Embed Size (px)
Citation preview

Copper Deficiency in Patients with Cystinosis with Cysteamine Toxicity
Martine T. P. Besouw, MD, PhD1,2, Jerry Schneider, MD, PhD3, Mirian C. Janssen, MD, PhD4, Marcella Greco, MD5,
Francesco Emma, MD5, Elisabeth A. Cornelissen, MD, PhD6, Koen Desmet, PharmD7, Flemming Skovby, MD, PhD8,
Francois Nobili, MD9, Marc R. Lilien, MD, PhD10, Anne De Paepe, MD, PhD11, Fransiska Malfait, MD, PhD11,
Sofie Symoens, PhD11, Lambertus P. van den Heuvel, PhD2,6, and Elena N. Levtchenko, MD, PhD1,2
Objectives To assess whether copper deficiency plays a role in the recently described cysteamine toxicity inpatients with cystinosis, and to examine whether polymorphisms in copper transporters, lysyl oxidase, and/ortype I procollagen genes could be responsible for the occurrence of cysteamine toxicity in a small subset of patientswith cystinosis.Study design Thirty-six patients with cystinosis were included: 22 with Fanconi syndrome (including 7 withcysteamine toxicity), 12 after renal transplantation, 1 receiving hemodialysis, and 1 with ocular cystinosis. Serumcopper and ceruloplasmin levels and urinary copper/creatinine ratio were measured. Genes ATP7A and CTR1 (en-coding copper transporters), LOX (encoding lysyl oxidase), andCOL1A1 andCOL1A2 (encoding type I procollagen)were analyzed in patients with (n = 6) andwithout (n = 5) toxicity. Fibroblast (pro)collagen synthesis was compared inpatients with (n = 3) and those without (n = 2) cysteamine toxicity.Results All 22 patients with Fanconi syndrome had increased urinary copper excretion. Serum copper and ceru-loplasmin levels were decreased in 9 patients, including all 7 patients with cysteamine toxicity. No specificsequence variations were associated with toxicity. All fibroblasts exhibited normal (pro)collagen synthesis.Conclusion Patients with cystinosis with cysteamine toxicity demonstrate copper deficiency. This can causedecreased activity of lysyl oxidase, the enzyme that generates the aldehydes required for collagen cross-linking.Thus, copper supplementation might prevent cysteamine toxicity. (J Pediatr 2013;163:754-60).
Cystinosis is an autosomal recessive disorder marked by intralysosomal cystine accumulation in various tissues. It causesgeneralized proximal tubular dysfunction, termed renal Fanconi syndrome (FS), which usually leads to end-stage renaldisease in the second decade of life.1 The amino thiol cysteamine, currently the only available treatment for cystinosis,
depletes lysosomal cystine and postpones renal and extrarenal organ damage.2-5
Recent reports of bruise-like skin lesions, striae, bone abnormalities, and muscle weakness in patients with cystinosis treatedwith cysteamine has led to concerns regarding the use of high doses (above the recommended maximum of 1.95 g/m2/day),although only one-half of the reported patients received such high doses. Histological analysis of skin biopsy specimens ob-tained from the bruise-like lesions revealed proliferation of microvascular endothelial cells (reactive angioendotheliomatosis)and irregular collagen fiber calibers, resembling those found in classical Ehlers-Danlos syndrome; irregular elastin fibers werefound in some patients. The etiology of these lesions remained unclear; however, the causative role of cysteamine administra-tion was supported by the fact that symptoms ameliorated in all patients after cysteamine doses were decreased. There was noclear dose-dependent effect, however.6
From the 1Department of Pediatric Nephrology, LeuvenUniversity Hospital, 2Laboratory of Pediatrics, CatholicUniversity of Leuven, Leuven, Belgium; 3Department ofPediatrics, University of California at San Diego, La Jolla,CA; 4Department of Internal Medicine, RadboudUniversity Nijmegen Medical Center, Nijmegen, TheNetherlands; 5Division of Nephrology and Dialysis,Department of Nephrology and Urology, Bambino Ges�uChildren’s Hospital, IRCCS, Rome, Italy; 6Department ofPediatric Nephrology, Radboud University NijmegenMedical Center, Nijmegen, The Netherlands; 7Laboratoryof Medicine, Leuven University Hospital, Leuven,Belgium; 8Department of Clinical Genetics, Juliane MarieCenter, Copenhagen University Hospital, Copenhagen,Denmark; 9Department of Pediatric Nephrology,Besancon University Hospital, Besancon, France;10Department of Pediatric Nephrology, WilhelminaChildren’s Hospital, Utrecht, The Netherlands; and11Center for Medical Genetics, Ghent UniversityHospital, Ghent, Belgium
