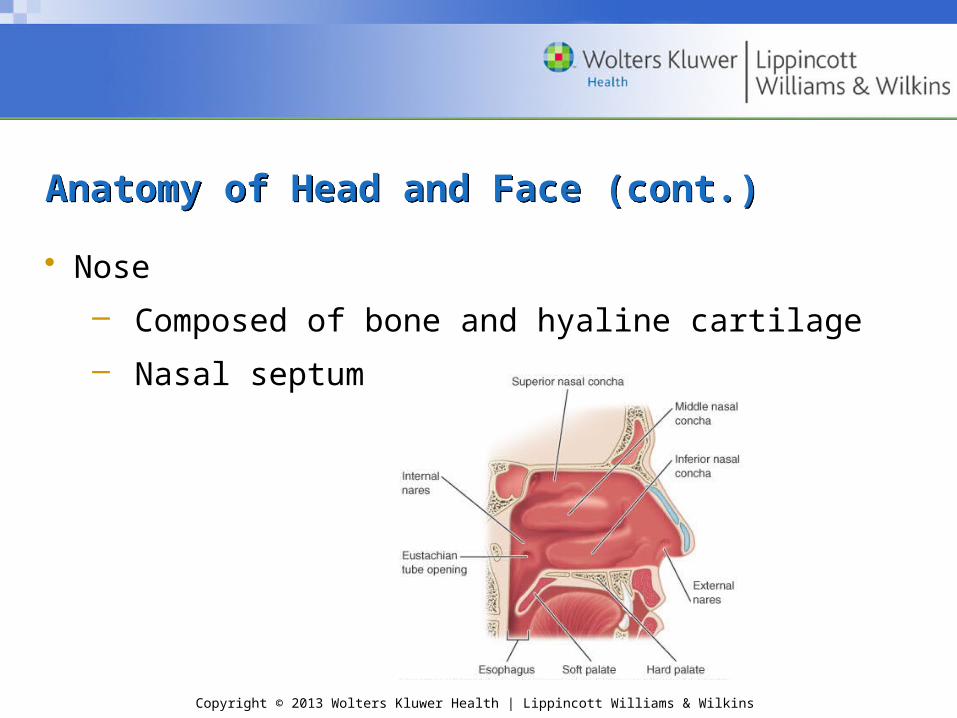
• Nose
– Composed of bone and hyaline cartilage
– Nasal septum
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy of Head and Face (cont.)Anatomy of Head and Face (cont.)
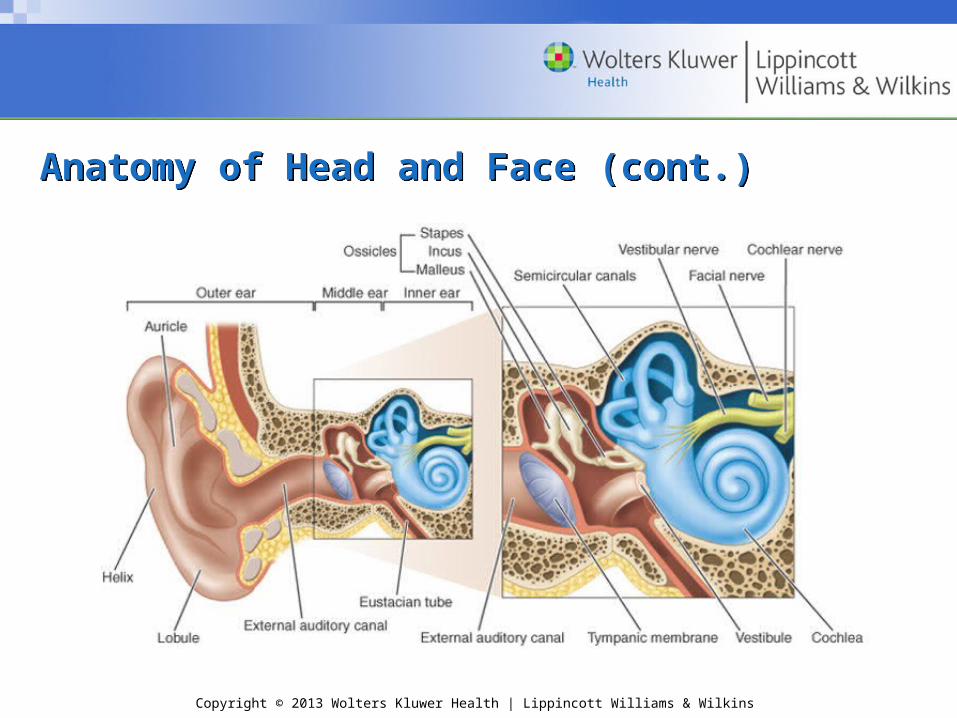
• Ear
– Major areas
• Outer ear (auricle and external auditory canal)
• Middle ear (tympanic membrane)
• Inner ear (labyrinth)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy of Head and Face (cont.)Anatomy of Head and Face (cont.)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy of Head and Face (cont.)Anatomy of Head and Face (cont.)
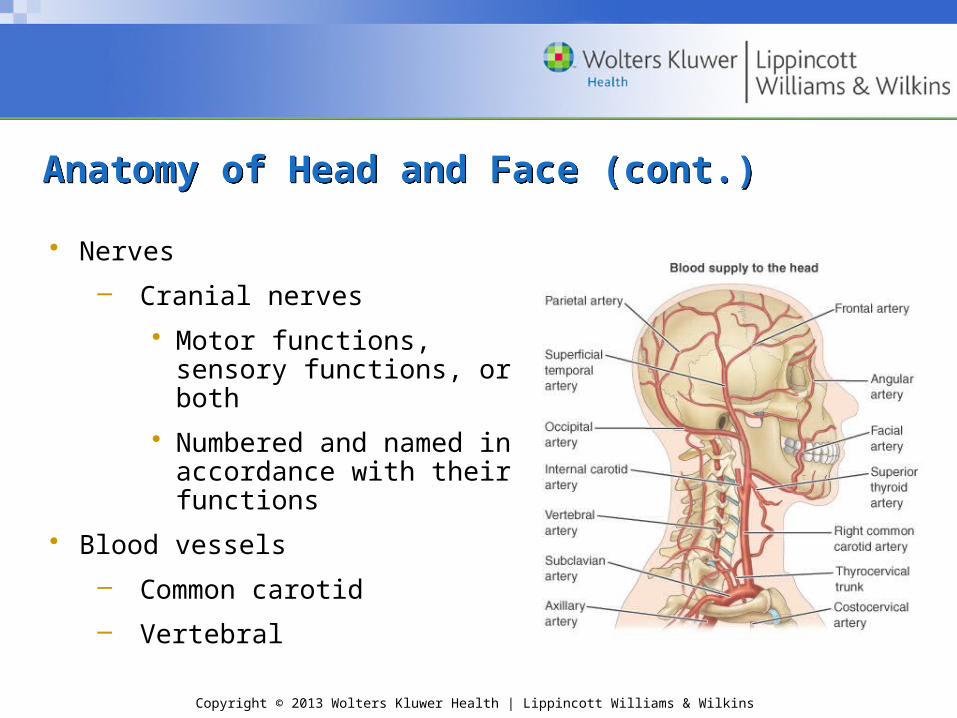
• Nerves
– Cranial nerves
• Motor functions, sensory functions, or both
• Numbered and named in accordance with their functions
• Blood vessels
– Common carotid
– Vertebral
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Prevention of Head and Facial InjuriesPrevention of Head and Facial Injuries
• Protective equipment
– Helmets
– Face guards
– Mouth guards
– Eye wear
– Ear wear
– Throat protectors
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Scalp InjuriesScalp Injuries
• Highly vascularized; bleeds freely
• Laceration
– Control bleeding
– Prevent contamination
– Assess for skull fracture (fx)
– Management:
• If no fx, cleanse, cover, and refer
• Abrasions and contusions
