Embed Size (px)
DESCRIPTION
COPD Flip part 1. JK Amorosa. Emphysema. Centriacinar (centrilobular) Panlobular Paraseptal Irregular. Emphysema definitions. Centriacinar : cigarette smoking, upper lobes Dilitation second order respiratory bronchioles, respiratory bronchiolitis may be precursor - PowerPoint PPT Presentation
Citation preview

COPD Flip part 1
JK Amorosa

Emphysema
• Centriacinar (centrilobular)• Panlobular• Paraseptal• Irregular

Emphysema definitions• Centriacinar: cigarette smoking, upper lobes Dilitation second order respiratory
bronchioles, respiratory bronchiolitis may be precursor
Panlobular: lower lobes, involves entire lobule, seen in senile emphysema and alpha-1-antiprotease deficiency
• Paraseptal: involves periphery of secondary pulmonary lobule, assoc with scars, ptx
• Bullae: Emphysema with more than 1 cm in diameter with wall thickness < 1mm

Emphysema Chest X-ray
• Hyperinflation• Flat diaphragms• Widened retrosternal air space• Lung height increased• Small narrow heart

Emphysema lung parenchyma
• Arterial deficiency, increased branching angle of remaining vessels
• Increased markings / bronchial wall thickening or superimposed enphysematous walls

Emphysema secondary manifestations
• PA hypertension

HRCT• Emphysematous holes have no walls, attenuation
values of −950 HU or less on thin-section CT scans with a 10-mm interval correlate well with pulmonary function test results and the pathologic distribution of emphysema, reduced CT attenuation coefficients
• Bronchial wall thickening• Hyperinflation• Expiratory air-trapping• Vascular pruning



Emphysema-predominant airway-dominant
Radiology Oct 2011

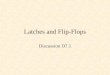
Figure 1 Axial CT image obtained in a 66- year-old man with COPD and severe airflow obstruction (percentage of predicted FEV1, 40.8%) shows mild emphysema (relative low-attenuation area with attenuation of −950 HU or lower, 5.8%). Low-attenuation areas representing emphysematous change (“holes”) are indicated by arrowheads.
RadioGraphics, http://pubs.rsna.org/doi/abs/10.1148/rg.301095110

Figure 3b (a) Axial CT image obtained in a 72-year-old man with COPD shows multiple low-attenuation areas of emphysema. (b) Axial CT image obtained with data segmentation shows the same lung field as in a. The total lung parenchymal area (areas with attenuation of −500 to −1024 HU) is depicted in red, and vascular and other structures are shown in gray. (c) Axial CT image obtained with data segmentation shows the same lung field as in a and b. Voxels with attenuation of −950 HU or lower are depicted in red, and those with attenuation of −500 to −949 HU are depicted in black. (Vascular and other nonparenchymal structures are shown in gray.) To quantify the extent of emphysema, the percentage of the total lung area occupied by voxels with attenuation of −950 HU or lower (ie, the relative low-attenuation area) can be calculated from these segmented CT image data.
RadioGraphics, http://pubs.rsna.org/doi/abs/10.1148/rg.301095110

Figure 3c (a) Axial CT image obtained in a 72-year-old man with COPD shows multiple low-attenuation areas of emphysema. (b) Axial CT image obtained with data segmentation shows the same lung field as in a. The total lung parenchymal area (areas with attenuation of −500 to −1024 HU) is depicted in red, and vascular and other structures are shown in gray. (c) Axial CT image obtained with data segmentation shows the same lung field as in a and b. Voxels with attenuation of −950 HU or lower are depicted in red, and those with attenuation of −500 to −949 HU are depicted in black. (Vascular and other nonparenchymal structures are shown in gray.) To quantify the extent of emphysema, the percentage of the total lung area occupied by voxels with attenuation of −950 HU or lower (ie, the relative low-attenuation area) can be calculated from these segmented CT image data.
RadioGraphics, http://pubs.rsna.org/doi/abs/10.1148/rg.301095110

