CLINICAL MANAGEMENT GUIDELINES
Entropion
Entropion Version 4 30.08.11
1 of 2 College of Optometrists
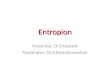
Aetiology Inward rotation of the tarsus and lid margin, causing
the lashes to come into contact with the ocular surface Most cases
have a single aetiology but in some are multi-factorial
Involutional (age-related) Most common cause of entropion, affects
lower lid Results from a combination of age related
degenerations
horizontal lid laxity resulting from thinning and atrophy of the
tarsus and the canthal tendons
weakness of the lower lid retractors
overriding of the preseptal over the pre-tarsal portion of the
orbicularis oculi muscle, at the lid margin. This causes inward
rotation of the tarsal plate on lid closure
Cicatricial Severe scarring and contraction of the palpebral
conjunctiva pulls the lid margin inwards (ocular cicatricial
pemphigoid, Steven-Johnson syndrome, trachoma, chemical burns)
Spastic Caused by spastic contraction of the orbicularis muscle
triggered by ocular irritation (including surgery) or due to
essential blepharospasm. Usually resolves spontaneously once the
cause has been removed Congenital Very rare entropion of the lower
lid due to improper attachment of the retractor muscles to the
inferior border of the tarsal plate
Predisposing factors Age-related degenerative changes in the lid
Severe cicatrising disease affecting the tarsal conjunctiva Ocular
irritation or previous surgery
Symptoms Foreign body sensation, irritation Red, watery eye
Blurring of vision
Signs Corneal and/or conjunctival epithelial disturbance from
abrasion by the lashes (wide range of severity) Localised
conjunctival hyperaemia Lid laxity (involutional entropion)
Conjunctival scarring (cicatricial entropion) Absence of lower lid
crease (congenital entropion)
Differential diagnosis Eyelid retraction (eg Graves disease):
retracted upper or lower lid causes the lashes to be hidden by
the
resulting fold of lid skin, resembling entropion
Distichiasis:
congenital additional row of lashes at the meibomian gland
orifices
Trichiasis:
lashes arise from normal position but are misdirected towards
the cornea, secondary to inflammation and scarring of the lash
follicles
Dermatochalasis:
degenerative condition, common in the elderly, leading to baggy
appearance due to redundant lid skin and protrusion of orbital fat.
Misdirection of lashes of upper lid may resemble entropion
Epiblepharon:
congenital condition in which a fold of skin and muscle extends
horizontally across the lid margin causing the lashes to be
CLINICAL MANAGEMENT GUIDELINES
Entropion
Entropion Version 4 30.08.11
2 of 2 College of Optometrists
directed vertically. Orientation of tarsal plate normal. Usually
asymptomatic and resolves with increasing age
Management by Optometrist Practitioners should recognise their
limitations and where necessary seek further advice or refer the
patient elsewhere Non pharmacological Taping the lid to the skin of
the cheek, so as to pull it away from the
globe, can give temporary relief (particularly for involutional
or spastic entropion) Epilation of lashes can be done where the
trichiasis is localised (eg in cicatricial entropion) Therapeutic
contact lens (hydrogel, silicone hydrogel, large diameter corneal
or scleral) to protect cornea from lashes
Pharmacological Ocular lubricants for tear
deficiency/instability related symptoms (drops for use during the
day, unmedicated ointment for use at bedtime) NB Patients on
long-term medication may develop sensitivity reactions which may be
to active ingredients or to preservative systems (see Clinical
Management Guideline on Conjunctivitis Medicamentosa). They should
be switched to unpreserved preparations
Management Category B1: Initial management (including drugs)
followed by routine referral Congenital entropion does not resolve
spontaneously and the potential for severe corneal complications
requires referral for prompt treatment
Possible management by Ophthalmologist
The choice of surgical procedure depends on the underlying
cause(s) Surgical intervention is indicated if any of the following
are persistent:
ocular irritation
recurrent bacterial conjunctivitis
reflex tear hypersecretion
superficial keratopathy
risk of ulceration and microbial keratitis
Evidence base
Authors conclusion: there are no randomised controlled trials to
support any intervention for lower lid entropion. Published case
series indicate that the combination of horizontal and vertical
lower lid shortening in the form of lateral canthal sling and Jones
retractor plication give the most favourable results. (The Oxford
2011 Levels of Evidence = 4)