Embed Size (px)
Citation preview

Copyright © 2010, Research To Practice, All rights reserved.
Part I: Myelodysplastic Syndromes/Acute Myeloid Leukemia Monday, September 20, 20107:30 PM - 8:30 PM ET
Monday Night with Research To Practice: An 8-Part Live CME Webcast Series


Mikkael A Sekeres, MD, MSAssociate Professor of MedicineDirector, Leukemia ProgramTaussig Cancer InstituteDepartment of Hematologic Oncology and Blood DisordersCleveland, Ohio
Hagop M Kantarjian, MDChairman and Professor, Leukemia DepartmentThe University of Texas MD Anderson Cancer CenterHouston, Texas
Neil Love, MDModeratorResearch To PracticeMiami, Florida

Disclosures for Moderator Neil Love, MD
Dr Love is president and CEO of Research To Practice, which receives funds in the form of educational grants to develop CME activities from the following commercial interests: Abraxis BioScience, Allos Therapeutics, Amgen Inc, AstraZeneca Pharmaceuticals LP, Aureon Laboratories Inc, Bayer HealthCare Pharmaceuticals/Onyx Pharmaceuticals Inc, Biogen Idec, Boehringer Ingelheim Pharmaceuticals Inc, Bristol-Myers Squibb Company, Celgene Corporation, Cephalon Inc, Eisai Inc, EMD Serono Inc, Genentech BioOncology, Genomic Health Inc, Genzyme Corporation, Lilly USA LLC, Millennium Pharmaceuticals Inc, Monogram BioSciences Inc, Myriad Genetics, Inc, Novartis Pharmaceuticals Corporation, OSI Oncology, Sanofi-Aventis and Spectrum Pharmaceuticals Inc.

Disclosures for Mikkael A Sekeres, MD, MS
N/A = Not Applicable
Advisory Committee Celgene Corporation, Seattle Genetics
Paid Research N/A
Speakers Bureau Celgene Corporation

Disclosures for Hagop M Kantarjian, MD
Advisory Committee N/A
Paid ResearchBristol-Myers Squibb Company, Genzyme Corporation, Novartis Pharmaceuticals Corporation
Speakers Bureau N/A
N/A = Not Applicable

Myelodysplastic Syndromes (MDS)
• Case 1: 71-year-old man with MDS and pancytopenia 2 years after initial growth factor treatment - Dr Sekeres
• Case 2: 79-year-old man with 5q minus MDS - Dr Kantarjian
Acute Myeloid Leukemia (AML)
• Case 1: An otherwise healthy 82-year-old man presenting with AML - Dr Sekeres
• Case 2: 64-year-old man with FLT3+ AML - Dr Kantarjian

Case History: Dr Sekeres
• 71-yo man with fatigue and isolated anemia
• Bone marrow biopsy: hypercellular marrow; 20% dysplastic erythroid precursors, < 5% blasts
• Normal cytogenetics
• Serum erythropoietin level 80mU/mL (normal 4-24 mU/mL)
• IPSS 0

0%
8%
9%
53%
30%
0% 10% 20% 30% 40% 50% 60%
Nothing – I would choose watchful waiting
An erythropoiesis stimulating agent, such as erythropoietin
or darbepoetin
Lenalidomide
Azacitidine
Decitabine
1) What therapy would you recommend for this patient?

Case History: Dr Sekeres (continued)
• Patient treated with darbepoetin
• Hemoglobin improved to 11-12 g/dL
• After 2-3 years, developed pancytopenia
• Bone marrow biopsy: 8% myeloblasts
• Cytogenetics: Del 20q
• IPSS 1.0

2) What therapy would you now recommend for this patient?
Nothing – I would choose watchful waiting
Continue the erythropoiesis stimulating agent
Lenalidomide
Azacitidine
Decitabine 6%
57%
16%
20%
1%
0% 10% 20% 30% 40% 50% 60%

Case History: Dr Sekeres (continued)
• Patient treated with SC azacitidine days 1-6 q 4-weeks
• CBC showed objective hematologic improvement (HI) after cycle 4
• Repeat bone marrow evaluation after four cycles: < 5% blasts
• After cycle 7, CBC normalized, and azacitidine administration frequency changed to q 5-weeks
• After 2 years, blood counts dropped• Bone marrow aspirate and biopsy: 40% blasts• Cytogenetics: Del 20q plus Trisomy 8

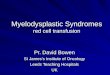
Slide courtesy of David Steensma
5-9% Blasts
10-19% Blasts
>20% Blasts = AML!
Lower Risk
Lower Risk

Copyright © 2010, Research To Practice, All rights reserved.
Characteristics of US Patients With Myelodysplastic Syndromes: Results of Six Cross-sectional Physician Surveys
Sekeres MA et al.J Natl Cancer Inst 2008;100(21):1542-51.

