Embed Size (px)
Citation preview

Controversial therapies in Controversial therapies in Neonatal CareNeonatal Care
Julia Trintis, D.O.Julia Trintis, D.O.

ObjectivesObjectives
Discuss respiratory failure in premature Discuss respiratory failure in premature newborns. newborns.
Discuss current indications for inhaled Discuss current indications for inhaled nitric oxide therapy in newborns.nitric oxide therapy in newborns.
Discuss chronic lung disease in newborns. Discuss chronic lung disease in newborns.
Discuss the benefits and hazards of Discuss the benefits and hazards of postnatal steroids.postnatal steroids.

Respiratory Failure: Risk FactorsRespiratory Failure: Risk Factors
PrematurityPrematurity
Pulmonary DiseasePulmonary Disease
Respiratory infectionsRespiratory infections
Congenital AnomaliesCongenital Anomalies
Congenital heart Congenital heart diseasedisease
Surfactant protein Surfactant protein deficienciesdeficiencies

Bronchopulmonary DysplasiaBronchopulmonary Dysplasia
Described by Northway in 1967Described by Northway in 1967
Severe chronic lung injury in premature infants Severe chronic lung injury in premature infants who survived hyaline membrane diseasewho survived hyaline membrane disease
Four distinct stagesFour distinct stages– Respiratory distress syndromeRespiratory distress syndrome– Alveolar interstitial edemaAlveolar interstitial edema– Extensive bronchial and bronchioalar metaplasia and Extensive bronchial and bronchioalar metaplasia and
hyperplasia, Cystic emphysema and overinflationhyperplasia, Cystic emphysema and overinflation– Massive fibrosis, destruction of alveoli and airways, Massive fibrosis, destruction of alveoli and airways,
and consolidationand consolidation

Evolution of “Bronchopulmonary Evolution of “Bronchopulmonary Dysplasia”Dysplasia”
Classic BPDClassic BPD New BPDNew BPD– Extensive, diffuse fibroproliferationExtensive, diffuse fibroproliferation Rare fibrosisRare fibrosis– Alternating atelectasis with hyperinflationAlternating atelectasis with hyperinflation Less heterogeneityLess heterogeneity– Severe airway epithelial lesionsSevere airway epithelial lesions Mild airway Mild airway
epithelial lesionsepithelial lesions– Marked airway smooth muscle hyperplasiaMarked airway smooth muscle hyperplasia Milder airway changesMilder airway changes

Definition of BPD and Diagnostic Definition of BPD and Diagnostic CriteriaCriteria

EpidemiologyEpidemiology
BPD relatively rare in infants born beyond 32 BPD relatively rare in infants born beyond 32 weeksweeksNICHD (501-1500 grams): 22%NICHD (501-1500 grams): 22%– Less than 1000 grams: 40%Less than 1000 grams: 40%
““Although there has been a marked decrease in Although there has been a marked decrease in BPD in larger infants, recent data from Vermont BPD in larger infants, recent data from Vermont Oxford database and NICHD network indicate Oxford database and NICHD network indicate that in the years since 1996, there has been no that in the years since 1996, there has been no further decrease in the incidence of BPD.” further decrease in the incidence of BPD.” (Taeusch)(Taeusch)

Pathogenesis of BPDPathogenesis of BPD
CP Spear 2006

Strategies for preventing BPDStrategies for preventing BPD
Antenatal steroidsAntenatal steroids
SurfactantSurfactant
Permissive hypercapniaPermissive hypercapnia
Ventilator strategiesVentilator strategies
Reduce “excessive” O2 Reduce “excessive” O2 useuse
Good nutritionGood nutrition
Postnatal steroidsPostnatal steroids
Inhaled Nitric Oxide???Inhaled Nitric Oxide???

Current indications for inhaled Current indications for inhaled nitric oxide therapy in newbornsnitric oxide therapy in newborns
Selective pulmonary Selective pulmonary vasodilatorvasodilatorImproves oxygenation Improves oxygenation and reduces need for and reduces need for ECMO in term infants ECMO in term infants with PPHNwith PPHN

Inhaled NO Therapy in Premature Newborns
Initial reports showed iNO Initial reports showed iNO improved oxygenation in improved oxygenation in preterm infants with preterm infants with severe respiratory failure severe respiratory failure and with developing or and with developing or established BPDestablished BPD
Kinsella 1999, Banks 1999, Clark 2002

