Embed Size (px)
Citation preview

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 1/13
You are here: Home / Case Study / Chronic Obstructive Pulmonary Disorder (COPD) Case
Study
Chronic Obstructive Pulmonary Disorder
(COPD) Case StudyAugust 10, 2009 by Lhynnelli, RN · 3 Comments · Email This Post · Print This Post
INTRODUCTION:
Chronic obstructive pulmonary disease (COPD) is a disease state characterized by airflowlimitation that is not fully reversible. This newest definition COPD, provided by the Global
Initiative for Chrnonic Obstructive Lung Disease (GOLD), is a broad description that better
explains this disorder and its signs and symptoms (GOLD, World Health Organization [WHO] & National Heart, Lung and Blood Institute [NHLBI], 2004). Although previous definitions have
include emphysema and chronic bronchitis under the umbrella classification of COPD, this was
often confusing because most patient with COPD present with over lapping signs and symptoms
of these two distinct disease processes.
COPD may include diseases that cause airflow obstruction (e.g., Emphysema, chronic
bronchitis) or any combination of these disorders. Other diseases as cystic fibrosis,
bronchiectasis, and asthma that were previously classified as types of chronic obstructive lung
disease are now classified as chronic pulmonary disorders. However, asthma is now consideredas a separate disorder and is classified as an abnormal airway condition characterized primarily
by reversible inflammation. COPD can co-exist with asthma. Both of these diseases have the

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 2/13

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 3/13
When you breathe in, air enters your body through your nose or mouth. From there, it travels
down your throat through the larynx (or voicebox) and into the trachea (or windpipe) before
entering your lungs. All these structures act to funnel fresh air down from the outside world intoyour body. The upper airway is important because it must always stay open for you to be able to
breathe. It also helps to moisten and warm the air before it reaches your lungs.
The Lungs
Structure
The lungs are paired, cone-shaped organs which take up most of the space in our chests, along
with the heart. Their role is to take oxygen into the body, which we need for our cells to live and
function properly, and to help us get rid of carbon dioxide, which is a waste product. We eachhave two lungs, a left lung and a right lung. These are divided up into ‘lobes’, or big sections of
tissue separated by ‘fissures’ or dividers. The right lung has three lobes but the left lung has only
two, because the heart takes up some of the space in the left side of our chest. The lungs can also
be divided up into even smaller portions, called ‘bronchopulmonary segments’.
These are pyramidal-shaped areas which are also separated from each other by membranes.
There are about 10 of them in each lung. Each segment receives its own blood supply and air
supply.
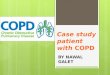
COPD VERSUS HEALTHY LUNG
How they work
Air enters your lungs through a system of pipes called the bronchi. These pipes start from the
bottom of the trachea as the left and right bronchi and branch many times throughout the lungs,until they eventually form little thin-walled air sacs or bubbles, known as the alveoli. The alveoli
are where the important work of gas exchange takes place between the air and your blood.
Covering each alveolus is a whole network of little blood vessel called capillaries, which are

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 4/13
very small branches of the pulmonary arteries. It is important that the air in the alveoli and the
blood in the capillaries are very close together, so that oxygen and carbon dioxide can move (or
diffuse) between them. So, when you breathe in, air comes down the trachea and through the bronchi into the alveoli. This fresh air has lots of oxygen in it, and some of this oxygen will
travel across the walls of the alveoli into your bloodstream. Traveling in the opposite direction is
carbon dioxide, which crosses from the blood in the capillaries into the air in the alveoli and isthen breathed out. In this way, you bring in to your body the oxygen that you need to live, and
get rid of the waste product carbon dioxide.
Blood Supply
The lungs are very vascular organs, meaning they receive a very large blood supply. This is
because the pulmonary arteries, which supply the lungs, come directly from the right side of your heart. They carry blood which is low in oxygen and high in carbon dioxide into your lungs so
that the carbon dioxide can be blown off, and more oxygen can be absorbed into the
bloodstream. The newly oxygen-rich blood then travels back through the paired pulmonary veinsinto the left side of your heart. From there, it is pumped all around your body to supply oxygen
to cells and organs.
The Work of Breathing
The Pleurae
The lungs are covered by smooth membranes that we call pleurae. The pleurae have two layers, a
‘visceral’ layer which sticks closely to the outside surface of your lungs, and a ‘parietal’ layer
which lines the inside of your chest wall (ribcage). The pleurae are important because they helpyou breathe in and out smoothly, without any friction. They also make sure that when your
ribcage expands on breathing in, your lungs expand as well to fill the extra space.
The Diaphragm and Intercostal Muscles

