Embed Size (px)
Citation preview
Klebsiella Pneumoniae Carbapenemase
APPE Cycle 1, June 2016Kirk Benack & Kimberly TsaiPharm D. 2017 Candidates
Objectives
2
● Describe background of traditional treatment with carbapenems as well as the mechanisms behind emerging multidrug resistance
● Specify characteristics and clinical significance unique to Klebsiella Pneumoniae Carbapenemase (KPC)-producing organisms
● Explore the available agents used most commonly to treat KPC organisms
● Review available evidence to identify benefits and limitations of various agents
● Identify newly-approved agents as well as those currently in the pipeline that may offer potential use against KPC

Background
3
Background
Mechanisms of Resistance
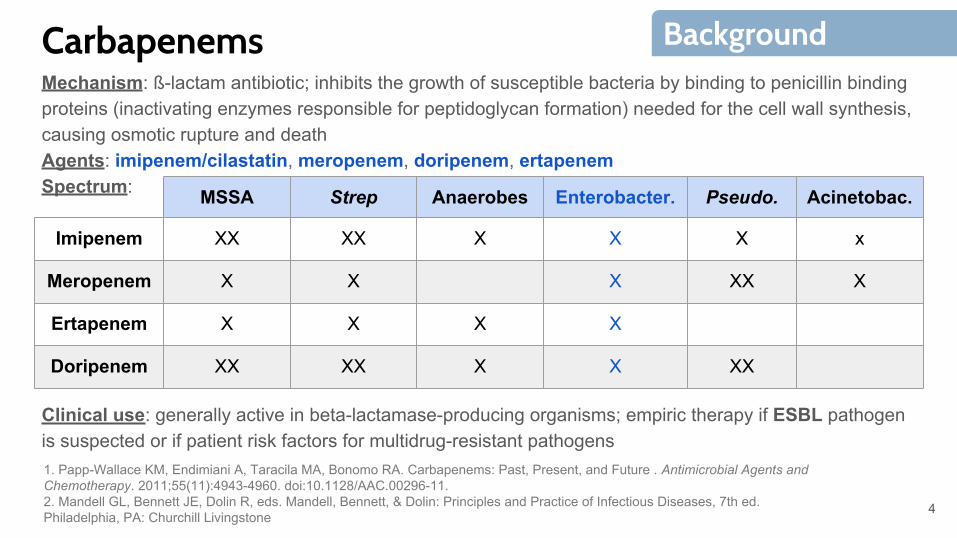
CarbapenemsMechanism: ß-lactam antibiotic; inhibits the growth of susceptible bacteria by binding to penicillin binding proteins (inactivating enzymes responsible for peptidoglycan formation) needed for the cell wall synthesis, causing osmotic rupture and deathAgents: imipenem/cilastatin, meropenem, doripenem, ertapenemSpectrum:
Clinical use: generally active in beta-lactamase-producing organisms; empiric therapy if ESBL pathogen is suspected or if patient risk factors for multidrug-resistant pathogens
MSSA Strep Anaerobes Enterobacter. Pseudo. Acinetobac.
Imipenem XX XX X X X x
Meropenem X X X XX X
Ertapenem X X X X
Doripenem XX XX X X XX
4
Background
1. Papp-Wallace KM, Endimiani A, Taracila MA, Bonomo RA. Carbapenems: Past, Present, and Future . Antimicrobial Agents and Chemotherapy. 2011;55(11):4943-4960. doi:10.1128/AAC.00296-11.2. Mandell GL, Bennett JE, Dolin R, eds. Mandell, Bennett, & Dolin: Principles and Practice of Infectious Diseases, 7th ed. Philadelphia, PA: Churchill Livingstone
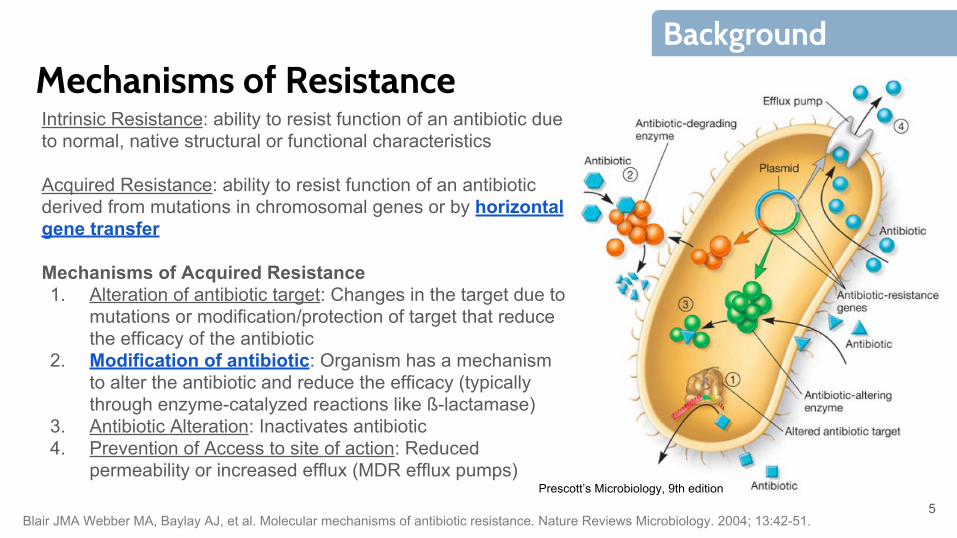
Mechanisms of ResistanceIntrinsic Resistance: ability to resist function of an antibiotic due to normal, native structural or functional characteristics
Acquired Resistance: ability to resist function of an antibiotic derived from mutations in chromosomal genes or by horizontal gene transfer
Mechanisms of Acquired Resistance1. Alteration of antibiotic target: Changes in the target due to
mutations or modification/protection of target that reduce the efficacy of the antibiotic
2. Modification of antibiotic: Organism has a mechanism to alter the antibiotic and reduce the efficacy (typically through enzyme-catalyzed reactions like ß-lactamase)
3. Antibiotic Alteration: Inactivates antibiotic4. Prevention of Access to site of action: Reduced
permeability or increased efflux (MDR efflux pumps)Prescott’s Microbiology, 9th edition
5
Background
Blair JMA Webber MA, Baylay AJ, et al. Molecular mechanisms of antibiotic resistance. Nature Reviews Microbiology. 2004; 13:42-51.
Carbapenem Resistance
6
Terms
Epidemiology
Klebsiella Pneumoniae Carbapenemase (KPC)
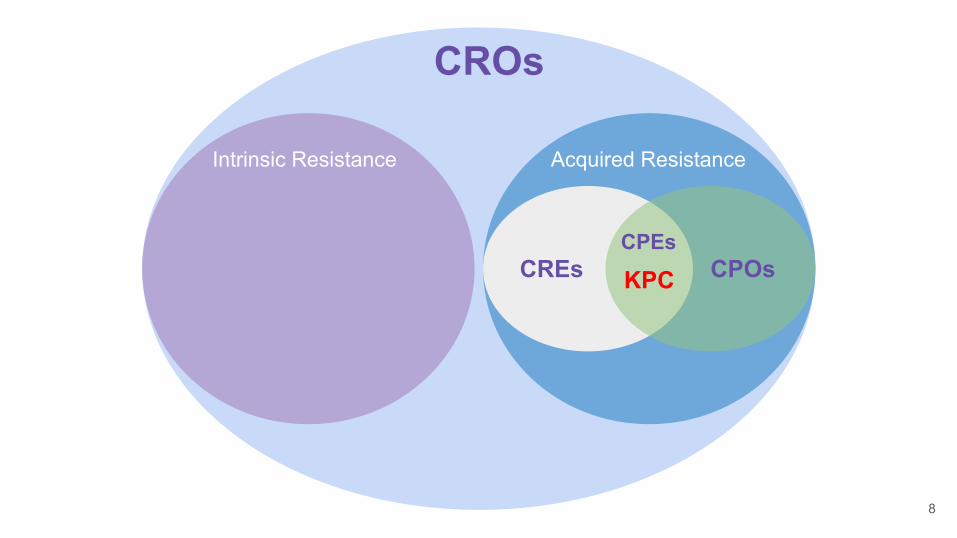
CROs / CPOs / CREs / CPEsCarbapenem-Resistant Organism (CRO): a term used to describe gram negative bacteria that are resistant to carbapenems (and most other ß-lactams) by means of inherent resistance or through the production of a carbapenemase (Carbapenemase-Producing Organisms (CPOs)), ESBL, or AmpC
Carbapenem-resistant Enterobacteriaceae (CRE): Enterobacteriaceae that are resistant to carbapenems by means of the production of a carbapenemase (CP-CRE), ESBL, and/or AmpC
Carbapenemase-producing Enterobacteriaceae (CPE): Enterobacteriaceae that are resistant to carbapenems solely by means of the production of a carbapenemase
7
Carbapenem Resistance
Carbapenem-resistant enterobacteriaceae in healthcare settings. Centers for Disease Control and Prevention website http://www.cdc.gov/HAI/organisms/cre/index.html. Updated January 1, 2016. Accessed June 10, 2016.
(KPC)
CROs
Intrinsic Resistance Acquired Resistance
CREs CPOsCPEs
KPC
8
Epidemiology- Summary trends from the MYSTIC Program show that meropenem resistance of Klebsiella pneumoniae (K. pneumoniae) increased significantly from 0.5% in 2004 to 5.6% in 2008
- Carbapenem resistance was reported in 4.0% of Escherichia coli and 10.8% of K. pneumoniae cases associated with device-related infections from 2006-2007
- As of February 2016, KPC-producing organisms have been reported in 48 out of 50 states
- In a study conducted at Mount Sinai Hospital, patients infected with KPC infections were more likely to die during hospitalization (48% vs. 20%; P<.001) and from infection (38% vs. 12%; P<.001)
9
Carbapenem Resistance
1. Rhomberg P, Jones R. Summary trends for the Meropenem Yearly Susceptibility Test Information Collection Program: a 10-year experience in the United States (1999-2008). Diagnostic Microbiology and Infectious Disease 2009. 65:414-4262. Jones R, Mendes C, Turner P, et al. An overview of the Meropenem Yearly Susceptibility Test Information Collection (MYSTIC) Program: 1997-2004. Diagnostic Microbiology and Infectious Disease 2005. 53:247-456. 3. Hidron AI, Edwards JR, Patel J, et al. NHSN annual update: Antimicrobial-resistant pathogens associated with healthcare-associated infections: Annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006-2007. Infect Control Hosp Epiemiol 2008; 29996-1011.4. Patel G, Huprikar S, Factor SH, Jenkins SG, Calfee DP. Outcomes of carbapenem-resistant Klebsiella pneumoniae infection and the impact of antimicrobial and adjunctive therapies. Infect Control Hosp Epidemiol. 2008; 29:1099-106.