Given the structural similarity between cysteamine and D-penicillamine, wesuggested that cysteamine can interfere with collagen cross-linking.6 Aldehydesrequired for collagen and elastin cross-linking are synthetized in the presenceof copper by an enzyme, lysyl oxidase.7,8 It has been demonstrated that D-peni-cillamine can block aldehydes, making them unavailable for cross-linking.7
Interestingly, the bone problems related to cysteamine toxicity clinically resembleosteolathyrism, which is caused by b-aminopropionitrile–induced inhibition oflysyl oxidase.8 Previous reports of osteolathyrism have described bone pains andskeletal deformities, including lack of ossification centers in the iliac creasts,ischial tuberosities, and vertebrae, as well as bowing with thickening of the fem-oral shaft.9-12 Because copper is a cofactor of lysyl oxidase,13 symptoms of copperdeficiency also overlap with those of osteolathyrism.8
We hypothesized that copper deficiency might have contributed to the adverseeffect of cysteamine on collagen cross-linking in patients with cystinosis. We
J.S. serves as a consultant for Raptor Pharmaceuticals.The other authors declare no conflicts of interest.
0022-3476/$ - see front matter. Copyright ª 2013 Mosby Inc.
All rights reserved. http://dx.doi.org/10.1016/j.jpeds.2013.03.078
FS Fanconi syndrome
754

Vol. 163, No. 3 � September 2013
examined whether polymorphisms in copper transporters,lysyl oxidase, and/or type I procollagen genes could beresponsible for the occurrence of cysteamine toxicity inonly a small subset of patients with cystinosis.
Methods
Physicians treating patients with cystinosis diagnosed withcysteamine toxicity were invited to include their patients inthis study. The physicians collected samples for serum copperand ceruloplasmin measurements and urinary copper excre-tion. These patients were treated in 5 different centers:Radboud University Nijmegen Medical Center (Nijmegen,The Netherlands), Bambino Ges�u Children’s Hospital(Rome, Italy), Copenhagen University Hospital (Copenha-gen, Denmark), Besancon University Hospital (Besancon,France), and Leuven University Hospital (Leuven, Belgium).In 3 centers (The Netherlands, Italy, and Belgium), samplesfrom patients with cystinosis but without cysteamine toxicitywere collected as well; these patients served as a controlgroup. A total of 36 patients with cystinosis were included,7 of whom were diagnosed with cysteamine toxicity. DNAsamples were obtained from 6 of the patients with cysteaminetoxicity; fibroblasts, from 3 of these patients. DNA samplesand fibroblasts from patients with cystinosis without cyste-amine toxicity were obtained from local biobanks in Belgiumand The Netherlands and served as controls.
The study protocol was approved by the Ethical Board ofLeuven University Hospital, the center that coordinated thestudy. Informed consent was obtained from all patients in-cluded in the study. The subjects who provided the biobankspecimens had provided consent for use of their material forscientific research at the time of sample collection. Informedconsent forms were signed either by the patients (if aged$18years) or their parents (if aged <18 years).
Copper and Ceruloplasmin MeasurementsBlood samples for copper and ceruloplasmin measurementwere collected in a vacutainer tube containing clot activatorand gel for serum separation (BD, Erebodegem, Belgium).Serum was collected by allowing blood samples to clot for30 minutes, followed by centrifugation at 1700 � g for 10minutes at 4�C. Midstream urine samples were not centri-fuged. Both serum and urine samples were immediatelyfrozen and shipped to Leuven on dry ice, where they werestored at�80�C until analysis. Copper was measured by elec-trothermal atomic absorption spectrometry (Varian Spec-trAA 220Z; Varian Medical Systems, Diegem, Belgium).Ceruloplasmin was measured by nephelomatic analysis (IM-MAGE 800; Beckman Coulter, Suarl�ee, Belgium).