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 5/13
When you breathe in (inspiration), your muscles need to work to fill your lungs with air. The
diaphragm, a large, sheet-like muscle which stretches across your chest under the ribcage, does
much of this work. At rest, it is shaped like a dome curving up into your chest. When you breathein, the diaphragm contracts and flattens out, expanding the space in your chest and drawing air
into your lungs. Other muscles, including the muscles between your ribs (the intercostal muscles)
also help by moving your ribcage in and out. Breathing out (expiration) does not normallyrequire your muscles to work. This is because your lungs are very elastic, and when your
muscles relax at the end of inspiration your lungs simply recoil back into their resting position,
pushing the air out as they go.
The Respiratory System and Ageing
The normal process of ageing is associated with a number of changes in both the structure andfunction of the respiratory system. These include:
• Enlargement of the alveoli. The air spaces get bigger and lose their elasticity, meaning
that there is less area for gases to be exchanged across. This change is sometimes referredto as ’senile emphysema’.
• The compliance (or springiness) of the chest wall decreases, so that it takes more effort to
breathe in and out.
• The strength of the respiratory muscles (the diaphragm and intercostal muscles)decreases. This change is closely connected to the general health of the person.
All of these changes mean that an older person might have more difficulty coping with increased
stress on their respiratory system, such as with an infection like pneumonia, than a younger
person would.
PREDISPOSING FACTORS

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 6/13
Risk factors for COPD include environmental exposures and host factors. The most important
risk factor for COPD is cigarette smoking. Other risk factors are pipe, cigar, and other types of
tobacco smoking. In addition, passive smoking contributes to respiratory symptoms and COPD.Smoking depresses the activity of scavenger cells and affects the respiratory tract’s ciliary
cleansing mechanism, which keeps breathing passages free of inhaled irritants, bacteria, and
other foreign matter. When smoking damages this cleansing mechanism, airflow is obstructedand air becomes trapped behind the obstruction. The alveoli greatly distend, diminished lung
capacity. Smoking also irritates the goblet cells and mucus glands, causing an increased
accumulation of mucus, which in turn produces more irritation, infection, and damage to thelung. In addition, carbon monoxide (a by product of smoking) combines with hemoglobin to
form carboxyhemoglobin. Hemoglobin that is bound by carboxyhemoglobin cannot carry
oxygen efficiently.
A host risk factor for COPD is a deficiency of alpha antitrypsin, an enzyme inhibitor that protects the lung parenchyma from injury. This deficiency predisposes young people to rapid
development of lobular emphysema, even if they do not smoke. Genetically susceptible people
are sensitive to environmental factors (eg. Smoking, air pollution, infectious agents, allergens)and eventually developed chronic obstructive symptoms. Carriers of this genetic defect must beidentified so that they can modify environmental risk factors to delay or prevent overt symptoms
of disease.
PATHOPHYSIOLOGY
In COPD, the airflow limitation is both progressive and associated with an abnormalinflammatory response of the lungs to noxious particles or gases. The inflammatory response
occurs throughout the airways, parenchyma, and pulmonary vasculature. Because of the chronic
inflammation and the body’s attempts to repair it, narrowing occurs in the small peripheral
airways. Over time, this injury-and-repair process causes scar tissue formation and narrowing of the airway lumen. Airflow obstruction may also be caused by parenchymal destruction, as is seen
with emphysema, a disease of the alveoli or gas exchange units.
In addition to inflammation, processes related to imbalances of proteinases and antiproteinases inthe lung may be responsible for airflow limitation. When activated by chronic inflammation,
proteiness and other substances may be released, damaging the parenchyma of the lung. The
parenchymal changes may occur as a consequence of inflammation or environmental or geneticfactors (eg. Alpha1-antitrypsin deficiency).
Early in the course of COPD, the inflammatory response causes pulmonary vasculature changes
that are characterized by thickening of the vessel wall. These changes may result from exposure
to cigarette smoke, use of tobacco products, and therelease of inflammatory medicators.
CHRONIC BRONCHITIS
Lung damage and inflammation in the large airways
results in chronic bronchitis. Chronic bronchitis is

