Embed Size (px)
Citation preview

Copyright © 2006 by Mosby, Inc.Slide 1
Respiratory system moduleRespiratory system module
Asthma Asthma
BronchitisBronchitis
Flail chest Flail chest

Copyright © 2006 by Mosby, Inc.Slide 2
CASE SCENARIOCASE SCENARIO
A 30 YRS OLD MALE NON SMOKER A 30 YRS OLD MALE NON SMOKER PRESENTED IN EMERGENCY DEPARTMENT PRESENTED IN EMERGENCY DEPARTMENT WITH SEVERE SHORTNESS OF BREATH WITH SEVERE SHORTNESS OF BREATH FOR LAST 2 DAYS IT HAS WORSENED OVER FOR LAST 2 DAYS IT HAS WORSENED OVER FEW HRS TO SUCH AN EXTENT THAT HE FEW HRS TO SUCH AN EXTENT THAT HE HAS TO COME TO EME DEPARTMENT .HE HAS TO COME TO EME DEPARTMENT .HE HAS REVIOUS HISTORY OF SIMILAR HAS REVIOUS HISTORY OF SIMILAR ATTACKS OF SHORTNESS OF BREATH ATTACKS OF SHORTNESS OF BREATH WITH WHEEZE ESPECIALLY IN WINTERS WITH WHEEZE ESPECIALLY IN WINTERS USED TO RELIEVE AFTER TAKING USED TO RELIEVE AFTER TAKING MEDICATIONS .THERE IS HISTORY OF MEDICATIONS .THERE IS HISTORY OF NOCTURNAL COUGH ON AN OFFNOCTURNAL COUGH ON AN OFF

Copyright © 2006 by Mosby, Inc.Slide 3
THERE IS NO HISTORY OF ORTHOPNEA AND PND THERE IS NO HISTORY OF ORTHOPNEA AND PND NO HISTORY OF ANY HEART PROBLEM NO HISTORY NO HISTORY OF ANY HEART PROBLEM NO HISTORY OF ANY feverCONNECTIVE TISSUE DISEASE OR OF ANY feverCONNECTIVE TISSUE DISEASE OR KIDNEY DISORDER NO HISTORYOF KEEPING PETS KIDNEY DISORDER NO HISTORYOF KEEPING PETS AT HOME HE HAS LEFT HIS MEDICATION AND LOST AT HOME HE HAS LEFT HIS MEDICATION AND LOST FOLLOW UP WITH GPE FOR LAST 6 MONTHS FOLLOW UP WITH GPE FOR LAST 6 MONTHS

Copyright © 2006 by Mosby, Inc.Slide 4
WHAT IS THE LIKELY DIAGNOSIS IN THIS WHAT IS THE LIKELY DIAGNOSIS IN THIS PATIENT?PATIENT?
WHAT PHYSICAL FINDINGS HELP TO WHAT PHYSICAL FINDINGS HELP TO REACH A DIAGNOSIS?REACH A DIAGNOSIS?
WHAT INVESTIGATIONS SHOULD BE WHAT INVESTIGATIONS SHOULD BE DONE ?DONE ?
WHAT ARE MANAGEMENT OPTIONS?WHAT ARE MANAGEMENT OPTIONS?

Copyright © 2006 by Mosby, Inc.Slide 5
Asthma is a common and potentially serious chronic disease Asthma is a common and potentially serious chronic disease that can be controlled but not curedthat can be controlled but not cured
Asthma causes symptoms such as wheezing, shortness of Asthma causes symptoms such as wheezing, shortness of breath, chest tightness and cough that vary over time in their breath, chest tightness and cough that vary over time in their occurrence, frequency and intensityoccurrence, frequency and intensity
Symptoms are associated with variable expiratory airflow, Symptoms are associated with variable expiratory airflow, i.e. difficulty breathing air out of the lungs due to i.e. difficulty breathing air out of the lungs due to Bronchoconstriction (airway narrowing)Bronchoconstriction (airway narrowing)
Airway wall thickeningAirway wall thickening
Increased mucusIncreased mucus
Symptoms may be triggered or worsened by factors such as Symptoms may be triggered or worsened by factors such as viral infections, allergens, tobacco smoke, exercise and stressviral infections, allergens, tobacco smoke, exercise and stress
What is known about asthma?What is known about asthma?
GINA 2014

Copyright © 2006 by Mosby, Inc.Slide 6
Asthma can be effectively treatedAsthma can be effectively treated
When asthma is well-controlled, patients canWhen asthma is well-controlled, patients can Avoid troublesome symptoms during the day and Avoid troublesome symptoms during the day and
nightnight
Need little or no reliever medicationNeed little or no reliever medication
Have productive, physically active livesHave productive, physically active lives
Have normal or near-normal lung functionHave normal or near-normal lung function
Avoid serious asthma flare-ups (also called Avoid serious asthma flare-ups (also called exacerbations, or severe attacks)exacerbations, or severe attacks)
What is known about asthma?What is known about asthma?
GINA 2014

Copyright © 2006 by Mosby, Inc.Slide 7
Asthma is a heterogeneous disease, usually characterized Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation. by chronic airway inflammation.
It is defined by the history of respiratory symptoms such as It is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough wheeze, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable that vary over time and in intensity, together with variable expiratory airflow limitation.expiratory airflow limitation.
Definition of asthmaDefinition of asthma
NEW!
GINA 2014

Copyright © 2006 by Mosby, Inc.Slide 8
ASTHMA DEFINITIONASTHMA DEFINITION
“a common chronic disorder of the airways that is complex and characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation. The interaction of these features of asthma determines the clinical manifestations and severity of asthma and the response to treatment