– Cleanse; ice and pressure
– 24 hours: no improvement – refer
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
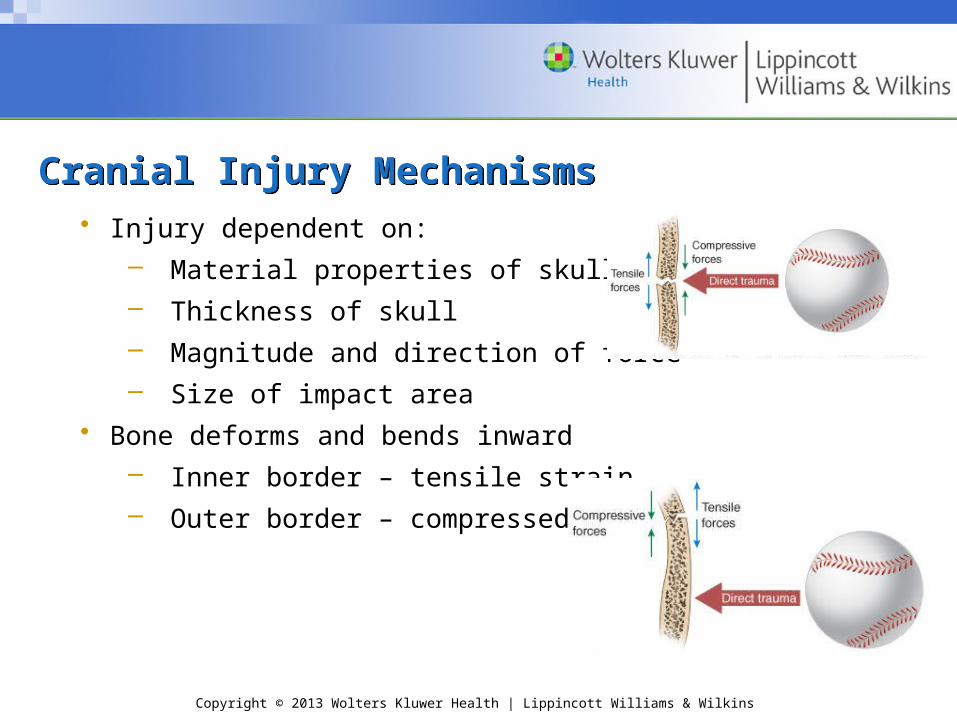
Cranial Injury MechanismsCranial Injury Mechanisms• Injury dependent on:
– Material properties of skull– Thickness of skull– Magnitude and direction of force– Size of impact area
• Bone deforms and bends inward– Inner border – tensile strain– Outer border – compressed
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cranial Injury Mechanisms (cont.)Cranial Injury Mechanisms (cont.)
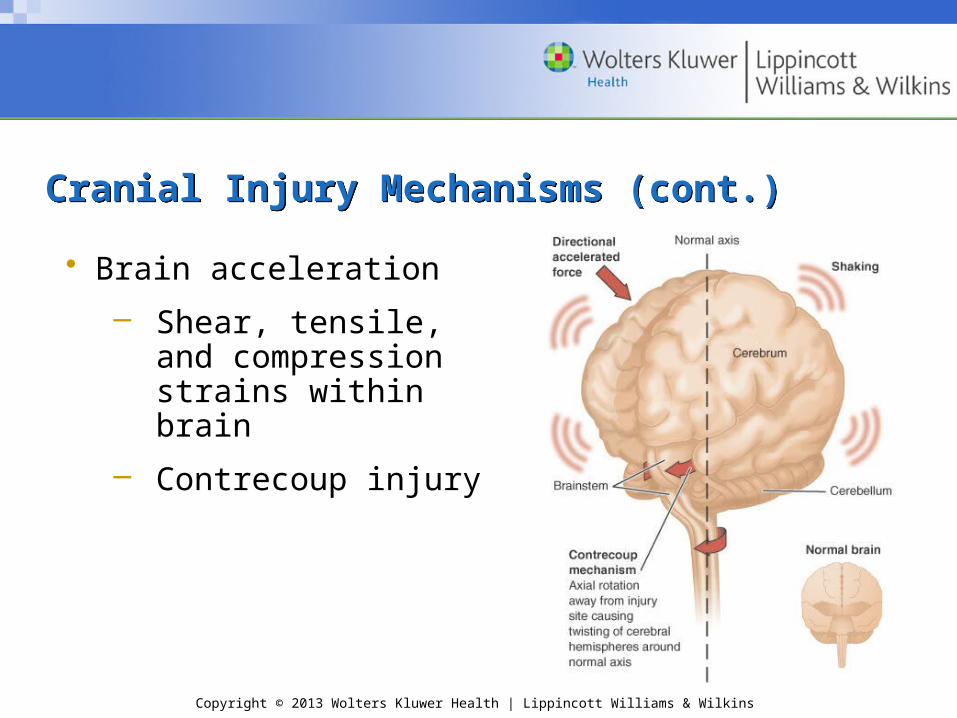
• Brain acceleration
– Shear, tensile, and compression strains within brain
– Contrecoup injury
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cranial Injury Mechanisms (cont.)Cranial Injury Mechanisms (cont.)
• Focal injury
– Localized damage
– Epidural, subdural, or intracerebral hematomas
• Diffuse injury
– Widespread disruption
– Concussion
• Accurate assessment of head injury is essential
• Conscious, ambulatory individual should not be considered to have only a minor injury
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
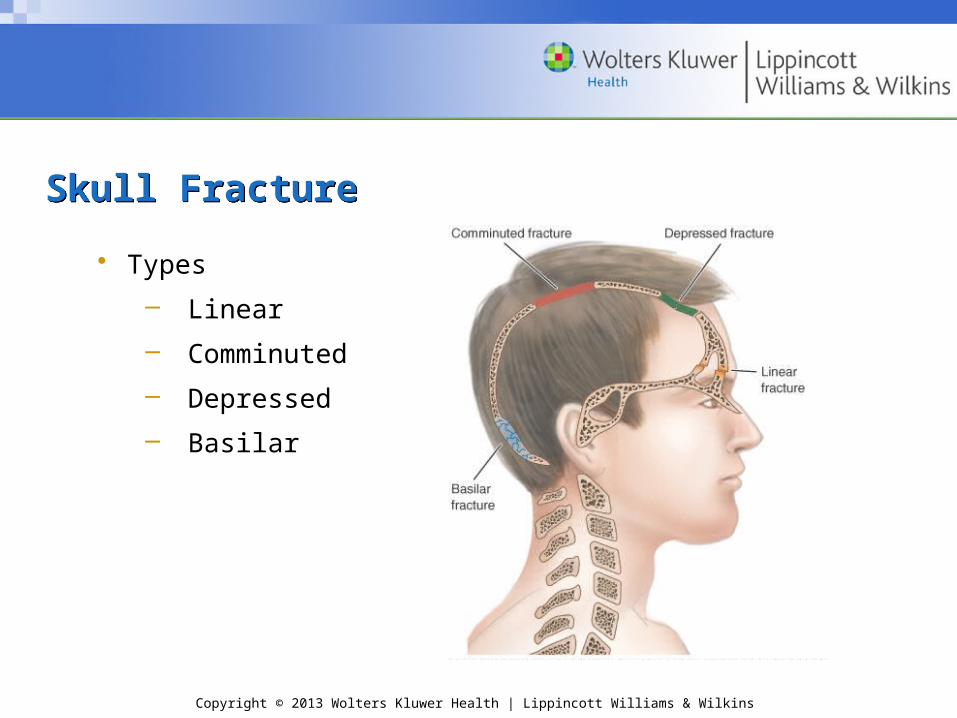
Skull FractureSkull Fracture
• Types
– Linear
– Comminuted
– Depressed
– Basilar
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Skull Fracture (cont.)Skull Fracture (cont.)
