Embed Size (px)
Citation preview
S P E C I A L ARTICLE
Controversies in Antithrombotic Therapy for Patients with Mechanical Heart Valves
Henry I. Bussey, Pharm.D., FCCF‘, and Roger M. Lyons, M.D., FACP
Current anticoagulation guidelines for patients with mechanical heart valves are based on studies that are seriously flawed in that they used prothrombin time ratios rather than the international normalized ratio (INR) and failed to consider the level of anticoagulation actually achieved. Available data suggest that the appropriate INR range varies according to risk factors and that “tight control” of the INR is of critical importance in reducing thromboembolic and hemorrhagic events. Whether antiplatelet therapy adds benefit to an appro- priately controlled level of anticoagulation is not clear. During pregnancy, warfarin is contraindicated; adjusted-dose heparin is recommended by published American and European guidelines. Even so, one small study suggests that this may be inadequate. Topical antifibrinolytic agents can negate the need to alter systemic anticoagulation during dental surgery. (Pharmacotherapy 1998; 18(3):45 1-455)
OUTLINE
Correct INR Range Addition of Aspirin or Dipyridamole versus “Tight
Anticoagulation dur ing Pregnancy Anticoagulation dur ing Dental Procedures Summary
Control”
What is the correct level of anticoagulation for the patient with a mechanical heart valve? Should aspirin or dipyridamole be added to the regimen? How should anticoagulation be managed during pregnancy and dental procedures? Although definitive answers do not exist, it is imperative that these questions be understood when making decisions to minimize the risk of thromboembolism and major hemorrhage in
From the College of Pharmacy, University of Texas at Aus t in , a n d t h e Division of Pharmacotherapy, The University of Texas Health Science Center at San Antonio (Dr. Bussey); and Anticoagulation Clinics of North America, and Hematology and Oncology Associates of South Texas (Drs. Bussey and Lyons), San Antonio, Texas.
Address reprint requests to Henry 1. Bussey, Pharm.D., Division of Pharmacotherapy, The University of Texas Health Science Center at San Antonio, San Antonio, TX 78284-6220.
patients with mechanical heart valves.
Correct INR Range
The American College of Chest Physicians (ACCP) Consensus Conference on Antithrombotic Therapy recommended an international normalized ratio ( I N R ) of 2.5-3.5 for mechanical heart valves, but this is a grade C recommendation, meaning that data supporting it are weak.’ The fact that the mean INR before a stroke was 2.8 in one key study suggests that a value of 2.5-3.5 is not optimal for all patients.2 A higher INR is suggested for caged ball or caged disk valves, and the addi t ion of aspirin or dipyridamole is suggested to provide additional benefit, but at an increased risk of bleeding.’ Two primary weaknesses in data on the recommended INR range are that most studies used the prothrombin time ratio (PTR) rather than the INR, and they considered only the targeted INR range, not the range actually achieved.
