Embed Size (px)
Citation preview

COOL RCNA Prospective, Randomized Trial
Examining the Safety and Efficacy of Systemic Hypothermia for the Prevention
of Radiocontrast Nephropathy
Gregg W. Stone, MDColumbia University Medical Center
The Cardiovascular Research Foundation

Background• Contrast induced renal insufficiency after
invasive cardiology procedures has been strongly associated with early and late mortality
• Preclinical and pilot studies have suggested that systemic hypothermia can ameliorate or prevent radiocontrast nephropathy (RCN)
• We therefore performed a prospective, randomized trial to determine the utility of systemic hypothermia in pts receiving iodinated contrast

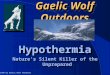
Prevention of Experimental Contrast-Induced Nephropathy with Hypothermia, Fenoldopam, N-
Acetylcysteine, and Bicarbonate
Serum Creatinine(mg/dl)
Baseline24 hr48 hr
Normo-thermia
39ºC, N=6
BicarbN=6
Fenold-opamN=6
NACN=6
37ºCN=5
35ºCN=5
32ºCN=6
0.0
1.0
2.0
3.0
4.0
5.0
6.0
Dae MW et al. JACC 2004;43:48A
Rabbit modelN=40
Control
Hypothermia

The COOL RCN Pilot
• 30 pts (median age 71, 50% diabetes) with estimated CrCl 20 – 50 mL/min (mean 35.2 ± 8.9) were hydrated and cooled to 33 – 34ºC >90 mins prior to and for 3 hrs after contrast
• Mean 150 ± 65 [range 49-320] mL contrast used during angiography (60%) or PCI (40%)
• SCr measured at 24, 48 and 72 - 96 hrs• RCN (SCr ↑>25% from baseline) developed in
3 pts (10%), vs. 40% predicted
Stone GW. TCT2006

Pts at risk for RCN (CrCl 20-50 mL/min)Undergoing diagnostic and/or interventional cath with >50 cc dye
N = 400 pts at up to 35 sites
Hypothermia (33-34°C)Pre contrast and 3 hrs post
+Hydration (NaCl & NaHCO3 )
COOL RCNRandomized Trial
SCr measured at 24, 48 and 72-96 hrs* (core lab)1º efficacy endpoint = RCN (SCr ↑>25% from baseline)
1º safety endpoint = 30d AE (death, MI, dialysis, VF, venous compl requiring surgery, bleed requiring ≥2U transf., rehosp.)
ControlHydration (NaCl & NaHCO3 )
R
*Pts w/SCr ↑25% or ≥0.5 mg/dL at day 3 had an additional blood draw between day 7 – 10

Key Exclusion Criteria• Unstable renal function, acute renal failure or dialysis• Renal artery angiography, renal drug infusion, or known RAS• Receiving mannitol or IV diuretics• Decompensated HF, intubated, or hypotension (SBP <100)• STEMI within 72 hours• Severe allergy (contrast, heparin, meperidine, buspirone) or recent MAOI• Additional contrast within 10 days pre or post procedure• IVC filter, or height < 4’ 11”• Hypersensitivity to hypothermia (Raynaud’s), bleeding
diathesis, coagulopathy, sickle cell disease, severe hepatic impairment, cryoglobulinemia, untreated hypoth, Addison’s, BPH or urethral stricture, or will refuse blood transfusions

Reprieve® System
Heparin / hydrogelcoated PET balloon
12 Fr venous catheter with a 25 cm heat exchange balloon

Cooling Procedures
• Cooling must be achieved before 1st contrast• Target core temp 33ºC; no contrast before 34ºC• Shivering suppression protocol (45-60’ pre
cool):o Buspirone 60 mg poo Meperidine 50 mg slow IV bolus; 15’ later 25-50
mg slow IV bolus; 15’ later start 25-35 mg/hr IV infusion
o Surface forced air warming blanket (at high)• Rewarming initiated 3 hours post procedure
towards a target of 36ºC at a rate of 1°C/hr

Study procedures
• IV Hydrationo 2-12 hrs pre cath: NS 1.5 cc/kg/hr (1.0 cc/kg/hr
of ½ NS for pts with CHF or LV dysfunction)o 1 hr pre cath: Stop NS, start NaHCO3 (150 mEq
in 1 L D5W): bolus of 0.45mEq/kg (3mL/kg/hr) for the first hour, then 0.15 mEq/kg/hr (1 mL/kg/hr) during the cath and for 5-7 hrs post procedure
• N-acetylcysteine was allowed per PI discretion• Low osmolar contrast only; iodixanol
preferred

Power Analysis
• Primary efficacy endpointo RCN, defined as a relative SCr ↑ >25% from
baseline anytime within 96 hrs)o Assumed RCN rates: 35% control, 21% Rx
(40% treatment effect)o Randomizing 358 pts provided 80% power
(α=0.05) → 400 pts randomized to allow 10% lost to FU, inadequate samples or study procedures

Study Organization• Principal Investigator: Gregg W. Stone• Data Management: Harvard Clinical Research Institute
(HCRI)• Site and Data Monitoring: Radiant Medical• Clinical Events Committee: HCRI (Don Cutlip, chair)• Biochem Core Lab: ACM Medical Laboratory• DSMB: Julian Aroesty, Chair; J. Lopez; F. Ling; J. Orav• Sponsor: Radiant Medical (subsequently assumed by
ZOLL Circulation)

Top Enrolling SitesSite Principal
Investigator
Owensboro Hospital, Owensboro, KY Kishor Vora
UPMC Presbyterian, Pittsburgh, PA John Schindler
Methodist North Hospital, Memphis, TN Claro Diaz
Wake Med, Raleigh, NC Tiff Mann
Columbia University Medical Cntr, NY, NY George Dangas
Mayo Clinic, Rochester, Minnesota Patricia Best

