Embed Size (px)
DESCRIPTION
kedokteran
Citation preview

7/17/2019 Copd With Chf2
http://slidepdf.com/reader/full/copd-with-chf2 1/9
CASE REPORT
Acute COPD Exacerbation with Congestive Heart Failure
Riski Dohartua, Amira Permatasari T Division of COPD
Departent of Pulonolog! an" Respirator! #e"icineSchool of #e"icine $niversitas Suatera $tara% A"a #ali& 'eneral
Hospital#e"an
Abstract
It has been reported in male patients aged 53 years, came to the hospital
with complaints of shortness of breath and early diagnosis of patients with
COPD exacerbations with CPC. Patients in the hospital joint with the cardiology.
rom the chest x!ray shows a pict"re emfisemat"s, diaphragm lies low, and
hiperl"sen pict"re, heart pict"re of the pend"l"m. #C$ showed a pict"re of the
CPC. %he res"lts showed abnormal spirometry obstr"ction and restriction. %he
res"lts showed #chocardiography C&. Patients were gi'en treatment therapy
(.)* +aCl with minophilin - mg -( drips/min"te, lixotide and 0entoline 1
ho"rly 'ia a neb"ls, Ceftriaxon injection of 2 g / 1 ho"rs, dexamethason injection
5gr amp/1 ho"rs, f"rosemide injection amp / 1 ho"r, salb"tamol tablets mg 3
times daily, digoxintablets (,-5 mg 3 times daily, spironolactone tablets -5 mg
daily, simarc tablets - mg daily, with stable COPD treatment res"lts and patient
was taen to the cardiac care.
Key Words : COPD, CHF.
()TROD$CT(O)
C& and COPD are two commonly enco"ntered conditions in clinical
practice. C& acco"nts for their fre4"ent coexistence. %he pre'alence of COPD
1
7/17/2019 Copd With Chf2
http://slidepdf.com/reader/full/copd-with-chf2 2/9
ranges from -(* to 3-* in patients with. #02 is as good a predictor of
cardio'asc"lar mortality as ser"m cholesterol Ischemic heart disease, and not
respiratory fail"re, is the leading ca"se of death in COPD patients, with only a
small fraction dying of respiratory fail"re. %he relationship between COPD and
cardio'asc"lar e'ents remains "nclear. Patients with COPD are not at
increased ris for hypertension or left 'entric"lar hypertrophy howe'er, they
consistently show e'idence of low!grade systemic inflammation that plays an
increasingly recogni6ed role in the pathogenesis of atherosclerosis. Patients
with se'ere COPD are -.217-.8 times more liely to ha'e ele'ated or highly
ele'ated circ"lating C9P le'els than control s"bjects. woring hypothesisto
acco"nt for the high pre'alence of systolic dysf"nction in patients with COPD is
that low!grade systemic inflammation accelerates the progression of coronary
atherosclerosis, which "ltimately res"lts in ischemic cardiomyopathy. :"ch a
hypothesis fits the clinical obser'ation of a high incidence of left 'entric"lar wall
motion abnormalities noted in patients with COPD and left 'entric"lar
dysf"nction.2
CASE REPORT
Patients admitted to dam ;ali &ospita with main complain of
shortness of breath since < / ! = years ago, and become worse in 3 day. Chest
pain happened since 3 years ago and become worse if patient ha'e co"gh, lie
a p"nct"red!pric pain. Co"gh has occ"red since 2 months with yellowish.
:wellingon the both of legs happened since 2 wee ago.
0ital signs showed alert, >P ? 2-(/)( mm&g, P"lse ? 12 times/min"te,
9espiratory rate ? 3= times/min"te, %emperat"re ? 3=.3(C.
Physical examination showed inspection simetrical chest inspection,
tactil fremit"s was decreased on both of the l"ng. Perc"ssion was hypersonor
on both of the l"ng. 0esic"lar decreased breath so"nd on both of the l"ng. irst
and second heart so"nd irreg"lar, mid!diastolic m"rm"r grade - / = at the apex,
gallops not fo"nd.
