Embed Size (px)
DESCRIPTION
Citation preview

Controversies in Hospital Controversies in Hospital Medicine: Beta Blockers, Medicine: Beta Blockers,
Heparin and HypergylcemiaHeparin and HypergylcemiaJeff Glasheen, MDJeff Glasheen, MD
Director, Hospital Medicine ProgramDirector, Hospital Medicine ProgramUniversity of Colorado HospitalUniversity of Colorado HospitalAssociate Professor of MedicineAssociate Professor of MedicineUniversity of Colorado DenverUniversity of Colorado Denver

To block or not to blockTo block or not to block
Should I beta block my Should I beta block my patient peri-operatively?patient peri-operatively?

What is the next best step?What is the next best step?
A) A) Metoprolol to HR < 60 bpm Metoprolol to HR < 60 bpm
B)B) Metoprolol to HR 60-80 bpm Metoprolol to HR 60-80 bpm
C)C) Metoprolol to HR 80-100 bpmMetoprolol to HR 80-100 bpm
D)D) Metoprolol not indicatedMetoprolol not indicated
64 yo man w/ DM & CAD undergoing R THA64 yo man w/ DM & CAD undergoing R THAExam: 131/69,72,10; OtherwiseExam: 131/69,72,10; Otherwise normalnormalMeds: Glargine, Lispro, ACE, Amlodipine, Meds: Glargine, Lispro, ACE, Amlodipine, ASAASA

Perioperative Beta Blockade Perioperative Beta Blockade BeneficialBeneficial
19961996 200 noncardiac surgery pts200 noncardiac surgery pts11
Atenolol DOS and t/o hosp stayAtenolol DOS and t/o hosp stay 50% reduction in mortality at 2 years50% reduction in mortality at 2 years
1999 1999 112 high risk vascular surgery pts112 high risk vascular surgery pts22
Bisoprolol 1 wk prior and t/o hosp stayBisoprolol 1 wk prior and t/o hosp stay 90% reduction in cardiac death/MI at 28 days90% reduction in cardiac death/MI at 28 days
20002000 107 noncardiac surgery pts107 noncardiac surgery pts33
Esmolol DOS and 48 hours post-opEsmolol DOS and 48 hours post-op 67% reduction in postoperative MI*67% reduction in postoperative MI*
20012001 ~1000 lower risk vascular surgery pts~1000 lower risk vascular surgery pts44
70% reduction in adjusted RR of MI70% reduction in adjusted RR of MI
*not statistically significant
1Mangano NEJM 1996;335:1713-17202Poldermans NEJM 1999;341:1789-17943Urban Anesth Analg 2000;90:1257-12614Boersma JAMA 2001;285:1865-1873

Since the 2001 Report…Since the 2001 Report… 20052005 POBBLEPOBBLE11
Metoprolol in 103 vascular surgery patientsMetoprolol in 103 vascular surgery patients No effect of beta blockers on cardiac eventsNo effect of beta blockers on cardiac events
20052005 Meta-analysisMeta-analysis22 22 RCT of periop BB22 RCT of periop BB Non-statistically sign trend toward better Non-statistically sign trend toward better
outcomes at 30 daysoutcomes at 30 days ↑↑risk of intraop hypotension and bradycardiarisk of intraop hypotension and bradycardia Concluded that use of PBB requires cautionConcluded that use of PBB requires caution
1 Brady, J Vasc Surg 2005;41:602-6092 Devereaux, BMJ 2005;331:313-321

Since the Meta-analysis…Since the Meta-analysis… 20052005 Large observational trialLarge observational trial
>600,000 patients undergoing major >600,000 patients undergoing major noncardiac surgerynoncardiac surgery
Compared pts who received BB w/in 2d Compared pts who received BB w/in 2d of hospitalization vs. those that did notof hospitalization vs. those that did not
Only high risk patients benefited from Only high risk patients benefited from perioperative BBperioperative BB
Lindenauer NEJM 2005;353:349-3361

Beta Blockers: Raising the Beta Blockers: Raising the Threshold for UseThreshold for Use
Lindenauer NEJM 2005;353:349-3361
Revised Cardiac Risk Revised Cardiac Risk IndexIndex
High risk surgeryHigh risk surgeryCoronary artery dzCoronary artery dzCerebrovascular dzCerebrovascular dzChronic kidney dzChronic kidney dzDiabetes mellitusDiabetes mellitus