DNA AnalysisGenomic DNA was extracted from blood or cultured fibro-blasts from 6 patients with cystinosis with cysteamine toxicityand compared with samples from 5 patients with cystinosiswithout cysteamine toxicity. The open reading frames ofATP7A (23 exons), CTR1 (4 coding exons), and LOX (7
coding exons) were investigated by polymerase chainreaction, followed by bidirectional fluorescent DNA sequenc-ing. The primer sequences of ATP7A14 and LOX15 have beendescribed previously; primer sequences of CTR1 are availableon request. Then the open reading frames of COL1A1 (52exons) and COL1A2 (52 exons) were investigated bypolymerase chain reaction, followed by bidirectionalfluorescent DNA sequencing, as described previously.16
(Pro)collagen Synthesis StudiesThese experiments were performed on 3 fibroblast cell linesobtained from patients with cystinosis with cysteaminetoxicity and 2 fibroblast cell lines from patients with cystino-sis without cysteamine toxicity. Cells were cultured in culturemedium supplemented with ascorbic acid, to ameliorate theproduction of type I and type III (pro)collagen. Each cell linewas cultured both with and without the addition of 0.1 mMcysteamine, close to the peak cysteamine plasma levels mea-sured in patients with cystinosis.17 A patient with cystinosiswith cysteamine toxicity was reported to have a similarplasma level.6 Synthesis of (pro)collagens was examined asdescribed previously.18 In brief, fibroblasts were grown toconfluency and then incubated with [14C]proline at 37�Cfor 16 hours. Medium and cell layer fractions were harvestedseparately; both were supplemented with protein inhibitorsand stored at �80�C until analysis. Both medium and celllayer procollagens were converted to the respective collagenmolecules by pepsin digestion, lyophilized, and redissolvedin sample buffers. Analyses of secreted pro-a-collagen chainsand secreted and intracellular a-collagen chains wereperformed by sodium dodecyl sulfate–polyacrylamide gelelectrophoresis. Gels were fixed and processed for fluorogra-phy, dried, and exposed to an X-ray film.
Statistical AnalysesThe Student t test and Pearson correlation were used forstatistical analyses. Values were considered statisticallysignificant at a P value <.05.
Results
Patients’ characteristics are summarized in Table I. Copperand ceruloplasmin data are reported for 36 patients withcystinosis, including 22 patients with renal FS (including 7with signs of cysteamine toxicity), 12 patients whounderwent transplantation with a functional renal graft, 1anuric patient who was treated with hemodialysis afterrenal graft failure, and 1 patient with ocular cystinosiswithout renal involvement. All patients with cysteaminetoxicity exhibited skin abnormalities, including bruise-likelesions and/or red skin striae. In addition, patients 3 and 4had severe musculoskeletal pain, limiting their ability towalk. Patient 3 also suffered from neurologic complicationscausing behavioral changes. Severe bone deformities werereported despite adequate phosphate and vitamin Dsupplementations in 3 of 6 patients with cysteaminetoxicity, including severe genu valgum requiring surgical
755

Table I. Overview of patients with cystinosis included in the copper study
Patient Sex Age, y Renal statusGlomerular filtrationrate, mL/min/1.73 m2*
Cysteaminetoxicity
Daily cysteaminedose, g/m2†
Serum copper,mg/dL
Serumceruloplasmin,
g/LUrinary copper/creatine
ratio, mg/g
1 M 21 FS 41 Yes 1.15 55 0.19 2202 M 14 FS 45 Yes 1.90 55 0.17 1133 M 20 FS 18 Yes 0.97 68 0.22 2274 M 12 FS 57 Yes 1.11 59 0.20 1565 M 20 FS 37 Yes 1.60 74 0.22 2036 M 19 FS 48 Yes 1.60 65 0.19 787 M 12 FS 114 Yes 1.74 46 0.18 1358 M 6 FS 87 No 1.13 88 0.33 739 F 5 FS 71 No 1.26 89 0.36 13710 M 14 FS 65 No 0.96 88 0.37 13911 M 16 FS 41 No 1.41 68 0.27 15012 M 11 FS 108 No 1.19 94 0.34 5813 F 11 FS 15 No 0.80 83 0.31 20714 F 7 FS 86 No 1.29 94 0.34 30915 F 8 FS 94 No 0 112 0.39 6216 M 3 FS 77 No 1.05 125 0.37 14117 M 7 FS 13 No 0.98 126 0.33 16718 F 14 FS 31 No 1.02 71 0.20 13619 F 6 FS 38 No 1.06 81 0.25 19320 M 4 FS 26 No 1.31 104 0.32 25821 M 6 FS 60 No 1.21 92 0.28 22822 F 4 FS 40 No 0.95 162 0.52 31223 F 31 Transplanted 54 No 1.38 81 0.24 2224 F 14 Transplanted 85 No 1.21 76 0.25 4125 F 16 Transplanted 73 No 0.83 119 0.45 5426 M 25 Transplanted 82 No 2.30 84 0.26 3427 M 18 Transplanted 77 No 1.20 83 0.25 7428 M 24 Transplanted 85 No 0.85 91 0.26 1829 M 22 Transplanted >90 No 1.64 99 0.29 1330 F 19 Transplanted 59 No 1.81 107 0.29 2931 F 39 Transplanted 65 No 1.41 106 0.26 3132 F 24 Transplanted 79 No 1.56 145 0.43 5033 M 26 Transplanted 18 No 1.77 80 0.27 6534 M 36 Transplanted 53 No 1.29 64 0.20 2135 M 25 Hemodialysis - No 0.31 80 0.25 -36 F 36 Ocular cystinosis >90 No 0 158 0.47 13