• Potential for varying signs and symptoms (S&S)
– Visible deformity–do not be misled by a “goose egg”; a fracture may be under the site
– Deep laceration or severe bruise to scalp
– Palpable depression or crepitus
– Unequal pupils
– Raccoon eyes or Battle’s sign
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Skull Fracture (cont.)Skull Fracture (cont.)
– Bleeding or CSF from nose and/or ear
– Loss of smell
– Loss of sight or major vision disturbances
– Unconsciousness 2 minutes after direct trauma to the head
• Management: activation of EMS (refer to Application Strategy 10.1)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Focal Cerebral ConditionsFocal Cerebral Conditions
• Epidural hematoma
– Direct blow to side of head
– Meningeal artery tear
– Rapid “high-pressure” hematoma
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Focal Cerebral Conditions (cont.)Focal Cerebral Conditions (cont.)
• Epidural hematoma (cont.)– S&S
• LOC• Lucid interval • Gradual deterioration
Head pain, dizziness, nausea, dilation of one pupil, sleepiness
• Possible: Deteriorating consciousness, neck rigidity,
depression of pulse and respiration, convulsions
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Focal Cerebral Conditions (cont.)Focal Cerebral Conditions (cont.)
• Epidural hematoma (cont.)
– Life threatening … death
– Management: activate EMS; ABCs, vitals, shock
– Requires surgical decompression
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Focal Cerebral Conditions (cont.)Focal Cerebral Conditions (cont.)
• Subdural hematoma
– Acceleration forces
– Involves bleeding of the veins
– S&S slower to develop
• Acute – 48-72 hours post-injury
• Chronic – later time frame
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
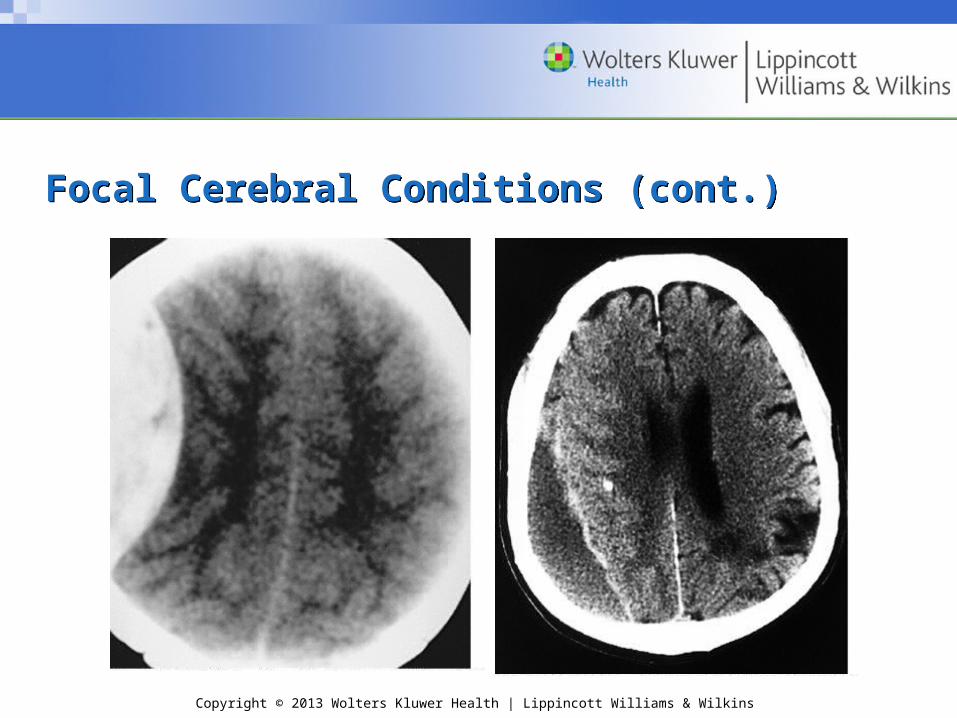
Focal Cerebral Conditions (cont.)Focal Cerebral Conditions (cont.)• Subdural hematoma (cont.)
– Simple • Blood in subdural space—no injury to cerebrum
– Complicated • Cerebral swelling
– S&S • Headache, nausea, dizziness, sleepiness• simple – usually no LOC• complicated – unconscious, pupil dilation on one side
– Management: activate EMS; ABCs, vitals, shock
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Focal Cerebral Conditions (cont.)Focal Cerebral Conditions (cont.)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Focal Cerebral Conditions (cont.)Focal Cerebral Conditions (cont.)
• Cerebral contusion
– Focal injury, without mass-occupying lesion
– Acceleration-deceleration
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Focal Cerebral Conditions (cont.)Focal Cerebral Conditions (cont.)
• Cerebral contusion (cont.)– S&S (can vary greatly)
• Develop over hours and days• Normal function or neurologic deterioration• Danger sign:
Neurological exam—normal But presence of headaches, dizziness, and
nausea– Management: activate EMS; ABCs, vitals, shock
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Diffuse Cerebral ConditionsDiffuse Cerebral Conditions
• Concussion– common features incorporate clinical, pathological, &
biomechanical injury constructs• caused by direct blow to head, face, neck, or elsewhere with
an impulsive force transmitted to head; typically result in rapid onset of short-lived impairment of neurologic function that resolves spontaneously.
• neuropathologic changes may occur, but acute clinical symptoms typically reflect a functional disturbance rather than a structural injury.
• may or may not involve an LOC …may lead to a gradient of clinical symptoms associated with grossly normal structural neuroimaging studies.
• resolution of the clinical and cognitive symptoms usually follows a sequential course
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Diffuse Cerebral Conditions (cont.)Diffuse Cerebral Conditions (cont.)
• Classification of concussion
– Numerous!!! …potentially problematic!
– Zurich panel 2008
• diagnosis of a concussion will involve the assessment of a range of clinical signs and symptoms in four categories: physical, emotional, cognitive, and sleep
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
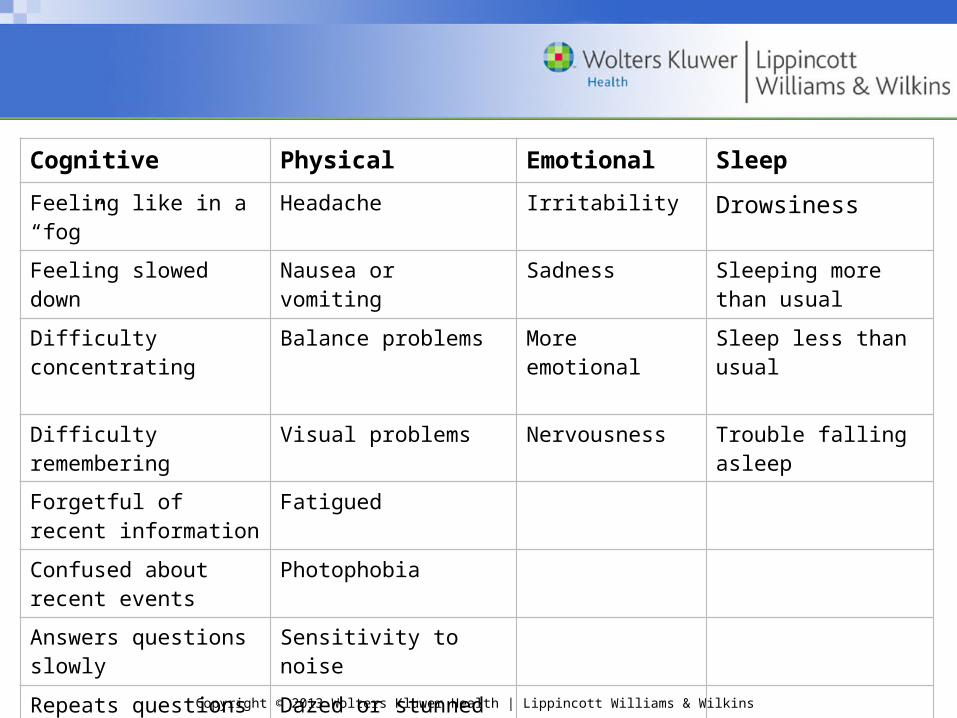
Cognitive Physical Emotional Sleep
Feeling like in a “fog” Headache Irritability Drowsiness
Feeling slowed down Nausea or vomiting Sadness Sleeping more than usual
Difficulty concentrating
Balance problems More emotional Sleep less than usual
Difficulty remembering
Visual problems Nervousness Trouble falling asleep
Forgetful of recent information
Fatigued
Confused about recent events
Photophobia
Answers questions slowly
Sensitivity to noise
Repeats questions Dazed or stunned
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Diffuse Cerebral Conditions (cont.)Diffuse Cerebral Conditions (cont.)