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 7/13
defined in clinical terms as a cough with sputum production on most days for 3 months of a year,
for 2 consecutive years. In the airways of the lung, the hallmark of chronic bronchitris is an
increased number (hyperplasia) and increased size (hypertrophy) of the goblet cells and mucousglands of the airway. As a result, there is more mucus than usual in the airways, contributing to
narrowing of the airways and causing a cough with sputum. Microscopically there is infiltration
of the airway walls with inflammatory cells. Inflammation is followed by scarring andremodeling that thickens the walls and also results in narrowing of the airways. As chronic
bronchitis progresses, there is squamous metaplasia (an abnormal change in the tissue lining the
inside of the airway) and fibrosis (further thickening and scarring of the airway wall). Theconsequence of these changes is a limitation of airflow.
Patients with advanced COPD that have primarily chronic bronchitis rather than emphysema
were commonly referred to as “blue bloaters” because of the bluish color of the skin and lips
(cyanosis) seen in them. The hypoxia and fluid retention leads to them being called “BlueBloaters.”
ACUTE BRONCHITIS
PHYSICAL MANIFESTATIONS
One of the most common symptoms of COPD is shortness of breath (dyspnea). People with
COPD commonly describe this as: “My breathing requires effort”, “I feel out of breath”, or “Ican not get enough air in”. People with COPD typically first notice dyspnea during vigorous
exercise when the demands on the lungs are greatest. Over the years, dyspnea tends to get
gradually worse so that it can occur during milder, everyday activities such as housework. In the
advanced stages of COPD, dyspnea can become so bad that it occurs during rest and isconstantly present. Other symptoms of COPD are a persistent cough, sputum or mucus
production, wheezing, chest tightness, and tiredness. People with advanced (very severe) COPDsometimes develop respiratory failure. When this happens, cyanosis, a bluish discoloration of thelips caused by a lack of oxygen in the blood, can occur. An excess of carbon dioxide in the blood
can cause headaches, drowsiness or twitching (asterixis). A complication of advanced COPD is
cor pulmonale, a strain on the heart due to the extra work required by the heart to pump bloodthrough the affected lungs. Symptoms of cor pulmonale are peripheral edema, seen as swelling of
the ankles, and dyspnea.
There are a few signs of COPD that a healthcare worker may detect although they can be seen in
other diseases. Some people have COPD and have none of these signs. Common signs are:
•
tachypnea, a rapid breathing rate• wheezing sounds or crackles in the lungs heard through a stethoscope
• breathing out taking a longer time than breathing in
• enlargement of the chest, particularly the front-to-back distance (hyperinflation)
• active use of muscles in the neck to help with breathing
• breathing through pursed lips increased anteroposterior to lateral ratio of the chest (i.e.
barrel chest).

