-
8/2/2019 Controversies PEE ClinObstGyn05
1/18
Controversies Withthe Diagnosis andManagement of
HELLP SyndromeJOHN M. OBRIEN, MD and JOHN R. BARTON, MD
Perinatal Diagnostic Center, Central Baptist Hospital,Lexington,
Kentucky
IntroductionThe spectrum of disease resulting from the
pathophysiology of preeclampsia continuesto challenge the
diagnostic acumen of clini-
cians. One of preeclampsias various mani-festations includes the
specific entity ofHELLP syndrome. Recently, investigatorshave
provided evidence some cases ofHELLP syndrome represent a
vasculopathymediated by an abnormal concentration ofvascular growth
factors.1 However, untilthe underlying etiology for preeclampsia
is
better defined and testing for such factorsis commonplace,
controversies in the diag-nosis and management of HELLP
syndromewill persist as its numerous clinical findingswill lead to
varied inpressions of severityand to varied thresholds for
intervention.
Controversies in DiagnosisThe preeclamptic patient with the
constella-tion of hemolysis, hepatic dysfunction, and
low platelets has been described in the liter-ature for decades
with early accurate descrip-tions by Prichard et al and Chesley.2,3
It wasnot until 1982, however, when Weinstein
coined the acronym HELLP syndrome (he-molysis, elevated liver
enzymes, and low
platelets) that clinicians could more easilyrecognize and
discuss this group of patientswith remarkable hepatic involvement
bysevere preeclampsia.4
Investigations into the pathophysiologyof preeclampsia, and
specifically HELLPsyndrome, have revealed a disorder charac-terized
by hepatic endothelial disruptionfollowed by platelet activation,
aggregation,and consumption ultimately resulting in dis-tal
ischemia and hepatocyte death.5,6 Thisvasculopathy can be limited
to a hepaticsegment or occur diffusely throughout theliver. Most
commonly, HELLP syndromeinvolves smaller terminal arterioles
yieldinga process with characteristic histologic fea-tures. The
classic hepatic lesion associa-ted with HELLP syndrome is
periportal orfocal parenchymal necrosis in which hyalinedeposits of
fibrin-like material can be seen
Correspondence: John M. OBrien, MD, Director,
PerinatalDiagnostic Center, Central Baptist Hospital, 1740
Nicholas-villeRoad, Lexington,KY 40503.E-mail:[email protected]
CLINICAL OBSTETRICS AND GYNECOLOGY / VOLUME 48 / NUMBER 2 / JUNE
2005
CLINICAL OBSTETRICS AND GYNECOLOGYVolume 48, Number 2, 460477
2005, Lippincott Williams & Wilkins
460
-
8/2/2019 Controversies PEE ClinObstGyn05
2/18
in the sinusoids.79 Alternatively and lessfrequently,
larger-vessel disease can impactwider vascular distributions in the
liver withmore catastrophic outcomes such as hepaticinfarction or
subcapsular hematoma. Thisrare large-vessel disease is more readily
vis-ible by imaging studies such as magneticresonance imaging (MRI)
or computed to-mography (CT) scanning and is associatedwith worse
laboratory values indicating moredramatic hepatic
dysfunction.10
The greatest controversy involving HELLP
syndrome is in the diagnosis of the condi-tion. The syndrome
outlined by Weinsteinin the early 1980s provided a descriptionof
the disease process and gave cliniciansan easier framework to
understand the path-ophysiology. Namely, his group of 29 pa-tients
with severe preeclampsia/eclampsiamanifested more pronounced
hepatic in-volvement rather than primarily cerebral orrenal
disease. Later, Sibai et al establishedlaboratory criteria for the
diagnosis and pro-vided standards for subsequent discussionsin the
literature (see Table 1).11 In his clas-
sification, Sibai defined laboratory abnor-malities sufficient
for the diagnosis of eachelement of the syndrome: hemolysis by
anabnormal peripheral smear, elevated biliru-
bin .1.2 mg/dL, or elevated lactate dehy-drogenase (LDH) .600
U/L; elevated liverenzymes by an aspartate aminotransferase(AST)
.70 IU/L (which was greater than2 standard deviations of normal)
and lactatedehydrogenase (LDH) .600 U/L; and low
platelets defined as 100,000/mm3, as this valuewas standard in
other fields of medicine.
Martin et al also attempted to classify thedisease noting an
increase in untoward out-comes, including cardiopulmonary,
centralnervous system, and renal dysfunction, asthe degree of
thrombocytopenia worsened.12
In their retrospective review of 302 casesof HELLP syndrome,
they defined class 1HELLP syndrome as a platelet nadir
below50,000/mm3, whereas those with platelet na-dirs between 51,000
and 100,000/mm3 weredefined as class 2. Class 3 HELLP syn-drome
represented a newly classified group
of patients with hepatocyte death buta higher platelet count
nadir, 101,000 to150,000/mm3. In this series, thrombocyto-
penia in women with HELLP syndromewas found to represent a
marker for moreextensive endothelial disruption and hepato-cyte
death as peak aminotransferase valuescorrelated well with platelet
nadirs. Stillothers have offered differing criteria forthe
diagnosis of HELLP syndrome to Sibaisand Martins, each assessing
varyingdegrees of hepatic involvement as evidenced
by liver function test abnormalities to repre-
sent thresholds for diagnosis (see Table1).13,14 Despite the
best of intentions, thesediffering depictions of HELLP syndromewith
differing criteria for platelet countand liver function test
abnormalities havecreated a rationale for questioning findingsof
individual reports and have likely con-fused clinicians.
Compared with the 1980s, when Weinsteinfirst coined the term,
HELLP syndrome andits variants are now more commonly recog-nized
earlier when platelet consumption yields
TABLE 1. Classifications of HELLP Syndrome
Platelet Count AST LDH
Sibai et al11 ,100,000/mm3 $70 U/L $600 U/LMartin et al12
,150,000/mm3 $40 U/L $600 U/Lvan Pampus13 ,100,000/mm3 .50 U/L .600
U/LVisser and Wallenburg14 ,100,000/mm3 .30 U/L *
* Not included in their criteria.
Reprinted from Sibai BM. Diagnosis, controversies, and
management of the syndrome of hemolysis, elevated liver enzymes,
and low platelet count. Obstet Gynecol. 2004;103:981991.
AST, aspartate aminotransferase; LDH, lactic dehydrogenase.
Controversies With HELLP Syndrome 461
-
8/2/2019 Controversies PEE ClinObstGyn05
3/18
milder degrees of thrombocytopenia and ele-vated liver function
tests document hepaticischemia. It appears, however, the same
path-ophysiology is ongoing whether the patienthas evidence of
thrombocytopenia and elevatedliver function tests alone or whether
schisto-cytes are present in the peripheral smear, theserum
bilirubin is elevated, or other abnor-malities such as coagulopathy
or renal insuf-ficiency have unfolded. With greater involve-ment of
the endothelium of the liver by
preeclampsia, more red blood cells are he-
molyzed and more hepatic ischemia re-sults with the combination
yielding higher
bilirubin levels and impaired coagulationstudies.