Because of variability in thromboplastin sensitivity, any given level of anticoagulation with warfarin will yield significantly different PTR values when tested in different laboratories
452 PHARMACOTHERAPY Volume 18, Number 3, 1998
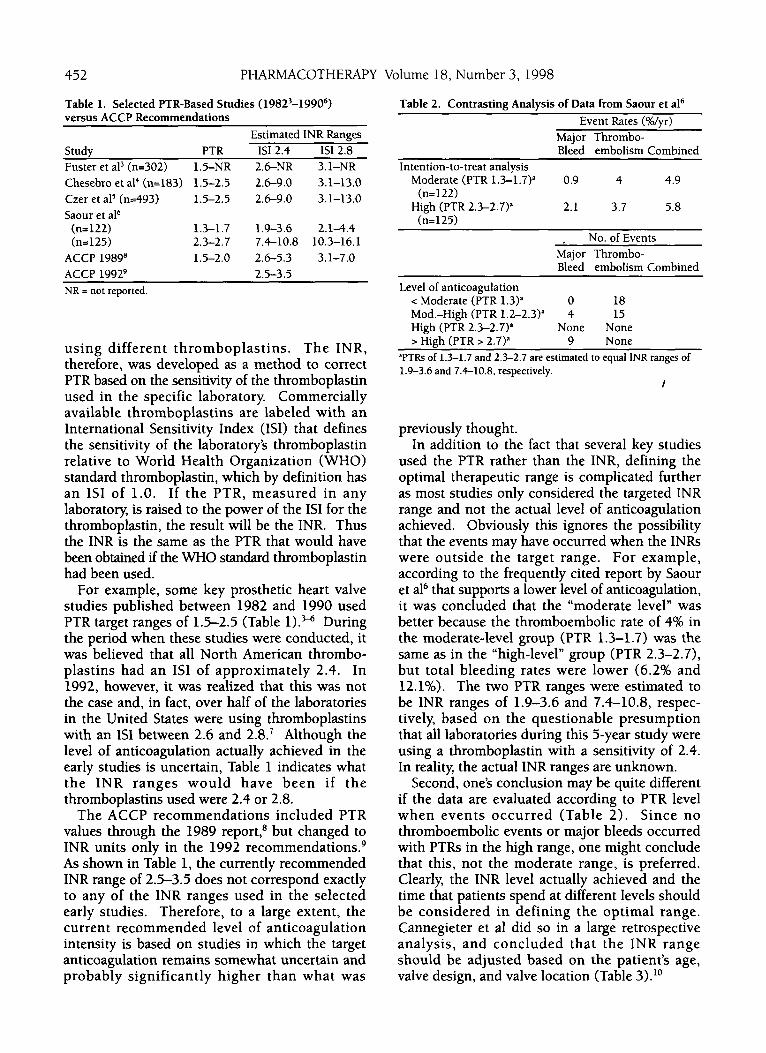
Table 1. Selected PTR-Based Studies ( 19823-19906) versus ACCP Recommendations
Study PTR Fuster et a13 (n=302) 1.5-NR Chesebro et a14 (n=183) 1.5-2.5
Saour et aI6 Czer et a15 (n=493) 1.5-2.5
(n- 1 22) 1.3-1.7 (n= 125) 2.3-2.7
ACCP 1989” 1.5-2.0 ACCP 19929
Estimated INR Ranges IS1 2.4 IS1 2.8 2.6-NR 3.1-NR 2.6-9.0 3.1-13.0 2.6-9.0 3.1-13.0
1.9-3.6 2 . 1 4 . 4 7.4-10.8 10.3-16.1 2.6-5.3 3.1-7.0 2.5-3.5
NR = not reported.
using different thromboplastins. The INR, therefore, was developed as a method to correct PTR based on the sensitivity of the thromboplastin used in the specific laboratory. Commercially available thromboplastins are labeled with an International Sensitivity Index (ISI) that defines the sensitivity of the laboratory’s thromboplastin relative to World Health Organization (WHO) standard thromboplastin, which by definition has an IS1 of 1.0. If the PTR, measured in any laboratory, is raised to the power of the IS1 for the thromboplastin, the result will be the INR. Thus the INR is the same as the PTR that would have been obtained if the WHO standard thromboplastin had been used.
For example, some key prosthetic heart valve studies published between 1982 and 1990 used PTR target ranges of 1.5-2.5 (Table l).M During the period when these studies were conducted, it was believed that all North American thrombo- plastins had an IS1 of approximately 2.4. In 1992, however, it was realized that this was not the case and, in fact, over half of the laboratories in the United States were using thromboplastins with an IS1 between 2.6 and 2.8.’ Although the level of anticoagulation actually achieved in the early studies is uncertain, Table 1 indicates what the INR ranges would have been i f the thromboplastins used were 2.4 or 2.8.
The ACCP recommendations included PTR values through the 1989 report: but changed to INR units only in the 1992 recommendation^.^ As shown in Table 1, the currently recommended INR range of 2.5-3.5 does not correspond exactly to any of the INR ranges used in the selected early studies. Therefore, to a large extent, the current recommended level of anticoagulation intensity is based on studies in which the target anticoagulation remains somewhat uncertain and probably significantly higher than what was
Table 2. Contrasting Analysis of Data from Saour et a16 Event Rates (%/yr)
Major Thrombo- Bleed embolism Combined
Intention-to-treat analysis Moderate (PTR 1.3-1.7)” 0.9 4 4.9
High (PTR 2.3-2.7)a 2.1 3.7 5.8 (n= 122)
(n=125) , No. of Events
Major Thrombo- Bleed embolism Combined
Level of anticoagulation < Moderate (PTR 1.3)” 0 18 Mod.-High (PTR 1.2-2.3)” 4 15 High (PTR 2.3-2.7)a None None > High (PTR > 2.7)a 9 None
‘PTRs of 1.3-1.7 and 2.3-2.7 are estimated to equal INR ranges of 1.9-3.6 and 7.4-10.8, respectively.