Animal ModelsAnimal Models
Reduces lung inflammationReduces lung inflammation
Improves surfactant functionImproves surfactant function
Attenuates hyperoxic lung injuryAttenuates hyperoxic lung injury
Promotes lung growthPromotes lung growth
Kang 2002, Ballard 2006, Cotton 2006
Potential Therapeutic TargetsPotential Therapeutic Targets
Surfactant function/ productionSurfactant function/ production
Improve gas exchangeImprove gas exchange
Reduce FiO2Reduce FiO2
Lower pulmonary artery pressureLower pulmonary artery pressure
Anti-inflammatory effectsAnti-inflammatory effects
Preserve or stimulate angiogenesis and Preserve or stimulate angiogenesis and alveolarization in the developing lungalveolarization in the developing lung

Inhaled NO in Premature Newborns:Randomized Placebo-Controlled Trials
Author Year Patient # Design
Schreiber 2003 207 Early, single center
Van Meurs 2005 420 Early, Brief, sick
Kinsella 2006 793 Early mild disease
Ballard 2006 582 Evolving BPD
EUNO 2008 800 Early, mild disease
Abman

Schreiber, 2003Schreiber, 2003
Single center studySingle center studyRandomized, double-blind, placebo controlled trialRandomized, double-blind, placebo controlled trial207 patients 207 patients Showed reduction in the combined outcome of death Showed reduction in the combined outcome of death and BPD in preterm infants treated with inhaled Nitric and BPD in preterm infants treated with inhaled Nitric Oxide Oxide

Van Meurs, 2005Van Meurs, 2005
Large, Multicenter studyLarge, Multicenter studyRandomized, double-blind, placebo controlled trialRandomized, double-blind, placebo controlled trial420 neonates420 neonatesShowed no significant reduction in rates of death or BPD Showed no significant reduction in rates of death or BPD with inhaled nitric oxide in preterm infants with a birth with inhaled nitric oxide in preterm infants with a birth weight of less than 1500 gramsweight of less than 1500 grams

Kinsella, 2006Kinsella, 2006
Large, Multicenter studyLarge, Multicenter studyRandomized, double-blind, placebo controlled trialRandomized, double-blind, placebo controlled trial793 neonates793 neonatesLow dose inhaled NO (5 ppm) did not reduce the overall incidence Low dose inhaled NO (5 ppm) did not reduce the overall incidence of BPD, except among infants with a birth weight of at least 1000 g, of BPD, except among infants with a birth weight of at least 1000 g, but it did reduce the overall risk of brain injury.but it did reduce the overall risk of brain injury.

Ballard, 2006Ballard, 2006
Large, Multicenter studyLarge, Multicenter studyRandomized, double-blind, placebo controlled trialRandomized, double-blind, placebo controlled trial582 neonates582 neonatesEnrolled infants who were ventilator dependent at 7 to 21 Enrolled infants who were ventilator dependent at 7 to 21 days of age.days of age.Randomly assigned to 24 day course of nitrogen placebo Randomly assigned to 24 day course of nitrogen placebo or inhaled NO at initial dose of 20 ppmor inhaled NO at initial dose of 20 ppmNO treatment improved survival at 36 weeks PMA NO treatment improved survival at 36 weeks PMA without BPD ( 43.9% vs 36.8%) and reduced the without BPD ( 43.9% vs 36.8%) and reduced the duration of oxygen therapy and hospitalization.duration of oxygen therapy and hospitalization.

European NO (EUNO) trialEuropean NO (EUNO) trial
Large, Multicenter study (35 centers)Large, Multicenter study (35 centers)Randomized, double-blind, placebo controlled trialRandomized, double-blind, placebo controlled trial800 neonates800 neonatesPreemies 24-29 weeks GAPreemies 24-29 weeks GAMild to moderate respiratory failureMild to moderate respiratory failureRandomized to receive iNO 5ppm or placebo for 7-21 Randomized to receive iNO 5ppm or placebo for 7-21 daysdaysResults pending Results pending – primary endpoint of chronic oxygen dependency reduction at 36 primary endpoint of chronic oxygen dependency reduction at 36
weeks' postconceptional age weeks' postconceptional age – long-term lung and brain will be followed-up until 7 years of age. long-term lung and brain will be followed-up until 7 years of age.

Conclusion: Does inhaled NO have a role in the treatment Conclusion: Does inhaled NO have a role in the treatment of preterm infants with respiratory failure?of preterm infants with respiratory failure?
Offering the critically ill, very preterm infant Offering the critically ill, very preterm infant early, sustained low dose prophylactic treatment early, sustained low dose prophylactic treatment with NO does not appear to improve survival or with NO does not appear to improve survival or BPD.BPD.Data on effective dose, duration, time of Data on effective dose, duration, time of initiation, and selection of infants most likely to initiation, and selection of infants most likely to benefit remain unclear.benefit remain unclear.Additional studies need to be performed before Additional studies need to be performed before the precise role of iNO in preventing BPD can be the precise role of iNO in preventing BPD can be defined.defined.Long term follow up is essential!Long term follow up is essential!