F, female; M, male.Patients 1-7 suffered from cysteamine toxicity.*GFR was calculated by the bedside Schwartz formula in patients aged <18 years and calculated by the modification of diet in renal disease study equation in patients aged $18 years.†Daily cysteamine dose at the moment of this study, not at the time of development of cysteamine toxicity. Patient 15 was included at diagnosis; patient 36 was not treated with systemic cysteamine.Normal levels: serum copper 80-120 mg/dL; serum ceruloplasmin 0.22-0.58 g/L; urinary copper/creatinine ratio <50 mg/g.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 163, No. 3
correction in patients 3 and 5 and pronounced pes planus inpatient 1. In these patients, signs of rickets that were presentat diagnosis disappeared after the onset of therapy and beforethe development of cysteamine toxicity. Moreover, allpatients had normal blood levels of vitamin D, calcium,and phosphate, indicating that the bone deformities inthese patients were not caused by rickets. In patients withcysteamine toxicity, daily cysteamine doses were decreasedat the time of symptom development, which was before theonset of this study, but no other therapeutic changes weremade in these patients.
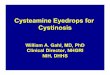
Copper and Ceruloplasmin MeasurementsSerum copper and ceruloplasmin levels, along with urinarycopper/creatinine ratio, are shown in Figure 1 andTable I. All patients with cystinosis and cysteaminetoxicity had serum copper and ceruloplasmin levels belowthe normal range; these levels were significantly lower thanthose in the patients with cystinosis without cysteaminetoxicity (P < .01).
756
All patients with functional native kidneys and FS hadincreased urinary copper excretion. Urinary copper excretionwas slightly increased in 3 of the 12 patients who underwentrenal transplantation (patients 24, 27, and 33; maximum, 74mg/g; normal, <50 mg/g). Patient 33 was the only patient whounderwent a bilateral nephrectomy; all other patients still hadat least 1 native kidney. The slightly increased copper excretionin patient 33 might be attributed to chronic allograft nephrop-athywith pronounced renal interstitial damage. The patient re-ceiving hemodialysis was anuric, but had normal serumcopperand ceruloplasmin levels. The patient with ocular cystinosishadnormal serumcopper and ceruloplasmin levels andnormalurinary copper excretion. There was no difference in urinarycopper/creatinine ratio between the patients with cysteaminetoxicity and those without cysteamine toxicity (P = .17).An inverse correlation was found between glomerular fil-
tration rate and urinary copper excretion (r = �0.46; P <.01). However, when the patients with FS and those who un-derwent transplantation were analyzed separately, the inversecorrelation between glomerular filtration rate and urinary
Besouw et al

Figure 1. Comparison of A, serum copper levels, B, serumceruloplasmin levels, and C, urinary copper/creatinine ratiobetween patients with renal FS and thosewho underwent renaltransplantation. Patients with cysteamine toxicity are indicatedin black, the patient with ocular cystinosis is indicated in lightgray, and the anuric patient on hemodialysis is indicated indarkgray. Asterisks indicate statistically significant differences (P <.01), andhorizontal bars indicate lower limits of normal levels forserum copper and ceruloplasmin and the upper limit of normallevel for urinary copper excretion.Normal levels: serumcopper,80-120 mg/dL; serum ceruloplasmin, 0.22-0.58 g/L; urinarycopper/creatinine ratio, <50 mg/g.