70 pts normothermia
58 pts hypothermia
136 pts randomizedbetween March 2006 and August 2007
Study terminated early due to financial insolvency of Radiant;Radiant assets were purchased by ZOLL Circulation, who funded
completion of the study
136 pts randomized
128 pts evaluable
4 pts – Withdrawn prior to initiating study procedures*
Sites did not turn in CRFs – 4 pts
73 pts normothermia
63 pts hypothermia
*Pul edema (1); IV diuretics (1); polycythemia (1); pt withdrew (1)

Baseline FeaturesNormothermia
N=70Hypothermia
N=58P
value
Age (yrs) 72 ± 10 74 ± 10 0.45
Female 31.4% 48.3% 0.07
Diabetes 61.4% 32.8% <0.01
Hypertension 88.6% 91.4% 0.77
Dyslipidemia 91.4% 84.4% 0.27
Current smoking 26.3% 17.5% 0.47
Prior MI 36.2% 36.2% 1.00
Prior CABG 33.3% 29.3% 0.70
Prior PCI 48.6% 43.1% 0.59
Serum creatinine (mg/dL) 1.97 ± 0.8 1.78 ± 0.6 0.16
Creatinine clearance (mL/min) 36.2 ± 8.1 36.8 ± 8.8 0.70

Procedural SummaryNormothermia
N=70Hypothermia
N=58P
value
N-acetylcysteine administered 77.1% 62.1% 0.06
Pre hydration volume (mL) 799 ± 492 1,114 ± 1,556 0.12
Post hydration volume (mL) 854 ± 791 882 ± 760 0.84
Procedure type
Diagnostic 58.6% 51.7% 0.45
Interventional 41.4% 48.3% 0.45
Total contrast volume (mL) 138 ± 78.3 150 ± 94.3 0.44
Contrast type*
Non-ionic, iso-osmolar 75.4% 79.3% 0.60
Non-ionic, low osmolar 24.3% 24.1% 0.98
Temp. @ 1st contrast (ºC) 36.1 ± 0.7 33.6 ± 0.5 <0.001
* Some pts received 2 types of contrast during the index procedure

Cooling Efficiency
Baseline temp (ºC) 36.8 ± 8.8Time to 35ºC (mins): 6.2 ± 3.7Time to 34ºC (mins): 13.0 ± 5.5Time to 33ºC (mins): 29.4 ± 16.434ºC reached before contrast: 92.5%Meperidine dose (mg, mean) 245 ± 70Premature cooling cessation: 0%
Aggregate cooling data (N=50)
33.0
33.5
34.0
34.5
35.0
35.5
36.0
Time (min)
Patient Temperature (ºC)
0 10 20 30 40

Results
NormothermiaN=70
HypothermiaN=58
Pvalue
Serum creatinine (mg/dL)
- Baseline 1.97 ± 0.80(n=70)
1.78 ± 0.60(n=58)
0.16
- 24 hr 1.91 ± 0.77 (n=68)
1.77 ± 0.66 (n=58)
0.30
- 48 hr 2.21 ± 0.94 (n=58)
1.94 ± 0.73 (n=53)
0.09
- 72 – 96 hr 2.11 ± 0.87 (n=68)
1.92 ± 0.72 (n=56)
0.18

Development of RCN
Primary endpoint
OR [95%CI] =1.27 [0.53-3.00]
P=0.59
OR [95%CI] =0.83 [0.34-2.05]
P=0.69
OR [95%CI] =1.16 [0.51-2.67]
P=0.71

Randomization to HypothermiaMultivariate Analysis (16 variables)
Logistic regression adjusted for: age, gender, total contrast volume, renal medications, pre hydration time, post hydration time, pre hydration volume, post hydration volume, dyslipidemia, weight, baseline SCr and CrCl, cath vs.
PCI, and anemia (variables selected from Mehran RCN Risk Score)
Serum creatinine change Odds ratio[95% CI]*
Pvalue
Relative ↑ >25% 0.83 [0.18 - 3.78] 0.81
Absolute ↑ >0.5 mg/dL 0.57 [0.14 - 2.38] 0.44
Absolute or relative ↑ 0.90 [0.25 - 3.40] 0.87
*<1 → Hypothermia is protective

Adverse Events at 30 Days
NormothermiaN=70
HypothermiaN=58
Pvalue
Mortality, all cause 1.4% 5.2% 0.22
AMI 1.4% 3.4% 0.45
Dialysis 2.9% 0% 0.50
Ventricular fibrillation 0% 0% 1.0
Venous compl. → surgery 0% 0% 1.0
Bleeding → transf. ≥2U 12.9% 6.9% 0.26
Rehospitalization 18.6% 22.4% 0.59
Composite adverse events 37.1% 37.9% 0.93

• The observed rate of RCN in the control arm (18.6%) was lower than anticipated (35%)
• This fact, coupled with the enrollment of only 136 of a planned 400 pts (34%), resulted in a wide point estimate for the treatment effect of systemic hypothermia (odds 47% better to 200% worse)
Limitations

COOL RCNConclusions
• In pts at high risk for RCN undergoing invasive cardiology procedures hydrated with NS + NaHCO3, systemic hypothermia using the Reprieve® system:o May be safely achieved and is well toleratedo Does not result in a significant reduction in
RCN







![Therapeutic Hypothermia in Traumatic Brain Injurycdn.intechopen.com/pdfs/42406/InTech-Therapeutic... · 80 Therapeutic Hypothermia in Brain Injury hypothermia [13-50]. In addition,](https://img.pdfslide.us/doc/110x75/5e902d36c9c187069d5dbc10/therapeutic-hypothermia-in-traumatic-brain-80-therapeutic-hypothermia-in-brain-injury.jpg)