Postnatal Steroids and Chronic Lung Disease: Postnatal Steroids and Chronic Lung Disease: The Good, the Bad, and the UglyThe Good, the Bad, and the Ugly

Chronic lung diseaseChronic lung disease
defined as oxygen dependence at 36 defined as oxygen dependence at 36 weeks postconceptual age or oxygen weeks postconceptual age or oxygen requirement for >28 days. requirement for >28 days.
Associated with:Associated with:– poor nutrition and growthpoor nutrition and growth– poor feeding skillspoor feeding skills– prolonged hospitalization and episodes of prolonged hospitalization and episodes of
nosocomial infectionnosocomial infection

Story of steroids: “hastened Story of steroids: “hastened weaning from ventilator”weaning from ventilator”
1980’s: initial reports suggested short term benefits of 1980’s: initial reports suggested short term benefits of steroids in vent dependent childrensteroids in vent dependent childrenMammel 1983Mammel 1983– Dexamethasone used with severe BPDDexamethasone used with severe BPD– N=6N=6– Gestational age ranged from 27 to 33 weeks Gestational age ranged from 27 to 33 weeks – birth weight from 800 to 1730 g.birth weight from 800 to 1730 g.– Patients received Dexamethasone (0.5 mg/kg/day) or normal Patients received Dexamethasone (0.5 mg/kg/day) or normal
saline for the first 3 days, then treatment was crossed over for saline for the first 3 days, then treatment was crossed over for the next 3 days.the next 3 days.
– all six patients had improved during dexamethasone therapyall six patients had improved during dexamethasone therapy
Mammel et al. Lancet 1983.Mammel et al. Lancet 1983.

Faster weaning from ventilator and Faster weaning from ventilator and oxygenoxygen
Cummings, et al 1989Cummings, et al 1989– Double blinded study on 36 preterm infants who were Double blinded study on 36 preterm infants who were
dependent on O2 and mechanical ventilation at 2 dependent on O2 and mechanical ventilation at 2 weeksweeks
– Dexamethasone given for 42 days improved Dexamethasone given for 42 days improved pulmonary and neurodevelopmental outcome at 6 and pulmonary and neurodevelopmental outcome at 6 and 15 months of age15 months of age
O’Shea, et al 1993O’Shea, et al 1993– Longitudinal follow up on 61 preterm infantsLongitudinal follow up on 61 preterm infants– Infants had been treated with 42 day course of dex Infants had been treated with 42 day course of dex
starting at 2 weeksstarting at 2 weeks– Dex associated with fewer days of assisted ventilation Dex associated with fewer days of assisted ventilation
but not with improved outcome at age 1 but not with improved outcome at age 1

Dexamethasone became widely Dexamethasone became widely used to prevent and/or treat CLDused to prevent and/or treat CLD
– Retrospective study examining the outcome Retrospective study examining the outcome of neonates between 500 g and 749 g of neonates between 500 g and 749 g showed that 43% of infants born between showed that 43% of infants born between 1990-1992 received dexamethasone vs 84% 1990-1992 received dexamethasone vs 84% between 1993-1995.between 1993-1995.
– Hack M, Fanaroff AA. Early Hum Dev 1999Hack M, Fanaroff AA. Early Hum Dev 1999

The pendulum swings…The pendulum swings…
Dex is good, the more the better
All steroids are bad, no babies should get them
1998: Increase in 1998: Increase in neurodevelopmental dysfunctionneurodevelopmental dysfunctionYeh, et al Yeh, et al large multicenter follow-up study large multicenter follow-up study Outcomes at 2 year corrected age of infants who Outcomes at 2 year corrected age of infants who participated in a double blinded controlled trial of participated in a double blinded controlled trial of early dexamethasone for the prevention of CLDearly dexamethasone for the prevention of CLD133 children133 children marked increase in neurodevelopmental marked increase in neurodevelopmental dysfunction in neonates treated with dysfunction in neonates treated with dexamethasone compared with controlsdexamethasone compared with controls
Yeh, et al. Pediatrics 1998.Yeh, et al. Pediatrics 1998.