Copyright © 2006 by Mosby, Inc.Slide 9
The diagnosis of asthma should be based on:The diagnosis of asthma should be based on: A history of characteristic symptom patterns A history of characteristic symptom patterns
Evidence of variable airflow limitation, from bronchodilator Evidence of variable airflow limitation, from bronchodilator reversibility testing or other tests reversibility testing or other tests
Document evidence for the diagnosis in the patient’s Document evidence for the diagnosis in the patient’s notes, preferably before starting controller treatmentnotes, preferably before starting controller treatment It is often more difficult to confirm the diagnosis after It is often more difficult to confirm the diagnosis after
treatment has been startedtreatment has been started
Asthma is usually characterized by airway Asthma is usually characterized by airway inflammation and airway hyperresponsiveness, but inflammation and airway hyperresponsiveness, but these are not necessary or sufficient to make the these are not necessary or sufficient to make the diagnosis of asthma.diagnosis of asthma.
Diagnosis of asthmaDiagnosis of asthma
GINA 2014

Copyright © 2006 by Mosby, Inc.Slide 10GINA 2014, Box 1-1 © Global Initiative for Asthma
NEW!

Copyright © 2006 by Mosby, Inc.Slide 11
IncreasedIncreased probability that symptoms are due to asthma if: probability that symptoms are due to asthma if: More than one type of symptom (wheeze, shortness of breath, cough, chest More than one type of symptom (wheeze, shortness of breath, cough, chest
tightness)tightness)
Symptoms often worse at night or in the early morningSymptoms often worse at night or in the early morning
Symptoms vary over time and in intensitySymptoms vary over time and in intensity
Symptoms are triggered by viral infections, exercise, allergen exposure, Symptoms are triggered by viral infections, exercise, allergen exposure, changes in weather, laughter, irritants such as car exhaust fumes, smoke, or changes in weather, laughter, irritants such as car exhaust fumes, smoke, or strong smellsstrong smells
DecreasedDecreased probability that symptoms are due to asthma if: probability that symptoms are due to asthma if: Isolated cough with no other respiratory symptomsIsolated cough with no other respiratory symptoms
Chronic production of sputumChronic production of sputum
Shortness of breath associated with dizziness, light-headedness or peripheral Shortness of breath associated with dizziness, light-headedness or peripheral tinglingtingling
Chest painChest pain
Exercise-induced dyspnea with noisy inspiration (stridor)Exercise-induced dyspnea with noisy inspiration (stridor)
Diagnosis of asthma – symptomsDiagnosis of asthma – symptoms
GINA 2014

Copyright © 2006 by Mosby, Inc.Slide 12
Confirm presence of airflow limitationConfirm presence of airflow limitation Document that FEVDocument that FEV11/FVC is reduced (at least once, when FEV/FVC is reduced (at least once, when FEV11 is low) is low) FEVFEV11/ FVC ratio is normally >0.75 – 0.80 in healthy adults, and / FVC ratio is normally >0.75 – 0.80 in healthy adults, and
>0.90 in children>0.90 in children Confirm variation in lung function is greater than in healthy individualsConfirm variation in lung function is greater than in healthy individuals
The greater the variation, or the more times variation is seen, the greater The greater the variation, or the more times variation is seen, the greater probability that the diagnosis is asthmaprobability that the diagnosis is asthma
Excessive bronchodilator reversibility (adults: increase in FEVExcessive bronchodilator reversibility (adults: increase in FEV11 >12% and >12% and >200mL; children: increase >12% predicted)>200mL; children: increase >12% predicted)
Excessive diurnal variability from 1-2 weeks’ twice-daily PEF monitoring (daily Excessive diurnal variability from 1-2 weeks’ twice-daily PEF monitoring (daily amplitude x 100/daily mean, averaged)amplitude x 100/daily mean, averaged)
Significant increase in FEVSignificant increase in FEV11 or PEF after 4 weeks of controller treatment or PEF after 4 weeks of controller treatment If initial testing is negative:If initial testing is negative:
• Repeat when patient is symptomatic, or after withholding bronchodilatorsRepeat when patient is symptomatic, or after withholding bronchodilators
• Refer for additional tests (especially children ≤5 years, or the elderly)Refer for additional tests (especially children ≤5 years, or the elderly)
Diagnosis of asthma – variable Diagnosis of asthma – variable airflow limitationairflow limitation
GINA 2014, Box 1-2

Copyright © 2006 by Mosby, Inc.Slide 13 © Global Initiative for Asthma
Time (seconds)
Volume
Note: Each FEV1 represents the highest of three reproducible measurements
Typical spirometric tracingsTypical spirometric tracings
FEV1
1 2 3 4 5
Normal
Asthma (after BD)
Asthma (before BD)
Volume
Normal
Asthma (after BD)
Asthma (before BD)
GINA 2014

Copyright © 2006 by Mosby, Inc.Slide 14
Physical examination in people with asthmaPhysical examination in people with asthma Often normalOften normal
The most frequent finding is wheezing on auscultation, especially on The most frequent finding is wheezing on auscultation, especially on forced expirationforced expiration
Wheezing is also found in other conditions, for example:Wheezing is also found in other conditions, for example: Respiratory infectionsRespiratory infections
COPDCOPD
Upper airway dysfunctionUpper airway dysfunction
Endobronchial obstruction Endobronchial obstruction
Inhaled foreign bodyInhaled foreign body
Wheezing may be absent during severe asthma Wheezing may be absent during severe asthma exacerbations (‘silent chest’)exacerbations (‘silent chest’)
Diagnosis of asthma – physical Diagnosis of asthma – physical examinationexamination
GINA 2014

Copyright © 2006 by Mosby, Inc.Slide 15 © Global Initiative for Asthma
Step 1 – as-needed inhaled short-acting Step 1 – as-needed inhaled short-acting betabeta22-agonist (SABA) -agonist (SABA)
*For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS**For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy
GINA 2014, Box 3-5, Step 1