Age (Median) Newly diagnosed 71 years
Established 72-75 years
Sex (Mean)Male (Newly diagnosed)
(Established)
55%
51-57%
Duration of MDS
(Median)13-16 months
MDS Status Primary 88 – 93%
Secondary 7 – 12%
Secondary Chemotherapy 55 – 80%
Cause Radiation 6 – 21%
Chemical exposure 2 – 9%
US MDS Characteristics
Sekeres et al. J National Cancer Inst 2008;100:1542

Copyright © 2010, Research To Practice, All rights reserved.
Perceptions of Disease State, Treatment Expectations, and Prognosis Among Patients with Myelodysplastic Syndromes
Sekeres MA et al.
Proc ASH 2009;Abstract 1771.

Disease Understanding Among Patients with MDS
• 6%-7% recognized this as "cancer" or leukemia
• More than half did not understand the treatment goal or recall prognosis being discussed
• Mixed perceptions of curability
Sekeres MA et al. Proc ASH 2009;Abstract 1771

Copyright © 2010, Research To Practice, All rights reserved.
Efficacy of Azacitidine Compared with That of Conventional Care Regimens in the Treatment of Higher-Risk Myelodysplastic Syndromes: A Randomised, Open-Label, Phase III StudyFenaux P et al.
Lancet Oncol 2009;10(3):223-32.

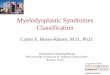
Azacitidine Improves Survival in High-Risk MDS
N=179
N=179
Fenaux. Lancet Oncology 10:223, 2009
Screening/CentralPathology Review
Investigator CCRTx Selection
Randomization
AZA 75 mg/m2/d x 7 d q28 d
CCR
• Best Supportive Care (BSC) only• Low Dose Ara-C (LDAC, 20 md/m2/d x 14 d q28-42 d)• Std Chemo (7 + 3)

Number at riskAZA 179 152 130 85 52 30 10 1CCR 179 132 95 69 32 14 5 0
Survival with Azacitidine vs CCR
p = 0.0001HR = 0.58 Deaths: AZA = 82, CCR = 113
0 5 10 15 20 25 30 35 40Time (months) from Randomization
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
port
ion
Sur
vivi
ng
CCRAZA
Fenaux. Lancet Oncology 10:223, 2009

Copyright © 2010, Research To Practice, All rights reserved.
Low Dose Decitabine versus Best Supportive Care in Elderly Patients with Intermediate or High Risk MDS Not Eligible for Intensive Chemotherapy: Final Results of the Randomized Phase III Study (06011) of the EORTC Leukemia and German MDS Study GroupsWijerMans P et al.
Proc ASH 2008;Abstract 226.

• 233 pts; median age 70 yrs; IPSS int-2 55%, high 38%; poor CG 46%; prior Rx 20%
• Decitabine 15 mg/m2 over 4 hrs Q8 hrs x 3 days (135mg/m2/course) Q 6 wks; maximum 8 courses; median 4 courses; ≤ 2 cycles 40%
Decitabine vs Supportive Care in MDS (EORTC)
Parameter Decitabine Support p-value
% CR+PR+HI 13 + 6 + 15 0 + 0 + 2 <0.001
Median survival (mos) 10.1 8.5 0.38
Median PFS (mos) 6.6 3.0 0.004
Median to AML or death 8.8 6.1 0.24
Wijermans. Blood 112:abst 226, 2008

Copyright © 2010, Research To Practice, All rights reserved.
A Study Comparing Dosing-Regimens and Efficacy of Subcutaneous to Intravenous Azacitidine (AZA) for the Treatment of Myelodysplastic Syndromes (MDS)
Sekeres MA et al.
Proc ASH 2009;Abstract 3797.