1999: Dexamethasone has 1999: Dexamethasone has some more side effectssome more side effects
Shinwell, et al Shinwell, et al
Long term neurodevelopmental outcome of children who Long term neurodevelopmental outcome of children who participated in early postnatal dexamethasone treatment for participated in early postnatal dexamethasone treatment for prevention of chronic lung diseaseprevention of chronic lung diseaseDexamethasone treated group associated with:Dexamethasone treated group associated with:– HypertensionHypertension– HyperglycemiaHyperglycemia– Gastrointestinal hemorrhageGastrointestinal hemorrhage– no reduction in either the incidence or severity of chronic no reduction in either the incidence or severity of chronic
lung disease or mortalitylung disease or mortality
Shinwell Es, et al. Arch Dis Child Fetal Neonatal Ed 2000Shinwell Es, et al. Arch Dis Child Fetal Neonatal Ed 2000..
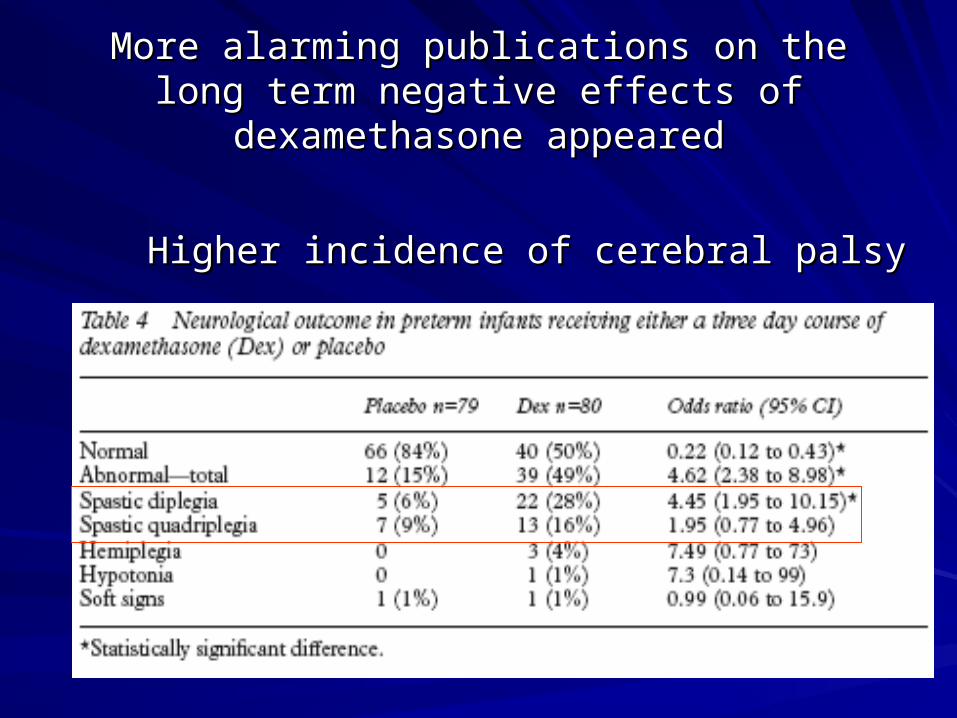
More alarming publications on the long term More alarming publications on the long term negative effects of dexamethasone appearednegative effects of dexamethasone appeared
Higher incidence of cerebral palsyHigher incidence of cerebral palsy

Reduced brain volumesReduced brain volumes
MRI study at term equivalent age showed MRI study at term equivalent age showed reduced brain volumes in infants treated reduced brain volumes in infants treated with a moderately low dose of with a moderately low dose of dexamethasone after 28 days of lifedexamethasone after 28 days of life
Parikh, et al. Pediatrics, 2007.Parikh, et al. Pediatrics, 2007.

20022002
American Academy of Pediatrics stated outside clinical American Academy of Pediatrics stated outside clinical trials, postnatal steroid use should be reserved only for trials, postnatal steroid use should be reserved only for “exceptional clinical circumstances”.“exceptional clinical circumstances”.““routine use of systemic dexamethasone for the routine use of systemic dexamethasone for the prevention or treatment of CLD in infants with VLBW is prevention or treatment of CLD in infants with VLBW is not recommended.”not recommended.”““the use of corticosteroids should be limited to the use of corticosteroids should be limited to exceptions clinical circumstances…parents should be exceptions clinical circumstances…parents should be fully informed about the known short-and long-term risks fully informed about the known short-and long-term risks and agree to treatment.”and agree to treatment.”
AAP, Committee on Fetus and Newborn. Pediatrics, 2002.AAP, Committee on Fetus and Newborn. Pediatrics, 2002.