Emphysema Pathology
• Abnormal enlargement of airspaces distal to terminal bronchioles with destruction of alveolar walls

Figure 4 Coronal CT image obtained in a 62-year-old man with COPD shows upper-lung–predominant emphysema. The relative low-attenuation area with attenuation of −950 HU or lower (red) is 46.8%, and the percentage of predicted FEV1 is 56.8%.
RadioGraphics, http://pubs.rsna.org/doi/abs/10.1148/rg.301095110

Figure 5 Coronal CT image obtained in a 72-year-old man shows lower-lung–predominant emphysema. The relative low-attenuation area with attenuation of −950 HU or lower (red) is 45.8%, and the percentage of predicted FEV1 is 45.6%. The extent of lower-lung–predominant emphysema is more closely correlated with the result of pulmonary function testing than the extent of upper-lung–predominant emphysema. (In both figures, black indicates areas with attenuation of −500 to −949 HU and gray indicates vascular and other nonparenchymal structures.)
RadioGraphics, http://pubs.rsna.org/doi/abs/10.1148/rg.301095110

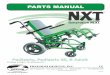
Figure 8a Volumetric CT-based measurement of airway dimensions. (a) Schema obtained with the region-growing method shows airway segmentation and selection of a bronchial pathway (black line) for measurement. A curved multiplanar reformatted image is reconstructed along the selected pathway, and a short-axis image is reconstructed in a plane exactly perpendicular to the long axis of the airway. The red dot indicates the location of the short-axis image in b. (b) Short-axis image with overlaid diagram shows the radii (red and green lines) used to delimit the inner lumen and calculate its area. From the point of their intersection, the centroid point, rays (blue lines) are drawn over a 360° radius through the airway wall to allow calculation of the airway wall thickness by using the full width at half maximum principle.
RadioGraphics, http://pubs.rsna.org/doi/abs/10.1148/rg.301095110

Figure 8b Volumetric CT-based measurement of airway dimensions. (a) Schema obtained with the region-growing method shows airway segmentation and selection of a bronchial pathway (black line) for measurement. A curved multiplanar reformatted image is reconstructed along the selected pathway, and a short-axis image is reconstructed in a plane exactly perpendicular to the long axis of the airway. The red dot indicates the location of the short-axis image in b. (b) Short-axis image with overlaid diagram shows the radii (red and green lines) used to delimit the inner lumen and calculate its area. From the point of their intersection, the centroid point, rays (blue lines) are drawn over a 360° radius through the airway wall to allow calculation of the airway wall thickness by using the full width at half maximum principle.
RadioGraphics, http://pubs.rsna.org/doi/abs/10.1148/rg.301095110

• Airway-predominant Rx: medicalSmall airway disease
cannot be visualized directly with current radiographic techniques, calculate: the expiratory-inspiratory attenuation ratio see volumetric CT based measurement
• Emphysema-predominant Rx: Sx

• 30% of lung has to be destroyed to alter pulmonary function

Pulmonary functions
• Increased total and residual volumes• RV(residual volume) >120% predicted• Decreased flow volumes • FEV Forced Expiratory Volume) <80%
predicted• Decreased diffusion capacity <80% predicted

Alpha 1-Antiprotease deficiency, normally enzyme blocks proteolytic enzymes
• Panlobular emphysema• Lower lobes• Common Pi ZZ phenotype 1 in 200, gene 14• Normal phenotype: Pi MM; Pi MZ 60% normal• Liver disease in infancy• Premature development of emphysema,
worse with smoking

References
• Regan EA, Hokanson JE, Murphy JR, et al.. Genetic epidemiology of COPD (COPDGene) study design. COPD 2010;7(1):32–43. [CrossRef] [Medline]
• SS Kim … D Lynch: Chronic Obstructive Pulmonary Disease: Lobe-based Visual Assessment of Volumetric CT by Using Standard Images—Comparison with Quantitative CT and Pulmonary Function Test in the COPDGene Study Radiology, 2013, Vol.266: 626-635, 10.1148/radiol.12120385
• S Matsuoka : Quantitative CT Assessment of COPD