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 8/13
EMPHYSEMA
Emphysema is a chronic obstructive pulmonary
disease (COPD, as it is otherwise known, formerlytermed a chronic obstructive lung disease). It is often
caused by exposure to toxic chemicals, including long-
term exposure to tobacco smoke. Emphysema ischaracterized by loss of elasticity (increased pulmonary
compliance) of the lung tissue caused by destruction of
structures feeding the alveoli, owing to the action of
alpha 1 antitrypsin deficiency. This causes the smallairways to collapse during forced exhalation, as
alveolar collapsibility has decreased. As a result, airflow is impeded and air becomes trapped in
the lungs, in the same way as other obstructive lung diseases. Symptoms include shortness of
breath on exertion, and an expanded chest. However, the constriction of air passages isn’t alwaysimmediately deadly, and treatment is available.
PHYSICAL MANIFESTATIONS
Signs of emphysema include pursed-lipped breathing, central cyanosis and finger clubbing. Thechest has hyper resonant percussion notes, particularly just above the liver, and a difficult to
palpate apex beat, both due to hyperinflation. There may be decreased breath sounds and audible
expiratory wheeze. In advanced disease, there are signs of fluid overload such as pitting
peripheral edema. The face has a ruddy complexion if there is a secondary polycythemia.Sufferers who retain carbon dioxide have asterixis (metabolic flap) at the wrist.
DIAGNOSTIC EVALUATION
1. PFTs demonstrative airflow obstruction – reduced forced vital capacity (FVC), FEV1,
FEV1 to FVC ration; increased residual volume to total lung capacity (TLC) ratio, possibly increased TLC.
2. ABG levels- decreased PaO2, pH, and increased CO2.
3. Chest X-ray – in late stages, hyperinflation, flattened diaphragm, increased rettrosternalspace, decreased vascular markings, possible bullae.
4. Alpa1-antitrypsin assay useful in identifying genetically determined deficiency in
emphysema.
TREATMENT
The goals of COPD treatment are 1) to prevent further deterioration in lung function, 2) toalleviate symptoms, 3) to improve performance of daily activities and quality of life. The
treatment strategies include 1) quitting cigarette smoking, 2) taking medications to dilate airways
(bronchodilators) and decrease airway inflammation, 3) vaccinating against flu influenza and pneumonia and 4) regular oxygen supplementation and 5) pulmonary rehabilitation.

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 9/13
Quitting cigarette smoking
The most important treatment for COPD is quitting cigarette smoking. Patients who continue to
smoke have a more rapid deterioration in lung function when compared to others who quit.Aging itself can cause a very slow decline in lung function. In susceptible individuals, cigarette
smoking can result in a much more dramatic loss of lung function. It is important to note thatwhen one stops smoking the decline in lung function eventually reverts to that of a non-smoker.
Nicotine in cigarettes is addictive, and, therefore, cessation of smoking can cause symptoms of nicotine withdrawal including anxiety, irritability, anger, depression, fatigue, difficulty
concentrating or sleeping, and intense craving for cigarettes. Patients likely to develop
withdrawal symptoms typically smoke more than 20 cigarettes a day, need to smoke shortly after
waking up in the morning, and have difficulty refraining from smoking in non-smoking areas.However, some 25% of smokers can stop smoking without developing these symptoms. Even in
those smokers who develop symptoms of withdrawal, the symptoms will decrease after several
weeks of abstinence.
Bronchodilators
Treating airway obstruction in COPD with bronchodilators is similar but not identical to treating
bronchospasm in asthma. Bronchodilators are medications that relax the muscles surrounding the
small airways thereby opening the airways. Bronchodilators can be inhaled, taken orally or administered intravenously. Inhaled bronchodilators are popular because they go directly to the
airways where they work. As compared with bronchodilators given orally, less medication
reaches the rest of the body, and, therefore, there are fewer side effects.
Metered dose inhalers (MDIs) are used to deliver bronchodilators. An MDI is a pressurized
canister containing a medication that is released when the canister is compressed. A standardamount of medication is released with each compression of the MDI. To maximize the delivery
of the medications to the airways, the patient has to learn to coordinate inhalation with eachcompression. Incorrect use of the MDI can lead to deposition of much of the medication on the
tongue and the back of the throat instead of on the airways.
To decrease the deposition of medications on the throat and increase the amount reaching the
airways, spacers can be helpful. Spacers are tube-like chambers attached to the outlet of the MDIcanister. Spacer devices can hold the released medications long enough for patients to inhale
them slowly and deeply into the lungs. Proper use of spacer devices can greatly increase the
proportion of medication reaching the airways.
Oxygen Therapy
Other treatments
• Pulmonary rehabilitation has become a cornerstone in the management of moderate to severe COPD. Pulmonary rehabilitation is a program of education regarding lung
function and dysfunction, proper breathing techniques (diaphragmatic breathing, pursed