Klebsiella Pneumoniae Carbapenemase (KPC)- First KPC-producing isolate was reported in 1996 (not the first carbapenemase to be discovered); since then has become the most prevalent mechanism of carbapenem resistance in the US
- Broad hydrolysis spectrum -- enzyme hydrolyzes most ß-lactam classes including cefotaxime, cefoxitin, and ceftazidime
- Resistance to other antibiotic classes (fluoroquinolones & aminoglycosides) often exhibited
- Unique characteristic: gene for enzyme (bla-kpc) is located on transferable plasmids, therefore providing high potential for spread & difficult infection control
- Variants have been reported following discovery (KPC-1, KPC-2, KPC-3, KPC-4)
- A most optimal treatment for KPC currently remains unknown due to limited treatment data; limited treatment options have forced the revival of older agents that were historically avoided
10
Carbapenem Resistance
1. Queenan AM, Bush K. Carbapenemases: the versatile ß-lactamases. Clin Microbiol Rev 2007; 20:440-582. Arnold RS, Thom KA, Sharma S, et al. Emergence of Klebsiella pneumoniae carbapenemase (KPC)-producing bacteria. South Med J. 2011;104(1):40-45
Identifying KPCRisk factors associated with acquisition of KPC:
- Exposure to healthcare- Receipt of mechanical to ventilation- Previous exposure to antimicrobials - Poor functional status- ICU stay- Longer length of stay
- It has been noted that automatic susceptibility testing fails to detect KPC
- CLSI recommends that Enterobacteriaceae with elevated MICs to carbapenems (2-4 µg/mL) or reduced disk diffusion zones be tested for production of a carbapenemase using the modified Hodge test (MHT)
- Lower carbapenem breakpoints (Table 1) should also be established
11
Carbapenem Resistance
1. Anderson KF, Lonsway DR, Rasheed JK, et al. Evaluation of methods to identify the klebsiella pneumoniae carbapenemase in enterobacteraceae. Journal of Clinical Microbiology. 2007;2723-2725. 2. Schwaber MJ, Klarfeld-Laidjii S, Navon-Venezia S, et al. Predictors of carbapenem-resistant Klebsiella pneumoniae acquisition among hospitalized adults and effect of acquisition on mortality. Antimicrob Agents Chemother 2008; 52:1028-33.3. Hussein K, Sprecher H, Mashiach T, et al. Carbapenem resistance among Klebsiella pneumoniate isolates: risk factors, molecular characteristics, susceptibility patterns. Infect Control Hosp Epidemiol 2009; 30-666-71.
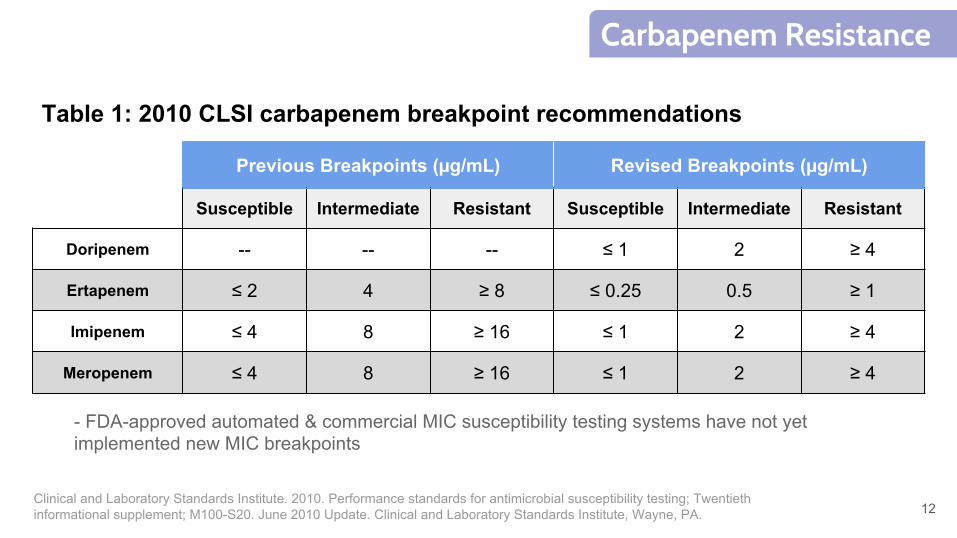
Table 1: 2010 CLSI carbapenem breakpoint recommendations
Previous Breakpoints (µg/mL) Revised Breakpoints (µg/mL)
Susceptible Intermediate Resistant Susceptible Intermediate Resistant
Doripenem -- -- -- ≤ 1 2 ≥ 4
Ertapenem ≤ 2 4 ≥ 8 ≤ 0.25 0.5 ≥ 1
Imipenem ≤ 4 8 ≥ 16 ≤ 1 2 ≥ 4
Meropenem ≤ 4 8 ≥ 16 ≤ 1 2 ≥ 4
- FDA-approved automated & commercial MIC susceptibility testing systems have not yet implemented new MIC breakpoints
12
Carbapenem Resistance
Clinical and Laboratory Standards Institute. 2010. Performance standards for antimicrobial susceptibility testing; Twentieth informational supplement; M100-S20. June 2010 Update. Clinical and Laboratory Standards Institute, Wayne, PA.
Current Treatment
13
Tigecycline
Polymyxins
Carbapenems
Aminoglycosides
Fosfomycin
Approach
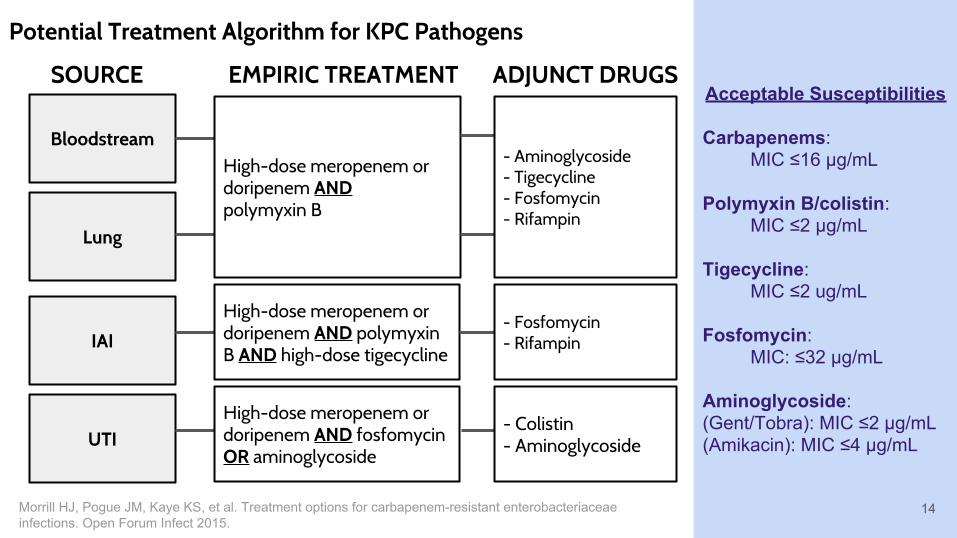
Potential Treatment Algorithm for KPC Pathogens
Bloodstream
Lung
IAI
UTI
SOURCE
High-dose meropenem or doripenem AND polymyxin B
High-dose meropenem or doripenem AND polymyxin B AND high-dose tigecycline
High-dose meropenem or doripenem AND fosfomycin OR aminoglycoside
EMPIRIC TREATMENT
- Aminoglycoside- Tigecycline- Fosfomycin- Rifampin
- Fosfomycin- Rifampin
- Colistin- Aminoglycoside
Acceptable Susceptibilities
Carbapenems:MIC ≤16 µg/mL
Polymyxin B/colistin:MIC ≤2 µg/mL
Tigecycline:MIC ≤2 ug/mL
Fosfomycin:MIC: ≤32 µg/mL
Aminoglycoside:(Gent/Tobra): MIC ≤2 µg/mL(Amikacin): MIC ≤4 µg/mL
ADJUNCT DRUGS
14Morrill HJ, Pogue JM, Kaye KS, et al. Treatment options for carbapenem-resistant enterobacteriaceae infections. Open Forum Infect 2015.
Limitations with Current Treatment● No randomized clinical trials to support use of current antimicrobials
for KPC-related infections, current data mostly relies on case reviews & small, observational studies
● Wide heterogeneity of published studies● Number of patients with KPC too small to hold proper randomized
clinical study ● Majority of patients with KPC already have significant comorbidities;
overall all-cause mortality rate is high ● Small sample sizes among current available studies; clinical
significance from results difficult to determine15
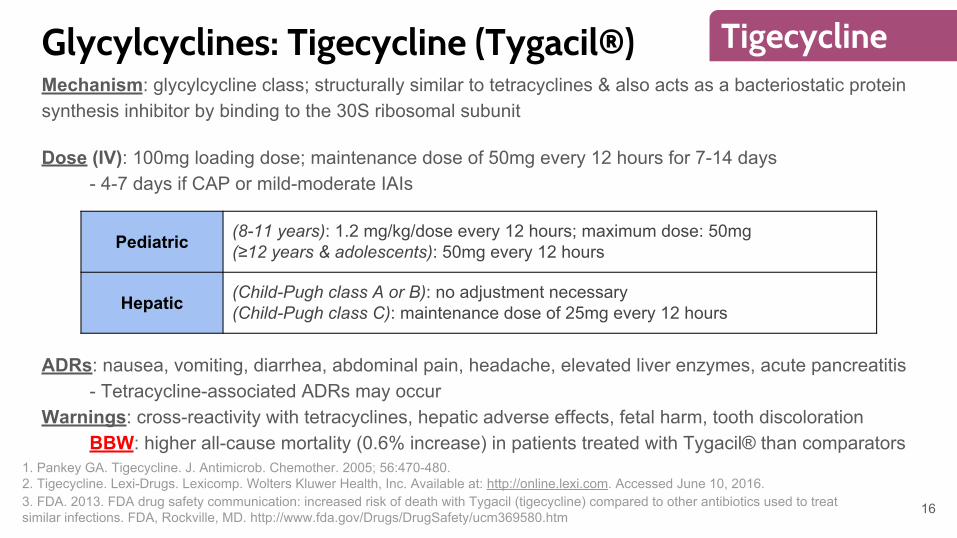
Glycylcyclines: Tigecycline (Tygacil®)Mechanism: glycylcycline class; structurally similar to tetracyclines & also acts as a bacteriostatic protein synthesis inhibitor by binding to the 30S ribosomal subunit
Dose (IV): 100mg loading dose; maintenance dose of 50mg every 12 hours for 7-14 days - 4-7 days if CAP or mild-moderate IAIs
ADRs: nausea, vomiting, diarrhea, abdominal pain, headache, elevated liver enzymes, acute pancreatitis- Tetracycline-associated ADRs may occur
Warnings: cross-reactivity with tetracyclines, hepatic adverse effects, fetal harm, tooth discolorationBBW: higher all-cause mortality (0.6% increase) in patients treated with Tygacil® than comparators
Pediatric (8-11 years): 1.2 mg/kg/dose every 12 hours; maximum dose: 50mg(≥12 years & adolescents): 50mg every 12 hours
Hepatic (Child-Pugh class A or B): no adjustment necessary(Child-Pugh class C): maintenance dose of 25mg every 12 hours
16
Tigecycline
1. Pankey GA. Tigecycline. J. Antimicrob. Chemother. 2005; 56:470-480.2. Tigecycline. Lexi-Drugs. Lexicomp. Wolters Kluwer Health, Inc. Available at: http://online.lexi.com. Accessed June 10, 2016.3. FDA. 2013. FDA drug safety communication: increased risk of death with Tygacil (tigecycline) compared to other antibiotics used to treat similar infections. FDA, Rockville, MD. http://www.fda.gov/Drugs/DrugSafety/ucm369580.htm
17
Tigecycline
Wikipedia: Tigecycline.