Thus, the primary controversy in the di-agnosis of HELLP
syndrome has been in
precisely defining when in the spectrumof the hepatic
involvement with preeclamp-sia does the true HELLP syndrome
de-velop. Some patients have been termed ashaving partial HELLP
syndrome, ELLPsyndrome, or class 3 HELLP syndrome.These women are
also at risk for signif-
icant maternal and fetal morbidity as aresult of this same
pathophysiology despitecriticisms that elements of the true
dis-ease may be missing. In a study by VanPampus et al, 10% of
women with ELLPsyndrome were identified as having
seriouscomplications, including eclampsia, cerebralischemia, and
abruptio placentae comparedwith a 24% rate for women with
trueHELLP.13 In a study by Abramovici et al,the rate of fetal
distress (13% vs. 18%) andintrauterine growth restriction (28%
vs.31%) was lower in women with HELLP syn-drome versus the partial
HELLP group.15
These data do not demonstrate that a suffi-ciently different
outcome occurs in patientswith hepatic involvement by
preeclampsiato justify subdividing these patients intominute
subclassifications. Unfortunately, itappears once severe
preeclampsia has man-ifested remarkable end-organ
involvement,adverse renal, central nervous system, and
pulmonary complications can arise and should be anticipated.
For diagnostic criteria to be most useful,they should be based
on objective criteria,testing should be readily available, and
theresults of these tests should not be subjectto interpretation.
These criteria should alsoattempt to identify earlier stages of the
dis-ease process rather than limiting the diagno-sis to a small
subset of only the most severecases. Finally, the definitions
should be easyto use for the clinician.
The diagnosis of HELLP syndrome ismade by laboratory parameters
alone, al-
though supporting typical findings of pre-eclampsia, including
hypertension and pro-teinuria, help rule out other potential
imita-tors (see the next section on differentialdiagnosis).
Laboratory evaluation should in-clude a complete blood count with
plateletcount, a peripheral smear, coagulation stud-ies, serum AST,
creatinine, glucose, biliru-
bin, and LDH levels. Ideally, the laboratoryparameters for HELLP
syndrome should beintuitive,easytoremember,andconsistentbe-tween
laboratories. Of the laboratory studiesroutinely obtained for
diagnostic purposes,
platelet count and liver function tests arethe best standardized
and can fulfill thesecriteria.
The platelet count historically used to di-agnose
thrombocytopenia is ,100,000/mm3
and is the threshold most consistent acrossall specialties of
medicine. The liver func-tion tests profile we use is that
presented
by Sibai as AST or ALT. 2 times the upperlimit of normal or 70
U/L. To assess thedegree of hemolysis, we do not evaluate
peripheral smears ourselves or ask hematol-ogists/pathologists
to provide middle-of-the-night evaluations. We do use an LDH
valueto give an indication for hemolysis as sug-gested by Sibai. We
are also cognizant, how-ever, that an elevated LDH, most of the
time,also reflects hepatocyte destruction in addi-tion to
hemolysis. Therefore, in our opinion,a complete blood count and
metabolic pro-file are readily available, rapidly performedtests,
which allow recognition and definitionof severe involvement of
liver parenchyma
by preeclampsia. The alphabet soup present
462 OBrien and Barton
-
8/2/2019 Controversies PEE ClinObstGyn05
4/18
in the literature attempting to differentiateHELLP versus ELLP
versus EL versusHEL syndrome, or partial HELLP versusHELLP, is of
limited value when attemptingto treat a patient identified with
significant he-
patic involvement from severe preeclampsia.We anticipate that
expert groups focused onthe care for women with hypertensive
disor-ders in pregnancy can better define the clinicalcondition of
hepatic involvement by pre-eclampsia and eliminate the current
confusionand controversy.
Differential DiagnosisSibai has noted that most patients
withHELLP syndrome present preterm withhypertension, and
proteinuria, and reportepigastric or right upper quadrant
pain.16
Unfortunately, however, other patients pres-ent with only nausea
or vomiting, and stillothers may have nonspecific
viral-likesymptoms. In Weinsteins second report,17
nausea or vomiting and epigastric pain werethe most common
symptoms. A pregnantwoman in the late second or early
thirdtrimester with right upper quadrant pain,epigastric pain, or
identified hepatic dys-function should be considered as havingHELLP
syndrome until other elements ofthe differential diagnosis are
excluded (seeTable 2). Epigastric pain may antedate the
laboratory abnormalities of HELLP syn-drome by several hours,
leading cliniciansto question initial impressions. Symptomsof upper
quadrant pain without laboratoryabnormalities may lead errantly to
diagnosesof gastritis or gallbladder disease. Reevalu-ation of
laboratory studies in 4 to 6 hoursafter onset of symptoms usually
confirmsan initial clinical suspicion of HELLPsyndrome.
Patients with HELLP syndrome frequentlydemonstrate significant
weight gain with
generalized edema. However, severe hyper-tension (systolic blood
pressure$160 mm Hg,diastolic blood pressure $110 mm Hg) isnot a
constant finding in HELLP syndrome.Although 69% of the 112 patients
studied bySibai et al had a diastolic blood pressure$110 mm Hg at
admission to the hospital,15% had a diastolic blood pressure of#90
mm Hg. In Weinsteins5 initial report,less than half (13) had an
admission blood
pressure$160/110 mm Hg. Thus, hyperten-sion is not obligatory to
diagnose HELLPsyndrome. More significant renal involve-
ment by preeclampsia compared with hepaticdisease appears better
correlated with the se-verity of hypertension.
Once laboratory abnormalities sufficientto diagnose HELLP
syndrome are observed,other hepatopathies may be considered
andeliminated as possibilities. Concomitant hy-
poglycemia, coagulopathy, elevated ammo-nia level, and renal
dysfunction are associatedwith acute fatty liver of pregnancy.
Cerebraldysfunction, fever, and rash may be part ofthrombotic
thrombocytopenic purpura. He-molytic uremic syndrome is primarily a
renaldisease in children and is related to infectionwith
Escherichia coli. In adults, almost allcases develop in the
postpartum period. Exac-erbation of systemic lupus erythematosus
withnephritis can also mimic severe preeclampsia.The clinical
manifestations and laboratoryfindings of the various conditions
presentedin Table 2 can be differentiated from severe
preeclampsia. Occasionally, however, the timecourse of the
condition and prompt postpar-tum resolution of laboratory studies
are the
TABLE 2. Medical and Surgical Disorders Potentially ConfusedWith
HELLP Syndrome
Acute fatty liveror pregnancy
Hyperemesis gravidarumIdiopathic thrombocytopenia
AppendicitisCholestasis of
pregnancy
Kidney stonesPeptic ulcerPyelonephritis
Diabetes insipidus Systemic lupus erythematosusGallbladder
diseaseGastroenteritis
Thromboticthrombocytopenic purpura
Glomerulonephritis Viral hepatitisHemolytic uremic
syndromeHepatic
encephalopathy
Controversies With HELLP Syndrome 463
-
8/2/2019 Controversies PEE ClinObstGyn05
5/18
only means to determine the etiology for ma-ternal disease.
Finally, clinicians should be familiar withthe various
endothelial vascular organs thatcan be affected by preeclampsia.
Althoughinvolvement in the renal and hepatic vesselsis most common,
other vessels potentiallyaffected include the cerebral, cardiac,
and
pulmonary. Involvement by this vasculop-athy of these organs can
yield concomitanteclampsia, myocardial dysfunction, and pul-monary
edema, and acute respiratory dis-
tress syndrome, adding to the diagnosticchallenges.
Management ControversiesThe diagnosis of HELLP syndrome has
long
been recognized as heralding the need foraggressive,
standardized therapies, includ-ing magnesium sulfate
administration, anti-hypertensive therapy, and delivery to
reduceassociated maternal morbidity and mortality(see Table 3).18
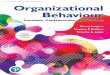
Several critical steps are in-volved in the management of these
casesand are summarized in Figure 1. This check-
list for the management of the condition pro-vides an orderly
sequential approach.
The clinical course of women withHELLP syndrome is usually
characterized
by progressive and sometimes sudden dete-rioration in maternal
and fetal conditions.Therefore, patients with suspected diagnosisof
HELLP syndrome should be hospitalizedimmediately and observed in a
labor and de-livery unit. The first priority is to assess
andstabilize the maternal condition, particularlycoagulation
abnormalities. Patients with
HELLP syndrome who are remote fromterm should be referred to a
tertiary carecenter.
