Embed Size (px)
Citation preview
1
Slide 1Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Chest and Abdominal TraumaChest and Abdominal TraumaChapter 27Chapter 27
Slide 2Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
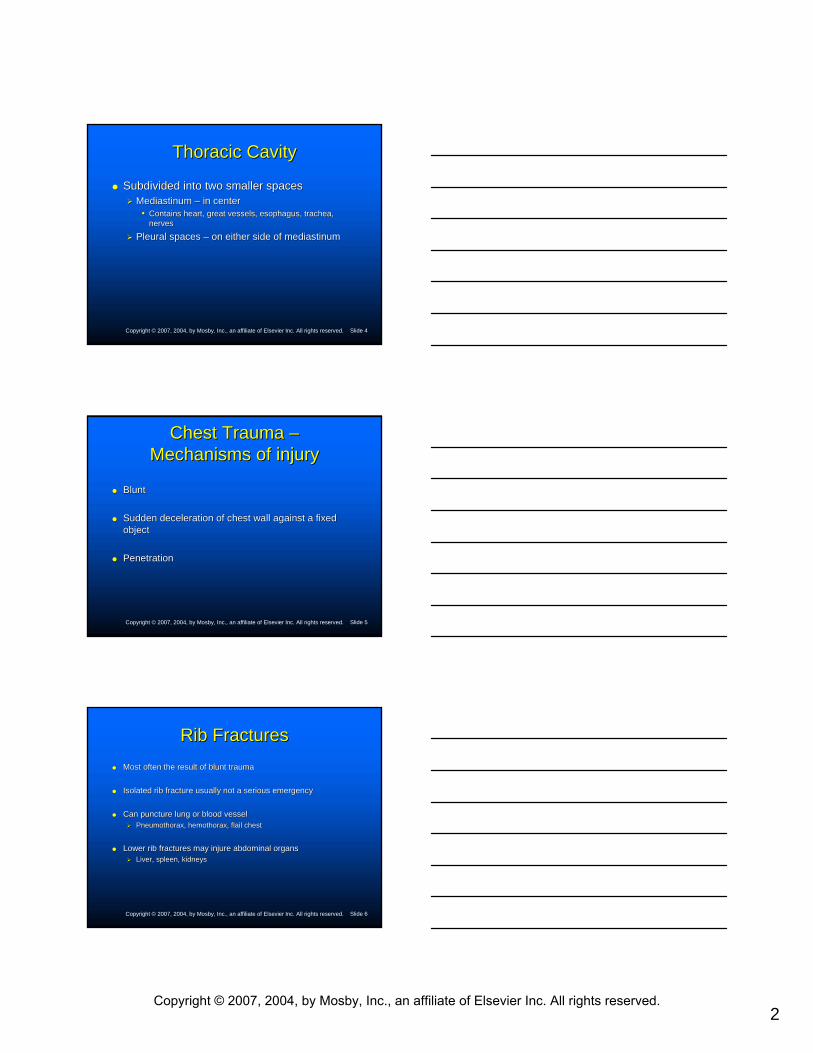
Anatomy and Physiology Anatomy and Physiology of the Chestof the Chest
Slide 3Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
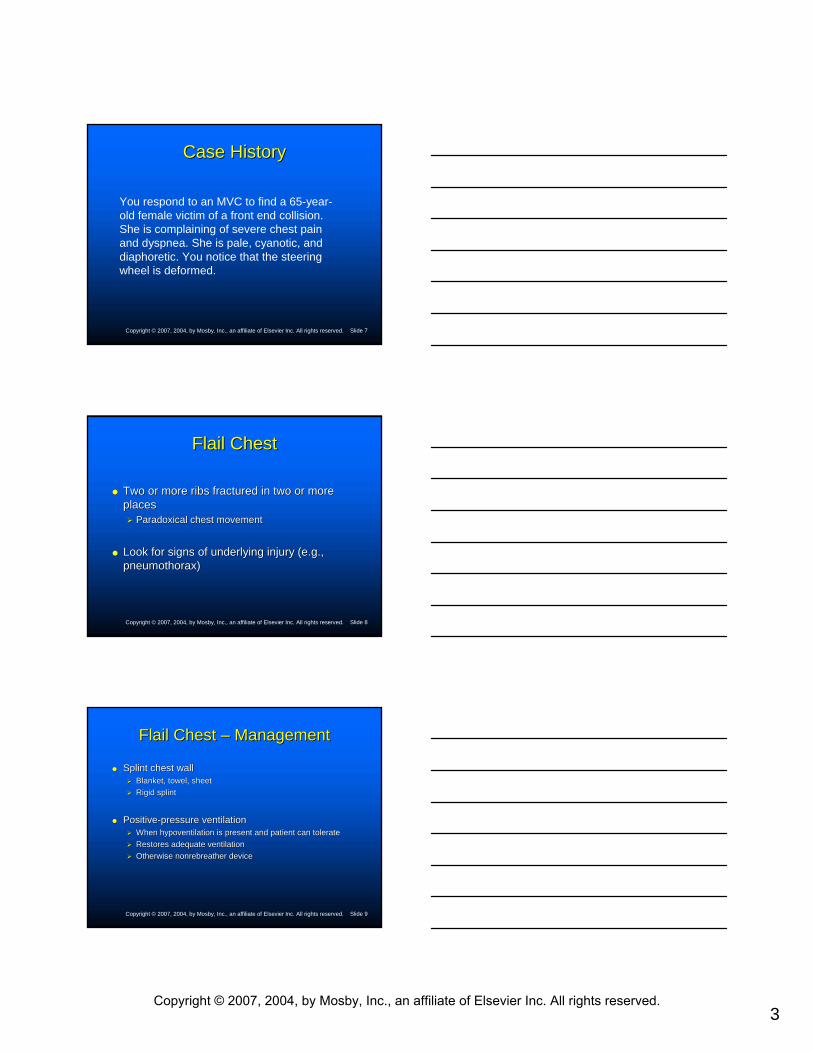
Anatomy and Physiology Anatomy and Physiology of the Chestof the Chest
Henry: EMT Prehospital Care, Revised 3rd Edition Lecture Notes
Chapter 27: Chest and Abdominal Trauma
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
2
Slide 4Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Thoracic CavityThoracic Cavity
Subdivided into two smaller spacesSubdivided into two smaller spacesMediastinumMediastinum –– in centerin center
•• Contains heart, great vessels, esophagus, trachea, Contains heart, great vessels, esophagus, trachea, nervesnerves
Pleural spaces Pleural spaces –– on either side of on either side of mediastinummediastinum
Slide 5Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Chest Trauma Chest Trauma ––Mechanisms of injuryMechanisms of injury
BluntBlunt
Sudden deceleration of chest wall against a fixed Sudden deceleration of chest wall against a fixed objectobject
PenetrationPenetration
Slide 6Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Rib FracturesRib FracturesMost often the result of blunt traumaMost often the result of blunt trauma
Isolated rib fracture usually not a serious emergencyIsolated rib fracture usually not a serious emergency
Can puncture lung or blood vesselCan puncture lung or blood vesselPneumothorax, Pneumothorax, hemothoraxhemothorax, flail chest, flail chest
Lower rib fractures may injure abdominal organsLower rib fractures may injure abdominal organsLiver, spleen, kidneysLiver, spleen, kidneys
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
3
Slide 7Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Case HistoryCase History
You respond to an MVC to find a 65-year-old female victim of a front end collision. She is complaining of severe chest pain and dyspnea. She is pale, cyanotic, and diaphoretic. You notice that the steering wheel is deformed.
