Embed Size (px)
Citation preview

Slide 1
Convergence of Primary and Implementation TB and HIV Research:
Are We Missing Opportunities?
Constance A. Benson, M.D.
Professor of Medicine
Division of Infectious Diseases
University of California, San Diego

Introduction • Knowledge gaps
– New TB and HIV drug development
• More effective TB and HIV cotreatment
• TB treatment shortening
• Treatment of M/XDR-TB
– TB biomarkers of treatment response
– Infection control
• Opportunities to promote closer collaboration in primary and implementation research in TB and HIV
Knowledge Gaps in TB and HIV Co-Treatment
• Most appropriate first, second and third-line ART regimens to use in combination with TB regimens (including how to incorporate new TB drugs)
– TB and HIV outcomes including TB relapse, TB and HIV drug resistance
– Effective interventions to prevent and treat IRIS
– Effect of HIV on drug absorption, synergistic toxicities, immune response
– Drug interactions that go beyond efavirenz and rifamycins

ANRS 12 180 REFLATE TB • HIV-infected patients with TB receiving rifampin treated with
raltegravir 400 or 800 mg BID vs EFV had similar virologic outcomes
Grinsztejn B et al, CROI 2013
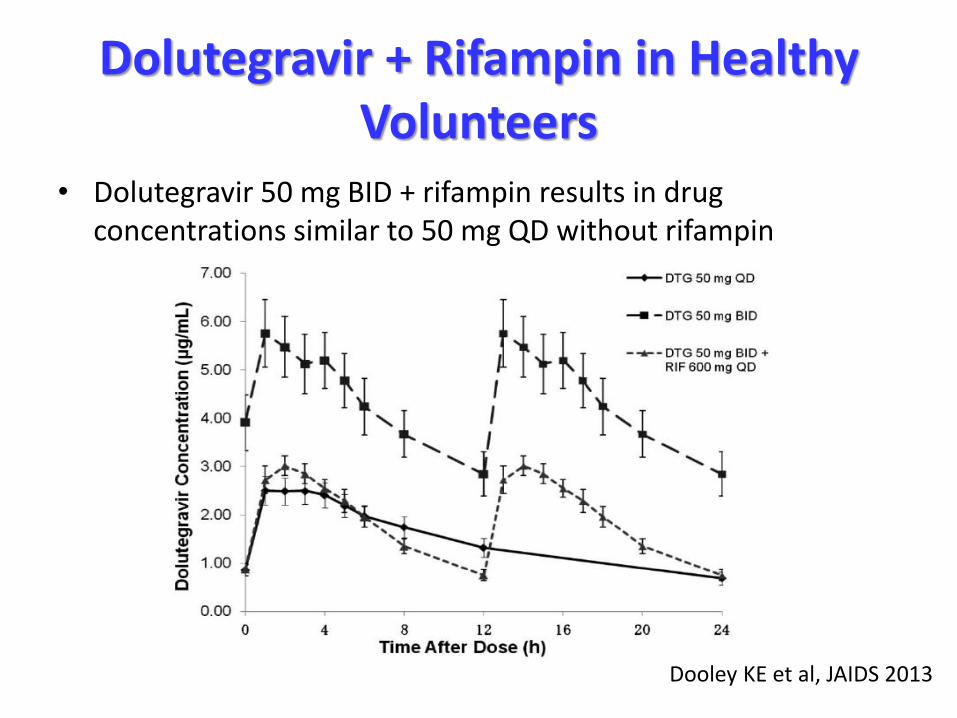
Dolutegravir + Rifampin in Healthy Volunteers