Beta Blockers: Raising the Beta Blockers: Raising the Threshold for UseThreshold for Use
Lindenauer NEJM 2005;353:349-3361
Beta
No beta, unless CAD

Since the Observational Since the Observational Study…Study… 20062006MAVSMAVS11
RCT vascular surg, metoprolol (246) vs. Placebo RCT vascular surg, metoprolol (246) vs. Placebo (250)(250)
No difference 30 d MI, USA, CHF, Death 10.2% v No difference 30 d MI, USA, CHF, Death 10.2% v 12%12%
Significantly more intraop hypotension and Significantly more intraop hypotension and bradycardiabradycardia
No titration of med: HR 69 bpm vs. 79 bpm No titration of med: HR 69 bpm vs. 79 bpm 20062006DIPOMDIPOM22
RCT 921 diabetics, major non-cardiac surgeryRCT 921 diabetics, major non-cardiac surgery No effect of metoprolol 100 mg daily, ave of 5 daysNo effect of metoprolol 100 mg daily, ave of 5 days No titration: HR in met 75 bpmNo titration: HR in met 75 bpm
1Yang, Am Heart J 2006;152:983-902Juul, BMJ 2006;332:1482-8

Titration is the Key!Titration is the Key! 20062006 Observational studyObservational study11
272 vascular surgery pts, target HR 55-70 bpm272 vascular surgery pts, target HR 55-70 bpm OverallOverall
31% had myocardial ischemia31% had myocardial ischemia 16% had troponin release16% had troponin release 24% mortality rate at 2.6 years24% mortality rate at 2.6 years
Higher Higher ββ-blocker dose assoc w/ lower MI & death-blocker dose assoc w/ lower MI & death Conversely, higher HR assoc w/ higher MI & deathConversely, higher HR assoc w/ higher MI & death Titration seems to matterTitration seems to matter
2006 2006 DECREASE-IIDECREASE-II22
770 vascular surgery pts, 770 vascular surgery pts, intermediateintermediate cardiac risk cardiac risk DSE (386)DSE (386)intervention v. no test (384)intervention v. no test (384)
All patients beta blocked to target HR 60-65All patients beta blocked to target HR 60-65 No difference in DSE v. No test groupNo difference in DSE v. No test group HR < 65 v. HR > 65 (1.3% v. 5.2% death/MI rate)HR < 65 v. HR > 65 (1.3% v. 5.2% death/MI rate)
1 Feringa, Circulation 2006;114:1344-92 Poldermans, JACC 2006;48:964-9

Perioperative Beta Blocker Perioperative Beta Blocker Dosing:Dosing:
ACC/AHA RecommendationACC/AHA Recommendation ““Available evidence suggests, but does not Available evidence suggests, but does not
prove that, when it is possible, BB should be prove that, when it is possible, BB should be started several days or weeks before elective started several days or weeks before elective surgerysurgery, with the dose titrated to achieve a , with the dose titrated to achieve a resting HR b/w resting HR b/w 50-60 bpm50-60 bpm, to assure that the , to assure that the patient is indeed receiving the benefit of BB patient is indeed receiving the benefit of BB and should and should continue during the intraoperative continue during the intraoperative and post operative period to maintain a HR < and post operative period to maintain a HR < 80 bpm80 bpm.”.”
No definitive evidence that one drug is best.No definitive evidence that one drug is best.Fleisher, JACC 2006;47:2343-2354
•PBB probably good:•High risk patients•Start wks b/4 surg•Titration

POISE TrialPOISE Trial
8351 pts w/ or at risk of CAD8351 pts w/ or at risk of CAD 4174 metoprolol vs. 4177 placebo4174 metoprolol vs. 4177 placebo
Metoprolol CR 100 mg pre Metoprolol CR 100 mg pre Metoprolol CR 100 mg 6 hrs post Metoprolol CR 100 mg 6 hrs post Metoprolol CR 200 mg daily x 30 daysMetoprolol CR 200 mg daily x 30 days
MetoprolMetoprololol
PlaceboPlacebo
MI MI 3.6%3.6% 5.1%5.1%
CompositeComposite 5.8%5.8% 6.9%6.9%
Total Total mortalitymortality
3.1%3.1% 2.3%2.3%
StrokeStroke 1.0%1.0% 0.5%0.5%All comparisons statistically significant
PBB ↓ MI and cardiac death but↑ overall mortality and stroke
•Started right b/4 surg•High initial dose•No dose titration•Probably doesn’t change recs yet
Devereaux, Lancet online May 13, 2008