Copyright © 2006 by Mosby, Inc.Slide 16 © Global Initiative for Asthma
Step 1 – as-needed inhaled short-acting Step 1 – as-needed inhaled short-acting betabeta22-agonist (SABA) -agonist (SABA)
*For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS**For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy
GINA 2014, Box 3-5, Step 1

Copyright © 2006 by Mosby, Inc.Slide 17
Preferred option: as-needed inhaled short-acting Preferred option: as-needed inhaled short-acting betabeta22-agonist (SABA)-agonist (SABA) SABAs are highly effective for relief of asthma symptomsSABAs are highly effective for relief of asthma symptoms
However …. there is insufficient evidence about the However …. there is insufficient evidence about the safety of treating asthma with SABA alonesafety of treating asthma with SABA alone
This option should be reserved for patients with This option should be reserved for patients with infrequent symptoms (less than twice a month) of short infrequent symptoms (less than twice a month) of short duration, and with no risk factors for exacerbationsduration, and with no risk factors for exacerbations
Other optionsOther options Consider adding regular low dose inhaled corticosteroid Consider adding regular low dose inhaled corticosteroid
(ICS) for patients at risk of exacerbations (ICS) for patients at risk of exacerbations
Step 1 – as-needed reliever inhalerStep 1 – as-needed reliever inhaler
GINA 2014

Copyright © 2006 by Mosby, Inc.Slide 18 © Global Initiative for Asthma
Step 2 – low-dose controller + as-needed Step 2 – low-dose controller + as-needed inhaled SABAinhaled SABA
*For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS**For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy
GINA 2014, Box 3-5, Step 2

Copyright © 2006 by Mosby, Inc.Slide 19
Preferred option: regular low dose ICS with as-needed inhaled SABAPreferred option: regular low dose ICS with as-needed inhaled SABA Low dose ICS reduces symptoms and reduces risk of exacerbations and Low dose ICS reduces symptoms and reduces risk of exacerbations and
asthma-related hospitalization and deathasthma-related hospitalization and death
Other optionsOther options Leukotriene receptor antagonists (LTRA) with as-needed SABALeukotriene receptor antagonists (LTRA) with as-needed SABA
• Less effective than low dose ICSLess effective than low dose ICS
• May be used for some patients with both asthma and allergic rhinitis, or if patient will not May be used for some patients with both asthma and allergic rhinitis, or if patient will not use ICS use ICS
Combination low dose ICS/long-acting beta2-agonist (LABA) Combination low dose ICS/long-acting beta2-agonist (LABA) with as-needed SABAwith as-needed SABA
• Reduces symptoms and increases lung function compared with ICSReduces symptoms and increases lung function compared with ICS
• More expensive, and does not further reduce exacerbationsMore expensive, and does not further reduce exacerbations
Intermittent ICS with as-needed SABA for purely seasonal allergic asthma with Intermittent ICS with as-needed SABA for purely seasonal allergic asthma with no interval symptomsno interval symptoms
• Start ICS immediately symptoms commence, and continue for Start ICS immediately symptoms commence, and continue for 4 weeks after pollen season ends4 weeks after pollen season ends
Step 2 – Low dose controller + as-Step 2 – Low dose controller + as-needed SABAneeded SABA
GINA 2014

Copyright © 2006 by Mosby, Inc.Slide 20 © Global Initiative for Asthma
Step 3 – one or two controllers + as-needed Step 3 – one or two controllers + as-needed inhaled relieverinhaled reliever
*For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS**For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy
GINA 2014, Box 3-5, Step 3

Copyright © 2006 by Mosby, Inc.Slide 21

Copyright © 2006 by Mosby, Inc.Slide 22
Before considering step-upBefore considering step-up Check inhaler technique and adherence, confirm diagnosisCheck inhaler technique and adherence, confirm diagnosis
Adults/adolescents: preferred options are either combination low dose ICS/LABA Adults/adolescents: preferred options are either combination low dose ICS/LABA maintenance with as-needed SABA, OR combination low dose ICS/formoterol maintenance with as-needed SABA, OR combination low dose ICS/formoterol maintenance and reliever regimen*maintenance and reliever regimen*
Adding LABA reduces symptoms and exacerbations and increases FEVAdding LABA reduces symptoms and exacerbations and increases FEV11, while allowing , while allowing
lower dose of ICSlower dose of ICS
In at-risk patients, maintenance and reliever regimen significantly reduces exacerbations In at-risk patients, maintenance and reliever regimen significantly reduces exacerbations with similar level of symptom control and lower ICS doses compared with other regimenswith similar level of symptom control and lower ICS doses compared with other regimens
Children 6-11 years: preferred option is medium dose ICS with Children 6-11 years: preferred option is medium dose ICS with as-needed SABAas-needed SABA
Other optionsOther options Adults/adolescents: Increase ICS dose or add LTRA or theophylline (less effective than Adults/adolescents: Increase ICS dose or add LTRA or theophylline (less effective than
ICS/LABA)ICS/LABA)
Children 6-11 years – add LABA (similar effect as increasing ICS)Children 6-11 years – add LABA (similar effect as increasing ICS)
Step 3 – one or two controllers + as-Step 3 – one or two controllers + as-needed inhaled relieverneeded inhaled reliever
*Approved only for low dose beclometasone/formoterol and low dose budesonide/formoterolGINA 2014

Copyright © 2006 by Mosby, Inc.Slide 23 © Global Initiative for Asthma
Step 4 – two or more controllers + as-needed Step 4 – two or more controllers + as-needed inhaled relieverinhaled reliever
*For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS**For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy
GINA 2014, Box 3-5, Step 4

