Embed Size (px)
Citation preview

Controlling Antimicrobial-Resistant Infections: MRSA & VRE
Barry M. Farr, MD, MSc
University of Virginia Health System
Charlottesville, VA

Trends of prevalence rates for penicillinase-producing MSSA in hospitals and the community
0
10
20
30
40
50
60
70
80
90
100
Year
% R
esis
tan
t
Hospital Community

Mechanisms Of Developing Antibiotic Resistance
1. Random genetic mutation.
2. Plasmid swapping during conjugation.
3. Movement of transposons to plasmids/chromosomes.
4. Transduction by bacteriophages.
5. Transformation (acquisition of resistant genes from a recently killed cell and incorporation into a chromosome or plasmid).
6. Binary fission (replication) can share any of the above.

Natural Selection
Mechanisms Of Developing Antibiotic Resistance
Darwin C. On the Origin of Species by Means of Natural Selection, London, 1859.

Univariate Analysis Of Antibiotic Exposure
Cases Controls p value
Vancomycin 46% 36% 0.219
Metronidazole 43% 21% 0.004
Clindamycin 31% 28% 0.755
Amp/sulbactam 27% 15% 0.073
Ticar/clav. 20% 14% 0.357
Imipenem 5% 4% 0.694
Ciprofloxacin 34% 24% 0.183
3rd gen. Ceph. 65% 50% 0.092
Aminoglycoside 45% 39% 0.492aminoglyco side

VRE Incidence Week
Hospital Ward 1 2 3 4
6th Floor ICU 0 0 0 0 Step-down Unit 0 0 0 0
5th Floor ICU 2 1 0 0 Step-down Unit 4 2 1 1
3rd Floor ICU 1 1 1 0 Step-down Unit 6 3 0 1
Byers KE, et al. ICHE 2001;22(3):140-147.


Transmission Of IndividualClones Of VRE
Boyce, J Cin Micro 1994;32:1148.Dembry, SHEA 1994 Abstract #28.Edmond, Clin Infect Dis 1995;20:1126.Handwerger, Clin Infect Dis 1993;16:750.Livornese, Ann Int Med 1992;117:112.Montecalvo, Anti Ag Chemo 1994;38:1363.Rubin, Infect Cont Hosp Epi 1992;13:700.


0
10
20
30
40
50
60
1989 1990 1991 1992 1993 1994 1995 1996 1997 1999
Year
% S
. au
reu
s r
esis
tan
t to
m
eth
icil
lin
Non-ICU ICU
Fridkin. Fridkin. Clin Chest MedClin Chest Med. 1999;20(2):303. 1999;20(2):303..Fridkin. Fridkin. Clin Chest MedClin Chest Med. 1999;20(2):303. 1999;20(2):303..ICU=intensive care unitICU=intensive care unitICU=intensive care unitICU=intensive care unit
MRSA Isolates From ICUs vs Non-MRSA Isolates From ICUs vs Non-ICUsICUs
MRSA Isolates From ICUs vs Non-MRSA Isolates From ICUs vs Non-ICUsICUs

Failure To Prevent MRSA Spread
1977 1979 1980
Pneumonia 0% 19% 24%
Blood stream infection
0% 13% 40%
Surgical site infection
0% 27% 49%
• Thompson et al. found that despite isolation of patients known to have MRSA from clinical cultures, the prevalence of MRSA infection continued to increase.
Thompson RL, Ann Intern Med 1982;97:309

0
5
10
15
20
25
30
35
D-80 J-81 F-81 M-81 A-81 M-81 J-81 J-81 A-81 S-81 O-81 N-81
New Cases Prevalence
Date
Cas
es
Incidence ( p < 0.002) and Prevalence (p < 0.001)
Control of MRSA Using Active Surveillance Cultures and Contact Precautions

MRSA (which had been out of control for 2.5 years) Was Completely Eradicated from the Hospital
Within 1.5 years
This was done with no antibiotic control effort of any kind.