What is the next best step?What is the next best step?
A) A) Metoprolol to HR < 60 bpm Metoprolol to HR < 60 bpm
B)B) Metoprolol to HR 60-80 bpm Metoprolol to HR 60-80 bpm
C)C) Metoprolol to HR 80-100 bpmMetoprolol to HR 80-100 bpm
D)D) Metoprolol not indicatedMetoprolol not indicated
64 yo man w/ DM & CAD undergoing R THA64 yo man w/ DM & CAD undergoing R THAExam: 131/69,72,10; OtherwiseExam: 131/69,72,10; Otherwise normalnormalMeds: Glargine, Lispro, ACE, Amlodipine, Meds: Glargine, Lispro, ACE, Amlodipine, ASAASA

Anti-coagulationAnti-coagulation
Should I heparinize a patient Should I heparinize a patient with an acute stroke?with an acute stroke?

What is the next best step?What is the next best step?
A) A) UFH at therapeutic dosesUFH at therapeutic doses
B)B) LMWH at therapeutic dosesLMWH at therapeutic doses
C)C) Warfarin at therapeutic dosesWarfarin at therapeutic doses
D)D) UFH/LMWH at VTE prophylactic dosesUFH/LMWH at VTE prophylactic doses
E) No anticoagulationE) No anticoagulation
68 yo woman w/ DM, hyperlipidemia & CAD68 yo woman w/ DM, hyperlipidemia & CAD6 hrs R-sided UE>LE weakness, aphasia6 hrs R-sided UE>LE weakness, aphasiaMeds: Glargine, Lispro, ACE, simvastatin, Meds: Glargine, Lispro, ACE, simvastatin, ASAASA

BackgroundBackground
700,000 strokes/yr in US700,000 strokes/yr in US 85% are ischemic85% are ischemic Most are caused by acute blood clots in an artery in the Most are caused by acute blood clots in an artery in the
brainbrain Recurrent stroke is commonRecurrent stroke is common1-13%1-13% Post-stroke DVT, PE are also commonPost-stroke DVT, PE are also common
Anticoagulants used in acute stroke for > 50 yrsAnticoagulants used in acute stroke for > 50 yrs Increased risk of intra- & extra-cranial bleedingIncreased risk of intra- & extra-cranial bleeding
ControversyControversy When to start? Which agent?When to start? Which agent? Which route? Bolus vs. drip?Which route? Bolus vs. drip? Level of anticoagulationLevel of anticoagulation Type of strokeType of strokecardioembolic vs. non-cardioemboliccardioembolic vs. non-cardioembolic

Anticoagulants for Acute Ischemic Stroke
Question:Question: What is the effect of anticoagulation (AC) in the early What is the effect of anticoagulation (AC) in the early treatment (< 14 days) of acute stroke? treatment (< 14 days) of acute stroke?
Design:Design: Sys rev of 24 RCT early AC v. control in ischemic Sys rev of 24 RCT early AC v. control in ischemic CVACVA
Cochrane Review 2008

ResultsResults 24 trials (23,748 pts)24 trials (23,748 pts)
13/24 enrolled w/in 48 hours13/24 enrolled w/in 48 hours Duration of AC 1-2 weeks in 20; 1 mo in 4Duration of AC 1-2 weeks in 20; 1 mo in 4 UFH 8, LMWH 8, VKA 2, hepranoid 3, DTI 3UFH 8, LMWH 8, VKA 2, hepranoid 3, DTI 3 Studies of variable quality/designStudies of variable quality/design
Randomization, dosing, CT scans, asses DVT, Randomization, dosing, CT scans, asses DVT, antiplatelet use, duration of f/uantiplatelet use, duration of f/u
Variability in outcomes measuredVariability in outcomes measured CVA, ICH, ECH, death, death and dependency, DVT, CVA, ICH, ECH, death, death and dependency, DVT,
PEPE
Cochrane Review 2008