• Dolutegravir 50 mg BID + rifampin results in drug concentrations similar to 50 mg QD without rifampin
Dooley KE et al, JAIDS 2013
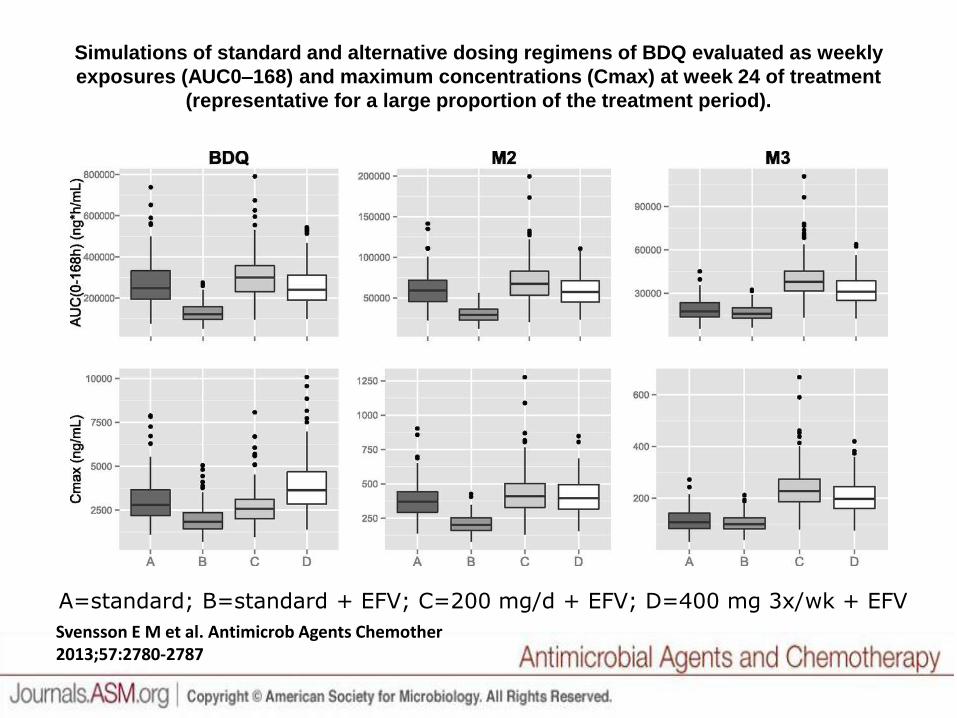
Simulations of standard and alternative dosing regimens of BDQ evaluated as weekly
exposures (AUC0–168) and maximum concentrations (Cmax) at week 24 of treatment
(representative for a large proportion of the treatment period).
Svensson E M et al. Antimicrob Agents Chemother 2013;57:2780-2787
A=standard; B=standard + EFV; C=200 mg/d + EFV; D=400 mg 3x/wk + EFV
New TB Drugs and Classes in Clinical Trials
• Bedaquiline: diarylquinoline; inhibits mycobacterial ATP synthase
• Delamanid and PA-824: nitroimidazoles; inhibit mycolic acid synthesis
• Sutezolid, linezolid, AZD-5847: oxazolidinones; inhibit protein synthesis
• SQ-109: ethambutol analogue; blocks cell wall synthesis, prevents efflux of companion drugs from macrophages
• Long acting rifamycins (rifapentine)
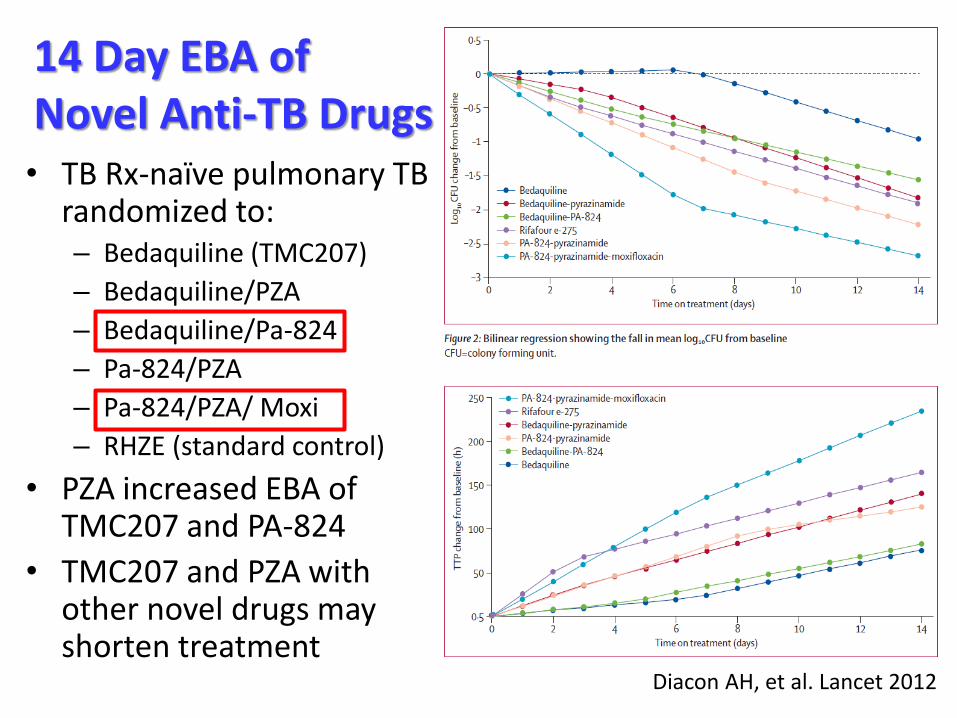
14 Day EBA of Novel Anti-TB Drugs • TB Rx-naïve pulmonary TB
randomized to: – Bedaquiline (TMC207)
– Bedaquiline/PZA
– Bedaquiline/Pa-824
– Pa-824/PZA
– Pa-824/PZA/ Moxi
– RHZE (standard control)
• PZA increased EBA of TMC207 and PA-824
• TMC207 and PZA with other novel drugs may shorten treatment
Diacon AH, et al. Lancet 2012