I
previously thought. In addition to the fact that several key studies
used the PTR rather than the INR, defining the optimal therapeutic range is complicated further as most studies only considered the targeted INR range and not the actual level of anticoagulation achieved. Obviously this ignores the possibility that the events may have occurred when the INRs were outside the target range. For example, according to the frequently cited report by Saour et a16 that supports a lower level of anticoagulation, it was concluded that the “moderate level” was better because the thromboembolic rate of 4% in the moderate-level group (PTR 1.3-1.7) was the same as in the “high-level” group (PTR 2.3-2.7), but total bleeding rates were lower (6.2% and 12.1%). The two PTR ranges were estimated to be INR ranges of 1.9-3.6 and 7.4-10.8, respec- tively, based on the questionable presumption that all laboratories during this 5-year study were using a thromboplastin with a sensitivity of 2.4. In reality, the actual INR ranges are unknown.
Second, one’s conclusion may be quite different if the data are evaluated according to PTR level when events occurred (Table 2). Since no thromboembolic events or major bleeds occurred with PTRs in the high range, one might conclude that this, not the moderate range, is preferred. Clearly, the INR level actually achieved and the time that patients spend at different levels should be considered in defining the optimal range. Cannegieter et a1 did so in a large retrospective analysis, and concluded that the INR range should be adjusted based on the patient’s age, valve design, and valve location (Table 3). lo
HEART VALVE ANTITHROMBOTIC THERAPY Bussey and Lyons 453
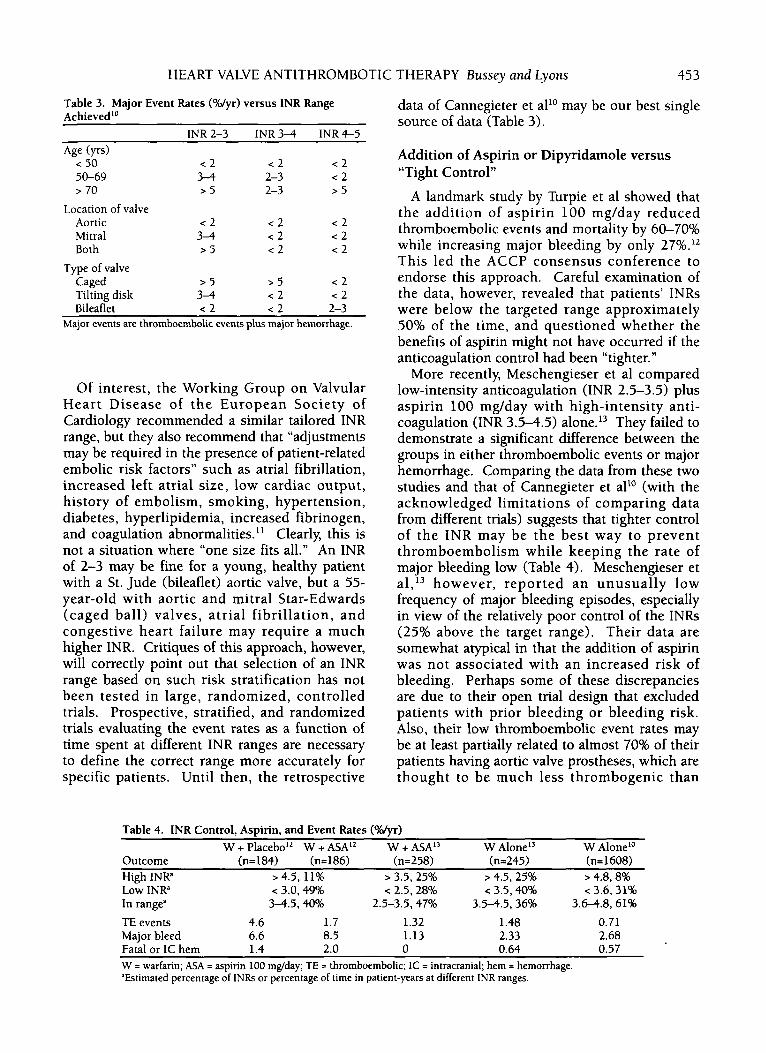
data of Cannegieter et all0 may be our best single source of data (Table 3).