Most US AZA Dosing Does Not Follow FDA Schedule
Sekeres et al. Blood 2009;114:3797a

Similar RR for IV vs SC Dosing in 331 Pts
Sekeres et al. Blood 2009;114:3797a


Case History: Dr Kantarjian
• 79-yo man with fatigue
• Hb 8.5 g/dL, WBC 2,300/µL, platelets 220,000/µL
• Bone Marrow Aspirate and Biopsy: Dysplastic changes with 3% blasts
• Cytogenetics: Del 5q
• Patient started on lenalidomide 10mg PO QD
• After 4 weeks… Hb 10.0 g/dL, WBC 1,000/µL, platelets 70,000/µL

Case History: Dr Kantarjian (continued)
• Lenalidomide administration held, and restarted at 5mg PO QD, after recovery of blood counts
• Good hemoglobin response to lenalidomide
• 14 months later… Hb 9.0 g/dL, WBC 1,500/µL, Platelets 30,000/µL
• Bone Marrow Aspirate and Biopsy: 12% blasts
• Cytogenetics: Complex Karyotype with Del 5q, Del 17p, Monosomy 7

Case History: Dr Kantarjian (continued)
• Patient started on azacitidine with good response
• After 12 months… worsening anemia and thrombocytopenia
• Bone Marrow Aspirate and Biopsy: 40% blasts
• Cytogenetics: Complex Karyotype
• ECOG PS 0
• No cardiac or pulmonary problems

Copyright © 2010, Research To Practice, All rights reserved.
Long-Term Clinical Benefit of Lenalidomide Treatment in Patients with Myelodysplastic Syndrome and Chromosome Deletion 5qList AF et al.
Proc ASH 2006;Abstract 251.
Phase 2 Study of Lenalidomide in Transfusion-Dependent, Low-Risk, and Intermediate-1-Risk Myelodysplastic Syndromes with Karyotypes Other Than Deletion 5q Raza A et al.
Blood 2008;111(1):86-93.

Lenalidomide in MDS
Parameter del 5q1 no del 5q2
No. treated 148 214
% Tx independence 67 26
% HI — E — 33
Median wks to resp. 5 4.8
Media Hb (g/dl) 5.4 3.2
Median resp. dur. (wks)
116 41
% CG CR 44 (25% of total) 9
% G3-4 myelosuppression
50-59 20-25
1 List AF et al. Proc ASH 2006;Abstract 251. 2 Raza A et al. Blood 2008;111(1):86-93.

Copyright © 2010, Research To Practice, All rights reserved.
Efficacy and Safety of Lenalidomide in Intermediate-2 or High-Risk Myelodysplastic Syndromes with 5q Deletion: Results of a Phase 2 Study
Ades L et al.Blood 2009;113:3947-52.

Efficacy of Lenalidomide in Higher Risk MDS by Baseline Characteristics
Cytogenetics n CR
Isolated del 5q 9 67%
Single Additional Abnormality
11 9%
> 1 Additional Abnormality 27 0%
Platelet Count n CR
> 100,000/mm3 20 35%
< 100,000/mm3 27 0%
Bone Marrow Blast n CR
< 20% 29 21%
> 20% 18 5%
Ades L et al. Blood 2009;113:3947-52.


Case History: Dr Sekeres
• 82-yo man with recent history of fatigue and dyspnea on exertion
• Hb 6.0 g/dL, WBC 2,700/µL, platelets 74,000/µL
• Transfused with 4 units of PRBC
• Bone marrow aspirate and biopsy: AML with 42% blasts and a background of dysplasia
• Cytogenetics: Complex karyotype with chromosome 5 and 7 abnormalities

3) Which of the following is NOT a valid treatment option for this octogenarian?
7 plus 3 induction chemotherapy
Low-dose cytarabine
A hypomethylating agent (azacitidine or decitabine)
Gemtuzumab ozogamicin
Watchful waiting 11%
13%
36%
26%
14%
0% 10% 20% 30% 40%

Copyright © 2010, Research To Practice, All rights reserved.
Sekeres MA et al.Haematologica 2008;93(12):1769-72.
Treatment of Older Adults with Acute Myeloid Leukemia: State of the Art and Current Perspectives

Challenges with Older Patient with AML
• Biological characteristics of AMLHigh prevalence of poor-risk cytogeneticsLess likely to have good risk cytogeneticsMore frequent secondary AMLLess responsiveness to chemotherapy
• Intolerance to intensive remission induction therapiesComorbid conditionsDifferential drug metabolism resulting in supra-
therapeutic drug levels• Reluctance of physician to treat with intensive induction
therapy
Sekeres MA et al. Haematologica 2008; 93(12):1769-72

Current Options for Older Patient with AML
• Standard remission induction therapy
Decision involves complex challenges even in a suitable patient
Wait for cytogenetics to rule out adverse cytogenetics• Novel cytotoxic agents
Clofarabine, Cloretazine• Hypomethylating agents
Azacitidine, Decitabine
33% of patients in AZA-001 study had 20% blasts or greater
Importance of prolonged administration• Low-dose cytarabine
Sekeres MA et al. Haematologica 2008;93(12):1769-72.