Such patients should be managed as hav-ing severe preeclampsia
and should initiallyreceive intravenous (IV) magnesium sulfateas
prophylaxis against seizures and antihy-
pertensive medications to keep systolicblood pressure below 160
mm Hg and/or di-astolic blood pressure below 105 mm Hg.19
This can be achieved with a 5-mg bolus doseof hydralazine, to be
repeated as neededevery 15 to 20 minutes for a maximum dose
of 20 mg per hour. Blood pressure is recordedevery 15 minutes
during therapy and everyhour once the desired values are
achieved.If hydralazine does not lower blood pressureadequately
and/or if maternal side effectssuch as tachycardia or headaches
develop,another drug such as labetalol or nifedipinecan be used.
The recommended dose oflabetalol is 20 to 40 mg IV every 10 to
15minutes for a maximum of 220 mg over1 hour, and the dose of
nifedipine is 10 to20 mg orally every 30 minutes for a maxi-mum
dose of 50 mg over 1 hour. During theobservation period, maternal
and fetal con-ditions are assessed.
The recommended regimen of magne-sium sulfate is a loading dose
of 6 g givenover 20 minutes followed by a maintenancedose of 2 g
per hour as a continuous IV so-lution. Magnesium sulfate is
initiated at the
beginning of the observation period andthen continued during
labor and for at least24 hours postpartum. The next step is
toevaluate fetal well-being using the nonstress
TABLE 3. Serious Maternal Complicationsin 442 Patients With
HELLP Syndrome
Complication No. Percent
Disseminated intravascularcoagulopathy 92 21
Abruptio placentae 69 16Acute renal failure 33 8Severe ascites
32 8
Pulmonary edema 26 6Pleural effusions 26 6Cerebral edema 4
1Retinal detachment 4 1Laryngeal edema 4 1Subcapsular liver
hematoma 4 1Acute respiratory distress
syndrome 3 1Death, maternal 4 1
Reprinted from Sibai BM. Diagnosis and management of
gesta-tional hypertension and preeclampsia. Obstet Gynecol.
2003;102:181192.
464 OBrien and Barton
-
8/2/2019 Controversies PEE ClinObstGyn05
6/18
test or biophysical profile, as well as to ob-tain
ultrasonographic biometry for assess-ment of possible intrauterine
growth retarda-tion. Finally, a decision must be made as towhether
immediate delivery is indicated.
Steroids and the Managementof HELLP SyndromeSeveral
retrospective studies have demon-strated glucocorticoids can also
impact the
maternal condition in patients with HELLPsyndrome, thereby
adding another newerintervention to this armementarium.2024
Five randomized trials comparing the useof high-dose
dexamethasone with either notreatment21,22,25,26 or with
betamethasone27
in women with presumed HELLP syndromewere summarized by Sibai28
and are pre-sented in Table 4. The results of these stud-ies
demonstrate improved laboratory valuesand urine output in patients
receiving
FIGURE 1. Checklist in the management of HELLP syndrome.
Controversies With HELLP Syndrome 465
-
8/2/2019 Controversies PEE ClinObstGyn05
7/18
dexamethasone, but provide limited evi-dence of reduced maternal
morbidity. How-ever, because most of these trials were
performed postpartum, the true extentglucocorticoids can
influence outcomes
has yet to be determined.The mechanism of action of this drug
is
unknown but appears to alter the final stepsin endothelial cell
disruption as evidenced
by steroids having the ability to improve lab-oratory values
postpartum when presumablythe ability to synthesize new mediators
ofdisease is limited after delivery of the pla-centa. Because HELLP
syndrome is charac-terized by the endothelial damage within
theliver, we can only surmise glucocorticoidsact to minimize the
degree of intravascularendothelial injury within the body,
improve
blood flow within the liver specifically, andhalt ongoing
hepatocyte death and plateletconsumption.
Because glucocorticoids are the only knowndrugs to improve the
maternal laboratoryfindings in cases of severe preeclampsia, weuse
this observation in our management.Our dosing of the medication is
directednot only to improve neonatal outcomes bylowering the
incidence of such complica-tions as respiratory distress syndrome
and
intraventricular hemorrhage, but also to at-tempt to reduce
maternal morbidity. Thedose, route of administration, and
durationof treatment of glucocorticoids is importantand has varied
between studies. These
aspects of therapy still require further studywith properly
controlled trials, but some in-formation is evident from the
literature.First, intravenous glucocorticoids appearto have a more
rapid onset of action com-
pared with intramuscular dosing. The ran-domized trial by Isler
et al demonstrated in-travenous dosing was superior to
intramus-cular dosing for several outcome variables,including
improving urine output and greaterimprovement in laboratory
values.27 Sec-ond, glucocorticoids improve the maternalcondition in
a dose-dependent manner.In a review of data collected at our
center,we observed maternal platelet count in-creased more
dramatically before deliverywith a high-dose protocol of
glucocorticoidsversus standard regimens used for enhanc-ing lung
maturity.24 We therefore use thishigh-dose protocol in our
management of
patients with severe maternal disease (seeTable 5). Finally, the
duration of action ofthis medication is limited and patients
mayexperience a worsening of their laboratory
TABLE 4. Randomized Trials of Corticosteroids In Women With ELLP
Or HELLP Syndrome
AuthorsDexamethasone(no.)
Control(no.) Key Finding
Magann et al21 12* 13 Improved platelet, ALT, LDH values
indexamethasone group
Magann et al22 20 20 Improved platelet, AST, LDH, urine
output,MAP in dexamethasone group
Vigil-De Gracia25 17 17 Improved platelet counts only with
dexamethasoneYalcin et al26 15 15 Improved platelet, AST, MAP, and
urine output
with dexamethasoneIsler et al27 19* 21 Improved AST, LDH, MAP,
and urine output
with dexamethasone
* Antepartum. Postpartum.
Received intramuscular betamethasone.
Reprinted from Sibai BM. Diagnosis, controversies, and
management of the syndrome of hemolysis, elevated liver enzymes,
and low platelet count. Obstet Gynecol. 2004;103:981991.
ELLP, elevated liver enzymes and low platelets; AST, aspartate
amino transferase; ALT, alanine amino transferase; LDH, lactic
dehy-drogenase; MAP, mean arterial pressure.
466 OBrien and Barton
-
8/2/2019 Controversies PEE ClinObstGyn05
8/18
studies 48 to 72 hours after dosing with glu-cocorticoids.23,24
We term this finding therebound phenomenon. Steroid
treatment,therefore, is not curative but may createa window of
opportunity for intervention
before the maternal condition may againdeteriorate.
During the period when the maternal sta-tus is being optimized,
adequate but notexcessive hydration of the patient is per-
formed, laboratory studies are followed toobserve the expected
response, and the fetalstatus is intermittently reassessed.
Becauseglucocorticoids do not appear to alter theunderlying
pathophysiology, delivery re-mains the only definitive therapy. We
do not
proceed with expectant management ofHELLP syndrome beyond an
appropriate in-terval to optimize the maternal status andobtain
fetal exposure to the drug (2448hours). Furthermore, if no
improvement inthe clinical or laboratory status is notedwithin 8 to
12 hours of administration ofthe medication, we reevaluate the
diagnosisconsidering other conditions such as acutefatty liver,
consider increasing the dose ofglucocorticoid, consider
transfusion, and ex-
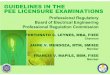
pedite delivery.With this information, we have created
flowsheets for the management of antepar-tum and postpartum
HELLP syndrome(see Figs. 2A and B). Understanding thegoals of
therapy are essential to optimal out-comes and are 2-fold: 1) to
improve the ma-
ternal status immediately before and duringdelivery if needed,
and 2) in women ,35weeks, to provide glucocorticoid exposureto the
fetus for enhancement of fetal lungmaturation.