Table 3. Major Event Rates (“Myr) versus INR Range Achieved1“
INR2-3 INR3-4 INR4-5 Age (yrs)
c 50 50-69
Addition of Aspirin or Dipyridamole versus c 2 c 2 c 2 3 4 2-3 c 2 “Tight Control”
7 70 > 5 2-3 > 5
Aortic < 2 c 2 < 2 Mitral 3-4 c 2 < 2 Both > 5 c 2 < 2
Location of valve
Type of valve Caged > 5 > 5 < 2 Tilting disk 3-4 < 2 < 2 Bileaflet c 2 < 2 2-3
Major events are thromboembolic events plus major hemorrhage.
Of interest, the Working Group on Valvular Heart Disease of the European Society of Cardiology recommended a similar tailored INR range, but they also recommend that “adjustments may be required in the presence of patient-related embolic risk factors” such as atrial fibrillation, increased left atrial size, low cardiac output, history of embolism, smoking, hypertension, diabetes, hyperlipidemia, increased fibrinogen, and coagulation abnormalities. l1 Clearly, this is not a situation where “one size fits all.” An INR of 2-3 may be fine for a young, healthy patient with a St. Jude (bileaflet) aortic valve, but a 55- year-old with aortic and mitral Star-Edwards (caged ball) valves, atrial fibrillation, and congestive heart failure may require a much higher INR. Critiques of this approach, however, will correctly point out that selection of an INR range based on such risk stratification has not been tested in large, randomized, controlled trials. Prospective, stratified, and randomized trials evaluating the event rates as a function of time spent at different INR ranges are necessary to define the correct range more accurately for specific patients. Until then, the retrospective
A landmark study by Turpie et a1 showed that the addition of aspirin 100 mg/day reduced thromboembolic events and mortality by 60-70% while increasing major bleeding by only 27%.12 This led the ACCP consensus conference to endorse this approach. Careful examination of the data, however, revealed that patients’ INRs were below the targeted range approximately 50% of the time, and questioned whether the benefits of aspirin might not have occurred if the anticoagulation control had been “tighter.”
More recently, Meschengieser et a1 compared low-intensity anticoagulation (INR 2.5-3.5) plus aspirin 100 mg/day with high-intensity anti- coagulation (INR 3.5-4.5) a10ne.l~ They failed to demonstrate a significant difference between the groups in either thromboembolic events or major hemorrhage. Comparing the data from these two studies and that of Cannegieter et all0 (with the acknowledged limitations of comparing data from different trials) suggests that tighter control of the I N R may be the best way to prevent thromboembolism while keeping the rate of major bleeding low (Table 4). Meschengieser et al,13 however, reported an unusually low frequency of major bleeding episodes, especially in view of the relatively poor control of the INRs (25% above the target range). Their data are somewhat atypical in that the addition of aspirin was not associated with an increased risk of bleeding. Perhaps some of these discrepancies are due to their open trial design that excluded patients with prior bleeding or bleeding risk. Also, their low thromboembolic event rates may be at least partially related to almost 70% of their patients having aortic valve prostheses, which are thought to be much less thrombogenic than
Table 4. INR Control, Aspirin, and Event Rates (Wyr) W + Placebo” W + ASA” W + ASA” W Alone” W Alone”
Outcome (n=184) (n=186) (n=258) (n=245) (n= 1608) High lNRa > 4.5, 11% > 3.5, 25% > 4.5, 25% > 4.8,8% Low INRa < 3.0,49% < 2.5, 28% < 3.5,40% < 3.6,31% In rangea 34 .5 ,40% 2.5-3.5,47% 3.54.5,36% 3.6-4.8, 61% TE events 4.6 1.7 1.32 1.48 0.71 Major bleed 6.6 8.5 1.13 2.33 2.68 Fatal or 1C hem 1.4 2.0 0 0.64 0.57 W = warfarin; ASA = aspirin 100 mg/day; TE = thromboembolic; 1C = intracranial; hem = hemorrhage. “Estimated percentage of INRs or percentage of time in patient-years at different INR ranges.