Slide 8Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Flail ChestFlail Chest
Two or more ribs fractured in two or more Two or more ribs fractured in two or more placesplaces
Paradoxical chest movementParadoxical chest movement
Look for signs of underlying injury (e.g., Look for signs of underlying injury (e.g., pneumothorax)pneumothorax)
Slide 9Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Flail Chest Flail Chest –– ManagementManagement
Splint chest wallSplint chest wallBlanket, towel, sheetBlanket, towel, sheetRigid splintRigid splint
PositivePositive--pressure ventilationpressure ventilationWhen hypoventilation is present and patient can tolerateWhen hypoventilation is present and patient can tolerateRestores adequate ventilationRestores adequate ventilationOtherwise nonrebreather deviceOtherwise nonrebreather device
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
4
Slide 10Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Traumatic AsphyxiaTraumatic AsphyxiaSevere compression of thoraxSevere compression of thorax
HighHigh--velocity or steering wheel injuries, heavy weight dropped on velocity or steering wheel injuries, heavy weight dropped on chestchest
Heart compressed; blood driven to thorax and neckHeart compressed; blood driven to thorax and neckEcchymosisEcchymosis and edemaand edemaLifeLife--threatening injurythreatening injury
Look for associated injuries to lungs and chest wallLook for associated injuries to lungs and chest wall
Management: highManagement: high--concentration oxygen, possible PPVconcentration oxygen, possible PPV
Slide 11Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Traumatic AsphyxiaTraumatic Asphyxia
Slide 12Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Case HistoryCase History
You respond to a call for “difficulty breathing” to find a 19-year-old male complaining of dyspnea and chest pain. He states that it started suddenly while he was running. His breathing difficulty has gotten worse over the last hour.
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
5
Slide 13Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
PneumothoraxPneumothorax
Occurs when air enters visceral and parietal pleuraOccurs when air enters visceral and parietal pleuraCollapses lungCollapses lung
Less alveolar surface for diffusion of oxygenLess alveolar surface for diffusion of oxygenResults in hypoxiaResults in hypoxiaTwo mechanismsTwo mechanisms
TraumaTraumaSpontaneous ruptureSpontaneous rupture
Slide 14Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
TraumaticTraumatic
Penetrating Penetrating MissileMissileSharp objectSharp objectBroken ribBroken rib
BluntBluntPerson takes deep breath just before auto collisionPerson takes deep breath just before auto collision
•• ““Paper bag effectPaper bag effect””
Slide 15Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
SpontaneousSpontaneous
Ruptured bleb in lung tissueRuptured bleb in lung tissue
Young, muscular males Young, muscular males
COPD patientsCOPD patients
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.

6
Slide 16Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Open PneumothoraxOpen Pneumothorax
Slide 17Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Open Pneumothorax Open Pneumothorax ––Assessment and RecognitionAssessment and Recognition
Sucking woundSucking wound
DyspneaDyspnea
PleuriticPleuritic chest painchest pain
Slide 18Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Open Pneumothorax Open Pneumothorax ––Assessment and Recognition Assessment and Recognition
Absent or diminished breath sounds on affected side Absent or diminished breath sounds on affected side
Signs of respiratory distressSigns of respiratory distress
Subcutaneous emphysemaSubcutaneous emphysema
Historical profileHistorical profile
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
7
Slide 19Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Open Pneumothorax Open Pneumothorax ––ManagementManagement
Check ABCs.Check ABCs.
Administer oxygen; positiveAdminister oxygen; positive--pressure ventilation, if needed pressure ventilation, if needed (carefully).(carefully).Seal wound with airtight dressing on three sides.Seal wound with airtight dressing on three sides.
Place patient in position of comfort.Place patient in position of comfort.
Transport to definitive care.Transport to definitive care.
Slide 20Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Closed PneumothoraxClosed Pneumothorax
Also called simple pneumothoraxAlso called simple pneumothorax
ManagementManagementHighHigh--concentration oxygen; possible PPVconcentration oxygen; possible PPVTransport without delay.Transport without delay.
•• Watch for signs of a developing tension pneumothorax.Watch for signs of a developing tension pneumothorax.
Slide 21Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Case HistoryCase History
You respond to an MVC and find a 32-year-old female involved in victim of a front end collision complaining of severe chest pain and dyspnea. She is pale, cyanotic, and diaphoretic. The police on scene says she was fine when they arrived but she suddenly started to become “very sick.”