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 10/13
lip breathing), and proper use of respiratory equipment and medications. An essential
ingredient in this program is the use of increasing physical exercise to overcome the
reduced physical capacity that usually has developed over time. In addition, occupationaland physical therapy are used to teach optimal and efficient body mechanics.
• Lung volume reduction surgery (LVRS) has received much fanfare in the lay press.
LVRS is a surgical procedure used to treat some patients with COPD. The premise behind this surgery is that the over-inflated, poorly-functioning upper parts of the lung
compress and impair function of the better-functioning lung elsewhere. Thus, if the over-
inflated portions of lung are removed surgically, the compressed lung may expand andfunction better. In addition, the diaphragm and the chest cavity achieve more optimal
positioning following the surgery, and this improves breathing further. The best criteria
for choosing patients for LVRS are still uncertain. A national study was completed in
2003. Patients primarily with emphysema at the top of their lungs, whose exercisetolerance was low even after pulmonary rehabilitation, seemed to do the best with this
procedure. On average, lung function and exercise capacity among surviving surgical
patients improved significantly following LVRS, but after two years returned to about the
same levels as before the procedure. Patients with forced expiratory volume in FEVI of less than 20% of predicted and either diffuse disease on the CAT scan or lower than 20%
diffusing capacity or elevated carbon dioxide levels had higher mortality. The role of LVRS is at present is very limited.
PHARMACOLOGIC INTERVENTIONS
• Beta-agonists
o Beta-2 agonists have the bronchodilating effects of adrenaline without many of its
unwanted side effects. Beta-2 agonists can be administered by MDI inhalers or orally. They are called “agonists” because they activate the beta-2 receptor on the
muscles surrounding the airways. Activation of beta-2 receptors relaxes themuscles surrounding the airways and opens the airways. Dilating airways helps torelieve the symptoms of dyspnea (shortness of breath). Beta-2 agonists have been
shown to relieve dyspnea in many COPD patients, even among those without
demonstrable reversibility in airway obstruction. The action of beta-2 agonistsstarts within minutes after inhalation and lasts for about 4 hours. Because of their
quick onset of action, beta-2 agonists are especially helpful for patients who are
acutely short of breath. Because of their short duration of action, thesemedications should be used for symptoms as they develop rather than as
maintenance. Evidence suggests that when these drugs are used routinely, their
effectiveness is diminished. These are referred to as rescue inhalers. Examples of
beta-2 agonists include albuterol (Ventolin, Proventil), metaproterenol (Alupent), pirbuterol (Maxair), terbutaline (Brethaire), and isoetharine (Bronkosol).
Levalbuterol (Xopenex) is a recently approved Beta-2 agonist.
o In contrast, Beta-2 agonists with a slower onset of action but a longer period of
activity, such as salmeterol xinafoate (Serevent) and formoterol fumarate
(Foradil) may be used routinely as maintenance medications. These drugs last
twelve hours and should be taken twice daily and no more. Along with some of these inhalers to be mentioned, these are often referred to as maintenance inhalers.