20062006
Finer et al prospective evaluation of Finer et al prospective evaluation of postnatal steroid administration in postnatal steroid administration in California, from April 2002 to March 2003.California, from April 2002 to March 2003.
19.3% of children less than or equal to 19.3% of children less than or equal to 1500 grams were still receiving steroids.1500 grams were still receiving steroids.
Finer NN, et al. Pediatrics 2006.Finer NN, et al. Pediatrics 2006.

Dexamethasone dosing
Most previous studies started with a dose of 0.5 mg/kg/day
Lower doses (0.15 mg/kg/day) were not associated with adverse neurodevelopmental outcomes in 2 studies– Stark, et al: Early treatment (n=123)– Doyle, et al: Later extubation study (n=58)
Watterberg

Side effects seen with early Side effects seen with early Dexamethasone therapyDexamethasone therapy
Infection and sepsisInfection and sepsis
HyperglycemiaHyperglycemia
HypertensionHypertension
Cardiac hypertrophyCardiac hypertrophy
Delay in weight gainDelay in weight gain
Worse neurodevelopmental outcomesWorse neurodevelopmental outcomes

Not all steroids are the sameNot all steroids are the same
Hydrocortisone has lower potencyHydrocortisone has lower potency
Shorter half-lifeShorter half-life
Mineralocorticoid vs glucocorticoidMineralocorticoid vs glucocorticoid
In in vitro neuronal cells, dexamethasone In in vitro neuronal cells, dexamethasone stimulates apoptosis while stimulates apoptosis while mineralocorticoids, are protective against mineralocorticoids, are protective against apoptosis.apoptosis.

DexamethasoneDexamethasone HydrocortisoneHydrocortisone
Half lifeHalf life 36-72 hours36-72 hours 8-12 hours8-12 hours
SteroidSteroid GlucocorticoidGlucocorticoid MineralocorticoidMineralocorticoid
PreservativePreservative Sodium Sodium bisulphitebisulphite
No sodium No sodium bisulphitebisulphite
ApoptosisApoptosis StimulatesStimulates ProtectsProtects

Hydrocortisone for chronic lung Hydrocortisone for chronic lung diseasedisease
Six reports have been published on Six reports have been published on postnatal hydrocortisone administration for postnatal hydrocortisone administration for prevention (n=5) or treatment (n=1) of prevention (n=5) or treatment (n=1) of CLDCLD



19721972
First randomized placebo controlled trial of First randomized placebo controlled trial of hydrocortisone treatmenthydrocortisone treatmentevaluated the ability of postnatally administered evaluated the ability of postnatally administered hydrocortisone to alter the course of outcome in infants hydrocortisone to alter the course of outcome in infants with hyaline membrane disease. with hyaline membrane disease. 44 infants (mean gestational age 32.5 weeks) were 44 infants (mean gestational age 32.5 weeks) were treated with hydrocortisone or a lactose placebo within treated with hydrocortisone or a lactose placebo within 24 h after birth. 24 h after birth. no remarkable effect on PaO2, PaCO2, need for no remarkable effect on PaO2, PaCO2, need for assisted mechanical ventilation or survival.assisted mechanical ventilation or survival.
Baden, et al. Pediatrics 1972.Baden, et al. Pediatrics 1972.

27 years later…199927 years later…1999
Watterberg et al enrolled 40 preterm infants Watterberg et al enrolled 40 preterm infants into a randomised pilot study to test into a randomised pilot study to test whether hydrocortisone would increase the whether hydrocortisone would increase the likelihood of survival without CLDlikelihood of survival without CLD
started low-dose hydrocortisone within 48 started low-dose hydrocortisone within 48 hours after birthhours after birth
Treated for 12 daysTreated for 12 days
Watterberg, et al. Pediatrics 1999.Watterberg, et al. Pediatrics 1999.

ResultsResults
Among those treated with hydrocortisone, 60% Among those treated with hydrocortisone, 60% survived without supplemental oxygen at 36 survived without supplemental oxygen at 36 weeks’ PMA vs 35% in placebo group.weeks’ PMA vs 35% in placebo group.Treatment decreased number of days on:Treatment decreased number of days on:– .40% oxygen.40% oxygen– .25% oxygen.25% oxygen– Days on ventilatorDays on ventilator– Oxygen at dischargeOxygen at dischargeAdverse short term complications were similar between Adverse short term complications were similar between
the two groupsthe two groups
– Watterberg KL, Gerdes JS, Gifford KL, et al. Pediatrics 1999Watterberg KL, Gerdes JS, Gifford KL, et al. Pediatrics 1999

20032003
Retrospective matched-cohort study Retrospective matched-cohort study
compared 25 preterm infants w/ CLD who compared 25 preterm infants w/ CLD who were treated with a much higher dose of were treated with a much higher dose of hydrocortisone with 25 controlshydrocortisone with 25 controls
From day 7, no significant differences in From day 7, no significant differences in amount of extra oxygen needed between 2 amount of extra oxygen needed between 2 groupsgroupsHeide-Jalving, et al. Acta Paediatr 2003.Heide-Jalving, et al. Acta Paediatr 2003.

