Embed Size (px)
Citation preview

3rd Congress of the European Academy of Neurology
Amsterdam, The Netherlands, June 24 – 27, 2017
Hands-on Course 5
Electromyography: Surface, needle conventional and single fiber - Level 1-2
Conventional needle electromyography
Christian Krarup Copenhagen, Denmark
Email: [email protected]

1
Conflict of interest: The author has no disclosures associated with this teaching course.
Introduction
Acute, subacute, relapsing or chronic progressive weakness may occur in
diseases of the motor neuron, peripheral nerve, neuromuscular junction or
muscle requiring evaluation of motor or sensory nerve fiber conduction
and EMG.
Factors to be considered
1. Clinical history, complaints and examination
2. Identification of the pathological and pathophysiological nature of the
disease
3. Demonstration of the anatomical distribution and extent of abnormali-
ties
Neurophysiological methods
The methods used to detect whether weakness is caused by peripheral
nerve or motor neuron disease or by muscle involvement include EMG and
nerve conduction studies.
2
EMG
The different parts of the EMG examination are intended to provide patho-
physiological information regarding the innervation and function of muscle
fibers and the motor unit, and they include recording at rest, during weak
effort and during maximal effort:
1. Recordings at rest to investigate the presence of spontaneous activity.
2. Recordings at weak effort to investigate the characteristics of motor
unit potentials (MUP).
3. Recordings at maximal voluntary contractions (MVC) to investigate the
interference pattern.
Each of these parameters provides different information about patho-
physiological alterations of muscle fibers and motor units, and the changes
occur at different time points in relation to the disease process. It is
therefore necessary to include all the different aspects to arrive at the
most likely cause of weakness.
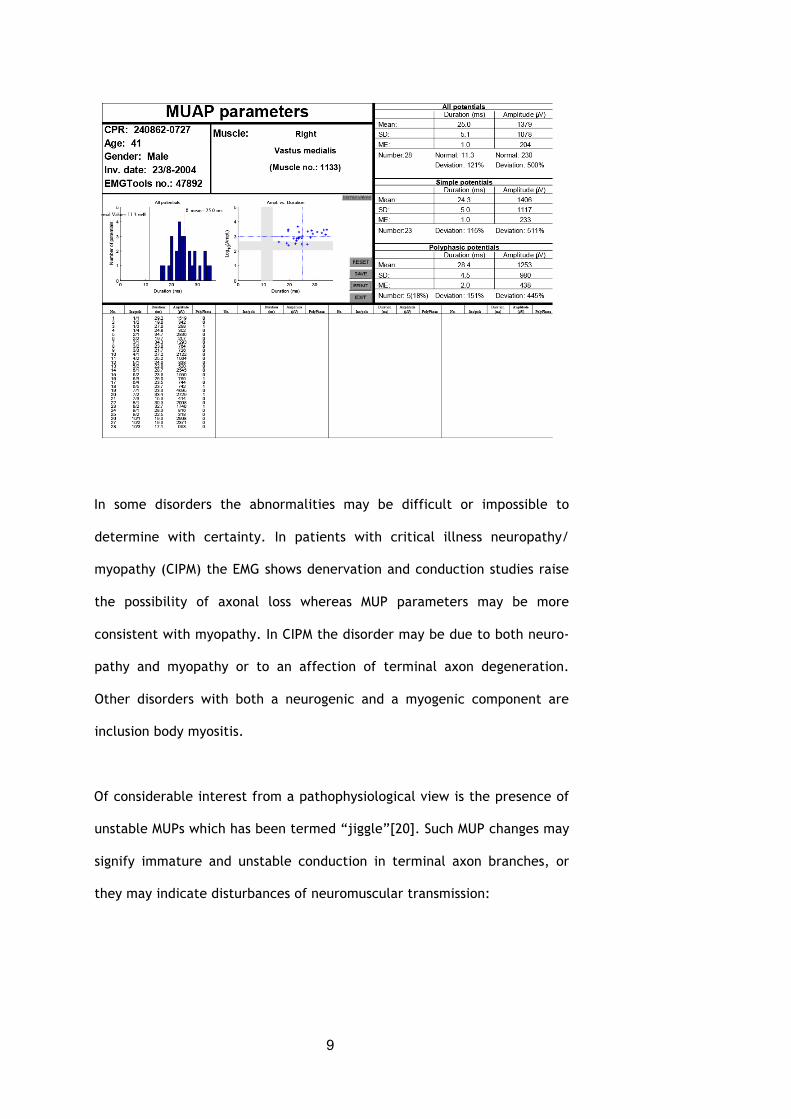
Measurements and interpretation of the EMG
Clinical interpretation of the EMG signal relies in many routine studies on
qualitative impressions of the recordings. This has the advantage that the
experienced electropmyographer quickly can make recordings from many
muscles; however, the approach has both methodological and biological
limitations. Methodologically the weakness of qualitative evaluation of
the EMG is related to its dependence on, 1) the experience of the person
carrying out the study and the lack of documentation, and 2) the bias
introduced by relatively limited recordings from the muscle. Biologically,
the limitation of qualitative EMG evaluation is mainly due to the wide
variability of signals from normal and pathological muscle. In this situa-
3
tion, too much reliance may be put on the presence of single abnormal
signals, whether these are denervation activity at rest or single abnormal
MUPs. In this connection it should, however, be mentioned that the pres-
ence of so-called “outliers” has been found to be a sensitive parameter by
some investigators[19].
The alternative methodological approach is so-called “quantitative” EMG
which mainly differs from the qualitative method by applying statistical
methods to the interpretation of EMG measurements. The method was
introduced by Buchthal and colleagues[1, 4, 6-8] by measurements of the
duration and amplitude of motor unit potentials (MUP). The basis for this
approach is that individual MUPs from the same muscle vary considerably
and that the use of recording from several sites in the muscle would allow
a more certain definition of abnormalities. Furthermore, the MUPs from
different muscles and at different ages vary considerably[9] and this
variability should be taken into consideration in the diagnostic approach.
The mechanism of the variable duration and amplitude of MUPs in the
same muscle is related to two main factors: 1) synchronization of arrival of
action potentials; the MUP is a compound response from the individual
muscle fibers in the motor unit, and the duration of the MUP is determined
mainly by the spatial dispersion of end-plates of each individual muscle
fiber. The amplitude of the MUP is determined by the proximity of the few
muscle fibers closest to the recording electrode. 2) the number of muscle
fibers in the motor unit; in general, the duration and amplitude of the
MUPs are correlated with the size of the motor unit.
The variability within the muscle requires that statistical evaluation is used
to ascertain whether the MUPs deviate from normal. 20-30 MUPs are
4
needed to calculate the mean duration and amplitude. Originally measure-
ments were carried out by manual measurements on MUPs recorded on
film using a trigger and delay-line and. This approach was by many busy
clinicians found too time consuming and cumbersome, and quantitative
evaluation was therefore only used in some laboratories. The use of less
stringent methods may be one of the reasons that EMG by many is
considered unsuitable for the diagnosis of for example myopathy.
One of the limitations of quantitative EMG is that a trigger and delay line is
used to capture the MUP signal and therefore may be biased towards larger
potentials.
Automatic decomposition of the EMG signal
The use of computers to analyze the EMG signal has considerably aided the
diagnostic certainty of the method[17]: 1) it is possible to rapidly collect
and analyze a large number of MUPs, and 2) the recording is less subject to
bias since analysis is not dependent on trigger to capture the MUP. The
main requirement of the algorithm is that it can extract and distinguish
both large and small MUPs from the EMG signal.
Spontaneous activity in voluntary muscle
In normal muscle, there is no activity at rest. Nevertheless, in the end-
plate zone recordings show base-line disturbances due to miniature end-
plate potentials (mepp) and in addition negative onset spike potentials
with amplitude of 100-150 µV with irregular intervals due to propagated
spontaneous end-plate potentials (epp). When recorded outside the end-
plate region these epp give rise to rare single fiber potentials that are
indistinguishable from fibrillation potentials or positive sharp waves. Thus
5
recordings of fibrillation potentials or sharp-waves at up to two of 10
investigated sites is not an abnormal phenomenon[5]. When the needle
electrode is inserted into the muscle, this elicits a burst of insertional
activity which rapidly disappears.
Abnormal spontaneous activity includes a variety of phenomena such as
denervation potentials, fasciculations, myotonia, neuromyotonia, myoky-
mia, and complex repetitive discharges:
Denervation activity:
Muscle fibers that lose their innervation undergo several changes including
spread of acetylcholine receptors outside the end-plate region and the
resting membrane potential becomes depolarized. These changes occur
with a delay which is related to the length of the distal nerve stump[16],
and in parallel the individual muscle fibers start to contract spontane-
ously[10] giving rise to action potentials that may be recorded with intra-
muscular needle or surface electrodes[2, 3]. Thus, following a proximal
nerve lesion, recording of denervation activity in the extremities may be
delayed by several weeks. Furthermore, denervation activity is tempera-
ture dependent being more frequent at physiological temperature than
after cooling and it is cyclic in its occurrence[21], which may explain that
1/3-1/4 of partially denervated muscles do not show denervation activity.