We believe that glucocorticoids may beused for maternal benefit
even if the patienthas previously received this medication forfetal
lung maturity in the current pregnancy.We therefore attempt to
delineate mater-nal versus fetal indications for the use
ofglucocorticoids in patients with HELLP
syndrome.An increase in maternal platelet count be-
fore delivery can alter management bypotentially minimizing
bleeding complica-tions. For instance, with treatment, we
haveobserved a significant increase in the use ofregional
anesthesia in those women withHELLP syndrome exposed to
glucocorti-coids for 24 hours compared with womenwho did not
receive this therapy or achievethis latency period.29 We therefore
coordi-nate our efforts with our anesthesiologists
before effecting delivery, attempting to max-
imize the maternal platelet count and there- by increase the use
of regional anesthesia.Regional anesthesia has been shown toavoid
complications of exacerbated hyper-tension, aspiration, and failed
intubationattributable to general anesthesia in this pop-ulation.
We have given glucocorticoids atany gestational age to address
maternal dis-ease because such a benefit may exist interm
gestations. However, the use of high-dose dexamethasone to improve
maternaloutcome in women with HELLP syndrome
beyond 34 weeks gestation and/or in the postpartum period
remains experimental.
A latency period before effecting deliveryis not appropriate or
necessary in all casesof HELLP syndrome but is required to expecta
benefit from glucocorticoid administration.If the gestational age
is$35 weeks, the patientis asymptomatic, and the platelet count is
suf-ficient to offer any type of anesthesia, we pro-ceed promptly
with delivery and do not sug-gest a latency period for
glucocorticoids toimpact the maternal status. Alternatively,
the
TABLE 5. High-Dose GlucocorticoidTherpy to Improve Laboratory
Abnormalities in Patients With HELLP Syndrome
For most patients with HELLP syndrome, 10 mgintravenous
dexamethasone every 6 hours for 2doses followed by 6 mg intravenous
dexamethasoneevery 6 hours for 2 additional doses.
For select patients at highest risk, including thosewith
profound thrombocytopenia (,20,000/mm3)or with central nervous
system dysfunction(ie, blindness, paralysis), 20 mg
intravenousdexamethasone every 6 hours for up to 4 doses.
Controversies With HELLP Syndrome 467
-
8/2/2019 Controversies PEE ClinObstGyn05
9/18
fetal status may not allow for expectant man-agement and a
sufficient latency period to op-timize both the fetal and maternal
condition. Ifa nonreassuring fetal assessment is observed,we
consider initiating our steroid protocolwhen the maternal disease
is severe. We pro-ceed with delivery and expect the impact ofour
therapy to begin postpartum.
Conservative ManagementProlonging the latency period beyond
48
hours from the time of the diagnosis ofHELLP syndrome to
delivery is controver-sial. van Pampus et al described the
clinical
progress and maternal outcome of theHELLP and ELLP (findings of
HELLP syn-drome but without evidence of hemolysis)syndrome in 127
patients managed in theAcademic Medical Center in Amsterdam
between 1984 and 1996 with a live fetusin utero.13 The patients
were treated by tem-
porizing management, including the use ofantihypertensives and
magnesium sulfate.The predominant indication for terminating
pregnancy was fetal distress or fetal deathand not maternal
condition. All serious ma-ternal complications occurred at the
onset ofthe syndrome (24% of cases with HELLPsyndrome vs. 10% with
ELLP). Two motherswith HELLP syndrome died after a
cerebralhemorrhage. Seventy-nine (62%) of womenwere not delivered
after 3 days and 65 (51%)after 7 days. Although the authors noted
it isunlikely that a more aggressive approachwould have reduced
maternal mortality ormorbidity, their sample size was inadequateto
evaluate rare serious maternal complica-tions of HELLP or ELLP
syndrome.
In a study by Visser and Wallenburg,14
128 consecutive preeclamptic patients withHELLP syndrome and a
gestational age lessthan 34 weeks gestation were matched
formaternal and gestational age with 128
preeclamptic patients without HELLP syn-drome. Both groups were
treated with vol-ume expansion and pharmacologic vasodila-tation
under invasive hemodynamic monitor-ing with the aim of prolonging
gestation and
enhancing fetal maturity. Except for variables pertaining to
HELLP syndrome, clinical andlaboratory data and median prolongation
of
pregnancy did not differ between the groups.Perinatal mortality
was 14.1% in patients withHELLP syndrome and 14.8% in patients
with-out HELLP. Because the perinatal outcomesin this study are
similar to studies performedin the United States where delivery was
af-fected within 48 hours of the diagnosis ofHELLP syndrome, the
benefit of temporizingmanagement of HELLP syndrome remains
questionable. Ultimately, only a well-designedrandomized trial
will resolve this managementissue.
The described conservative managementtechniques were often
associated with theuse of invasive procedures and numerousmedical
and surgical treatments. These con-founding variables make it
difficult to eval-uate any treatment modality proposed forthis
syndrome. Occasionally, some patientswithout true HELLP syndrome
may demon-strate antepartum reversal of hematologicabnormalities
after bedrest, the use of ste-
roids, or plasma volume expansion. How-ever, in our experience,
the majority of these
patients demonstrate progressive deteriora-tion in either
maternal or fetal condition.The potential risks associated with
conser-vative management of HELLP syndrome in-clude abruptio
placentae, pulmonary edema,acute renal failure, eclampsia,
perinatal death,and maternal death. Therefore, because onlya
limited prolongation of pregnancy can
be expected and because no difference infetal survival with
aggressive attempts atexpectant management has been observed,we
caution against expectant management
beyond a 24- to 48-hour latency to optimizethe maternal status
for delivery. We shouldspecifically caution women with
dissemi-nated intravascular coagulation (DIC) shouldnot be
expectantly managed.
TransfusionPlatelet transfusions are indicated either be-fore or
after delivery in all patients with
468 OBrien and Barton
-
8/2/2019 Controversies PEE ClinObstGyn05
10/18
FIGURE 2. A, Flowchart for antepartum HELLP syndrome. B,
Flow-chart for postpartum management of HELLP syndrome.
Controversies With HELLP Syndrome 469
-
8/2/2019 Controversies PEE ClinObstGyn05
11/18
HELLP syndrome in the presence of signif-icant bleeding from
puncture sites, wound,intraperitoneal, extensive ecchymosis, andso
on. Furthermore, transfusion is indicatedin all antepartum patients
whose plateletcount is less than 20,000/mm3. Correctionof profound
thrombocytopenia is particu-larly important before cesarean
section. Re-
peated platelet transfusions, however, maynot be necessary
because consumption occursrapidly and the effect is transient. Our
policyis to administer 6 to 10 units of platelets in
all patients with a platelet count less than40,000/mm3 before
intubating the patientfor cesarean section.
Platelets are the most commonly trans-fused blood component in
patients withHELLP syndrome. However, red cells andfresh-frozen
plasma may also be needed in
patients with more severe coagulopathies.The need for
transfusion may be reduced
by optimizing the patients status before de-livery and reducing
the severity of thrombo-cytopenia. Martin et al have demonstrateda
reduction in the rate for transfusion of both
cellular components and plasma in patientsexposed to
dexamethasone over 2 epochs.30
The association between dexamethasone ex-posure and a reduced
rate of transfusion hasalso been noted by our group. The decisionto
delay delivery to improve the maternal
platelet count by steroid exposure is againdependent on several
aspects of the clinicalsituation, including fetal status. A
large,multicenter, placebo-controlled, randomizedtrial of patients
with markedly thrombocyto-
penic, antepartum HELLP syndrome wouldbe necessary to quantitate
the potential ben-efit of reduced need for transfusion after
ste-roid exposure. Such a trial does not appearto be forthcoming,
however, especially whenconsidering the fetal benefits to
glucocorti-coid administration for lowering the rateof
complications of prematurity.