Copyright © 2006 by Mosby, Inc.Slide 24
Before considering step-upBefore considering step-up Check inhaler technique and adherenceCheck inhaler technique and adherence
Adults or adolescents: preferred option is combination low dose Adults or adolescents: preferred option is combination low dose ICS/formoterol as maintenance and reliever regimen*, ORICS/formoterol as maintenance and reliever regimen*, ORcombination medium dose ICS/LABA with as-needed SABAcombination medium dose ICS/LABA with as-needed SABA
Children 6–11 years: preferred option is to refer for expert Children 6–11 years: preferred option is to refer for expert adviceadvice
Other options (adults or adolescents)Other options (adults or adolescents) Trial of high dose combination ICS/LABA, but little extra benefit and Trial of high dose combination ICS/LABA, but little extra benefit and
increased risk of side-effectsincreased risk of side-effects
Increase dosing frequency (for budesonide-containing inhalers)Increase dosing frequency (for budesonide-containing inhalers)
Add-on LTRA or low dose theophyllineAdd-on LTRA or low dose theophylline
Step 4 – two or more controllers + Step 4 – two or more controllers + as-needed inhaled relieveras-needed inhaled reliever
GINA 2014
*Approved only for low dose beclometasone/formoterol and low dose budesonide/formoterol

Copyright © 2006 by Mosby, Inc.Slide 25 © Global Initiative for Asthma
Step 5 – higher level care and/or add-on Step 5 – higher level care and/or add-on treatmenttreatment
*For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS**For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy
GINA 2014, Box 3-5, Step 5

Copyright © 2006 by Mosby, Inc.Slide 26
Preferred option is referral for specialist investigation and Preferred option is referral for specialist investigation and consideration of add-on treatmentconsideration of add-on treatment If symptoms uncontrolled or exacerbations persist despite Step 4 If symptoms uncontrolled or exacerbations persist despite Step 4
treatment, check inhaler technique and adherence before referringtreatment, check inhaler technique and adherence before referring
Add-on omalizumab (anti-IgE) is suggested for patients with moderate Add-on omalizumab (anti-IgE) is suggested for patients with moderate or severe allergic asthma that is uncontrolled on Step 4 treatmentor severe allergic asthma that is uncontrolled on Step 4 treatment
Other add-on treatment options at Step 5 include:Other add-on treatment options at Step 5 include: Sputum-guided treatment: this is available in specialized centers; Sputum-guided treatment: this is available in specialized centers;
reduces exacerbations and/or corticosteroid dosereduces exacerbations and/or corticosteroid dose
Add-on low dose oral corticosteroids (≤7.5mg/day prednisone Add-on low dose oral corticosteroids (≤7.5mg/day prednisone equivalent): this may benefit some patients, but has significant equivalent): this may benefit some patients, but has significant systemic side-effects. Assess and monitor for osteoporosissystemic side-effects. Assess and monitor for osteoporosis
See Severe Asthma Guidelines (Chung et al, ERJ 2014) for more See Severe Asthma Guidelines (Chung et al, ERJ 2014) for more detaildetail
Step 5 – higher level care and/or Step 5 – higher level care and/or add-on treatmentadd-on treatment
GINA 2014

Copyright © 2006 by Mosby, Inc.Slide 27
Low, medium and high dose inhaled Low, medium and high dose inhaled corticosteroids corticosteroids
Adults and adolescents (≥12 years)Adults and adolescents (≥12 years)
This is not a table of equivalence, but of estimated clinical comparabilityThis is not a table of equivalence, but of estimated clinical comparability
Most of the clinical benefit from ICS is seen at low dosesMost of the clinical benefit from ICS is seen at low doses
High doses are arbitrary, but for most ICS are those that, with prolonged use, High doses are arbitrary, but for most ICS are those that, with prolonged use, are associated with increased risk of systemic side-effectsare associated with increased risk of systemic side-effects
Inhaled corticosteroid Total daily dose (mcg)Low Medium High
Beclometasone dipropionate (CFC) 200–500 >500–1000 >1000
Beclometasone dipropionate (HFA) 100–200 >200–400 >400
Budesonide (DPI) 200–400 >400–800 >800
Ciclesonide (HFA) 80–160 >160–320 >320
Fluticasone propionate (DPI or HFA) 100–250 >250–500 >500
Mometasone furoate 110–220 >220–440 >440
Triamcinolone acetonide 400–1000 >1000–2000 >2000
GINA 2014, Box 3-6 (1/2)

Copyright © 2006 by Mosby, Inc.Slide 28
Low, medium and high dose inhaled Low, medium and high dose inhaled corticosteroidscorticosteroids
Children 6–11 yearsChildren 6–11 years
This is not a table of equivalence, but of estimated clinical comparabilityThis is not a table of equivalence, but of estimated clinical comparability
Most of the clinical benefit from ICS is seen at low dosesMost of the clinical benefit from ICS is seen at low doses
High doses are arbitrary, but for most ICS are those that, with prolonged use, are High doses are arbitrary, but for most ICS are those that, with prolonged use, are associated with increased risk of systemic side-effectsassociated with increased risk of systemic side-effects
Inhaled corticosteroid Total daily dose (mcg)Low Medium High
Beclometasone dipropionate (CFC) 100–200 >200–400 >400
Beclometasone dipropionate (HFA) 50–100 >100–200 >200
Budesonide (DPI) 100–200 >200–400 >400
Budesonide (nebules) 250–500 >500–1000 >1000
Ciclesonide (HFA) 80 >80–160 >160
Fluticasone propionate (DPI) 100–200 >200–400 >400
Fluticasone propionate (HFA) 100–200 >200–500 >500
Mometasone furoate 110 ≥220–<440 ≥440
Triamcinolone acetonide 400–800 >800–1200 >1200
GINA 2014, Box 3-6 (2/2)

Copyright © 2006 by Mosby, Inc.Slide 29
Case scenarioCase scenario 2 2
A 60 yr old male heavy smoker presented in A 60 yr old male heavy smoker presented in pulmonology outdoor with progressive pulmonology outdoor with progressive worsening of shortnes of breath for last one worsening of shortnes of breath for last one yr .he also complains or cough wth scanty yr .he also complains or cough wth scanty sputum .there is no diurnal variation or history sputum .there is no diurnal variation or history of wheezing .of wheezing .
What can be possible underlying conditionWhat can be possible underlying condition

Copyright © 2006 by Mosby, Inc.Slide 30
On examination patient is of thin built with On examination patient is of thin built with B.p 150/90 mmHg pulse 88/min ,afebrile ,rr B.p 150/90 mmHg pulse 88/min ,afebrile ,rr 22/min.he was clubbed ,and cyanosed .chest 22/min.he was clubbed ,and cyanosed .chest movements limited breath sounds reduced movements limited breath sounds reduced vocal resonance increased vocal resonance increased
X-ray chest showed hyperinflated lungs with X-ray chest showed hyperinflated lungs with tubular hearttubular heart
FEV1/VC reduced FEV1/VC reduced
What can be ndelying lung condition?What can be ndelying lung condition?