Watterberg 2004Watterberg 2004
Multicenter trial Multicenter trial Prophylaxis of early adrenal insufficiency Prophylaxis of early adrenal insufficiency to prevent BPDto prevent BPDEnrolled mechanically ventilated infants Enrolled mechanically ventilated infants with a birth weight of 500-999 gram infants with a birth weight of 500-999 gram infants between 12 h and 48 h of lifebetween 12 h and 48 h of life

ResultsResults
Prophylactic treatment of early adrenal Prophylactic treatment of early adrenal insufficiency did not improve survival insufficiency did not improve survival without CLD or mortality at 36 weeks.without CLD or mortality at 36 weeks.
Enrollment stopped at 360 infants Enrollment stopped at 360 infants because of an increase in spontaneous because of an increase in spontaneous gastrointestinal perforation in the gastrointestinal perforation in the hydrocortisone treated group.hydrocortisone treated group.

2005 Peltoniemi2005 Peltoniemi
effect of early hydrocortisone treatment on effect of early hydrocortisone treatment on survival without CLD in infants less than or survival without CLD in infants less than or equal to 30 weeksequal to 30 weeks
tendency towards lower CLD in the tendency towards lower CLD in the hydrocortisone treated grouphydrocortisone treated group
Study was discontinued early due to Study was discontinued early due to higher incidence of GI perforation higher incidence of GI perforation
Peltoniemi O, Kari MA, Heinonen K, et al. J Pediatr 2005.Peltoniemi O, Kari MA, Heinonen K, et al. J Pediatr 2005.

2007 Bonasarte et al2007 Bonasarte et al
Double blinded, randomised, placebo controlled Double blinded, randomised, placebo controlled trialtrial
50 mechanically ventilated infants 50 mechanically ventilated infants
Birth weights 500-1249 gramsBirth weights 500-1249 grams
Oxygen free survival was higher in the Oxygen free survival was higher in the hydrocortisone treated grouphydrocortisone treated group
No difference in GI perforation between the No difference in GI perforation between the groups groups
Bonsante F, Latorre G, Iacobelli S, et al. Neonatology 2007Bonsante F, Latorre G, Iacobelli S, et al. Neonatology 2007

Long term follow-upLong term follow-up
Few follow-up reports based on the initial Few follow-up reports based on the initial 1972 hydrocortisone trial1972 hydrocortisone trial
no differences in lung, liver, adrenal, no differences in lung, liver, adrenal, thymus, heart and spleen pathology thymus, heart and spleen pathology attributable to steroid treatmentattributable to steroid treatment
Significant association between the Significant association between the occurrence of intraventricular hemorrhage occurrence of intraventricular hemorrhage and hydrocortisone treatmentand hydrocortisone treatmentTaeusch et al. Pediatrics1973.Taeusch et al. Pediatrics1973.

24 survivors examined at 1 year of age24 survivors examined at 1 year of age
Griffiths Developmental Scale showed aGriffiths Developmental Scale showed a
normal developmental quotient in both normal developmental quotient in both groupsgroups
substantial difference in the results for the substantial difference in the results for the gross motor development with a lower gross motor development with a lower mean score for the hydrocortisone groupmean score for the hydrocortisone group

Van de Heide et alVan de Heide et al
25 preterm infants treated with high-dose 25 preterm infants treated with high-dose hydrocortisonehydrocortisone
age of 5–7 years this group did not differ age of 5–7 years this group did not differ from a non-treated control group with from a non-treated control group with regard to: regard to: – neurological outcome neurological outcome – psychomotor developmentpsychomotor development– school performanceschool performance

Watterberg et alWatterberg et al
294 survivors, 252 (86%) infants who 294 survivors, 252 (86%) infants who participated in prophylactic hydrocortisone participated in prophylactic hydrocortisone trialtrial
evaluated at the age of 20.0 monthsevaluated at the age of 20.0 months
incidence of cerebral palsy was similar incidence of cerebral palsy was similar
significantly smaller percentage of infants significantly smaller percentage of infants treated with hydrocortisone had a Mental treated with hydrocortisone had a Mental Developmental Index below 70Developmental Index below 70