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 11/13
o Side effects of beta-2 agonists include anxiety, tremor, palpitations or fast heart
rate, and low blood potassium.
• Anti-cholinergic Agents
o Acetylcholine is a chemical released by nerves that attaches to receptors on the
muscles surrounding the airway causing the muscles to contract and the airways
to narrow. Anti-cholinergic drugs such as ipratropium bromide (Atrovent) dilateairways by blocking the receptors for acetylcholine on the muscles of the airways
and preventing them from narrowing. Ipratropium bromide (Atrovent) usually is
administered via a MDI. In patients with COPD, ipratropium has been shown toalleviate dyspnea, improve exercise tolerance and improve FEV1. Ipratropium has
a slower onset of action but longer duration of action than the shorter-acting beta-
2 agonists. Ipratropium usually is well tolerated with minimal side effects evenwhen used in higher doses. Tiotropium (SPIRIVA) is a long acting and more
powerful version of Ipratropium and has been shown to be more effective.
o In comparing ipratropium with beta-2 agonists in the treatment of patients with
COPD, studies suggest that ipratropium may be more effective in dilating airways
and improving symptoms with fewer side effects. Ipratropium is especiallysuitable for use by elderly patients who may have difficulty with fast heart rate
and tremor from the beta-2 agonists. In patients who respond poorly to either beta-2 agonists or ipratropium alone, a combination of the two drugs sometimes
results in a better response than to either drug alone without additional side
effects.
• Methylxanthines
o Theophylline (Theo-Dur, Theolair, Slo-Bid, Uniphyl, Theo-24) and
aminophylline are examples of methylxanthines. Methylxanthines areadministered orally or intravenously. Long acting theophylline preparations can
be given orally once or twice a day. Theophylline, like a beta agonist, relaxes the
muscles surrounding the airways but also prevents mast cells around the airwaysfrom releasing bronchoconstricting chemicals such as histamine. Theophyllinealso can act as a mild diuretic and increase urination. Theophylline also may
increase the force of contraction of the heart and lower pressure in the pulmonary
arteries. Thus, theophylline can help patients with COPD who have heart failureand pulmonary hypertension. Patients who have difficulty using inhaled
bronchodilators but no difficulty taking oral medications find theophylline
particularly useful.o The disadvantage of methylxanthines is their side effects. Dosage and blood
levels of theophylline or aminophylline have to be closely monitored. Excessively
high levels in the blood can lead to nausea, vomiting, heart rhythm problems, and
even seizures. In patients with heart failure or cirrhosis, dosages of methylxanthines are lowered to avoid high blood levels. Interactions with other
medications, such as cimetidine (Tagamet), calcium channel blockers (Procardia),
quinolones (Cipro), and allopurinol (Zyloprim) also can alter blood levels of methylxanthines.
• Corticosteroids
o When airway inflammation (which causes swelling) contributes to airflow
obstruction, anti-inflammatory medications (more specifically, corticosteroids)