Copyright © 2006 by Mosby, Inc.Slide 31
Chronic obstructive pulmonary disease.Chronic obstructive pulmonary disease.
Bronchitis, emphysema, and asthma may Bronchitis, emphysema, and asthma may present alone or in combination.present alone or in combination.
AsthmaBronchitis
Emphysema

Copyright © 2006 by Mosby, Inc.Slide 32
Chronic bronchitis. Chronic bronchitis. InsetInset, Weakened distal airways in emphysema, , Weakened distal airways in emphysema, a common secondary anatomic alteration of the lungsa common secondary anatomic alteration of the lungs..

Copyright © 2006 by Mosby, Inc.Slide 33
Anatomic Alterations of the LungsAnatomic Alterations of the Lungs
Chronic inflammation and swelling of the Chronic inflammation and swelling of the peripheral airwaysperipheral airways
Excessive mucus production and Excessive mucus production and accumulationaccumulation
Partial or total mucus pluggingPartial or total mucus plugging
Hyperinflation of alveoli (air-trapping)Hyperinflation of alveoli (air-trapping)
Smooth muscle constriction of bronchial Smooth muscle constriction of bronchial airways (bronchospasm)airways (bronchospasm)

Copyright © 2006 by Mosby, Inc.Slide 34
EtiologyEtiology
Cigarette smokingCigarette smoking
Atmospheric pollutantsAtmospheric pollutants
InfectionInfection
Gastroesophageal reflux diseaseGastroesophageal reflux disease

Copyright © 2006 by Mosby, Inc.Slide 35
Overview of the Cardiopulmonary Overview of the Cardiopulmonary Clinical Manifestations Associated Clinical Manifestations Associated
with CHRONIC BRONCHITISwith CHRONIC BRONCHITIS
The following clinical manifestations result from The following clinical manifestations result from the pathophysiologic mechanisms caused (or the pathophysiologic mechanisms caused (or activated) by activated) by Excessive Bronchial SecretionsExcessive Bronchial Secretions (see Figure 9-11) and (see Figure 9-11) and BronchospasmBronchospasm (see (see Figure 9-10)—the major anatomic alterations of Figure 9-10)—the major anatomic alterations of the lungs associated with chronic bronchitis the lungs associated with chronic bronchitis (see Figure 11-1).(see Figure 11-1).

Copyright © 2006 by Mosby, Inc.Slide 36
Figure 9-11. Excessive bronchial secretions clinical scenario.Figure 9-11. Excessive bronchial secretions clinical scenario.

Copyright © 2006 by Mosby, Inc.Slide 37
Figure 9-10. Bronchospasm clinical scenario (e.g., asthma).Figure 9-10. Bronchospasm clinical scenario (e.g., asthma).

Copyright © 2006 by Mosby, Inc.Slide 38
Clinical Data Obtained at the Clinical Data Obtained at the Patient’s BedsidePatient’s Bedside
Vital signsVital signs
Increased respiratory rateIncreased respiratory rate
Increased heart rate, cardiac output, blood Increased heart rate, cardiac output, blood pressurepressure

Copyright © 2006 by Mosby, Inc.Slide 39
Clinical Data Obtained at theClinical Data Obtained at the Patient’s Bedside Patient’s Bedside
Use of accessory muscles of inspirationUse of accessory muscles of inspiration
Use of accessory muscles of expirationUse of accessory muscles of expiration
Pursed-lip breathingPursed-lip breathing
Increased anteroposterior chest diameter Increased anteroposterior chest diameter (barrel chest)(barrel chest)
CyanosisCyanosis
Digital clubbingDigital clubbing

Copyright © 2006 by Mosby, Inc.Slide 40
Figure 2-36. Figure 2-36. The way a patient may appear when using the The way a patient may appear when using the pectoralis major muscles for inspiration.pectoralis major muscles for inspiration.

Copyright © 2006 by Mosby, Inc.Slide 41
Figure 2-41. Figure 2-41. A, Schematic illustration of alveolar compression of weakened bronchiolar A, Schematic illustration of alveolar compression of weakened bronchiolar airways during normal expiration in patients with chronic obstructive pulmonary disease airways during normal expiration in patients with chronic obstructive pulmonary disease (e.g., emphysema). B, Effects of pursed-lip breathing. The weakened bronchiolar airways (e.g., emphysema). B, Effects of pursed-lip breathing. The weakened bronchiolar airways
are kept open by the effects of positive pressure created by pursed lips during expiration.are kept open by the effects of positive pressure created by pursed lips during expiration.

Copyright © 2006 by Mosby, Inc.Slide 42
Digital Clubbing
Figure 2-46. Digital clubbing.Figure 2-46. Digital clubbing.

Copyright © 2006 by Mosby, Inc.Slide 43
Clinical Data Obtained at the Clinical Data Obtained at the Patient’s BedsidePatient’s Bedside
Peripheral edema and venous distentionPeripheral edema and venous distention
Distended neck veinsDistended neck veins
Pitting edemaPitting edema
Enlarged and tender liverEnlarged and tender liver

Copyright © 2006 by Mosby, Inc.Slide 44
DistendedDistendedNeck VeinsNeck Veins
Figure 2-48. Distended neck veins (Figure 2-48. Distended neck veins (arrowsarrows).).