– On-field management
• Remove from activity; examine immediately –standard emergency assessment & management
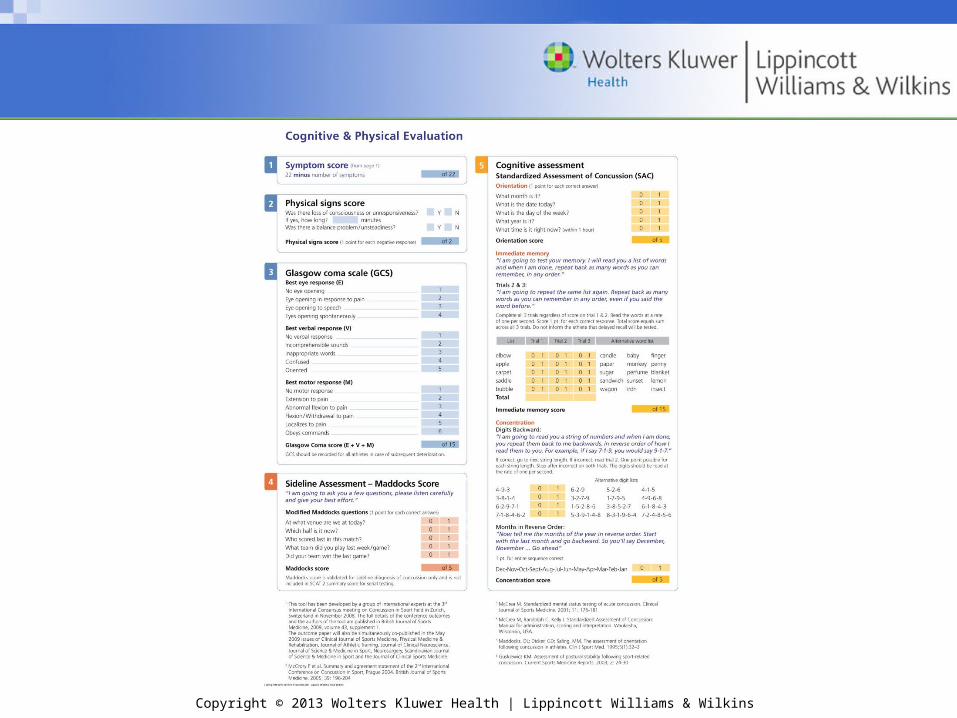
• Detailed clinical assessment of signs and symptoms using SCAT 2 or similar tool
• Presence of any signs/ symptoms – initiate appropriate management
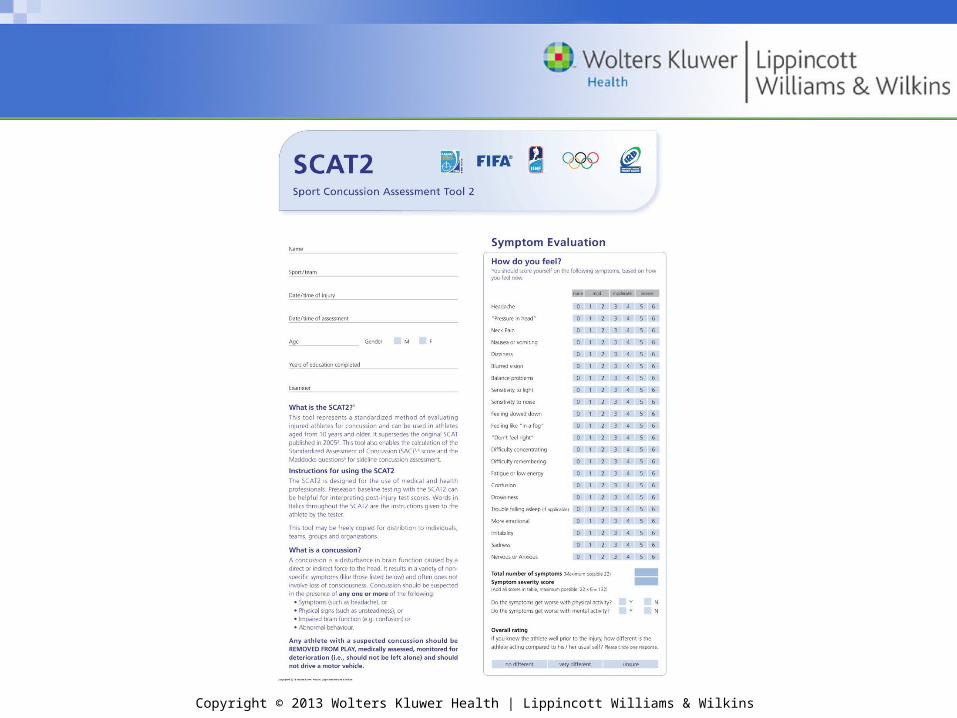
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Diffuse Cerebral Conditions (cont.)Diffuse Cerebral Conditions (cont.)
