Embed Size (px)
Citation preview

3108 (W0212) An independent licensee of the Blue Cross and Blue Shield Association.
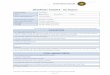
Conversion Request Form(one form per product change)
Group Name: _____________________________________________________________________________________
Group Number: ____________________________________
Effective Date: _____ / _____ / ________ Renewal Date (Internal Use Only): _____ / _____ / ________MM YYYY DD MMYYYY DD
Broker Name: _____________________________________ Vendor Number: _________________________________
If census is changing, please include enrollment forms for new employees and/or any contract changes forexisting members.
Please provide employee name and selected Primary Care Physician (if applicable).
PCP (if applicable) Current Subgroup # New Subgroup #Employee Name (J or K codes only) (Internal Use Only) (Internal Use Only)
* Please note that unless notified, all groups will be set up for one bill option.** Please submit quote with the Conversion Request Form.
Comments:
Group Signature: _________________________________________________________ Date: _____ / _____ / ________MM DD YYYY
Account Consultant Signature: ______________________________________________ Date: _____ / _____ / ________MM DD YYYY
You may complete the required fields below online and then save or print a copy for submission. To save a completed copy to your computer, choose File > Save As to rename the file and save the form with your information to your computer.


![DATED [dd/mm/yyyy] - assets.crowncommercial.gov.uk · RM1045 Network Services Framework Agreement PUBLISHED v3.0 20.02.2017 1 . DATED [dd/mm/yyyy] CROWN COMMERCIAL SERVICE . and [SUPPLIER](https://img.pdfslide.us/doc/110x75/5e03cd7d62ef2e7e4f32771a/dated-ddmmyyyy-rm1045-network-services-framework-agreement-published-v30.jpg)
![Exhibition Database chronology - Royal Ontario Museum · 9/5/2012 · Exhibition Database chronology Opening Date [yyyy-mm-dd] Exhibition Title Closing Date [yyyy-mm-dd] Locator](https://img.pdfslide.us/doc/110x75/5e88a3bad9e47b16f32faa0f/exhibition-database-chronology-royal-ontario-museum-952012-exhibition-database.jpg)