0
20
40
60
80
100
120
Unfavorable
Favorable
• Similar outcomes when moxifloxacin was substituted for INH
• 4 month regimen inferior to control
• All regimens safe and well-tolerated
• No difference in outcomes by HIV status
– No ART
RIFAQUIN: High Dose Rifapentine + Moxifloxacin for Shortening TB Treatment
Jindani A, et al., Abstr. 147LB, 20th CROI, 2013
Treatment-Shortening Trials for Drug-Susceptible TB
• OFLOTUB (data analysis underway)
– Phase 3 RCT of RHZE standard course vs.
– 2 mos RHZ + gatifloxacin then 2 mos RH + gatifloxacin
• REMox (completion 2Q 2014)
– Phase 3 RCT of RHZE standard course vs.
– 2 mos RHZ + moxifloxacin then 2 mos RH + moxifloxacin (replacing ethambutol)
– 2 mos RMZE then 2 mos RM (replacing INH)

Additional Knowledge Gaps in New TB Drug Development
• Drug resistance mechanisms not well characterized
• HIV co-treatment
– Effect of immunodeficiency, other physiologic abnormalities, higher bacillary burden on TB treatment response independent of drug interactions
• “Surrogate markers” of treatment response
– Reduce prolonged drug development timelines
– Monitor early efficacy in TB-HIV cotreatment
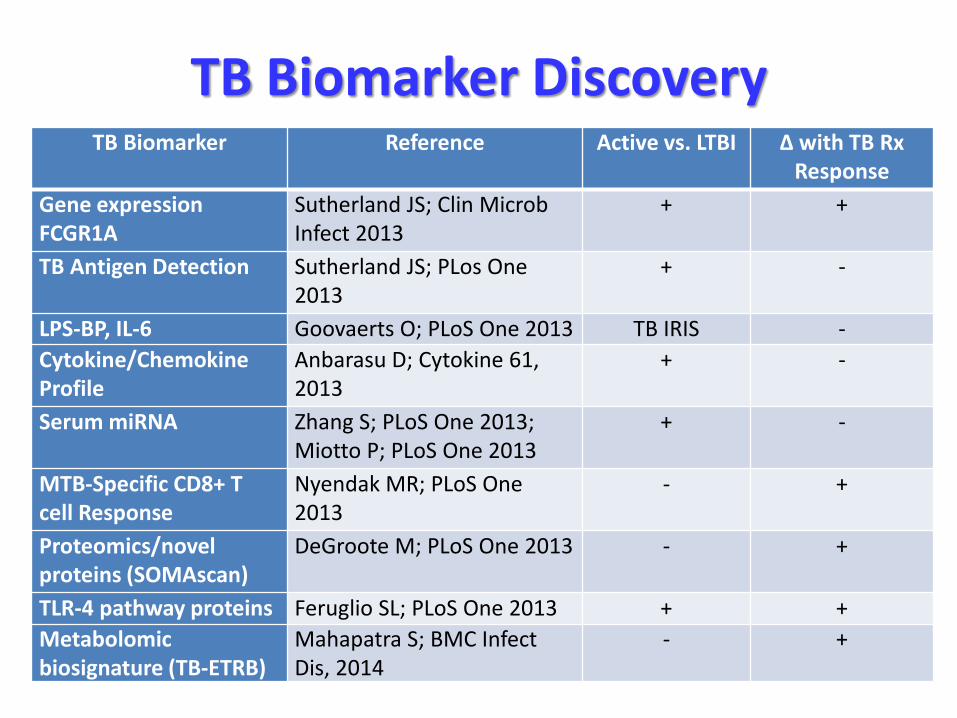
TB Biomarker Discovery TB Biomarker Reference Active vs. LTBI Δ with TB Rx
Response
Gene expression FCGR1A
Sutherland JS; Clin Microb Infect 2013
+ +
TB Antigen Detection Sutherland JS; PLos One 2013
+ -
LPS-BP, IL-6 Goovaerts O; PLoS One 2013 TB IRIS -
Cytokine/Chemokine Profile
Anbarasu D; Cytokine 61, 2013
+ -
Serum miRNA Zhang S; PLoS One 2013; Miotto P; PLoS One 2013
+ -
MTB-Specific CD8+ T cell Response
Nyendak MR; PLoS One 2013
- +
Proteomics/novel proteins (SOMAscan)
DeGroote M; PLoS One 2013 - +
TLR-4 pathway proteins Feruglio SL; PLoS One 2013 + +
Metabolomic biosignature (TB-ETRB)