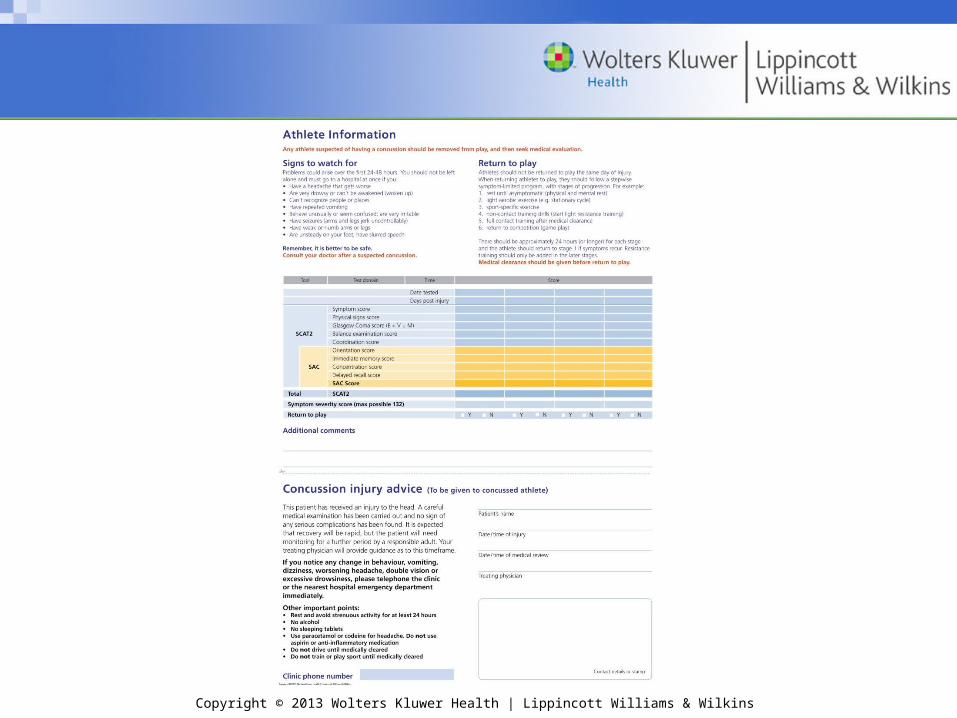
Return to activity after a concussion follows a sequential process:
1. No activity, complete rest; once asymptomatic, proceed to step 2
2. Light aerobic exercise such as walking or stationary cycling; no resistance training
3. Sport-specific exercise (e.g., skating in hockey, running in soccer);
4. Noncontact training drills; Progression to more complex training drills; may start progressive resistance training
5. Full-contact practice -- after medical clearance6. RTP – normal game play
(Refer to Table 10.4)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Diffuse Cerebral Conditions (cont.)Diffuse Cerebral Conditions (cont.)• Posttraumatic headache
– Result of vasospasm; doesn’t usually occur with impact, but develops shortly afterward
– S&S
• Localized area of blindness that may follow the appearance of brilliantly colored shimmering lights
• Posttraumatic migraines
– Management
• Immediate referral to a physician
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Diffuse Cerebral Conditions (cont.)Diffuse Cerebral Conditions (cont.)• Postconcussion syndrome
– Can occur following a mild or serious concussion– S&S
• Decreased attention span• Persistent headaches• Blurred vision• Vertigo• Memory loss• Irritability• Inability to concentrate on even simplest task• Exercise may lead to headache, dizziness, and
premature fatigue – Management
• No definitive treatment other than treat headache symptoms
• No activity
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Diffuse Cerebral Conditions (cont.)Diffuse Cerebral Conditions (cont.)
• Second impact syndrome– A second head injury before the symptoms
associated with a previous one have totally resolved
– Does not necessarily require a blow to the head
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Diffuse Cerebral Conditions (cont.)Diffuse Cerebral Conditions (cont.)
• Second impact syndrome (cont.)– S&S
• May not lose consciousness; stunned look; may leave field under own power
• Rapid deterioration of condition LOC, dilated pupils, loss of eye movement,
respiratory failure– Brainstem failure in 2-5 minutes– Management
• Activate EMS – Prevent it from happening!!!
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Cranial ConditionsAssessment of Cranial Conditions
• ALWAYS ASSUME A CERVICAL INJURY IS PRESENT!!!!!!!!!!!!!
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Cranial Conditions (cont.)Assessment of Cranial Conditions (cont.)
• Vitals– Pulse
• Small weak pulse • Short, rapid weak pulse • Slow bounding pulse • Accelerated pulse
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Cranial Conditions (cont.)Assessment of Cranial Conditions (cont.)
– Respiration • Slow breathing (bradypnea)• Cheyne-Stokes breathing • Ataxic (Biot’s) breathing• Apneustic breathing
– Blood pressure• Increase in the systolic blood pressure or a decrease in
the diastolic blood pressure indicates rising intracranial pressure
– Pulse pressure• >50 mm Hg indicates increased intracranial bleeding
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Cranial Conditions (cont.)Assessment of Cranial Conditions (cont.)
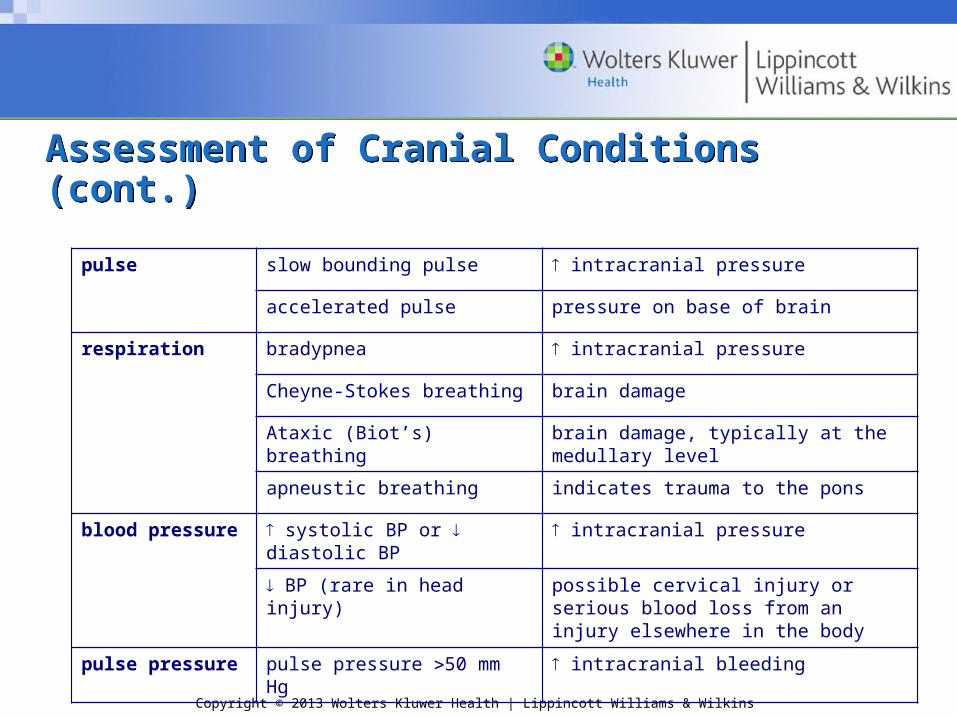
pulse slow bounding pulse intracranial pressure
accelerated pulse pressure on base of brain
respiration bradypnea intracranial pressure
Cheyne-Stokes breathing brain damage
Ataxic (Biot’s) breathing brain damage, typically at the medullary level
apneustic breathing indicates trauma to the pons
blood pressure systolic BP or diastolic BP intracranial pressure
BP (rare in head injury) possible cervical injury or serious blood loss from an injury elsewhere in the body
pulse pressure pulse pressure 50 mm Hg intracranial bleeding
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Cranial Conditions (cont.)Assessment of Cranial Conditions (cont.)
• History and mental status testing
– Orientation
– Concentration
– Memory
– Behavior
– Symptoms
– Loss of consciousness
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Cranial Conditions (cont.)Assessment of Cranial Conditions (cont.)• Observation and inspection
– Leakage of cerebrospinal fluid
– Signs of trauma (deformity, body posturing, raccoon eyes, and Battle’s sign)
– Skin color
– Loss of emotional control (irritability, aggressiveness, or uncontrolled crying)
– Graded symptom checklist
• Palpation
– Bony and soft tissue structures for point tenderness, crepitus, depressions, elevations, swelling, blood, or changes in skin temperature
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Cranial Conditions (cont.)Assessment of Cranial Conditions (cont.)• Neurologic examination
– Cranial nerve assessment
– Pupil abnormalities
• Pupil size
• Response to light
• Eye movement
• Nystagmus
• Blurred or double vision
– Babinski’s reflex
– Strength
– Neuropsychological assessments
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Cranial Conditions (cont.)Assessment of Cranial Conditions (cont.)