Pharmacokinetics: linear pharmacokinetics unaffected by age or sexDistribution: extensive distribution into tissues especially into the gallbladder, lungs, and colon yet limited CSF, plasma, and urinary distributionMetabolism: Hepatic via N-glucuronidation and N-acetylationElimination: mean half-life of 37-38 hours
- Not significantly affected by mild hepatic impairment (Child Pugh A) - Moderate hepatic impairment (Child Pugh B) resulted in 25% reduction in systemic clearance- Severe hepatic impairment (Child Pugh C) resulted in 55% reduction in systemic clearance
Pharmacodynamics: time-dependent effect with prolonged postantibiotic effects- AUC24:MIC ratio of 5-10 recommended for most organisms
18
Tigecycline
1. Stein GE, William CA. Tigecycline: A Critical Analysis. Clin Infect Dis. 2016; 43(4): 518-524.2, Tigecycline. Lexi-Drugs. Lexicomp. Wolters Kluwer Health, Inc. Available at: http://online.lexi.com. Accessed June 10, 2016.
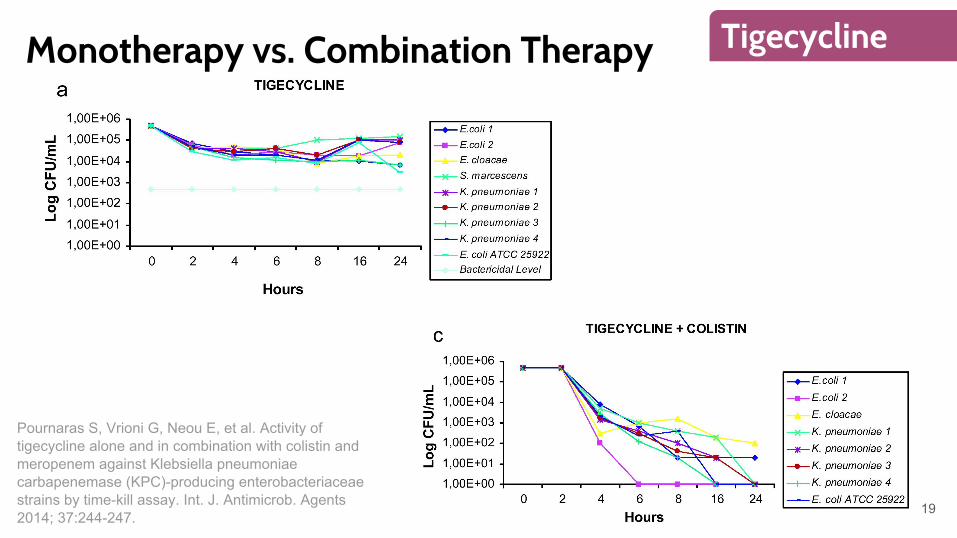
Monotherapy vs. Combination Therapy
19
Tigecycline
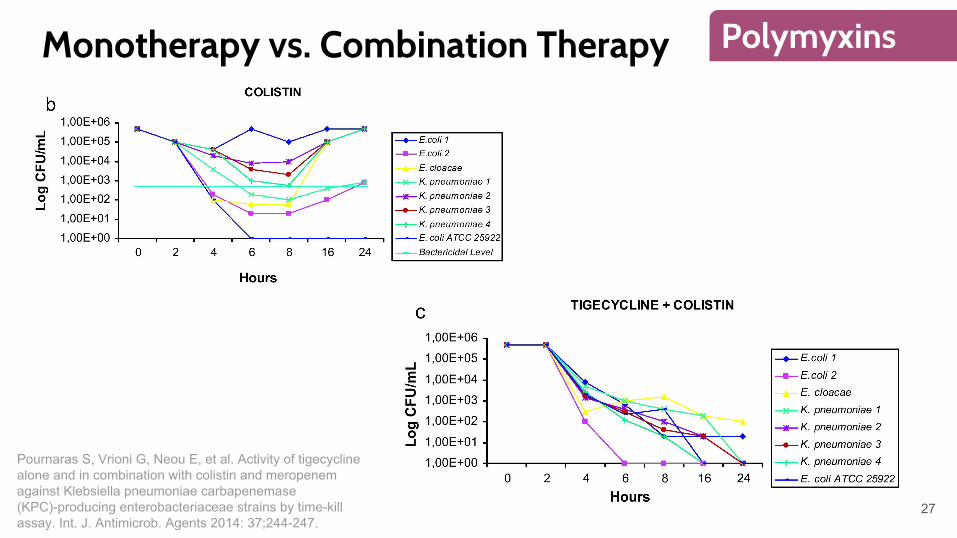
Pournaras S, Vrioni G, Neou E, et al. Activity of tigecycline alone and in combination with colistin and meropenem against Klebsiella pneumoniae carbapenemase (KPC)-producing enterobacteriaceae strains by time-kill assay. Int. J. Antimicrob. Agents 2014; 37:244-247.
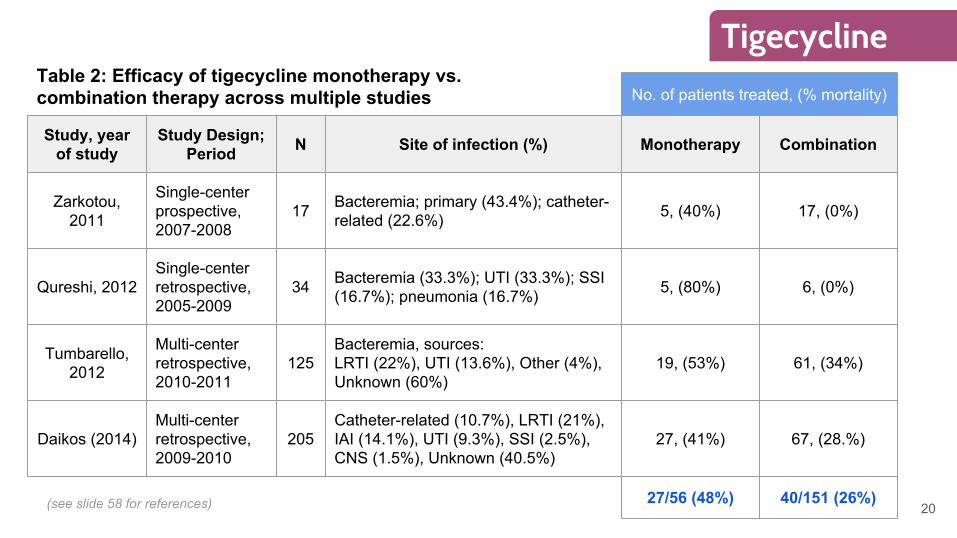
No. of patients treated, (% mortality)
Study, year of study
Study Design; Period N Site of infection (%) Monotherapy Combination
Zarkotou, 2011
Single-center prospective, 2007-2008
17 Bacteremia; primary (43.4%); catheter-related (22.6%) 5, (40%) 17, (0%)
Qureshi, 2012Single-center retrospective, 2005-2009
34 Bacteremia (33.3%); UTI (33.3%); SSI (16.7%); pneumonia (16.7%) 5, (80%) 6, (0%)
Tumbarello, 2012
Multi-center retrospective, 2010-2011
125Bacteremia, sources:LRTI (22%), UTI (13.6%), Other (4%), Unknown (60%)
19, (53%) 61, (34%)
Daikos (2014)Multi-center retrospective, 2009-2010
205Catheter-related (10.7%), LRTI (21%), IAI (14.1%), UTI (9.3%), SSI (2.5%), CNS (1.5%), Unknown (40.5%)
27, (41%) 67, (28.%)
27/56 (48%) 40/151 (26%)
Table 2: Efficacy of tigecycline monotherapy vs. combination therapy across multiple studies
20
Tigecycline
(see slide 58 for references)
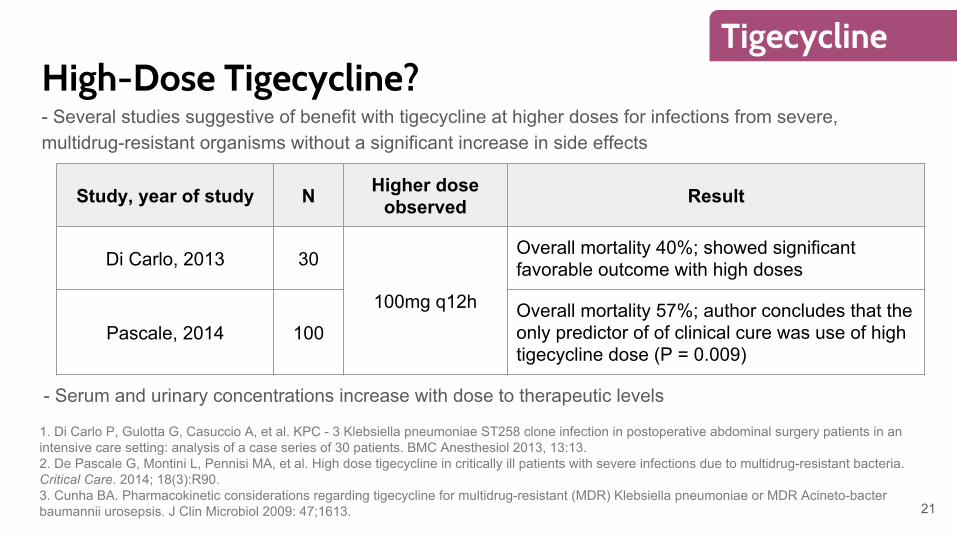
High-Dose Tigecycline?- Several studies suggestive of benefit with tigecycline at higher doses for infections from severe, multidrug-resistant organisms without a significant increase in side effects
21
Tigecycline
Study, year of study N Higher dose observed Result
Di Carlo, 2013 30
100mg q12h
Overall mortality 40%; showed significant favorable outcome with high doses
Pascale, 2014 100Overall mortality 57%; author concludes that the only predictor of of clinical cure was use of high tigecycline dose (P = 0.009)
1. Di Carlo P, Gulotta G, Casuccio A, et al. KPC - 3 Klebsiella pneumoniae ST258 clone infection in postoperative abdominal surgery patients in an intensive care setting: analysis of a case series of 30 patients. BMC Anesthesiol 2013, 13:13. 2. De Pascale G, Montini L, Pennisi MA, et al. High dose tigecycline in critically ill patients with severe infections due to multidrug-resistant bacteria. Critical Care. 2014; 18(3):R90.3. Cunha BA. Pharmacokinetic considerations regarding tigecycline for multidrug-resistant (MDR) Klebsiella pneumoniae or MDR Acineto-bacter baumannii urosepsis. J Clin Microbiol 2009: 47;1613.