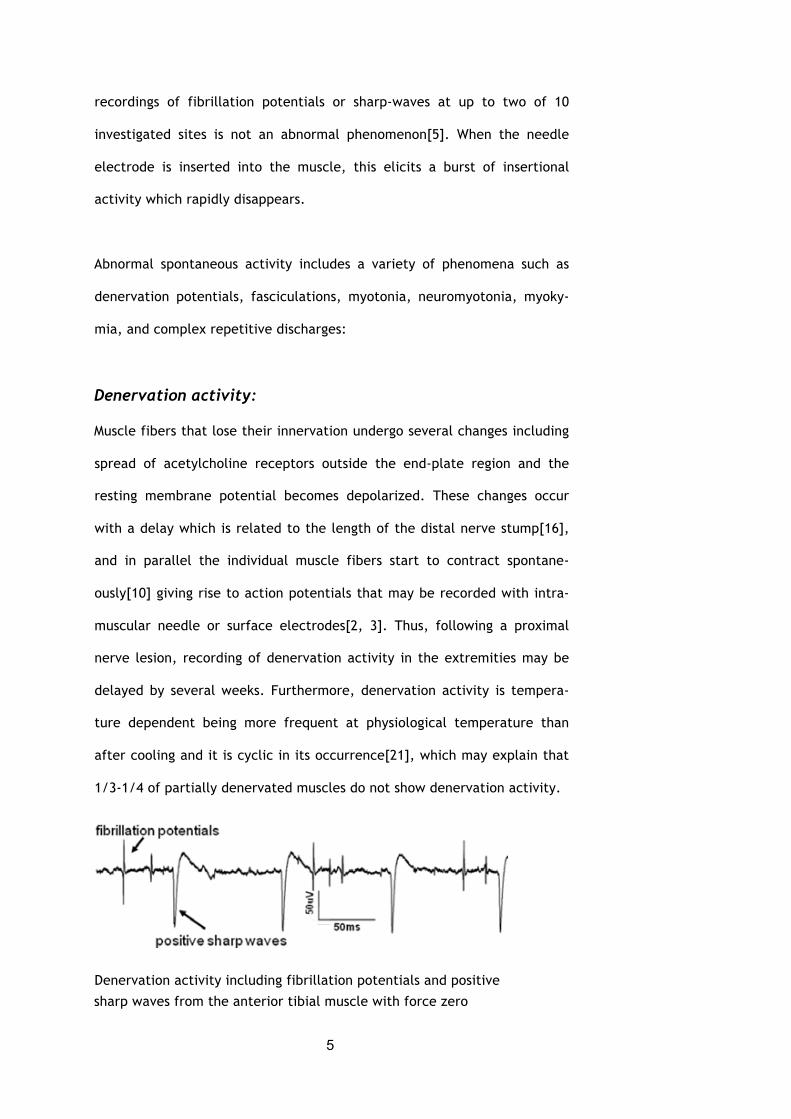
Denervation activity including fibrillation potentials and positive
sharp waves from the anterior tibial muscle with force zero
6
Fibrillation potentials have a diphasic or triphasic shape and a duration of
3-5 ms and positive sharp waves may have a duration up to 20 ms, and
these often occur in the same recording. The amplitudes of fibrillation
potentials vary widely in the range of 50-150 µV but may be as high as
several hundred µV dependent on how close the recording electrode is to
the active muscle fiber. There have been some claims that the amplitude
is higher in severely denervated muscles[12, 13]; however, this could be
explained by a greater chance that the recording needle is close to
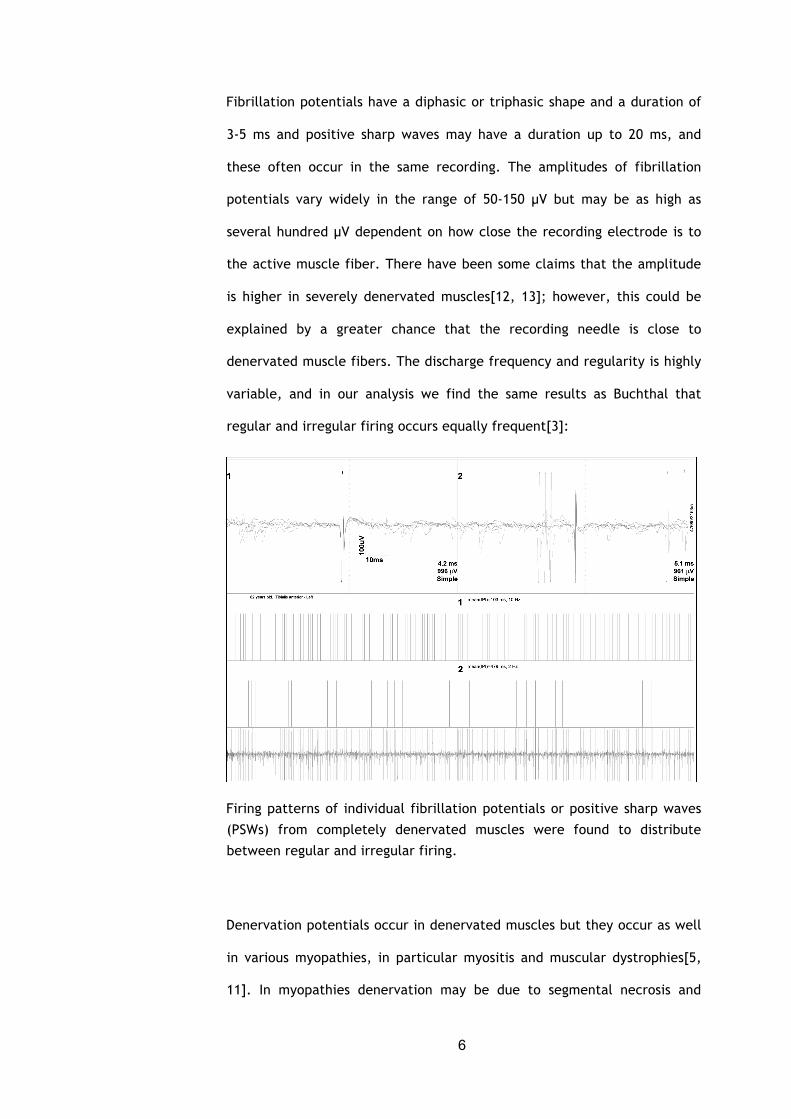
denervated muscle fibers. The discharge frequency and regularity is highly
variable, and in our analysis we find the same results as Buchthal that
regular and irregular firing occurs equally frequent[3]:
Firing patterns of individual fibrillation potentials or positive sharp waves
(PSWs) from completely denervated muscles were found to distribute
between regular and irregular firing.
Denervation potentials occur in denervated muscles but they occur as well
in various myopathies, in particular myositis and muscular dystrophies[5,
11]. In myopathies denervation may be due to segmental necrosis and
7
isolation of parts of the muscle fiber, or it may be due to ion channel
abnormalities.
Fasciculations:
Fasciculations occur as irregular firing of groups of muscle fibers[10] that
may correspond to the motor unit. As opposed to fibrillation potentials,
which occur to a greater extent on warming the muscle, fasciculations
occur more frequently on cooling the muscle. In comparisons of MUPs and
fasciculations from the same muscle, their durations and amplitudes were
similar, suggesting that they originate from the same groups of fibers
(Nikolic, Crone, Hultborn, Krarup, 2006).
Motor unit potential (MUP)
The duration, amplitude and shape of MUPs are parameters that change in
patients with myopathy and in neurogenic lesions. The amplitudes of the
MUP are considerably more variable than the duration. The incidence of
polyphasic potentials is 12% in most limb muscles except in the deltoid
where the incidence is 25%. In the anterior tibial muscle the incidence may
be up to 20% and in facial muscles up to 25%.
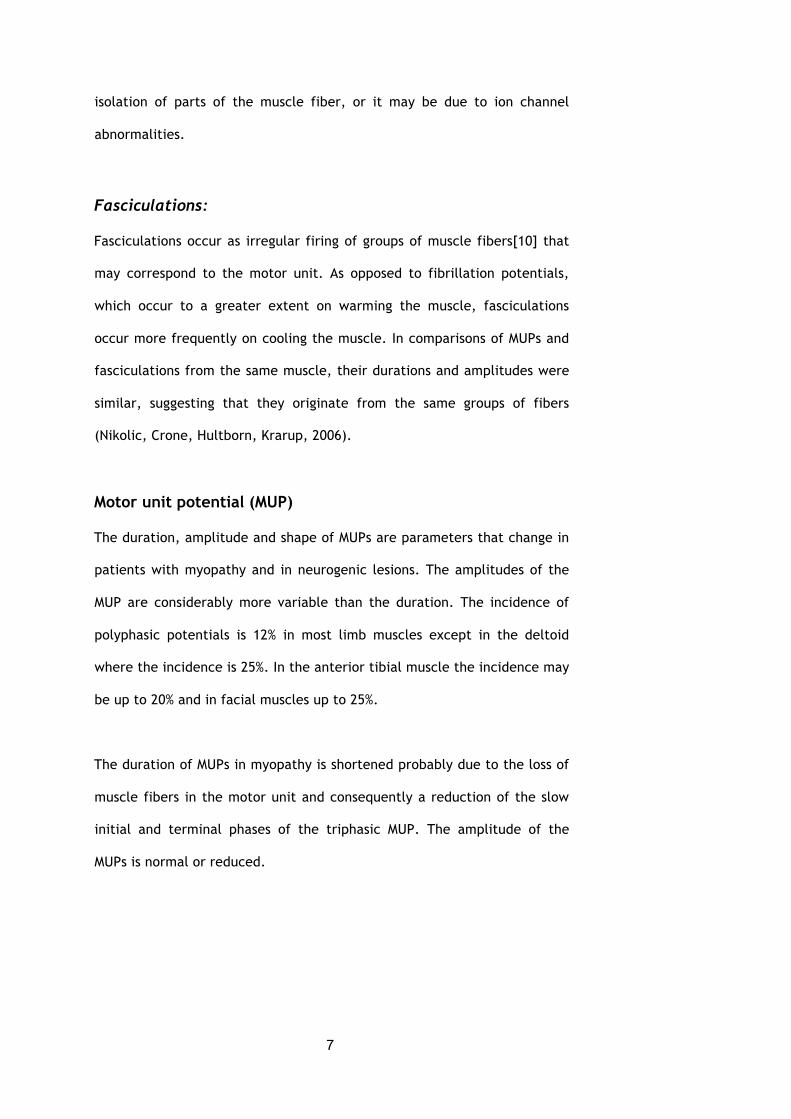
The duration of MUPs in myopathy is shortened probably due to the loss of
muscle fibers in the motor unit and consequently a reduction of the slow
initial and terminal phases of the triphasic MUP. The amplitude of the
MUPs is normal or reduced.