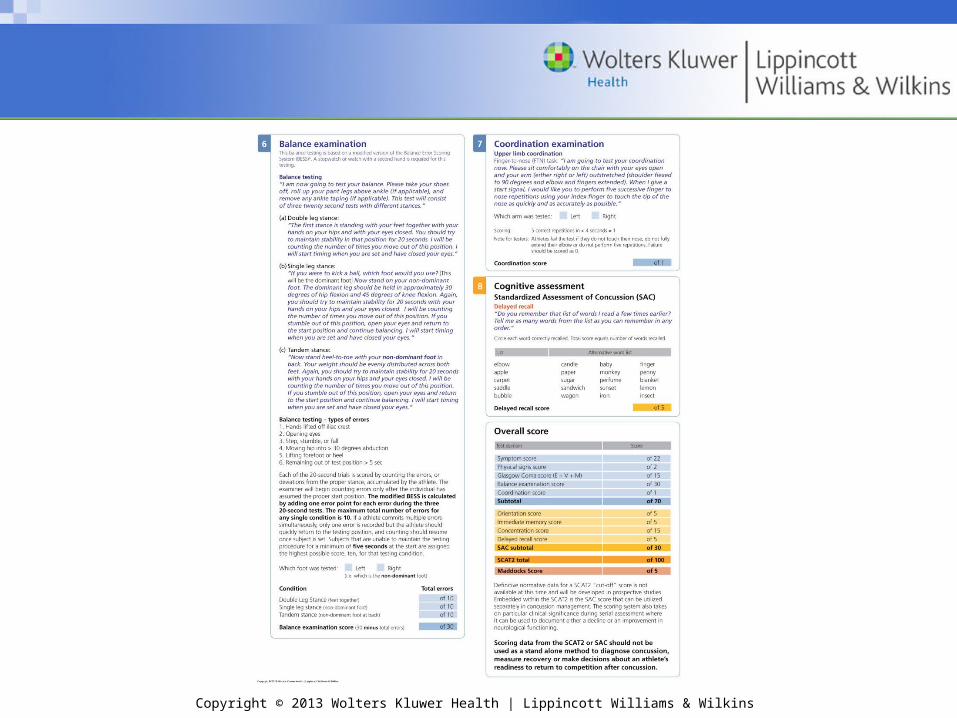
– Coordination and balance
• Finger to nose test
• Gait
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Cranial Conditions (cont.)Assessment of Cranial Conditions (cont.)• Romberg test
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Cranial Conditions (cont.)Assessment of Cranial Conditions (cont.)
• One-legged stork stand
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
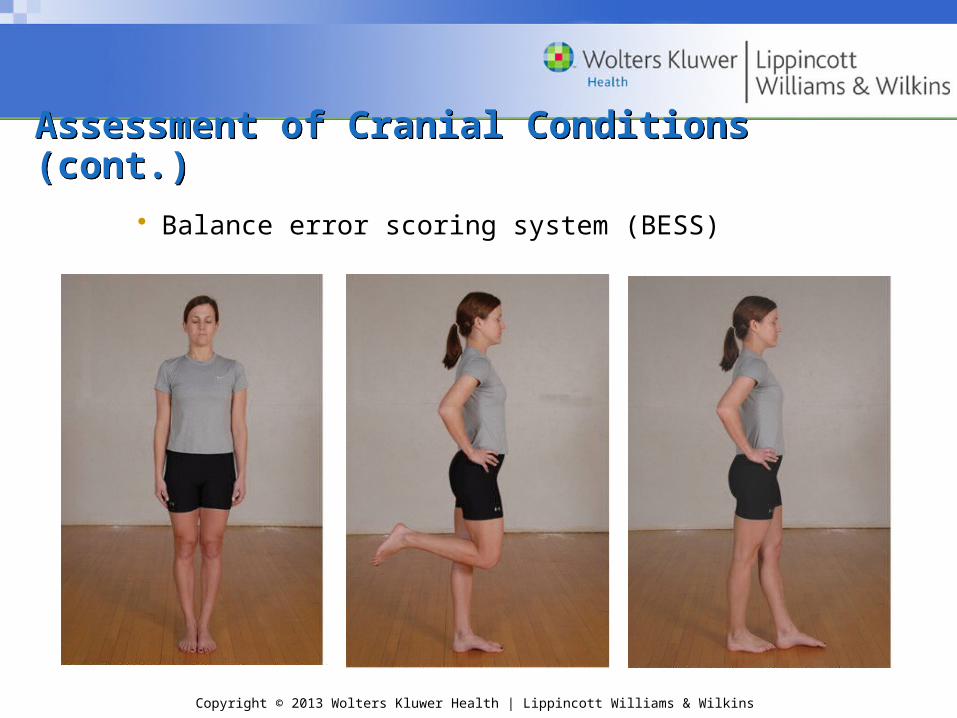
Assessment of Cranial Conditions (cont.)Assessment of Cranial Conditions (cont.)• Balance error scoring system (BESS)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Cranial Conditions (cont.)Assessment of Cranial Conditions (cont.)
• External provocative test
– 40-yard sprint
– 5 sit-ups
– 5 push-ups
– 5 knee bends
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Cranial Conditions (cont.)Assessment of Cranial Conditions (cont.)
• Determination of findings
– Re-assess every 5-7 minutes
– Immediate management and follow-up care
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Facial ConditionsFacial Conditions
• Facial soft tissue conditions– Contusions, abrasions, and lacerations are
managed the same as elsewhere on the body – Complicated injuries—immediate physician
referral
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Facial Conditions (cont.)Facial Conditions (cont.)• Temporomandibular joint conditions
– S&S
• Inability to open and/or close mouth (dislocation and meniscus displacement)
• Malocclusion
• Joint crepitus with opening and closing
• Pain with opening and biting
• Deviation of the mandible on opening (toward side of injury)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Facial Conditions (cont.)Facial Conditions (cont.)