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
8
Slide 22Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Tension PneumothoraxTension Pneumothorax
Slide 23Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
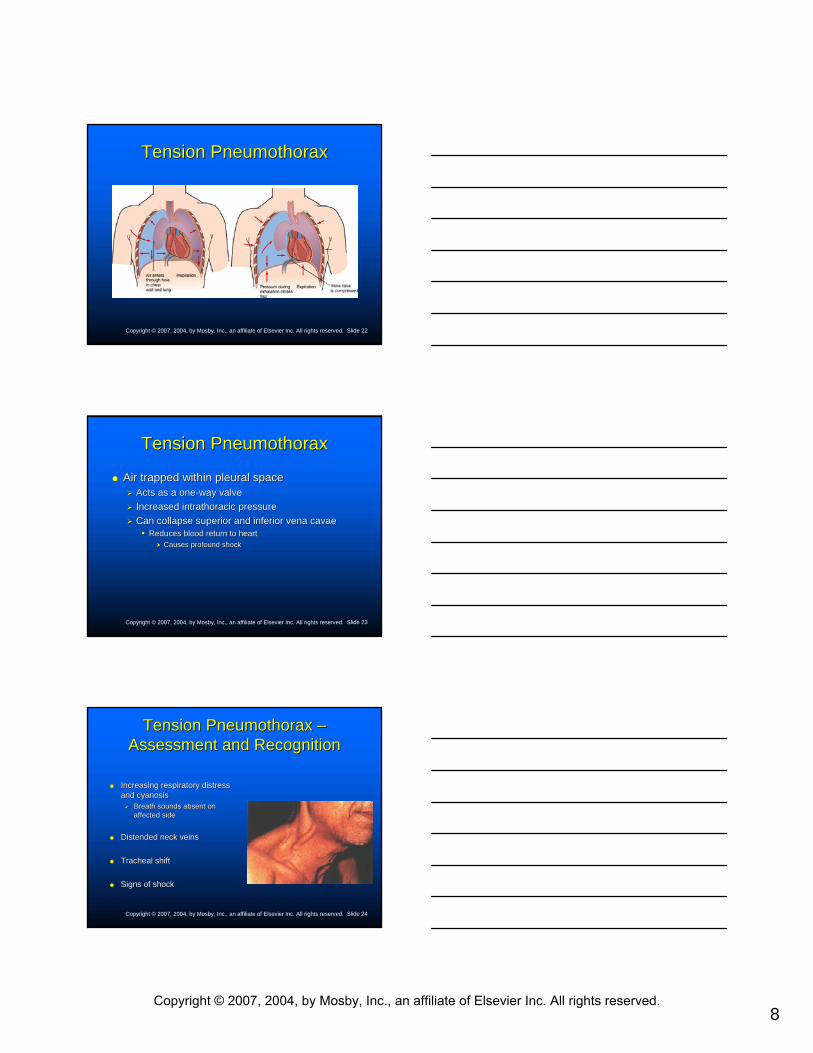
Tension PneumothoraxTension Pneumothorax
Air trapped within pleural spaceAir trapped within pleural spaceActs as a oneActs as a one--way valveway valveIncreased Increased intrathoracicintrathoracic pressurepressureCan collapse superior and inferior vena Can collapse superior and inferior vena cavaecavae
•• Reduces blood return to heartReduces blood return to heartCauses profound shockCauses profound shock
Slide 24Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Tension Pneumothorax Tension Pneumothorax ––Assessment and RecognitionAssessment and Recognition
Increasing respiratory distress Increasing respiratory distress and cyanosisand cyanosis
Breath sounds absent on Breath sounds absent on affected sideaffected side
Distended neck veinsDistended neck veins
Tracheal shiftTracheal shift
Signs of shockSigns of shock
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
9
Slide 25Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Tension Pneumothorax Tension Pneumothorax ––ManagementManagement
If airtight dressing was applied, remove dressingIf airtight dressing was applied, remove dressingReapply dressing after air escapes.Reapply dressing after air escapes.Watch for further tension.Watch for further tension.
Transport immediately.Transport immediately.
Consider ALS intercept (for needle decompression).Consider ALS intercept (for needle decompression).