8
EMG from a patient with limb-girdle myopathy showing markedly shortened
potential duration and borderline changes in the MUP amplitude.
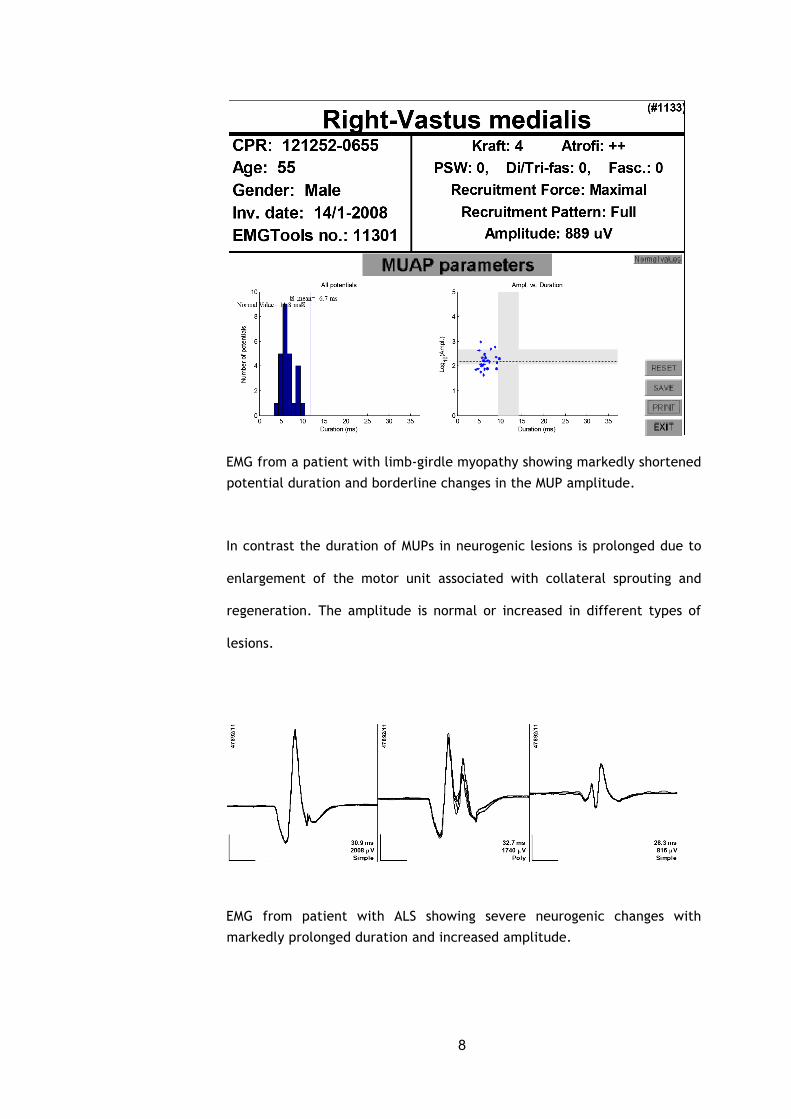
In contrast the duration of MUPs in neurogenic lesions is prolonged due to
enlargement of the motor unit associated with collateral sprouting and
regeneration. The amplitude is normal or increased in different types of
lesions.
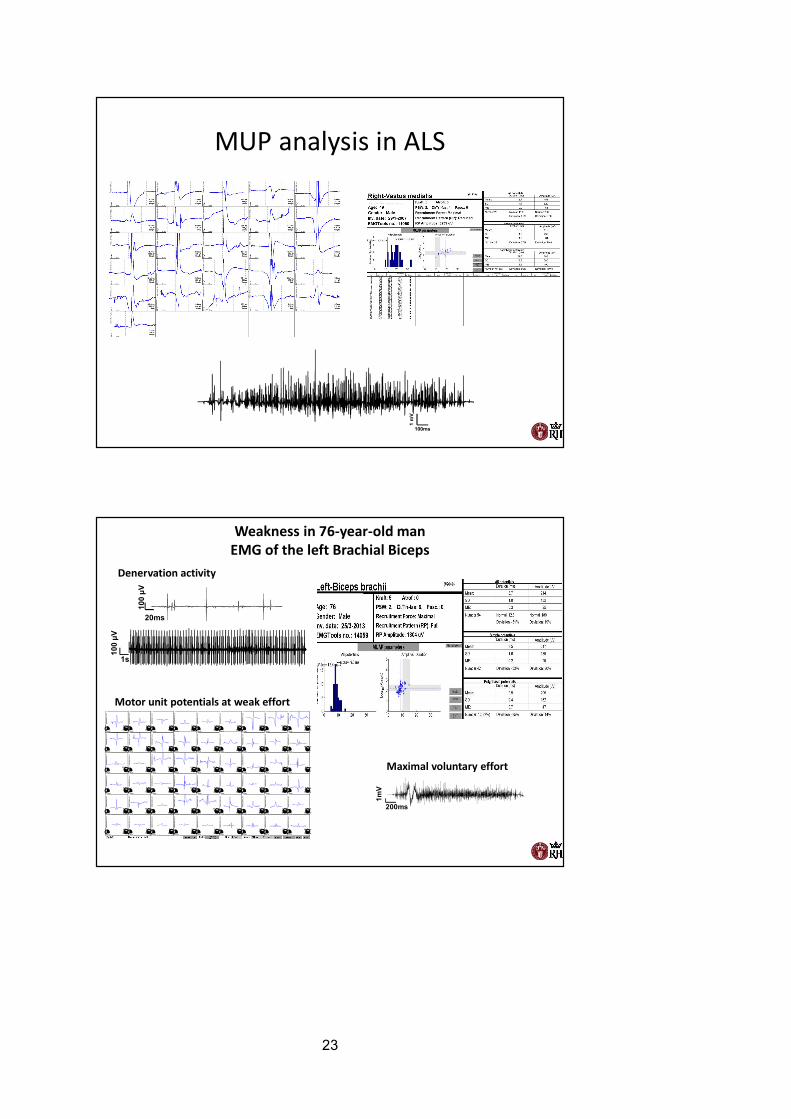
EMG from patient with ALS showing severe neurogenic changes with
markedly prolonged duration and increased amplitude.
9
In some disorders the abnormalities may be difficult or impossible to
determine with certainty. In patients with critical illness neuropathy/
myopathy (CIPM) the EMG shows denervation and conduction studies raise
the possibility of axonal loss whereas MUP parameters may be more
consistent with myopathy. In CIPM the disorder may be due to both neuro-
pathy and myopathy or to an affection of terminal axon degeneration.
Other disorders with both a neurogenic and a myogenic component are
inclusion body myositis.
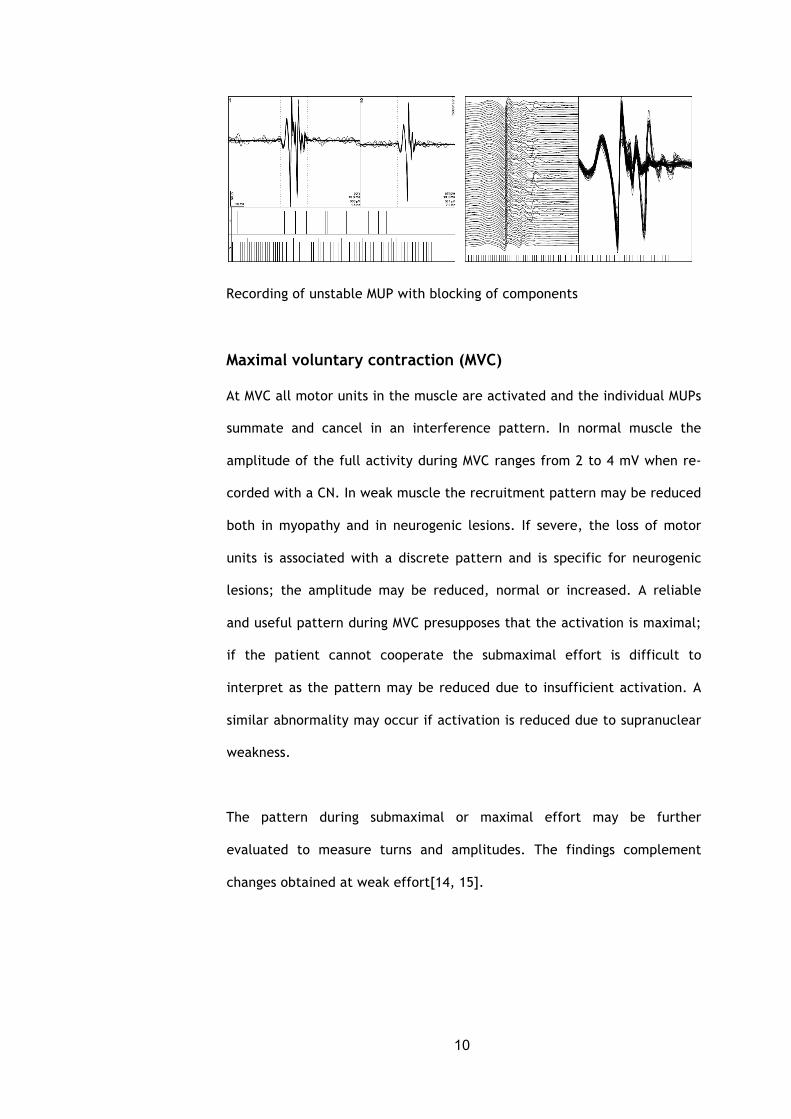
Of considerable interest from a pathophysiological view is the presence of
unstable MUPs which has been termed “jiggle”[20]. Such MUP changes may
signify immature and unstable conduction in terminal axon branches, or
they may indicate disturbances of neuromuscular transmission:
10
Recording of unstable MUP with blocking of components
Maximal voluntary contraction (MVC)
At MVC all motor units in the muscle are activated and the individual MUPs
summate and cancel in an interference pattern. In normal muscle the
amplitude of the full activity during MVC ranges from 2 to 4 mV when re-
corded with a CN. In weak muscle the recruitment pattern may be reduced
both in myopathy and in neurogenic lesions. If severe, the loss of motor
units is associated with a discrete pattern and is specific for neurogenic
lesions; the amplitude may be reduced, normal or increased. A reliable
and useful pattern during MVC presupposes that the activation is maximal;
if the patient cannot cooperate the submaximal effort is difficult to
interpret as the pattern may be reduced due to insufficient activation. A
similar abnormality may occur if activation is reduced due to supranuclear
weakness.