- Serum and urinary concentrations increase with dose to therapeutic levels
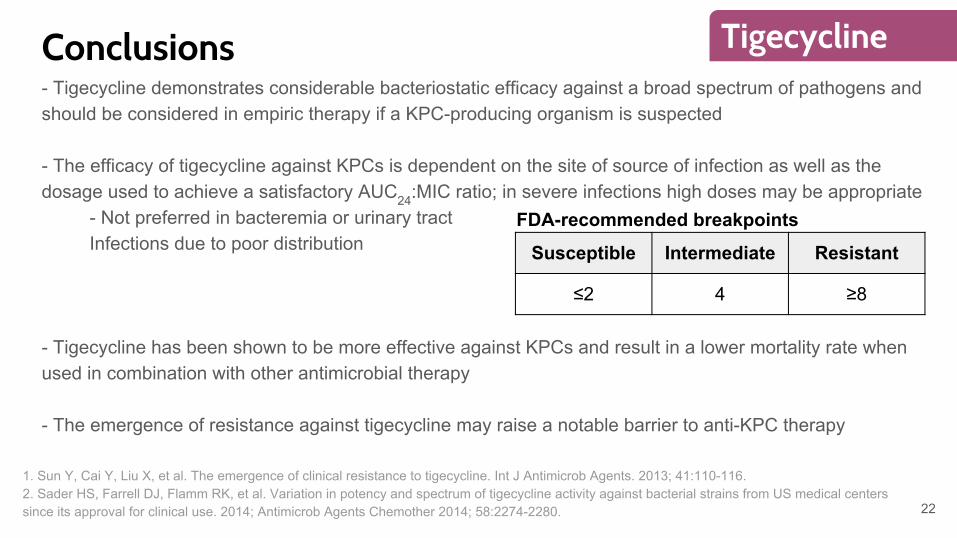
Conclusions- Tigecycline demonstrates considerable bacteriostatic efficacy against a broad spectrum of pathogens and should be considered in empiric therapy if a KPC-producing organism is suspected
- The efficacy of tigecycline against KPCs is dependent on the site of source of infection as well as the dosage used to achieve a satisfactory AUC24:MIC ratio; in severe infections high doses may be appropriate
- Not preferred in bacteremia or urinary tractInfections due to poor distribution
- Tigecycline has been shown to be more effective against KPCs and result in a lower mortality rate when used in combination with other antimicrobial therapy
- The emergence of resistance against tigecycline may raise a notable barrier to anti-KPC therapy
Susceptible Intermediate Resistant
≤2 4 ≥8
22
Tigecycline
1. Sun Y, Cai Y, Liu X, et al. The emergence of clinical resistance to tigecycline. Int J Antimicrob Agents. 2013; 41:110-116. 2. Sader HS, Farrell DJ, Flamm RK, et al. Variation in potency and spectrum of tigecycline activity against bacterial strains from US medical centers since its approval for clinical use. 2014; Antimicrob Agents Chemother 2014; 58:2274-2280.
FDA-recommended breakpoints
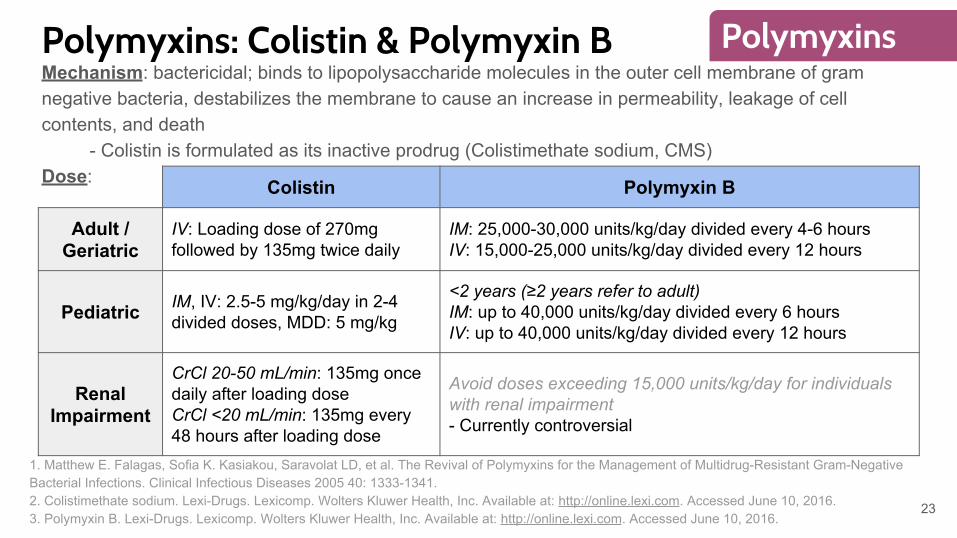
Polymyxins: Colistin & Polymyxin BMechanism: bactericidal; binds to lipopolysaccharide molecules in the outer cell membrane of gram negative bacteria, destabilizes the membrane to cause an increase in permeability, leakage of cell contents, and death
- Colistin is formulated as its inactive prodrug (Colistimethate sodium, CMS)Dose: Colistin Polymyxin B
Adult / Geriatric
IV: Loading dose of 270mg followed by 135mg twice daily
IM: 25,000-30,000 units/kg/day divided every 4-6 hoursIV: 15,000-25,000 units/kg/day divided every 12 hours
Pediatric IM, IV: 2.5-5 mg/kg/day in 2-4 divided doses, MDD: 5 mg/kg
<2 years (≥2 years refer to adult)IM: up to 40,000 units/kg/day divided every 6 hoursIV: up to 40,000 units/kg/day divided every 12 hours
Renal Impairment
CrCl 20-50 mL/min: 135mg once daily after loading doseCrCl <20 mL/min: 135mg every 48 hours after loading dose
Avoid doses exceeding 15,000 units/kg/day for individuals with renal impairment- Currently controversial
23
Polymyxins
1. Matthew E. Falagas, Sofia K. Kasiakou, Saravolat LD, et al. The Revival of Polymyxins for the Management of Multidrug-Resistant Gram-Negative Bacterial Infections. Clinical Infectious Diseases 2005 40: 1333-1341.2. Colistimethate sodium. Lexi-Drugs. Lexicomp. Wolters Kluwer Health, Inc. Available at: http://online.lexi.com. Accessed June 10, 2016.3. Polymyxin B. Lexi-Drugs. Lexicomp. Wolters Kluwer Health, Inc. Available at: http://online.lexi.com. Accessed June 10, 2016.
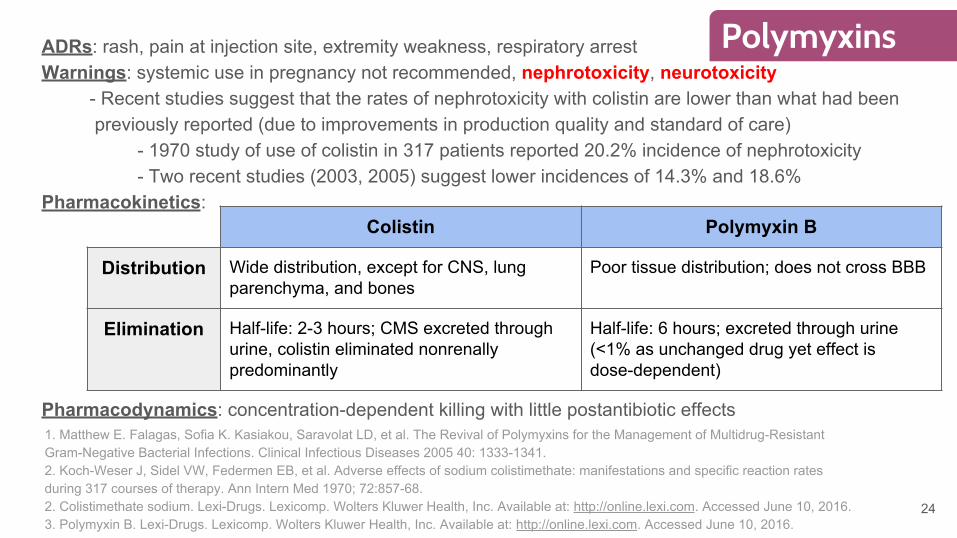
ADRs: rash, pain at injection site, extremity weakness, respiratory arrestWarnings: systemic use in pregnancy not recommended, nephrotoxicity, neurotoxicity
- Recent studies suggest that the rates of nephrotoxicity with colistin are lower than what had been previously reported (due to improvements in production quality and standard of care)
- 1970 study of use of colistin in 317 patients reported 20.2% incidence of nephrotoxicity- Two recent studies (2003, 2005) suggest lower incidences of 14.3% and 18.6%
Pharmacokinetics:
Pharmacodynamics: concentration-dependent killing with little postantibiotic effects
Colistin Polymyxin B
Distribution Wide distribution, except for CNS, lung parenchyma, and bones
Poor tissue distribution; does not cross BBB
Elimination Half-life: 2-3 hours; CMS excreted through urine, colistin eliminated nonrenally predominantly
Half-life: 6 hours; excreted through urine (<1% as unchanged drug yet effect is dose-dependent)
24
Polymyxins
1. Matthew E. Falagas, Sofia K. Kasiakou, Saravolat LD, et al. The Revival of Polymyxins for the Management of Multidrug-Resistant Gram-Negative Bacterial Infections. Clinical Infectious Diseases 2005 40: 1333-1341.2. Koch-Weser J, Sidel VW, Federmen EB, et al. Adverse effects of sodium colistimethate: manifestations and specific reaction rates during 317 courses of therapy. Ann Intern Med 1970; 72:857-68.2. Colistimethate sodium. Lexi-Drugs. Lexicomp. Wolters Kluwer Health, Inc. Available at: http://online.lexi.com. Accessed June 10, 2016.3. Polymyxin B. Lexi-Drugs. Lexicomp. Wolters Kluwer Health, Inc. Available at: http://online.lexi.com. Accessed June 10, 2016.