Copyright © 2006 by Mosby, Inc.Slide 45
Figure 2-47. Pitting edema. From Bloom A, Ireland J: Figure 2-47. Pitting edema. From Bloom A, Ireland J: Color atlas of diabetesColor atlas of diabetes, ed 2,, ed 2,London, 1992, Mosby-Wolfe.London, 1992, Mosby-Wolfe.

Copyright © 2006 by Mosby, Inc.Slide 46
Clinical Data Obtained at the Clinical Data Obtained at the Patient’s BedsidePatient’s Bedside
Cough, sputum production, hemoptysisCough, sputum production, hemoptysis
Chest assessment findingsChest assessment findings Hyperresonant percussion noteHyperresonant percussion note
Diminished breath soundsDiminished breath sounds
Diminished heart soundsDiminished heart sounds
Decreased tactile and vocal fremitusDecreased tactile and vocal fremitus
Crackles/rhonchi/wheezingCrackles/rhonchi/wheezing

Copyright © 2006 by Mosby, Inc.Slide 47
Figure 2-12. Figure 2-12. Percussion becomes more hyperresonant with alveolar hyperinflation.Percussion becomes more hyperresonant with alveolar hyperinflation.

Copyright © 2006 by Mosby, Inc.Slide 48
Figure 2-17. Figure 2-17. As air trapping and alveolar hyperinflation develop in obstructive As air trapping and alveolar hyperinflation develop in obstructive lung diseases, breath sounds progressively diminish.lung diseases, breath sounds progressively diminish.

Copyright © 2006 by Mosby, Inc.Slide 49
Clinical Data Obtained from Clinical Data Obtained from Laboratory Tests and Special Laboratory Tests and Special
ProceduresProcedures

Copyright © 2006 by Mosby, Inc.Slide 50
Pulmonary Function Study: Pulmonary Function Study: Expiratory Maneuver FindingsExpiratory Maneuver Findings
FVCFVC FEVFEVTT FEFFEF25%-75%25%-75% FEFFEF200-1200200-1200
PEFRPEFR MVVMVV FEFFEF50%50% FEVFEV1%1%

Copyright © 2006 by Mosby, Inc.Slide 51
Pulmonary Function Study: Pulmonary Function Study: Lung Volume and Capacity Findings Lung Volume and Capacity Findings
VVTT RV FRC TLC RV FRC TLC
N or N or N or N or
VCVC IC ERV RV/TLC ratio IC ERV RV/TLC ratio
N or N or
N or N or

Copyright © 2006 by Mosby, Inc.Slide 52
Arterial Blood GasesArterial Blood Gases
Mild to Moderate Chronic BronchitisMild to Moderate Chronic Bronchitis
Acute alveolar hyperventilation with Acute alveolar hyperventilation with hypoxemiahypoxemia
pH PaCO2 HCO3- PaO2
(Slightly)

Copyright © 2006 by Mosby, Inc.Slide 53
Time and Progression of Disease Time and Progression of Disease
100100
5050
3030
8080
00
PaCO2
1010
2020
4040
Alveolar HyperventilationAlveolar Hyperventilation
6060
7070
9090 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors
Point at which PaO2 declines enough to stimulate peripheral oxygen receptors
PaO2
Disease OnsetDisease OnsetP
aO2
or
PaC
O2
PaO
2 o
r P
aCO
2
Figure 4-2. PaO2 and PaCO2 trends during acute alveolar hyperventilation.

Copyright © 2006 by Mosby, Inc.Slide 54
Arterial Blood GasesArterial Blood Gases
Severe Chronic BronchitisSevere Chronic Bronchitis
Chronic ventilatory failure with hypoxemiaChronic ventilatory failure with hypoxemia
pH PapH PaCOCO22 HCO HCO33-- Pa PaOO2 2
Normal Normal (Significantly)(Significantly)

Copyright © 2006 by Mosby, Inc.Slide 55
Time and Progression of DiseaseTime and Progression of Disease
100100
5050
3030
80
0
PaO2
1010
2020
4040
Alveolar HyperventilationAlveolar Hyperventilation
6060
7070
9090Point at which PaO2 declines enough to stimulate peripheral oxygen receptors
Point at which PaO2 declines enough to stimulate peripheral oxygen receptors
PaCO 2
Chronic Ventilatory Failure Chronic Ventilatory FailureDisease OnsetDisease Onset
Point at which disease becomes severe and patient begins to become fatigued
Point at which disease becomes severe and patient begins to become fatigued
Pa0
2 o
r P
aC0 2
Pa0
2 o
r P
aC0 2
Figure 4-7. PaO2 and PaCO2 trends during acute or chronic ventilatory failure.

Copyright © 2006 by Mosby, Inc.Slide 56
Acute Ventilatory Changes Acute Ventilatory Changes Superimposed on Chronic Ventilatory Superimposed on Chronic Ventilatory
FailureFailure
Acute alveolar hyperventilation on chronic Acute alveolar hyperventilation on chronic ventilatory failureventilatory failure
Acute ventilatory failure on chronic Acute ventilatory failure on chronic ventilatory failureventilatory failure

Copyright © 2006 by Mosby, Inc.Slide 57
Abnormal Laboratory Tests and Abnormal Laboratory Tests and ProceduresProcedures
Hematology Hematology Increased hematocrit and hemoglobinIncreased hematocrit and hemoglobin
Electrolytes Electrolytes Hypochloremia (chronic ventilatory failure)Hypochloremia (chronic ventilatory failure) Increased bicarbonate (chronic ventilatory failure)Increased bicarbonate (chronic ventilatory failure)
Sputum examinationSputum examination Increased white blood cellsIncreased white blood cells Streptococcus pneumoniaeStreptococcus pneumoniae Haemophilus influenzaeHaemophilus influenzae Moraxella catarrhalisMoraxella catarrhalis

Copyright © 2006 by Mosby, Inc.Slide 58
Radiologic FindingsRadiologic Findings
Chest radiographChest radiograph
Translucent (dark) lung fieldsTranslucent (dark) lung fields
Depressed or flattened diaphragmsDepressed or flattened diaphragms
Long and narrow heartLong and narrow heart
Enlarged heartEnlarged heart

Copyright © 2006 by Mosby, Inc.Slide 59
Figure 11-2. Chest X-ray film of a patient with chronic bronchitis. Note the translucent (dark) lung fields, depressed diaphragms, and long and narrow heart.

