Embed Size (px)
Citation preview

E-Mail [email protected]
Cochrane Review Update
Neonatology 2013;104:260–262 DOI: 10.1159/000353681
Cooling for Newborns with Hypoxic Ischemic Encephalopathy
adverse effects of cooling and ‘early’ indicators of neurode-velopmental outcome. Data Collection and Analysis: Four review authors independently selected, assessed the quality of and extracted data from the included studies. Study au-thors were contacted for further information. Meta-analyses were performed using risk ratios (RR) and risk differences (RD) for dichotomous data, and weighted mean difference for continuous data with 95% confidence intervals (CI). Main
Results: We included 11 randomized controlled trials in this updated review, comprising 1,505 term and late preterm in-fants with moderate/severe encephalopathy and evidence of intrapartum asphyxia. Therapeutic hypothermia resulted in a statistically significant and clinically important reduction in the combined outcome of mortality or major neurodevel-opmental disability to 18 months of age (typical RR 0.75 (95% CI 0.68–0.83); typical RD –0.15, 95% CI –0.20 to –0.10); num-ber needed to treat for an additional beneficial outcome (NNTB) 7 (95% CI 5–10) (8 studies, 1,344 infants). Cooling also resulted in statistically significant reductions in mortality (typical RR 0.75 (95% CI 0.64–0.88), typical RD –0.09 (95% CI –0.13 to –0.04); NNTB 11 (95% CI 8–25) (11 studies, 1,468 in-fants) and in neurodevelopmental disability in survivors (typical RR 0.77 (95% CI 0.63–0.94), typical RD –0.13 (95% CI –0.19 to –0.07); NNTB 8 (95% CI 5–14) (8 studies, 917 infants). Some adverse effects of hypothermia included an increase sinus bradycardia and a significant increase in thrombocyto-penia.
Cochrane Abstract
Background: Newborn animal studies and pilot studies in humans suggest that mild hypothermia following peripar-tum hypoxia-ischemia in newborn infants may reduce neu-rological sequelae without adverse effects. Objectives: To determine the effect of therapeutic hypothermia in enceph-alopathic asphyxiated newborn infants on mortality, long-term neurodevelopmental disability and clinically important side effects. Search Methods: We used the standard search strategy of the Cochrane Neonatal Review Group as outlined in The Cochrane Library (Issue 2, 2007). Randomized con-trolled trials evaluating therapeutic hypothermia in term and late preterm newborns with hypoxic ischemic encepha-lopathy were identified by searching the Oxford Database of Perinatal Trials, the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, 2007, Issue 2), MED-LINE (1966 to June 2007), previous reviews including cross-references, abstracts, conferences, symposia proceedings, expert informants and journal handsearching. We updated this search in May 2012. Selection Criteria: We included ran-domized controlled trials comparing the use of therapeutic hypothermia with standard care in encephalopathic term or late preterm infants with evidence of peripartum asphyxia and without recognizable major congenital anomalies. The primary outcome measure was death or long-term major neurodevelopmental disability. Other outcomes included
Published online: September 21, 2013
© 2013 S. Karger AG, Basel 1661–7800/13/1044–0260$38.00/0
www.karger.com/neo
Dow
nloa
ded
by:
Cle
mso
n U
nive
rsity
13
0.12
7.23
8.23
3 -
9/28
/201
3 4:
48:5
9 P
M

Cochrane Review Update Neonatology 2013;104:260–262DOI: 10.1159/000353681
261
Reviewers’ Conclusions
There is evidence from the 11 randomized controlled tri-als included in this systematic review (n = 1,505 infants) that therapeutic hypothermia is beneficial in term and late pre-term newborns with hypoxic ischemic encephalopathy. Cool - ing reduces mortality without increasing major disability in survivors. The benefits of cooling on survival and neurode-velopment outweigh the short-term adverse effects. Hypo-thermia should be instituted in term and late preterm infants with moderate-to-severe hypoxic ischemic encephalopathy if identified before 6 h of age. Further trials to determine the appropriate techniques of cooling, including refinement of patient selection, duration of cooling and method of provid-ing therapeutic hypothermia, will refine our understanding of this intervention.
Jacobs SE, Berg M, Hunt R, Tarnow-Mordi WO, Inder TE, Davis PG:
Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database of Systematic Reviews 2013, Issue 1. Art. No.: CD003311. DOI: 10.1002/14651858.CD003311.pub3.