September 2013 ORIGINAL ARTICLES
copper excretion disappeared (FS: r = �0.26, P = .24; trans-plantation: r =�0.38, P = .22). Thus, this correlation is likelyrelated to the fact that more children with FS (and thus in-creased tubular losses) had a rather low glomerular filtrationrate compared with those who underwent transplantation.
DNA AnalysisNo specific sequence variations in the ATP7A, CTR1, LOX,COL1A1, or COL1A2 genes were associated with cysteaminetoxicity.
Copper Deficiency in Patients with Cystinosis with Cysteamine T
(Pro)collagen Synthesis StudiesAnalysis of pro-a- and a-collagen chains by sodium dodecylsulfate–polyacrylamide gel electrophoresis showed a normalpattern for intracellular and secreted type I and type IIIcollagen in all patients tested. The addition of 0.1 mM cyste-amine had no effect on the electrophoretic migrationpatterns of the pro-a- and a-collagen chains of type I andtype III collagen.
Discussion
Copper deficiency was demonstrated in all patients with cys-teamine toxicity. Because 95% of serum copper is bound toceruloplasmin,19 ceruloplasmin is the most valuable bio-marker for assessing body copper status.20 Strikingly, serumceruloplasmin levels were also below the normal range in allpatients with toxicity. These data support our hypothesis thatcopper deficiency plays a role in the etiology of cysteaminetoxicity in patients with cystinosis. To unravel the cause ofcopper deficiency, we initially focused on urinary copper ex-cretion. We found increased urinary copper excretion in allof our patients with FS, indicating that renal copper trans-porters are affected by cystinosis.Copper is almost completely reabsorbed by proximal tu-
bular cells via a concerted action of the apical CTR1 andbasolateral copper transporter ATP7A.21 Along with renalcopper reabsorption, these transporters are involved in in-testinal (ATP7A) and liver (CTR1) copper uptake. Muta-tions in ATP7A cause severe copper deficiency, alsoknown as Menkes disease, or its milder variant, occipitalhorn syndrome.22,23 Interestingly, ATP7A is situated onthe X chromosome, and 7 of 8 patients with cystinosiswith cysteamine toxicity in a previous report were male,6
suggesting a possible X-linked inheritance. However, no ge-netic sequence variations were found in ATP7A, and thusthis hypothesis was rejected. CTR1 facilitates the uptakeof copper by hepatocytes after its initial uptake from thegastrointestinal tract.24 No diseases associated with muta-tions in CTR1 have been described in humans, likely owingto embryonic lethality, as has been described in a mousemodel deficient in this transporter.25 Although we were un-able to demonstrate a link between abnormalities in theCTR1 and ATP7A transporters and the copper deficiencyseen in our small group of patients with cystinosis, it wouldseem reasonable to further investigate the role of thesetransporters in other inherited renal diseases, such asDent disease and Lowe syndrome.Normally, approximately 4% of copper is excreted into
urine.26 Thus, a 2- to 4-fold increased copper excretion inpatients with FS is likely to underlie serum copper defi-ciency; however, no differences in urinary copper excretionwere seen between patients with cysteamine toxicity andthose without cysteamine toxicity. On the other hand, dif-ferences in intestinal or hepatic copper uptake or differencesin copper intake also could be responsible for the lower se-rum copper levels. The copper content of foods such as
oxicity 757

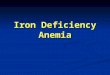
Figure 2. Proposed molecular mechanism of cysteamine toxicity. Because copper is a cofactor of lysyl oxidase, copper defi-ciency results in decreased aldehyde formation in collagen chains (1). Normally, these aldehydes are used to generate collagencross-links (2). Cysteamine binds aldehydes, making them unavailable for cross-linking (3). Thus, copper deficiency in combi-nation with cysteamine administration causes decreased collagen cross-linking by reducing the amount of available aldehydes.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 163, No. 3