Recurrent Ischemic Stroke or Recurrent Ischemic Stroke or ICHICH
Ischemic strokeIschemic stroke 11 trials (21,605 11 trials (21,605
pts)pts) ↓↓ ischemic stroke ischemic stroke
(0.76, 0.65-0.88)(0.76, 0.65-0.88) NNT = 108NNT = 108
Intracranial Intracranial hemorrhagehemorrhage
16 trials (22,943 pts)16 trials (22,943 pts) Increased rate of ICH Increased rate of ICH
(2.55, 1.95-3.33)(2.55, 1.95-3.33) NNH = 131NNH = 131
AC reduces ischemic strokeAC reduces ischemic strokeAC increases ICH in dose dependent fashionAC increases ICH in dose dependent fashion
Cochrane Review 2008

Post-Stroke DVT/PEPost-Stroke DVT/PE
DVTDVT 10 trials (916 pts)10 trials (916 pts)
Reduced DVT rate Reduced DVT rate (0.21, 0.15-0.29)(0.21, 0.15-0.29)
NNT = 114NNT = 114
PEPE 14 trials (22,544 14 trials (22,544
pts)pts) Reduced PE rate Reduced PE rate
(0.6, 0.44-0.81)(0.6, 0.44-0.81) NNT = 127NNT = 127
AC reduces DVTAC reduces DVTAC reduces PEAC reduces PE
Cochrane Review 2008

Death & DependencyDeath & Dependency
8 trials (22,125 pts)8 trials (22,125 pts) No evidence that AC reduced death or No evidence that AC reduced death or
dependency (0.99; 0.93-1.04)dependency (0.99; 0.93-1.04) SubgroupSubgroup
No difference based on drug, dosing (proph No difference based on drug, dosing (proph v. adjusted)v. adjusted)
Cochrane Review 2008

Anticoagulants for Acute Ischemic Stroke
Question:Question: What is the effect of anticoagulation (AC) in the early What is the effect of anticoagulation (AC) in the early treatment (< 14 days) of acute stroke? treatment (< 14 days) of acute stroke?
Design:Design: Sys rev of 24 RCT early AC v. control in Sys rev of 24 RCT early AC v. control in ischemic CVAischemic CVA
Results:Results: Reduced: Ischemic strokes, NNT 108 Reduced: Ischemic strokes, NNT 108 DVT, NNT 114 DVT, NNT 114 PE, NNT 127PE, NNT 127Increased: Intracranial bleed, NNH 131Increased: Intracranial bleed, NNH 131 Extracranial bleed, NNH 128Extracranial bleed, NNH 128No change in death or dependencyNo change in death or dependency
Conclusion:Conclusion: AC doesn’t reduce risk of stroke, death or disabilityAC doesn’t reduce risk of stroke, death or disability Cardioembolic, atrial fib, large vessel atherosclerosis, Cardioembolic, atrial fib, large vessel atherosclerosis,
vertebrobasilar, cresendo, carotid dissection vertebrobasilar, cresendo, carotid dissectionLower rate of VTE offset by similar increase in ECHLower rate of VTE offset by similar increase in ECH
Comment:Comment: Data don’t support use of any form of AC w/in 14 d of Data don’t support use of any form of AC w/in 14 d of CVA CVA Low dose UFH/LMWH Low dose UFH/LMWH ↓↓ VTE but slightly VTE but slightly ↑↑ risk of ICH & ECH risk of ICH & ECH
Cochrane Review 2008

What is the next best step?What is the next best step?
A) A) UFH at therapeutic dosesUFH at therapeutic doses
B)B) LMWH at therapeutic dosesLMWH at therapeutic doses
C)C) Warfarin at therapeutic dosesWarfarin at therapeutic doses
D)D) UFH/LMWH at VTE prophylactic dosesUFH/LMWH at VTE prophylactic doses
E) No anticoagulationE) No anticoagulation
68 yo woman w/ DM, hyperlipidemia & CAD68 yo woman w/ DM, hyperlipidemia & CAD6 hrs R-sided UE>LE weakness, aphasia6 hrs R-sided UE>LE weakness, aphasiaMeds: Glargine, Lispro, ACE, simvastatin, Meds: Glargine, Lispro, ACE, simvastatin, ASAASA

HyperglycemiaHyperglycemia
How should hyperglycemia be How should hyperglycemia be managed in the hospitalized managed in the hospitalized
patient?patient?