Mahapatra S; BMC Infect Dis, 2014
- +

Consortium for TB Biomarkers (CTB2) Primary Goals • Establish a collaborative biobank to
facilitate discovery and qualification of biomarkers of TB drug effect
– Early markers of drug effect
– Surrogates for failure/relapse
• Make samples available to the broader community through a peer review system
– To shorten/simplify registration trials for TB drugs and regimens
– To involve TB R&D community in the solution

Treatment Outcomes for M/XDR-TB
• Overall cure rate for ~34,000 MDR-TB globally ~40-60%; highest for the Americas and Eastern Mediterranean regions in 2010
• Subset of 795 with XDR-TB, success rate 20% overall and 44% died
MDR-TB: “Bangladesh Regimen”
• Observational study from 1997-2007 of 427 previously untreated MDR-TB pts sequentially assigned to one of six standardized regimens
– Subsequent cohorts treated with regimens adapted from the most successful regimens used in previous cohorts
• Most effective regimen: 9 mos of gatifloxacin, clofazimine, EMB, PZA throughout + initial 4 mos of high dose INH, prothionamide, kanamycin
– Relapse-free cure rate 87%
– 33 deaths; 41 “defaulted”
– Generally tolerated; GI upset most common AE
Van Duen A, et al. Am J Resp Crit Care Med 2010
New Drugs in Combination for Treatment of MDR-TB: ACTG A5319
• 240 participants with culture-confirmed MDR-TB with or without HIV co-infection
• RCT four arms stratified by HIV and EFV-based ART
– BDQ + Pa824 + Sutezolid (1200 mg/d) + PZA
– BDQ + Pa824 + Sutezolid (600 mg BID) + PZA
– BDQ + Pa824 + Linezolid + PZA
– Local SOC (optimized by DST) for MDR-TB
• Primary endpoints: Safety/tolerability; culture conversion rates to determine which regimens to move to Stage 2 (flexible study design to “play the winner”)