wheat, fruits, and vegetables is highly variable. Moreover,the copper content of drinking water and of nutrients culti-vated in different parts of the world varies,27,28 and thus theexact determination of a person’s daily copper intake wouldrequire determination in duplicate meals, which is ex-tremely labor-intensive.27 Interestingly, many patients withcystinosis ingest the dietary supplement chlorophyllin tomask the halitosis that results from cysteamine administra-tion, which contains 4 mg of elemental copper per 100 mg.Thus, differences in copper levels of drinking water, com-bined with the fact that chlorophyllin is widely availablein stores the US, but not in Europe (and is thus usedmore frequently used by US patients compared with Euro-pean patients) could explain why all of the previously re-ported patients with cysteamine toxicity were residents ofEurope.6
It has been known for decades that copper deficiency canmimic lathyrism.7 Interestingly, cysteamine administrationalso can provoke osteolathyrism and angiolathyrism whengiven at high doses to rats and turkeys.29-31 In addition, treat-ment of pregnant rats with cysteamine produced higherfrequencies of intrauterine death, intrauterine growth retar-dation, cleft palate, and skeletal development abnormalities,including kyphosis and rib abnormalities.32 In theory, cyste-amine can enhance copper deficiency by serving as a chelating
758
agent, given its structural resemblance to D-penicillamine.The chelating properties of D-penicillamine are thought tobe exerted by binding the metal with its S and N atoms,33
both of which are present in cysteamine. However, a trial us-ing cystamine (the oxidized form of cysteamine, which is rap-idly reduced into 2 cysteamine molecules) showed no effecton urinary copper excretion, whereas the administration ofD-penicillamine was associated with significantly increasedurinary copper excretion.34
One-half of the patients with cysteamine toxicity weretreated with high cysteamine doses above 1.95 g/m2/day,and the other patients received doses ranging between 1.2and 1.7 g/m2/day. In all patients, decreasing the cysteaminedose resulted in amelioration or even disappearance ofsymptoms6; thus, the dose threshold for developing cyste-amine toxicity could not be identified. Most likely, the com-bination of copper deficiency with cysteamine exposure wasresponsible for the appearance of the symptoms. This mightexplain why only a small subset of patients with cystinosisdeveloped adverse effects of the drug, and many patients re-ceived comparable cysteamine doses. The proposed mecha-nism is summarized in Figure 2. We suggest that copperdeficiency causes decreased activity of lysyl oxidase,leading to the decreased formation of aldehydes requiredfor the collagen cross-linking. This latter mechanism can
Besouw et al

Table II. Dietary reference intake (RDA) andmaximumdaily intake of copper37
Age group RDA Tolerable upper limit
Adults >19 years 900 mg 10 mgWomen, pregnant 1000 mg 10 mg; 8 if #18 yearsWomen, lactating 1300 mg 10 mg; 8 if #18 yearsAdolescents 14-18 years 890 mg 8 mgChildren 9-13 years 700 mg 5 mgChildren 4-8 years 440 mg 3 mgChildren 1-3 years 340 mg 1 mgInfants 7-12 months 220 mg* No data availableInfants 0-6 months 200 mg* No data available
RDA, recommended daily allowance.*Adequate intake; RDA is not established.
September 2013 ORIGINAL ARTICLES
be aggravated by the administration of cysteamine, whichbinds to aldehydes, decreasing their availability for thiscross-linking.
Definitive proof of our hypothesis would be provided bydetection of decreased lysyl oxidase activity in patients withtoxicity. Unfortunately, the activity of lysyl oxidase can onlybe measured invasively in tissue samples (eg, aorta),35,36 andits activity is not reflected by protein or mitochondrial RNAlevels.35 However, the increased variability in collagen fibrildiameter seen in the skin biopsy specimens from patientswith cysteamine toxicity might indicate defective collagencross-linking, thereby supporting our hypothesis. Nonethe-less, our findings implicate that copper supplementationmight prevent cysteamine toxicity or accelerate the reduc-tion of symptoms that are already present; thus, the admin-istration of copper supplements should be considered inpatients with cystinosis, especially in those with FS. Guide-lines regarding dosing strategies are provided in Table II;however, patients with FS might require higher copperdoses.