Slide 26Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
HemothoraxHemothorax
Blood within the pleural spaceBlood within the pleural spaceThorax has the capacity for massive blood loss.Thorax has the capacity for massive blood loss.
Physiologic effectsPhysiologic effectsPrimary effect Primary effect –– hypovolemichypovolemic shockshockMay exist with or without an associated pneumothoraxMay exist with or without an associated pneumothoraxMay occur due to penetrating injuries or to rib fracturesMay occur due to penetrating injuries or to rib fractures
Slide 27Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
HemothoraxHemothorax ––Assessment and RecognitionAssessment and Recognition
Signs of Signs of hypovolemichypovolemic shockshockDelayed or absent capillary refill (children)Delayed or absent capillary refill (children)Pale, cool, sweaty skinPale, cool, sweaty skinTachycardiaTachycardiaRapid and shallow breathingRapid and shallow breathing
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
10
Slide 28Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
HemothoraxHemothorax ––Assessment and RecognitionAssessment and Recognition
Breath sounds absent on the affected sideBreath sounds absent on the affected side
HemoptysisHemoptysis (coughing blood)(coughing blood)
Hypotension (late sign)Hypotension (late sign)
Altered mental state (late sign)Altered mental state (late sign)
Cardiovascular collapse (cardiac arrest)Cardiovascular collapse (cardiac arrest)
Slide 29Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
HemothoraxHemothorax –– ManagementManagement
Establish a patent airway.Establish a patent airway.
Suction available to manage Suction available to manage hemoptysishemoptysis
HighHigh--concentration oxygen; possible PPVconcentration oxygen; possible PPV
Transport immediately.Transport immediately.
Slide 30Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Pulmonary ContusionPulmonary Contusion
From severe blows to chest wallFrom severe blows to chest wall
Can result in swelling and fluid buildupCan result in swelling and fluid buildupDecreases diffusion of oxygen into capillariesDecreases diffusion of oxygen into capillaries
ManagementManagementHighHigh--concentration oxygenconcentration oxygen
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
11
Slide 31Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Cardiac Cardiac TamponadeTamponade
Fluid accumulation in the pericardial sac Fluid accumulation in the pericardial sac caused by bleeding or fluid losscaused by bleeding or fluid loss
May result from blunt or penetrating traumaMay result from blunt or penetrating trauma
Slide 32Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Cardiac Cardiac TamponadeTamponade ——Physiologic EffectsPhysiologic Effects
Bleeding places pressure on atria, ventricles, Bleeding places pressure on atria, ventricles, and vena cava.and vena cava.
Venous return is obstructed. Venous return is obstructed. Interferes with the normal dynamics of contraction.Interferes with the normal dynamics of contraction.
Cardiac output is decreased.Cardiac output is decreased.
Slide 33Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Cardiac Cardiac TamponadeTamponade ——Assessment and RecognitionAssessment and Recognition
Penetrating wound or Penetrating wound or precordialprecordial contusion may be present.contusion may be present.
Signs of shockSigns of shock
Decreased pulse pressureDecreased pulse pressure
Muffled heart soundsMuffled heart sounds
Distended neck veinsDistended neck veins
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.

12
Slide 34Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Cardiac Cardiac TamponadeTamponade ——ManagementManagement
Early recognition and rapid hospital Early recognition and rapid hospital intervention intervention –– most essentialmost essential
Slide 35Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Case HistoryCase History
You respond to a “man down” to find a 20-year-old construction worker who fell 30 feet from a rooftop. He is complaining of pain in his chest and back. He is pale and diaphoretic. His pulse is 130 and thready. He is responsive to painful but not verbal stimuli.
Slide 36Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Aortic TearAortic TearComplete tear results in Complete tear results in exsanguinationexsanguination and death.and death.
Partial tear causes leak and hemorrhage.Partial tear causes leak and hemorrhage.
HypovolemicHypovolemic shock is main problem.shock is main problem.