Delivery ControversiesDelivery of a patient with HELLP
syndromeis associated with numerous potential com-
plications, including postpartum hemor-rhage, vaginal/labial
hematoma for vaginaldelivery, wound hematomas/separation
forcesarean delivery, and infection resultingfrom prolonged
induction. The choice be-tween attempted vaginal delivery
versuscesarean section should be based on assess-ment of various
predictors for success of anattempted induction, including 1)
cervicalstatus, 2) fetal heart rate tracing or biophys-ical
profile, and 3) umbilical artery Dopplerstudies. We have observed a
very poor suc-
cess rate for attempted induction in the faceof a preterm
gestation with intrauterinegrowth restriction and markedly
abnormalDoppler studies. We proceed directly tocesarean section
under such circumstances.31
Briggs et al32 evaluated wound complica-tions between patients
with antepartumHELLP syndrome with primary closure ver-sus delayed
closure and Pfannenstiel versusmidline skin incisions. A total of
104 patientswere identified; 75 had a primary skin closureand 29
had a delayed closure 48 to 72 hours
postoperatively. Immediate wound complica-
tions (wound infection, hematoma) occurredin 18 (26%) patients
who had primary closureversus 8 (24%) who had a delayed
closure(odds ratio, 1.13; 95% confidence interval,0.393.27). A late
wound breakdown wasseen in only 1 patient with primary closure
but in none with delayed closure. No statisti-cal difference in
wound complication wasfound between midline (primary or delayed)and
Pfannenstiel (primary, delayed) incisions(odds ratio, 0.65; 95%
confidence interval,0.231.88). The authors concluded that forwomen
with antepartum HELLP syndromedelivered by cesarean section, the
frequencyof wound complications is not influenced bytype of skin
incision or time of skin closure(primary or delayed).
Generalized oozing from any operativesite is very common in
thrombocyto-
penic patients. To minimize the risk of he-matoma formation, the
bladder flap should
be left open and a subfascial drain may beused for 24 to 48
hours. A subcutaneousdrain may also be considered if the skin
is
470 OBrien and Barton
-
8/2/2019 Controversies PEE ClinObstGyn05
12/18
approximated attempting to minimize the in-cidence of wound
complications. Subcutane-ous tissues should be approximated
withsutures as evidenced by randomized trialsand metaanalysis for
skin closure at cesareandelivery.33
Controversies in Managementof Subcapsular HematomaThe most
dramatic sequelae of hepatic in-
volvement by preeclampsia is the develop-ment of segmental
hepatic infarction, exten-sive parenchymal hemorrhage, or
subcapsu-lar hematoma. Hepatic imaging findings inselected patients
with HELLP syndromecan identify these abnormalities.10 Ruptureof a
subcapsular hematoma is particularlyconcerning because it can lead
to death byexsanguination from the inability to control
bleeding as a result of surgical difficultieswith repair of the
liver and coagulopathy.Of the 34 patients evaluated by Bartonand
Sibai, 16 patients (47%) had abnormal
hepatic imaging results. The most commonCT abnormalities were
subcapsular hema-toma of the liver (n = 13) and intraparenchy-mal
hemorrhage (n = 6).
Comparison of the clinical characteristicsand laboratory
evaluations of patients withnormal and abnormal hepatic imaging
find-ings demonstrated a significant difference in
platelet count nadir between the patientswith normal and
abnormal imaging findings
but failed to show any statistically signifi-cant difference in
gestational age, meanarterial pressure, or the other laboratory
parameters studied. Of the 13 patients withsevere
thrombocytopenia (platelet count,20,000/mm3), 10 (77%) had
abnormalhepatic imaging findings. Emergency inter-vention was
needed for 6 patients on the ba-sis of these imaging findings. CT
and MRIhave excellent sensitivity for detecting acuteliver
hemorrhage, but because CT was moreavailable, faster, and safer for
potentially un-stable patients, and hence was the imagingmodality
of choice.
The differential diagnosis of an unrupturedsubcapsular hematoma
of the liver in preg-nancy should include acute fatty liver of
pregnancy, abruptio placentae with dissemi-nated intravascular
coagulation, ruptureduterus, or sepsis. Most patients with a
subcap-sular hematoma of the liver are seen in thelate second or
third trimester of pregnancy,although cases have been reported in
the im-mediate postpartum period. Patients typicallyreport right
upper quadrant pain, but local-ized pain may be absent. Stimulation
of the
phrenic nerve at the diaphragm can producereferred pain along
this nerves distribution toits origin in the C4C5 cervical plexus,
in-cluding the pericardium, peritoneum, pleura,and shoulder.
Physical examination findingsconsistent with peritoneal irritation
and hepa-tomegaly may be present.
Surgical repair has been recommendedfor hepatic hemorrhage
without liver rup-ture. More recent experience suggests, how-ever,
this complication should be managedconservatively in patients who
remainhemodynamically stable.34,35 Management
should include close monitoring of hemody-namics and coagulation
status. Serial assess-ment of the subcapsular hematoma with
ul-trasound or CT is necessary with immediateintervention for
rupture or worsening of ma-ternal status. It is important with
conserva-tive management to avoid exogenous sour-ces of trauma to
the liver such as abdominal
palpation, convulsions, or emesis, and to usecare in
transportation of the patient. Indeed,any sudden increase in
intraabdominal pres-sure could potentially lead to rupture of
thesubcapsular hematoma.36
In most instances, rupture of a subcapsularhematoma involves the
right lobe and is pre-ceded by the development of a
parenchymalhematoma. Patients frequently present withshoulder pain,
shock, or evidence of massiveascites, respiratory difficulty, or
pleural effu-sions, and often with a dead fetus. An ultra-sound or
computed axial tomography of theliver should be performed to rule
out the pres-ence of subcapsular hematoma of the liverand assess
for the presence of intraperitoneal
Controversies With HELLP Syndrome 471
-
8/2/2019 Controversies PEE ClinObstGyn05
13/18
bleeding. Paracentesis confirms the presenceof intraperitoneal
hemorrhage suspected byexamination or hepatic imaging.
The presence of ruptured subcapsular liverhematoma resulting in
shock is a surgicalemergency requiring acute
multidisciplinarytreatment. Resuscitation should consist ofmassive
transfusions of blood, correction ofcoagulopathy with fresh-frozen
plasma and
platelets, and immediate laparotomy. Optionsat laparotomy
include packing and drainage(preferred), surgical ligation of the
hemor-
rhaging hepatic segments, embolization ofthe hepatic artery to
the involved liver seg-ment, and loosely suturing omentum or
surgi-cal mesh to the liver to improve integrity. Evenwith
appropriate treatment, maternal and fetalmortality is over 50%.