- Colistin has been more widely used in practice due to a perceived safety benefit from outdated studies- 2014 analysis evaluating 76 patients have suggested that the incidence of nephrotoxicity is higher with colistin than with polymyxin B (55.3% vs. 21.1%; P = 0.004)
- In renally-competent patients, the conversion of CMS to colistin is low (20-25% of dose is converted to active drug) while polymyxin B is minimally excreted in the urine as unchanged drug
- Greater inter-individual variability for colistin pharmacokinetics; problematic due to concentration-dependent effect- CMS is extensively treated into the urine where it can be partially converted to colistin
- Possible benefit in UTIs- Plasma concentrations of active colistin rise slowly (even with a loading dose) due to rate of conversion, yet compensation through dose increase is limited by nephrotoxicity
- Polymyxin B achieves rapid plasma concentrations
Colistin vs. Polymyxin B
25
Polymyxins
1. Phe K, Lee Y, McDaneld PM. In vitro assessment and multicenter cohort study of comparative nephrotoxicity rates associated with colistimethate versus polymyxin B therapy. Antimicrob Agents Chemother. 2014; 58:2740-2746.2. Garonzik SM, Li J, Thamlikitkul V, et al. Population pharmacokinetics of colistin methanesulfonate and formed colistin in critically ill patients from a multicenter study provide dosing suggestions for various categories of patients. Antimicrob Agents Chemother 2011; 55(7): 3284‐94.3. Couet W, Gregoire N, Gobin P, et al. Pharmacokinetics of colistin and colistimethate sodium after a single 80‐mg intravenous dose of CMS in young healthy volunteers. Clin Pharmacol Ther 2011; 89(6): 875‐9.4. Zavascki AP, Goldani LZ, Cao GY, et al. Pharmacokinetics of intravenous polymyxin B in critically‐ill patients. Clin Infect Dis 2008; 47(10): 1298‐304
26
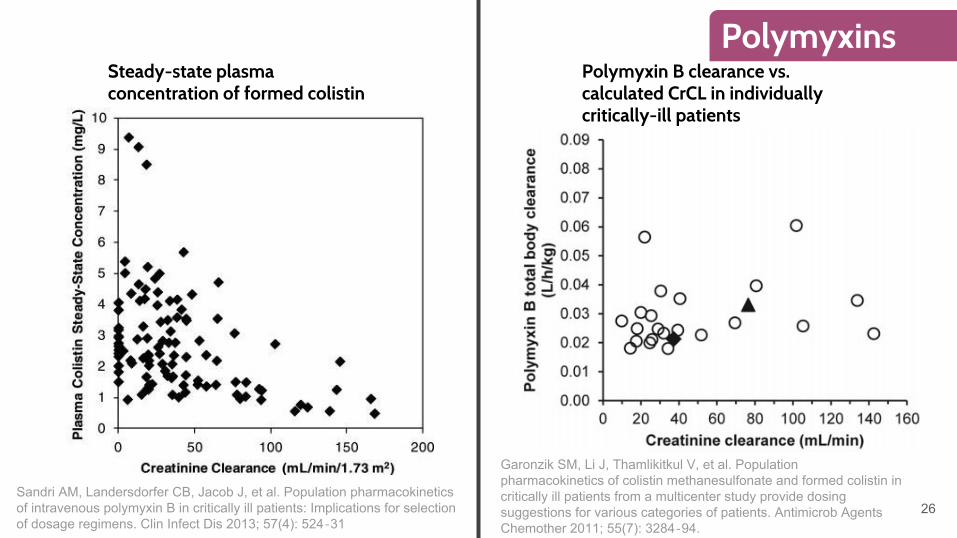
PolymyxinsSteady-state plasma concentration of formed colistin
Polymyxin B clearance vs. calculated CrCL in individually critically-ill patients
Sandri AM, Landersdorfer CB, Jacob J, et al. Population pharmacokinetics of intravenous polymyxin B in critically ill patients: Implications for selection of dosage regimens. Clin Infect Dis 2013; 57(4): 524‐31
Garonzik SM, Li J, Thamlikitkul V, et al. Population pharmacokinetics of colistin methanesulfonate and formed colistin in critically ill patients from a multicenter study provide dosing suggestions for various categories of patients. Antimicrob Agents Chemother 2011; 55(7): 3284‐94.
Monotherapy vs. Combination Therapy
27
Polymyxins
Pournaras S, Vrioni G, Neou E, et al. Activity of tigecycline alone and in combination with colistin and meropenem against Klebsiella pneumoniae carbapenemase (KPC)-producing enterobacteriaceae strains by time-kill assay. Int. J. Antimicrob. Agents 2014: 37;244-247.
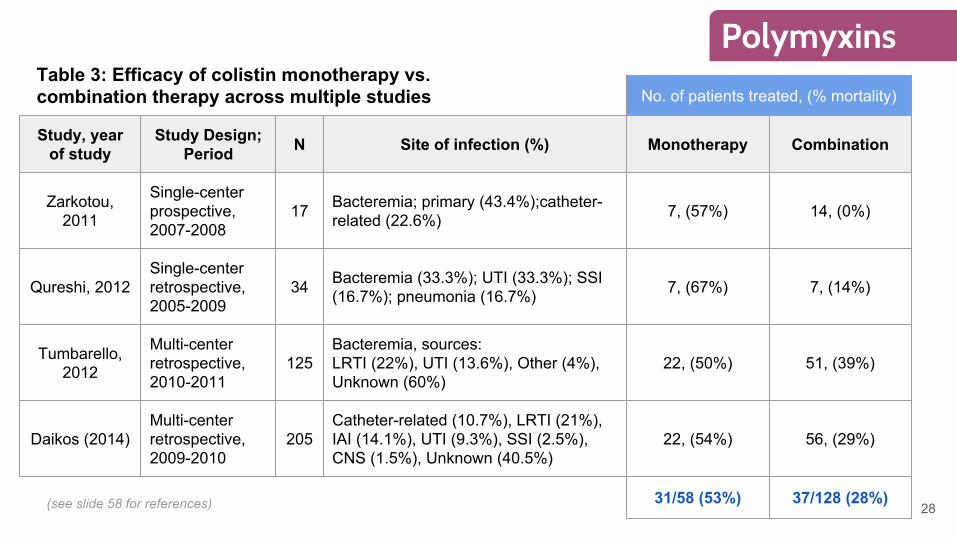
No. of patients treated, (% mortality)
Study, year of study
Study Design; Period N Site of infection (%) Monotherapy Combination
Zarkotou, 2011
Single-center prospective, 2007-2008
17 Bacteremia; primary (43.4%);catheter-related (22.6%) 7, (57%) 14, (0%)
Qureshi, 2012Single-center retrospective, 2005-2009
34 Bacteremia (33.3%); UTI (33.3%); SSI (16.7%); pneumonia (16.7%) 7, (67%) 7, (14%)
Tumbarello, 2012
Multi-center retrospective, 2010-2011
125Bacteremia, sources:LRTI (22%), UTI (13.6%), Other (4%), Unknown (60%)
22, (50%) 51, (39%)
Daikos (2014)Multi-center retrospective, 2009-2010
205Catheter-related (10.7%), LRTI (21%), IAI (14.1%), UTI (9.3%), SSI (2.5%), CNS (1.5%), Unknown (40.5%)
22, (54%) 56, (29%)
31/58 (53%) 37/128 (28%)
Table 3: Efficacy of colistin monotherapy vs. combination therapy across multiple studies
28
Polymyxins
(see slide 58 for references)
Conclusions- Polymyxins (Colistin, polymyxin B) have recently been revived in an effort to combat the increasing incidence of multidrug resistant organisms
- Polymyxins provide a beneficial bactericidal effect that is limited by an insignificant postantibiotic effect
- The use of polymyxins is limited by their substantial nephrotoxic and neurotoxic effects
- On-treatment resistance development is a concern especially for polymyxin monotherapy and so, polymyxins may serve the most efficacy as part of combination therapy
- Further studies are required to determine appropriate dosing in critically-ill patients as well as to determine any significant advantages / disadvantages between both agents
29
Polymyxins
1. Lee J, Patel G, Huprikar S, et al. Decreased susceptibility to polymyxin B during treatment for carbapenem-resistant Klebsiella pneumoniae infection. J Clin Microbiol 2009; 47:1611–2. 2. Tzouvelekis LS, Markogiannakis A, Piperaki E, et al. Treating infections caused by carbapenemase-producing Enterobacteriaceae. Clin Micro- biol Infect 2014; 20:862–72.
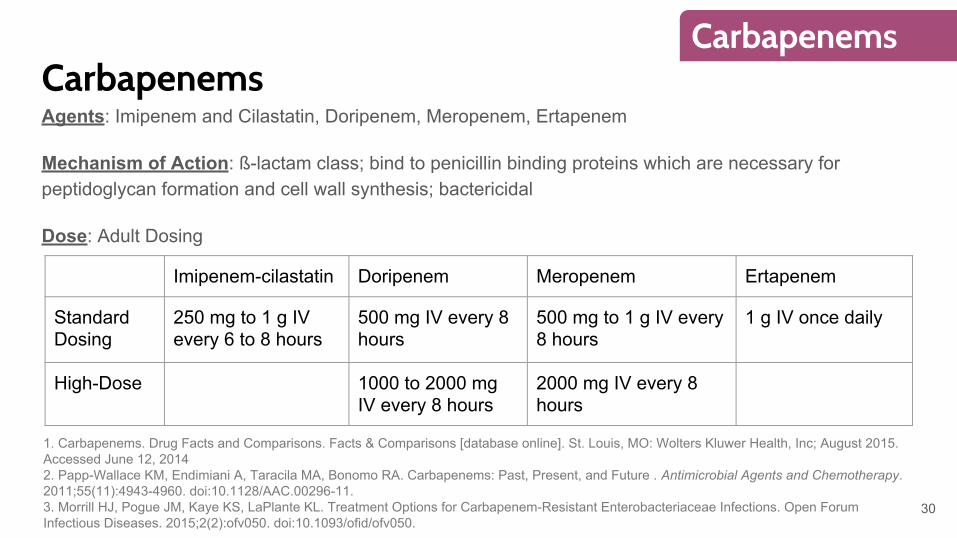
CarbapenemsAgents: Imipenem and Cilastatin, Doripenem, Meropenem, Ertapenem
Mechanism of Action: ß-lactam class; bind to penicillin binding proteins which are necessary for peptidoglycan formation and cell wall synthesis; bactericidal
Dose: Adult Dosing
Imipenem-cilastatin Doripenem Meropenem Ertapenem
Standard Dosing
250 mg to 1 g IV every 6 to 8 hours
500 mg IV every 8 hours
500 mg to 1 g IV every 8 hours
1 g IV once daily
High-Dose 1000 to 2000 mg IV every 8 hours
2000 mg IV every 8 hours
30
Carbapenems
1. Carbapenems. Drug Facts and Comparisons. Facts & Comparisons [database online]. St. Louis, MO: Wolters Kluwer Health, Inc; August 2015. Accessed June 12, 20142. Papp-Wallace KM, Endimiani A, Taracila MA, Bonomo RA. Carbapenems: Past, Present, and Future . Antimicrobial Agents and Chemotherapy. 2011;55(11):4943-4960. doi:10.1128/AAC.00296-11.3. Morrill HJ, Pogue JM, Kaye KS, LaPlante KL. Treatment Options for Carbapenem-Resistant Enterobacteriaceae Infections. Open Forum Infectious Diseases. 2015;2(2):ofv050. doi:10.1093/ofid/ofv050.