Reservoir for the Spread of Antibiotic Resistant Pathogens
Clinical Infections
Colonized Patients

Prevalence of MRSA Colonization During the Outbreak
0
1
2
3
4
5
6
7
8
July Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
1991 1992
Nu
mb
er
of
Co
lon
ize
d P
ati
en
ts
= Index Case
= Acquired MRSA from unisolated patient
= Acquired MRSA from isolated infant

Follow-up After Control of MRSA Outbreak in NICURSA in any patient during the next 10 years and about 100,000 patient-days.
This suggests a low frequency of de novo development of methicillin resistance despite prolonged hospital stay and frequent antibiotic therapy in the NICU.
It also suggests a very low rate of MRSA colonization among NICU workers and mothers in central Virginia.

Control of 2 MRSA NICU Outbreaks Using ASC and Barrier Precautions
Without Antibiotic ControlFirst outbreak in a 50-bed NICU controlled over several months
32 colonized over 5 weeks
5 colonized infants (16%) became infected and one died of MRSA BSI.
2nd outbreak of 14 colonized and 4 infected (29%) (with another death due to MRSA BSI) controlled in less than one month.
Back NA, et al. ICHE 1996;17:227-231.

HaleyRW et al, JID 1995;171:614-624.

Countries Controlling MRSA to < 1% of Nosocomial S. aureus Infections Using ASC and Barrier Precautions
Denmark
Netherlands
Finland
(Belgium has started and rate is falling)

Methicillin
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96
Penicillin
Tetracycline
Fusidic AcidGentamicinCiprofloxacin
Erythromycin
Year
Antimicrobial Resistance Surveillance in Staphylococcus aureus blood isolates, Denmark, 1960-1995
Source: DANMAP Report, 1997.
Stap
hyl
ococ
cus
aure
us A
nti
mic
robi
al R
esis
tanc
e

0
5
10
15
20
25
30
89 90 91 92 93 94 95 96 97 98 99
Year
% V
an
co
mycin
-Resis
tan
t E
nte
roco
cci
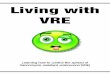
Percentage of Nosocomial Enterococci Reported as Resistant to Vancomycin,
by Year
*National Nosocomial Infections Surveillance (NNIS) System Data, 1989-1999.

Byers KE et al. ICHE 2001;22:140-7.

Follow-up After Control of VRE in ICU Reaching 100% Prevalence Early in Outbreak
Prevalence rapidly decreased to 0%. No VRE isolated from any patient in the ICU during the next year despite weekly cultures of all patients at risk and the lack of an antibiotic control program.
This suggests a low frequency of de novo mutation to vancomycin resistance despite prolonged hospital stay and frequent antibiotic therapy.

Relationship Between Antibiotic Therapy and Development of VRE
Culture Positivity
“Antibiotics alone will not select for VRE if resistant bacteria are not already present or if a patient does not come into contact with them.”
Murray BE. NEJM 2000;342:710-721.

Control of VRE with Active Surveillance Cultures and Contact Isolation in California Hospital

VRE compliance and positivity rates
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
Week
Com
plia
nce
rate
0%
5%
10%
15%
20%
25%
30%
35%
VR
E p
ositi
vity
rat
e
COMP RATE POS RATE Linear (POS RATE) Linear (COMP RATE)
Week 45
0 20
40 60
Muto CA, et al. IDSA 2001, abstract 210, p. 75.

VRE Prevalence in 30 Healthcare Facilities, Siouxland, 1997 vs 1999
Facility Number (%) VRE-Colonized 1997 1999 Relative p-value Risk
All 40 (2.2) 9 (0.5) 0.23 <0.001
Acute Care 10 (6.6) 0 0 <0.001
Long-TermCare
30 (1.8) 9 (0.5) 0.31 0.001
Ostrowsky BE, et al., NEJM 2001;344:1427-1433.

MRSA BSI
VRE BSI
A B C D E F UVA
Hospital
No
. o
f B
SI
in 1
99
9VRE and MRSA Bacteremias at Hospitals of
Comparable Size and Complexity, 1999
Calfee DP,et al.SHEA 2001, abstract 127, p 66.