Mortality is most com-monly associated with exsanguination
andcoagulopathy. Initial survivors are at increasedrisk for
developing adult respiratory distresssyndrome, pulmonary edema,37
and acute re-nal failure in the postoperative period.38
Smith et al39 reviewed their managementof 7 patients with
spontaneous rupture of the
liver occurring during pregnancy. Of the 4survivors, the mean
gestational age was32.8 weeks and the mean duration of
hospi-talization was 16 days. All the survivorsmanaged with packing
and drainage of theliver survived, whereas the 3 patients
treatedwith hepatic lobectomy died. The authors al-so extracted 28
cases from the literaturereported since 1976. From a total of
35cases, 27 patients (82%) managed by pack-ing and drainage
survived, whereas only25% of 8 patients undergoing hepatic
lobec-tomy survived. The authors emphasized he-
patic hemorrhage with persistent hypoten-sion unresponsive to
transfusion of blood
products may be managed surgically withlaparotomy, evacuation of
the hematoma,
packing of the damaged liver, and drainingof the operative site.
In certain cases inwhich the patient is stable enough to under-go
angiography, transcatheter embolother-apy is a reasonable
alternative to surgery.40
In a review of 442 cases of HELLP syn-drome managed at the
University of Ten-
nessee, Memphis, 4 patients with HELLPsyndrome were complicated
by a rupturedsubcapsular hematoma.18 Three cases re-quired
transfusion of 22 to 40 units of
packed red blood cells and multiple unitsof platelets and
fresh-frozen plasma. Twoof these 3 cases were complicated by
pul-monary edema and acute renal failure, butall survived without
any residual deficiency.The fourth case was a patient who
presentedin profound shock and with disseminatedintravascular
coagulopathy. This patient
subsequently died secondary to a ruptured pulmonary
emphysematous bleb duringmanagement of adult respiratory
distresssyndrome.
TABLE 6. Management of Patients With Subcapsular Hematoma of the
Liver
General considerations:I. Have the blood bank aware of the
potential
need for large amounts of packed red bloodcells, fresh-frozen
plasma, and plateletconcentrate (ie, 30 units of blood, 20 units
offresh-frozen plasma, 3050 units ofplatelets)
II. Consultation of a general or vascular surgeonIII. Avoid
direct and indirect manipulation of the
liverIV. Close monitoring of hemodynamic statusV. Intravenous
magnesium sulfate to prevent
seizuresIf the hematoma is unruptured:
I. Conservative management with serialcomputed tomography scans
or ultrasound
If the hematoma is ruptured and patienthemodynamically
unstable:I. Massive transfusions
II. Immediate laparotomyA. If bleeding is minimal:
1. Observation2. Draining area with closed suction
B. If bleeding is severe:1. Application of laparotomy sponges
as
packsfor pressure
2. Embolization of the hepatic artery totheinvolved liver
segment
472 OBrien and Barton
-
8/2/2019 Controversies PEE ClinObstGyn05
14/18
On the basis of review of the literature, anoutline for the
management of hepatic com-
plications of HELLP syndrome was devel-oped (Table 6). This
outline emphasizesthe potential for transfusion of large amountsof
blood and blood products and the need foraggressive intervention if
rupture of the he-matoma is suspected and the patient is
he-modynamically unstable. We recommend30 units of packed red blood
cells, 20 unitsof fresh-frozen plasma, 30 to 50 units of
platelets, and 20 to 30 units of cryoprecipi-
tate be available if rupture of a subcapsularhematoma is
suspected. Our experience isin agreement with the recent
observationsof Smith et al39 in that a stable patientwith an
unruptured subcapsular hematomashould be conservatively managed.
Constantmonitoring must continue during this man-agement, however,
because patients canrapidly become unstable after rupture ofthe
hematoma. Survival clearly is associatedwith rapid diagnosis and
immediate medicalor surgical stabilization. Coagulopathy must
be aggressively managed. These patients
should be managed in an intensive care unitwith close monitoring
of hemodynamic
parameters and fluid status to avoid pulmo-nary edema or
respiratory compromise.
Postpartum ManagementThe diagnostic criteria for HELLP
syndromemay develop antepartum or postpartum. Sibaiand associates18
revealed that 70% hadevidence of the syndrome antepartum, and30%
developed the criteria postpartum. Inthe postpartum period, the
time of onsetranged from a few hours to 7 days, withthe majority
developing within 48 hours afterdelivery. Patients in this group
are at in-creased risk for the development of pulmo-nary edema with
acute renal failure.37,38
HELLP syndrome may be diagnosed post-partum following 1 of 3
clinical scenarios:1) worsening of antepartum severe pre-eclampsia
with delivery not yet altering thetime course of the disease, 2)
new onset ofsevere preeclampsia postpartum, or 3) re-
bound deterioration of a patient with antepar-tum HELLP syndrome
after exposure to cor-ticosteroid antepartum.
The goals of therapy postpartum differcompared with antepartum
and are aimedsolely at improving the maternal status.Management of
seizure prophylaxis is sim-ilar to the antepartum patient with
HELLPsyndrome, including the need for magne-sium sulfate.
Hypertension control may bemore aggressive, however, because there
isno longer concern about compromising the
uteroplacental circulation. Blood pressuregoals of systolic
blood pressure,155 mm Hgand/or diastolic blood pressure,105 mm
Hgare suggested.
After delivery, the patient should be mon-itored closely in an
intensive care setting for24 to 48 hours. Most patients show
evidenceof resolution of the disease process within48 hours after
delivery. The differential diag-nosis of postpartum hypertension
and pro-teinuria should include thrombotic throm-
bocytopenic purpura, hemolytic uremicsyndrome, and exacerbation
of systemic lu-
pus. These alternative diagnoses may be con-sidered if
resolution of the disease is pro-longed. However, some patients
with HELLPsyndrome, especially those with DIC, maydemonstrate
delayed resolution or even dete-rioration. Such patients may
require longer,intensive monitoring. These patients are atrisk for
developing pulmonary edema as aresult of transfusions of blood and
blood
products, fluid mobilization, and compro-mised renal
function.38
As a result of the persistent potential foradverse outcomes
postpartum, severalreports have advocated the use of
corticoste-roids to more promptly restore vascular in-tegrity. In a
retrospective study, Martin et al41
reported the puerperal courses of 43 womenwith postpartum HELLP
syndrome whowere treated with dexamethasone and com-
pared them with 237 similar patients whodid not receive
corticosteroids. Dexametha-sone at a dosage of 10 mg IV at
12-hourintervals was given until disease remissionwas noted in
treated patients, at which time
Controversies With HELLP Syndrome 473
-
8/2/2019 Controversies PEE ClinObstGyn05
15/18
up to 2 additional 5-mg IV doses were givenat 12-hour intervals.
Patients who receiveddexamethasone for postpartum-onset
HELLPsyndrome experienced a shorter diseasecourse, faster recovery,
less morbidity, andless need for other interventionist
therapycompared with a historical group of patientswith HELLP
syndrome who did not receivedexamethasone.
Postpartum patients with delayed resolu-tion of HELLP syndrome
(including persis-tent severe thrombocytopenia) represent
a management dilemma. Exchange plas-mapheresis with fresh-frozen
plasma has
been advocated as a treatment by someauthors.4244 Because the
majority of these
patients will have spontaneous resolutionof their disease, early
initiation of plasma-
pheresis may result in unnecessary treat-ment. Schwartz44
suggested serial studiesindicating a progressive elevation of
biliru-
bin or creatinine associated with hemolysisand thrombocytopenia
may be an indicationfor plasmapheresis. Martin and coworkers42
reported the use of plasma exchange with
fresh-frozen plasma in 7 women in the post-partum period with
HELLP syndrome thatpersisted .72 hours after delivery. All patients
had persistent thrombocytopenia,rising lactic dehydrogenase, and
evidenceof multiorgan dysfunction. The authors rec-ommended that a
trial of plasma exchangewith fresh-frozen plasma be considered
inHELLP syndrome that persists past 72 hoursfrom delivery and in
which there is evidenceof a life-threatening microangiopathy.