Carbapenems
31
Carbapenems
Adverse Effects/Monitoring: headache, abdominal pain, nausea, diarrhea, seizures/CNS reactions, hypersensitivity reactions, Clostridium difficile-associated diarrhea
Pharmacokinetics:
- The carbapenems distribute widely throughout the body into most tissues- Doripenem and ertapenem undergo non-CYP-mediated hydrolysis. Meropenem undergoes hepatic
metabolism. Imipenem metabolism by dehydropeptidase 1 is inhibited by cilastatin.- Carbapenems are mainly renally excreted
Pharmacodynamics: Time dependent, bactericidal
1. Carbapenems. Drug Facts and Comparisons. Facts & Comparisons [database online]. St. Louis, MO: Wolters Kluwer Health, Inc; August 2015. Accessed June 12, 2014
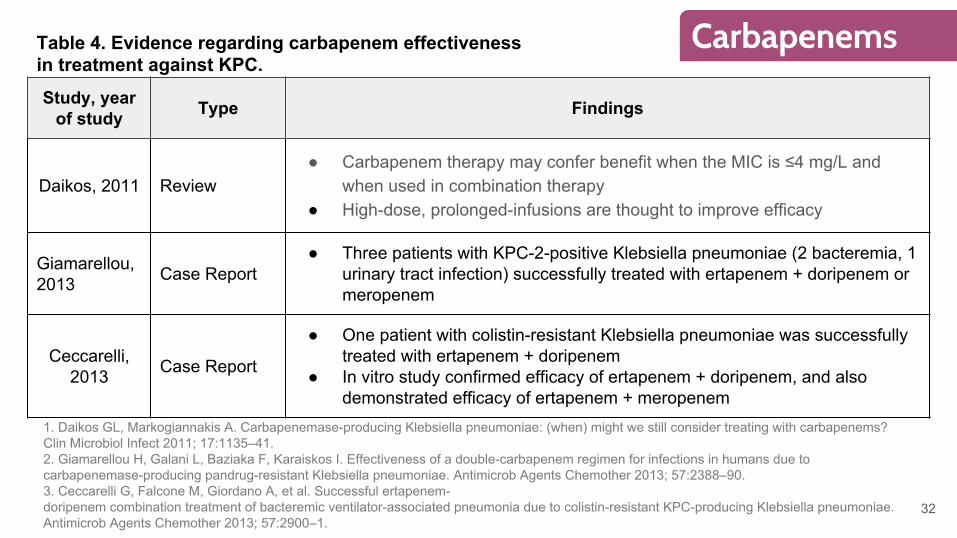
Study, year of study Type Findings
Daikos, 2011 Review● Carbapenem therapy may confer benefit when the MIC is ≤4 mg/L and
when used in combination therapy● High-dose, prolonged-infusions are thought to improve efficacy
Giamarellou, 2013 Case Report
● Three patients with KPC-2-positive Klebsiella pneumoniae (2 bacteremia, 1 urinary tract infection) successfully treated with ertapenem + doripenem or meropenem
Ceccarelli, 2013 Case Report
● One patient with colistin-resistant Klebsiella pneumoniae was successfully treated with ertapenem + doripenem
● In vitro study confirmed efficacy of ertapenem + doripenem, and also demonstrated efficacy of ertapenem + meropenem
32
CarbapenemsTable 4. Evidence regarding carbapenem effectiveness in treatment against KPC.
1. Daikos GL, Markogiannakis A. Carbapenemase-producing Klebsiella pneumoniae: (when) might we still consider treating with carbapenems? Clin Microbiol Infect 2011; 17:1135–41.2. Giamarellou H, Galani L, Baziaka F, Karaiskos I. Effectiveness of a double-carbapenem regimen for infections in humans due to carbapenemase-producing pandrug-resistant Klebsiella pneumoniae. Antimicrob Agents Chemother 2013; 57:2388–90.3. Ceccarelli G, Falcone M, Giordano A, et al. Successful ertapenem-doripenem combination treatment of bacteremic ventilator-associated pneumonia due to colistin-resistant KPC-producing Klebsiella pneumoniae. Antimicrob Agents Chemother 2013; 57:2900–1.
No. of patients treated, (% mortality)
Study, year of study
Study Design; Period N Site of infection (%) Monotherapy Combination
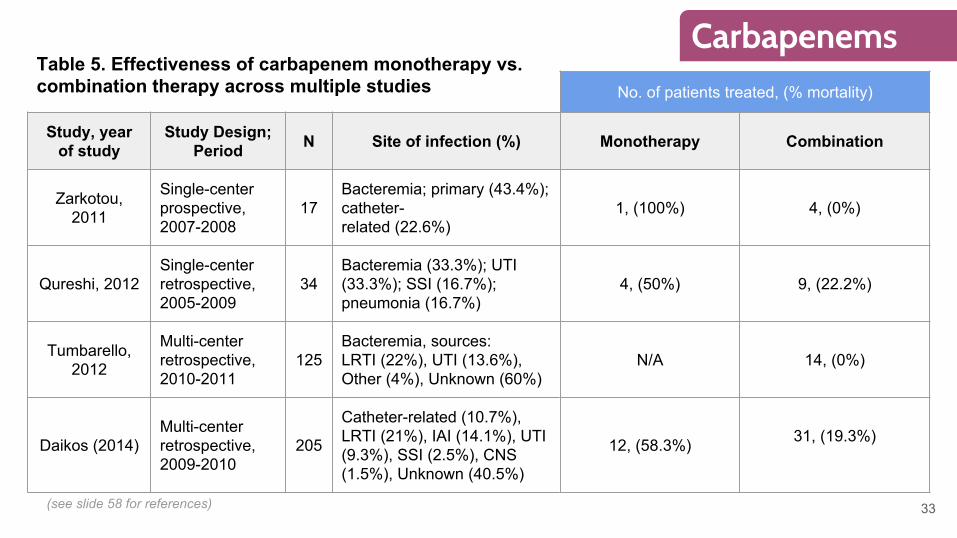
Zarkotou, 2011
Single-center prospective, 2007-2008
17Bacteremia; primary (43.4%); catheter-related (22.6%)
1, (100%) 4, (0%)
Qureshi, 2012Single-center retrospective, 2005-2009
34Bacteremia (33.3%); UTI (33.3%); SSI (16.7%); pneumonia (16.7%)
4, (50%) 9, (22.2%)
Tumbarello, 2012
Multi-center retrospective, 2010-2011
125Bacteremia, sources:LRTI (22%), UTI (13.6%), Other (4%), Unknown (60%)
N/A 14, (0%)
Daikos (2014)Multi-center retrospective, 2009-2010
205
Catheter-related (10.7%), LRTI (21%), IAI (14.1%), UTI (9.3%), SSI (2.5%), CNS (1.5%), Unknown (40.5%)
12, (58.3%) 31, (19.3%)
33
CarbapenemsTable 5. Effectiveness of carbapenem monotherapy vs. combination therapy across multiple studies
(see slide 58 for references)
Dual Carbapenem Therapy● Limited options have led to attempts of dual carbapenem combinations● Carbapenemase is thought to have a higher affinity for ertapenem
○ Ertapenem hypothesized to function as a suicide substrate
● Bulik et al. showed enhanced activity of ertapenem + doripenem against KPC in the in vitro chemostat model and in vivo murine thigh infection model
● Several case reports show success ○ Giamarellou et al. reported success in treating 3/3 patients with KPC positive Klebsiella pneumoniae
using high dose meropenem or high dose ertapenem combined with ertapenem○ Ceccarelli et al. reported success in treating 1/1 patient with KPC positive Klebsiella pneumoniae
ventilator associated pneumonia that did not respond to colistin combination therapy previously● Although further investigation is needed, dual carbapenem therapy may be
useful for treating multidrug resistant or pandrug-resistant infections
34
1. Bulik CC, Nicolau DP. Double-carbapenem therapy for carbapenemase-producing Klebsiella pneumoniae. Antimicrob Agents Chemother 2011; 55:3002–4.2. Giamarellou H, Galani L, Baziaka F, Karaiskos I. Effectiveness of a double-carbapenem regimen for infections in humans due to carbapenemase-producing pandrug-resistant Klebsiella pneumoniae. Antimicrob Agents Chemother 2013; 57:2388–90.3. Ceccarelli G, Falcone M, Giordano A, et al. Successful ertapenem-doripenem combination treatment of bacteremic ventilator-associated pneumonia due to colistin-resistant KPC-producing Klebsiella pneumoniae. Antimicrob Agents Chemother 2013; 57:2900–1.
Carbapenems
Conclusions
● Carbapenems should be used in combination with other agents to treat CRE
● Choice of carbapenem should be driven by susceptibility testing● Consider using high-dose prolonged infusions● In the event of a pandrug-resistant organism, consider dual
carbapenem coverage with ertapenem + meropenem or ertapenem + doripenem
● Carbapenem-containing combination therapies have been associated with lower mortality than combination therapies without carbapenems
351. Morrill HJ, Pogue JM, Kaye KS, LaPlante KL. Treatment Options for Carbapenem-Resistant Enterobacteriaceae Infections. Open Forum Infectious Diseases. 2015;2(2):ofv050. doi:10.1093/ofid/ofv050.