Copyright © 2006 by Mosby, Inc.Slide 60
Radiologic FindingsRadiologic Findings
BronchogramBronchogram
Small spikelike protrusionsSmall spikelike protrusions

Copyright © 2006 by Mosby, Inc.Slide 61
Figure 11-3. Chronic bronchitis. Bronchogram with localized view of left hilum. Rounded collections of contrast lie adjacent to bronchial walls and are particularly well seen below the left main stem bronchus (arrow) in this film. They are caused by contrast in dilated mucous gland ducts. (From Armstrong P, Wilson AG, Dee P: Imaging of diseases of the chest, St. Louis, 1990, Mosby.)

Copyright © 2006 by Mosby, Inc.Slide 62
General Management of General Management of Chronic BronchitisChronic Bronchitis
Patient and family educationPatient and family education
Behavioral managementBehavioral management Avoidance of smoking and inhaled irritantsAvoidance of smoking and inhaled irritants
Avoidance of infectionsAvoidance of infections
Respiratory care treatment protocolsRespiratory care treatment protocols Oxygen therapy protocolOxygen therapy protocol
Bronchopulmonary hygiene therapy protocolBronchopulmonary hygiene therapy protocol
Aerosolized medication protocolAerosolized medication protocol
Mechanical ventilation protocolMechanical ventilation protocol

Copyright © 2006 by Mosby, Inc.Slide 63
Global Initiative for Chronic
Obstructive
Lung
Disease
GOLD StandardsGOLD Standards

Copyright © 2006 by Mosby, Inc.Slide 64
Figure 11-4. Acute exacerbation of COPD (AECOPD): Guideline algorithm (ACCP/ACP-ASIM). CXR, Chest X-ray; NPPV, noninvasive positive pressure ventilation; PEFR, peak expiratory flow rate; URI, upper respiratory infection. (From GUIDELINES Pocketcard: Managing Chronic Obstructive Pulmonary Disease. Baltimore, 2004, Version 4.0, International Guidelines Center.)

Copyright © 2006 by Mosby, Inc.Slide 65
Figure 11-4. (Close-ups). (From GUIDELINES Pocketcard: Managing Chronic Obstructive Pulmonary Disease. Baltimore, 2004, Version 4.0, International Guidelines Center.)

Copyright © 2006 by Mosby, Inc.Slide 66
Figure 11-4. (Close-ups). (From GUIDELINES Pocketcard: Managing Chronic Obstructive Pulmonary Disease. Baltimore, 2004, Version 4.0, International Guidelines Center.)

Copyright © 2006 by Mosby, Inc.Slide 67
Figure 11-4. (Close-ups). (From GUIDELINES Pocketcard: Managing Chronic Obstructive Pulmonary Disease. Baltimore, 2004, Version 4.0, International Guidelines Center.)

Copyright © 2006 by Mosby, Inc.Slide 68
Figure 11-4. (Close-ups). (From GUIDELINES Pocketcard: Managing Chronic Obstructive Pulmonary Disease. Baltimore, 2004, Version 4.0, International Guidelines Center.)

Copyright © 2006 by Mosby, Inc.Slide 69
Figure 11-4. Acute exacerbation of COPD (AECOPD): Guideline algorithm (ACCP/ACP-ASIM). CXR, Chest X-ray; NPPV, noninvasive positive pressure ventilation; PEFR, peak expiratory flow rate; URI, upper respiratory infection. (From GUIDELINES Pocketcard: Managing Chronic Obstructive Pulmonary Disease. Baltimore, 2004, Version 4.0, International Guidelines Center.)

Copyright © 2006 by Mosby, Inc.Slide 70
FLAIL CHESTFLAIL CHEST

Copyright © 2006 by Mosby, Inc.Slide 71
A 22 yr old male presented in emergency A 22 yr old male presented in emergency department with history of road traffic trauma to department with history of road traffic trauma to chest he was ishirt of breath and was in severe chest he was ishirt of breath and was in severe painpain
What are possibilities?What are possibilities?

Copyright © 2006 by Mosby, Inc.Slide 72
On examination patient was tachycadic and On examination patient was tachycadic and tachypnic cyanosed his chest wall moves in tachypnic cyanosed his chest wall moves in duing inspiration at certain points and out duing inspiration at certain points and out during expirationduring expiration
These findings suggest what?These findings suggest what?