Mortality is very high from massive hemorrhage.Mortality is very high from massive hemorrhage.80% die within first hour80% die within first hour
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
13
Slide 37Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Abdominal TraumaAbdominal Trauma
Slide 38Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
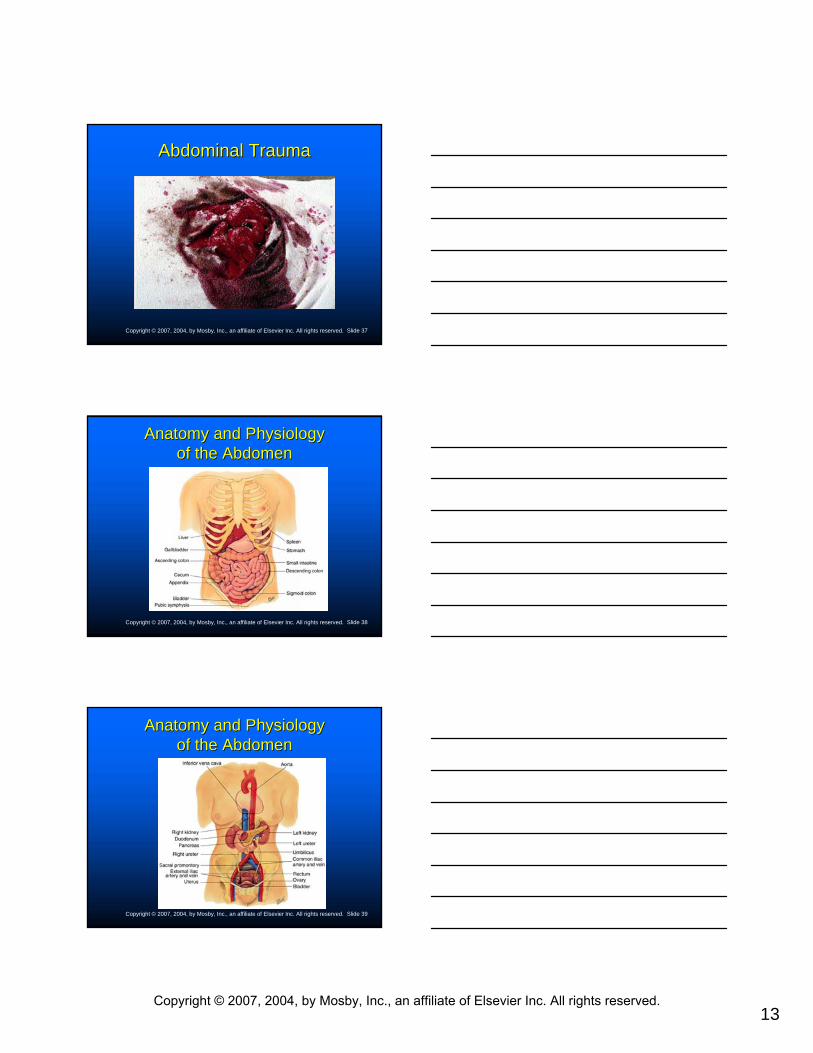
Anatomy and Physiology Anatomy and Physiology of the Abdomenof the Abdomen
Slide 39Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Anatomy and Physiology Anatomy and Physiology of the Abdomenof the Abdomen
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
14
Slide 40Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Anatomy and Physiology Anatomy and Physiology of the Abdomenof the Abdomen
Slide 41Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Abdominal InjuriesAbdominal InjuriesLarge vessels and highly vascular organs within abdomenLarge vessels and highly vascular organs within abdomen
Rapid blood loss and deathRapid blood loss and deathMaintain high level of suspicionMaintain high level of suspicion
May be from blunt or penetrating traumaMay be from blunt or penetrating trauma
Primary goal Primary goal Recognize lifeRecognize life--threatening injuries.threatening injuries.Administer essential life support.Administer essential life support.Transport without delay (requires surgical intervention).Transport without delay (requires surgical intervention).