What is the next best step?What is the next best step?
A) A) Continue home meds aloneContinue home meds alone
B)B) Continue home meds w/ sliding scale Continue home meds w/ sliding scale insulininsulin
C)C) Substitute sliding scale insulin aloneSubstitute sliding scale insulin alone
D)D) Substitute basal-bolus insulin regimenSubstitute basal-bolus insulin regimen
49 yo man w/ DM 49 yo man w/ DM Admitted to ward with CAP, BS 180 mg/dL Admitted to ward with CAP, BS 180 mg/dL Meds: Metformin, GlyburideMeds: Metformin, Glyburide

Blood Glucose TargetsBlood Glucose Targets
SettingSetting Blood Glucose TargetBlood Glucose Target
SICUSICU Close to 110 mg/dl; <140 Close to 110 mg/dl; <140 mg/dlmg/dl
MICUMICU <140 mg/dl<140 mg/dl
Med-SurgMed-Surg <126 mg/dl fasting; All <180-<126 mg/dl fasting; All <180-200200
ADA Guideline Diabetes Care 2009;32:S13-71

Diabetic ArmamentariumDiabetic ArmamentariumClassClass ExamplExampl
eeCommentComment
SulfonylureasSulfonylureas GlyburideGlyburide Hypoglycemia if NPOHypoglycemia if NPO
BiguanideBiguanide MetforminMetformin Lactic acidosis w/ AKILactic acidosis w/ AKI
ThiazolidinedioThiazolidinedionene
PioglitazoPioglitazonene
Increased fluid retentionIncreased fluid retention
MeglitinidesMeglitinides RepaglinidRepaglinidee
Parandial med; often Parandial med; often NPONPO
GLP-1 AnalogsGLP-1 Analogs ExenatideExenatide Parandial med; often Parandial med; often NPONPO
DPP-IV DPP-IV inhibitorsinhibitors
SitagliptinSitagliptin Parandial med; often Parandial med; often NPONPO
αα-glucosidase -glucosidase InhInh
AcarboseAcarbose Parandial med; often Parandial med; often NPONPO
Which leaves us with insulin...
ADA Guideline Diabetes Care 2009;32:S13-71

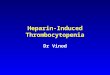
RABBIT-2: Changes in BG Concentration RABBIT-2: Changes in BG Concentration Basal-Bolus vs. SSI RegimenBasal-Bolus vs. SSI Regimen
*P < 0.01, †P < 0.05 vs. basal-bolus; RABBIT = Randomized Study of Basal-Bolus Insulin Therapy in the Inpatient Management of Patients With Type 2 Diabetes
Admit 1 2 3 4 5 6 7 8 9 10Days
BG
(m
g/d
L) *
* *† †
††
SSI
Basal-bolus
Umpierrez GE et al. Diabetes Care. 2007;30:2181.
N = 130 hospitalized insulin-naive T2DM patients
240
220
200
180
160
140
120
100
Mean BS < 14066% of Basal-Bolus38% of SSI No diff in hypoglycemia

How’d they do that?How’d they do that?
BS 140-200 = 0.4 BS 140-200 = 0.4 u/kg/du/kg/d
BS 201-400 = 0.5 BS 201-400 = 0.5 u/kg/du/kg/d ½ given as long-acting½ given as long-acting ½ given as short-acting ½ given as short-acting
divided b/4 mealsdivided b/4 meals 100kg patient, BS 180100kg patient, BS 180
100 x 0.4 = 40 units100 x 0.4 = 40 units 20 units glargine20 units glargine 7 units glulisine before 7 units glulisine before
each mealeach meal
If fasting BS > 140 If fasting BS > 140 ↑↑ glargine by 20%glargine by 20%
If fasting BS < 70 If fasting BS < 70 ↓↓ glargine by 20%glargine by 20%
If pre-meal BS > 140 If pre-meal BS > 140 Correctional glulisine Correctional glulisine
givengiven
Umpierrez GE et al. Diabetes Care. 2007;30:2181.
Generally d/c oralsDon’t use SSIBasal-bolus insulin