2

7/17/2019 Copd With Chf2
http://slidepdf.com/reader/full/copd-with-chf2 3/9
@aboratory findings ? &b ? 25,3 g/dl, A>C ? 22,1 x 2() /@, platelet ?21=
2(3/mm-, rterial blood gases ? p& ? 8.), PaO- ? 2( mm&g, PaCO- ? 32
mm&g, ># ? 2,(, &Co3 ? -5, mmol/@, :aO- ? ))*, interpretation ? respiratory
alcalosis.
Chest x 7 ray showed emphysemato"s on both of the l"ng, diapraghm
was flattein, tracheal in the midle position. C%9 53 *,Bfig.2. rom the #C$
showed 909 < 9D < 90&. #chocardiography showed :tenosis ;itral ec
P"lmonary &ypertension Big. -. :pirometry showed obstr"cti'e and restricti'e
abnormalities.
ig"re 2. %horax P, 2th :eptember -(22 dam ;ali &ospital
3

7/17/2019 Copd With Chf2
http://slidepdf.com/reader/full/copd-with-chf2 4/9
ig"re -. #chocardiography, -th :eptember -(22 dam ;ali &ospital
#arly diagnosis of this patient COPD with CPC, was -th :eptember -(22
the woring diagnosis was COPD with C& c I!II ec :tenosis ;itral moderate.
Patients were gi'en treatment therapy (.)* +aCl with minophilin -
mg -( drips/min"te, lixotide and 0entoline 1 ho"rly 'ia a neb"ls, Ceftriaxon
injection of 2 g / 1 ho"rs, dexamethason injection 5gr amp/1 ho"rs, f"rosemide
injection amp / 1 ho"r, salb"tamol tablets mg 3 times daily, digoxintablets (,-5
mg 3 times daily, spironolactone tablets -5 mg daily, simarc tablets - mg daily.
D(SC$SS(O)
COPD is characteri6ed by progressi'e blood gas abnormalities. ;ild
hypoxaemia may be present in the early stages of COPD, and it "s"ally
progresses as the disease worsens. &ypercapnia may accompany more se'ere
disease. ntreated hypoxaemia and hypercapnia can ca"se p"lmonary
hypertension and cor p"lmonale, which contrib"te to the morbidity and mortality
associated with this disease. %he str"ct"ral derangements and specific
mechanisms responsible for gas exchange abnormalities in COPD are
exceedingly complex and imperfectly "nderstood. -
COPD is a disease state characteri6ed by airflow limitation that is not
f"lly re'ersible. %he airflow limitation is "s"ally both progressi'e and associated
with an abnormal inflammatory response of the l"ngs to noxio"s particles or
gases.3
4

7/17/2019 Copd With Chf2
http://slidepdf.com/reader/full/copd-with-chf2 5/9
Patients with COPD characteristically complain of the symptoms of
breathlessness on exertion, sometimes accompanied by whee6e and co"gh.
%he co"gh is often, b"t not in'ariably, prod"cti'e. >reathlessness is the
symptom that commonly ca"ses the patient to see medical attention and is
"s"ally the most disabling problem. Patients often date the onset of their illness
to an ac"te exacerbation of co"gh with sp"t"m prod"ction, which lea'es them
with a degree of chronic breathlessness. Close 4"estioning, howe'er, "s"ally
re'eals many years of a Esmoers co"ghF with the prod"ction of small amo"nts
of m"coid sp"t"m B"s"ally G=( m@/day often in the morning for many years.
prod"cti'e co"gh occ"rs in "p to 5(* of cigarette smoers and may precede
the onset of breathlessness. ;any patients may dismiss this as simply being
related to their smoing. %he fre4"ency of noct"rnal co"gh does not seem to be
increased in stable COPD. Paroxysms of co"ghing in the presence of se'ere
airway obstr"ction generate high intrathoracic press"res, which can prod"ce
syncope and Eco"gh fract"resF of the ribs.