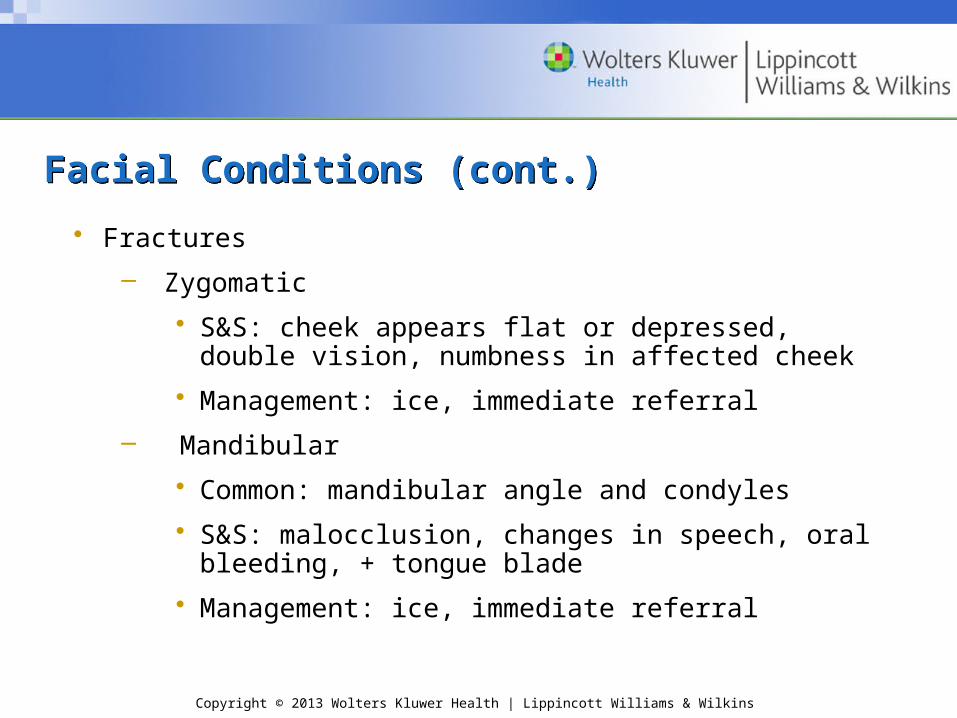
• Fractures
– Zygomatic
• S&S: cheek appears flat or depressed, double vision, numbness in affected cheek
• Management: ice, immediate referral
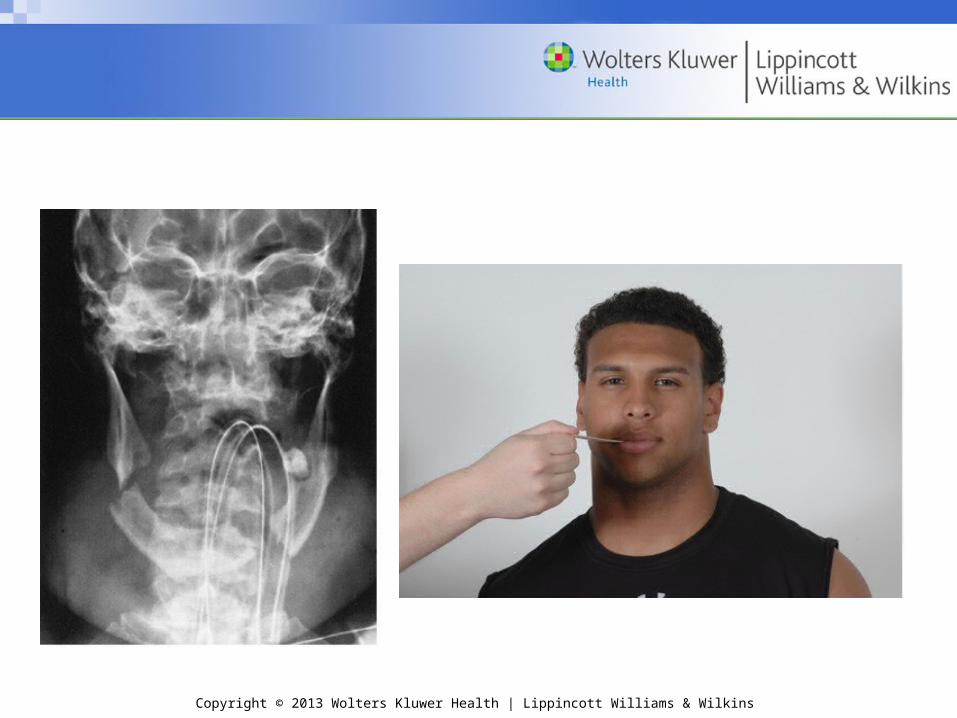
– Mandibular
• Common: mandibular angle and condyles
• S&S: malocclusion, changes in speech, oral bleeding, + tongue blade
• Management: ice, immediate referral
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
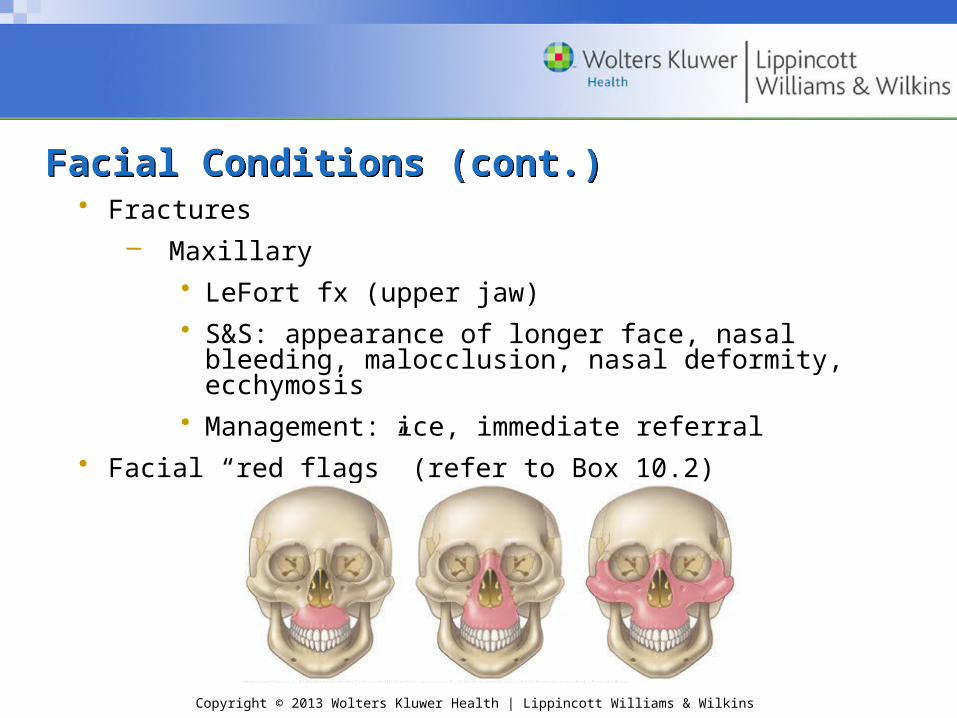
Facial Conditions (cont.)Facial Conditions (cont.)• Fractures
– Maxillary • LeFort fx (upper jaw)• S&S: appearance of longer face, nasal bleeding,
malocclusion, nasal deformity, ecchymosis• Management: ice, immediate referral
• Facial “red flags” (refer to Box 10.2)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Nasal ConditionsNasal Conditions• Epistaxis
– Anterior – bleeding from anterior septumPosterior – bleeding from lateral wall
– Management: ice, mild pressure, slight forward head tilt; nasal plug; 5 minutes – physician referral
• Deviated septum
– S&S
• Consistent difference in airflow between the 2 sides of the nose when one nostril is blocked
• Confirm using otoscope
– Management: physician referral
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Nasal Conditions (cont.)Nasal Conditions (cont.)• Fractures
– Most common: lateral displacement
– Range of severity varies
– S&S
• Asymmetry – especially with lateral force
• Epistaxis
• Crepitus
– Management: control bleeding; refer
• Nasal “red flags” (refer to Box 10.3)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Oral and Dental ConditionsOral and Dental Conditions
• Periodontal disease– S&S of gingivitis
• Tender, swollen, or bleeding gums• Change in the gums' color from pink to dusky
red• Plaque and bacteria that cover the teeth not
readily visible
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Oral and Dental Conditions (cont.)Oral and Dental Conditions (cont.)
– S&S of periodontitis • Swollen or recessed gums• Unpleasant taste in the mouth• Bad breath• Tooth pain• Drainage or pus around one or more teeth
– Management: referral to dentist
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Oral and Dental Conditions (cont.)Oral and Dental Conditions (cont.)
• Dental caries (tooth decay)
– Primarily caused by plaque...dissolves the tooth enamel…allows bacteria to infect the center of the tooth
– S&S
• Pain during chewing
• Sensitivity to hot/cold foods and beverages
• If tooth abscess is present:
Throbbing pain
Sharp or shooting pain
– Management: refer to dentist
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Oral and Dental Conditions (cont.)Oral and Dental Conditions (cont.)