Copyright © 2006 by Mosby, Inc.Slide 73
73
AnatomyAnatomy

Copyright © 2006 by Mosby, Inc.Slide 74
74
Overview of Chest InjuriesOverview of Chest Injuries
Can be life-threateningCan be life-threatening
May result in damage to either theMay result in damage to either the heart or the lung heart or the lung and cause severe internaland cause severe internal bleedingbleeding
Rib cage fractures may result in serious injury toRib cage fractures may result in serious injury to vital vital organsorgans
Deep, Deep, open open wounds allow air to enter the chestwounds allow air to enter the chest cavitycavity
ClosedClosed wounds usually involve injury to wounds usually involve injury to the ribs and the ribs and possibly underlying structurespossibly underlying structures

Copyright © 2006 by Mosby, Inc.Slide 75
75
Signs of Chest InjuriesSigns of Chest Injuries
An obvious chest woundAn obvious chest wound
Impaired breathingImpaired breathing
Irregular –Irregular – or lack ofor lack of – chest expansion– chest expansion
Coughing-up of bloodCoughing-up of blood
ShockShock
Subcutaneous emphysema: crackling Subcutaneous emphysema: crackling sensationsensation

Copyright © 2006 by Mosby, Inc.Slide 76
76
Closed Chest InjuriesClosed Chest Injuries
Rib fractureRib fracture
Flail chestFlail chest
PneumothoraxPneumothorax

Copyright © 2006 by Mosby, Inc.Slide 77
77
Rib FractureRib Fracture
Rib fractures are almost always the result of Rib fractures are almost always the result of trauma (a blow) to the rib cagetrauma (a blow) to the rib cage
Signs and SymptomsSigns and Symptoms leaning toward the injured side leaning toward the injured side
if the rib has punctured a lung, air can escape into the if the rib has punctured a lung, air can escape into the tissues of the chest wall creating a crackling sensation tissues of the chest wall creating a crackling sensation (- Subcutaneous Emphysema)(- Subcutaneous Emphysema)
unwillingness to take a deep breathunwillingness to take a deep breath
complaining of local pain and tendernesscomplaining of local pain and tenderness
pain when moving the rib cage when breathing or pain when moving the rib cage when breathing or coughingcoughing

Copyright © 2006 by Mosby, Inc.Slide 78
78
Rib FractureRib Fracture
TreatmentTreatment Give oxygenGive oxygen
Make the patient as comfortable as possibleMake the patient as comfortable as possible
Activate EMS and treat as Load and GoActivate EMS and treat as Load and Go
Transport patientTransport patient in the position of maximum comfort on the injured in the position of maximum comfort on the injured
sideside

Copyright © 2006 by Mosby, Inc.Slide 79
79
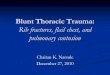
Flail ChestFlail Chest
Several adjacent ribs fractured in more than Several adjacent ribs fractured in more than one place can produce a loose section of the one place can produce a loose section of the chest wallchest wall
The flail section moves inward when the The flail section moves inward when the patient breathes in, and outward when the patient breathes in, and outward when the patient breathes outpatient breathes out
This phenomenon is known as paradoxical This phenomenon is known as paradoxical movementmovement

Copyright © 2006 by Mosby, Inc.Slide 80
80
Flail ChestFlail Chest
Signs and symptomsSigns and symptoms shortness of breathshortness of breath
swelling over the injury siteswelling over the injury site
shockshock
muscle splinting of the injury sitemuscle splinting of the injury site
severe pain on inhalation/exhalationsevere pain on inhalation/exhalation
possible paradoxical movementpossible paradoxical movement

Copyright © 2006 by Mosby, Inc.Slide 81
81
Flail ChestFlail Chest
TreatmentTreatment Give oxygen as soon as possibleGive oxygen as soon as possible
Be prepared to give ARBe prepared to give AR
Help the patient get in a comfortable position and Help the patient get in a comfortable position and transport to medical aidtransport to medical aid
Continue to monitor vital signsContinue to monitor vital signs
Unless there is substantial bleeding, do not apply Unless there is substantial bleeding, do not apply bulky padding or dressingsbulky padding or dressings

Copyright © 2006 by Mosby, Inc.Slide 82
82
Use of Dressings on a Flail ChestUse of Dressings on a Flail Chest
Only consider taped-on pad as a treatment in the following Only consider taped-on pad as a treatment in the following cases:cases: if there is likely to be a prolonged time before evacuation and access if there is likely to be a prolonged time before evacuation and access
to medical care to medical care
if the patient has fatigued their chest musclesif the patient has fatigued their chest muscles
To apply dressingsTo apply dressings Press the segment inward with your gloved hand to stabilize itPress the segment inward with your gloved hand to stabilize it
Splint in the inward position with a pillow, large bulky dressing, or Splint in the inward position with a pillow, large bulky dressing, or folded blanket or parkafolded blanket or parka
Secure this thoroughly in place with tapeSecure this thoroughly in place with tape
Be prepared to help breathing with ARBe prepared to help breathing with AR
Do not hold in place with bandages encircling the chest. This would Do not hold in place with bandages encircling the chest. This would further impair the patient’s breathing effortfurther impair the patient’s breathing effort

Copyright © 2006 by Mosby, Inc.Slide 83
83
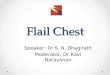
PneumothoraxPneumothorax
IIs a condition that results froms a condition that results from air entering the air entering the interpleural space. The air in theinterpleural space. The air in the interpleural interpleural space compresses the lung andspace compresses the lung and prevents prevents normal breathing.normal breathing.
There are two types of pneumothorax:There are two types of pneumothorax: Tension pneumothoraxTension pneumothorax
Spontaneous pneumothoraxSpontaneous pneumothorax

Copyright © 2006 by Mosby, Inc.Slide 84
84
PneumothoraxPneumothorax
Signs and symptomsSigns and symptoms reduction of normal respiratory movements on the reduction of normal respiratory movements on the
affected sideaffected side
a fall in blood pressurea fall in blood pressure
weak and rapid pulseweak and rapid pulse
a sudden sharp chest paina sudden sharp chest pain

Copyright © 2006 by Mosby, Inc.Slide 85
85
PneumothoraxPneumothorax
Treatment for Tension PneumothoraxTreatment for Tension Pneumothorax Give oxygenGive oxygen
Activate EMS and treat as Load and GoActivate EMS and treat as Load and Go
Continue to monitor vital signsContinue to monitor vital signs
Treatment for Spontaneous PneumothoraxTreatment for Spontaneous Pneumothorax Give oxygenGive oxygen
Transport to medical aidTransport to medical aid
The patient may prefer to be transported sitting up.The patient may prefer to be transported sitting up.