P"lmonary f"nction is often dist"rbed d"ring left 'entric"lar fail"re.
d'anced left 'entric"lar fail"re prod"ces mared impairment in p"lmonary
f"nction, whereas early left 'entric"lar fail"re, with its attendant mild p"lmonary
hypertension Be.g., p"lmonary artery wedge press"re HPAP of 25 to -( mm
&g, act"ally impro'es gas exchange thro"gh an increased p"lmonary blood
'ol"me and impro'ed 'entilation!perf"sion B0./J.matching. s left 'entric"lar
f"nction deteriorates and increasing p"lmonary congestion occ"rs, l"ng water
increases. %his ca"ses decreases in l"ng 'ol"me and diff"sion capacity and
increases in airway resistance and 0./J. mismatching. :e'ere fail"re and franal'eolar flooding are often accompanied by a dramatic deterioration in forced
'ital capacity B0C, forced expiratory 'ol"me in 2 second B#02, l"ng
compliance, and gas exchange, as well as a mixed respiratory and metabolic
acidosis. %hese changes can ca"se f"rther heart fail"re, which ca"ses f"rther
p"lmonary dysf"nction, and th"s a 'icio"s circle of fail"re begins. 5
5
7/17/2019 Copd With Chf2
http://slidepdf.com/reader/full/copd-with-chf2 6/9
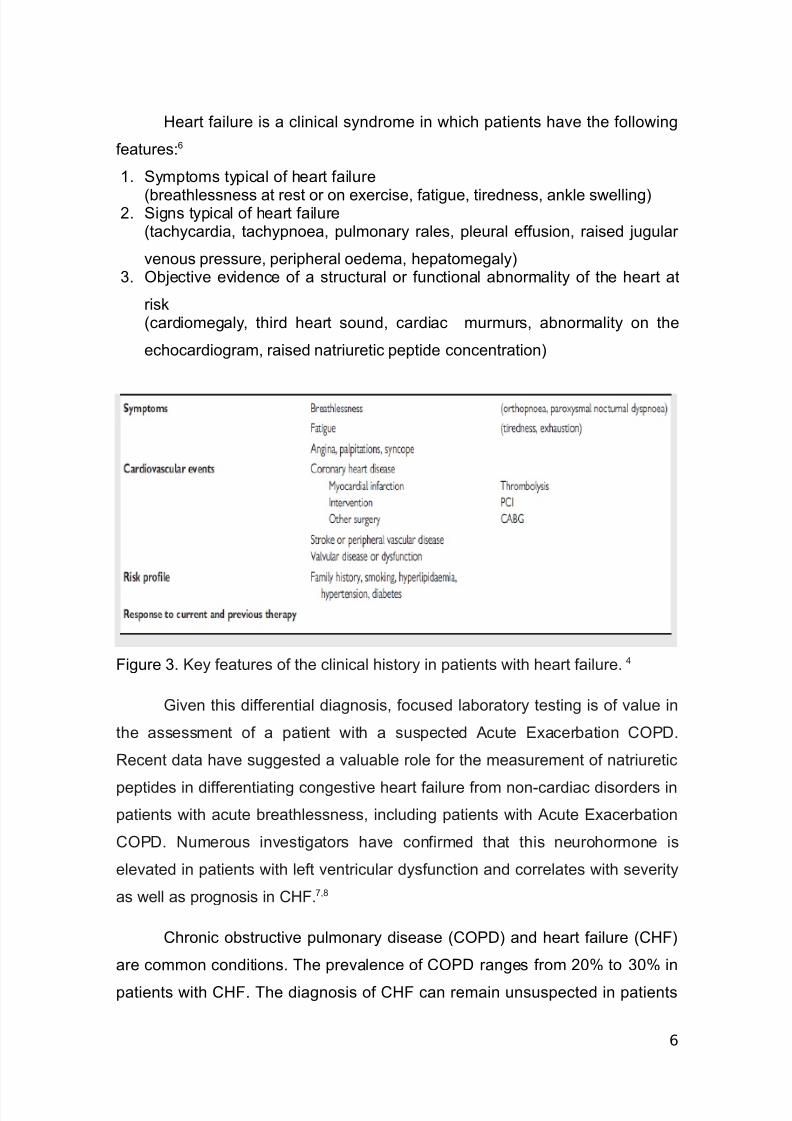
&eart fail"re is a clinical syndrome in which patients ha'e the following
feat"res?=
2. :ymptoms typical of heart fail"re
Bbreathlessness at rest or on exercise, fatig"e, tiredness, anle swelling-. :igns typical of heart fail"re
Btachycardia, tachypnoea, p"lmonary rales, ple"ral eff"sion, raised j"g"lar
'eno"s press"re, peripheral oedema, hepatomegaly3. Objecti'e e'idence of a str"ct"ral or f"nctional abnormality of the heart at
risBcardiomegaly, third heart so"nd, cardiac m"rm"rs, abnormality on the
echocardiogram, raised natri"retic peptide concentration
ig"re 3. Key feat"res of the clinical history in patients with heart fail"re.