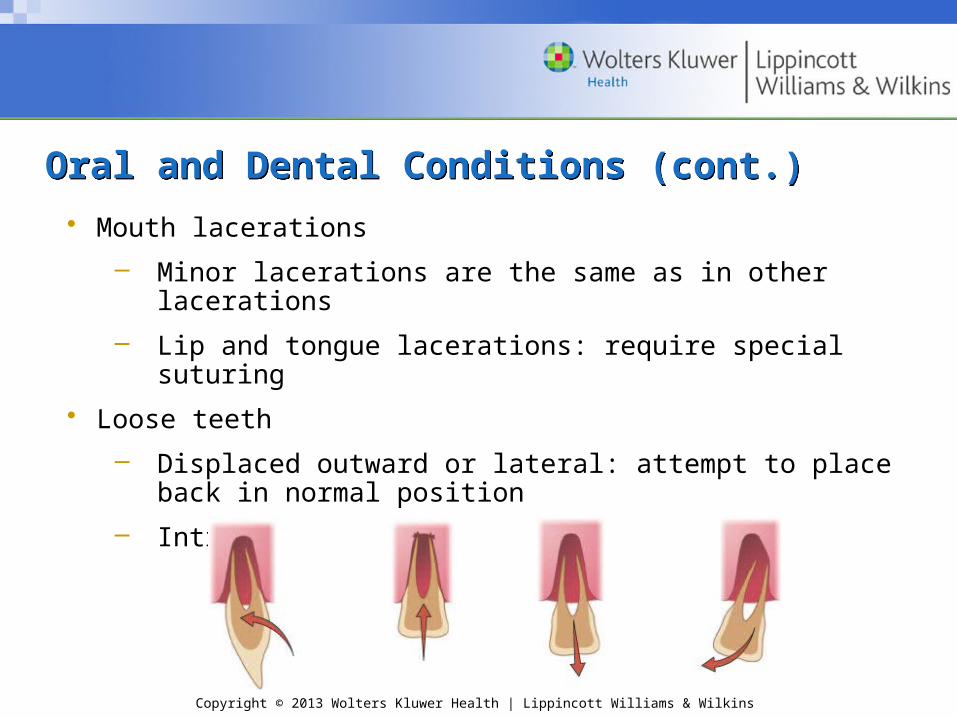
• Mouth lacerations
– Minor lacerations are the same as in other lacerations
– Lip and tongue lacerations: require special suturing
• Loose teeth
– Displaced outward or lateral: attempt to place back in normal position
– Intruded: immediate referral to dentist
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Oral and Dental Conditions (cont.)Oral and Dental Conditions (cont.)
• Fractured tooth
– Enamel: no symptoms
– Dentin: pain and increased sensitivity to heat and cold
– Pulp or root: severe pain and sensitivity
– Management: refer to dentist
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Oral and Dental Conditions (cont.)Oral and Dental Conditions (cont.)
• Dislocated tooth
– Time is of the essence; refer
– Hold tooth by crown
– Do not rub the tooth or remove any dirt; milk or saline
• Oral and dental “red flags” (refer to Box 10.4)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Ear ConditionsEar Conditions
• Cauliflower ear (auricular hematoma)
– Repeated trauma pulls cartilage away from perichondrium – hematoma forms
– Untreated – forms a fibrosis
– Management: ice; possible aspiration by physician
– Key is prevention!
• Impacted cerumen (wax)
– Possible hearing loss or muffled hearing
– Management: irrigate canal with warm water
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Ear Conditions (cont.)Ear Conditions (cont.)
• Otitis externa (swimmer’s ear)
– Bacterial infection to lining of external auditory canal
– S&S: pain, itching
– Management: ear drops, custom ear plugs
• Otitis media
– Middle ear infection due to bacteria or virus
– S&S: earache, hearing difficulty, possible serous otitis
– Management: physician referral
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Ear Conditions (cont.)Ear Conditions (cont.)
• Tympanic membrane rupture– Caused by:
• Infection • Direct trauma • Changes in pressure • Loud, sudden noises • Foreign objects in the ear
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Ear Conditions (cont.)Ear Conditions (cont.)– S&S
• Very painful• Tinnitus• Pus-filled or bloody drainage from the ear• Sudden decrease in ear pain followed by
drainage• Hearing loss
– Management: physician referral• Ear “red flags” (refer to Box 10.5)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Eye ConditionsEye Conditions
• Preorbital ecchymosis (black eye)
– Assessment
– Management: ice, referral to ophthalmologist
• Foreign bodies
– S&S: intense pain, tearing
– Management
• Not embedded: removal, inspection
• Embedded: do not touch, activate EMS
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Eye Conditions (cont.)Eye Conditions (cont.)
• Sty
– Infection of sebaceous gland of eyelash
– Starts as a red nodule; progresses into a painful pustule
– Management: moist heat compress
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Eye Conditions (cont.)Eye Conditions (cont.)• Conjunctivitis (pink eye)
– S&S: itching, burning, watering, red appearance
– Management: infectious; refer to physician
• Corneal abrasion
– S&S: pain, tearing, photophobia, irritated with blinking and eye movement, feeling of “something in the eye”
– Management: drops and eye patch
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Eye Conditions (cont.)Eye Conditions (cont.)
• Corneal laceration
– S&S: severe pain, decreased visual acuity
– Management: cover with no pressure, activate EMS, transport supine or upright
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
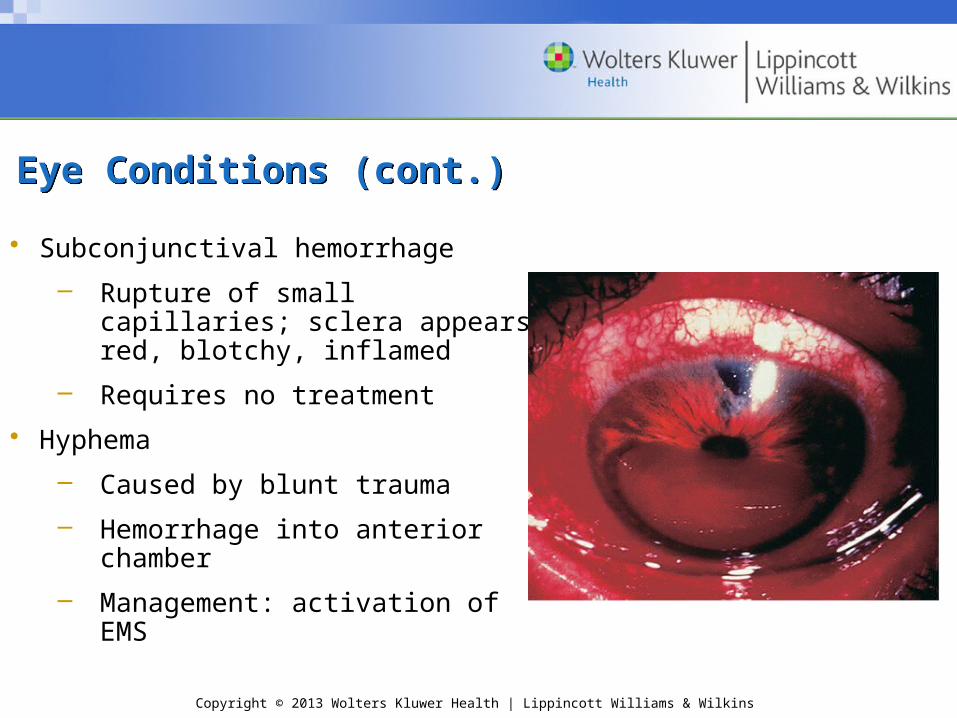
• Subconjunctival hemorrhage
– Rupture of small capillaries; sclera appears red, blotchy, inflamed
– Requires no treatment
• Hyphema
– Caused by blunt trauma
– Hemorrhage into anterior chamber
– Management: activation of EMS
Eye Conditions (cont.)Eye Conditions (cont.)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Eye Conditions (cont.)Eye Conditions (cont.)
• Detached retina– Can occur with or without trauma– S&S: floaters and light flashes– Management: patch both eyes; refer to
ophthalmologist
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Eye Conditions (cont.)Eye Conditions (cont.)
• Orbital “blowout” fracture– Impact from a blunt object, usually larger than the eye
orbit – S&S:
• Diplopia• Numbness below eye• Lack of eye movement• Recessed downward displacement of globe
– Management: ice; immediate referral to physician• Eye “red flags” (refer to Box 10.6)