The pattern during submaximal or maximal effort may be further
evaluated to measure turns and amplitudes. The findings complement
changes obtained at weak effort[14, 15].
11
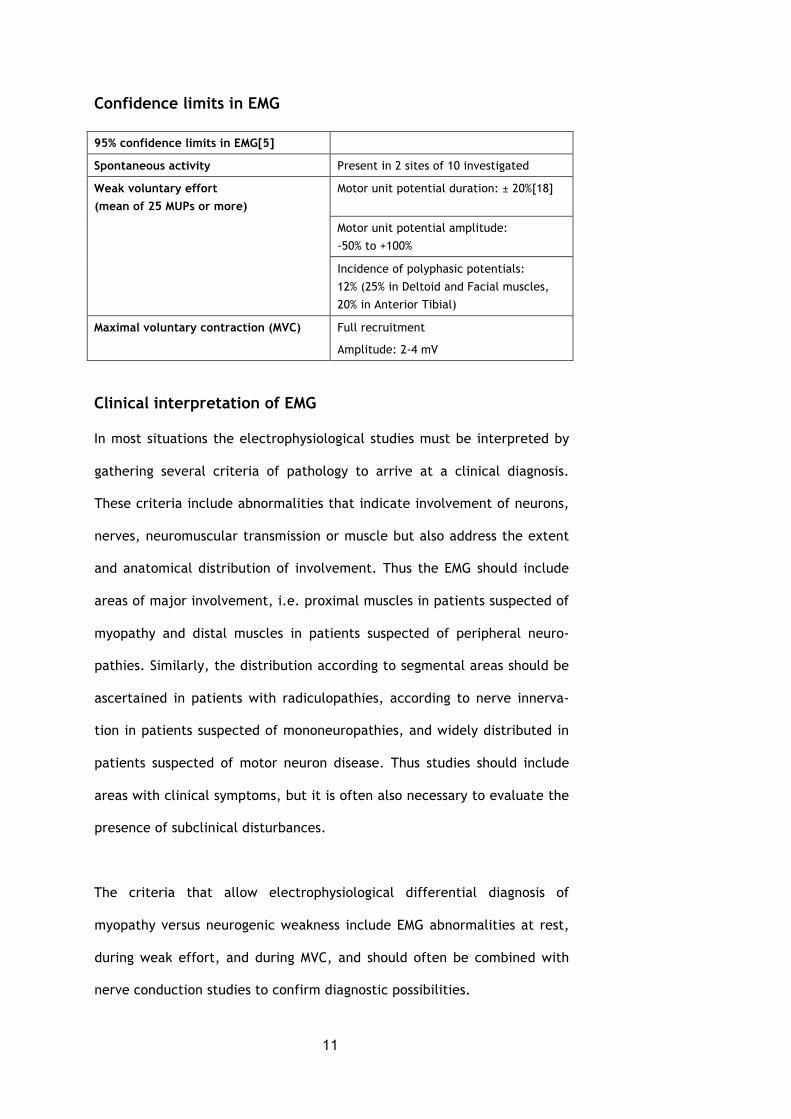
Confidence limits in EMG
95% confidence limits in EMG[5]
Spontaneous activity Present in 2 sites of 10 investigated
Weak voluntary effort (mean of 25 MUPs or more)
Motor unit potential duration: ± 20%[18]
Motor unit potential amplitude:
-50% to +100%
Incidence of polyphasic potentials:
12% (25% in Deltoid and Facial muscles,
20% in Anterior Tibial)
Maximal voluntary contraction (MVC) Full recruitment
Amplitude: 2-4 mV
Clinical interpretation of EMG
In most situations the electrophysiological studies must be interpreted by
gathering several criteria of pathology to arrive at a clinical diagnosis.
These criteria include abnormalities that indicate involvement of neurons,
nerves, neuromuscular transmission or muscle but also address the extent
and anatomical distribution of involvement. Thus the EMG should include
areas of major involvement, i.e. proximal muscles in patients suspected of
myopathy and distal muscles in patients suspected of peripheral neuro-
pathies. Similarly, the distribution according to segmental areas should be
ascertained in patients with radiculopathies, according to nerve innerva-
tion in patients suspected of mononeuropathies, and widely distributed in
patients suspected of motor neuron disease. Thus studies should include
areas with clinical symptoms, but it is often also necessary to evaluate the
presence of subclinical disturbances.
The criteria that allow electrophysiological differential diagnosis of
myopathy versus neurogenic weakness include EMG abnormalities at rest,
during weak effort, and during MVC, and should often be combined with
nerve conduction studies to confirm diagnostic possibilities.

12
Abnormalities at EMG may be classified as specific or non-specific
according to whether they occur only in myopathy or neurogenic disorder
or in both types of diseases. Thus denervation activity is present in both
myopathy and in neurogenic lesions and the abnormality is classified as
non-specific. In contrast MUP duration and amplitude are reduced only in
myopathy, whereas an increase is seen only in neurogenic lesions, and
these abnormalities are classified as specific. The recruitment pattern at
MVC may be reduced in myopathy as well as in neurogenic lesions indi-
cating a non-specific abnormality, while a discrete pattern occurs only in
neurogenic lesions indicating a specific abnormality. A reduced amplitude,
full recruitment pattern is specific for myopathy whereas an increased
amplitude of the recruitment pattern occurs only in neurogenic lesions[5].
EMG criteria of myopathy
Specific criteria Non-specific criteria
Weak effort:
Decrease in MUP duration
MVC:
Full recruitment in weak and wasted
muscle Reduced amplitude of full
recruitment pattern
Activity at rest:
Increased denervation activity
Weak effort:
Increased incidence of polyphasic MUPs
MVC:
Reduced recruitment pattern
EMG criteria of neurogenic impairment
Weak effort:
Increase in MUP duration
Increase in MUP amplitude
MVC:
Discrete recruitment pattern
Increased amplitude
Activity at rest:
Increased denervation activity
Weak effort:
Increased incidence of polyphasic
potentials
MVC:
Reduced recruitment pattern
Decreased amplitude

13
References
1. Buchthal F: An introduction to electromyography. København,
Stockholm, Oslo: Scandinavian University Books; 1957.
2. Buchthal F: Fibrillations: clinical electrophysiology. In Abnormal
nerves and muscles as impulse generators. Edited by Culp WJ,
Ochoa J: Oxford University Press; 1982:632-662.
3. Buchthal F: Spontaneous electrical activity: an overview.
Muscle Nerve 1982, 5:S52-S59.
4. Buchthal F: Electromyography in the evaluation of muscle disease. Neurol.Clin. 1985, 3:573-598.
5. Buchthal F, Kamieniecka Z: The diagnostic yield of quantified electromyography and quantified muscle biopsy in neuromuscular disorders. Muscle & Nerve 1982, 5:265-280.
6. Buchthal F, Pinelli P: Action potentials in muscular atrophy of neurogenic origin. Neurology 1953, 3:591-603.
7. Buchthal F, Pinelli P: Muscle action potentials in polymyositis. Neurology 1953, 3:424-436.
8. Buchthal F, Pinelli P, Rosenfalck P: Action potential parameters in normal human muscle and their physiological determinants. Acta Physiol Scand. 1954, 32:219-229.
9. Buchthal F, Rosenfalck P: Action potential parameters in different human muscles. Acta Psychiatr.Neurol.Scand.
1955, 30:125-131.
10. Denny-Brown D, Pennybacker JB: Fibrillation and fasciculation in voluntary muscle. Brain 1938, 61:311-334.
11. Desmedt JE, Borenstein S: Relationship of spontaneous fibrillation potentials to muscle fibre segmentation in human muscular dystrophy. Nature 1975, 258:531-534.
12. Kraft GH: Fibrillation potential amplitude and muscle atrophy following peripheral nerve injury. Edited by: American
Association of Electromyography and Electrodiagnosis; 1989:45-50.
13. Kraft GH: Are fibrillation potentials and positive sharp waves the same? No. Muscle & Nerve 1996, 19:216-220.
14. Liguori R, Dahl K, Fuglsang-Frederiksen A: Turns-amplitude analysis of the electromyographic recruitment pattern disregarding force measurement. I. Method and reference values in healthy subjects. Muscle & Nerve 1992, 15:1314-1318.

14
15. Liguori R, Dahl K, Fuglsang-Frederiksen A, Trojaborg W: Turns-amplitude analysis of the electromyographic recruitment pattern disregarding force measurement. II. Findings in patients with neuromuscular disorders. Muscle & Nerve 1992, 15:1319-1324.
16. Luco JV, EYZAGUIRRE C: Fibrillation and hypersensitivity to ACh in denervated muscle: effect of length of degenerating nerve fibers. J Neurophysiol. 1955, 18:65-73.
17. Nikolic M, Krarup C: EMGTools, an adaptive and versatile tool for detailed EMG analysis. IEEE Trans.Biomed.Eng 2011, 58:2707-2718.