Commentary
Roger F. Soll, Burlington, Vt.
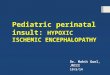
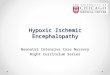
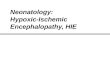
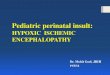
The updated review of Jacobs et al. [1] provides further convincing evidence of the efficacy of moderate thera-peutic hypothermia (33–34 ° C) for term and late preterm infants with moderate or severe hypoxic ischemic en-cephalopathy (HIE). Therapeutic hypothermia results in both a statistically significant and clinically important re-duction in mortality or major neurodevelopmental dis-ability ( fig. 1 , 2 ). The number needed to treat suggests that for every 7 infants with moderate to severe HIE we treat, 1 will benefit by surviving without developmental disabil-ity.
The addition of several more studies allows insight into interesting secondary outcomes. Short-term adverse effects of hypothermia include an increase in sinus bra-dycardia and a significant increase in thrombocytopenia. There also appears to be more persistent pulmonary hy-pertension than clinicians were previously aware of. However, the benefits of cooling on survival and neuro-development far outweigh these short-term adverse events.
In the current update, Jacobs et al. report a significant decrease in the risk of MRI abnormalities in infants who received cooling (typical RR 0.73, 95% CI 0.60–0.89).
These MRI abnormalities are highly predictive of poor developmental outcome and may be an important bio-marker as we try to further define treatment strategies for cerebral protection with hypothermia [2] .
Practice regarding therapeutic hypothermia varies greatly from the practices defined in the clinical trials (for example, gestation 35 weeks upwards, cooling to 33–34 ° C for 72 h starting within 6 h of birth). In preliminary results from the Vermont Oxford Network Neonatal En-cephalopathy Registry, only 57% of the 2,457 cooled in-fants met the key eligibility criteria used in the random-ized trials. In those infants who did not meet key eligibil-ity criteria, 40% were cooled that did not have moderate or severe encephalopathy or seizures prior to cooling, 17% were <36 weeks’ gestation and 60% had hypothermic therapy initiated after 6 h from birth [3] . Although the results regarding cooling are quite promising, it is some-what disconcerting to see the diffusion of this technology without adequate study in these related groups of infants.
Acknowledgment
Editorial support of the Cochrane Neonatal Review Group has been funded with Federal Funds from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Na-tional Institutes of Health, Department of Health, USA, under Contract No. HHSN275201100016C.
References
1 Jacobs SE, Berg M, Hunt R, Tarnow-Mordi WO, Inder TE, Davis PG: Cooling for newborns with hypoxic ischaemic encephalopathy. Co-chrane Database Syst Rev 2013, Issue 1. Art. No.: CD003311. DOI: 0.1002/14651858.CD003311.pub3.
2 Rutherford M, Ramenghi LA, Edwards AD, Brocklehurst P, Halliday H, Levene M, Strohm S, Thoresen M, Whitelaw A, Azzopardi D: Assess-ment of brain tissue injury after moderate hypothermia in neonates with hypoxic-ischaemic encephalopathy: a nested substudy of a randomised controlled trial. Lancet Neurol 2010; 9: 39–45. DOI: 10.1016/S1474-4422(09)70295-9.
3 Pfister RH, Edwards EE, Soll RF, Bingham P, Inder TE, Nelson KB, Raju TNK, Horbar JD: Do infants treated with hypothermic therapy in routine practice meet the eligibility criteria from the original randomized trials? Platform Session: Neonatal Hypoxic Ischemic Encephalopathy & Neu-roprotection. Washington, PAS, 2013.