$i'en this differential diagnosis, foc"sed laboratory testing is of 'al"e in
the assessment of a patient with a s"spected c"te #xacerbation COPD.
9ecent data ha'e s"ggested a 'al"able role for the meas"rement of natri"retic
peptides in differentiating congesti'e heart fail"re from non!cardiac disorders in
patients with ac"te breathlessness, incl"ding patients with c"te #xacerbation
COPD. +"mero"s in'estigators ha'e confirmed that this ne"rohormone is
ele'ated in patients with left 'entric"lar dysf"nction and correlates with se'erity
as well as prognosis in C&.8,1
Chronic obstr"cti'e p"lmonary disease BCOPD and heart fail"re BC&
are common conditions. %he pre'alence of COPD ranges from -(* to 3(* in
patients with C&. %he diagnosis of C& can remain "ns"spected in patients
6

7/17/2019 Copd With Chf2
http://slidepdf.com/reader/full/copd-with-chf2 7/9
with COPD, beca"se shortness of breath is attrib"ted to COPD. ;eas"rement
of plasma >!type natri"retic peptide B>+P le'els helps to "nco'er "ns"spected
C& in patients with COPD and clinical deterioration. +onin'asi'e assessment
of cardiac f"nction may be preferable to >+P to "nco'er "ns"spected left
'entric"lar B@0 systolic dysf"nction in patients with stable COPD. Patients with
COPD or C& de'elop seletal m"scle alterations that are striingly similar.
"nctional intolerance correlates with se'erity of seletal m"scle alterations b"t
not with se'erity of p"lmonary or cardiac impairment in COPD and C&,
respecti'ely. Impro'ement of p"lmonary or cardiac f"nction does not translate
into relief of f"nctional intolerance in patients with COPD or C& "nless seletal
m"scle alterations concomitantly regress. %he mechanisms responsible for
seletal m"scle alterations are incompletely "nderstood in COPD and in C&.
Dis"se and low!le'el systemic inflammation leading to protein
synthesis/degradation imbalance are liely to contrib"te. %he presence of
COPD impacts on the treatment of C&, as COPD is still 'iewed as a
contraindication to beta!blocade. %herefore, COPD often depri'es patients with
C& d"e to @0 systolic dysf"nction of the most beneficial pharmacologic
inter'ention. large body of data indicates that patients with COPD tolerate well
selecti'e beta!blocade that sho"ld not be denied to C& patients with
concomitant COPD.),2(
Conclusion
It has been reported in male patients aged 53 years, came to the hospital
with complaints of shortness of breath and early diagnosis of patients with
COPD exacerbations with CPC. Patients in the hospital joint with the cardiology.