18. Rosenfalck P, Rosenfalck A: Electromyography - sensory and motor
conduction. Findings in normal subjects. Copenhagen: Laboratory
of Clinical Neurophysiology, Rigshospitalet; 1975.
19. Stålberg E, Bischoff C, Falck B: Outliers, a way to detect abnormality in quantitative EMG. Muscle Nerve 1994, 17:392-399.
20. Stålberg EV, Sonoo M: Assessment of variability in the shape of the motor unit action potential, the ''jiggle,'' at consecutive discharges. Muscle & Nerve 1994, 17:1135-1144.
21. Thesleff S: Fibrillation in denervated mammalian skeletal muscle. In Abnormal nerves and muscles as impulse generators.
Edited by Culp WJ, Ochoa J: Oxford University Press; 1982:678-694.
15
21/03/2017
1
Electromyography - conventional
Christian Krarup, MD DMSc FRCP FEANDepartment of Clinical Neurophysiology,
Rigshospitalet and University of Copenhagen,Denmark
Needle EMG
EMG as a tool in motor pathophysiology
21/03/2017
1
Electromyography - conventional
Christian Krarup, MD DMSc FRCP FEANDepartment of Clinical Neurophysiology,
Rigshospitalet and University of Copenhagen,Denmark
Needle EMG
EMG as a tool in motor pathophysiology
16
21/03/2017
2
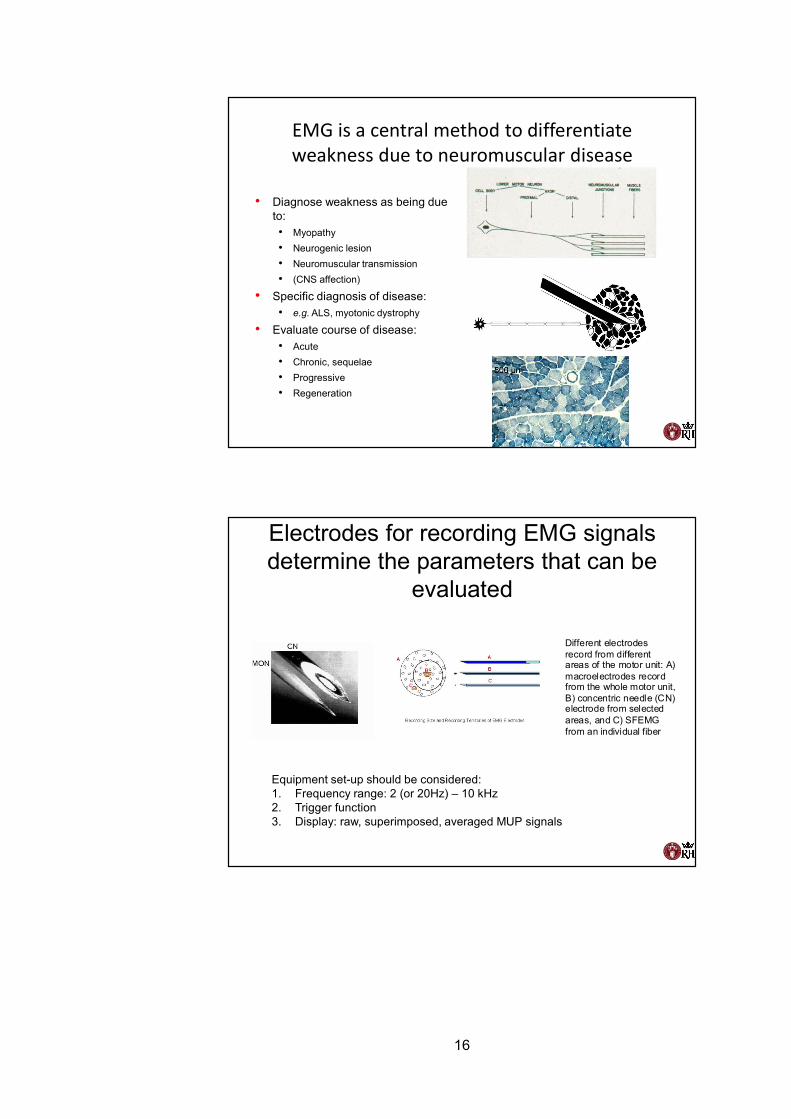
EMG is a central method to differentiate weakness due to neuromuscular disease
• Diagnose weakness as being due to:• Myopathy• Neurogenic lesion• Neuromuscular transmission• (CNS affection)
• Specific diagnosis of disease:• e.g. ALS, myotonic dystrophy
• Evaluate course of disease:• Acute• Chronic, sequelae• Progressive• Regeneration
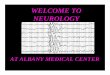
Electrodes for recording EMG signals determine the parameters that can be
evaluated
Different electrodes record from different areas of the motor unit: A) macroelectrodes record from the whole motor unit, B) concentric needle (CN) electrode from selected areas, and C) SFEMG from an individual fiber
Equipment set-up should be considered:1. Frequency range: 2 (or 20Hz) – 10 kHz2. Trigger function3. Display: raw, superimposed, averaged MUP signals
21/03/2017
2
EMG is a central method to differentiate weakness due to neuromuscular disease
• Diagnose weakness as being due to:• Myopathy• Neurogenic lesion• Neuromuscular transmission• (CNS affection)
• Specific diagnosis of disease:• e.g. ALS, myotonic dystrophy
• Evaluate course of disease:• Acute• Chronic, sequelae• Progressive• Regeneration
Electrodes for recording EMG signals determine the parameters that can be
evaluated
Different electrodes record from different areas of the motor unit: A) macroelectrodes record from the whole motor unit, B) concentric needle (CN) electrode from selected areas, and C) SFEMG from an individual fiber
Equipment set-up should be considered:1. Frequency range: 2 (or 20Hz) – 10 kHz2. Trigger function3. Display: raw, superimposed, averaged MUP signals
17
21/03/2017
3
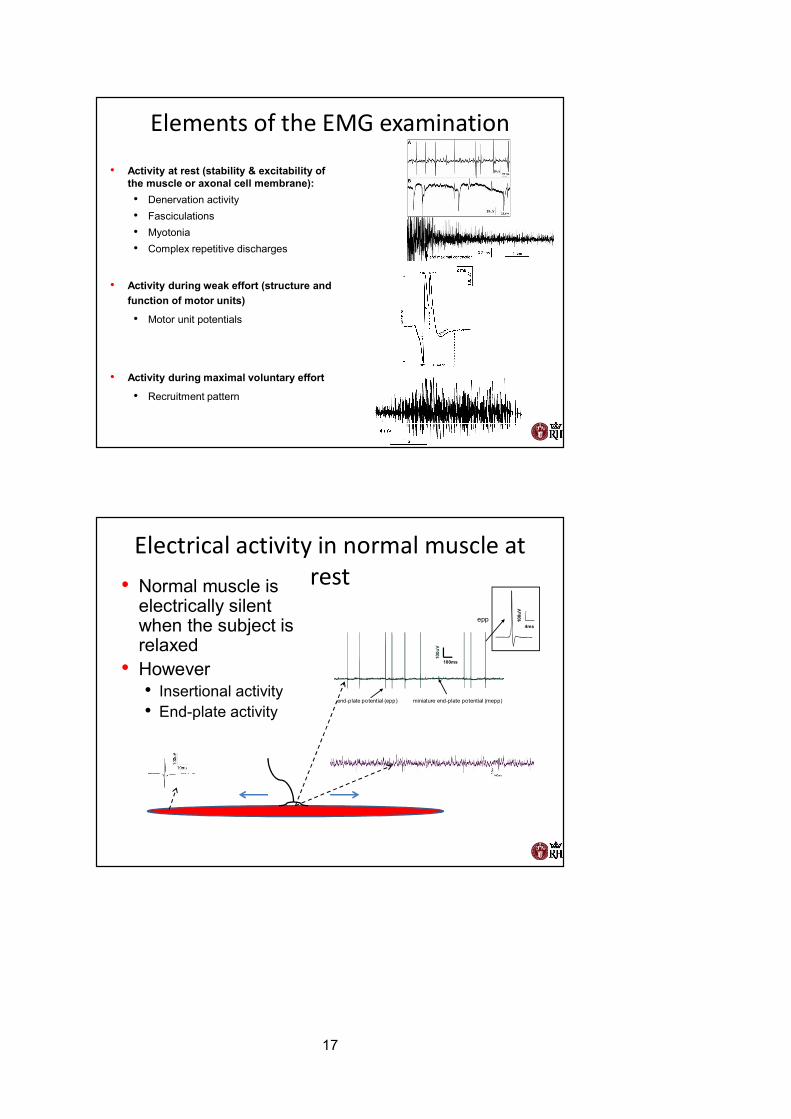
Elements of the EMG examination
• Activity at rest (stability & excitability of the muscle or axonal cell membrane):• Denervation activity• Fasciculations• Myotonia• Complex repetitive discharges
• Activity during weak effort (structure and function of motor units)
• Motor unit potentials
• Activity during maximal voluntary effort
• Recruitment pattern
Electrical activity in normal muscle at rest• Normal muscle is
electrically silentwhen the subject is relaxed
• However• Insertional activity• End-plate activity
4ms
100u
V
100ms
100u
V
miniature end-plate potential (mepp)end-plate potential (epp)
epp
21/03/2017
3
Elements of the EMG examination
• Activity at rest (stability & excitability of the muscle or axonal cell membrane):• Denervation activity• Fasciculations• Myotonia• Complex repetitive discharges
• Activity during weak effort (structure and function of motor units)
• Motor unit potentials
• Activity during maximal voluntary effort
• Recruitment pattern
Electrical activity in normal muscle at rest• Normal muscle is
electrically silentwhen the subject is relaxed
• However• Insertional activity• End-plate activity
4ms
100u
V
100ms
100u
V
miniature end-plate potential (mepp)end-plate potential (epp)
epp

18
21/03/2017
4
End-plate potentials (EPP), miniature end plate potentials (MEPP), fibrillation activity
30ms50
µV
Clin. Neurophysiol.