Implementation Knowledge Gaps in M/XDR-TB
• Impact of HIV infection and ART on transmission, acquisition and progression of TB drug resistance
– Impact of earlier start of ART on M/XDR-TB transmission
• Best models of care, hospital vs. community-based, of drug-resistant TB in resource-limited settings with high HIV burden
• Optimal management of household and community contacts of drug-resistant TB patients
Implementation Knowledge Gaps in Infection Control
• What are the best facility-based infection control interventions to effectively reduce TB transmission in all health care settings? – Operational models to implement IC and monitor
impact on TB rates
– Effectiveness (and cost-effectiveness) of individual infection control measures in reducing TB transmission
– Overcoming knowledge and stigma barriers
– Impact of HIV on relapse, reinfection, patterns of transmission in communities

Are We Missing Opportunities? Yes!

The Next “Three I’s?”
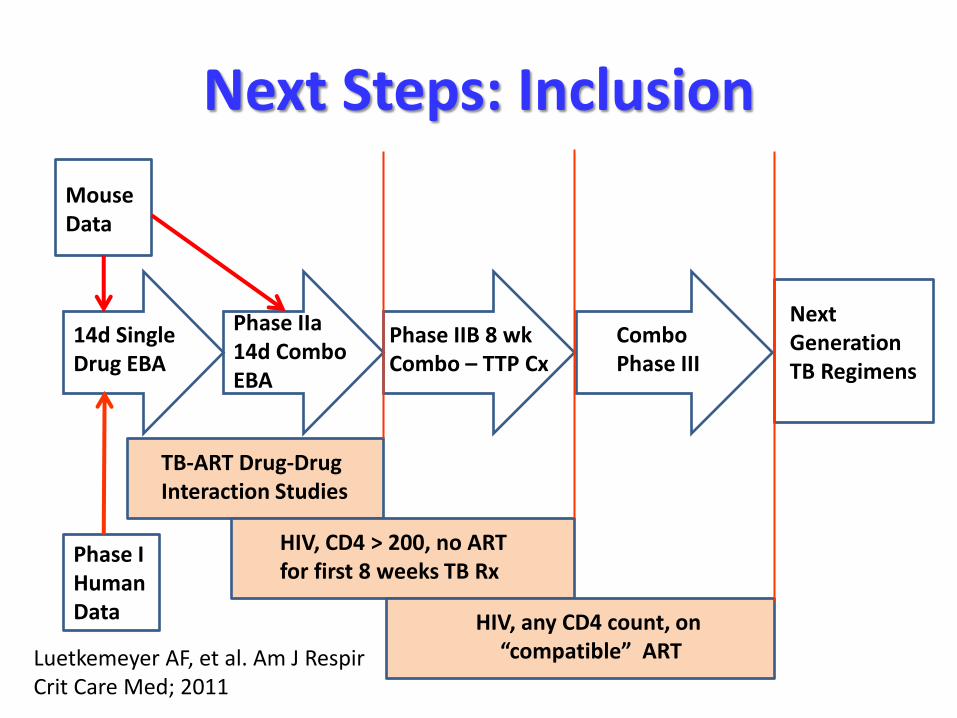
Next Steps: Inclusion
14d Single Drug EBA
Phase IIa 14d Combo EBA
Phase IIB 8 wk Combo – TTP Cx
Combo Phase III
Next Generation TB Regimens
Mouse Data
TB-ART Drug-Drug Interaction Studies
HIV, CD4 > 200, no ART for first 8 weeks TB Rx
HIV, any CD4 count, on “compatible” ART