Why Do Elderly Patients with AML Do Worse?
• Poor tolerance and mortality with intensive chemoRx
• Poor PS and co-morbid conditions
• Different disease biology
MDR
incidence of adverse CG
other adverse molecular events

Copyright © 2010, Research To Practice, All rights reserved.
Hypomethylating Agents for the Treatment of Elderly Patients with AML
Fenaux P et al. J Clin Oncol 2010;28(4):562-9.
Blum W et al. Proc Natl Acad Sci USA 2010;107(16):7473-8.
Cashen AF et al. J Clin Oncol 2010;28(4):556-61.

Studies of Hypomethylating Agents in the Treatment of Elderly Patients with AML
Study NMedian
AgeMedian %Blasts
Regimen (Median # cycles)
Median Overall Survival
1AZA-001 113 70 23%AZA (8 cycles)
CCR24.5 mos16.0 mos
2Blum 2010
53 74 52%Decitabine
20 mg/m2 d 1-10(4 cycles)
55 wks
3Cashen 2010
55 74 50%Decitabine
20 mg/m2 d 1-5(3 cycles)
7.7 mos
1 Fenaux P et al. J Clin Oncol 2010;28(4):562-9. 2 Blum W et al. Proc Natl Acad Sci USA 2010;107(16):7473-8. 3 Cashen AF et al. J Clin Oncol 2010;28(4):556-61.

Case History: Dr Kantarjian
• 64-yo man with fatigue and petechiae
• History of heavy smoking and COPD
• Hb 9.2 g/dL, WBC 9,200/µL, platelets 24,000/µL
• Bone marrow aspirate & biopsy: 72% blasts. Positive myeloid markers
• Cytogenetics: Complex karyotype with chromosome 5 and 7 deletions
• ECOG PS 2

4) What would you recommend for this patient?
Hydroxyurea and hospice care
Low-dose cytarabine
Daunorubicin 45 mg/m2 IV daily
x 3 with cytarabineDaunorubicin 90 mg/m2 IV
daily with cytarabine
Idarubicin with standard-dose cytarabine
Idarubicin with high-dose cytarabine
Azacitidine or decitabine
Referral to leukemia center for investigational therapies
Clofarabine with or without low-dose cytarabine
19%
24%
34%
2%
5%
5%
2%
7%
2%
0% 10% 20% 30% 40%

Copyright © 2010, Research To Practice, All rights reserved.
Questions Regarding Frontline Therapy of Acute Myeloid Leukemia
Kantarjian H, O’Brien S.Cancer 2010;[Epub ahead of print].

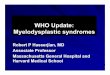
< 60 years > 60 years
Median Survival 17.5 6.2
AML: Median Survival (mos) by Patient Age and Treatment Era
Patient Age <1970 1970-1979 1980-1989 1990-1999 2000-2009
< 60 years 2.7 11.8 14.0 18.0 22.8
> 60 years 0.9 1.6 3.7 5.5 7.4
Kantarjian H, O’Brien S. Cancer 2010;[Epub ahead of print].
AML: Median Survival (mos) by Patient Age and Treatment Era — MDACC 1980 to Present

Questions Regarding Frontline Therapy of AML
Kantarjian H, O’Brien S. Cancer 2010 July 9 [Epub ahead of print].
• Prognosis for unselected patients with AML who receive standard frontline AML therapy?
• Significance of “residual leukemia” documented after 1 course of induction?– Should such bone marrow analyses be performed early
(Day 10-14) and be followed with a second course of induction if “residual leukemia” is noted?
• Is daunorubicin at a dose of 45 to 60 mg/m2 daily for 3 days and cytarabine 100 to 200 mg/m2 daily for 7 days (“3 + 7 regimen”) still considered standard frontline AML therapy?

Molecular Studies in AML
Marker % Prognosis
FLT3 ITD/mutation 30 Worse
MLL PTD 7 Worse
BAALC 6 Worse
BCL2 and WT1 mRNA 10-20 Worse
EVI1 expression 10 Worse
c-kit mutation in CBF 15 Worse
NPM1 mutation 50 Better
CEBPA mutation 8 Better