454 PHARMACOTHERAPY Volume 18, Number 3, 1998
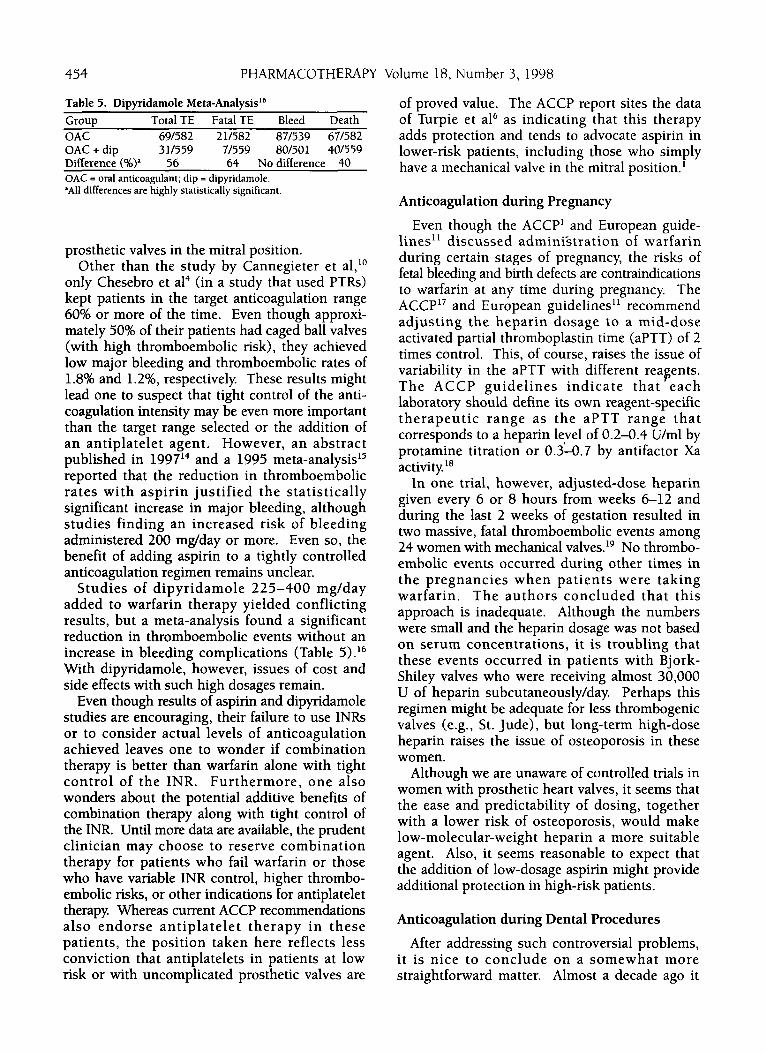
Table 5. Dipwidamole Meta-Analyd6 ~
Group Total TE Fatal TE Bleed Death OAC 69/582 211582 871539 671582 OAC + dip 31/559 7/559 80/501 401559 Difference (%>a 56 64 Nodifference 40 OAC = oral anticoagulant; dip = dipyridamole. 'All differences are highly statistically significant.
prosthetic valves in the mitral position. Other than the study by Cannegieter et al,1°
only Chesebro et a14 (in a study that used PTRs) kept patients in the target anticoagulation range 60% or more of the time. Even though approxi- mately 50% of their patients had caged ball valves (with high thromboembolic risk), they achieved low major bleeding and thromboembolic rates of 1.8% and 1.2%, respectively These results might lead one to suspect that tight control of the anti- coagulation intensity may be even more important than the target range selected or the addition of an antiplatelet agent. However, an abstract published in 199714 and a 1995 meta-analysis'* reported that the reduction in thromboembolic rates with aspirin justified the statistically significant increase in major bleeding, although studies finding an increased risk of bleeding administered 200 mg/day or more. Even so, the benefit of adding aspirin to a tightly controlled anticoagulation regimen remains unclear.
Studies of dipyridamole 225-400 mg/day added to warfarin therapy yielded conflicting results, but a meta-analysis found a significant reduction in thromboembolic events without an increase in bleeding complications (Table 5) .16
With dipyridamole, however, issues of cost and side effects with such high dosages remain.