Control of VRE Using Active Surveillance Cultures and
Contact PrecautionsKaranfil LV. ICHE 1992; 13: 195 Byers KE. ICAAC 1995 Boyce J. J Clin Micro 1994; 32: 1148 Rubin LG. ICHE 1992; 13: 700 Montecalvo M. AAC 1994; 38: 1363 Dembry L. ICHE 1996; 17: 2 Rupp ME. SHEA 1998; Abst. 54, p34 Malik RK. PIDJ 1999; 18: 352 Muto CA. SHEA 1998 Trick W. JID 1999; 180: 391 Jochimsen E. ICHE 1999; 20: 106 Calfee DP. SHEA 2000; Abst. P-T2-69, p217 Sohn A. SHEA 2000; Abst. S-Th-04, p261 Livornese LL. Ann Int Med 1992; 117: 112

STUDIES REPORTING FAILURE OF INFECTION CONTROL MEASURES TO CONTROL VRE
# of Wards on which Active Surveillance Cultures were Used:
Study: # Wards: % of Hospital Beds:
1 0 0% 2 1 <3% 3 2 <5% 4 4 ?
Slaughter Ann Int Med 1996;125:448.Morris Ann Int Med 1995;123:250.
Goetz, et al. AJIC 1998;26:558.Quayle, et al. CID 1996;23:1020.

Source of New VRE Cases in a Hospital with a High VRE Prevalence and Polyclonality
Molecular epidemiologic analysis showed that establishmentof endemicity had been mostly due to clonal spread with accumulation of new strains over time.
Kim NJ et al. JID 1999;179:163.

Source of New VRE Cases in a Medical ICU with a High VRE Prevalence and Polyclonality
The proportion of other patients with VRE was the most important risk factor for new patients becoming culture positive for VRE. In multivariable analysis, this was a more important predictor than other variables found to be significant in univariate analysis such as therapy with third generation cephalosporins.
Bonten MJ et al. Arch Int Med 1998;158:1127.

Another Explanation of VRE Polyclonality Despite Documentation of
Patient to Patient Spread
Transposons (e.g., TN 5482) spread from Enterococcus to Enterococcus to chromosomes or plasmids by conjugation.
de Lancastre, et al. Microbial Drug Resistance 1999;5:113.

Can Hand Hygiene/ Standard Precautions Control MRSA and VRE Infections (i.e., without using ASC
and barrier precautions)?1. Hand hygiene rates in most hospitals have not changed
since implementation of universal (standard) precautions.
2. Pittet showed decrease in MRSA with increase in hand hygiene, but with much bigger increase in ASC and CP for colonized patients. Lancet 2000;356:1307-12. J Hosp Infect 2000;46:43-9.
3. Larson reported significant 85% relative reduction in VRE but 44% drop in control hospital and no significant change in MRSA in same hospital with increase in hand hygiene. Behav Med 2000;26:14-22.

Can Hand Hygiene/ Standard Precautions Control MRSA and VRE Infections?
4. Austin et al reported that 80% compliance with hand hygiene would result in relative reduction in VRE prevalence of about 25% (PNAS 1999;96:6908-13).
5. Sebille et al reported that increasing hand hygiene compliance to 90% would only reduce MRSA prevalence by 33%. They recommended ASC and CP (ICHE 1997;18:84-92).
6. Some have claimed that switching to triclosan handwash alone ended 2 MRSA NICU outbreaks, but both used multiple measures and reported continuing “all IC measures” (e.g., one used weekly ASC and and the other used gowns, gloves, cohorting and bathing of every neonate with triclosan). Webster J et al, J Paed Child Health 1994;30:59-64. Zafar AB et al, AJIC 1995;3:200-8..

Rates of MRSA Transmission
Source
Isolated Unisolated
Transmissions 5 10
Patient-days 558 71.5
Rates 0.009 0.140
RR=15.6, 95% CI=5.3-45.6, p<0.0001
Jernigan, et al. Am J Epi 1996;143:496-504.

Conditional Logistic Regression Analysis
Variable OR P
Proximity to unisolated 2.04* 0.0014VRE patients
History of major trauma 9.27 0.020
Metronidazole therapy 3.04 0.040
* Per exposure-unit
Byers KE et al. ICHE 2001;22:140-7.