We found no specific sequence variations in the open read-ing frames and splice donor and acceptor sites of the coppertransporters ATP7A and CTR1, lysyl oxidase gene LOX, orthe type I procollagen encoding genes COL1A1 andCOL1A2 that could account for the development of cyste-amine toxicity in patients with cystinosis. However, possiblepolymorphisms in intronic or promotor regions, or geneticalterations in other genes involved in copper metabolism,cannot be excluded. Finally, we found no difference in thesynthesis of type I and type III (pro)collagens by fibroblastsobtained from patients with and without cysteamine toxicity,in either the absence or presence of 0.1 mM cysteamine.These results confirm our hypothesis that defective collagencross-linking, which occurs posttranslationally, and not de-fective collagen synthesis, underlies the cysteamine toxicityin patients with cystinosis. n
Submitted for publication May 3, 2012; last revision received Jan 9, 2013;
accepted Mar 28, 2013.
Reprint requests: Martine T. P. Besouw, MD, Department of Pediatric
Nephrology, University Hospitals Leuven, Herestraat 49, 3000 Leuven,
Belgium. E-mail: [email protected]
Copper Deficiency in Patients with Cystinosis with Cysteamine T
References
1. Gahl WA, Thoene JG, Schneider JA. Cystinosis. N Engl J Med 2002;347:
111-21.
2. Markello TC, Bernardini IM, GahlWA. Improved renal function in chil-
dren with cystinosis treated with cysteamine. N Engl J Med 1993;328:
1157-62.
3. Gahl WA, Balog JZ, Kleta R. Nephropathic cystinosis in adults: natural
history and effects of oral cysteamine therapy. Ann Intern Med 2007;
147:242-50.
4. Brodin-Sartorius A, Tete MJ, Niaudet P, Antignac C, Guest G,
Ottolenghi C, et al. Cysteamine therapy delays the progression of neph-
ropathic cystinosis in late adolescents and adults. Kidney Int 2012;81:
179-89.
5. Van Stralen KJ, Emma F, Jager KJ, Verrina E, Schaefer F, Laube GF, et al.
Improvement in the renal prognosis in nephropathic cystinosis. Clin J
Am Soc Nephrol 2011;6:2485-91.
6. Besouw MT, Bowker R, Dutertre JP, Emma F, Gahl WA, Greco M,
et al. Cysteamine toxicity in patients with cystinosis. J Pediatr 2011;
159:1004-11.
7. Nimni ME. Mechanism of inhibition of collagen crosslinking by penicil-
lamine. Proc R Soc Med 1977;70(Suppl 3):65-72.
8. Barrow MV, Simpson CF, Miller EJ. Lathyrism: a review. Q Rev Biol
1974;49:101-28.
9. Haque A, Hossain M, Lambein F, Bell EA. Evidence of osteolathyrism
among patients suffering from neurolathyrism in Bangladesh. Nat
Toxins 1997;5:43-6.
10. Cohn DF, Streifler M. Intoxication by the chickling pea (Lathyrus sati-
vus): nervous system and skeletal findings. Arch Toxicol Suppl 1983;6:
190-3.
11. CohnDF, StreiflerM. Human neurolathyrism, a follow-up study, part II:
special investigations. Schweiz Arch Neurol Neurochir Psychiatr 1981;
128:157-63.
12. Weintroub S, Cohn DF, Salama R, Streifler M, Weissman SL. Skeletal
findings in human neurolathyrism. Is there a human osteolathyrism?
Eur Neurol 1980;19:121-7.
13. Siegel RC, Pinnell SR, Martin GR. Cross-linking of collagen and elastin:
properties of lysyl oxidase. Biochemistry 1970;9:4486-92.
14. Liu PC, McAndrew PE, Kaler SG. Rapid and robust screening of the
Menkes disease/occipital horn syndrome gene. Genet Test 2002;6:
255-60.
15. De Bonis P, Laborante A, Pizzicoli C, Stallone R, Barbano R, Longo C,
et al. Mutational screening of VSX1, SPARC, SOD1, LOX, and TIMP3
in keratoconus. Mol Vis 2011;17:2482-94.
16. Korkko J, La-Kokko L, De Paepe A, Nuytinck L, Earley J, Prockop DJ.
Analysis of the COL1A1 and COL1A2 genes by PCR amplification and
scanning by conformation-sensitive gel electrophoresis identifies only
COL1A1 mutations in 15 patients with osteogenesis imperfecta type I:
identification of common sequences of null-allele mutations. Am J
Hum Genet 1998;62:98-110.