rom the chest x!ray shows a pict"re emfisemat"s, diaphragm lies low, and
hiperl"sen pict"re, heart pict"re of the pend"l"m. #C$ showed a pict"re of the
CPC. %he res"lts showed abnormal spirometry obstr"ction and restriction. %he
res"lts showed #chocardiography C&. Patients were gi'en treatment therapy
(.)* +aCl with minophilin - mg -( drips/min"te, lixotide and 0entoline 1
ho"rly 'ia a neb"ls, Ceftriaxon injection of 2 g / 1 ho"rs, dexamethason injection
5gr amp/1 ho"rs, f"rosemide injection amp / 1 ho"r, salb"tamol tablets mg 3
times daily, digoxintablets (,-5 mg 3 times daily, spironolactone tablets -5 mg
7
7/17/2019 Copd With Chf2
http://slidepdf.com/reader/full/copd-with-chf2 8/9
daily, simarc tablets - mg daily, with stable COPD treatment res"lts and patient
was taen to the cardiac care.
REFERE)CES
2. abbri @eonardo ;, @"ppi abri6io, >eghe >ianca. %he ;"ltiple Components of
COPD. In? L +icola . &anania, mir :harafhaneh, #d. COPD $"de to
8

7/17/2019 Copd With Chf2
http://slidepdf.com/reader/full/copd-with-chf2 9/9
Diagnosis and Clinical ;anagement. &o"ston? >aylor College of ;edicine,
-(22. p. 2(-. +iewoehner Dennis #. :tr"ct"re!f"nction relationships? the pathophysiology of
airflow obstr"ction. In? Chronic Obstr"cti'e P"lmonary Disease. 2st #D p. 5,
12.3. ;acnee Ailliam. Chronic Obstr"cti'e P"lmonary Disease ? #pedemiology,
Physiology, and Clinical #'al"ation. In? Clinical 9espiratory ;edicine. 3rd #d.
Philadelpia? ;osby -((1. p. 5(1.. &ics $eorge &, ;arsha rth"r >. &eart ail"re. In? 9epiratory Disease
Case :t"dy pproach to Patient care. 3rd #D. Philadelpia? Da'is -((8. p.
28(.
5. ilippatos $erasimos, Dicstein Kenneth, Cohen!:olal lain, at all. #:C$"idelines for the diagnosis and treatment of ac"te and chronic heart fail"re
-((1. #"ropean L of &eart ail"re. p. )3= )31=. & ;arshall, &"nt :haron , >aer Da'id A, at all. CC/& $"idelines for the
#'al"ation and ;anagement of Chronic &eart ail"re in the d"lt? #xec"ti'e
:"mmary 9eport of the merican College of Cardiology/merican &eart
ssociation %as orce on Practice $"idelines BCommittee to 9e'ise the 2))5
$"idelines for the #'al"ation and ;anagement of &eart ail"re. L of the
merican heart ssociation -((2. p. 3(((.8. ;artine6 ernando L, C"rtis Leffrey @. c"te #xacerbations of Chronic
Obstr"cti'e P"lmonary Disease. In? ishmanMs P"lmonary Diseases and
Disorders. th #d, 0ol 2N-. +ew or? ;c$raw &ill ;edical -((1. p. -221.1. m"rphy timothy f, sethi sanjay. Infection in the pathogenesis and co"rse of
Chronic Obstr"cti'e P"lmonary Disease. L of the +ew #ngland Lo"rnal of
;edicine +o'ember -8, -((1. p. -355.). Lelic :anja, & %hierry, Lemtel @e. Diagnostic and %herape"tic Challenges in
Patients Aith coexistent Chronic Obstr"cti'e P"lmonary Disease and Chronic
&eart ail"re. L of the merican College of Cardiology.-((8. p. 28-.
10. :tromberg , ;artensson L, ridl"nd >, @e'in @, Karlsson L#, Dahlstrom
.+"rse!led heart fail"re clinics impro'e s"r'i'al and self!care beha'io"r
inpatients with heart fail"re? res"lts from a prospecti'e, randomised trial. #"r
&eart L -((3-?2(272(-3.
9