The motor unit• Anterior horn cell,
nerve fiber, muscle fibers
• Anterior horn cell in the CNS
• Great variation in ”innervation ratio”
21/03/2017
4
End-plate potentials (EPP), miniature end plate potentials (MEPP), fibrillation activity
30ms50
µV
Clin. Neurophysiol.
The motor unit• Anterior horn cell,
nerve fiber, muscle fibers
• Anterior horn cell in the CNS
• Great variation in ”innervation ratio”
19
21/03/2017
5
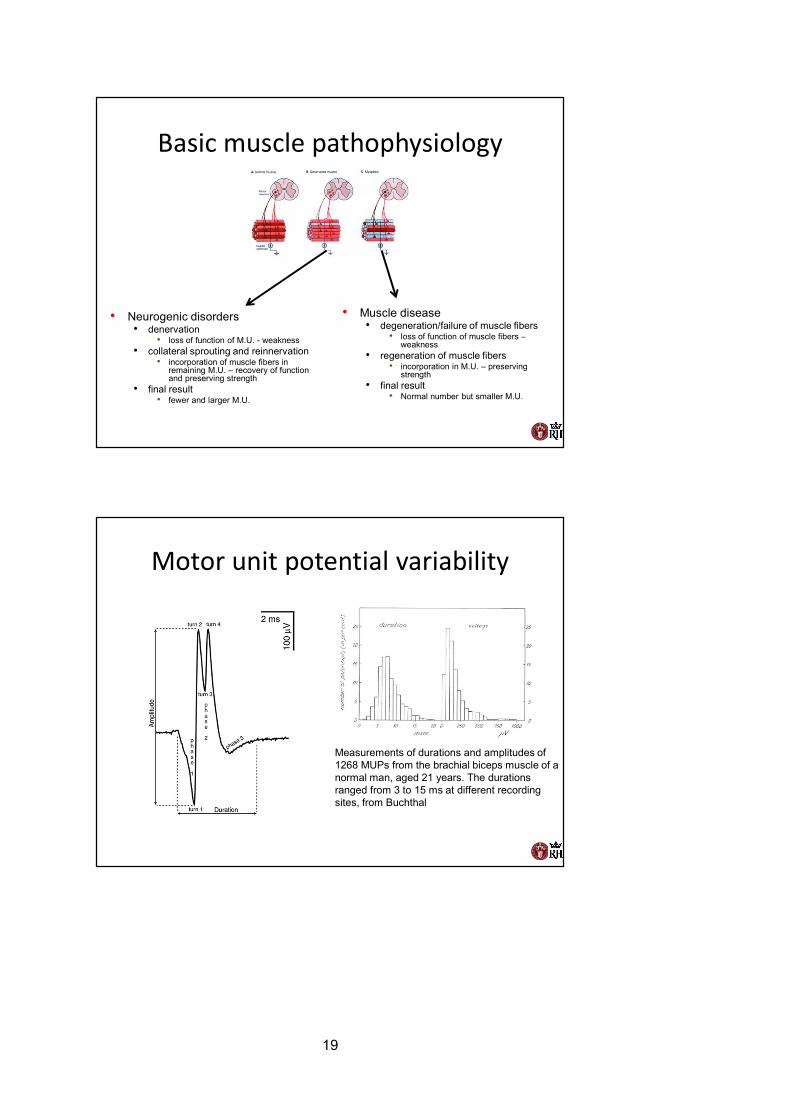
Basic muscle pathophysiology
• Muscle disease• degeneration/failure of muscle fibers
• loss of function of muscle fibers –weakness
• regeneration of muscle fibers• incorporation in M.U. – preserving
strength• final result
• Normal number but smaller M.U.
• Neurogenic disorders• denervation
• loss of function of M.U. - weakness• collateral sprouting and reinnervation
• incorporation of muscle fibers in remaining M.U. – recovery of function and preserving strength
• final result• fewer and larger M.U.
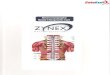
Motor unit potential variability
Measurements of durations and amplitudes of 1268 MUPs from the brachial biceps muscle of a normal man, aged 21 years. The durations ranged from 3 to 15 ms at different recording sites, from Buchthal
21/03/2017
5
Basic muscle pathophysiology
• Muscle disease• degeneration/failure of muscle fibers
• loss of function of muscle fibers –weakness
• regeneration of muscle fibers• incorporation in M.U. – preserving
strength• final result
• Normal number but smaller M.U.
• Neurogenic disorders• denervation
• loss of function of M.U. - weakness• collateral sprouting and reinnervation
• incorporation of muscle fibers in remaining M.U. – recovery of function and preserving strength
• final result• fewer and larger M.U.
Motor unit potential variability
Measurements of durations and amplitudes of 1268 MUPs from the brachial biceps muscle of a normal man, aged 21 years. The durations ranged from 3 to 15 ms at different recording sites, from Buchthal
20
21/03/2017
6
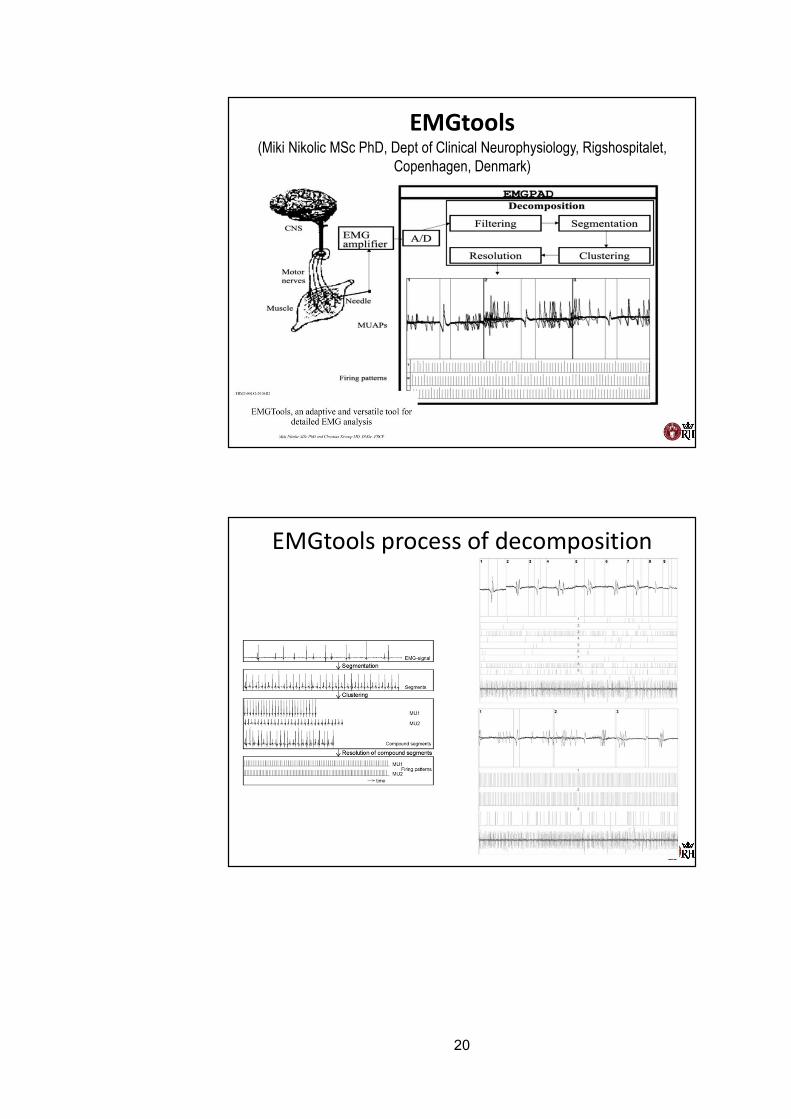
EMGtools(Miki Nikolic MSc PhD, Dept of Clinical Neurophysiology, Rigshospitalet,
Copenhagen, Denmark)
EMGtools process of decomposition
21/03/2017
6
EMGtools(Miki Nikolic MSc PhD, Dept of Clinical Neurophysiology, Rigshospitalet,
Copenhagen, Denmark)
EMGtools process of decomposition
21
21/03/2017
7
Clin. Neurophysiol.