Slide 42Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Mechanism of InjuryMechanism of Injury
Blunt traumaBlunt traumaCompression injuriesCompression injuriesDeceleration injuriesDeceleration injuriesSeat belt injuriesSeat belt injuries
Penetrating traumaPenetrating trauma
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
15
Slide 43Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
AssessmentAssessment
Scene sizeScene size--upupObtain MOIObtain MOI
Initial assessmentInitial assessmentLook for signs of Look for signs of hypovolemiahypovolemia
Slide 44Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
AssessmentAssessment
Focused history and physical examinationFocused history and physical examinationLook for bruises, tire marks, seat belt marks.Look for bruises, tire marks, seat belt marks.Is abdomen distended?Is abdomen distended?DCAPDCAP--BTLSBTLSPalpate abdomen for tenderness and guarding.Palpate abdomen for tenderness and guarding.
•• Save painful area for last.Save painful area for last.Palpate iliac crest.Palpate iliac crest.
•• If pelvic bones move, stop examination.If pelvic bones move, stop examination.
Slide 45Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
AssessmentAssessmentFocused history and physical examination (continued)Focused history and physical examination (continued)
Associated head or spinal injuries may present with loss of painAssociated head or spinal injuries may present with loss of painperception.perception.SAMPLE historySAMPLE historyElderly?Elderly?History of medications that slow heart rate?History of medications that slow heart rate?Signs of alcohol or drugsSigns of alcohol or drugs
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.

16
Slide 46Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
ManagementManagement
Management occurs in hospital.Management occurs in hospital.
Treat for shock.Treat for shock.
Transport without delay.Transport without delay.
Slide 47Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Special ConsiderationsSpecial Considerations
EviscerationEviscerationDo not attempt to put organs back in abdomen.Do not attempt to put organs back in abdomen.
•• Cover with moist, sterile dressing or airtight dressing.Cover with moist, sterile dressing or airtight dressing.
Transport in supine position with hips and legs Transport in supine position with hips and legs flexed with pillow under knees.flexed with pillow under knees.
Slide 48Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
EviscerationEvisceration
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
17
Slide 49Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Special ConsiderationsSpecial Considerations
Urinary tract injuriesUrinary tract injuriesLook for bruises over flank.Look for bruises over flank.Injuries to pelvis can cause bladder or urethral tears.Injuries to pelvis can cause bladder or urethral tears.
Injuries to male genitaliaInjuries to male genitaliaMay result in lacerations, bruising, avulsion, or amputationMay result in lacerations, bruising, avulsion, or amputation
Injuries to female genitaliaInjuries to female genitaliaMay occur from direct trauma or straddle injuriesMay occur from direct trauma or straddle injuries
Slide 50Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Acute AbdomenAcute Abdomen
Recent onset of abdominal painRecent onset of abdominal pain
Requires early diagnosis and surgical Requires early diagnosis and surgical interventionintervention
Slide 51Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Acute Abdomen Acute Abdomen ––AssessmentAssessment
Identify life threats and transport immediately.Identify life threats and transport immediately.
Initial assessmentInitial assessmentIf shock present, rapid transport.If shock present, rapid transport.Establish and maintain patent airway.Establish and maintain patent airway.Administer highAdminister high--concentration oxygen.concentration oxygen.Place patient in position of comfort, if not contraindicated.Place patient in position of comfort, if not contraindicated.
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
18
Slide 52Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Acute Abdomen Acute Abdomen ––AssessmentAssessment
Focused historyFocused historyGather SAMPLE history with OGather SAMPLE history with O--PP--QQ--RR--SS--T approach.T approach.
Slide 53Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
SAMPLE History for SAMPLE History for Patients with Abdominal ComplaintsPatients with Abdominal Complaints
Slide 54Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
SAMPLE History for SAMPLE History for Patients with Abdominal ComplaintsPatients with Abdominal Complaints
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
19
Slide 55Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
SAMPLE History for SAMPLE History for Patients with Abdominal ComplaintsPatients with Abdominal Complaints
Slide 56Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Acute Abdomen Acute Abdomen ––AssessmentAssessment
Focused physical examinationFocused physical examinationLook for findings associated with abdominal Look for findings associated with abdominal complaints.complaints.
•• Jaundice in sclera or skin?Jaundice in sclera or skin?•• Signs of dehydration?Signs of dehydration?
Ask patient to point to area of pain.Ask patient to point to area of pain.•• Palpate that quadrant last.Palpate that quadrant last.
Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.