Even though results of aspirin and dipyridamole studies are encouraging, their failure to use IN% or to consider actual levels of anticoagulation achieved leaves one to wonder if combination therapy is better than warfarin alone with tight control of the INR. Furthermore, one also wonders about the potential additive benefits of combination therapy along with tight control of the INR. Until more data are available, the prudent clinician may choose to reserve combination therapy for patients who fail warfarin or those who have variable INR control, higher thrombo- embolic risks, or other indications for antiplatelet therapy Whereas current ACCP recommendations also endorse antiplatelet therapy in these patients, the position taken here reflects less conviction that antiplatelets in patients at low risk or with uncomplicated prosthetic valves are
of proved value. The ACCP report sites the data of Turpie et a16 as indicating that this therapy adds protection and tends to advocate aspirin in lower-risk patients, including those who simply have a mechanical valve in the mitral position.'
Anticoagulation during Pregnancy
Even though the ACCP' and European guide- lines" discussed admini'stration of warfarin during certain stages of pregnancy, the risks of fetal bleeding and birth defects are contraindications to warfarin at any time during pregnancy. The ACCP17 and European guidelines" recommend adjusting the heparin dosage to a mid-dose activated partial thromboplastin time (aPTT) of 2 times control. This, of course, raises the issue of variability in the aPTT with different reagents. The ACCP guidelines indicate that each laboratory should define its own reagent-specific therapeutic range as the aPTT range that corresponds to a heparin level of 0.2-0.4 U/ml by protamine titration or 0.3-0.7 by antifactor Xa activity '*
In one trial, however, adjusted-dose heparin given every 6 or 8 hours from weeks 6-12 and during the last 2 weeks of gestation resulted in two massive, fatal thromboembolic events among 24 women with mechanical ~a1ves.l~ No thrombo- embolic events occurred during other times in the pregnancies when patients were taking warfarin. The authors concluded that this approach is inadequate. Although the numbers were small and the heparin dosage was not based on serum concentrations, it is troubling that these events occurred in patients with Bjork- Shiley valves who were receiving almost 30,000 U of heparin subcutaneously/day Perhaps this regimen might be adequate for less thrombogenic valves (e.g., St. Jude), but long-term high-dose heparin raises the issue of osteoporosis in these women.
Although we are unaware of controlled trials in women with prosthetic heart valves, it seems that the ease and predictability of dosing, together with a lower risk of osteoporosis, would make low-molecular-weight heparin a more suitable agent. Also, it seems reasonable to expect that the addition of low-dosage aspirin might provide additional protection in high-risk patients.
Anticoagulation during Dental Procedures
After addressing such controversial problems, it is nice to conclude on a somewhat more straightforward matter. Almost a decade ago it

HEART VALVE ANTITHROMBOTIC THERAPY Bussey and Lyons 455
was reported that an antifibrinolytic could be used as a mouthwash in fully anticoagulated patients to prevent bleeding from dental proce- dures.20 Either tranexamic acid or aminocaproic acid can be used as a mouthwash to maintain local hemostasis without altering the patient’s systemic anticoagulation.” Although different regimens have been tried, one published approach is to wash the mouth with the solution every 6 hours for approximately 2 days.
Summary
Available data are inadequate to define the appropriate anticoagulation range for all patients with mechanical heart valves, but a number of identified risk factors can stratify patients according to risk of thromboembolism and major hemorrhage. The appropriate intensity of anti- coagulation can then be estimated by carefully weighing these two risks. Whether combined warfarin and antiplatelet therapy is superior to tight control with warfarin alone is not established. Even so, one may choose to add low-dose aspirin or dipyridamole to warfarin therapy for patients who appear to be at increased risk of thrombo- embolism or those who require antiplatelet therapy for other indications. Although aspirin is prescribed more commonly in such patients, a meta-analysis suggests that dipyridamole may offer equivalent protection without the bleeding risk reported in some aspirin studies.
Anticoagulation during pregnancy in these patients is problematic. Warfarin is contra- indicated, but the recommended adjusted dosage of subcutaneous heparin may be inadequate. Low-molecular-weight heparin may offer a significant advantage, but studies have not been done in patients with mechanical heart valves. Finally, i t is not necessary to interrupt anti- coagulation for dental procedures since bleeding can be controlled locally with an antifibrinolytic mouthwash.
References 1. Stein PD, Alpert JS, Copeland JG 111, et al. Antithrombotic
therapy in patients with mechanical and biological prosthetic heart valves. Chest 1995;108(4 suppl):371S9.
2. Turpie AGG, Laupacis A, Hirsh J. Warfarin and aspirin after heart valve replacement [letter]. N Engl J Med 1994;330:508-9.