Dow
nloa
ded
by:
Cle
mso
n U
nive
rsity
13
0.12
7.23
8.23
3 -
9/28
/201
3 4:
48:5
9 P
M

Cochrane Review Update
Neonatology 2013;104:260–262DOI: 10.1159/000353681
262
Study or subgroup Hypothermia Standard care Weight, %
Risk ratioM-H, fixed (95% CI)
Risk ratioM-H, fixed, 95% CI
even ts total events total
1.1.1 Selective head cooling with mild systemic hypothermia Gunn, 1998 7 18 4 13 1.1 1.26 (0.46, 3.44) Cool Cap Study, 2005 59 108 73 110 17.6 0.82 (0.66, 1.02) Zhou, 2010 31 100 46 94 11.5 0.63 (0.44, 0.91) Subtotal (95% CI) 226 217 30.3 0.77 (0.64, 0.92) Total events 97 123 Heterogeneity: χ 2 = 2.46, d.f. = 2 (p = 0.29), I 2 = 19% Test for overall effect: Z = 2.78 (p = 0.005)
1.1.2 Whole body cooling Eicher, 2005 14 27 21 25 5.3 0.62 (0.41, 0.92) NICHD Study, 2005 45 102 64 103 15.5 0.71 (0.54, 0.93) TOBY Study, 2009 74 163 86 162 21.0 0.86 (0.68, 1.07) neo.nEURO Study, 2010 27 53 48 58 11.2 0.62 (0.46, 0.82) ICE Study, 2011 55 107 67 101 16.8 0.77 (0.62, 0.98) Subtotal (95% CI) 452 449 69.7 0.75 (0.66, 0.84) Total events 215 286 Heterogeneity: χ 2 = 4.25, d.f. = 4 (p = 0.37), I 2 = 6% Test for overall effect: Z = 4.80 (p < 0.00001)
Total (95% CI) 678 666 100.0 0.75 (0.68, 0.83) Total events 312 409 Heterogeneity: χ 2 = 6.89, d.f. = 7 (p = 0.44), I 2 = 0% Test for overall effect: Z = 5.53 (p < 0.00001) Test for subgroup differences: χ 2 = 0.06, d.f. = 1 (p = 0.81), I 2 = 0%
0.2 0.5 1 2Favors
hypothermiaFavors
standard care
5
Fig. 1. Therapeutic hypothermia versus standard care. Effect on death or disability in survivors assessed (by method of cooling).
Study or subgroup Hypothermia Standard care Weight, %
Risk ratioM-H, fixed (95% CI)
Risk ratioM-H, fixed, 95% CI events total events to tal
1.2.1 Selective head cooling with mild systemic hypothermia Gunn, 1998 3 18 3 13 1.4 0.72 (0.17, 3.03) Akisu, 2003 0 11 2 10 1.0 0.18 (0.01, 3.41) Cool Cap Study, 2005 36 108 42 110 16.7 0.87 (0.61, 1.25) Lin, 2006 2 32 2 30 0.8 0.94 (0.14, 6.24) Zhou, 2010 20 100 27 94 11.2 0.70 (0.42, 1.15) Subtotal (95% CI) 269 257 31.1 0.78 (0.59, 1.04) Total events 61 76 Heterogeneity: χ 2 = 1.56, d.f. = 4 (p = 0.82), I 2 = 0% Test for overall effect: Z = 1.72 (p = 0.09)
1.2.2 Whole body cooling Shankaran, 2002 2 9 3 10 1.1 0.74 (0.16, 3.48) Eicher, 2005 10 32 14 33 5.5 0.74 (0.38, 1.41) NICHD Study, 2005 24 102 38 103 15.2 0.64 (0.41, 0.98) TOBY Study, 2009 42 163 44 162 17.7 0.95 (0.66, 1.36) neo.nEURO Study, 2010 20 53 33 58 12.6 0.66 (0.44, 1.00) ICE Study, 2011 27 108 42 109 16.8 0.65 (0.43, 0.97) Subtotal (95% CI) 467 475 68.9 0.73 (0.61, 0.89) Total events 125 174 Heterogeneity: χ 2 = 2.92, d.f. = 5 (p = 0.71), I 2 = 0% Test for overall effect: Z = 3.18 (p = 0.001)
Total (95% CI) 736 732 100.0 0.75 (0.64, 0.88) Total events 186 250 Heterogeneity: χ 2 = 4.72, d.f. = 10 (p = 0.91), I 2 = 0% Test for overall effect: Z = 3.59 (p = 0.0003) Test for subgroup differences: χ 2 = 0.13, d.f. = 1 (p = 0.72), I 2 = 0%
0.01 0.1 1 10Favors
hypothermiaFavors
standard care
100
Fig. 2. Therapeutic hypothermia versus standard care. Effect on death (by method of cooling).
Dow
nloa
ded
by:
Cle
mso
n U
nive
rsity
13
0.12
7.23
8.23
3 -
9/28
/201
3 4:
48:5
9 P
M