Lodygensky and Rademaker 2005Lodygensky and Rademaker 2005
Follow up studyFollow up study23 preterm-born children received 23 preterm-born children received hydrocortisone treatment for chronic lung hydrocortisone treatment for chronic lung diseasediseasestarting dose of 5 mg/kg/day, tapered over a starting dose of 5 mg/kg/day, tapered over a minimum of 3 weeksminimum of 3 weeks 35 children not treated35 children not treatedquantitative MRI and neurocognitive assessment quantitative MRI and neurocognitive assessment at 8 years of ageat 8 years of ageBoth groups had similar volumes of grey matter, Both groups had similar volumes of grey matter, white matter, cerebral fluid and hippocampuswhite matter, cerebral fluid and hippocampus

Rademaker 2007Rademaker 2007
62 preterm-born children treated with 62 preterm-born children treated with hydrocortisone for CLD were compared hydrocortisone for CLD were compared with 164 children who did not receive with 164 children who did not receive steroids during their admission to the steroids during their admission to the NICUNICUmean IQ, and visual-motor integration and mean IQ, and visual-motor integration and memory test results, were similar in the memory test results, were similar in the hydrocortisone-treated and non-treated hydrocortisone-treated and non-treated groupsgroups

Karemaker et alKaremaker et al
retrospective matched-cohortretrospective matched-cohort
long-term effects on behavior and motor long-term effects on behavior and motor skills in school age (7–10 years) children skills in school age (7–10 years) children who received either dexamethasone or who received either dexamethasone or hydrocortisone for CLDhydrocortisone for CLD
dexamethasone group had more dexamethasone group had more neuromotor problems than children in the neuromotor problems than children in the control group control group

Puzzled yet?Puzzled yet?

SummarySummary
In long-term follow-up studies at 5–8 years In long-term follow-up studies at 5–8 years of age preterm infants not treated with of age preterm infants not treated with hydrocortisone compared with those who hydrocortisone compared with those who were treated for CLD, no differences have were treated for CLD, no differences have been found:been found:– in neurocognitive or motor outcomein neurocognitive or motor outcome– incidence of brain abnormalities on MRIincidence of brain abnormalities on MRI

SummarySummary
2 prophylactic hydrocortisone studies, 2 prophylactic hydrocortisone studies, stopped early due to increased incidence stopped early due to increased incidence of spontaneous GI perforation with of spontaneous GI perforation with combined indomethacin txcombined indomethacin tx
two publications reported an increased risk two publications reported an increased risk of disseminated Candida infections in of disseminated Candida infections in infants treated with hydrocortisoneinfants treated with hydrocortisone

SummarySummary
Moderately early steroid treatment can result in Moderately early steroid treatment can result in reductions in:reductions in:– Failure to extubateFailure to extubate– CLDCLD– Neonatal mortalityNeonatal mortality
Risks of short term and potentially long term Risks of short term and potentially long term adverse effectsadverse effects– Limited long term outcomes, especially in school age Limited long term outcomes, especially in school age
childrenchildren

SummarySummary
modify the dosagemodify the dosage
Limit the drug–drug interactions Limit the drug–drug interactions
Scrutinise patient selection in Scrutinise patient selection in corticosteroid trials on very high-riskcorticosteroid trials on very high-risk
infants in early life infants in early life
Treat beyond 2 weeks of postnatal age to Treat beyond 2 weeks of postnatal age to avoid the interactive effect of avoid the interactive effect of hydrocortisone with indometacin hydrocortisone with indometacin

Questions?