3. Fuster V, Pumphrey CW, McGoon MD, Chesebro JH, Pluth JR, McGoon DC. Systemic thromboembolism in mitral and aortic Starr-Edwards prostheses: a 10-19 year follow-up.
Circulation 1982;66(suppl 1):1-157-61, 4. Chesebro JH, Fuster V, Elveback LR, et al. Trial of combined
warfarin plus dipyridamole or aspirin therapy in prosthetic heart valve replacement: danger of aspirin compared with dipyridamole. Am J Cardiol 1983;51:153741.
5. Czer LSC, Matloff JM, Chaux A, De Robertis M, Steward ME, Gray RJ. The St. Jude valve: analysis of thromboembolism, warfarin-related hemorrhage, and survival. Am Heart J
6. Saour JN, Seck JO, Mamo LAR, Gallus AS. Trial of different intensities of anticoagulation in patients with prosthetic heart valves. N Engl J Med 1990;322:42f3-32.
7. Bussey HI, Force RW, Bianco TM, Leonard AD. Reliance on prothrombin time ratios causes significant errors in anticoagulation therapy. Arch Intern Med 1992;152:27H2.
8. American College of Chest Physicians and National Heart, Lung, and Blood Institute. ACCP/NHLBI national conference on antithrombotic therapy. Chest 1989;89(suppl): 1-169.
9. American College of Chest Physicians. Third ACCP Consensus Conference on antithrombotic therapy. Chest 1992;102(suppl): 1S-549.
10. Cannegieter SC, Rosendaal FR, Wintzen AR, et al. Optimal oral anticoagulant therapy in patients with mechanical heart valves. N Engl J Med 1995;333:11-17.
1. Gohlke-Banvolf C, Acar J, Oakley C, et al. Guidelines for prevention of thromboembolic events in valvular heart disease. Eur Heart J 1995;16:1320-30.
2. Turpie AGG, Gent M, Laupacis A, et al. A comparison of aspirin with placebo in patients treated with warfarin after heart-valve replacement. N Engl J Med 1993;329:524-9.
3. Meschengieser SS, Fondevila CG, Frontroth J, Santarelli MT, Lazzari MA. Low-intensity oral anticoagulation plus low-dose aspirin versus high-intensity oral anticoagulation alone: a randomized trial in patients with mechanical prosthetic heart valves. J Thorac Cardiovasc Surg 1997;
14. Laffort P, Roudaut R, Roques E, et al. Frequency of prosthetic valve related complications with oral anticoagulant combined with aspirin after mitral valve replacement by St. Jude medical prosthesis [abstr]. J Am Coll Cardiol 1997;29:427A.
15. Cappelleri JC, Fiore LD, Brophy MT, Deykin D, Lau J. Efficacy and safety of combined anticoagulant and antiplatelet therapy versus anticoagulant monotherapy after mechanical heart-valve replacement; a meta-analysis. Am Heart J
16. Pouleur H, Buyse M. Effects of dipyridamole in combination with anticoagulant therapy on survival and thromboembolic events in patients with prosthetic heart valves; a meta-analysis of the randomized trials. J Thorac Cardiovasc Surg 1995;llO: 463-72.
17. Ginsburg JS, Hirsh J. Use of antithrombotic agents during pregnancy. Chest 1995;108(4 suppl):305Sll.
18. Hirsh J, Raschke R, Warkentin TE, et al. Heparin: mechanism of action, pharmacokinetics, dosing considerations, moni- toring, efficacy, and safety. Chest 1995;108(4 suppl):258S75.
19. Salazar E, Izaguirre R, Verdeijo J, Mutchinick 0. Failure of adjusted doses of subcutaneous heparin to prevent thromboembolic phenomena in pregnant patients with mechanical cardiac valve prostheses. J Am Coll Cardiol 1996;27: 1698-1703.
20. Sindet-Pedersen S , Ramstrom G, Bernvil S , et al. Hemo- static effect of tranexamic acid mouth wash in anticoagulant- treated patients undergoing oral surgery. N Engl J Med 1989;320:840.
21. Souto JC, Oliver A, Zauzu-Jausoro I, Vives A, Fontcuberta J. Oral surgery in anticoagulated patients without reducing the dose of oral anticoagulant: a prospective randomized study. J Oral Maxillofac Surg 1996;54:27-32.
1987;114:389-97.
113:9 10-16.
1995;130:547-52.