Since their publication, however, the Mis-sissippi group has
reviewed 18 patients withHELLP syndrome who were treated
postpar-tum with single or multiple plasma ex-change with
fresh-frozen plasma.43 Each pa-tient was entered into the clinical
trial either
because of persistent evidence of atypical preeclampsiaeclampsia
as HELLP syn-drome .72 hours after delivery (group 1)or with
evidence of worsening HELLP syn-drome at any time postpartum in
associationwith single- or multiple-organ injury (group2). In the
absence of other disease conditions,
the 9 patients in group 1 responded rapidly to1 or 2 plasma
exchange procedures with fewcomplications and no maternal deaths.
In con-trast, in the 9 patients in group 2 with HELLPsyndrome
presentations complicated by otherend-organ disease, the response
to plasma ex-change was variable and there were 2 deaths inthis
group. This series details the postpartumapplication of plasma
exchange therapy forunremitting HELLP syndrome, but revealsthat a
uniformly positive response to this ther-apy is not observed when
there is additional
single or multiple organ injury.44 Potential ad-verse effects of
this plasma exchange include
plasma-transmitted infections, anaphylaxis,volume overload,
sepsis, and maternal death.
Maternal CounselingPregnancies complicated by HELLP syn-drome
are associated with life-threateningcomplications for both the
mother and her in-fant. Therefore, clinicians should be able
toanswer questions regarding subsequent preg-nancy outcome and
long-term prognosis.
Women with a history of HELLP syndromeare at increased risk of
all forms of pre-eclampsia in subsequent pregnancies. In gen-eral,
the rate of preeclampsia in subsequent
pregnancies is approximately 20% withsignificantly higher rates
if the onset ofHELLP syndrome was in the second tri-mester. The
rate of recurrent HELLP syn-drome ranges from 2% to 19%. We quotea
recurrence risk of less than 5%.4547 Be-cause of these risks, these
women areinformed that they are at increased riskfor adverse
pregnancy outcome (pretermdelivery, fetal growth restriction,
abruptio
placentae, and fetal death) in subsequentpregnancies. Therefore,
they require closemonitoring during subsequent
gestations.Currently, there is no preventive therapyfor recurrent
HELLP syndrome. Liverfunction tests were studied in 54 womenat a
median of 31 months (range, 3101months) after pregnancies
complicated
by the HELLP syndrome.48 Serum levelsof AST, LDH, and conjugated
bilirubin
474 OBrien and Barton
-
8/2/2019 Controversies PEE ClinObstGyn05
16/18
were found to be normal. Total bilirubinlevels, however, were
elevated in 11(20%) of the studied women. The authorsof this report
suggested the possibility thata dysfunction of the
bilirubin-conjugatingmechanism represents a risk factor for
thedevelopment of this syndrome.48
There are 2 reports describing long-term renal function after
HELLP syn-drome.38,49 One of the reports included23 patients whose
pregnancies were com-
plicated by HELLP syndrome and acute
renal failure; 8 of these women had 11 sub-sequent pregnancies
with 9 resulting interm gestation.38 All 23 women also hadnormal
blood pressures and renal functionat an average follow up of 4.6
years (range,0.511 years). The other study comparedrenal function
after at least 5 years afterHELLP syndrome in 10 patients with
therespective findings in 22 patients with pre-vious normotensive
gestation.49 Therewere no differences in renal function tests
between the 2 groups. These findings sug-gest that the
development of HELLP syn-
drome with or without renal failure doesnot affect long-term
renal function.
SummarySignificant hepatic involvement by pre-eclampsia leading
to hepatocyte necrosisand thrombocytopenia should alarm the
cli-nician regardless of whether criteria forHELLP syndrome have
been fully achieved.Liver parenchyma is relatively unforgivingof
the endovascular insult presented by se-vere preeclampsia. This
vasculopathy canresult in adverse maternal outcomes suchas DIC,
subcapsular hematoma, hepatic in-farction, and death. The greatest
challengesin caring for women with this disease are ap-
preciating the diagnosis, instituting timelyinterventions, and
avoiding associated com-
plications. The addition of high-dose gluco-corticoids to the
armamentarium of therapyfor HELLP syndrome may improve out-comes
for both the mother and fetus, but de-finitive proof by randomized
trials is lack-
ing. Delivery is the ultimate cure, and opti-mizing the status
of a seriously ill patient
before delivery improves outcome.
References1. Levine RJ, Maynard SE, Qian C, et al. Circu-
lating angiogenic factors and the risk of pre-eclampsia. N Engl
J Med. 2004;350:672683.
2. Pritchard JA, Weisman R, Ratnoff OD, et al.Intravascular
hemolysis, thrombocytopeniaand other hemologic abnormalities
associatedwith severe toxemia of pregnancy. N Engl JMed.
1954;250:8998.
3. Chesley LC. Disseminated intravascular co-agulation. In:
Hypertensive Disorders inPregnancy. New York:
Appleton-Century-Crofts; 1978:88118.
4. Weinstein L. Syndrome of hemolysis, elevat-ed liver enzymes,
and low platelet count: asevere consequence of hypertension in
preg-nancy. Am J Obstet Gynecol. 1982;142:159167.
5. Roberts JM, Cooper DW. Pathogenesis andgenetics of
pre-eclampsia. Lancet. 2001;357:5356.
6. Roberts JM. Preeclampsia, what we knowand what we do not
know. Semin Perinatol.2000;24:2428.
7. Barton JR, Riely CA, Adamel TA, et al. He- patic
histopathologic condition does notcorrelate with laboratory
abnormalities inHELLP syndrome (hemolysis, elevated liverenzymes,
and low platelet count). Am J Ob- stet Gynecol.
1992;167:15381543.
8. Aarnoudse JG, Houthoff HF, Weits J, et al. Asyndrome of liver
damage and intravascularcoagulation in the last trimester of
normoten-sive pregnancy. A clinical and histopatholog-ical study.
Br J Obstet Gynaecol. 1986;93:145155.
9. Arias F, Mancilla-Jimenez R. Hepatic fibrin-ogen deposits in
pre-eclampsia. Immunoflu-orescent evidence. N Engl J Med.
1976;295:578582.
10. Barton JR, Sibai BM. Hepatic imaging inHELLP syndrome
(hemolysis, elevated liverenzymes, and low platelet count). Am
JObstet Gynecol. 1996;174:18201827.
11. Sibai BM, Taslimi MM, El-Nazer A, et al.Maternal-perinatal
outcome associatedwith the syndrome of hemolysis, elevated
Controversies With HELLP Syndrome 475
-
8/2/2019 Controversies PEE ClinObstGyn05
17/18
liver enzymes, and low platelets in
severepreeclampsia-eclampsia. Am J Obstet Gyne-col.
1986;155:501509.
12. Martin JN Jr, Rinehart B, May WL, et al. Thespectrum of
severe preeclampsia:Comparativeanalysis by HELLP syndrome
classification.Am J Obstet Gynecol. 1999;180:13731384.
13. VanPampus MG, Wolf H, Westenberg SM,et al. Maternal and
perinatal outcome afterexpectant management of the HELLP syn-drome
compared with preeclampsia withoutHELLP syndrome. Eur J Obstet
GynecolReprod Biol. 1998;76:3136.
14. Visser W, Wallenburg HCS. Temporisingmanagement of severe
pre-eclampsia withand without the HELLP syndrome. Br JObstet
Gynaecol. 1995;102:111117.
15. Abramovici D, Friedman SA, Mercer BM,et al. Neonatal outcome
in severe preeclamp-sia at 24 to 36 weeks gestation: does theHELLP
(hemolysis, elevated liver enzymes,and low platelet count) syndrome
matter?Am J Obstet Gynecol. 1999;180:221225.