What is the next best step?What is the next best step?
A) A) Continue home meds aloneContinue home meds alone
B)B) Continue home meds w/ sliding scale Continue home meds w/ sliding scale insulininsulin
C)C) Substitute sliding scale insulin aloneSubstitute sliding scale insulin alone
D)D) Substitute basal-bolus insulin regimenSubstitute basal-bolus insulin regimen
49 yo man w/ DM 49 yo man w/ DM Admitted to ward with CAP, BS 180 mg/dL Admitted to ward with CAP, BS 180 mg/dL Meds: Metformin, GlyburideMeds: Metformin, Glyburide

ConclusionsConclusions
Perioperative Beta blockersPerioperative Beta blockers High risk patients (RCRI >/= 2)High risk patients (RCRI >/= 2) Start weeks before Start weeks before Titrate to HR < 60 bpmTitrate to HR < 60 bpm
Heparin in acute stroke doesn’t add benefitHeparin in acute stroke doesn’t add benefit Consider low dose SQ UFH for VTE prophylaxisConsider low dose SQ UFH for VTE prophylaxis
Basal-bolus insulin best achieves BG controlBasal-bolus insulin best achieves BG control Goal <140 for SICU/MICU & < 180 for med-surg ptsGoal <140 for SICU/MICU & < 180 for med-surg pts


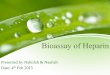
Hospital Mortality Rate and Mean Hospital Mortality Rate and Mean Glucose Levels in Critically Ill PatientsGlucose Levels in Critically Ill Patients
0
5
10
15
20
25
30
35
40
45
80–99 100–119 120–139 140–159 160–179 180–199 200–249 250–299 > 300
Mortality Rate (%)
Mean Glucose Value (mg/dL)
Retrospective review of 1,826 consecutive intensive care unit patients.
Krinsley JS. Mayo Clin Proc. 2003;78:1471–1478.

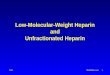
Hyperglycemia Is an Independent Marker of Hyperglycemia Is an Independent Marker of Inpatient Mortality RiskInpatient Mortality Risk
Umpierrez GE, et al. J Clin Endocrinol Metab. 2002;87:978–982.
1.73
16
0
2
4
6
8
10
12
14
16
18
In-hospital Mortality Rate
(%)
New Hyperglycemia
Known
Diabetes
Normoglycemia
P < 0.01
P < 0.01

Current PracticeCurrent Practice
ScenariosScenarios Neurologist AC Neurologist AC UseUse Stroke in evolutionStroke in evolution 51%51% Vertebrobasilar CVAVertebrobasilar CVA 30%30% Carotid territory CVACarotid territory CVA 31%31% Multiple TIAsMultiple TIAs 47%47% Atrial fibrillation and CVAAtrial fibrillation and CVA 88%88%
Al-Sadt Stroke 2002;33;1574-77

ConclusionsConclusions AC is not recommended to reduce risk of AC is not recommended to reduce risk of
death, disability or recurrent strokedeath, disability or recurrent stroke AC is not recommended in any specific AC is not recommended in any specific
sub-group after ischemic strokesub-group after ischemic stroke Cardioembolic, atrial fib, large vessel Cardioembolic, atrial fib, large vessel
atherosclerosis, vertebrobasilar, cresendo, atherosclerosis, vertebrobasilar, cresendo, carotid dissectioncarotid dissection
SQ UFH or low dose LMWH may be used SQ UFH or low dose LMWH may be used for VTE prophylaxis in high-risk patients for VTE prophylaxis in high-risk patients but non-pharmacologic/aspirin therapy but non-pharmacologic/aspirin therapy may be just as good w/o risk of bleedingmay be just as good w/o risk of bleeding
AHA Guideline Stroke 2007;38:1655-711Cochrane Review 2008

Blood Glucose TargetsBlood Glucose Targets
SettingSetting Blood Glucose TargetBlood Glucose Target
SICUSICU Close to 110 mg/dl; <140 Close to 110 mg/dl; <140 mg/dlmg/dl
MICUMICU <140 mg/dl<140 mg/dl
Med-SurgMed-Surg <126 mg/dl fasting; All <180-<126 mg/dl fasting; All <180-200200
Data for SICU pts strongestData for SICU pts strongestData for MICU pts less strongData for MICU pts less strong M/S little evidence for interventionM/S little evidence for intervention
ADA Guideline Diabetes Care 2009;32:S13-71