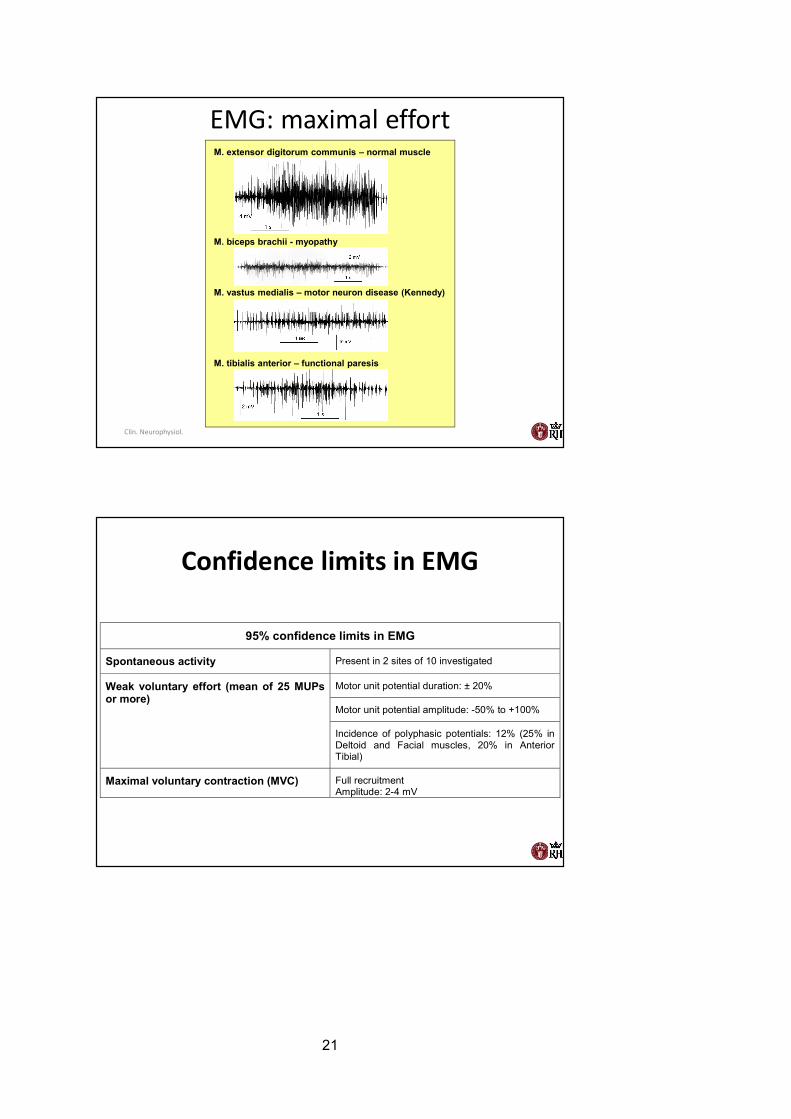
EMG: maximal effortM. extensor digitorum communis – normal muscle
M. biceps brachii - myopathy
M. vastus medialis – motor neuron disease (Kennedy)
M. tibialis anterior – functional paresis
Confidence limits in EMG
95% confidence limits in EMG
Spontaneous activity Present in 2 sites of 10 investigated
Weak voluntary effort (mean of 25 MUPs or more)
Motor unit potential duration: ± 20%
Motor unit potential amplitude: -50% to +100%
Incidence of polyphasic potentials: 12% (25% in Deltoid and Facial muscles, 20% in Anterior Tibial)
Maximal voluntary contraction (MVC) Full recruitment Amplitude: 2-4 mV
21/03/2017
7
Clin. Neurophysiol.
EMG: maximal effortM. extensor digitorum communis – normal muscle
M. biceps brachii - myopathy
M. vastus medialis – motor neuron disease (Kennedy)
M. tibialis anterior – functional paresis
Confidence limits in EMG
95% confidence limits in EMG
Spontaneous activity Present in 2 sites of 10 investigated
Weak voluntary effort (mean of 25 MUPs or more)
Motor unit potential duration: ± 20%
Motor unit potential amplitude: -50% to +100%
Incidence of polyphasic potentials: 12% (25% in Deltoid and Facial muscles, 20% in Anterior Tibial)
Maximal voluntary contraction (MVC) Full recruitment Amplitude: 2-4 mV
22
21/03/2017
8
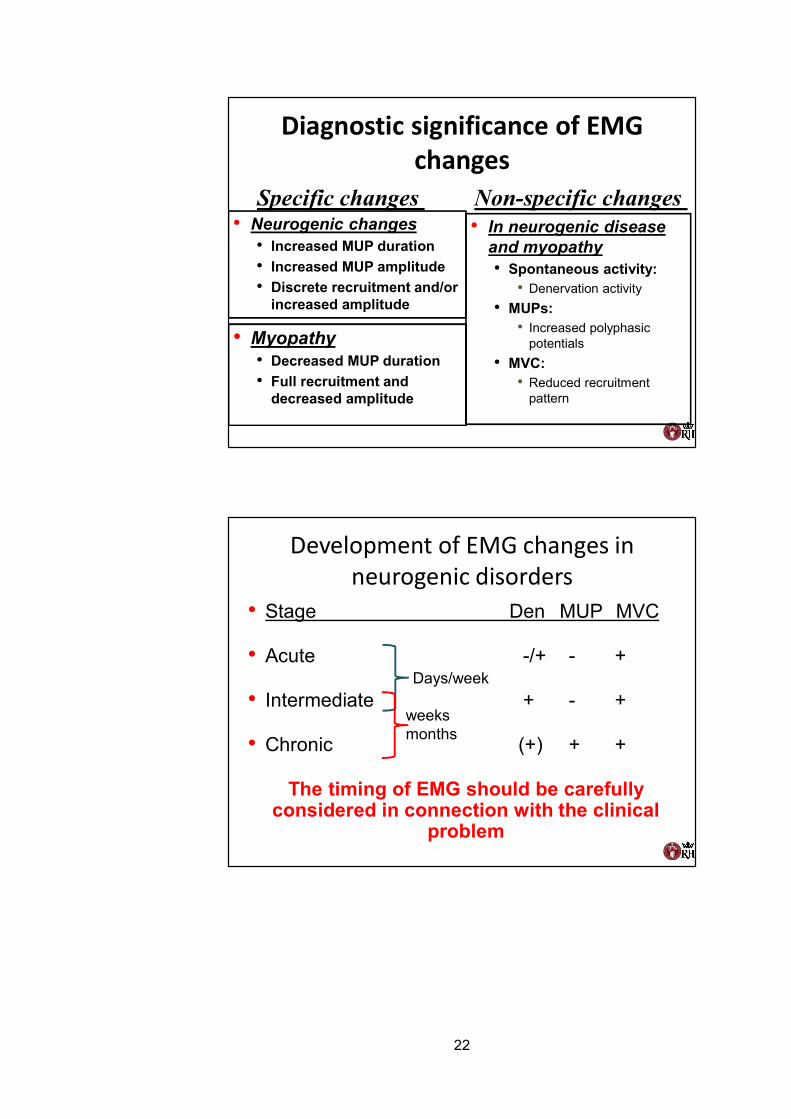
Diagnostic significance of EMG changes
• In neurogenic disease and myopathy• Spontaneous activity:
• Denervation activity• MUPs:
• Increased polyphasic potentials
• MVC:• Reduced recruitment
pattern
• Neurogenic changes• Increased MUP duration• Increased MUP amplitude• Discrete recruitment and/or
increased amplitude
• Myopathy• Decreased MUP duration• Full recruitment and
decreased amplitude
Specific changes Non-specific changes
Development of EMG changes in neurogenic disorders
• Stage Den MUP MVC
• Acute -/+ - +
• Intermediate + - +
• Chronic (+) + +
The timing of EMG should be carefully considered in connection with the clinical
problem
Days/week
weeksmonths
21/03/2017
8
Diagnostic significance of EMG changes
• In neurogenic disease and myopathy• Spontaneous activity:
• Denervation activity• MUPs:
• Increased polyphasic potentials
• MVC:• Reduced recruitment
pattern
• Neurogenic changes• Increased MUP duration• Increased MUP amplitude• Discrete recruitment and/or
increased amplitude
• Myopathy• Decreased MUP duration• Full recruitment and
decreased amplitude
Specific changes Non-specific changes
Development of EMG changes in neurogenic disorders
• Stage Den MUP MVC
• Acute -/+ - +
• Intermediate + - +
• Chronic (+) + +
The timing of EMG should be carefully considered in connection with the clinical
problem
Days/week
weeksmonths
23
21/03/2017
9
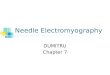
MUP analysis in ALS
100ms
1m
V
Weakness in 76-year-old manEMG of the left Brachial Biceps
1s
100
µV
20ms
100
µV
Denervation activity
200ms
1mV
Maximal voluntary effort
Motor unit potentials at weak effort
1405
9/20
48/1
/2,c
h:1
100 m
V
10 ms
9.2 ms171 mVSimple
1405
9/20
48/1
/3,c
h:1
100 m
V
10 ms
7.5 ms134 mVSimple
1405
9/20
48/1
/4,c
h:1
100 m
V
10 ms
6.7 ms96 mV
Simple
1405
9/20
48/1
/5,c
h:1
100 m
V
10 ms
7.5 ms94 mV
Simple
1405
9/20
48/1
/6,c
h:1
100 m
V
10 ms
7.3 ms89 mV
Simple
1405
9/20
48/1
/1,c
h:2
100 m
V
10 ms
8.7 ms809 mVSimple
1405
9/20
48/1
/2,c
h:2
100 m
V
10 ms
10.0 ms524 mVSimple
1405
9/20
48/1
/3,c
h:2
100 m
V
10 ms
12.2 ms514 mVSimple
1405
9/20
48/1
/4,c
h:2
100 m
V
10 ms
8.5 ms487 mVSimple
1405
9/20
48/1
/5,c
h:2
100 m
V
10 ms
9.0 ms388 mVSimple
1405
9/20
48/1
/6,c
h:2
100 m
V
10 ms
8.8 ms374 mVSimple
1405
9/20
48/1
/7,c
h:2
100 m
V
10 ms
8.5 ms275 mV
Poly
1405
9/20
48/1
/8,c
h:2
100 m
V
10 ms
8.5 ms150 mVSimple
1405
9/20
48/1
/9,c
h:2
100 m
V
10 ms
9.2 ms94 mV
Simple
1405
9/20
48/2
/1,c
h:1
100 m
V
10 ms
8.1 ms224 mV
Poly
1405
9/20
48/2
/2,c
h:1
100 m
V
10 ms
7.6 ms167 mVSimple
1405
9/20
48/2
/3,c
h:1
100 m
V
10 ms
12.3 ms153 mV
Poly
1405
9/20
48/2
/4,c
h:1
100 m
V
10 ms
10.9 ms93 mVPoly
1405
9/20
48/2
/5,c
h:1
100 m
V
10 ms
8.3 ms42 mV
Simple
1405
9/20
48/2
/1,c
h:2
100 m
V
10 ms
11.3 ms512 mVSimple
1405
9/20
48/2
/2,c
h:2
100 m
V
10 ms
11.8 ms416 mVSimple
1405
9/20
48/2
/3,c
h:2
100 m
V
10 ms
10.0 ms268 mVSimple
1405
9/20
48/2
/4,c
h:2
100 m
V
10 ms
7.1 ms217 mVSimple
1405
9/20
48/2
/5,c
h:2
100 m
V
10 ms
8.2 ms116 mVSimple
1405
9/20
48/2
/6,c
h:2
100
mV
10 ms
8.0 ms100 mVSimple
1405
9/20
48/3
/1,c
h:1
100
mV
10 ms
9.7 ms237 mV
Poly
1405
9/20
48/3
/2,c
h:1
100 m
V
10 ms
8.6 ms87 mVPoly
1405
9/20
48/3
/3,c
h:1
100 m
V
10 ms
9.0 ms67 mV
Simple
1405
9/20
48/3
/4,c
h:1
100 m
V
10 ms
10.9 ms49 mV
Simple
1405
9/20
48/3
/1,c
h:2
100 m
V
10 ms
14.6 ms331 mV