Phase I Human Data
Luetkemeyer AF, et al. Am J Respir Crit Care Med; 2011
Next Steps: Integration • Integrate TB-HIV primary and implementation
research at local site levels
– Research sites with experienced staff and sufficient diagnostic and laboratory infrastructure to manage both TB and HIV disease to serve as the catalyst for integration and implementation of TB and HIV services
• Personnel training
• Evaluation of models of care and outcomes (both TB and HIV) as new drugs and regimens become more widely used
Next Steps: Innovation • Develop TB clinical trials with flexible,
modifiable designs
• Use them as a platform to more rapidly evaluate…
– Surrogate TB biomarkers of drug efficacy and treatment response
– Point-of-care and other simplified platforms for diagnosis and monitoring of outcomes
– Models to change how TB and HIV treatment is delivered
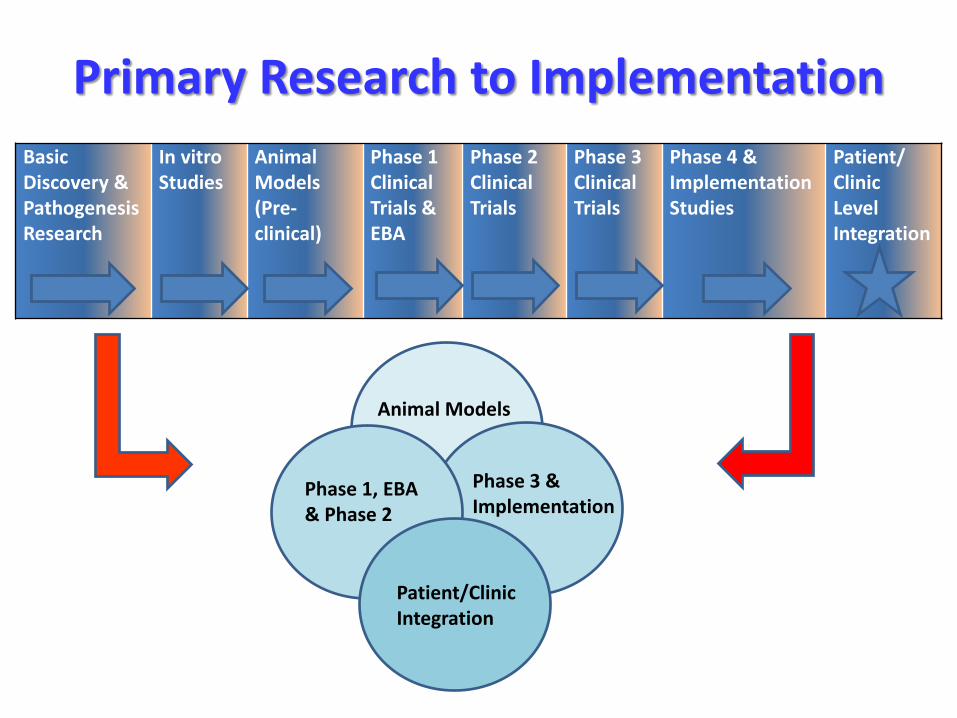
Primary Research to Implementation
Basic Discovery & Pathogenesis Research
In vitro Studies
Animal Models (Pre-clinical)
Phase 1 Clinical Trials & EBA
Phase 2 Clinical Trials
Phase 3 Clinical Trials
Phase 4 & Implementation Studies
Patient/ Clinic Level Integration
Animal Models
Phase 1, EBA & Phase 2
Phase 3 & Implementation
Patient/Clinic Integration

Discussion