Carbapenems
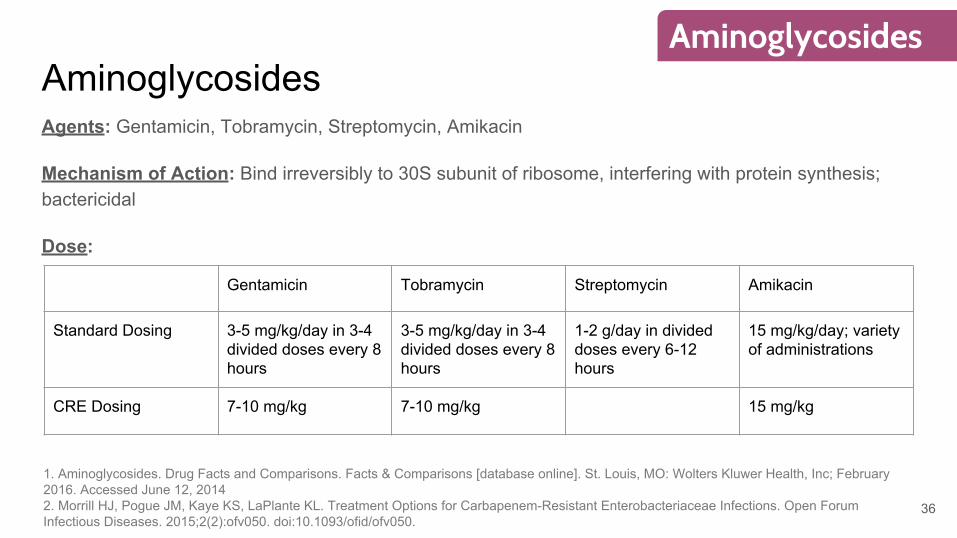
AminoglycosidesAgents: Gentamicin, Tobramycin, Streptomycin, Amikacin
Mechanism of Action: Bind irreversibly to 30S subunit of ribosome, interfering with protein synthesis; bactericidal
Dose:
Gentamicin Tobramycin Streptomycin Amikacin
Standard Dosing 3-5 mg/kg/day in 3-4 divided doses every 8 hours
3-5 mg/kg/day in 3-4 divided doses every 8 hours
1-2 g/day in divided doses every 6-12 hours
15 mg/kg/day; variety of administrations
CRE Dosing 7-10 mg/kg 7-10 mg/kg 15 mg/kg
36
Aminoglycosides
1. Aminoglycosides. Drug Facts and Comparisons. Facts & Comparisons [database online]. St. Louis, MO: Wolters Kluwer Health, Inc; February 2016. Accessed June 12, 20142. Morrill HJ, Pogue JM, Kaye KS, LaPlante KL. Treatment Options for Carbapenem-Resistant Enterobacteriaceae Infections. Open Forum Infectious Diseases. 2015;2(2):ofv050. doi:10.1093/ofid/ofv050.
AminoglycosidesAdverse Effects/Monitoring: hearing loss/deafness, headache, confusion, fever, nausea, vomiting, diarrhea, eosinophilia, thrombocytopenia, leukopenia, rash, increased creatinine, apnea
BBW: nephrotoxicity, irreversible ototoxicity, and neurotoxicity are all associated with aminoglycosides. Avoid in pregnancy.
Pharmacokinetics:
- Widely distributed, but do not have good CSF penetration- Primarily renally excreted
Pharmacodynamics: Concentration dependent, bactericidal
37
Aminoglycosides
1. Aminoglycosides. Drug Facts and Comparisons. Facts & Comparisons [database online]. St. Louis, MO: Wolters Kluwer Health, Inc; February 2016. Accessed June 12, 20142. Morrill HJ, Pogue JM, Kaye KS, LaPlante KL. Treatment Options for Carbapenem-Resistant Enterobacteriaceae Infections. Open Forum Infectious Diseases. 2015;2(2):ofv050. doi:10.1093/ofid/ofv050.
38
Aminoglycosides
1. Benenson S, Navon-Venezia S, Carmeli Y, et al. Carbapenem-resistant Klebsiella pneumoniae endocarditis in a young adult. Successful treatment with gentamicin and colistin. Int J Infect Dis 2009; 13:e295–8.2. Lee GC, Burgess DS. Treatment of Klebsiella pneumoniae carbapenemase (KPC) infections: a review of published case series and case reports. Ann Clin Microbiol Antimicrob 2012; 11:32.
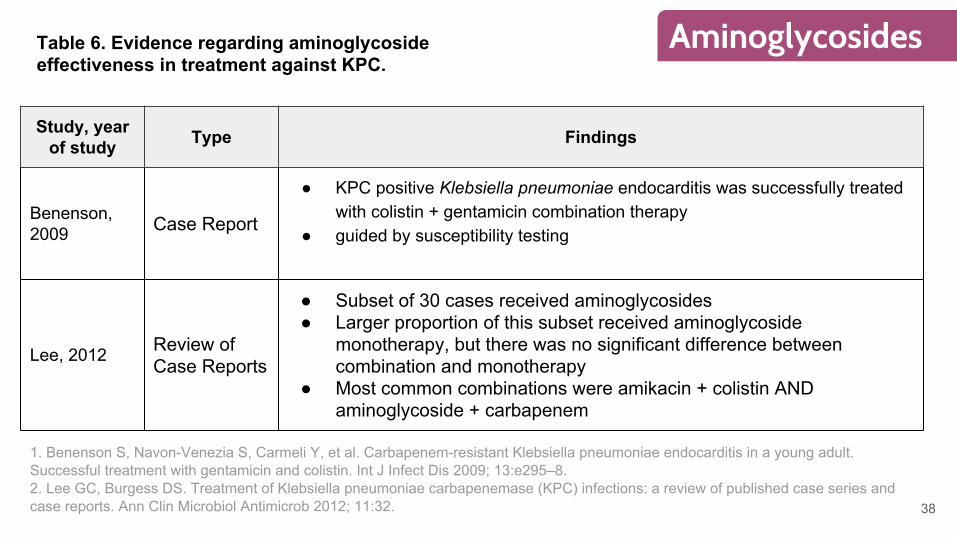
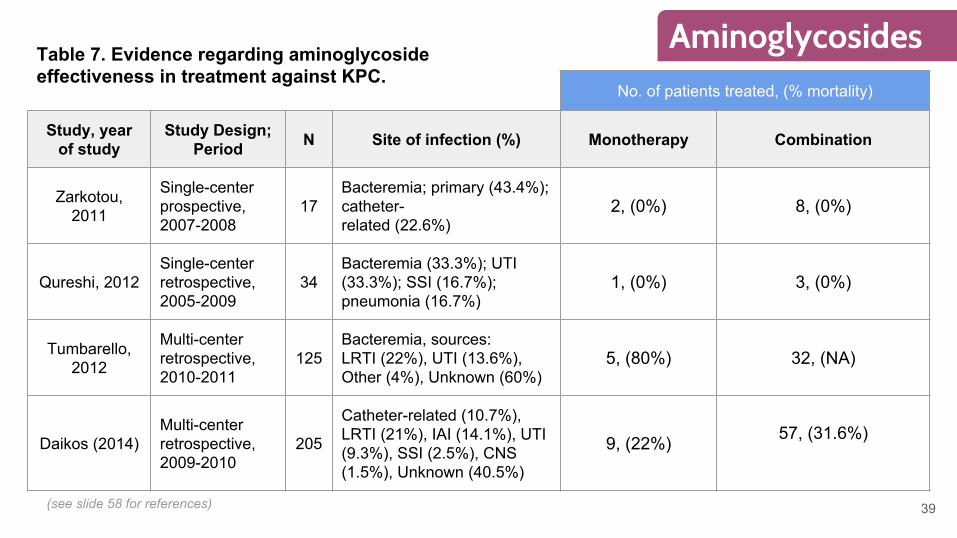
Study, year of study Type Findings
Benenson, 2009 Case Report
● KPC positive Klebsiella pneumoniae endocarditis was successfully treated with colistin + gentamicin combination therapy
● guided by susceptibility testing
Lee, 2012 Review of Case Reports
● Subset of 30 cases received aminoglycosides● Larger proportion of this subset received aminoglycoside
monotherapy, but there was no significant difference between combination and monotherapy
● Most common combinations were amikacin + colistin AND aminoglycoside + carbapenem
Table 6. Evidence regarding aminoglycoside effectiveness in treatment against KPC.
No. of patients treated, (% mortality)
Study, year of study
Study Design; Period N Site of infection (%) Monotherapy Combination
Zarkotou, 2011
Single-center prospective, 2007-2008
17Bacteremia; primary (43.4%); catheter-related (22.6%)
2, (0%) 8, (0%)
Qureshi, 2012Single-center retrospective, 2005-2009
34Bacteremia (33.3%); UTI (33.3%); SSI (16.7%); pneumonia (16.7%)
1, (0%) 3, (0%)
Tumbarello, 2012
Multi-center retrospective, 2010-2011
125Bacteremia, sources:LRTI (22%), UTI (13.6%), Other (4%), Unknown (60%)
5, (80%) 32, (NA)
Daikos (2014)Multi-center retrospective, 2009-2010
205
Catheter-related (10.7%), LRTI (21%), IAI (14.1%), UTI (9.3%), SSI (2.5%), CNS (1.5%), Unknown (40.5%)
9, (22%) 57, (31.6%)
39
AminoglycosidesTable 7. Evidence regarding aminoglycoside effectiveness in treatment against KPC.
(see slide 58 for references)
Conclusions
● Mostly considered as an adjuvant for treatment combinations● Choice of aminoglycoside should be driven by susceptibility testing● Consider high-dose therapy● May be a good choice for urinary tract infections● Consider nephrotoxicity and ototoxicity
40
Aminoglycosides
1. Morrill HJ, Pogue JM, Kaye KS, LaPlante KL. Treatment Options for Carbapenem-Resistant Enterobacteriaceae Infections. Open Forum Infectious Diseases. 2015;2(2):ofv050. doi:10.1093/ofid/ofv050.
FosfomycinAgents: Fosfomycin Tromethamine
MOA: Inhibits the enolpyruvyl transferase enzyme which is necessary for cell wall synthesis
Dose: 3 grams as a single dose, or every 2-3 days for 3 doses (depending on indication)
Adverse Effects/Monitoring: nausea, diarrhea, headache, vaginitis, dizziness, rash
Pharmacokinetics:
- Excreted in urine and feces
Pharmacodynamics: bactericidal
41
Fosfomycin
Facts and Comparisons.
Fosfomycin Evidence● Two case reports indicate fosfomycin was effective in treating KPC-positive
Klebsiella pneumoniae urinary tract infections● A small prospective study treated carbapenem-resistant Klebsiella
pneumoniae with IV fosfomycin (2-4 g every 6 hours) in combination with piperacillin/tazobactam, gentamicin, and colistin. Overall mortality was 18.2%.
● Karageorgopoulos et al. report 3 cases where IV fosfomycin was administered in combination therapy to treat KPC-positive Klebsiella pneumoniae bacteraemia. Despite initial improvements, treatment was not successful in all 3 cases.