0
10
20
30
40
50
60
1989 1990 1991 1992 1993 1994 1995 1996 1997 1999
Year
% S
. au
reu
s r
esis
tan
t to
m
eth
icil
lin
Non-ICU ICU
Fridkin. Fridkin. Clin Chest MedClin Chest Med. 1999;20(2):303. 1999;20(2):303..Fridkin. Fridkin. Clin Chest MedClin Chest Med. 1999;20(2):303. 1999;20(2):303..ICU=intensive care unitICU=intensive care unitICU=intensive care unitICU=intensive care unit
MRSA Isolates From ICUs vs Non-MRSA Isolates From ICUs vs Non-ICUsICUs
MRSA Isolates From ICUs vs Non-MRSA Isolates From ICUs vs Non-ICUsICUs
UPSP

0
5
10
15
20
25
30
89 90 91 92 93 94 95 96 97 98 99
Year
% V
an
co
mycin
-Resis
tan
t
En
tero
co
cci
Percentage of Nosocomial Enterococci Reported as Resistant to Vancomycin,
by Year
*National Nosocomial Infections Surveillance (NNIS) System Data, 1989-1999.
UP SP

ISOLATION GOWNS PREVENT HCWs FROM CONTAMINATING THEIR
CLOTHES/HANDS14 (40%) of 35 HCWs’ gowns were culture (+) for MRSA and ARE on exiting room (2-200 colonies recovered). Clothing underneath was culture (-). 11 (69%) of 16 HCWs wearing freshly laundered white coats had detectable contamination. 3 of 11 developed (+) hand cultures after touching the white coat.
Boyce, et al. SHEA 1998, Abstract S74.

CONTAMINATION OF GOWNS, GLOVES AND STETHOSCOPES
•Two thirds of examinations of VRE patients resulted in VRE contamination of gown, gloves and/or stethoscopes.
•Same rate of contamination whether the patient was infected or merely colonized.
Zachary KC et al. 4th Decennial Conference on Nosocomial Infections, Atlanta, p. 75.

11Boyce. Boyce. Infect Control Hosp Epidemiol.Infect Control Hosp Epidemiol. 1997;18:622.1997;18:622.2 2 Cohen. Cohen. Fam PractFam Pract. 1997;14:446. 1997;14:4463 3 Marinella. Marinella. Arch Intern MedArch Intern Med. 1997;157:786. 1997;157:786..
11Boyce. Boyce. Infect Control Hosp Epidemiol.Infect Control Hosp Epidemiol. 1997;18:622.1997;18:622.2 2 Cohen. Cohen. Fam PractFam Pract. 1997;14:446. 1997;14:4463 3 Marinella. Marinella. Arch Intern MedArch Intern Med. 1997;157:786. 1997;157:786..
Environmental MRSA ContaminationEnvironmental MRSA ContaminationEnvironmental MRSA ContaminationEnvironmental MRSA Contamination• 70% of rooms had environmental contamination 70% of rooms had environmental contamination
when the patient was colonized or infected and 42% when the patient was colonized or infected and 42% of nurses’ gloves were contaminated after touching of nurses’ gloves were contaminated after touching environmental surfaces without touching patient.environmental surfaces without touching patient.11
• 7% of stethoscopes were contaminated with MRSA7% of stethoscopes were contaminated with MRSA22
– Wiping with 70% isopropyl alcohol significantly reduced Wiping with 70% isopropyl alcohol significantly reduced colony counts on stethoscopes (p < 0.02).colony counts on stethoscopes (p < 0.02).33
• Contaminated surfaces include patient’s gowns, Contaminated surfaces include patient’s gowns, floor, bed linens, blood pressure cuffs, overbed floor, bed linens, blood pressure cuffs, overbed tables, stethoscopes, etc.tables, stethoscopes, etc.11
• 70% of rooms had environmental contamination 70% of rooms had environmental contamination when the patient was colonized or infected and 42% when the patient was colonized or infected and 42% of nurses’ gloves were contaminated after touching of nurses’ gloves were contaminated after touching environmental surfaces without touching patient.environmental surfaces without touching patient.11
• 7% of stethoscopes were contaminated with MRSA7% of stethoscopes were contaminated with MRSA22
– Wiping with 70% isopropyl alcohol significantly reduced Wiping with 70% isopropyl alcohol significantly reduced colony counts on stethoscopes (p < 0.02).colony counts on stethoscopes (p < 0.02).33
• Contaminated surfaces include patient’s gowns, Contaminated surfaces include patient’s gowns, floor, bed linens, blood pressure cuffs, overbed floor, bed linens, blood pressure cuffs, overbed tables, stethoscopes, etc.tables, stethoscopes, etc.11