16. Sibai BM. The HELLP syndrome (hemoly-sis, elevated liver
enzymes, and low plate-lets): much ado about nothing? Am J
ObstetGynecol. 1990;162:311316.
17. Weinstein L. Preeclampsia/eclampsia withhemolysis, elevated
liver enzymes andthrombocytopenia. Obstet Gynecol.
1985;66:657660.
18. Sibai BM, Ramadan MK, Usta I, et al.Maternal morbidity and
mortality in 442pregnancies with hemolysis, elevated liverenzymes,
and low platelets (HELLP syn-drome). Am J Obstet Gynecol.
1993;169:10001006.
19. Sibai BM. Diagnosis and management ofgestational
hypertension and preeclampsia.Obstet Gynecol. 2003;102:181192.
20. Clark SL, Phelan JR, Allen SH, et al. Ante-partum reversal
of hematologic abnormali-ties associated with the HELLP syndrome.J
Reprod Med. 1987;32:781784.
21. Magann EF, Bass D, Chauhan SP, et al. An-tepartum
corticosteroids: disease stabiliza-tion in patients with the
syndrome ofhemolysis, elevated liver enzymes, and lowplatelets
(HELLP). Am J Obstet Gynecol.1994;171:11481153.
22. Magann EF, Perry KG Jr, Meydrech EF, et al.Postpartum
corticosteroids: acceleratedrecovery from the syndrome of
hemolysis,
elevated liver enzymes, and low platelets(HELLP). Am J Obstet
Gynecol. 1994;171:11541158.
23. Tompkins MJ, Thiagarajah S. HELLP (he-molysis, elevated
liver enzymes, and lowplatelet count) syndrome: the benefit of
cor-ticosteroids. Am J Obstet Gynecol. 1999;181:304309.
24. OBrien JM, Milligan DA, Barton JR. Im- pact of high-dose
corticosteroid therapy forpatients with HELLP (hemolysis,
elevatedliver enzymes, and low platelet count) syn-drome. Am J
Obstet Gynecol. 2000;183:
921924.25. Vigil-DeGracia P, Garcia-Caceres E. Dexa-
methasone in the postpartum treatment ofHELLP syndrome. Int J
Gynaecol Obstet.1997;59:217221.
26. Yalcin OT, Sener T, Hassa H, et al. Effects ofpostpartum
corticosteroids in patients withHELLP syndrome. Int J Gynaecol
Obstet.1998;61:141148.
27. Isler CM, Barrilleaux PS, Magann EF, et al.A prospective,
randomized trial comparingthe efficacy of dexamethasone and
betame-thasone for the treatment of antepartumHELLP syndrome. Am J
Obstet Gynecol.
2001;184:13321339.28. Sibai BM. Diagnosis, controversies,
and
management of the syndrome of hemolysis,elevated liver enzymes,
and low plateletcount. Obstet Gynecol. 2004;103:981991.
29. OBrien JM, Shumate SA, Satchwell SL,et al. Maternal benefit
to corticosteroidtherapy in patients with HELLP (hemolysis,elevated
liver enzymes, and low platelets)syndrome: impact on the rate of
regional an-esthesia. Am J Obstet Gynecol. 2002;186:475479.
30. Martin JN Jr, Thigpen BD, Rose CH, et al.Maternal benefit of
high-dose intravenouscorticosteroid therapy for HELLP syn-drome. Am
J Obstet Gynecol. 2003;189:830834.
31. Bush K, OBrien JM, Milligan DA, et al. Theutility of
umbilical artery Doppler in womenwith the HELLP (hemolysis,
elevated liverenzymes, and low platelets) syndrome. AmJ Obstet
Gynecol. 2001;184:10871089.
32. Briggs R, Chari RS, Mercer B, et al. Post-operative incision
complications aftercesarean section in patients with antepar-tum
syndrome of hemolysis, elevated liver
476 OBrien and Barton
-
8/2/2019 Controversies PEE ClinObstGyn05
18/18
enzymes, and low platelets (HELLP): doesdelayedprimary
closuremake a difference?Am J Obstet Gynecol. 1996;175:893896.
33. Chelmow D, Rodriguez EJ, Sabatini MM.Suture closure of
subcutaneous fat andwound disruption after cesarean delivery:a
meta-analysis. Obstet Gynecol. 2004;103:974980.
34. Goodlin RC, Anderson JC, Hodgson PE.Conservative treatment
of liver hematomain the postpartum period. J Reprod
Med.1985;30:368370.
35. Manas KJ, Welsh JD, Rankin RA, et al.
Hepatic hemorrhage without rupture inpreeclampsia. N Engl J Med.
1985;312:424426.
36. Neerhof MG, Zelman W, Sullivan T. Hepaticrupture in
pregnancy: a review. Obstet Gyne-col Surv. 1989;44:407409.
37. Sibai BM, Mabie BC, Harvey CJ. Pulmonaryedema in severe
preeclampsia-eclampsia:analysis of 37 consecutive cases. Am J
ObstetGynecol. 1987;156:11741179.
38. Sibai BM, Ramadan MK. Acute renal failurein pregnancies
complicated by hemolysis,elevated liver enzymes, and low
platelets.AmJ Obstet Gynecol. 1993;168:16821687.
39. Smith LG Jr, Moise KJ Jr, Dildy GA, et al.Spontaneous
rupture of the liver during preg-nancy: current therapy. Obstet
Gynecol.1991;77:171175.
40. Loevinger EH, Lee WM, Anderson MC.Hepatic rupture associated
with preg-nancy: treatment with transcatheterembolotherapy. Obstet
Gynecol. 1985;65:281284.
41. Martin JN Jr, Perry KG, Blake PG, et al.Better maternal
outcomes are achievedwith dexamethasone therapy for postpartumHELLP
(hemolysis, elevated liver enzymes,
and thrombocytopenia) syndrome. Am J
Obstet Gynecol. 1997;177:10111017.42. Martin JN Jr, Files JC,
Blake PG, et al.
Plasma exchange for preeclampsia: I. Post- partum use for
persistently severe pre-
eclampsia-eclampsia with HELLP syndrome.Am J Obstet Gynecol.
1990;162:126137.
43. Martin JN Jr, Files JC, Blake PG, et al. Post-
partum plasma exchange for atypical pre-eclampsia-eclampsia as
HELLP syndrome.Am J Obstet Gynecol. 1995;172:11071127.
44. Schwartz ML. Possible role for exchange plasmapheresis with
fresh frozen plasma
for maternal indications in selected casesof preeclampsia and
eclampsia. ObstetGynecol. 1986;68:136139.
45. Sibai BM, Ramadan MK, Chari RS, et al.Pregnancies
complicated by HELLP syn-drome (hemolysis, elevated liver
enzymes,
and low platelets): Subsequent pregnancy
outcome and long-term prognosis. Am JObstet Gynecol.
1995;172:125129.
46. Van Pampus MG, Wolf H, Mayruhu G, et al.Long-term follow-up
in patients with a histo-
ry of (H)ELLP syndrome. Hypertens Preg-nancy. 2001;20:1523.
47. Chames MC, Haddad B, Barton JR, et al.Subsequent pregnancy
outcome in women
with a history of HELLP syndrome at#28weeks of gestation. Am J
Obstet Gynecol.
2003;188:15041508.48. Knapen M, VanAltena A, Peters WHM, et
al. Liver function following pregnancycomplicated by the HELLP
syndrome. Br
J Obstet Gynaecol. 1998;105:12081210.49. Jacquemyn Y, Jochems L,
Duiker E, et al.
Long-term renal function after HELLP
syndrome. Gynecol Obstet Invest. 2004;57:117120.
Controversies With HELLP Syndrome 477