17. Smolin LA, Clark KF, Thoene JG, GahlWA, Schneider JA. A comparison
of the effectiveness of cysteamine and phosphocysteamine in elevating
plasma cysteamine concentration and decreasing leukocyte-free cystine
in nephropathic cystinosis. Pediatr Res 1988;23:616-20.
18. Malfait F, Symoens S, Coucke P, Nunes L, De Almeida S, De Paepe A.
Total absence of the alpha2(I) chain of collagen type I causes a rare
form of Ehlers-Danlos syndrome with hypermobility and propensity
to cardiac valvular problems. J Med Genet 2006;43:e36.
19. Gubler CJ, Lahey ME, Cartwright GE, Wintrobe MM. Studies on copper
metabolism, IX: the transportation of copper in blood. J Clin Invest
1953;32:405-14.
20. Harvey LJ, Ashton K, Hooper L, Casgrain A, Fairweather-Tait SJ.
Methods of assessment of copper status in humans: a systematic review.
Am J Clin Nutr 2009;89:2009S-24S.
21. Ellingsen D, Horn N, Aaseth J. Copper. In: Nordberg G, Fowler B,
Nordberg M, Friberg L, eds. Handbook of toxicology of metals. Stock-
holm, Sweden: Elsevier; 2007. p. 529-46.
oxicity 759

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 163, No. 3
22. Kodama H, Fujisawa C, Bhadhprasit W. Inherited copper transport dis-
orders: biochemical mechanisms, diagnosis, and treatment. Curr Drug
Metab 2012;13:237-50.
23. Cox DW, Moore SD. Copper transporting P-type ATPases and human
disease. J Bioenerg Biomembr 2002;34:333-8.
24. Tao TY, Gitlin JD. Hepatic copper metabolism: insights from genetic
disease. Hepatology 2003;37:1241-7.
25. Lee J, Prohaska JR, Thiele DJ. Essential role for mammalian copper
transporter Ctr1 in copper homeostasis and embryonic development.
Proc Natl Acad Sci USA 2001;98:6842-7.
26. Cartwright GE, Wintrobe MM. Copper metabolism in normal subjects.
Am J Clin Nutr 1964;14:224-32.
27. Klevay LM. Is the Western diet adequate in copper? J Trace Elem Med
Biol 2011;25:204-12.
28. Georgopoulos PG, Roy A, Yonone-Lioy MJ, Opiekun RE, Lioy PJ. Envi-
ronmental copper: its dynamics and human exposure issues. J Toxicol
Environ Health B Crit Rev 2001;4:341-94.
29. Dasler W, Milliser RV. Osteolathyrogenic action of mercaptoethylamine
and of cystamine. Proc Soc Exp Biol Med 1958;98:759-62.
30. McDonald BE, Bird HR, Strong FM. Effects of amino acids and related
compounds on aortic aneurysms in turkeys. Proc Soc Exp Biol Med
1963;113:728-32.
760
31. Jayaraj AP. Dissecting aneurysm of aorta in rats fed with cysteamine. Br J
Exp Pathol 1983;64:548-52.
32. Beckman DA, Mullin JJ, Assadi FK. Developmental toxicity of cyste-
amine in the rat: effects on embryo-fetal development. Teratology
1998;58:96-102.
33. Chisolm JJ Jr. The use of chelating agents in the treatment of
acute and chronic lead intoxication in childhood. J Pediatr 1968;
73:1-38.
34. Walshe JM. Penicillamine, a new oral therapy for Wilson’s disease. Am J
Med 1956;21:487-95.
35. Rucker RB, Kosonen T, Clegg MS, Mitchell AE, Rucker BR, Uriu-
Hare JY, et al. Copper, lysyl oxidase, and extracellular matrix protein
cross-linking. Am J Clin Nutr 1998;67:996S-1002S.
36. Pestov NB, Okkelman IA, Shmanai VV, Hurski AL, Giaccia AJ,
Shchepinov MS. Control of lysyl oxidase activity through site-
specific deuteration of lysine. Bioorg Med Chem Lett 2011;21:
255-8.
37. Food and Nutrition Board and Institute of Medicine. Copper. In: Die-
tary reference intakes for vitamin A, vitamin K, arsenic, boron, chro-
mium, copper, iodine, iron, manganese, molybdenum, nickel, silicon,
vanadium, and zinc. Washington, DC: National Academies Press;
2001. p. 224-57.
Besouw et al