Rates of Persistent Environmental VRE Contamination
Conventional 60/376 = 15.9%
Bucket 0/135 = 0%
Chi Square = 25.7
p < 0.001
Byers KE et al. ICHE 1998;19:261-4.

Excess Cost of MRSA Infection
MRSA infections cost significantly more than MSSA infections.
Engelmann J et al, ICAAC 2001 abst. K-2056, p. 441.
Cosgrove SE et al, ICAAC 2001 abst. K-1221, p. 415.
Abramson, ICHE 1999;20:408.
Wakefield, AJIC 1988;16:185-192.
Cheng, J Hosp Infect 1988;12:91-101.

Comparison of Primary MSSA and MRSA Nosocomial Bloodstream
Infections
MSSA MRSA P-value
Attributable excess lengthof stay median, days
4 12 0.023
Attributable total costmedian
$9,661 $27,083 0.043
Attributable variable directcost median
$4,989 $14,783 0.043
Abramson, ICHE 1999;20:408.

Costs Of VRE Bacteremia
•VRE bacteremia associated with significant increases in length of stay (p=0.004), and hospital costs (more than $27,000 per episode, p=0.04).1
•VRE BSI associated with 19-day increase in length of stay (p<0.001), and increased hospital costs ($79,589 per episode, p<0.001).2
1) Stosor V, et al., Arch Int Med 1998;158:522.
2) Song X, et al, 37th IDSA, 1999, abstract 500, p 126.

Studies Reporting Cost Benefit of Surveillance Cultures and Contact Precautions for
Controlling MRSA & VRE
Chaix, et al. JAMA 1999;282:1745.
Jernigan JA, et al. ICHE 1995;16:686.
Montecalvo MA, et al. ICHE 2001 July;22:437-42.
Karchmer TB et al, J Hosp Infect. In press.
Muto CA et al, SHEA 1999 abstract 74, p. 44.
Calfee DP, et al. SHEA 2001, abstract 127, p 66.

•Association with death was almost two-fold Association with death was almost two-fold higher for MRSA bloodstream infections than for higher for MRSA bloodstream infections than for MSSA BSI (OR=1.9, 95% CI, 1.5,2.4, pMSSA BSI (OR=1.9, 95% CI, 1.5,2.4, p < 0.001) < 0.001) after adjustment for severity of illness in a recent after adjustment for severity of illness in a recent meta-analysis.meta-analysis.
Cosgrove. SHEA 2001. Abstract #96Cosgrove. SHEA 2001. Abstract #96..
Attributable Mortality of MRSA Bacteremia

Mortality with S. aureus Pneumonia
MRSA 54.5%
MSSA 2.6%
(RR=20.7, 95% CI=2.8-154)
Rello, Am J Resp Crit Care Med 1994;150:1545.

Factors Independently Associated with Mortality Among Patients with Pneumonia
due to S. aureus
Factor OR 95% CI
Septic Shock 61.5 5.63-672.2
Vancomycintreatment
14.5 1.43-145.6
RespiratoryDistress
8.3 1.47-46.1
Gonzalez, et al. CID 1999;29:1171.

Attributable Morbidity and Mortality Of VRE Bacteremia
Compared to VSE, available data suggest Compared to VSE, available data suggest that VRE bacteremia has:that VRE bacteremia has: higher rates of recurrencehigher rates of recurrence
16.9% vs. 3.7% 16.9% vs. 3.7% pp<0.0001<0.0001 higher crude case fatality rateshigher crude case fatality rates
RR=2.57 [95%CI= 2.27-2.91]RR=2.57 [95%CI= 2.27-2.91] higher mortality due to bacteremia per sehigher mortality due to bacteremia per se
RR=1.79 [95%CI= 1.28-2.50]RR=1.79 [95%CI= 1.28-2.50]
Salgado, CD. SHEA 2002, Abstract #113.Salgado, CD. SHEA 2002, Abstract #113.