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 12/13
may be beneficial. Examples of corticosteroids include Prednisone and
Prednisolone. Twenty to thirty percent of patients with COPD show improvement
in lung function when given corticosteroids by mouth. Unfortunately, high dosesof oral corticosteroids over prolonged periods can have serious side effects,
including osteoporosis, bone fractures, diabetes mellitus, high blood pressure,
thinning of the skin and easy bruising, insomnia, emotional changes, and weightgain. Therefore, many doctors use oral corticosteroids as the treatment of last
resort. When oral corticosteroids are used, they are prescribed at the lowest
possible doses for the shortest period of time to minimize side effects. When it isnecessary to use long term oral steroids, medications are often prescribed to help
reduce the development of the above side effects.
o Corticosteroids also can be inhaled. Inhaled corticosteroids have many fewer side
effects than long term oral corticosteroids. Examples of inhaled corticosteroidsinclude beclomethasone dipropionate (Beclovent, Beconase, Vancenase, and
Vanceril), triamcinolone acetonide (Azmacort), fluticasone (Flovent), budesonide
(Pulmicort), mometasone furoate (Asmanex) and flunisolide (Aerobid). Inhaled
corticosteroids have been useful in treating patients with asthma, but in patientswith COPD, it is not clear whether inhaled corticosteroid have the same benefit as
oral corticosteroids. Nevertheless, doctors are less concerned about using inhaledcorticosteroids because of their safety. The side effects of inhaled corticosteroids
include hoarseness, loss of voice, and oral yeast infections. A spacing device
placed between the mouth and the MDI can improve medication delivery andreduce the side effects on the mouth and throat. Rinsing out the mouth after use of
a steroid inhaler also can decrease these side effects.
• Treatment of Alpha-1 antitrypsin deficiency
o Emphysema can develop at a very young age in some patients with severe alpha-1
antitrypsin deficiency (AAT). Replacement of the missing or inactive AAT by
injection can help prevent progression of the associated emphysema. This therapyis of no benefit in other types of COPD.
COMPLICATIONS
1. Respiratory failure
2. Pneumonia, overwhelming respiratory infection
3. Right-sided heart failure, dysrhythmias4. Depression
5. Skeletal muscle dysfunction
NURSING INTERVENTIONS
Monitoring
1. Monitor for adverse effects of bronchodilators – tremulousness, tachycardia, cardiacarrhythmias, central nervous system stimulation, hypertension.
2. Monitor condition after administration of aerosol bronchodilators to assess for improved
aeration, reduced adventitious sounds, reduced dyspnea.

8/8/2019 Copd Case Pres
http://slidepdf.com/reader/full/copd-case-pres 13/13
3. Monitor serum theophylline level, as ordered, to ensure therapeutic level and prevent
toxicity.
4. Monitor oxygen saturation at rest and with activity.
Supportive Care
1. Eliminate all pulmonary irritants, particularly cigarette smoke. Smoking cessation usually
reduces pulmonary irritation, sputum production, and cough. Keep the patient’s room as
dust-free as possible.2. Use postural drainage positions to help clear secretions responsible for airway
obstructions.
3. Teach controlled coughing.
4. Encourage high level of fluid intake ( 8 to 10 glasses; 2 to 2.5 liters daily) within level of cardiac reserve.
5. Give inhalations of nebulized saline to humidify bronchial tree and liquefy sputum. Add
moisture (humidifier, vaporizer) to indoor air.
6. Avoid dairy products if these increases sputum production. 7. Encourage the patient to assume comfortable position to decrease dyspnea.
8. Instruct and supervise patient’s breathing retraining exercises. 9. Use pursed lip breathing at intervals and during periods of dyspnea to control rate and
depth of respiration and improve respiratory muscle coordination.
10. Discuss and demonstrate relaxation exercises to reduce stress, tension, and anxiety. 11. Maintain the patient’s nutritional status.
12. Reemphasize the importance of graded exercise and physical conditioning programs.
13. Encourage use of portable oxygen system for ambulation for patients with hypoxemia
and marked disability.14. Train the patient in energy conservation technique.
15. Assess the patient for reactive-behaviors such as anger, depression and acceptance.
Education and health maintenance
1. Review with the patient the objectives of treatment and nursing management. 2. Advise the patient to avoid respiratory irritants. Suggest that high efficiency particulate
air filter may have some benefit.
3. Warn patient to stay out of extremely hot or cold weather and to avoid aggravating bronchial obstruction and sputum obstruction.
4. Warn patient to avoid persons with respiratory infections, and to avoid crowds and areas
with poor ventilation.
5. Teach the patient how to recognize and report evidence of respiratory infection promptlysuch as chest pain, changes in character of sputum (amount, color and consistency),
increasing difficulty in raising sputum, increasing coughing and wheezing, increasing of
shortness of breath.