ReferencesReferencesMammel MC, Green , Johnson, et al. Controlled trial of dexamethasone therapy in infants with bronchopulmonary Mammel MC, Green , Johnson, et al. Controlled trial of dexamethasone therapy in infants with bronchopulmonary dysplasia. dysplasia. LancetLancet 1983; 1:1356-8. 1983; 1:1356-8.Yeh, et al. Outcomes at school age after postnatal dexamethasone therapy for lung disease of prematurity. Yeh, et al. Outcomes at school age after postnatal dexamethasone therapy for lung disease of prematurity. N N Engl J MedEngl J Med 2004;350:1304-13. 2004;350:1304-13.Yeh, et al. Early dexamethasone therapy in preterm infants: a follow-up study. Yeh, et al. Early dexamethasone therapy in preterm infants: a follow-up study. PediatricsPediatrics 1998;101:E7. 1998;101:E7.Shinwell Es, et al. Early postnatal dexamethasone treatment and increased incidence of cerebral palsy. Shinwell Es, et al. Early postnatal dexamethasone treatment and increased incidence of cerebral palsy. Arch Dis Arch Dis Child Fetal Neonatal EdChild Fetal Neonatal Ed 2000. 2000.AAP, Committee on Fetus and Newborn. Pediatrics, 2002.AAP, Committee on Fetus and Newborn. Pediatrics, 2002.Finer NN, et al. Finer NN, et al. PediatricsPediatrics 2006. 2006.Parikh, et al. Postnatal dexamethasone therapy and cerebral tissue volumes in extremely low birth weight Parikh, et al. Postnatal dexamethasone therapy and cerebral tissue volumes in extremely low birth weight infants. Pediatrics, 2007; 119:265-72.infants. Pediatrics, 2007; 119:265-72.Baden, et al. A controlled trial of hydrocortisone therapy in infants with respiratory distress syndrome. Pediatrics Baden, et al. A controlled trial of hydrocortisone therapy in infants with respiratory distress syndrome. Pediatrics 1972, 50:526-34.1972, 50:526-34.Heide-Jalving M, Kamphuis PJ, van der Laan MJ, et al. Short- and long-termHeide-Jalving M, Kamphuis PJ, van der Laan MJ, et al. Short- and long-term
effects of neonatal glucocorticoid therapy: is hydrocortisone an alternative to dexamethasone? Acta Paediatr effects of neonatal glucocorticoid therapy: is hydrocortisone an alternative to dexamethasone? Acta Paediatr 2003;92:827–35.2003;92:827–35.Watterberg KL, Gerdes JS, Gifford KL, et al. Prophylaxis against early adrenal insufficiency to prevent chronic Watterberg KL, Gerdes JS, Gifford KL, et al. Prophylaxis against early adrenal insufficiency to prevent chronic lung disease in premature infants. Pediatrics1999;104:1258–63.lung disease in premature infants. Pediatrics1999;104:1258–63.
Hack M, Fanaroff AA. Outcomes of children of extremely low birthweight and gestational age in the 1990s. Early Hack M, Fanaroff AA. Outcomes of children of extremely low birthweight and gestational age in the 1990s. Early Hum Dev 1999;53:193–218.Hum Dev 1999;53:193–218.

References cont.References cont.
Watterberg KL, Gerdes JS, Gifford KL, et al. Prophylaxis against Watterberg KL, Gerdes JS, Gifford KL, et al. Prophylaxis against early adrenal insufficiency to prevent chronic lung disease in early adrenal insufficiency to prevent chronic lung disease in premature infants. Pediatrics 1999;104:1258–63.premature infants. Pediatrics 1999;104:1258–63.Watterberg KL, Gerdes JS, Cole CH, et al. Prophylaxis of early adrenal Watterberg KL, Gerdes JS, Cole CH, et al. Prophylaxis of early adrenal insufficiency to prevent bronchopulmonary dysplasia: a multicenter trial. insufficiency to prevent bronchopulmonary dysplasia: a multicenter trial. Pediatrics 2004;114:1649–57.Pediatrics 2004;114:1649–57.Peltoniemi O, Kari MA, Heinonen K, et al. Pretreatment cortisol values may Peltoniemi O, Kari MA, Heinonen K, et al. Pretreatment cortisol values may predict responses to hydrocortisone administration for the prevention of predict responses to hydrocortisone administration for the prevention of bronchopulmonary dysplasia in high-risk infants. J Pediatr 2005;146:632–7.bronchopulmonary dysplasia in high-risk infants. J Pediatr 2005;146:632–7.Bonsante F, Latorre G, Iacobelli S, et al. Early low-dose Bonsante F, Latorre G, Iacobelli S, et al. Early low-dose hydrocortisone in very preterm infants: a randomized, placebo-hydrocortisone in very preterm infants: a randomized, placebo-controlled trial. Neonatology 2007;91:217–21controlled trial. Neonatology 2007;91:217–21Taeusch HW Jr, Wang NS, Baden N, et al. A controlled trial of Taeusch HW Jr, Wang NS, Baden N, et al. A controlled trial of hydrocortisone therapy in infants with respiratory distress syndrome: hydrocortisone therapy in infants with respiratory distress syndrome: II. Pathology. Pediatrics 1973;52:850–4.II. Pathology. Pediatrics 1973;52:850–4.