Studies Comparing VRE and VSE Studies Comparing VRE and VSE Bacteremic Patients Matched for Bacteremic Patients Matched for
Severity of IllnessSeverity of Illness
STUDY SAMPLE SIZE
CASE FATALITY RATE (%) ATTRIBUTABLE MORTALITY
*Jernigan J. IDSA 1996;Pg 219
13 VRE BSI 7 VSE BSI
VRE VSE 6/13(46) 0/7(0) p=.05
46%
**Stosor V. Arch IM 1998;158
21 VRE BSI 32 VSE BSI
VRE VSE 8/21(38) 3/32(9) p=.01
29%
*Lodise T. CID 2002;34
53 VRE BSI 53 VSE BSI
VRE VSE 20/53(38) 11/53 (21) p=.05
17%
**Patients matched by APACHE II ScorePatients matched by APACHE II Score****Patients matched by other severity of illness scorePatients matched by other severity of illness score
Salgado, CD. SHEA 2002, Abstract #113.Salgado, CD. SHEA 2002, Abstract #113.

Multivariable Analyses of Mortality Risks Multivariable Analyses of Mortality Risks for Enterococcal Bacteremiafor Enterococcal Bacteremia
• Of 10 multivariate analyses of patients with Of 10 multivariate analyses of patients with enterococcal bacteremia, enterococcal bacteremia, – 3 reported no elevated risk of death associated 3 reported no elevated risk of death associated
with vancomycin resistancewith vancomycin resistance– 3 reported an elevated risk of death with 3 reported an elevated risk of death with
vancomycin resistance that was not statistically vancomycin resistance that was not statistically significant but with wide 95% CIssignificant but with wide 95% CIs
– 4 reported a significantly elevated risk of death 4 reported a significantly elevated risk of death (with similar ORs to 3 other studies). These 4 (with similar ORs to 3 other studies). These 4 studies tended to be larger and have greater studies tended to be larger and have greater statistical power than the negative studies. statistical power than the negative studies.
Salgado, CD. SHEA 2002, Abstract #113.Salgado, CD. SHEA 2002, Abstract #113.

0
10
20
30
40
50
60
1989 1990 1991 1992 1993 1994 1995 1996 1997 1999
Year
% S
. au
reu
s r
esis
tan
t to
m
eth
icil
lin
Non-ICU ICU
Fridkin. Fridkin. Clin Chest MedClin Chest Med. 1999;20(2):303. 1999;20(2):303..Fridkin. Fridkin. Clin Chest MedClin Chest Med. 1999;20(2):303. 1999;20(2):303..ICU=intensive care unitICU=intensive care unitICU=intensive care unitICU=intensive care unit
MRSA Isolates From ICUs vs Non-MRSA Isolates From ICUs vs Non-ICUsICUs
MRSA Isolates From ICUs vs Non-MRSA Isolates From ICUs vs Non-ICUsICUs

Methicillin
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96
Penicillin
Tetracycline
Fusidic AcidGentamicinCiprofloxacin
Erythromycin
Year
Antimicrobial Resistance Surveillance in Staphylococcus aureus blood isolates, Denmark, 1960-1995
Source: DANMAP Report, 1997.
Stap
hyl
ococ
cus
aure
us A
nti
mic
robi
al R
esis
tanc
e

Estimated Deaths Due To Antimicrobial Resistant Infections Compared With Deaths Due To Tuberculosis In The United States
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
1992 1993 1994 1995 1996 1997 1998 1999
Year
Nu
mb
er
Of
De
ath
s
TB Deaths
ARI Deaths

Methicillin
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96
Penicillin
Tetracycline
Fusidic AcidGentamicinCiprofloxacin
Erythromycin
Year
Antimicrobial Resistance Surveillance in Staphylococcus aureus blood isolates, Denmark, 1960-1995
Source: DANMAP Report, 1997.
Stap
hyl
ococ
cus
aure
us A
nti
mic
robi
al R
esis
tanc
e