Poly
1405
9/20
48/3
/2,c
h:2
100 m
V
10 ms
5.2 ms213 mVSimple
1405
9/20
48/3
/3,c
h:2
100 m
V
10 ms
5.4 ms131 mVSimple
1405
9/20
48/3
/4,c
h:2
100 m
V
10 ms
5.7 ms69 mVPoly
1405
9/20
48/3
/5,c
h:2
100
mV
10 ms
8.0 ms66 mV
Simple
1405
9/20
48/4
/1,c
h:1
100
mV
10 ms
9.7 ms307 mVSimple
1405
9/20
48/4
/2,c
h:1
100 m
V
10 ms
8.3 ms261 mVSimple
1405
9/20
48/4
/3,c
h:1
100 m
V
10 ms
11.6 ms141 mVSimple
1405
9/20
48/4
/4,c
h:1
100 m
V
10 ms
6.7 ms78 mV
Simple
1405
9/20
48/4
/1,c
h:2
100 m
V
10 ms
8.8 ms691 mVSimple
1405
9/20
48/4
/2,c
h:2
100 m
V
10 ms
11.4 ms645 mV
Poly
1405
9/20
48/4
/3,c
h:2
100 m
V
10 ms
9.4 ms354 mVSimple
1405
9/20
48/4
/4,c
h:2
100 m
V
10 ms
8.4 ms149 mVSimple
1405
9/20
48/4
/5,c
h:2
100 m
V
10 ms
7.7 ms128 mVSimple
1405
9/20
48/5
/1,c
h:1
100 m
V
10 ms
7.3 ms88 mV
Simple
1405
9/20
48/5
/2,c
h:1
100 m
V
10 ms
6.5 ms66 mV
Simple
1405
9/20
48/5
/3,c
h:1
100 m
V
10 ms
7.3 ms61 mV
Simple
1405
9/20
48/5
/4,c
h:1
100 m
V
10 ms
6.8 ms57 mV
Simple
1405
9/20
48/5
/5,c
h:1
100 m
V
10 ms
7.4 ms46 mV
Simple
1405
9/20
48/5
/6,c
h:1
100 m
V
10 ms
7.3 ms28 mV
Simple
1405
9/20
48/5
/1,c
h:2
100 m
V
10 ms
7.9 ms141 mV
Poly
1405
9/20
48/5
/2,c
h:2
100 m
V
10 ms
8.2 ms106 mV
Poly
1405
9/20
48/5
/3,c
h:2
100 m
V
10 ms
7.8 ms93 mVPoly
1405
9/20
48/5
/4,c
h:2
100 m
V
10 ms
10.3 ms83 mV
Simple
1405
9/20
48/1
/1,c
h:1
100 m
V
10 ms
8.1 ms279 mVSimple
21/03/2017
9
MUP analysis in ALS
100ms
1m
V
Weakness in 76-year-old manEMG of the left Brachial Biceps
1s
100
µV
20ms
100
µV
Denervation activity
200ms
1mV
Maximal voluntary effort
Motor unit potentials at weak effort
1405
9/20
48/1
/2,c
h:1
100 m
V
10 ms
9.2 ms171 mVSimple
1405
9/20
48/1
/3,c
h:1
100 m
V
10 ms
7.5 ms134 mVSimple
1405
9/20
48/1
/4,c
h:1
100 m
V
10 ms
6.7 ms96 mV
Simple
1405
9/20
48/1
/5,c
h:1
100 m
V
10 ms
7.5 ms94 mV
Simple
1405
9/20
48/1
/6,c
h:1
100 m
V
10 ms
7.3 ms89 mV
Simple
1405
9/20
48/1
/1,c
h:2
100 m
V
10 ms
8.7 ms809 mVSimple
1405
9/20
48/1
/2,c
h:2
100 m
V
10 ms
10.0 ms524 mVSimple
1405
9/20
48/1
/3,c
h:2
100 m
V
10 ms
12.2 ms514 mVSimple
1405
9/20
48/1
/4,c
h:2
100 m
V
10 ms
8.5 ms487 mVSimple
1405
9/20
48/1
/5,c
h:2
100 m
V
10 ms
9.0 ms388 mVSimple
1405
9/20
48/1
/6,c
h:2
100 m
V
10 ms
8.8 ms374 mVSimple
1405
9/20
48/1
/7,c
h:2
100 m
V
10 ms
8.5 ms275 mV
Poly
1405
9/20
48/1
/8,c
h:2
100 m
V
10 ms
8.5 ms150 mVSimple
1405
9/20
48/1
/9,c
h:2
100 m
V
10 ms
9.2 ms94 mV
Simple
1405
9/20
48/2
/1,c
h:1
100 m
V
10 ms
8.1 ms224 mV
Poly
1405
9/20
48/2
/2,c
h:1
100 m
V
10 ms
7.6 ms167 mVSimple
1405
9/20
48/2
/3,c
h:1
100 m
V
10 ms
12.3 ms153 mV
Poly
1405
9/20
48/2
/4,c
h:1
100 m
V
10 ms
10.9 ms93 mVPoly
1405
9/20
48/2
/5,c
h:1
100 m
V
10 ms
8.3 ms42 mV
Simple
1405
9/20
48/2
/1,c
h:2
100 m
V
10 ms
11.3 ms512 mVSimple
1405
9/20
48/2
/2,c
h:2
100 m
V
10 ms
11.8 ms416 mVSimple
1405
9/20
48/2
/3,c
h:2
100 m
V
10 ms
10.0 ms268 mVSimple
1405
9/20
48/2
/4,c
h:2
100 m
V
10 ms
7.1 ms217 mVSimple
1405
9/20
48/2
/5,c
h:2
100 m
V
10 ms
8.2 ms116 mVSimple
1405
9/20
48/2
/6,c
h:2
100
mV
10 ms
8.0 ms100 mVSimple
1405
9/20
48/3
/1,c
h:1
100
mV
10 ms
9.7 ms237 mV
Poly
1405
9/20
48/3
/2,c
h:1
100 m
V
10 ms
8.6 ms87 mVPoly
1405
9/20
48/3
/3,c
h:1
100 m
V
10 ms
9.0 ms67 mV
Simple
1405
9/20
48/3
/4,c
h:1
100 m
V
10 ms
10.9 ms49 mV
Simple
1405
9/20
48/3
/1,c
h:2
100 m
V
10 ms
14.6 ms331 mV
Poly
1405
9/20
48/3
/2,c
h:2
100 m
V
10 ms
5.2 ms213 mVSimple
1405
9/20
48/3
/3,c
h:2
100 m
V
10 ms
5.4 ms131 mVSimple
1405
9/20
48/3
/4,c
h:2
100 m
V
10 ms
5.7 ms69 mVPoly
1405
9/20
48/3
/5,c
h:2
100
mV
10 ms
8.0 ms66 mV
Simple
1405
9/20
48/4
/1,c
h:1
100
mV
10 ms
9.7 ms307 mVSimple
1405
9/20
48/4
/2,c
h:1
100 m
V
10 ms
8.3 ms261 mVSimple
1405
9/20
48/4
/3,c
h:1
100 m
V
10 ms
11.6 ms141 mVSimple
1405
9/20
48/4
/4,c
h:1
100 m
V
10 ms
6.7 ms78 mV
Simple
1405
9/20
48/4
/1,c
h:2
100 m
V
10 ms
8.8 ms691 mVSimple
1405
9/20
48/4
/2,c
h:2
100 m
V
10 ms
11.4 ms645 mV
Poly
1405
9/20
48/4
/3,c
h:2
100 m
V
10 ms
9.4 ms354 mVSimple
1405
9/20
48/4
/4,c
h:2
100 m
V
10 ms
8.4 ms149 mVSimple
1405
9/20
48/4
/5,c
h:2
100 m
V
10 ms
7.7 ms128 mVSimple
1405
9/20
48/5
/1,c
h:1
100 m
V
10 ms
7.3 ms88 mV
Simple
1405
9/20
48/5
/2,c
h:1
100 m
V
10 ms
6.5 ms66 mV
Simple
1405
9/20
48/5
/3,c
h:1
100 m
V
10 ms
7.3 ms61 mV
Simple
1405
9/20
48/5
/4,c
h:1
100 m
V
10 ms
6.8 ms57 mV
Simple
1405
9/20
48/5
/5,c
h:1
100 m
V
10 ms
7.4 ms46 mV
Simple
1405
9/20
48/5
/6,c
h:1
100 m
V
10 ms
7.3 ms28 mV
Simple
1405
9/20
48/5
/1,c
h:2
100 m
V
10 ms
7.9 ms141 mV
Poly
1405
9/20
48/5
/2,c
h:2
100 m
V
10 ms
8.2 ms106 mV
Poly
1405
9/20
48/5
/3,c
h:2
100 m
V
10 ms
7.8 ms93 mVPoly
1405
9/20
48/5
/4,c
h:2
100 m
V
10 ms
10.3 ms83 mV
Simple
1405
9/20
48/1
/1,c
h:1
100 m
V
10 ms
8.1 ms279 mVSimple