42
Fosfomycin
1. Kitchel B, Sundin DR, Patel JB. Regional dissemination of KPC-producing Klebsiella pneumoniae. Antimicrob Agents Chemother2009; 53:4511–3.2. Michalopoulos A, Virtzili S, Rafailidis P, et al. Intravenous fosfomycinfor the treatment of nosocomial infections caused by carbapenem-resistant Klebsiella pneumoniae in critically ill patients: a prospective evaluation. Clin Microbiol Infect 2010; 16:184–6.3. Karageorgopoulos DE, Miriagou V, Tzouvelekis LS, et al. Emergence of resistance to fosfomycin used as adjunct therapy in KPC Klebsiella pneumoniae bacteraemia: report of three cases. J Antimicrob Chemo-ther 2012; 67:2777–9.
Conclusions
● Evidence is very limited● May be a good choice for urinary tract infection● IV fosfomycin is not available in the United States
431. Morrill HJ, Pogue JM, Kaye KS, LaPlante KL. Treatment Options for Carbapenem-Resistant Enterobacteriaceae Infections. Open Forum Infectious Diseases. 2015;2(2):ofv050. doi:10.1093/ofid/ofv050.
Fosfomycin
1. Identify source of infection 2. Select empiric therapy based on source of infection and distribution properties of specific
agents- Combination therapy is generally preferred over monotherapy due to synergy of
mechanisms and suppression of resistance- In a comprehensive review which included data on 889 patients, combination
therapy was associated with lower mortality (27% (121/441)) than monotherapy (38.7% (134/346))
3. Consider adjunctive therapy depending on severity of infection4. Ideally, adjust following susceptibility testing, keeping in mind that MICs for KPC are
controversial and for some agents, unconfirmed by the FDA or CLSI
44
General Approach to Antimicrobial Selection
Tzouvelekis LS, Markogiannakis A, Piperaki E, et al. Treating infections caused by carbapenemase-producing Enterobacteriaceae. Clin Microbiol Infect 2014; 20:862-72.
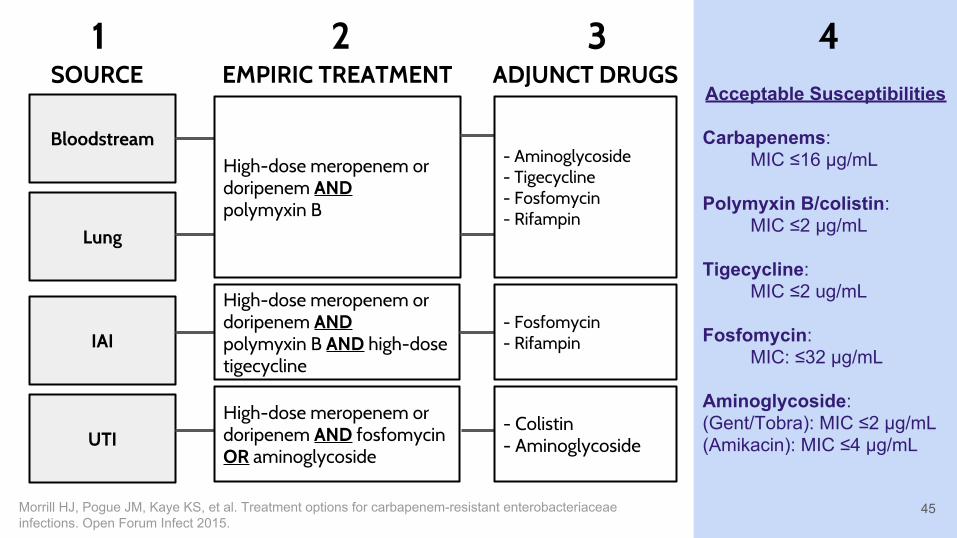
Bloodstream
Lung
IAI
UTI
SOURCE
High-dose meropenem or doripenem AND polymyxin B
High-dose meropenem or doripenem AND polymyxin B AND high-dose tigecycline
High-dose meropenem or doripenem AND fosfomycin OR aminoglycoside
EMPIRIC TREATMENT
- Aminoglycoside- Tigecycline- Fosfomycin- Rifampin
- Fosfomycin- Rifampin
- Colistin- Aminoglycoside
Acceptable Susceptibilities
Carbapenems:MIC ≤16 µg/mL
Polymyxin B/colistin:MIC ≤2 µg/mL
Tigecycline:MIC ≤2 ug/mL
Fosfomycin:MIC: ≤32 µg/mL
Aminoglycoside:(Gent/Tobra): MIC ≤2 µg/mL(Amikacin): MIC ≤4 µg/mL
ADJUNCT DRUGS
45Morrill HJ, Pogue JM, Kaye KS, et al. Treatment options for carbapenem-resistant enterobacteriaceae infections. Open Forum Infect 2015.
1 2 3 4

Future of Treatment
46
Ceftazidime-avibactam
Eravacycline
Meropenem-vaborbactam
Plazomicin
Prevention
47
- Focus efforts on identifying CRE infections- Review microbiology records for 6-12 months to look for unrecognized
cases- If unrecognized case found, perform surveillance cultures in high-risk
areas- Identified cases should be placed on contact precautions- Limit invasive devices- Prevention strategies may have utility in settings beyond acute care
Gupta N, Limbago BM, Patel JB, Kallen AJ (2011). Carbapenem resistant Enterobacteriaceae: epidemiology and prevention. Clin. Infect. Dis 53:60-67.
Ceftazidime-Avibactam (Avycaz®)- Approved in February 2015 for the treatment of complicated IAIs and complicated UTIs in patients with limited or no alternative treatment options
- Combination of broad-spectrum cephalosporin (ceftazidime) with a novel ß-lactamase inhibitor found to have activity against KPC
- RECLAIM-1 & RECLAIM-2: phase 3, randomized, multi-center, double-blind, double-dummy, parallel-group, comparative studies conducted to determine efficacy, safety, and tolerability of Avycaz® plus metronidazole compared to meropenem
- Combination found to be non-inferior- Most common ADRs: nausea, vomiting, constipation, anxiety
- AWP (per vial): $3 42
48
Newly-Approved Drug
1. Avycaz [package insert]. Actavis Inc; 2015.2. Aktas Z, Kayacan C, Oncul O. In vitro activity of avibactam (NXL104) in combination with beta-lactams against Gram-negative bacteria, including OXA-48 beta-lactamase-producing Klebsiella pneumoniae. Int J Antimicrob Agents 2012; 39:86–9.
Eravacycline- Investigational synthetic fluorocycline antibiotic; structurally similar to tigecycline with two modifications to the D-ring of the tetracycline core that replaces the glycylamido group at C-9
- Demonstrates broad spectrum coverage against gram-positive, gram-negative, and anaerobic bacteria with the exception of Pseudomonas aeruginosa
- Two- to eightfold more potent than tigecycline vs. gram (-) pathogens in in vivo studies
- Phase 3 studies: Investigating Gram-Negative Infections Treated with Eravacycline (IGNITE)- Investigating safety and efficacy compared to ertapenem in complicated IAI and complicated cUT- Results produced so far have been showing favorable potential over ertapenem
- Common adverse effects: nausea, vomiting
49
Pipeline Drug
Zhanel GG, Cheung D, Adam H, et al. Review of eravacycline, a novel fluorocycline antibacterial agent. Drugs. 2016; 76:567-588.
Meropenem-Vaborbactam (Carbovance®)- Granted fast track status in April 2016; currently undergoing phase 3 study
- Combination of meropenem with vaborbactam, a novel boron-based ß-lactamase inhibitor that has so far shown considerable efficacy against CRE
- Study: Efficacy, safety, tolerability of carbavance compared to best available therapy in serious infections due to carbapenem resistant enterobacteriaceae, in adults
- Phase 3 multi-center, randomized, open-label study (N = 150)- Primary outcome: overall success (clinical cure & microbiological eradication, differs based on source of infection)- Secondary outcome: all-cause mortality, relapse/recurrence rates of baseline infection, etc.- “Best available therapy”: aminoglycosides, polymyxin B, colistin, tigecycline, & various combinations- Expected completion date: December 2016
50
Pipeline Drug
Rempex Pharmaceuticals. Efficacy, Safety, Tolerability of Carbavance Compared to Best Available Therapy in Serious Infections Due to Carbapenem Resistant Enterobacteriaceae, in Adults. Available from: https://clinicaltrials.gov/ct2/show/NCT02168946. NLM identifier: NCT02168946. Accessed June 10, 2016.
Table 2, 3, 5, 7 References1. Zarkotou O, Pournaras S, Tselioti P, et al. Predictors of mortality in patients with bloodstream infections caused by KPC-producing Klebsiella pneumoniae and impact of appropriate antimicrobial treatment. Clin Microbiol Infect 2011; 17:1798–803.
2. Qureshi ZA, Paterson DL, Potoski BA, et al. Treatment outcome of bacteremia due to KPC-producing Klebsiella pneumoniae: superiority of combination antimicrobial regimens. Antimicrob Agents Chemother 2012; 56:2108–13.
3. Daikos GL, Tsaousi S, Tzouvelekis LS, et al. Carbapenemase-producing Klebsiella pneumoniae bloodstream infections: lowering mortality by antibiotic combination schemes and the role of carbapenems. Antimicrob Agents Chemother 2014; 58:2322-8.
4. Tumbarello M, Viale P, Viscoli C, et al. Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase- producing K. pneumoniae: importance of combination therapy. Clin Infect Dis 2012; 55:943–50.
51
Plazomicin- Novel aminoglycoside antibiotic designed to treat serious gram-negative infections, including CRE
- Demonstrated potent in vitro and in vivo efficacy in nonclinical studies against CRE
- Granted fast track status in January 2015; currently undergoing two Phase 3 studies (EPIC; CARE)
- Phase 3 study: A study of plazocin compared with colistin in patients with infection due to carbapenem-resistant enterobacteriaceae (CRE)” (CARE)
- Phase 3 randomized, open-label superiority cohort study comparing efficacy and safety of plazomicin vs. colistin when combined with a second antibiotic (meropenem or tigecycline) in the treatment of various infections due to CRE (N = 480)- Primary outcome: all-cause mortality at day 28 or significant disease-related complications- Secondary outcomes: plazomicin PK parameters, adverse effects, etc.- Expected completion date: February 2018
52
Pipeline Drug
Achaogen. A Study of Plazomicin Compared With Colistin in Patients With Infection Due to Carbapenem-Resistant Enterobacteriaceae (CRE) (CARE). Available from: https://clinicaltrials.gov/ct2/show/NCT01970371. NLM identifier: NCT01970371. Accessed June 10, 2016.

53
Questions?